Embed Size (px)
Citation preview

Introduction to Complex Health Systems
Notes for Facilitators
This is a document developed by members of the CHEPSAA project.
CHEPSAA (Consortium for Health Policy and Systems Analysis in Africa) is a project funded by the European Union which aims to extend sustainable African capacity to produce and use high quality health policy and systems research by harnessing synergies among a Consortium of African and European universities with relevant expertise.
This document is an output from a project funded by the European Commission (EC) FP7-Africa (Grant no. 265482). The views expressed are not necessarily those of the EC.
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 1

Introduction to Complex Health Systems is licensed under a
Creative Commons Attribution-Non-Commercial-Share Alike License
September 2014
You are free:
to Share – to copy, distribute and transmit the work
to Remix – to adapt the work
Under the following conditions:
Attribution. You must attribute the work in the manner specified by the author or licensor (but not in any way that suggests that they endorse you or your use of the work)
Non-commercial. You may not use this work for commercial purposes
Share Alike. If you alter, transform, or build upon this work, you may distribute the resulting work but only under the same or similar license to this one
For any reuse or distribution, you must make clear to others the license terms of this work. One way to do this is with a link to the license web page: http://creativecommons.org/licenses/by-nc-sa/2.5/za
Any of the above conditions can be waived if you get permission from the copyright holder.
Nothing in this license impairs or restricts the authors’ moral rights.
Nothing in this license impairs or restricts the rights of authors whose work is referenced in this document.
Cited works used in this document must be cited following usual academic conventions
Citation of this work must follow normal academic conventions
A suggested citation is: Introduction to Complex Health Systems: Facilitators’ Guide. CHEPSAA (Consortium for Health Policy & Systems Analysis in Africa) 2014, www.hpsa-africa.org
www.healthedu.uct.ac.za or contact [email protected]
We would appreciate your feedback for this Open Educational Resource (OER), by emailing us at [email protected]
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 2

Introduction
Health systems are inescapably complex. It is accepted now that in order to understand the functioning of health systems, and act towards strengthening them, it is necessary to grasp the notion of complexity and see how it plays out, through the behaviours, actions and relationships between people in the system. The course provides an opportunity to explore this important aspect of health systems, for anyone involved in public health and interested in developing a deeper understanding of systems at work. The course explores how the health system is a platform from which health services are delivered, and how a well-functioning system is therefore necessary for the provision of quality – effective and caring – services for the sick and vulnerable.
Overall course aim
This course aims to provide an introduction to understanding health systems as complex systems, by considering the components, actors and inter-relationships of the Health System (HS) as a platform for health systems analysis, action and research.
Course map
The Introduction to Complex Health Systems course is made up of ten sessions. It starts with the introduction and exploration of key concepts, moving through the study of examples of these concepts and frameworks in practice, and application of them in participants’ own contexts, to case studies and papers with which they engage.
Sessions 1 & 2 work together, introducing and discussing health systems; sessions 3 & 4 look at and develop ideas around a particular example of health system functioning; sessions 5-7 together develop analysis of the roles and behaviour of people in the health system; sessions 8 & 9 pull the strands of the course together through case studies; and finally session 10 wraps up the course concepts.
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 3
Overview of the sessions
Session 1: What is a health system?
Session 2: Frameworks for describing and analysing health systems
Session 3: Understanding the Thai experience of health system development
Session 4: Whole system change – PHC and UHC
Session 5: Recognising agents in health systems
Session 6: Exploring power, agency and mindsets
Session 7: Managing change in health systems
Sessions 8 & 9: Intervening in health systems (case studies)
Session 10: Health system complexity and change

The session outlines in this facilitators’ guide include:
guidelines for input sessions, with some key points to consider and questions to help participants relate the learning to their experience and the session activities;
suggested timing of activities – however this is only a guide;
some ideas for feedback after group activities instructions for activities and ideas for facilitation background information to supplement input
The course is designed to be taught over ten weeks, in one three-hour session weekly, with self-study preparation and assignments done between the sessions. If necessary, it can be taught in a five day block, in which case the between-session tasks would have to be adjusted, and some left out. However, the course is carefully structured as a coherent whole, so any changes would have to be well thought out, and re-configured if session times are changed (e.g. from 3-hour to 2-hour sessions).
Approach to teaching and learning
This module follows a constructivist approach to learning which is based on the understanding that learners are not ‘empty vessels’ to be filled with ‘knowledge’, but that their understanding of new information is built upon and shaped by their existing knowledge, skills, values and attitudes. Therefore, many of the activities in the module have been designed to encourage participants to think through issues for themselves before providing them with new information or theory, or to apply their learning in individual or group activities. In this way learning can be more effective as participants relate the ideas and concepts to their own experience and existing knowledge. This also means that input needs to be adapted by the facilitator to suit the needs of particular learning groups.
Sessions consist of a range of activities including lectures, group and individual work, games, videos, podcasts and discussions, designed to support participants’ learning based on an interactive and participatory approach.
Presentation style
During the presentations, asking relevant questions can help to draw out what participants already think about certain issues or terms. In this way new information can be provided in a way that helps to either reinforce participants’ understanding, or correct any misunderstanding they may have. Questions can also be used to encourage participants to apply their knowledge and to assess their understanding of new concepts and theories. However, if time is short it is easy to let a lecture-mode of imparting knowledge dominate. To
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 4
At the start of each session
recap and make links back to
the last session, to help
participants see the coherence
of the course;
At the end of each session -
review and summarise, to help
clarify and reinforce what has
been covered.

Remember that permission to distribute photocopies of any journal articles or chapters from
books must be obtained from the relevant copyright holders in some cases.
How well did it go?
After each session, you may find it useful to record any issues that participants found difficult or points that need to be clarified later in the course. Also note anything that you thought worked particularly well. This can inform future courses.
avoid this, facilitators are encouraged to use the activities to guide discussion and draw out key themes or concepts and to be flexible in when, and how, theoretical input is given.
A key challenge of this style of teaching is time-management, which involves the ability to keep the discussions to the point and manage the group dynamics (i.e. encouraging contributions from quieter participants and avoiding discussions being dominated by the more vocal participants).
Learning through doing
An active-learning approach also informs the module. The Group Work Sessions allow participants to apply what they have learnt and grapple with some of the complexities of policy analysis. It is worth emphasising to participants that this is a valuable learning opportunity and the more time and effort they put into it the more they will gain from the learning experience.
Assessment
Assessment of the course outcomes is through two assignments during the course, which participants do as individual work; one group presentation and one individual assignment which forms the summative assessment. The summative assessment could be done as a take-home assignment, or as an open-book examination. You can decide when the assignments should be submitted, but preferably on the following session, so the tasks serve as reinforcement of learning and relevant, timeous feedback can be given. The assessment tasks are outlined in the Assessment Guide in the Course Overview document (Appendix 1).
Resources
In addition to this facilitators’ guide and Powerpoint slides for lectures, the materials for this course include resources for participants, consisting of:
Course overview with lists of required readings; Assessment Guide; Handouts, including a set of case studies. The handouts
are sequentially numbered for the whole course, with the relevant session clearly indicated on each, so you know when to give them out.
The facilitators’ guide indicates at what points to use or give out these resources. You can decide which are appropriate to give to participants in your setting, and you may also want to
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 5

give them additional notes that you prepare. At the end of the facilitators’ guide is a list of recommended readings for participants to which you can refer them for further reading.
For each session you will also need flip-chart (or newsprint/large sheets of paper) and marker pens to record key points during discussion. It is helpful if these are displayed on the walls and left for participants to refer to as needed during the course.
Managing group work
If possible choose a venue which allows participants to move into and work in small groups around separate tables. A lecture theatre setting is not conducive to group work, participation or discussion, and does not allow you to move around the groups to give guidance.
The ideal size for most group tasks or discussion is 4 – 6 participants. For some activities, such as buzz groups or thinking pairs, groups of 2 – 3 participants work well. The facilitator guide provides guidance on group size for particular activities.
Examples of interventions to facilitate the group work
If one person dominates the group: ask questions to encourage other participants to contribute.
If the group gets ‘stuck’ on one issue: ask questions to encourage them to think of other issue, prompt them to move on.
Remind participants to record their ideas or the consensus reached. Remind them of the time and help them pace themselves, for example: Use the last 10
minutes to focus on question X or plan your presentation.
An outcomes-based approach
Outcomes-based education involves identifying clear learning outcomes that can be shown, and assessed, at the end of the learning programme. Participants need to know what they are expected to work towards at the beginning of the learning programme.
To facilitate this, relevant learning outcomes (for the course as a whole, and for specific sessions) and assessment guidelines and criteria have been provided. We suggest that you refer to these at the beginning of each session as appropriate.
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 6

Course learning outcomes
This course has six learning outcomes. While not all sessions address all the outcomes, most of them weave through the majority of the sessions, albeit with different weightings in each session. The introduction to each session signals the focus of the session and its’ specific aims.
By the end of this course students are expected to be able to:
1. Show understanding of the dynamic and complex nature of health systems by reflecting on and describing their value bases and functioning, their components and the central roles and behaviours of a range of agents.
2. Discuss health systems as social constructions, influenced by and influencing the agents within them, as well as influenced by broader political and economic forces, generating public value and contributing to societal development.
3. Apply these understandings to assessment of own health system and comparison between health systems.
4. Apply relevant analytical skills and an understanding of complex systems in order to develop ideas about action to strengthen health systems.
5. Develop the personal communication, teamwork and leadership skills which are important for supporting health system change.
6. Demonstrate understanding of and openness to different perspectives on the nature of health systems.
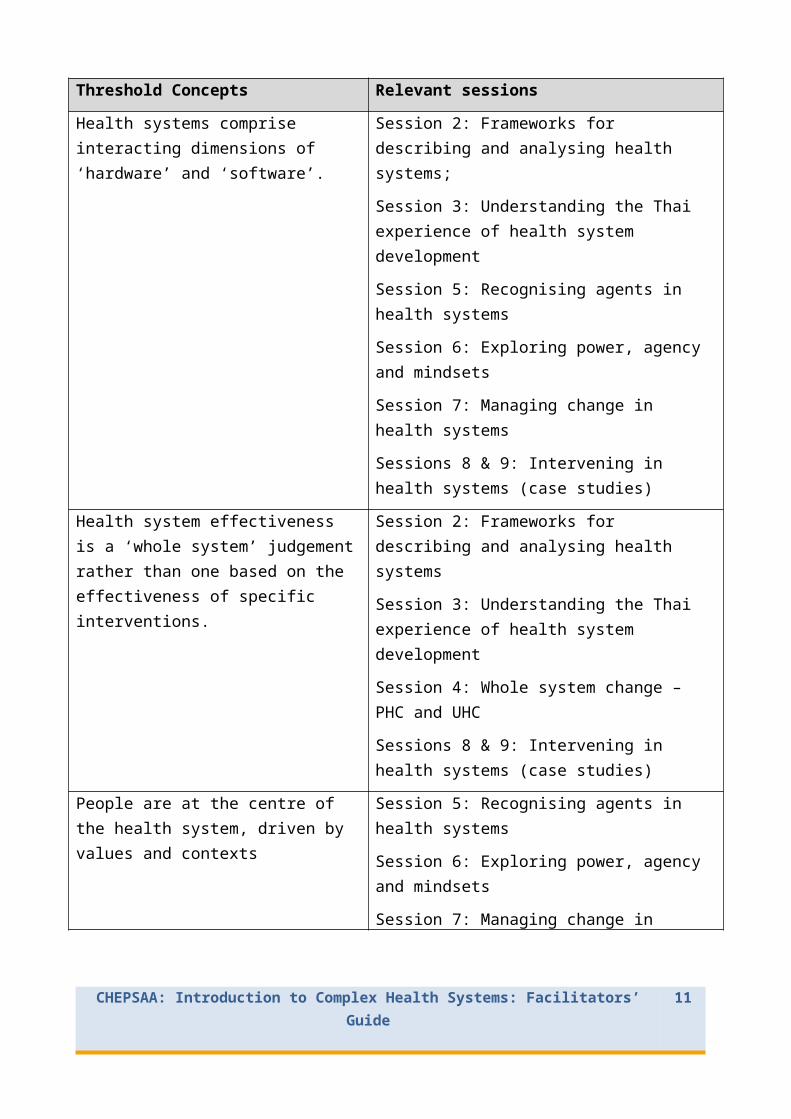
A number of threshhold concepts (key underpinning ideas) have been identified for this course. The table below indicates the sessions in which each is introduced and addressed:
Threshold Concepts Relevant sessions
Health systems are socially constructed; they exist within contexts and histories and are driven by and impact on a range of agents.
Session 1: What is a health system?
Session 2: Frameworks for describing and analysing health systems
Health systems are integrative by nature, and consist of complex inter-relationships; we all have a role in the system.
Session 1: What is a health system?
Session 2: Frameworks for describing and analysing health systems
Sessions 8 & 9: Intervening in health systems (case studies)
Health systems comprise interacting dimensions of ‘hardware’ and ‘software’.
Session 2: Frameworks for describing and analysing health systems;
Session 3: Understanding the Thai experience of
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 7

