Embed Size (px)
Citation preview

Viral-based immunotherapies to transform the fight against cancers and infectious diseases
November 2017Corporate Presentation
This presentation contains forward-looking statements, which are subject to numerous risks and uncertainties,which could cause actual results to differ materially from those anticipated. There can be no guarantee that (i) theresults of pre-clinical work and prior clinical trials will be predictive of the results of the clinical trials currentlyunder way, (ii) regulatory authorities will agree with the Company’s further development plans for its therapies, or(iii) the Company will find development and commercialization partners for its therapies in a timely manner and onsatisfactory terms and conditions, if at all. The occurrence of any of these risks could have a significant negativeoutcome for the Company’s activities, perspectives, financial situation, results and development.
For a discussion of risks and uncertainties which could cause the Company's actual results, financial condition,performance or achievements to differ from those contained in the forward-looking statements, please refer to theRisk Factors (“Facteurs de Risque") section of the Document de Référence, available on the AMF website(http://www.amf-france.org) or on Transgene’s website (www.transgene.fr). Forward-looking statements speakonly as of the date on which they are made and Transgene undertakes no obligation to update these forward-looking statements, even if new information becomes available in the future.
Disclaimer
2

Management | Experienced team focused on delivery
3
Philippe Archinard, PhDChairman & Chief Executive Officer
Eric Quéméneur, PhDExecutive VP and Chief Scientific Officer
Christophe Ancel, PharmDVP Quality and Qualified Person
Maud Brandely, MD, PhDChief Medical Officer
Jean-Philippe DelVP Finance
Thibaut du Fayet, MBAVP Marketing, Alliance, and Project Mgt
John Felitti, JD, MBAGeneral Counsel and VP Legal
Hemanshu Shah, PhD, MBAVP Corporate Development & Medical Affairs
E
C
D
A
B
F
EC DA B F
Transgene | Poised to play a key role in immunotherapy
4
A pioneer in developing viral vector-based immunotherapies
2Cutting-edge immunotherapy platforms
• Therapeutic vaccines• Oncolytic viruses
Focus on cancers and infectious diseases:
• High level of unmet medical need
• New treatments leave significant opportunities
5Immunotherapy products
in clinical trials – focus on combinations

Anti-PD-1/PD-L1 | A new paradigm – need for improvementTargeting substantial non-responder populations
5
0
50
100
OR
R %
ORR = approximate objective response rate %
FDA approved agent available
Transgene’s indications of interest
Source: from ASCO Annual meeting 2017, by Gregory L. Beatty, MD PhD
*Anti-PD-1 FDA approved in Sept. 2017
Non-responders

The power of immunotherapy combinationsStrong scientific rationale for adding our immunotherapies to ICIs
6
Immune Checkpoints Inhibitors (ICIs)
Positive effects of the combination of Transgene’s immunotherapies with ICIs have been demonstrated in several preclinical tumor models
Increased response rate, longer duration of response, extended OS
Block the signal that preventsactivated T-cells from attacking cancer cells
Enhance the efficacy of anti-tumor T-cell response Need for increased response rate
Therapeutic Vaccines Stimulate the immune response to kill cancer cells
Oncolytic Viruses Directly attack tumor cells and boost the immune system
Safety - Preserve healthy cells
Transgene’s immunotherapies
Compelling preclinical and clinical packages

Readouts expectedon 5 products
Sep 2017Launch OV platformfor a new generation OV
Transgene | Building momentum in immuno-oncologyClinical collaborations validate the potential of ICI+TG immunotherapy combinations
7
2016 2017 2018
Clinical collaborations made possible by Transgene’s compelling clinical and pre-clinical packages
Oct 2016Clinical collaboration
for TG4001
Dec 2016Clinical collaboration
for TG4010 (NSCLC 2L)
Apr 2017Clinical collaborationfor TG4010 (NSCLC 1L)
Refocused clinical development on combination trials with ICIs
Jun 2017Research
collaboration agreement for
UCART-19 production
7 clinical trials initiated in last 18 months

Diversified portfolio of clinical-stage immunotherapies
8
Product IndicationPreclinical Clinical Phase
Major Expected Milestones1 2 3
THERAPEUTIC VACCINES
TG4010
Non-small cell lung cancer – 1st line
Non-small cell lung cancer – 2nd line
Non-small cell lung cancer
FPI YE17
First data 1Q 2018
TG4001 HPV positive cancers First data in 2H 18
TG1050 Chronic hepatitis B Full data in 1H 18
ONCOLYTIC VIRUSES
Pexa-Vec*
HCC – 1st line (PHOCUS)
HCC – 1st line
Other solid tumors
Sarcoma – Breast cancer
Solid tumors
First data 2019
First data in 2H 2018
TG6002 Glioblastoma First data in 2H 18
+ nivolumab (ICI) + CT
Neo-adjuvant (translational)
+ avelumab (ICI)
+ antiviral
+ sorafenib
+ ipilimumab (ICI)
+ nivolumab (ICI)
+ nivolumab (ICI)
+ cyclophosphamide
Neo-adjuvant (translational)
Ongoing FPI < 6 months
* Transgene has commercial rights to Pexa-Vec in Europe and additional selected countries. SillaJen has a co-promote option in five European countries.

Ideally suited for combination immunotherapy regimens
Therapeutic Vaccines

Our Therapeutic Vaccine platform
10
– Antigen (MUC1) expressionleading to maturation of Antigen Presenting Cell (APC)
– Mature APCs present MUC1antigen to naive T-cells
– Activated T-cells infiltrate the tumor, recognize and kill MUC1+ tumor cells
SC injection
Therapeutic vaccines express tumor/viral antigens
To stimulate a safe and specific immune response
– T-cells get activated , multiplyand reach the blood stream
Important benefit when combinedwith CT and ICIs
Modified Virus Ankara (MVA)
expressing MUC1 antigen & interleukin 2
TG4010 targeting 1st and 2nd line NSCLC
Clinical collaborations with

