Embed Size (px)
Citation preview

Viral Gastroenteritis –
patient management and the need for rapid
diagnostics
Susan Feeney
Regional Virus Lab, BHSCT
September 2017

Viral gastroenteritis
5 significant
enteric
pathogens
1. Faecal Adenovirus family Adenoviridae
Serogroups 40 41
Non-enveloped DNA virus
Infant association
Nosocomial associations in CH Haematology
2. Astrovirus , family Astroviridae
Non-enveloped RNA virus
May be asymptomatic
Infant association
90% children antibody by age 9
3. Sapovirus, family Caliciviridae
Non-enveloped RNA virus
Mild gastroenteritis
Infant association
4. Rotavirus, family Reoviridae
dsRNA non-enveloped, segmented virus
>90% antibody positive by age 5
Sept 2013 Rotarix Vaccine UK
Oral vaccine at 8 and 12 weeks
85% efficacy
2014, 2015, 2016 reported cases
fell by 70%
5. Norovirus, family Caliciviridae
RNA non-enveloped virus
Most common cause gastroenteritis
Affects all ages
Associated with outbreaks in closed
Or semi-closed environments
5 Genogroups , GI GII human associated

Diagnostics
EM
ELISA
IF

Virology Enterics:
Taqman™ real time PCR in-house (LDT) Norovirus/IC; Rotavirus/IC, Adenovirus/Astrovirus/IC.
Approx 4000 faeces/vomit specimens per year

Seasonal distribution of Norovirus GI/GII positive
specimens in both paediatric (Yellow) and adult (Blue)
population over a three year period March 2014-February
2016.
Paediatric yellow
Adult Blue
‘Winter Vomiting Bug’

EntericBio Realtime Norovirus Assay
The Serosep EntericBio Norovirus real time assay is a recently released semi-automated, CE-marked assay.
Taqman™ PCR assay for the qualitative detection of NoVs genogroup I and II in faecal specimens.
Employs a novel system for liberation of nucleic acid directly from faecal samples and does not require nucleic acid extraction and purification steps.
PCR assays are internally controlled and set-up is from pre-dispensed, lyophilized mastermix test strips.
This system offers speed (46 specimens <3hrs), minimal hands-on and LIMs interfacing to ensure optimum turn-around with patient safety and result reliability as priority.

Assay Steps
Faecal sample is re-suspended in EntericBio realtime SPS solution
Heat Treat 103°C (30 min)
Centrifuge (1 min)
No Extraction! No associated Instrumentation.. No associated Maintenance.. No associated Consumables.. No associated Reagents.. No Time lost on extraction run!

Shake (1 min)
Centrifuge (1 min)
PCR Set-up:
Eppendorf transfer of faeces suspension to PCR
strips containing predispensed mastermix (30 min)
LightCycler 480 (Roche) PCR (1 hr)
Automated EnterBio Realtime macro analysis.
Multicentre Clinical Validation
Clinical validation of this system was carried out through a series of retrospective and prospective test trials completed in the North and South of Ireland:
site 1. Belfast
site 2. Cork
site 3. Limerick
All sites carried out both ‘Retrospective’ studies using stored samples, and ‘Prospective’ studies using fresh faeces tested in real time.
The specimens were ran in parallel with Reference Lab Taqman® assays as Gold standard (RVL Belfast, NVRL Dublin).
Discrepant results retested with EntericBio and confirmed using gene RealStar®Norovirus RT-PCR Kit 2.0 (Altona) – extraction based internally controlled kit for detection of GI and GII
(Retrospective and Prospective)
Retrospective Trail
Retrospective testing (using stored faecal and vomitus specimens)
Samples which had been positive for Norovirus using routine in-house Norovirus LDT assay were collected and frozen (-80 °C),
Frozen samples were slowly thawed overnight in a fridge and vortexed before testing using EntericBio Realtime Norovirus Assay

Prospective Trail
Inclusion: Routine specimens from patients presenting with symptoms of norovirus infection, and requesting Norovirus studies
Samples were tested using EntericBio Realtime Norovirus Assay in parallel with routine testing using the in-house Taqman ™ assay on the Flow system (Roche) platform on the same day (Belfast), and by Taqman ™ assay at NVRL (Dublin) .