Threshold Concepts Relevant sessions
health system development
Session 5: Recognising agents in health systems
Session 6: Exploring power, agency and mindsets
Session 7: Managing change in health systems
Sessions 8 & 9: Intervening in health systems (case studies)
Health system effectiveness is a ‘whole system’ judgement rather than one based on the effectiveness of specific interventions.
Session 2: Frameworks for describing and analysing health systems
Session 3: Understanding the Thai experience of health system development
Session 4: Whole system change – PHC and UHC
Sessions 8 & 9: Intervening in health systems (case studies)
People are at the centre of the health system, driven by values and contexts
Session 5: Recognising agents in health systems
Session 6: Exploring power, agency and mindsets
Session 7: Managing change in health systems
Sessions 8 & 9: Intervening in health systems (case studies)
People make sense of the system around them and act based on their understandings and mind sets
Session 5: Recognising agents in health systems
Session 6: Exploring power, agency and mindsets
Session 7: Managing change in health systems
Sessions 8 & 9: Intervening in health systems (case studies)
Power is everywhere: in agency, service delivery and decision-making.
Session 5: Recognising agents in health systems
Session 6: Exploring power, agency and mindsets
Session 7: Managing change in health systems
Sessions 8 & 9: Intervening in health systems (case studies)
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 8

Threshold Concepts Relevant sessions
Everyone has a part to play in the system, working towards shared goals
Session 5: Recognising agents in health systems
Session 6: Exploring power, agency and mindsets
Session 7: Managing change in health systems
Sessions 8 & 9: Intervening in health systems (case studies)
The health system is knowable and changeable.
Session 3: Understanding the Thai experience of health system development
Session 7: Managing change in health systems
Sessions 8 & 9: Intervening in health systems (case studies)
The health system is a complex adaptive system.
Session 1: What is a health system?
Session 2: Frameworks for describing and analysing health systems
Session 3: Understanding the Thai experience of health system development
Session 5: Recognising agents in health systems
Sessions 8 & 9: Intervening in health systems (case studies)
Session 10: Health system complexity and change
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 9

Session 1: Introductions; What is a Health System?
This session aims to orientate participants into the course, and provides an introduction to thinking about health systems, how they are constructed and function in particular contexts, their value bases and their place in history and society.
Topics and activities:
1. Introductions and course overview: Participatory activity2. What is a health system and why is it important?: Group work3. The ‘life’ and experience of a health system (with Nigeria as a
particular example), considering political economy: Lecture; Podcast on a Nigerian example; ‘Gap-minder’ review and task
1. Class and course introductions (1hour)
a. Situating ourselves in the health system.
This course understands that, critically, every health system is about people and people are at the heart of their complexity. It is therefore good to start the course with an activity that encourages participants to begin to think about these issues and, at the same time, to loosen any barriers between them so that they can learn from each other during the course, whatever their past experiences.
To do this, prepare on a large piece of flip chart paper a schematic of a health system (such as the example on the next page) before the first session: in the centre draw a circle for ‘patients/citizens’; coming from that draw lines for each of community based services, facilities, district governance, region/province governance, and national government; around those an encompassing circle for ‘country and society’, and a final circle for the global/international level. The idea of this schematic is to get away from hierarchical and functional models of health systems, whilst retaining critical elements that participants will recognize and which provide a place for all.
Purpose of the exercise: The aim of this activity is get participants to think about their own and others’ relative places in the health system, as a baseline for the central idea in the course that we are all part of the system and have a range of multiple roles in it.
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 10
Resources needed:
1. Flip chart with schematic of health system (see below)
2. 3 objects which can be thrown easily for Group Juggle game
3. PPTs (and handouts of PPTs?) for lecture 1
4. Gap-minder exercise (access to internet)
5. Handout 1 – timeline of a country’s HS
Explain the task to participants and ask them to write their names in an appropriate place on the chart to indicate how they see themselves situated in the HS. They should:
i) write their name where it reflects their current position in or experience of their ‘own’ health system.
ii) indicate any specification they feel important (e.g. some might want to identify themselves as advocates in the community or as working in NGO-managed community based services or in private facilities).
Once everyone is seated, if the class size is not too large, ask everyone briefly to introduce themselves, with reference to the flipchart, giving their name and current health system position or experience. Start by introducing yourself, perhaps as patient and citizen (in the centre of the flipchart), as well as a researcher. Once everyone has introduced themselves, ask them to look at the chart and recognize that together, as a class, they:
Have experience of many different elements of the health system (even if each only has primary experience of one or two), and there may be a rich spread of experience across countries and of both global and country levels that can be emphasised – so there is much to learn from each other;
Make up a network that underpins and is fundamental to, the health system – a network of people, each with their own experience, ideas, understandings and perspectives, and yet
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 11

somehow part of the whole. If there is a group of participants from one country then this point could be made particularly strongly for them.
b. Short systems thinking ice breaker game – Group Juggle (30 minutes – can be omitted if time is short)
Time: You will probably need approximately 20 -30 minutes for this game – about 10-15 minutes for the game itself and 10-15 minutes for the debriefing discussion.
What you will need: For this activity you will need three different objects which can be easily thrown and caught (e.g. a bean-bag, soft ball, small stuffed toy, orange), a digital watch or other means of timing the activity, and enough space for the participants to stand in a circle to throw the objects to each other. If your group is bigger than 20, you might want to divide them into two teams.
The purposes of the game are:
To build awareness of team learning and problem-solving; To build awareness of how we are limited by our existing mental models; To develop systems thinking; To get to know each other and to have fun
Instructions:
All stand in a circle. Clearly explain the TWO rules: 1. Everyone must touch the object once; 2. They must
touch the objects in the same order every time (so they must remember who they throw to!). The aim of the game is to see how fast they can do it.
You start by throwing one of the objects to someone across the circle. That person throws to another, and each person in turn throws to someone else who has not had the object yet, until everyone has had a turn to throw and catch. At some point you can start throwing another two objects into the circle, to be caught and thrown in the same sequence - to make the game more fun and more of a challenge.
If the group does not know each other yet, the thrower can say her own name as she throws, and the catcher can say, ‘Thank you .. X’, and so on, as a way of learning each other’s names.
After a trial run to get the idea, start to time the group (choose someone to be the timer). When everyone has had their turn, the last person calls, ‘Stop’, and the time is noted. Then another round begins and the time noted. Challenge the group to cut their time down each round. Carry on until the group feels they have done it as fast as they can.
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 12

Possible solution
The participants might have worked out that the quickest way to do the exercise is to arrange themselves in such a way that they are standing next to the person they have to throw to, so they can just pass the object quickly around. This is not breaking the rules, but rather approaching them differently in order to get the best result.
Debriefing questions and discussion
To guide participants to reflect on the activity and draw learning from it, ask them:
What happened in the game – what did they do to try and improve their time? What were the constraints? (e.g. They might have assumed there were more ‘rules’
than in fact there were, or they might not have stopped to reflect and strategise enough.)
How did they feel about their efforts and the results? Can they now think of a better way of approaching the task? (Help them to see the
‘possible solution’ above if they did not work it out themselves) What can they note about how groups work and learn together within a ‘system’, and
how might this relate to their workplace experience?
(This game is adapted from Sweeney, L.B. and Meadows, D. (1995) The systems thinking playbook. Page 38 - 44)
c. Getting an overview of the course:
Hand out and take participants through the course overview document (Appendix 1), which explains the outline, outcomes and assessment of the course. You should also prepare and hand out the course timetable. Include a very brief rationale for the course’s focus on health systems and policy in the context of national and international health system debates. You could mention issues such as system focus, a) as part of the continuing thread of discussions about health care and service over decades internationally – the pendulum swing from diseases and clinical concerns to system concerns; b) as central to current global and national health system debates: e.g. a systems platform is essential to address disease needs (2000’s); and to achieve universal health care coverage.
2. What is a health system and why is it important? (45 minutes)
a. Describe a health System (20 minutes)
Working in groups, participants imagine they are meeting a visitor from Mars, and together draw a picture to explain to ‘it’ what a health system is, and why it is important to society. As a group, think about their different experiences and seek to identify the common key features of a health system as you they it, and have experienced it. Draw the picture on one large sheet of flip chart paper.
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 13

Task purpose: The idea of this exercise is to get people talking to each other, discussing different country experiences and perspectives, and then to try and tease out some common dimensions and elements to form a picture. The picture might be more of a diagram (perhaps an organogram), or might aim to tell more of a story (such as the patient experience of a health system), or might try to depict key but hidden elements of a health system (such as relations and context) or might primarily focus on a particular country. Every and any approach is acceptable! However, the intention of the group task is to try and get people to think beyond the specifics of any one health system, so as to get them thinking about generic, universal features. This is also important if the groups include people with different experiences.
b. Group presentations of health system pictures and feedback (25 minutes)
Once all the groups have finished, stick the pictures on the walls and ask each group to provide a rationale and narrative for their picture – what were they seeking to reflect on in the picture? Why that set of issues? What sort of experiences/perspectives drove them? Also ask the whole class to think about the similarities and differences across the pictures, how other groups’ pictures differed from their own, what they could take from other people’s pictures to add to their own understanding.
After the presentations, pick out some key issues to comment on. Also look for and comment on similarities and differences between groups. Try to get some feedback from the whole class on what they are taking from the comparison among groups – and link that to your own comments, so that they can see connections between points. Try to
The issues for you to look out for and comment on are, firstly, those that will be picked up again in the next lecture, such as:
The use of a building block approach, and the types of building blocks highlighted (specifically pick out not just service delivery, but funding, people, etc.);
The use of a patient perspective (perhaps focused on service delivery in particular, with recognition of providers, and referral systems, but not much acknowledgement of system functions such as funding, HR, drug supply, etc);
The role of actors within health systems, and who are identified as key actors; The importance of relationships among e.g. facilities and people; The hidden influence of context, and what features of context; The use of mechanical/structured models in the pictures; The acknowledgement of complexity, and what complexity – perhaps reflected in people
and relationships, various inputs combining in unclear ways, feedback loops, potential for unintended consequences, etc.;
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 14