TG4010 | Strong lung cancer clinical data Improved response rate & duration of response
12
TG4010
+ CT
Placebo
+ CT
Non-squamous (n)
ORR
Median duration of response (wks)
98
40%
41
98
28%
18
✓ Improved response rate & duration of response
✓ Good safety profile
Source: Quoix, E. et al., TG4010 immunotherapy and first-line chemotherapy for advanced non-small-cell lung cancer (TIME): results from the phase 2b part of a randomised, double-blind, placebo-controlled, phase 2b/3 trial, The Lancet Oncology, Dec. 2015, (17:212)
TG4010 + chemotherapy (n=39)40.9 [23.9 – 54.1] wks
Chemotherapy (n=27)18.1 [13.7 – 36.4] wks
TG4010 + chemotherapy40.9 [23.9 – 54.1] wks
Placebo + chemotherapy18.1 [13.7 – 36.4] wks
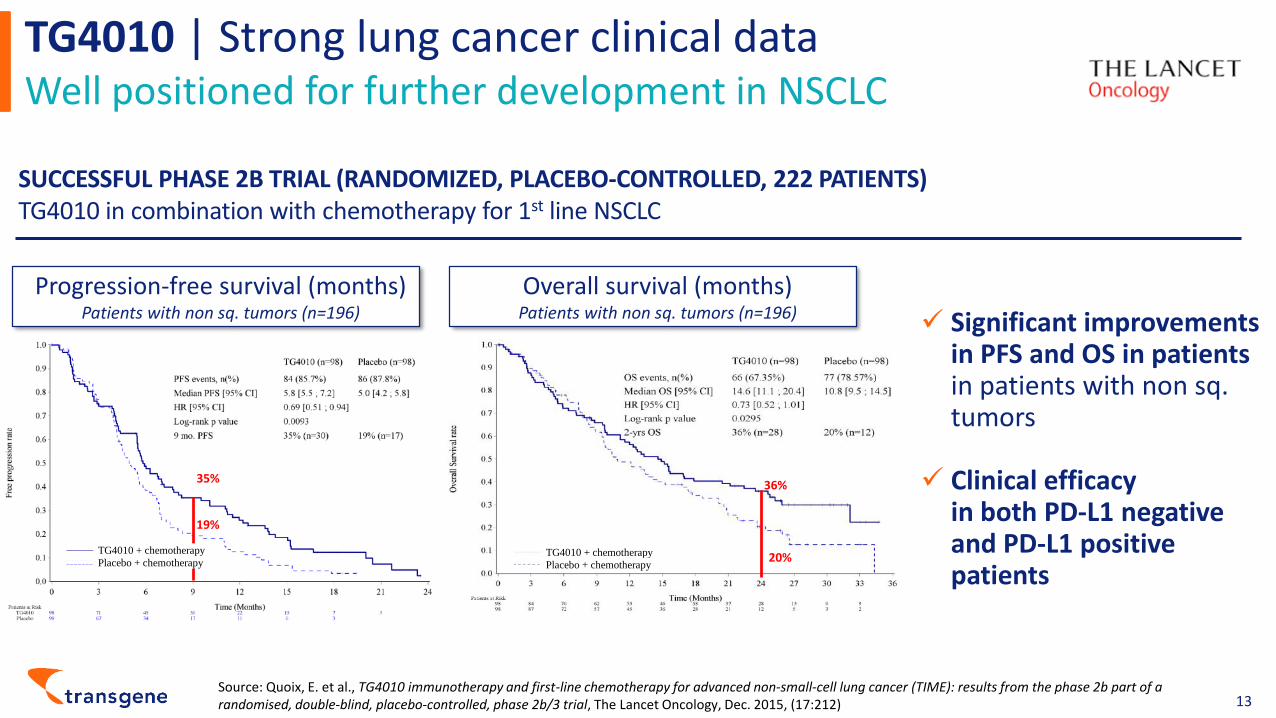
TG4010 | Strong lung cancer clinical data Well positioned for further development in NSCLC
13
✓ Significant improvements in PFS and OS in patients in patients with non sq. tumors
✓ Clinical efficacy in both PD-L1 negative and PD-L1 positive patients
Progression-free survival (months)Patients with non sq. tumors (n=196)
Overall survival (months)Patients with non sq. tumors (n=196)
SUCCESSFUL PHASE 2B TRIAL (RANDOMIZED, PLACEBO-CONTROLLED, 222 PATIENTS)TG4010 in combination with chemotherapy for 1st line NSCLC
36%
20%
35%
19%
Source: Quoix, E. et al., TG4010 immunotherapy and first-line chemotherapy for advanced non-small-cell lung cancer (TIME): results from the phase 2b part of a randomised, double-blind, placebo-controlled, phase 2b/3 trial, The Lancet Oncology, Dec. 2015, (17:212)
TG4010 + chemotherapy
Placebo + chemotherapyTG4010 + chemotherapy
Placebo + chemotherapy

TG4010 | Proven mechanism of actionEfficacy driven by T-cell response (CD8+)
14Source: Tosch et al., Viral based vaccine TG4010 induces broadening of specific immune response and improves outcome in advanced NSCLC, Journal for ImmunoTherapy of Cancer, 2017 (5:70)
Specific CD8+ T cell response to MUC1 epitopes is associated with increased survival
OS improvement during TG4010 treatment is driven by the development of a larger CD8+ T cell anti-MUC1 repertory
Specific CD8+ T cell response to MUC1 after TG4010 administration is associated with responses against other lung tumor antigens
Increased CD8+ response without increase in inhibitory T reg frequency

- 100 000 200 000 300 000 400 000 500 000 600 000 700 000 800 000
2ND LINE (INDEPENDENT OF PD-L1 STATUS)
LOW PD-L1 - 1ST LINE
NON-MUTATED (ALK, EGFR, …)
NON-SQUAMOUS
STAGE IV
265 K
331 K
441 K
532 K
710 K
Eligible Population (US, EU, JP), in thousands of patients
TG4010 | Clinical positioningA very large population in NSCLC, stage IV, non-squamous patients
15
1L - TG4010 positioning
2L - TG4010 positioning
Source: Globocan, Company estimates
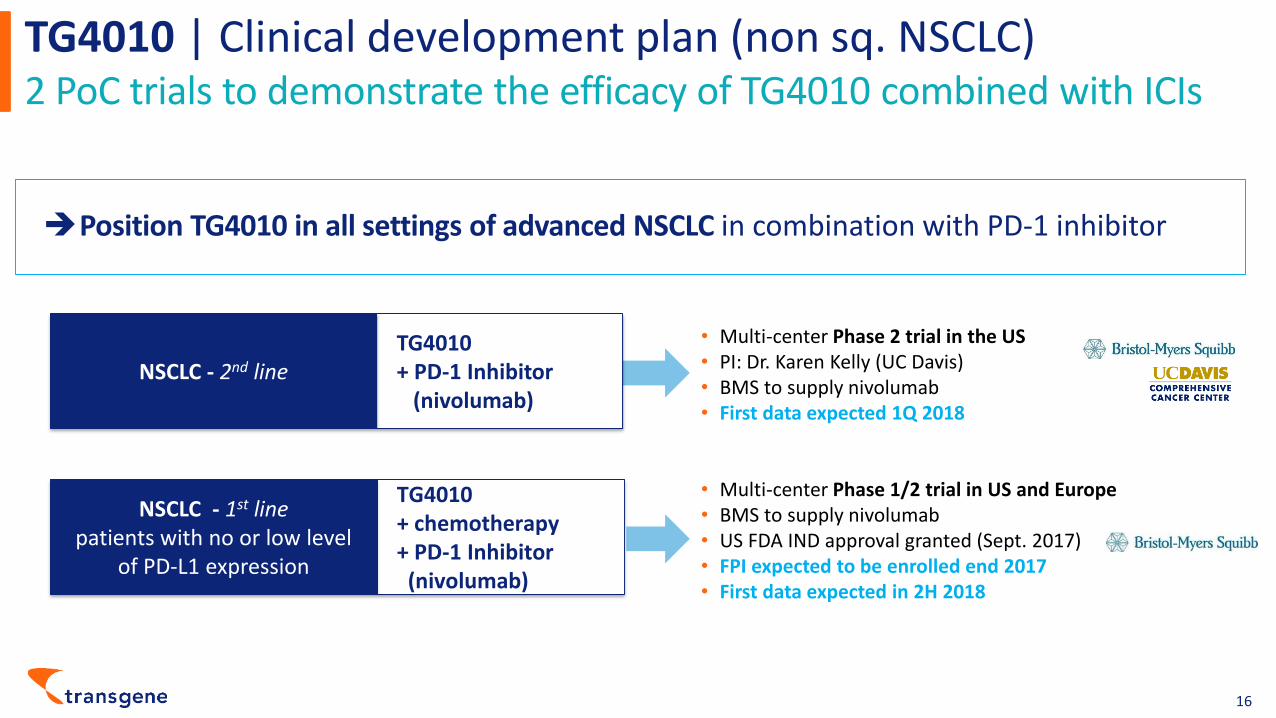
TG4010 | Clinical development plan (non sq. NSCLC)2 PoC trials to demonstrate the efficacy of TG4010 combined with ICIs
16
TG4010 + PD-1 Inhibitor
(nivolumab) NSCLC - 2nd line
• Multi-center Phase 2 trial in the US• PI: Dr. Karen Kelly (UC Davis)• BMS to supply nivolumab• First data expected 1Q 2018
Position TG4010 in all settings of advanced NSCLC in combination with PD-1 inhibitor
TG4010 + chemotherapy+ PD-1 Inhibitor
(nivolumab)
NSCLC - 1st linepatients with no or low level
of PD-L1 expression
• Multi-center Phase 1/2 trial in US and Europe• BMS to supply nivolumab• US FDA IND approval granted (Sept. 2017)• FPI expected to be enrolled end 2017• First data expected in 2H 2018