Multicentre clinical validation
Over the three sites a total of 985 samples were tested; 275 retrospectively and 710 prospectively.
Both GI and GII targets amplified, and both faeces and vomit samples were processed during validation.
Discrepant specimens were retested with EntericBio® and also tested alternative CE-marked commercial kit (Altona Real-Star).
Majority of discordant results between both methods had high Ct values.

Non-extraction based
EntericBio PCR:
n=275 PCR Positive PCR Negative
Extraction
based
Reference
Lab
PCR:
PCR Positive 139 4*
PCR Negative 0 132
Retrospective study – frozen samples:
Retrospective results: specificity 1.00; sensitivity 0.97, PPV 1.00 and NPV 0.97

Retrospective discrepant analysis
• 4* samples (1.4%) testing as Negative with EntericBio® were from the one test site.
• All Four were retested through the EntericBio® process and confirmed as negative.
Discrepant PCR analysis with extraction based Altona™ kit - only positive for 1 of the 4, with a high Ct 37.29.
These retest results illustrate that very weak, frozen samples may be borderline in detection, even with extraction based assays.

PCR Analysis
1.Controls
within range
2. Curves smooth
And sigmoidal ‘S’ In shape
3. CT value within accepted range (typically < CT35/36)

Non-extraction based
EntericBio PCR
n=710 PCR Positive PCR Negative
Extraction-
Based
Reference
Lab PCR
PCR Positive 170 3**
PCR Negative 7# 530
Prospective study – fresh samples:
Prospective Results : sensitivity 0.98 , specificity 0.99, PPV 0.96 and NPV 0.99

Prospective discrepant analysis
3 ** samples (0.4%) tested as Negative with EntericBio®
Retested with EntericBio®, one of the three became positive with Norovirus GII.
All three tested positive for Norovirus GII with Altona™ extraction based commercial method.
Of the 7# (0.98%) EntericBio® tested as positive:
four were GI (Ct 30.62, 36.91, 38.13 and 40.63)
No GI repeated with EntericBio®, Ref lab or Altona™.
Total 4 false positive GI
Of the three GII (Ct 20.59, 32.77 and 33.94), only one failed to repeat with either EntericBio® or Altona™(CT 33.94)
Total 1 false positive GII, 2 false negative with LDT

Results Breakdown
Norovirus GI 11% of total Positives
belonged to GI
90% Faeces , 10% Vomit
Ct range –
EntericBio Realtime Norovirus Assay
(17.93-27.43)
In-house Taqman ™ assay (22.19-31.8)
Result Breakdown
Norovirus GII 86% of total positives belonged to
GII
85% Faeces, 15% vomit
Ct range-
EntericBio Realtime Norovirus Assay
(16.33 – 36.68)
In-house Taqman ™ assay (15.12-37.43)