The dynamism of systems and the extent to which that is reflected in the pictures, and what gives it dynamism (people and relationships);
Specific identification of policy issues, ideas, actors – to talk to the nature of policy as relevant to health systems (the focus of HS policy, the nature of policy as process, as more than document, as critically about practice);
The hidden influence of disciplinary perspectives on the pictures (e.g. an economics perspective, or economics issues vs. a more sociological/anthropological vs a more political issue), reflecting the particular experiences and perspectives of the people in the group.
It is useful to note the very fact of similarities and differences between groups – indicating that there are multiple perspectives on what health systems are, demonstrating that we have different ways of understanding health systems, and different experiences of them. Then link this point to the fact that these differences show the socially constructed nature of health systems, and have bearing on how to do research on systems and system issues. This point can then be picked up again in the discussion of different paradigms of knowledge and research strategies of preference.
Leave the groups’ diagrams of health systems on the walls if possible, to refer back to them in later sessions as appropriate.
3. Lecture 1: The ‘life’ and experience of a health system (with Nigeria as a particular example), considering political economy (75 mins)
Lecture purpose and rationale: The purpose of the lecture is to give a sense of: the historical forces that shape health system development; how health systems are politically and socially constructed, with both national and global forces influencing them; how ideas about how to strengthen health systems are themselves politically influenced; and why health systems matter to societies. This provides a background to the subsequent discussions of what health systems are – and to the case study exercise on health system development.
Lecture outline: (See PPT slides)
a) Provide an initial overview of historical health system development trends across countries (e.g. using Van Olmen et al., 2012) and drivers of change, and a comparison of country health and health systems performance by level of development, both within Africa and compared with other countries. Relate points to the groups’ diagrams of health systems, which should still be displayed.
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 15

b) Use the podcast, or PPT slides and readings of a lecture on the example of Nigeria, covering:
major periods and reforms, drivers of these, the social, cultural and political context of the system and systems performance;
identification of values base of different reform periods.
The podcast is available at https://www.youtube.com/watch?v=V-cXDl20i5k&feature=youtu.be
After the lecture or podcast, draw comparisons between Nigeria and other countries, and link back to the health system diagrams participants created. Ask them to compare aspects of the Nigerian case with their own countries. If there are any participants from Nigeria, ask them for their observations and comments on the podcast/ lecture.
c) Present Gapminder World data http://www.gapminder.org/ to show variation within Africa and other areas, and change over time in indicators, including for Nigeria and Thailand specifically, perhaps also e.g. South Africa and Tanzania. Use health data to show changes over time – using data for e.g. life expectancy at birth, IMR, Childhood Mortality; also use data on e.g. newborn deaths all causes, births attended by skilled staff, HIV ART coverage, Vaccine DPT3 coverage, percentage share government spending on health, out of pocket spending as percent share total spending (all available only for one datapoint). It may also be useful to show that some data are lacking for some countries and years, and ask participants to speculate on the significance of this.
d) Introduce and show a video of Hans Rosling, ‘Poor beat rich in MDG race’, presenting data showing that some lower income countries have had health improvements at a faster rate than higher income countries did for the same period. The video can be accessed at: http://www.gapminder.org/videos/poor-beats-rich/#.U9uFFaiMXdQ
After watching the video, ask participants for their impressions, and the most important idea they took from the video.
For next session:
Hand out a range of readings for participants to prepare for next session – choose from the readings in the box below. Allocate so that all the chosen readings are read by some participants, in order that they can share the main points they took from them. These are open access materials which you can find online. There are other readings listed at the end of the facilitators’ guide which you can give as useful general references for course reading (e.g. Gilson, in Smith and Hanson 2012; Frenk, 1994).
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 16

Explain the self-study task outlined in the box below, and refer participants to the session hand out, where they will find an explanation of the task. Give out the task and table required (Handout 1).
Self- study for participants:
a. Readings on introduction to health systems. These readings will consolidate the concepts introduced in this session, and prepare participants for the next session:
Sheikh, K., et al. 2014. People-centred science: strengthening the practice of health policy and systems research. Health research policy and systems. 12:19. url: http://www.health-policy-systems.com/content/12/1/19.
Van Olmen, J. et al., 2012. The Health System Dynamics Framework: The introduction of an analytical model for health system analysis and its application to two case-studies. Health, Culture and Society, 2(1), pp.0–21. url: http://www.itg.be/itg/GeneralSite/InfServices/Downloads/shsop28.pdf.
De Savigny, D. & Adam, T., 2009. Systems thinking for health systems strengthening. World Health Organization. url: http://whqlibdoc.who.int/publications/2009/9789241563895_eng.pdf.
b. Task: Drawing a timeline of your own country health system.Participants gather information on timelines of own countries’ health system development by consulting others from same country and doing brief research, then draw a timeline of the health system’s development – milestones, social/political/economic context, drivers of change. Use the template in Handout 1 as a guide.
UNDERSTANDING YOUR HEALTH SYSTEM’S EVOLUTION OVER TIME
DATE MILESTONE IN SYSTEM DEVELOPMENT
CONTEXT: SOCIAL POLITICAL, ECONOMIC
DRIVERS OF CHANGE IN SYSTEM
1800s
1900
1920
1940
1950
1960
1970
1980
1990
2000
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 17

2010
2020
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 18

Session 2: Frameworks for describing and analysing health systems
This session fleshes out the discussion of what a health system is and why it is important in a society. Concepts, measures and frameworks for thinking about systems are introduced and the integrative nature of health systems is emphasised. Participants then apply these to their own country’s health system. The session also introduces and guides a reflection on teamwork skills.
Topics and activities:
1. Participants discuss own countries’ health systems histories and make comparisons between them: Group discussion and feedback;
2. Understanding systems: Flashmob Game3. Ideas and frameworks for thinking about health
systems and policy: Video and lecture; group discussion.
4. Application of frameworks to specific country scenarios: Thinking pairs to prepare for homework
5. What makes for effective group work? Readings and discussion
1. Self-study feedback and group discussion (15 minutes)
Put up questions such as those below, to guide participants (in small groups of 3 -4, preferably from the same country) in discussing the session 1 self-study task. Ask them to note any important points they would like to share with the whole group later:
What were the key points you drew from the reading, in relation to what you learned in session 1?
How similar or different are your timeline template and answers from others in the group? Why do you think this is? Note the main differences.
After about 10 minutes of small group discussion, bring them together to share their key points and tricky or interesting questions. Give feedback and guidance where you think it is necessary, and highlight areas of commonality, divergence and particular importance.
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 19
Resources needed:
1. Video: What makes Maya cry?
2. PPTs (and handouts of PPTs) for lecture 2.
3. Handout 2 – Building successful group work
4. Assessment guide for participants – assignment 1
5. Thai case study, or reference for it
6. Handout 3 – questions for the Thai case study, or reference, and questions (for overnight reading)
2. Understanding more about systems (15 minutes)
Flashmob game
Purpose of the game: To make visible some connections between people which might not normally be apparent, showing the complex inter-relationships that exist in groups and systems, and that people and things in a system can be connected in unexpected ways.
Instructions:
Clear a large space in the room, and ask participants to walk around freely and silently until you give a signal and instruction, when they should stop and listen.
After about 30 seconds, clap your hands loudly, (or blow a whistle or ring a bell). When they stop, give an instruction for them to gather for few minutes, with a purpose.
Here are some ideas; you can probably think of others that will be relevant to your group:
o Gather with people from your own country/region and talk about how relevant the course is for your context.
o Get into a line in the sequence you threw the ball in the Group Juggle gameo Find others who have the same main area of expertise/interest as you – e.g.
clinical practice, research, teaching, management - and briefly talk about what you do.
o Get into groups of 2 – 3 with people you have not spoken with much yet, and introduce yourselves.
After each ‘gathering’, give a signal for them to move freely around the room again – until the next signal to stop and instruction to gather. End the game with free movement.
Debriefing: When participants have returned to their usual places, lead a discussion about what happened in the game and what can be learned about the complexity of relationships in a group or system. Ask questions such as:
What did you note about the relationships in the group? Were you ever uncertain about where you fitted or which group you should be part of?
If so, why was this? When you were walking around freely, were you aware of any inter-relationships
within the large group?
3. Ideas and frameworks for thinking about health systems and why they are important
a. Video about health systems (15 minutes)
Show the short World Bank video ‘Making Maya cry’ at: www.youtube.com/watch?v=PFVCNUOM5Us.
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 20

Before starting the video - ask participants to think about the question, “What makes Maya cry?”, while they are watching.
After watching the video – ask them for their responses to the preliminary question. Then ask, “Is there any one part of the health system that is more important than any other; or any part that could be left out? What would they be? Why?”
There might be different views on this. Allow a few participants to give their views, but this should not be a long discussion; the purpose of showing the video is to give a short and lighthearted (and positive) overview of health systems, their complexity and the essential interconnectedness of their parts, as a starting point for deeper exploration.
b. Lecture 2 – What is a health system? (1 hour)
Lecture purpose and rationale: The purpose of this lecture is to give an overview of ideas and frameworks for thinking about health systems. It should pick up and consolidate the discussions of the first group work task around health systems, as well as provide the background for much of the rest of the course. It considers dimensions of health system performance, various health systems frameworks and introduces some key ideas about complex adaptive systems.
The lecture seeks primarily to provide an overview of different approaches to thinking about health systems – importantly, it distinguishes between a more inventory/building blocks approach, and a more actor-oriented, relational approach. Both are linked back to the notion of complex adaptive systems. The distinction between health and health care systems should also be made clear through the lecture.
Some time is given to the WHO building blocks approach (WHO 2007), acknowledging, first, the range of performance dimensions it considers – and their links to the values base of the broader society. The Antwerp ‘health system dynamics’ framework (van Olmen et al. 2012) is also presented as an evolution of the WHO framework. Possible strengths and weaknesses of these frameworks are discussed. The issue of the values base of health systems can specifically be picked up from van Olmen et al. (2012) and Frenk (1994) (and this could be linked back to why health systems matter to societies, a point raised later in the course).
Three different relational frameworks are then presented to highlight the role of agents and relationships within health systems as well as to highlight the influence of disciplinary perspective (the economics framework), show how it is possible to look at a health system
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 21

through one dimension (accountability) and to step back and look at the whole – including other sectors, and community participation (Frenk 1994). The particular features of each framework should be highlighted as well as their similarities and differences, rather than their details. Finally, the nature of complexity in systems and health systems specifically is picked up at the start and the end of the lecture, including by emphasizing the role of people in the system, the interacting levels of the system and the notions of system hardware and software. The role of people and software in health systems also allows consideration of the socially constructed nature of the health system.
In the discussion of frameworks it is important to emphasise that health care does not equate to the health system – that some frameworks are primarily health care focused, and indeed, only Frenk (1994) explicitly talks to other sectors.
As this is a long and potentially dry lecture it is important both to make links back to the health system pictures the groups developed – to draw out common ideas; and to give the class time to absorb some of the frameworks during the course of the lecture (e.g. comparing van Olmen et al 2012 and Frenk 1994 models with diagrams groups have prepared).
Lecture outline (see PPT slides):
The lecture covers:
Definitions of a health system;
Conceptual frameworks for thinking about health systems – their features, strengths and weaknesses: WHO building blocks, Van Olmen, Frenk, WHO financing, Brinkerhoff;
Ideas about systems – making link to complex adaptive systems and nature of these: tight linkage, feedback loops, unpredictability, dynamic and interconnected;
Different levels of systems – macro, meso, micro;
Different perspectives on health systems;
Hardware and software of health systems;
Caveat about health systems development – no easy answer as politics and values matter.
References:
Frenk 1994
Smith and Hanson 2012
Van Olmen et al. 2012
WHO 2007 (Everybody’s Business)
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 22

4. Application of frameworks to specific country scenarios (20 minutes)
Think-pair-share
This activity gives participants an opportunity to prepare for the assignment, by thinking about how they could apply the theoretical frameworks they have been introduced to, to their own country health systems. Refer participants to assignment 1 in the Assessment Guide.
Think - Start by asking them to go back, individually, to their notes on the models introduced in the lecture, as well as their self-study task (timeline). They should consider which of the models they think will be most appropriate to use in analyzing their own country situation, and why they would use this model.
Pair - They then link up with a partner, and discuss their ideas. This provides a chance for them to clarify their own thinking, and pick up any misunderstandings or questions they have.
Share - Next, the pairs share their main points and questions with the whole group. At this stage you as facilitator will be able to give input or clarification if necessary.
5. Considering what makes for effective group work (30 minutes)
During this course, participants will be expected to participate in collaborative learning, by working in groups on a variety of tasks. If this approach to learning is to be successful, they need to develop some strategies for effective team or group work. A good way to help build their awareness of group work skills is to roleplay a common group work scenario, and let them reflect on what happened in the roleplay, in order to generate their own list of what makes successful group work. Follow the activity outlined below:
Set up a roleplay – 4-6 participants should volunteer to be the ‘group’. They sit in the centre, with the rest of the class around the outside, observing (fish-bowl method).
Explain a group work scenario to the small ‘fish-bowl’ group - e.g. They are discussing how to present the information they have collected in their group work task. One group member wants to do it in one way, which will take longer and be more thorough, and another demands that they do it in a different way, which will be quicker and easier. A few other members of the group try to support one of the ‘leaders’, but most are silenced by this conflict, feeling uncomfortable, irritated or bored.
Reflection – After the group has played out the scenario, ask the observers to think about what they noticed. Pose questions to guide them, such as:
What was happening in this group?
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 23