TG4010 | Non-Small Cell Lung Cancer (NSCLC) - 2nd linePhase 2 in combination with Opdivo® (nivolumab)
17
Endpoints
• Principal Investigator: Dr. Karen Kelly
• Collaborative arrangement
– UC Davis Medical Center, USA (sponsor)
– Bristol-Myers Squibb (supply of nivolumab)
– Transgene (supply of TG4010)
• First patient treated in March 2017
• First planned data expected 1Q 2018 (15 patients)
Support of
Primary endpoint: Objective response rate (ORR)•
Secondary endpoints: progression• -free survival (PFS), overall survival (OS), duration of response and safety
Protocol
• Up to 33 patients• Multi-center, single-arm, open-label study• Stage IV non-squamous NSCLC who have
progressed after one line of systemic therapy
Participating centers
• UC Davis• UC San Francisco
• City of Hope• UC San Diego

• Collaborative agreement with BMS (supply of nivolumab)
• US FDA IND Approval (Sept. 2017)
• First patient expected to be enrolled by the end of 2017
• First data expected in 2H 2018
TG4010 | Non-Small Cell Lung Cancer (NSCLC) - 1st linePhase 1/2 in combination with Opdivo® (nivolumab) + chemotherapy
18
Support of
Endpoints (Phase 2 part)
• Primary endpoint: Objective response rate (ORR)• Secondary endpoints: progression-free survival
(PFS), overall survival (OS), duration of response and safety
Protocol
• Up to 39 patients• Multi-center, single-arm, open-label study• Stage III B-IV or delayed relapse, tumors
with low or undetectable PD-L1 expression
• TG4010 108 PFU weekly for 6 weeks then every 3 weeks by SC route
• Nivolumab 360 mg every 3 weeks by IV route• Pemetrexed-carboplatin (or cisplatin) every 3 weeks for 4 cycles
Study regimen
Participating countries
USA•
Belgium•
• Denmark • France

MVA expressing HPV16 E6 & E7 antigens & interleukin 2
TG4001 targeting HPV-positivehead and neck cancer
Supported by

TG4001 | No specific treatment regimens for HPV+ head and neck cancer patients
20
~60% of oropharyngeal SCCHN are HPV+
• Increasing incidence in western countries 25,000 patients*
• Dismal prognosis
• Much better therapeutic options needed
Current treatment options for all head and neck cancer cases
First-line therapyFor patients with good • performance status: historically platinum-based doublet (e.g. Cisplatin/5-FU or carboplatin/paclitaxel)
ORR: – 30% to 40%
Median OS: – 6-9 months regardless of specific drug
For patient with poor • performance status: use single agent CT or cetuximab
Second-line therapyNivolumab, pembrolizumab•
ORR: – 16% to 19%
Median OS: – 7-8 months
Significant opportunity for TG4001 to improve the ORR of ICIs in a large head and neck cancer population
* Source: Globocan, Company estimates