Result breakdown
3 % of total Positive’s had dual infection with both GI and GII NoV
The inhibition rate for EntericBio non-extracted Norovirus PCR was 0.5% (4/710 samples).
Internal control:
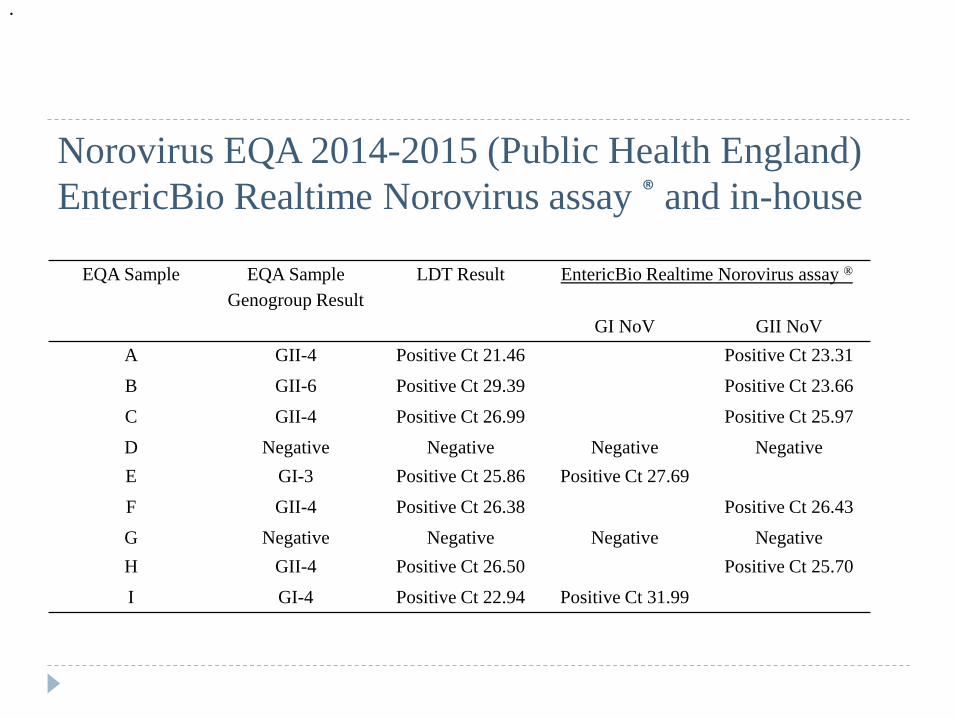
EQA Sample EQA Sample
Genogroup Result
LDT Result EntericBio Realtime Norovirus assay ®
GI NoV GII NoV
A GII-4 Positive Ct 21.46 Positive Ct 23.31
B GII-6 Positive Ct 29.39 Positive Ct 23.66
C GII-4 Positive Ct 26.99 Positive Ct 25.97
D Negative Negative Negative Negative
E GI-3 Positive Ct 25.86 Positive Ct 27.69
F GII-4 Positive Ct 26.38 Positive Ct 26.43
G Negative Negative Negative Negative
H GII-4 Positive Ct 26.50 Positive Ct 25.70
I GI-4 Positive Ct 22.94 Positive Ct 31.99
.
Norovirus EQA 2014-2015 (Public Health England)
EntericBio Realtime Norovirus assay ® and in-house
Conclusion of multicenter study
EntericBio Rapid NoV assay less labour intensive
Shorter TAT, no extraction
Rapid detection can lead to better patient management, implementation of appropriate infection control procedures
Can differentiate between NoV genogroups GI and GII, Beneficial for surveillance
CT values available – not black box pos/neg – semi-quantitative
Rapid diagnostics for better patient
management .....
The IPCT should ensure
that faeces specimens from
cases are collected without
delay for norovirus detection,
bacterial culture and, if
appropriate, Clostridium difficile
tests. All microbiological analysis
of stool specimens associated
with potential outbreaks must
be available on a seven days a
week, including holidays, basis.
The turnaround time for
non-culture analysis as measured
from specimen production to
provision of a telephoned or
electronically-transmitted result
should be within the same day
or, at most, 24h in order to
minimize bed closures. Up to a
maximum of six specimens of faeces
from the group of affected
detection in the first instance.
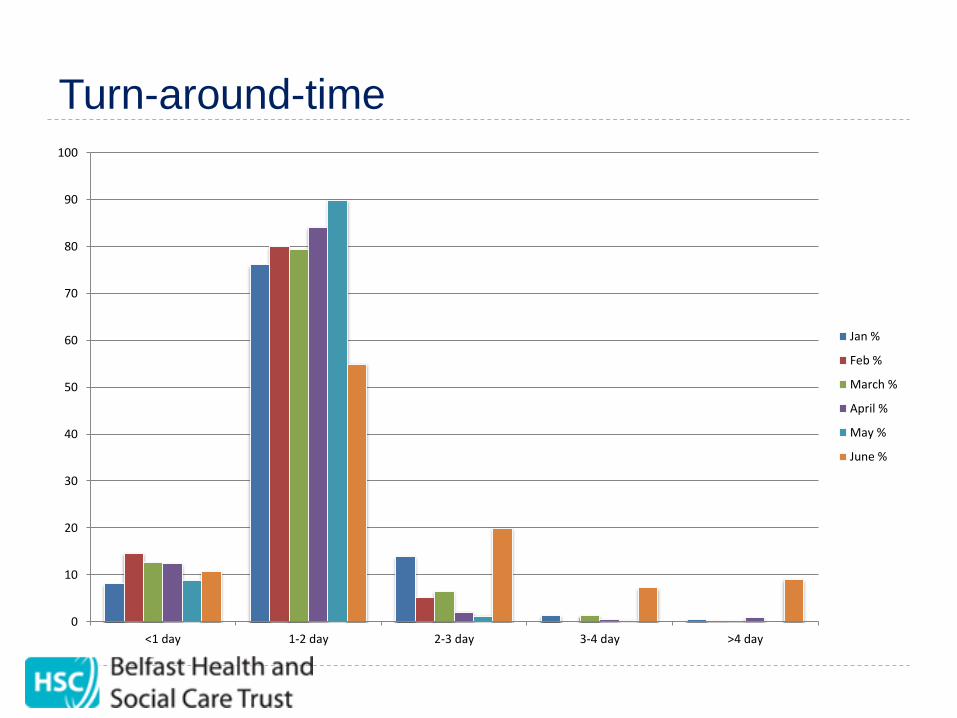
Turn-around-time
0
10
20
30
40
50
60
70
80
90
100
<1 day 1-2 day 2-3 day 3-4 day >4 day
Jan %
Feb %
March %
April %
May %
June %