What prevented them from working together successfully? What could they (or the facilitator) have done differently to make their group work
more successful?
Write up the points participants make. In the box below are some useful ideas they will hopefully include. If not, you can add them. The points can be put up on the wall to refer to and possibly add to later, as the group builds their teamwork skills. They are also to be found in Handout 2:
Building successful group work
1. Be aware of and open-minded about my own style, and the role I usually play in a group. If I tend to speak a lot, or be pushy or dogmatic about my point of view, try to consciously hold back a bit to allow others space to speak more.
2. Be sensitive to diversity in the group, and the way gender, culture, language, class, education level, etc. can impact on power-relations, and therefore interactions, in the group.
3. Assume all members are doing their best, and want to collaborate, for the group or team to succeed.
4. Communicate clearly, directly and respectfully, to build understanding, and a spirit of cooperation.
5. Make sure we are all clear about the objectives, learning goals, expectations and timing, at the start of the task.
As a facilitator, you can also ensure better group learning by:
Designing well-structured and clear group tasks and assignments, and giving clear instructions, including time;
Constructing groups or teams carefully, taking into account diversity, styles, number of members (not more than 10, but 4-6 is optimal for most tasks);
Monitoring the group work to ensure everyone is on track; Build group work skills (such as in the roleplay above); Assessing and/or giving feedback on the group work.
[Adapted from Finelli, Bergam & Meser: Centre for Research in Learning and Teaching: Occasional papers, 29. University of Michigan]
For next session:
Explain assignment 1 again (refer participants to their Assessment Guides for this)
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 24
Hand out copies of the Thai case study (or refer them to the online reference in their session guide and in the box below), which they will read in preparation for next session. There are guiding questions in Handout 3, which you should also give out to accompany the reading.
Self-study for participants
1. Assignment task 1 – (to be handed in for assessment - see Assessment Guide)
Draw a diagram of own country’s health system, showing its’ key features and their inter-relationships. Use one of the health systems frameworks introduced in this session to help analyse and depict the health system.
Draw a diagram of own country’s health system, showing its’ key features and their inter-relationships. Use one of the health systems frameworks introduced in this session to help you analyse and depict the health system.
Explain why you chose the framework you did –i.e. what about it did you find helpful or particularly applicable?
Write a paragraph on the values base of the system – i.e. What key ethical principles or values underpin it?
2. Read the Thai case study, in Chapter 7 of Good Health at Low Cost (London School of Hygiene and Tropical Medicine), which can be accessed at: http://ghlc.lshtm.ac.uk/files/2011/10/GHLC-book-mono_Chapter-7.pdf
This case of health system improvement will be the focus of next session. To make the best use of the session contact time, they need to read and have a good idea about the case study before the session. The questions in Handout 3 will guide their reading; they should make notes in response to the questions, for better participation in class discussions.
Reading tip for participants: Before you start to read, do a quick survey of the chapter, to get a sense of its structure, and of where you will need to look to find answers to each of the questions. This will save you time, and make your reading more focused.
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 25

Session 3: Key issues in Health System Development: learning from the Thai experience
This session deepens the ideas about what health systems are, showing that they are complex and integrative, and that health system development is a long-term task, influenced by broader political, economic and social forces, and requiring persistence, vision and adaptability.
The session introduces the notion of system effectiveness, and relevant indicators. It uses a case study of Thailand to develop ideas about understanding and strengthening health systems, including the interactions between system hardware and software.
Finally, this session allows time for reflection on teamwork and other ways of learning.
Topics and activities :
1. Feedback on self-study2. Thai case study as an example of health systems
strengthening: Group and class discussion.3. Assessing health system performance and wrap-up of the
Thai experience - Lecture.4. Own learning style. – Individual reflection
1. Self-study feedback (10 minutes)
Start the session with a quick round of comments from participants on how they found their first assignment. The other part of the self-study from last session will be picked up in the next section.
2. Understanding health system development
Reading and discussing a case study (1 hour, 30 minutes):
Task purpose: The task seeks to encourage participants not only to think again about what health systems are, but also – and more importantly – to think about what actions are encompassed within health system development, drawing on a concrete experience. Such actions focus on system development rather than programme development.
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 26
Resources needed:
1. Handout 3 - Thai case study questions.
2. PPT slides (and handouts of PPT) for lecture 3.
Silent reading - Give participants about 10 minutes to re-read the case study, which they should have read before the session. They can start to do this as they arrive for the session.
Video on the Thai case – show the video ‘Good health at low cost – Thailand’, to support the reading and help prepare for the group discussion [download at vimeo.com/45237856] (20 minutes).
Note: If there is not enough time in the session to watch this video, participants can access and watch it in their own time, either before or after this session.
Group discussion - Participants get into groups of approximately 5 - 6 to discuss and make notes on the three questions they were given at the end of the last session in Handout 3. Make sure each group chooses a facilitator and a scribe, to facilitate their group discussion and task. (30 minutes)
Questions for discussion:
What indicators of HS performance improvement does the chapter present? (How do you know the health system has improved over time?)
What health system developments underpin these improvements? Think about a) what health care interventions were of importance and b) what underpinning health system elements were important? Specifically consider what building blocks were addressed over time.
Why/how did these health system developments come about, and generate performance improvements? Think about health policy and system actors, as well as health leadership and governance issues, and the broader political, economic, institutional and socio-cultural context.
Feedback (20 minutes)
Deal with the questions one at a time after groups have had a chance to discuss and record their main points, rather than having formal group presentations about all the questions at the end. Ask each group for one point in response to each question, to limit the feedback time but still give all groups a chance to contribute, then offer your own views to weave into and add to the discussion. Below are some points you might raise:
Question 1. Responses on the first question should be fairly quick and allow you to emphasise that health system performance is multidimensional (linking back to the WHO Building Blocks framework). The chapter data could also be supplemented by the broader data on health inequity change over time. It is also possible to talk about how the data presented covers a
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 27
30-40 year period, so is a really good perspective on health system change. And it would be good to point to some of the broader economic and social/human development indicators (either in the chapter or from elsewhere) to situate health system performance in the wider context.
Question 2. Responses on the second question should focus on service delivery (e.g. types of services, facilities), physical infrastructure, human resource (HR) and financing change, in particular. The details of financing change, in particular, are not necessary to clarify but it is useful to talk to the broad outline of change. It would also be possible to link these developments to access and its dimensions, emphasizing the way service delivery, infrastructure, HR and financing (different building blocks) changes need to support each other – and noting that we do not know much about responsiveness from this chapter. It is possible that people will – quite rightly – also raise improvements in water, education, etc. as health system improvements, taking on board the broad definition of a health system. This is important to note – and then discuss which of the presented health system performance data might reflect such improvements (maybe only IMR), and which other data are important (e.g.basic water and sanitation coverage data). The software of professional values may also be identified and raised and should be noted as relevant. Any issues to do with governance gains (eg decision making processes) should be noted as relevant, but held over to the third question.
Question 3. Responses on the third question are to do with e.g. decision-making processes, consistency in implementation, values, community engagement/perspectives. These can be discussed as governance issues of various types – emphasizing that governance underpins the other building blocks (as proposed by van Olmen et al).
In this discussion, you should also mention some of the issues about health systems raised earlier – complexity, actors, etc., and the links from the experience to HPSR – the types of questions it identifies as relevant, the challenges (e.g. of linking HS interventions to performance measures).
3. Lecture 3: Assessing health system performance and understanding the Thai experience (60 mins)
Lecture purpose and rationale: The lecture aims to consolidate the reading and group discussion. It first considers how to think about health system performance assessment, adding to the issues raised in the ‘What is a health system?’ lecture; and second, it presents a structured analysis about the gains in Thailand and how and why they were achieved. This
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 28

analysis illuminates access issues, the role of health care interventions (interventions that address mortality) and broader system change, action across the Building Blocks, system hardware/software, key actors and relationships, and the governance factors underpinning HS change. It finishes with conclusions from the Good Health at Low Cost book, drawing from across cases, and emphasizes HS and governance issues.
The lecture presents the experience in a particular structure and order to emphasise a way of thinking about health system development, and to highlight key issues that will have been presented earlier in relation to frameworks. Discussion of the system building blocks slide re-emphasises the nature of health systems and the breadth of action relevant in strengthening them. Additional/specific issues that the ‘why and how sustained action’ slides point to are: the time it takes for health system development, complexity (e.g. multiple causality (access), software as an input and output), decision-making processes as key (linked to the notion of policy as process), values and ideology influential, community values/roles, economic resilience in the country (but deliberate decisions!) and that come with being a MIC.
Note: It may be helpful to have wider knowledge of Thailand for presenting this lecture. We suggest you refer to the reference list at the end of the chapter for further reading. A Google Scholar search will also reveal a wealth of references addressing the development of the Thai health system.
Lecture outline (see PPT’s):
Health performance and health system performance – performance dimensions and measures, challenges in measuring and going beyond measurement.
Related to the Thai experience:
health performance and health care performance HS measures - effectiveness, equity and efficiency analysing the experience in terms of the building blocks of health model factors explaining the experience the hardware and software of changes to promote access generating broader societal value sustained action over time : how and why?; beyond specific interventions to system
development social determinants of health involve other sectors more to be done to achieve good health at low cost
Broader related experience
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 29

Remember the caution about health system development.
Try to make this lecture as interactive as possible, by linking back to the group discussions, and getting participants’ input where relevant – for example they can ‘shout out’ ideas for tagging the building blocks model (in the PPT slides), and using the hardware/software model to analyse the Thai case. Wrap up by summarising the lecture, activities and overall intention of the Thai case in the course.
4. Reflecting on learning for own countries (20 minutes)
In country groups, think broadly about the learnings from the Thai experience which could be applied in the case of their own country. They should record some ideas and report these back to the plenary group as key points to take away from the discussion. As the facilitator, summarise the feedback from groups, and highlight common features and interesting points to emerge.
5. Reflecting on ways of learning (10 minutes)
Pair discussion: Ask participants to reflect on the types of activities they have participated in, in preparation for and during this session: self-study, individual reading and note-taking, watching a video, small group discussion and note-taking, plenary brainstorming and facilitator feedback, lecture and note-taking. Share with a partner their own experiences of these as ways of learning, considering:
Which learning mode they found most helpful, and why; What they found particularly helpful in lecture 3; Whether there was any activity they had difficulty with, and why.
Allow a few minutes for feedback to you and the whole class of any insights the pairs think are important to share. It might be useful for you to note these, to help build your future planning and facilitation skills.
If you are interested in finding out more about learning and curriculum, in order to guide the participants’ discussion, you can refer to the following article: ‘Constructive Alignment - and why it is important to the learning process’
http://exchange.ac.uk/learning-and-teaching-theory-guide/constructive-alignment.html
For next session:
Refer participants back to the checklist they developed in Session 2 on Building successful group work. They will use this to reflect on this session.
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 30

Hand out or refer participants to online versions of the WHO reports for 2008 and 2010, as outlined in the box below, for them to read in preparation for next session.
Participants’ Self-study
a. Reflection on group work and own contribution – Refer back to the checklist developed in Session 2 on Building successful group work (Handout 2).
o Which of the points on the checklist do you think are your strongest points, based on your experience over the past 3 sessions?
o Which point/s do you think you personally need to improve on?o What do you think has been your main contribution to group work so far?
b. Reading in preparation for session 4: WHO 2008 report: Primary Health Care: Now more than ever. Pages xi-xx:
Introduction and overview. WHO 2010 report: Health Systems financing: the path to universal coverage. Pages
ix-xxii.
Note: In addition to the focus pages given above for the reports, try to scan the rest of the contents of both reports.
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 31
Session 4: Whole system change – Towards Primary health Care (PHC) renewal and Universal Health Coverage (UHC)
1. Reflections on group work in the last session (10 minutes)
To start the session, ask participants to share briefly with a partner their reflections from the self-study tasks on how the group work went in the last session, and their personal contributions, strengths and challenges.
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 32
This session develops and consolidates ideas about what systems are and how to strengthen them. It focuses on primary health care and universal health coverage as changes affecting all aspects of the health system.
It then asks participants to apply lessons from the Thai case study as well as UHC and PHC to think about and articulate concise ideas about strengthening key elements of their own country’s health system by writing a policy briefing note as an exercise in communication.
Topics and activities:
1. Reflections on self-study task2. PHC and UHC as ‘whole systems’ change’: lecture and
discussion.3. Lessons from Thai experience and UHC/PHC debate for own
country health systems: individual work, thinking pairs, plenary discussion
4. What is required for developing a policy briefing?: Guided brainstorm and discussion, handout
5. Develop a policy brief on an aspect of the Thai experience, for own health system: preparatory brainstorming exercise
Resources needed:
1. PPTs (and handouts of ppts) for lecture 4.
2. Handout 4 - Discussing whole system change in your own country.
3. Handout 5 – Developing a policy briefing
4. Handout 6 - Recognising agents in health systems