• TG4001 - already demonstrated efficacy in the clinic: – Randomized, placebo-controlled Phase 2b (n=206) in HPV+ high grade cervical carcinoma in
situ (CIN2/3) – Demonstrated immunogenicity– Demonstrated efficacy (resolution and viral clearance) – Study confirmed safety (injection site reaction – most common adverse event) – TG4001 was nevertheless not progressed further in CIN 2/3 (LEEP efficacy)
• Thanks to KOLs and Merck KGaA/Pfizer’s commitment, decision to progress rather in advanced HPV positive cancers in combination with avelumab
TG4001 | Strong rationale for combining a vaccine targeting HPV with an ICI in advanced/metastatic HPV-positive SCCHN
21
Very strong scientific rationale for combining TG4001 and avelumab to address the high unmet medical in this important HPV-positive cancer population
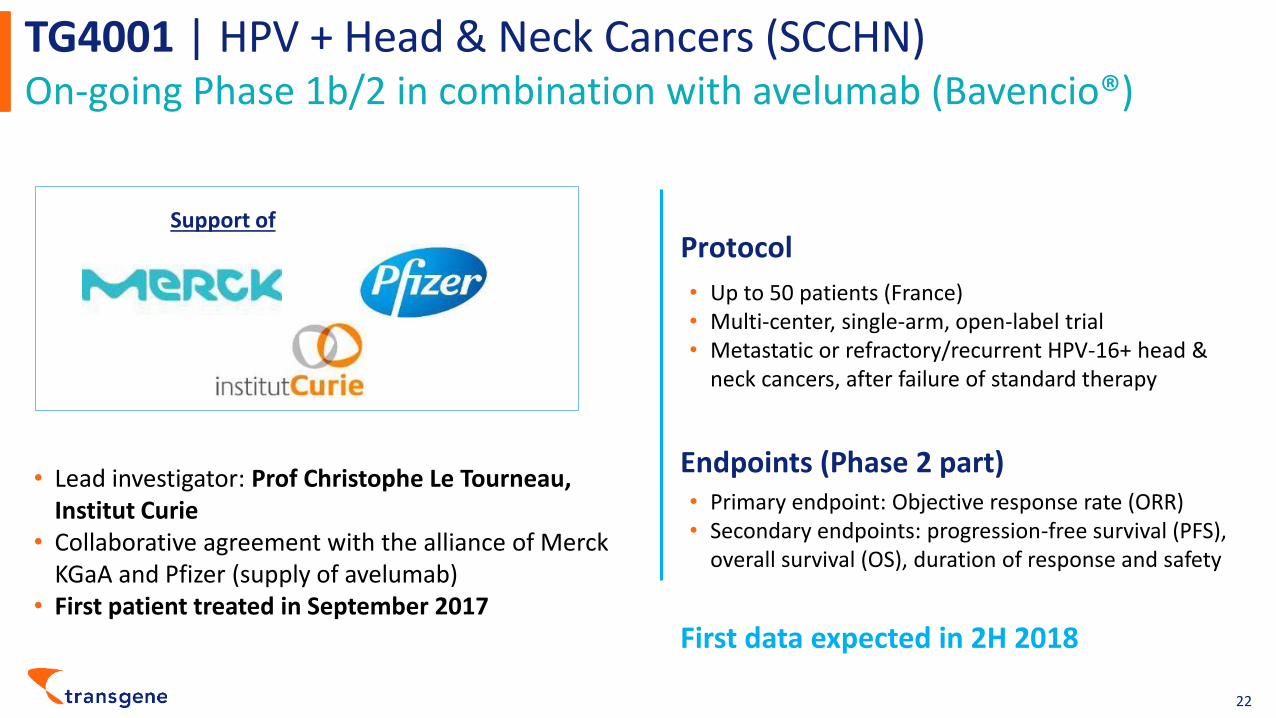
TG4001 | HPV + Head & Neck Cancers (SCCHN)On-going Phase 1b/2 in combination with avelumab (Bavencio®)
22
• Lead investigator: Prof Christophe Le Tourneau, Institut Curie
• Collaborative agreement with the alliance of Merck KGaA and Pfizer (supply of avelumab)
• First patient treated in September 2017
Support of
Endpoints (Phase 2 part)• Primary endpoint: Objective response rate (ORR)• Secondary endpoints: progression-free survival (PFS),
overall survival (OS), duration of response and safety
First data expected in 2H 2018
Protocol
• Up to 50 patients (France)• Multi-center, single-arm, open-label trial• Metastatic or refractory/recurrent HPV-16+ head &
neck cancers, after failure of standard therapy
Modified Adenovirus 5 that expresses 3 different HBV (Hepatitis B Virus) antigens
TG1050 targeting chronic hepatitis B

TG1050 | Current therapies focus on disease management, not cure
24
Large unmet medical need as cure rate is extremely low
Need to improve clinical outcome:High risk of developing cirrhosis and hepatocellular carcinoma
500,000 eligible patients*
Treatment recommendations (EASL 2017 clinical guidelines)
Long• -term administration of entecavir (Baraclude®), tenofovir disoproxil fumarate (Viread®) or tenofovir alafenamide (Vemlidy®) as monotherapy
High level of viral suppression – 9̴8 %
Low level of functional cure (HBsAg loss) < – 3 % per year
PegIFN• for 48 weeks in highly selected patientsModerate level of viral suppression – 5̴0 %Low level of functional cure < – 9% per year
* Source: Decision Resources, Company estimates | Note: Includes patients from the US, EU, and Japan

• Only viral-based therapeutic vaccine that integrates the 3 relevant HBV antigens (polymerase, core, HBsAg)
• Demonstrated immunogenicity & functionality
– Similar to those of spontaneous resolvers i.e. robust and broad CD8 T-cell responses
– Capacity of HBV-specific T cells induced by TG1050 to recognize epitopes all HBV genotypes
– Capacity to induce functional T-cells in tolerant HBV mouse models (Novel AAV-based model, other)
• Antiviral properties
– Capacity to control HBsAg and induce HBsAg seroconversion with no detectable liver inflammation in tolerant HBV mouse models
• Ongoing preclinical experiments (direct/indirect antivirals, immuno-modulators,…)
TG1050 | Strong pre-clinical data Sustained anti-viral effects in HBV mouse models (AAV)
25
HBV DNA (viral load)Mean viral load at D28 : 1.4x106 copies/mL
HB
V D
NA
Fo
ld C
han
ge(M
ean
+/-
SEM
)
0.01
0.1
1
10
28 39 55 67 84 105 126 147 158
Days post AAV-HBV injection
Circulating HBsAgMean HBsAg titers at D28 : 20µg/mL
HB
sAg
Fold
Ch
ange
(Me
an +
/-SE
M)
0.1
1
28 39 55 67 84 105 126 147 158
2
0.5
Days post AAV-HBV injectionMartin et al., Gut, 2014Inschauspé et al., EASL, 2015
TG1050
Empty Ad
TG1050
Empty Ad

TG1050 | Phase 1/1b trial
26
Primary objectives✓ Evaluate safety and tolerability of TG1050
administered in single and multiple doses (3 injections at one week interval)
✓ Determine dose and schedule of administration for further development
Secondary endpoints✓ Antiviral activity: HBsAg levels✓ Cellular and humoral immune responses
Phase I/Ib enrolment completed
Preliminary data (AASLD Liver Meeting 2017):✓ Good safety profile in 12 patients✓ TG1050 induces a robust specific cell-mediated
immune response in patients that have received a single dose of TG1050
Principal investigator• Prof Fabien Zoulim,
Hospices civils, Lyon (France)
Protocol• Up to 48 patients• International, randomized safety and dose-
finding study• Patients currently being treated with
standard-of-care antiviral therapy (tenofovir or entecavir)
• Initial safety data in 12 patients reported• First efficacy data expected 1H 2018
(n=48)
Participating countries• Canada, France, Germany