Transit times Feb 2017
(specimen date to Lims entry/receipt)
0
100
200
300
400
500
600
700
<1 day 1-2 day 2-3 day 3-4 day 4-5 day >5 day
Transit time
Transit time

So how could the RVL gain from EntericBio
Norovirus Assay?
.. Business cases and Tender ...
Northern Ireland: 5 Trusts – Trust Ownership of Noro screening to enable rapid TAT
Outbreak screening
Infection Control
Meet National Guidelines
Support from RVL for elderly care query Rotavirus
RVL to focus on REGIONAL ICU/PICU/NICU, Haematology, Transplant, SCUBU, immunocompromised, immunosuppressed for all 5 targets

Thank you! Christine Meenan,
Microbiology Laboratory,
Royal Victoria Hospital, Belfast
Michael O’Donoghue, Isabelle O’Callaghan,
Liam Blake, Louise Barry, Bartley Cryan.
Microbiology Department,
Cork University Hospital, Cork
Colm McDonnell, Anita O’Connell
Virology Department,
University Hospital Limerick, Limerick
Dave Clancy, Serosep®EntericBio
Monika Lambert, Serosep®EntericBio

Microbiology Belfast
Service BHSCT
Regional service for Virology, TB and Mycology
Microbiology: 680,000 specimens per year (2014) – 410,000 Bacteriology (274,000 Virology-54,000 Molecular, 220,000 serology)
Micro/TB/Mycology: 38 BMS staff, 8 MLA
Virology: 17 BMS (10 Molecular), 5 MLA (2 belong to Micro, on rotation)
Micro/TB/Mycology: 16 Medics: 8 Medical Consultants, 8 Reg grade
Virology: 5 FRCPath Duty Virologists (2 Medical Consultants & 3 Senior Clinical Scientists)
Micro/TB/Mycology: Core Service Hours: 8:00am – 21:00pm, urgents only from 21:00
Virology: Core Service Hours: 8:30am-5:30pm, ‘urgents only’ 5:30pm on

Microbiology Enterics:
EntericBio (March 2015)
EntericBio Gastro panel 2:
Salmonella
Shiga Toxin 1 (Stx 1)
Shiga Toxin 2 (Stx 2)
Shigella
Campylobacter
Cryptosporidium
Giardia
Confirmation:
• Culture
• Microscopy Approx 19,000 faeces/year



















![Comparative Evaluation Regulation Gmcrops Containing Dsrna[1]](https://img.dokumen.tips/doc/110x75/577cc69e1a28aba7119eb167/comparative-evaluation-regulation-gmcrops-containing-dsrna1.jpg)