2. Lecture 4: Whole system change: towards PHC renewal and universal coverage (UHC) (1 hour)
Lecture purpose and rationale: The lecture provides a brief outline of these two globally recognised health system reform thrusts, building on the Thai experience. It shows how these two areas of reform overlap, as well as pointing out some differences between them (the PHC stronger focus on service delivery, the UHC focus on financing). It notes that they propose change across multiple building blocks. It identifies as a common area of concern, the need for leadership in bringing about health system change, and discusses the nature of that leadership. It ends with five rules for systems change derived from a Canadian realist review on whole system change. The leadership focus is a foundation for sessions 5-7.
Lecture outline (see PPT)
The lecture presents key issues from the 2008 and 2010 WHO Annual reports addressing PHC and UHC respectively. It shows the links between the two reform movements and highlights key elements of each, emphasising key common focus points on leadership, as a governance issue. It addresses:
Building blocks, contemporary system-level interventions and underlying principles Service delivery issues Why PHC and what it consists of; what distinguishes it from conventional health care Definitions of UHC and what is needed to achieve it – model: 3 ways of moving to UHC Tackling the waste problem Actions to be taken in different settings Governance and leadership of whole system change
3. Lessons from Thai experience and UHC/PHC debate for own country health systems (40 minutes)
In thinking pairs, participants consider the following questions (in Handout 4) about health system improvement in their own countries for about 10 minutes, then share these in their country groups, noting 3-5 points to take back to plenary:
Discussing whole system change in your own country
In country groups, discuss the following questions:
What health system improvements (similar to or different from those in the Thai experience) have taken place in your country recently? Which relate to PHC and which to UHC? Use one of the diagrams presented in the lecture on whole systems change (Lecture 4), as well as the timeline you developed for your own country’s health system to think about the changes.
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 33

Why/how did these health system developments come about? Think about health policy and system agents, as well as health leadership and governance issues, and the broader political, economic, institutional and socio-cultural context, as drivers of the changes.
In plenary, gather a few key points from each pair, and guide a discussion on common themes emerging, picking up on and reflecting back to the lecture.
4. What is required for developing a policy briefing? (20 minutes) – leave sub-section on policy brief out, depending on time available
A policy brief is a short document which can be written to inform and advise actors in the health system – probably non-specialist decision makers - about an important issue which requires new or changed policy or action in a particular context. The brief presents research findings, and makes recommendations or a ‘call-to-action’ based on these. A policy briefing provides an opportunity for intervention for strengthening health system performance.
Participants can gain a sense of what is involved in writing a policy briefing by working in pairs or groups to discuss and think through an example, as in the guided activity below (Handout 5). You will need to move around the groups, checking that they are clear about the questions and suggested responses in the table.
Activity: Thinking about what should go into a policy briefing
Work through an example of a policy briefing, as outlined below:
1. Identify a scenario in which a policy brief is required in order to implement a change in the HS. You can choose a topical or widely applicable scenario (for example - motivating for a change in policy about advertising and/or selling soft drinks in schools in an attempt to reduce sugar intake of youth), or you can choose a scenario which is specifically relevant to the participants, or taken from the Thai experience.
2. Work through the questions in the second column in the table below to guide their thinking about how they should structure the brief, what it should include, and why. The kinds of responses they could consider are suggested in the third column. They should use the table as a guide, but come up with their own specific responses, in relation to the topic they have chosen for their policy brief.
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 34

Topic of Policy Briefing:
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 35

Question about Questions Possible responses
Purpose What is the purpose of the policy brief? What aspect of the health system is it aiming to address?
To convince decision-makers that there should be a policy related to this issue, or that the existing policy needs to be changed.
Audience Who will be the audience the policy brief will address?
What will they need to know?
Are they likely to be open to your recommendations on the issue or resistant?
The audience is decision- or policy-makers who are not necessarily experts on this issue. They will need scientific/technical as well as contextual information in order to understand the issue properly. They will probably need to be convinced about the issue, and might be resistant to a change in policy for various reasons.
Content What information do you need to include, in order to get your message across convincingly to your audience?
We would need to include focused information about: purpose of the brief; background or context of the issue; description and scope of the issue; research done on it, including methods used; implications of the research; recommendations based on the research; summary of main points; statement of key message; references; contact details of the writers/experts.
Structure How could you structure this information so it is clear and concise for the readers?
The briefing should have at least the following components, in this order:
Introduction to/identification of the problem;
Description of background/context;
Summary of key research done on the issue, methods used and relevant results;
Implications of the research for policy/ practice;
Recommendations based on implications of the research;
Summary of main points and statement of the key message – a ‘Call to action’;
References for research, and contact details of writers/experts for follow-up.
Language In what way should you write the brief, to convince your audience of the importance of the issue and action to be taken?
The issue should be clearly focused and written in clear, concise and direct language. Use active, not passive verbs; include questions to focus attention; use shorter sentences for impact; avoid
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 36

jargon.
Format How can you make the brief easy to read and interesting to look at?
Keep the brief short (about 1500 words); use strong headings, and bullet points or tables to clarify; highlight key points in boxes or sidebars; use graphics where possible; don’t crowd too much onto a page.
5. Develop a policy brief on an aspect of Thai experience for own health system (30 minutes)
Note: This activity and the self-study task following it can be omitted if you prefer, or if you have a time constraint.
Working in country groups of 3- 5, or groups whose countries have similar health system issues, participants plan writing a policy brief for their own context:
Brainstorm - In the groups, brainstorm possible policy brief issues for strengthening the HS in their countries, based on the lecture and their reflections from the self-study on ‘lessons from the Thai experience for my own country’. Remind them that in a brainstorm, all ideas are acceptable, and all will be ‘put into the pot’ to consider. A scribe should be chosen to note all the ideas offered.
Sort and discuss – Discuss the ideas which emerged from the brainstorm session, discarding those which do not seem good options for developing policy briefings. Each participant choose an issue they would like to focus on, and clarify it with other group members.
Plan the writing of the brief – Groups go through the ideas in the table above, discussing how they could apply these to their own policy briefs and making sure they are clear about each of the points, in preparation for their individual work. As facilitator, you can move around, making suggestions and giving explanations where helpful. This is participants’ opportunity for guidance and clarification, so encourage them to ask questions!
For next session
Hand out the five readings in the box below, for them to read in preparation for next session, and Handout 6, which has the questions they need to think about. Allocate readings so that equal numbers of participants read each paper.
Participants’ self-study
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 37

1. (Note: Can be omitted) Develop a policy briefing note on strengthening an aspect of own health system environment, learning from the Thai experience. The policy brief should be approximately 1500 words, and should use appropriate headings, format and language to convey important information about the issue you have chosen to promote. You will have to research the issue to supplement your own knowledge and be able to provide convincing information. Complete the table you were given in the session and your group discussion to help you plan and write your brief.
2. Readings: Read one of the papers below, on people in systems, as allocated by the facilitator. All the papers focus on actors and decision-making, and all talk to some aspects of organizational decision-making. In your reading, try to identify the factors influencing implementation of agents’ attitudes and behaviours, and how power is exercised in this implementation:
Mumtaz, Z. et al. (2003).Gender based barriers to health care provision in Pakistan: the experience of female providers. Health Policy and Planning. 18(3): 261-269
Wibulpolprasert, S. & Pengpaibon, P. (2003). Integrated strategies to tackle inequitable distribution of doctors in Thailand: four decades of experience. Human Resources for Health. 1(12). http://www.human-resources-health.com/content/1/1/12
Penn-Kekana, L. et al. (2004). ‘It makes me want to run away to Saudi Arabia.’: management and implementation challenges for public finance reforms from a maternity ward perspective. Health Policy and Planning. 19 (suppl 1): i71-i77.
Meuwissen, L. E. (2002). Problems of cost recovery implementation in district health care: a case study from Niger. Health Policy and Planning. Sept: 17(3): 304 – 13
George, A et al. (2011). Community case management in Nicaragua: lessons in fostering adoption and expanding implementation. Health Policy and Planning 26(4): 327-37
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 38

Session 5: Recognising agents in health systems
This session focuses on the central role of people in health systems. It focuses on the importance of people’s values and mindsets, agency and power as drivers of their behaviour, and that all these impact on how health systems function.
Topics and activities:
1. 1. Readings about people in systems: Group discussion of range of papers; plenary discussion
2. 2. Systems dynamics - people in the system: Squaring the circle exercise
3. 3. What drives health system actors?: Lecture; plenary discussion
1. Discussion of papers about people in systems (1 hour)
Re-read of the papers – Participants quickly read over the paper they prepared for the session. (10 minutes)
Group discussion – In groups of 3-5 participants who have read the same paper, discuss the set of questions below (Handout 6). They should have thought about these questions in their preparatory reading. Remind groups, in their thinking, to make the link back to the influence of system interventions over behaviour and attitudes. They should select a facilitator and a scribe to note their responses, which they will report back. (30 minutes)
Questions for discussion: Who are the health system agents of focus in this paper? What routine behaviours and practices are discussed in the paper, and what consequences are
identified for: other agents, any dimension of health system functioning and performance (think, for example, about different building blocks, the relationships among them, access to health care, health care provision and quality, or broader performance dimensions)?
What factors are identified as influencing those behaviours and practices? Can you discern whether and how power and trust are present in these experiences?
Plenary report back – Gather points from each group on one question at a time and write onto newsprint, so the papers can be compared more easily. Close by summarizing the key points
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 39
Resources needed:
1. Handout 6 – Questions for readings on recognising agents in health systems
2. Handout 7 – Summary of readings on agents in systems
3. PPTs (and handouts of PPTs) for lecture 5.
4. Gorilla video (in lecture)
5. Reading (optional) – Lehmann & Gilson 2013
6. Handout 8a – Budgeting scenario

emerging from the groups, and inviting participants’ comments or questions on these. Hand out a summary of the papers (Handout 7). (20 minutes)
2. Systems dynamics – people in the system (30 mins)
Squaring the circle Game - A good way of introducing students to the concept of people in systems is to involve them in an activity in which they have to participate as a member of a team to solve a systems problem. ‘Squaring the circle’ is a game which does this, by challenging the group to re-design a system and become a ‘self-organising unit which finds its own order through teamwork, visualization and systematic thinking.’ (Sweeney and Meadows, 1995: 115)
What you will need: A space large enough for all the participants to stand in a loose circle; a rope, cord or thick string at least 10 metres long, tied together at the ends to make a big loop; a scarf, bandage or other cloth as a blindfold for each of the students.
Purposes of the game:
To work out a way of making a square with the rope, while they are all blindfolded; To work as a team in order to develop a strategy to solve the problem- i.e. to become a
self-organising system in order to succeed in a task; To explore the concept of team learning; To examine what happens when communication is limited.
Instructions:
1. Stand in a row, side by side, and put on your blindfolds.2. Take hold of the rope lying on the ground in front of you (the loop of rope should have
one half at their feet and the other half further away from them, so they are all bunched together along half of the rope).
3. You are going to make a square with the rope. Don’t let go of the rope, but you can move along it to space yourselves out. You can speak while you do this.
4. When any one of you thinks the square is ready, put up your hand. I will then take a vote, and if most of the group agrees the task is completed, I will tell you and you can stop and take off your blindfolds. If not, the group must carry on until most members think you are done.
5. When you are satisfied with your square, I will tell you to put the rope down carefully in front of you, and take off your blindfolds.
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 40