A new highly promising therapeutic class in the fight against cancer
Oncolytic Viruses – Pioneered by Transgene
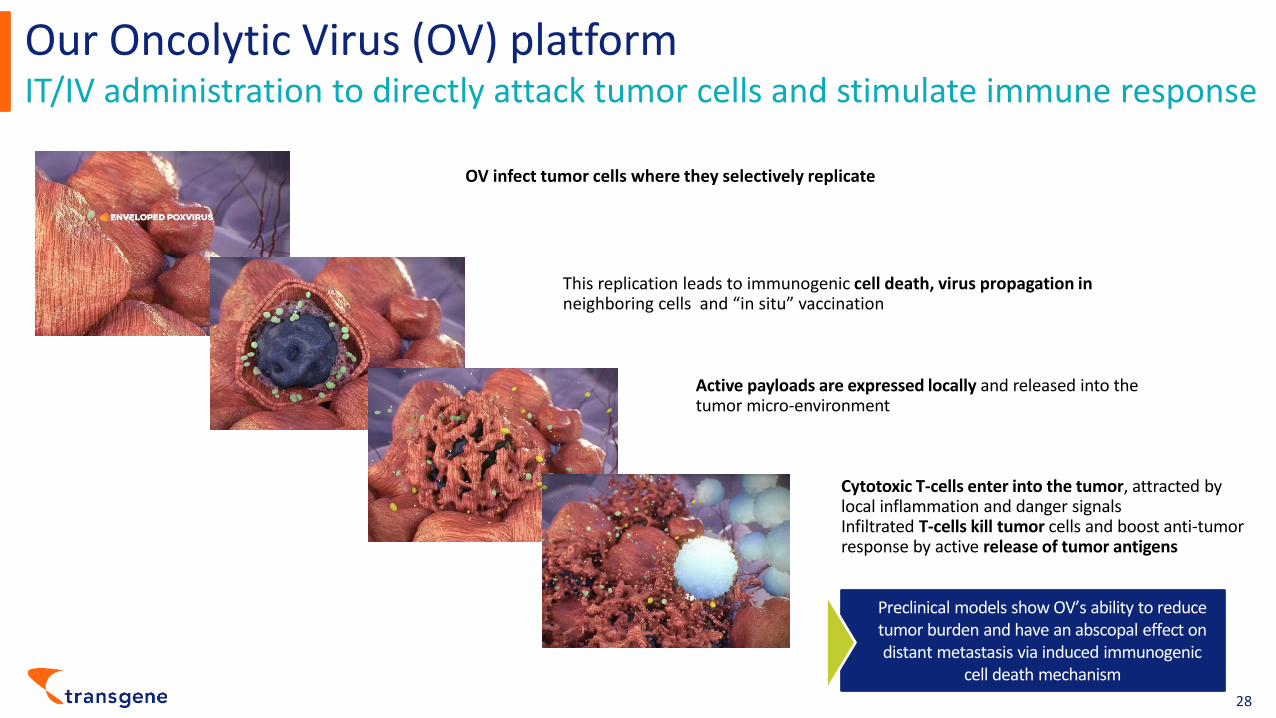
Our Oncolytic Virus (OV) platformIT/IV administration to directly attack tumor cells and stimulate immune response
28
Preclinical models show OV’s ability to reduce tumor burden and have an abscopal effect on distant metastasis via induced immunogenic
cell death mechanism
OV infect tumor cells where they selectively replicate
Active payloads are expressed locally and released into the tumor micro-environment
Cytotoxic T-cells enter into the tumor, attracted by local inflammation and danger signalsInfiltrated T-cells kill tumor cells and boost anti-tumor response by active release of tumor antigens
This replication leads to immunogenic cell death, virus propagation in neighboring cells and “in situ” vaccination

Replicative Vaccinia Virus expressing GM-CSF
Pexa-Vec in hepatocellular carcinoma (HCC)

Pexa-Vec | Collaboration with SillaJen
Ongoing pivotal Phase 3 trial in HCC 1LSillaJen responsible for conducting •
Phase 3 trial
Transgene own all rights for its territory•
Transgene’s remaining funding obligation •
amounts to $1.5 million
30
Transgene owns development and commercialization rights in Europe
EU rights of Pexa-Vec in-licensed in 2010 Current licensor: SillaJen (KOSDAQ: 215600)
4 Phase 2 trials conducted by Transgene
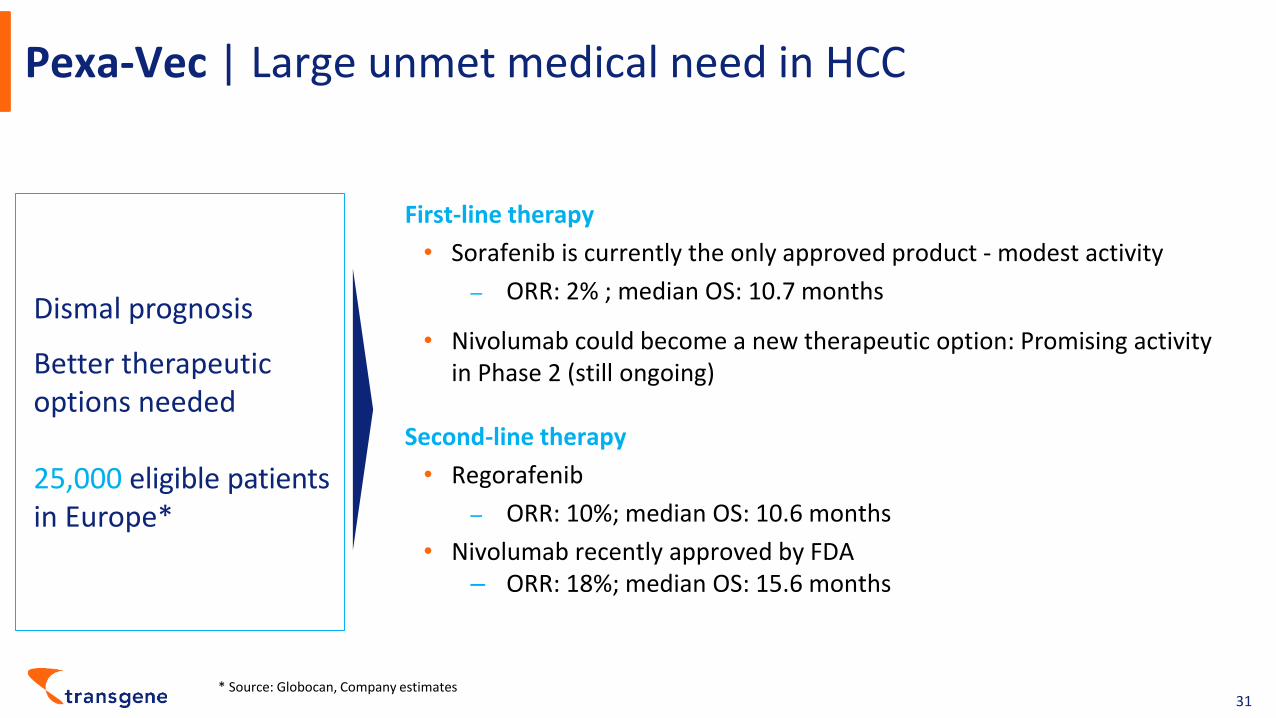
Pexa-Vec | Large unmet medical need in HCC
31
Dismal prognosis
Better therapeutic options needed
25,000 eligible patients in Europe*
First-line therapy
Sorafenib is currently the only approved product • - modest activity
ORR: – 2% ; median OS: 10.7 months
Nivolumab could become a new therapeutic option: Promising activity •
in Phase 2 (still ongoing)
Second-line therapy
Regorafenib •
ORR: – 10%; median OS: 10.6 months
Nivolumab recently approved by FDA•
ORR: – 18%; median OS: 15.6 months
* Source: Globocan, Company estimates