Debriefing questions and discussion - To guide the reflection and learning from this game, ask the following questions (and any others you think will be helpful to achieve the purposes of the game):
What was the group’s strategy and how did you develop it? How effective was your communication, and how did being blindfold affect it? How effective was your teamwork and what were its strengths and weaknesses? What were the group dynamics? Did a leader emerge, and was s/he successful? What did you learn as a team about successfully completing the task, and how did you
learn it? How is what happened in the game similar to what happens in real life, for example in
workplaces?
What will probably emerge is that the process of (re-)designing a system is more effective if all participants listen to each other and try to understand and agree on a plan before taking action. It is not usually helpful for an authoritarian ‘leader’ to try and dictate what everyone must do to solve the problem.
(Adapted from Sweeney, L.B. and Meadows, D. (1995) The systems thinking playbook. Page 114 - 119)
3. Recognising agents in health systems, and complexity - Lecture 5 (1 hour)
Lecture purpose and rationale: To encourage deeper thinking about health system agents and what influences their behaviour, as a basis for thinking about leadership for health system change. Specifically introduces the understandings that agents’ behaviour is driven by mindsets, values and interests; and that they exercise power in acting. Makes links back to the readings, and to the discussion of the complexity of health systems, and that they are socially constructed. Introduces the ideas that health system change is unpredictable, shaped by the past and by agents, and generating unintended consequences: that change is emergent. This is taken forward in session 7.
Lecture outline (see PPT)
The lecture considers who health system agents are and discusses how their behaviour is driven by mindsets, values and interests and how they exercise power in acting.
It includes the “Invisible gorilla” video clip and an activity identifying the number of letters in a short text, to illustrate differences of perception of the same image/idea. It also considers implications for what systems ‘are’ and how to change systems.
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 41

As this is a long lecture, encourage some interaction, both through use of the slides and by asking participants questions at relevant points relating to the papers they read, such as, “In the paper you read, what power did you identify?”. Think of further questions you could ask to engage participants.
It is also a good idea to break the lecture briefly in the middle to ask participants to reflect individually on themselves as agents in the health system, by noting their own primary position in the system, their interests and power in that position, and how it impacts on others. Ask for a ‘shout out’ of some of their responses.
For next session:
(Optional) Hand out Lehmann & Gilson reading for consolidation of this session if you have chosen to set this additional task, as a way of developing participants’ critical reading skills.
Hand out the budgeting scenario for participants to read for next session (Handout 8a). Do not give out the tasks or Forms 1- 3 (Handout 8b) for the budgeting scenario until next session.
Questions and points to guide the readings are in the box below, and included with the scenario.
Participants’ Self-study:
a. Read the scenario on HS budgeting, to prepare for doing stakeholder analysis next session. As you read, think about:
what the main features of this case are – i.e. what happened; who the key agents are in this case and what their positions are; what impact the new policy and procedures will be likely to have on them; what power they might have, in turn, to impact on the implementation of the policy.
b. (Optional) Read the following paper to support your reflections on the concepts introduced in this session, and write up your responses, focusing on people in systems, their different values, power and mindsets:
Lehmann, U. & Gilson, L. (2013) Actor interfaces and practices of power in a community health worker programme: a South African study of unintended policy outcomes. Health Policy Plan. 2013 Jul; 28(4):358-66.
In reading the paper, consider some of the following questions:i. What is the main message you took from the paper with regard to
agents and power?ii. What are the roles of different agents in the case, and what kind of
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 42

power do they have?iii. What are the implications for managing change and for policy
implementation in the case described?iv. What were the causes of the unintended policy outcomes?v. What influences the agents’ behaviour, values and judgements?
vi. What did you like or find particularly interesting about the paper?vii. What questions are you left with, after reading the paper?
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 43

Session 6: Understanding agents’ mindsets, interests and power
The focus of this session is on applying the ideas from Session 5 and thinking about the roles of health system actors in relation to the process of system change. The session looks at agents’ values, beliefs, mindsets, and power relations, and considers how behaviour and attitudes influence system performance. It then considers the significance of the different views actors have of health systems and the world, for health systems development, reflecting also on the interaction between system software and hardware.
Topics and activities:
1. Feedback on academic reading task (if done): Group discussion2. What is stakeholder analysis? Lecture; discussion3. Stakeholder analysis in practice: Group exercise based on
budgeting scenario; de-briefing
1. Feedback on academic reading task (if done as self-study task) - (20 minutes)
Count off, or otherwise allocate participants to mixed groups of 4 – 6 which they will work with for the whole session, and the next session. In these groups they start by discussing the reading, comparing notes about the main points they took from the reading, what they found most interesting about it in relation to the concepts of people in systems, mindsets, values and power, as well as any questions they had emerging from the paper.
In plenary, gather a few key points from each group, and give relevant feedback on these, discussing and responding to any questions that arose from the paper for participants.
2. What is Stakeholder Analysis? – Lecture 6 (20 mins)
Lecture purpose and rationale:
This short lecture aims to introduce participants to stakeholder analysis (SHA) as a management tool, in order to prepare for an application exercise. Through the lecture, they
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 44
Resources needed:
1. PPT slides and handouts of slides for Lecture 6
2. Handout 8a – Budget scenario
3. Handout 8b – Tasks on recognising agents in systems (+ 3 forms)

should have a sense of what is involved in doing stakeholder analysis, and what it aims to achieve.
Lecture outline (see PPT’s):
The concept of stakeholder analysis and a definition are introduced. Ask participants to briefly share any knowledge or experience they have of SHA and its use. The lecture explores the concept of a stakeholder as someone with a vested interest in a situation, who may be visible or invisible. The function and challenges of SHA as a management tool are explained. The lecture also discusses relevant agents to consider when doing SHA, and why they should be considered. Finally, a useful table for analyzing stakeholders’ levels of power and commitment is presented and discussed.
Some of the main considerations for a stakeholder analysis include:
Stakeholders positions on a policy or reform proposal Levels of influence and resources they hold and potential power struggles Their level of interest in the reform as a priority for them Group and individual associations and alliances among stakeholders Divergences and confluences of viewpoints Possible impact of the reform Potential strategies for negotiation
The needs and purposes of particular contexts dictate the criteria chosen for consideration in any particular stakeholder analysis.
Depending on the purpose of the stakeholder analysis, levels of interest and power can be indicated on a scale for each actor, to establish their relative positions on an issue or policy and therefore how to approach them. Categories such as these can be helpful in identifying actions to be taken to influence and lead change in agents.
Using stakeholder analysis – In small groups participants share ideas about how they have used or could use stakeholder analysis in their own contexts, then feed some points of interest back to plenary.
3. Doing a stakeholder analysis (2 hours)
Mapping health system agents – Group task (1 hour)
In groups, participants work through the instructions in the box below (Handout 8b). The handout includes Forms 1, 2 and 3, to be completed as part of this exercise.
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 45

1. Quickly review the health system change story related to HS budgeting which you read in preparation for this session (no more than 15 minutes).
2. In your groups, identify 4 key health system agents located at district and hospital levels.
3. For each of the chosen actors discuss and complete Forms 1 and 2 in your handout, focusing in particular on their experience around the newly introduced budgeting procedures.
Note that you will also need to use your own judgements about the actors and how they are likely to react/behave – drawing as relevant from lecture 5 and the set of papers discussed in session 5.
4. With your responses on these issues for each selected actor, complete Form 3 by plotting them on the agent map, as they would be positioned in early days of the implementation of the new budgeting procedures. Their positions might change over time. Copy this form onto a large chart which can be put up and seen by the whole group.
5. Be prepared to present and answer questions on your agent map (Form 3) in plenary, drawing on your discussions and responses in Forms 1 & 2 to explain why you have mapped the agents where you did, and how and why their positions might change over time. You can elect a rapporteur to do this, or choose to respond to questions as a team.
De-briefing (20 mins)
Gallery walk - Put up the agent maps from all the groups, where participants can move around and read them, comparing the maps and noting any differences in location of actors across the groups.
Presentation – Each group present and explain their map, with reference to their group discussion around Forms 1 & 2.
Q and A – In plenary gathering, participants and facilitator pose any questions they have to groups for clarification of their rationale for locating agents where they did on the maps.
After each presentation, lead a round of applause, to acknowledge the work done by each group, and encourage lively responsiveness from the audience.
Discussion – Ask questions to analyse and summarise the agent maps overall, such as:
Who seem to be the key highly committed agents in this scenario with power, and why are they important to focus on?
Who seem to be the most hostile agents, and why are they likely to be so?
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 46

Are there any uncooperative/ hostile agents who have high power, and are these important to focus on?
Task feedback (20 mins)
After the de-briefing, give further input on agents in HS, picking up on points emerging from the group discussion, and highlighting, for example, the points below:
All agents have some form of power, not just central level policy agents Even central level actors have power limits in bringing about change, in terms of front line
service delivery Complexity results from many different actors with different understandings and
interests, and from different but concurrent streams of change The power of agents at the periphery is important to and for health system functioning and change
Power can be exercised overtly or covertly, and includes the power to shape the mindsets of others
Agents exercise their power in response to concerns about how new HS developments will impact on them
Agents responses to new HS developments reflects their ‘mindsets’ (both individual and group mindsets about, for example, past experience of change, rumours of bad experiences) and values (e.g. responses to the principles of performance-related pay, or the need for team working)
Summary of the task and process (15 mins)
Summarise the process and purpose of the stakeholder analysis task, asking participants for their responses to questions such as: How did they find the task?; What do they see as the potential value of doing stakeholder analysis?; Any weaknesses or difficulties they envisage with the process?
For next session
Hand out (or give online reference for) the reading for next session, and refer participants to the session 6 guide for questions to guide their reading.
Self-study
Read the following paper in preparation for session 7, and think about the questions below as you read:
Barnes, P.C. (1995) Managing change. BMJ. 310: 590-2
Questions:
What were the main management challenges posed in the case?
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 47

What are the five aspects of change leadership that Barnes describes in the paper?
Session 7: Leading change in health systems
The main aim of this session is to introduce ideas for understanding and managing agents in health system change. Using a range of analytic frameworks it will focus on complexity and agency, but also, the understanding that health systems are knowable and changeable. Participants will begin to develop strategies which support intervention and change in systems.
Topics and activities:
1. Managing agents and change: Discussion of readings; lecture (commitment planning; small wins; sense-making)
2. Video on complexity and development: Viewing and discussion3. Managing agents and commitment planning: Group task
developing strategies for managing change using SHA scenario; feedback discussion
1. Leadership of change in health systems – Lecture 7 (40 mins)
Lecture purpose and rationale
The lecture introduces ideas and approaches to thinking about leadership of change within health systems, picking up the prior discussion of leadership in relation to PHC and UHC, the session on agents, and the stakeholder analysis. It also links back to the Barnes reading, and provides the basis for the subsequent task(s). It considers key dimensions of leadership, as distinct from management, and introduces ideas relevant to understanding, and working to change, health systems as complex adaptive systems – such as sensemaking and the importance of relationship building. It covers both the basic ideas needed to think about leadership of design processes and of implementation processes.
Lecture outline:
Leadership: where things can go wrong; starting points and processes;
Leadership of design: re-design; managing co-design;
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 48
Resources needed:
1. PPTs (and handouts of PPTs) for lecture 7.
2. Handout 8a – Budgeting scenario
3. Handout 9 - Leading the implementation of change in systems
4. Three case studies