Pexa-Vec | Key Phase 2 clinical trial resultsClinical activity demonstrated in multiple trials
32
Proof of concept for MOA: active immunotherapy
30-patient dose-finding Phase 2 trial in HCC (80% of patients first-line)• OS results - high dose versus low dose
– Median OS: 14.1 (high dose) vs. 6.7 months (low dose)
– Hazard Ratio = 0.39
– p = 0.020
Nature Medicine, Volume 19, Issue 2, February 2013
Trials with >300 patients treated with Pexa-Vec in variety of tumor types, including liver, colorectal and kidney

Pexa-Vec | Clinical development plan in HCC - 1st linePivotal Phase 3 and combination Phase 2
33
Pexa-Vec + Opdivo® (nivolumab)
Advanced HCC1st line
• Multi-center Phase 1/2 trial in France, Italy, US• Sponsor: Transgene• Open-label, single-arm trial• 1st patient dosed in July 2017• Efficacy data expected in 2H 2018
Pexa-Vec + sorafenib
Advanced HCC1st line
• Multi-center Phase 3 trial in Europe, US, Asia• Randomized, two arm trial• Ongoing recruitment • First data (efficacy vs SoC) expected in 2019
Position Pexa-Vec with SoC treatment for all PD-L1 status patients

Pexa-Vec | Ongoing Phase 3 clinical trial (PHOCUS trial)1st line advanced hepatocellular carcinoma
34
Conducted by
Phase 3 study in combination with sorafenib (Kinase inhibitor)
✓ Orphan drug designation granted✓ SPA with FDA✓ SFDA authorization (July 2017)
Pexa• -Vec + sorafenib versus sorafenib (only approved drug for advanced HCC)
N=• 600 patients (Europe, North America, and Asia), 140 clinical centers
1:1 • randomized trialDesign
Endpoints
Primary: overall survival (OS)•
Secondary: safety, time to progression, progression• -free survival, overall response rate and disease control rate
• First patient enrolled in January 2016• Recruitment ongoing • First efficacy data expected in 2019
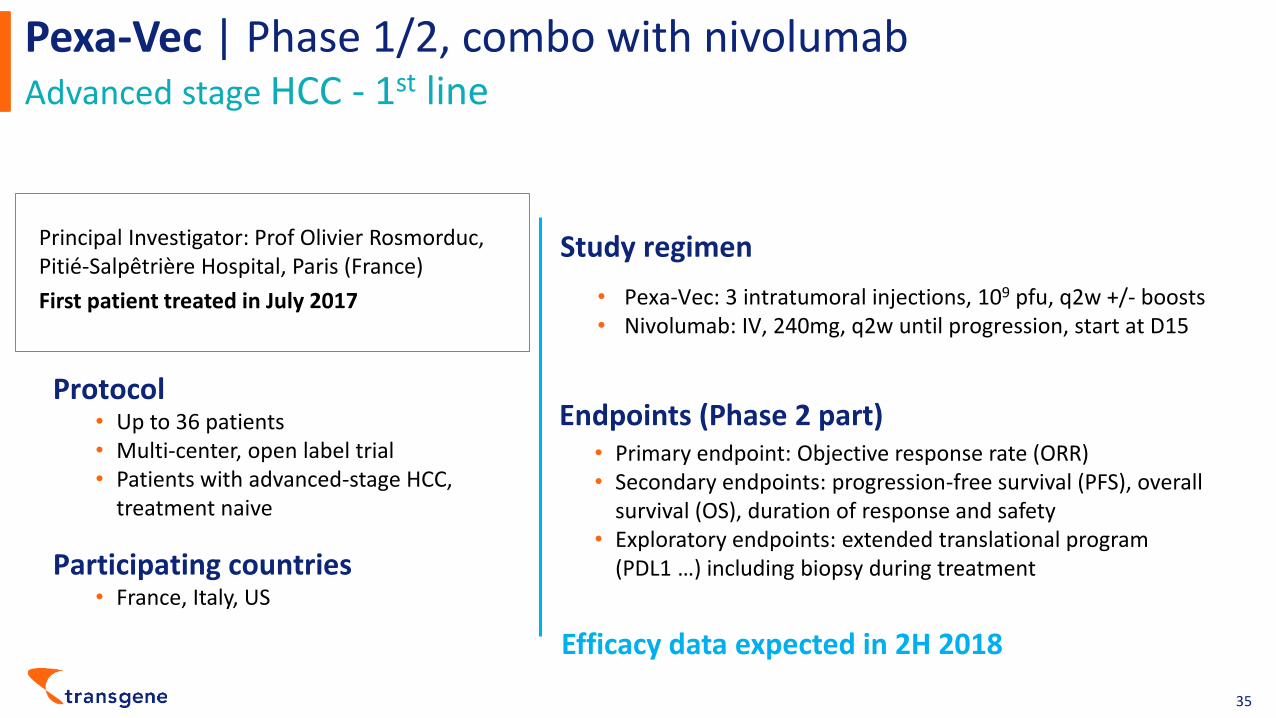
Pexa-Vec | Phase 1/2, combo with nivolumab Advanced stage HCC - 1st line
35
Principal Investigator: Prof Olivier Rosmorduc, Pitié-Salpêtrière Hospital, Paris (France)
First patient treated in July 2017
Protocol• Up to 36 patients• Multi-center, open label trial• Patients with advanced-stage HCC,
treatment naive
Endpoints (Phase 2 part)• Primary endpoint: Objective response rate (ORR)• Secondary endpoints: progression-free survival (PFS), overall
survival (OS), duration of response and safety• Exploratory endpoints: extended translational program
(PDL1 …) including biopsy during treatment
Pexa• -Vec: 3 intratumoral injections, 109 pfu, q2w +/- boostsNivolumab: IV, • 240mg, q2w until progression, start at D15
Study regimen
Participating countries• France, Italy, US
Efficacy data expected in 2H 2018
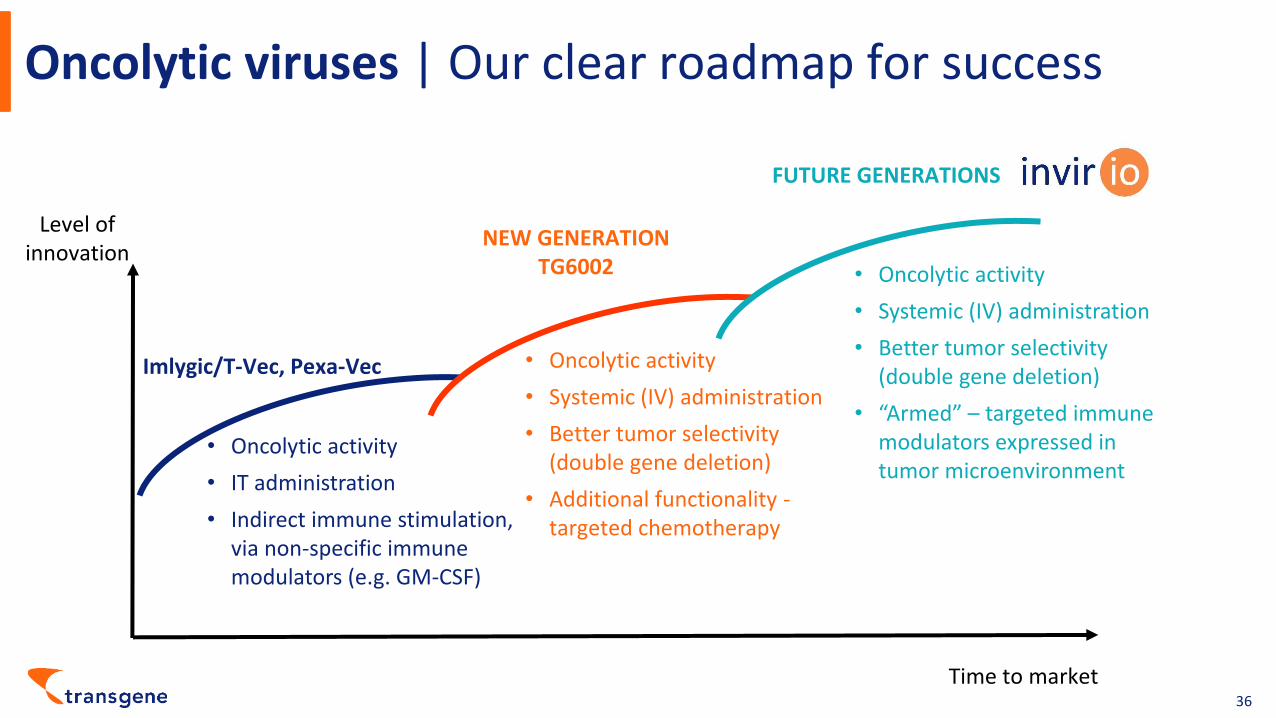
Oncolytic viruses | Our clear roadmap for success
36
Time to market
Level of innovation
Imlygic/T-Vec, Pexa-Vec
NEW GENERATIONTG6002
FUTURE GENERATIONS
• Oncolytic activity
• IT administration
• Indirect immune stimulation, via non-specific immune modulators (e.g. GM-CSF)
Oncolytic activity•
Systemic (IV) administration•
Better tumor selectivity •
(double gene deletion)
Additional functionality • -targeted chemotherapy
• Oncolytic activity
• Systemic (IV) administration
• Better tumor selectivity (double gene deletion)
• “Armed” – targeted immune modulators expressed in tumor microenvironment
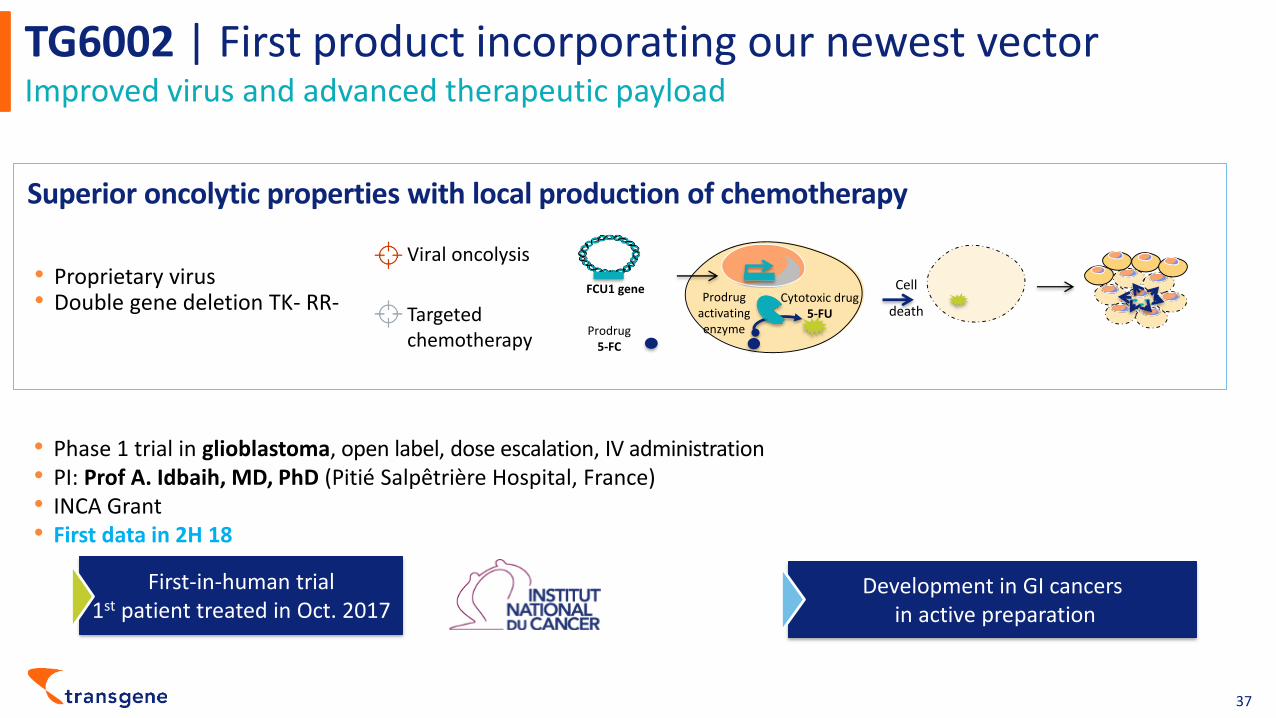
TG6002 | First product incorporating our newest vectorImproved virus and advanced therapeutic payload
37
FCU1 gene
Prodrug5-FC
Cytotoxic drug5-FU
Prodrug activating enzyme
Cell
deathTargeted chemotherapy
• Proprietary virus• Double gene deletion TK- RR-
Viral oncolysis
• Phase 1 trial in glioblastoma, open label, dose escalation, IV administration• PI: Prof A. Idbaih, MD, PhD (Pitié Salpêtrière Hospital, France) • INCA Grant • First data in 2H 18
First-in-human trial1st patient treated in Oct. 2017
Development in GI cancersin active preparation
Superior oncolytic properties with local production of chemotherapy