Leadership of implementation: recognizing complexity; starting points for leaders; use of power; sensemaking; paying attention to relationships; commitment planning and building commitment; small wins; learning through doing; building chances of success in HS change.
Try to use a discursive approach to the lecture, by asking questions where relevant, giving examples participants can relate to and asking them for ideas and examples based on their experience of leading change. Refer to the examples from the Barnes reading, and to the Duncan Green video they will view next, focusing on the role of complexity in leadership.
2. Video on complexity and development - Duncan Green (video 30 mins; discussion 10 minutes)
https://www.youtube.com/watch?v=yeE78qgC2ag#t=196
Introduce the video, by a development specialist from Oxfam, making links back to the lecture. This video also links with the rest of the course, especially the last session, which focuses on complexity.
Ask participants to think about the following question as they watch the video:
According to Green, how does complexity influence the approach we should take to managing/leading, in relation to planning, responding, enabling change and working with people?
Discussion - After watching the video, participants break into thinking pairs to take turns to share their thoughts on the video and the main points they took from it in relation to the lecture. Time each partner’s turn to speak for 5 minutes. Thereafter, in plenary, take some key ideas from each pair, and lead a discussion on the salient points emerging from the lecture and video relating to leadership of change and complexity. Summarise these points in preparation for the exercise.
3. Managing change (1 hour 30 mins)
Participants work in the same groups they had for the previous session, using Handout 9 - as below. They can refer to the agent maps they produced in that session, as well as the lecture and readings, as a basis for this group exercise on managing change. You will need to move around, guiding the groups to ensure they are on track and managing their time well. Groups should once again choose a facilitator and a scribe (preferably different from those in the previous session).
Exercise: Leading implementation of change in systems (45 mins)
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 49
In this exercise, you will work with the agents map you produced in the last session. You may want to adapt this now, as a result of the plenary discussions during the session.
Position yourselves in the role of a returning district manager - a medical doctor who has just completed an MPH (health policy and systems specialization). You see real potential for better managing the district with the new budget procedures, and plan to develop strategies for change. Start by thinking about yourself in the role of district manager/doctor in the scenario. In this role, consider what key principles and approaches will drive your behaviour in leading change - your hopes and aspirations, your interests, how you engage with others, how others see you, what power you have and what the limits are on that power.
Now develop your strategies for taking forward the new budgeting procedures. Record your main points to report back briefly on each of the following: (15 minute report back)
i. Describe the future & publicise the change
Given the change being planned/ implemented, and the mindsets and interests of the key agents you are considering, what overarching vision of the future might provide a cause that generates greater commitment across agents for the change? How can this vision be publicized? What channels of communication are relevant for different agents?
ii. Commitment and action planning:
Recognising your position, power and personality in your role as the district manager, consider:
Who might be key champions to offer leadership in different places? Who might your allies be? What role might there be for professional leaders (e.g. doctors), and for patients, their families and community members? (Use Form 4 to record your ideas for this)
What actions might be needed to change particular agents’ positions and generate commitment?
What small win(s) might generate commitment across agents – perhaps by tackling a key constraint on wider change?
Presentations (30 mins) – Bring two groups together, and each group takes a turn to present and share their ideas with the other. They should note any common or interesting points that emerged, and any questions or difficulties that arose. As facilitator, move between the groups, getting a sense of the presentations and providing feedback.
Plenary discussion (15 mins) – Lead a discussion with the whole group on the purpose of the tasks and the main points to emerge from them both, with reference back to the lecture on leadership of change. Highlight:
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 50
the central, enabling role of leadership in effecting change, working through and with people
the significance of mindsets and values in leading change – both those of the leader and others
the importance of sensemaking around shared vision
For next session:
Introduce and explain Assignment 2, as detailed in the Assessment guide. Allocate case studies to groups of 3-5. For a change of dynamics and to enable
participants to work with a wider range of others, these should preferably be different groups from previous sessions. Hand out the case studies for the relevant groups; they will read the narratives in preparation for their tasks next session, together with the set of questions to guide their reading (in their Session 7 guide).
Participants’ self-study
a. Assignment 2: Leadership moving towards action - Take forward your thinking about strengthening your own health system, incorporating ideas from this session and developing strategies for change in your own environment (This assignment should be handed in for marking - see assessment guide).
b. Guided reading of allocated case studies in preparation for next session. You don’t need to think about the tasks linked to the case study yet – these will be tackled in your groups next session. As you read the case, however, think about the following questions:
o Which aspects (building blocks) of HS is this case mainly about?o What are the key issues here?o Who are the most important agents involved and how do they impact on
implementation of the policy?
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 51
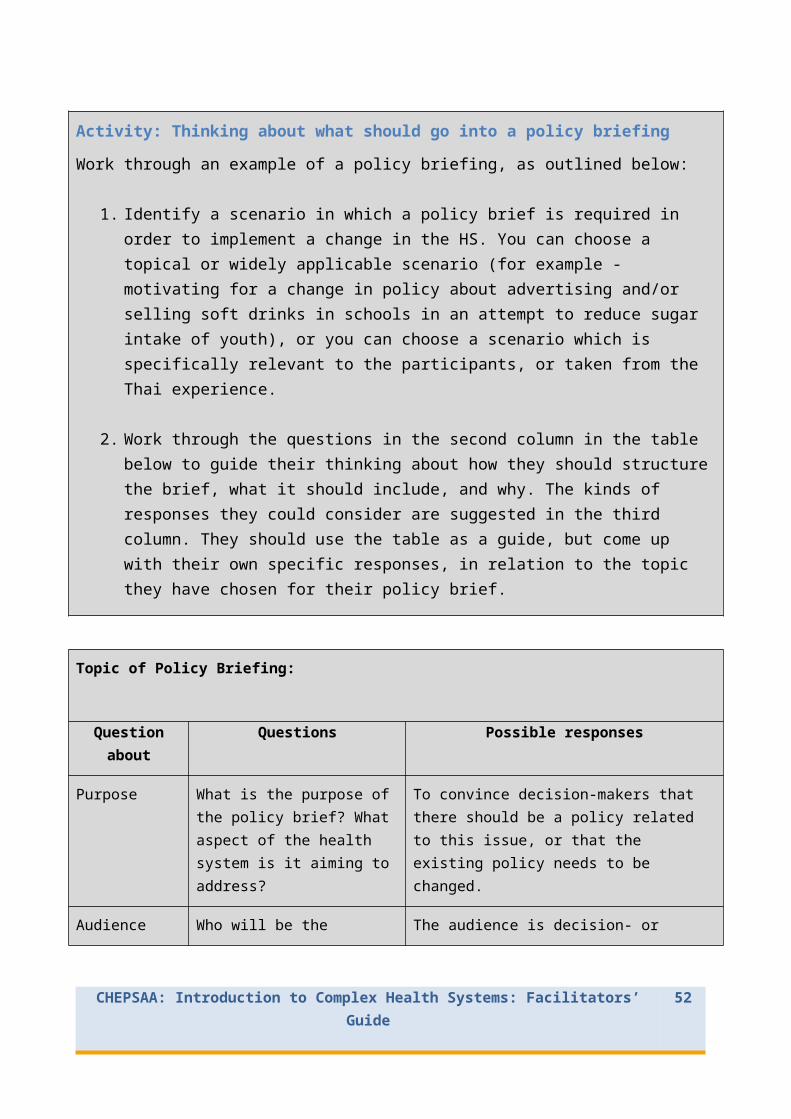
Session 8 - Intervening in health systems – case studies 1
This session starts to pull together all the strands of the course, by taking an in-depth look at a range of case studies of health systems’ change. Sessions 8 and 9 will talk to the integrative and dynamic nature of health systems, the centrality of agents in shaping these systems, and opportunities for generating change through addressing both the hard and the soft aspects of systems. The sessions will require teamwork skills.
Topics and activities:
1. Review reading of case studies: Group reading and discussion2. Health system strengthening – what the case studies reveal:
Guided group discussion and activities based on specific case study.3. Input and discussion of skills for making presentations: Buzz
groups; group discussion
1. Introduction to the use of case studies (10 minutes)
The next two sessions are based on a set of case studies, which have been chosen to highlight the complexity in HS, and the central role of agents in systems, with a focus on effecting systematic change towards improving health delivery. The purpose of working on case studies at this point is to bring together the concepts covered in the course in an integrated application exercise.
Give a brief overview of the three cases, and remind students that the group tasks will lead to a group presentation, which will be marked and contribute to their individual assessment.
Give a brief explanation of the purpose and value of using case studies in a course like this.
Cases offer the opportunity to apply, in an active way, the concepts learned on the course, in order to solve real-life problems and think about ways in which change can be generated for strengthening of HS. The cases we are using are integrative, drawing on concepts from the
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 52
Resources needed:
1. Three case studies with accompanying tasks
2. Handout 10 - Points to consider for making an effective presentation
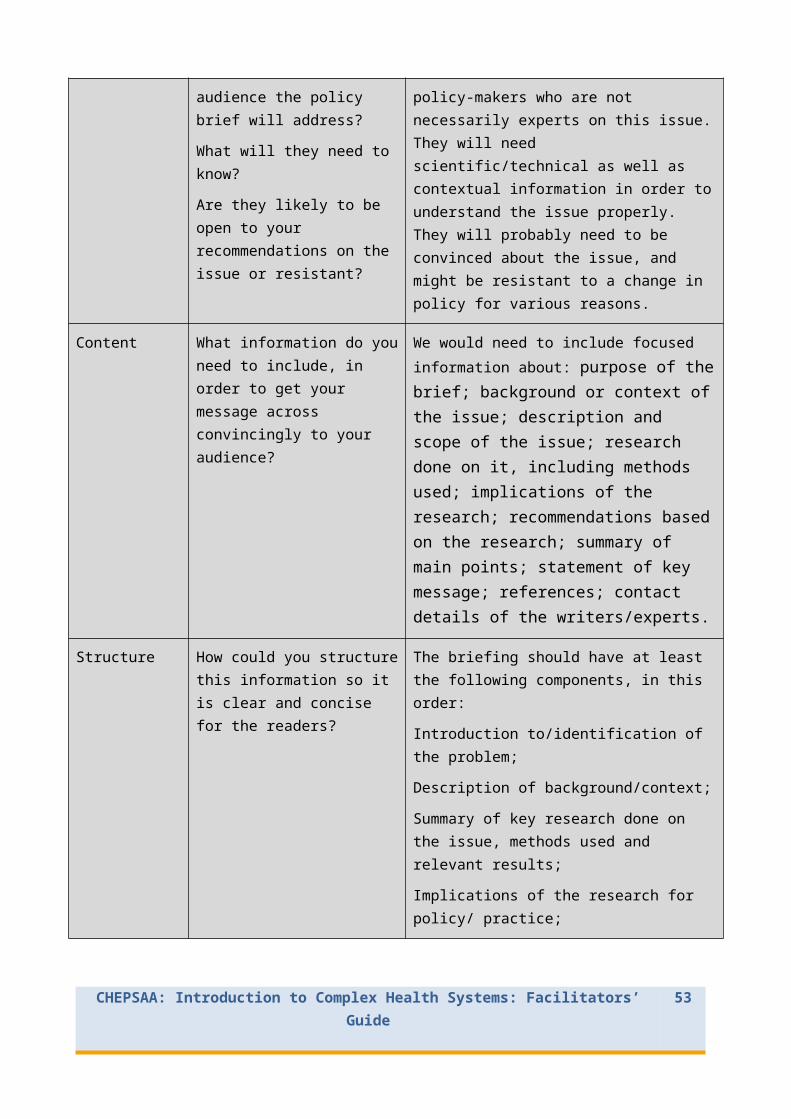
entire course and allowing consideration of both what to do to strengthen health systems and how to manage the process of institutional change that health system development entails, including actor management. The cases also aim to:
focus on an in-depth, specific (preferably African) experience, rather than a set of experiences;
address implementation dimensions, although not always including detailed front line implementation experience;
focus on macro-service delivery, governance, financing and/or HR related changes; or large scale programme development with system implications (not on programme only experiences);
encompass both public and ‘private’ sector experience.
The objectives of case studies should relate to the learning outcomes and threshold concepts underpinning the course. In line with these, some objectives of the case studies we are using are therefore that they should stimulate and guide students to:
Understand, in practice, the dynamic and complex nature, and the social constructedness of health systems
Analyse roles, inter-relationships, influence and power among stakeholders in a situation
Understand that health systems involve both ‘software’ and ‘hardware’. Analyse ways that policy impacts on actors Explore mechanisms that give actors power or influence over policy development Work out the types of strategic action that can be used for policy implementation
and/or development, towards health system strengthening
Working on the cases will require team skills and effective communication strategies, which are also intended learning outcomes of the course. Remind groups to refer back to the teamwork skills they considered in sessions 2 and 3, in order to work well as a team on their case studies. It will help to appoint a leader and a time-keeper in the group, to ensure that they stay on track with the discussion and tasks, as well as a scribe to record their discussion and main points, and a rapporteur who will present the work in the next session.
2. Working with the cases (2hrs 20 mins)
Groups briefly re-read and then discuss their case study narratives and the tasks, including the time-frame and how they will tackle the tasks (see Case study handouts). They should have read the case study already in preparation for the session, so the reading should not take more than about 15 minutes. Each group should appoint a facilitator, time-keeper and scribe. As overall facilitator, you might need to move from group to group, checking they are clear about the contexts of their cases, and offering guidance and additional information where appropriate, but not intervening unnecessarily.
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 53