Significant anticipated value-creating news flow through 2018Clinical readouts expected on all 5 products
38
5 productsin the clinic
TG4010 Lung cancer (NSCLC)
TG4001 HPV+ head & neck cancer (SCCHN)
TG1050 Chronic hepatitis B (HBV)
Pexa-Vec Liver cancer (HCC)
TG6002 Glioblastoma
First Phase 2 data 1Q 2018 (2nd line, TG4010 + nivolumab)
First Phase 2 data in 2H 2018 (TG4001 + avelumab)
Full Phase 1b data in 1H 2018
Phase 2 efficacy data in 2H 2018 (Pexa-Vec + nivolumab)
First Phase 1 data 2H 2018

Appendices
39

Company funded to deliver multiple value generating milestones
40
Free float40 %
60 %
Key shareholdersAs of September 30, 2017
• Market capitalization:~ €200 million as of September 30, 2017
• 56.4 million shares outstanding+ 1.1 million options and restricted stocks
• Listed on Euronext Paris• ISIN: FR0005175080 - Ticker: TNG
Key figures
Expected cash burn 2017
(~€ 14 million for 4Q 2017)~ € 30 million
Operating revenuesas of September 30, 2017
~ € 5 million
Cash and cash equivalentsas of September 30, 2017
€ 40 million
€10 million drawn down
(Due 2021)

Our strategy |Develop future disruptive innovationEngineer multifunctional oncolytic viruses
41
Anti-cancer Weapons
Patented Viruses
VV
TK- RR-
Cytokines / Chemokines
Receptor ligandsAntibodySdAb
Enzyme
+
Oncolytic activityImmunogenic properties
Tumor targeting from the IV route
Key effectors of the tumor microenvironmentPotent immunomodulators benefiting from local delivery
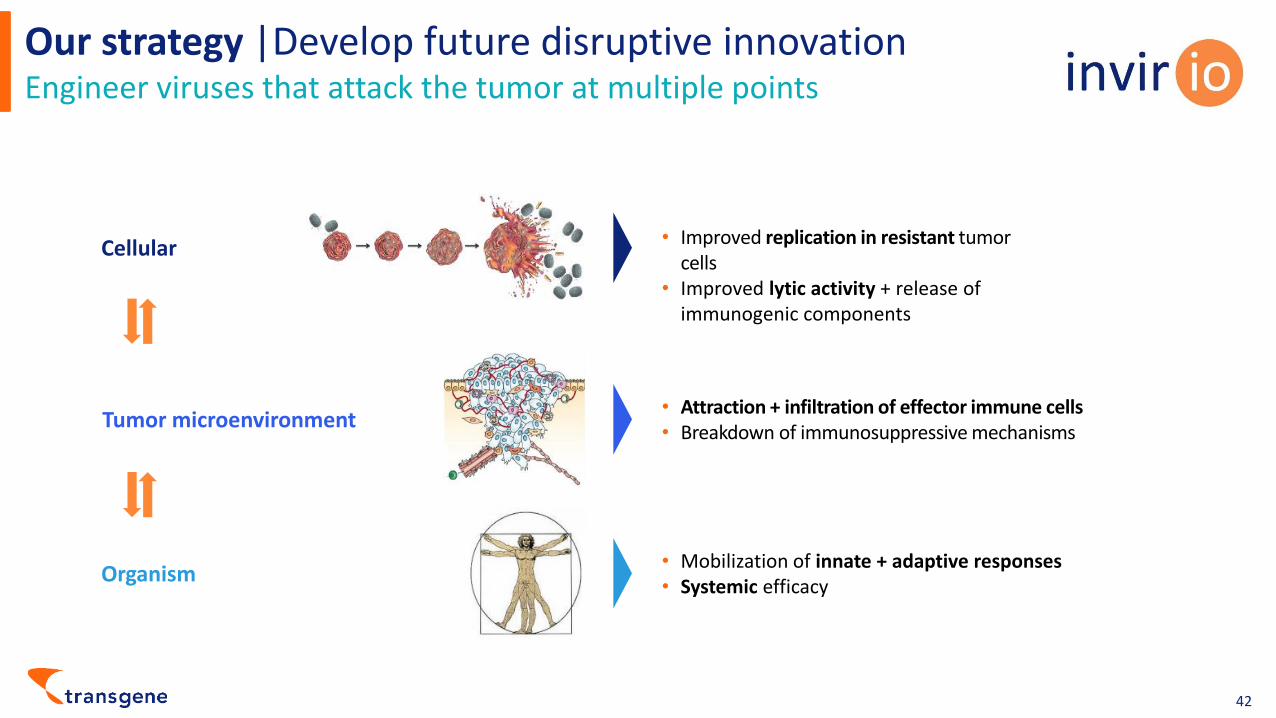
Our strategy |Develop future disruptive innovationEngineer viruses that attack the tumor at multiple points
42
Cellular
Organism
Tumor microenvironment
Improved• replication in resistant tumor cellsImproved • lytic activity + release of immunogenic components
• Mobilization of innate + adaptive responses• Systemic efficacy
• Attraction + infiltration of effector immune cells • Breakdown of immunosuppressive mechanisms

ICI clinical collaboration scheme
43
General approach
• Proof-of-concept trials• Collaborative design of the protocol with shared
expectations for outcomes• Open-label trials with joint access to results• No preferential rights granted over TG4010 or
TG4001
• Partner to provide ICI for the trial and participate in clinical sites selection
• Transgene to provide its product, fund the trials and ensure their execution
• TG4010, 1L, advanced lung cancer
• TG4010, 2L, advanced lung cancer
• TG4001, 2L, HPV+ head and neck cancers
3 ongoing clinical collaborations

TG4001 | Positive Phase 2b in HPV-associated CIN 2/3Demonstration of statistically significant curative activity at 6 months
44
0
5
10
15
20
25
30
35
40
HPV16 All Genotypes
P = 0.009 p = 0.0013
Resolution (%) Viral clearance (%) ✓ Single agent TG4001 is active, and able to address HPV-related carcinomas
✓ Data represent a strong POC of active immunotherapy‒ TG4001 was 5x superior in HPV16 patients
compared to placebo to induce complete disease regression
‒ TG4001 showed an efficacy 4 fold superior compared to placebo regarding the viral clearance
✓ Clinical experience in 300+ subjects, demonstrating good safety profile ‒ Injection site reactions were the most
common AE
PHASE 2B TRIAL (RANDOMIZED, PLACEBO-CONTROLLED, 206 PATIENTS)in patients with cervical carcinoma in situ of high grade (2/3)
0
5
10
15
20
25
HPV16 All Genotypes
TG4001monotherapy
Placebo
P = 0.0498 P = 0.0126

400 Boulevard Gonthier d’Andernach - Parc d’Innovation - CS80166 67405 Illkirch Graffenstaden Cedex France
Tél.: + 33 (0)3 88 27 91 21 www.transgene.fr
Lucie LarguierDirector Corporate Communication and Investor Relations+33 3 88 27 91 04 / +33 6 76 24 72 27
[email protected] / [email protected]
Contact
@TransgeneSA Transgene





