30 minutes before the end of the session, stop the group work, to focus on presentation skills. Groups can complete their group tasks after the session if necessary.
3. How to make an effective presentation (30 minutes)
Buzz groups – Discuss what makes a presentation effective, considering two aspects – preparation, and delivery. Gather points from the groups and list them, adding from those below, if they were not raised. These are in Handout 10 as well, which you can give out now:
Points to consider for making an effective presentation
Preparationo Consider your audience, and design the presentation so that the level,
language and content are appropriate for them;o Make sure you have covered all the necessary/important information;o Organise your points/ideas in a logically and clearly structured way;o Introduce the presentation with an attention catching question or
comment, and a brief preview of the content;o The body of the presentation should have clear main and sub-points;o Conclude the presentation with a brief re-statement of the main points or a
summarising comment. Delivery
o Have your information ready (in Powerpoint or some other form);o Keep to the allocated time (if possible ask a colleague to check the timing
for you);o Speak clearly and not too fast;o Use eye contact with the audience; don’t just read;o If you use Powerpoint, face the audience, not the screen;o Powerpoint slides should be visually pleasing and not overloaded, with no
errors;o Try to vary your pace and intonation, and move around the space, to
maintain interest;o Use body language to maintain interest, but avoid distracting movements or
gestures.Practice your presentation beforehand, if possible getting feedback from a colleague.
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 54
Finalising presentations - Groups plan their presentations for next session, allocating specific tasks and roles to the group members, so all can contribute to the presentation in different ways. Marks will be allocated mainly for content of the presentation, so the actual delivery is not the most important factor.
For next session
Check that all groups are in a position to finalise their presentations for the next session. Some might need more guidance, or to arrange extra time to meet and work on their presentation; you might need to facilitate this.
Participants’ self-study
Work collectively or individually on whatever part of the group presentation members are responsible for, to finalise the preparation for next session.
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 55

Session 9: Intervening in health systems– case studies 2
This session continues the in-depth look at case studies and what they reveal about health policy and systems in practice, calling for the ability to demonstrate an understanding of health systems’ contribution to public value and societal development. The session will also require presentation and team work skills, and allow reflection on both. The group presentations can be marked by participants in class (as a peer assessment), and the marks included in the total course assessment.
Topics and activities:
1. Presentation of case studies: Group presentations and feedback
2. Cross case review of experiences; implications for action in and across cases: Plenary discussion
3. Reflection on teamwork and leadership in relation to the group task: Plenary discussion
1. Finalisation of presentations (15 mins)
Allow a short time for groups to finalise their presentations and ensure they have all the materials and equipment they need.
2. Group presentations, peer assessment and discussion (2 hrs 30 mins)
Before the presentations - hand out and briefly discuss the suggested assessment rubric (below and Handout 11) which groups in the audience will use to assess the presentations. You can decide whether peers allocate marks or just give comments. You can also decide whether each group should particularly observe, comment on and mark only one other group; or all groups comment on all other groups. Make this clear to participants at the start.
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 56
Resources needed:
1. Handout 11 - Group presentation assessment criteria
2. Papers to read for journal club next session (x3)
3. Handout 12 – Questions to guide reading of papers on complexity.
Group Presentation Assessment Criteria
Group:
Mark allocation
Group’s mark
The overview of the case is clear and succinct and gives a good sense of what the case is about, using clear images.
10
Comments:
The hardware and software issues at play in the case, and their relationship, are clearly explained.
10
Comments:
The roles of actors, their mindsets, interests and power are presented and explained convincingly; their relationships and changing positions in time are clearly shown.
10
Comments:
The suggested strategies for leading change are realistic and well- motivated, with reference to the theory introduced in the course.
10
Comments:
e) Delivery of the presentation (visual and oral) is clear, using appropriate pace and level, and content is coherently and logically structured.
10
Comments:
Total 50
General comments:
Presentations - Each group has a maximum of 15 - 20 minutes for their presentation (this is assuming there are about 4 groups - you can adjust the time if you have fewer or more groups).
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 57
After the presentations - Allow 5-10 minutes after each presentation for brief feedback, clarification and discussion questions to the group, then another 5 minutes after this for filling in the rubrics with marks and/or comments. These can be shared and discussed at the end (sharing them after each presentation could disadvantage the groups that present first, and distract those who present later!), or handed to the facilitator (to maintain anonymity) if there is likely to be sensitivity about peer marking. Try to encourage participants to see peer assessment as a constructive exercise, however, with learning for both the assessors and those being assessed.
For next session
Introduce the assessment/assignment and explain the procedure. Divide the class into three groups. Each group will read one of the papers in the box
below, in preparation for the journal club activity next session. Hand out the readings, together with the guiding questions (Handout 12). Make sure all participants are clear about which paper they should read.
Participants’ self-study
1. Reading on CAS in preparation for session 10.
Read one of the three papers below, as allocated by your facilitator, for the journal club activity next session. Use the questions in Handout 12 to guide your reading of the paper:
Blanchet, K. (2013). How to facilitate social contagion? International journal of health policy and management, 1(3), pp.189–92.
Gilson, L. et al. (2014). Advancing the application of systems thinking in health: South African examples of a leadership of sensemaking for primary health care. Health research policy and systems / BioMed Central, 12(1), p.30.
Rwashana, A.S., Williams, D.W. & Neema, S. (2009). System dynamics approach to immunization healthcare issues in developing countries: a case study of Uganda. Health informatics journal, 15(2), pp.95–107.
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 58

Session 10: Health system complexity and change
The final session aims to wrap up the course by deepening understanding of complex adaptive systems and linking this understanding to the different concepts, frameworks and ideas introduced in the course. The session will place particular emphasis on the analytic skills of participants in being able to apply new concepts in different contexts, and on communicating ideas and understandings to an audience.
Topics and activities:
1. Review of case studies; application of CAS concepts to case studies: Plenary discussion
2. Reflection on team work: Group discussion3. Participant-lead journal club, discussing papers applying complex
adaptive systems (CAS) thinking and concepts to health systems: Group and plenary discussion
4. Wrap-up lecture and discussion linking CAS thinking to core concepts discussed in the course: Interactive lecture
5. Course evaluation: Group discussion; individual written task
1. Review of case studies (20 mins)
Lead a discussion to draw together the various experiences in the case studies and summarise key concepts emerging, related to central issues in the course, by asking questions such as:
What were the main points emerging from the case studies? Were there any experiences or issues common to all the cases? What can we learn
from this? What implications for practice and action can we draw from the cases? Did the case studies reinforce or clarify any concepts introduced in the course? Which?
2. Reflection on team work (20 mins)
Groups re-gather to reflect on their experience of the group work, guided by the following questions in Handout 13:
In your group, consider:
a) How was the experience of working as a team, including:
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 59
Resources needed:
1. Handout 12 - Questions for journal club readings
2. Handout 13 - Reflection on team work
3. Handout 14 – Summary of papers on complexity
4. PPT’s and PPT handouts for lecture 8
5. Handout 15 - Course evaluation

i. Participation and openness?ii. Sharing of task?
iii. Time management?iv. Learning from each other?v. Enjoyment and value of the experience?
b) What can we learn from the feedback we received?c) What could we do to improve such group work and presentation in future?
After 10 minutes’ group discussion, invite each group then share two insights from their reflection with the whole class.
3. Participant-lead journal club (1 hour)
Explain the following reading process for the journal club and then guide participants through it. You will have to organise and time the steps carefully so they can change groups and follow the logistics of all the steps easily:
Paired co-readers – In pairs or 3’s who have read the same paper, participants discuss the main points for 15 minutes, to clarify and support their reading of the paper, guided by the questions they were given (Handout 12 below).
Questions to guide journal club readings:
1. What concepts and ideas presented in this course does the paper speak to?
2. What do you agree and disagree with in what you have read?
3. What does the paper tell you beyond what you heard in the course that is of importance to your understanding of health systems as complex adaptive systems?
Jig-saw reading – Re-group into 3’s who have all read different papers. Each group member has 5 minutes to present the key points of their paper to the others in the group, so that all participants will have a sense of all the papers. Time each 5 minutes, and clearly indicate when one reader should stop and the next should start to speak.
Establish common points – In the same groups, for another 10 minutes, readers of the different papers look for common points emerging from the papers, speaking to complexity in systems.
Plenary overview – Lead a plenary discussion on the key points in the papers, and their relevance to course concepts. This should link with and lead into the lecture that follows. Handout 14 offers a summary of the key points from all the papers.
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 60

3. Closing lecture: CAS and health systems – Lecture 8 (I hour)
Lecture purpose and rationale:
The lecture aims to draw together the main threads of the course and remind participants of these. It also aims to highlight key aspects of and concepts related to complexity and systems thinking as the culmination of the course thinking.
Lecture outline:
Summary of the course and where it was going;Threshold concepts underpinning the course – were they addressed?;Key concepts relating to complexity, referring back to the papers read;Systems thinking and change – leverage and tipping points, leadership for complexity, different approach to problem solving.
Try to create interaction in the lecture by asking questions and inviting contributions of ideas in relation to some of the slides – e.g. ask participants to comment on whether they ‘got’ each of the threshold concepts of the course; and to suggest other complexity concepts for the list, and whether these were adequately covered in the course. Also relate back to the key points from the journal club readings on complexity.
At the end of the lecture, ask for a shout-out on participants’ ‘freshest thoughts’ about complex adaptive systems – they should offer short, quick phrases or even single words to reflect a sense of the concepts they have taken from the session. Capture some of these on a flipchart as a summary of the session, commenting on them and providing some feedback to pull together the points as relevant.
4. Course evaluation (20 minutes)
Students complete the course evaluation form below individually (Handout 15).
To get a sense of the overall response, when they have completed the forms do a quick round in which each participant in turn reads out one of the things that they enjoyed in the course; another round for one of the things they learned; and another for the things that could have been better. If you have time and think it would be helpful, some discussion of some salient points could follow, to create a sense of closure to the course.
Participants’ Self Study
Summative assessment: See assessment guide for details.
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 61

1. Please rate the following from 1 – 5 (1 = not at all; 2 = a little; 3 = satisfactorily;
4 = more than adequately; 5 = very much):
The course was relevant to me and my work ____
I gained valuable knowledge on the course ____
The methods of presentation/facilitation were effective ____
2. Please complete each of the following:
Things I particularly enjoyed about the course were: ____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
___________________________________________________________________
Things I learned on the course which are important to me were: _______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
It would have been better if: ____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
___________________________________________________________________
Any other comments or suggestions (for example about networking with fellow students going ahead): _________________________________________________________________________________________________________________________________________________________________________________________________________
___________________________________________________________________
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 62

References and further reading
Aragón, A. O. (2010). A Case for Surfacing Theories of Change for Purposeful Organisational Capacity Development, IDS Bulletin 41(3).
Balogun J. (2006) Managing change: steering a course between intended strategies and unanticipated outcomes. Long Range Planning 39:29–49.
Balogun J. (2003). From blaming the middle to harnessing its potential: creating change intermediaries. British Journal of Management 14:69–83.
Barnes, P.C. (1995) Managing change. British Medical Journal. 310: 590-2
Best, A. et al. (2012) Large system transformation in health care: a realist review. The Milbank Quarterly 90 (3): 421 – 456
Birn A-E, Pillay Y., and Holtz TH. (2009) Textbook of International Health: Global Health in a Dynamic World. New York: Oxford University Press.
Blanchet, K. (2013). How to facilitate social contagion? International journal of health policy and management, 1(3), pp.189–92.
Brinkerhoff D.W., Bossert T.J. (2008). “Health Governance: Concepts, Experience, and Programming Options.” Health Systems 20/20. Washington, DC: USAID. February. http://www.healthsystems2020.org
Brinkerhoff D., Bossert T (2013) Health governance: principal–agent linkages and health system strengthening. Health Policy and Planning (2014) 29 (6): 685-693.
De Savigny, D. ,Adam, T., 2009. Systems thinking for health systems strengthening. World Health Organization. url: http://whqlibdoc.who.int/publications/2009/9789241563895_eng.pdf.
Drath WH (2003) Leading Together. Complex challenges require a new approach. Leadership in Action 23(1). http://www.centerforcreativeleadership.com/leadership/pdf/publications/lia/23_1leadingtogether.pdf
George, A et al. (2011). Community case management in Nicaragua: lessons in fostering adoption and expanding implementation. Health Policy and Planning 26(4): 327-37
Gilson, L. (2012) Health systems and institutions. In R. Smith & K. Hanson, eds. Health systems in low- and middle-income countries: an economic and policy perspective. Oxford: Oxford University Press.
Gilson, L. et al. (2014). Advancing the application of systems thinking in health: South African examples of a leadership of sensemaking for primary health care. Health research policy and systems 12: 30 http://www.health-policy-systems.com/content/pdf/1478-4505-12-30.pdf
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 63

Frenk J. (1994) Dimensions of health system reform. Health Policy 31;27(1):19-34.
Kruk M., Freedman L (2008). Assessing health system performance in developing countries: a review of the literature Health Policy. 2008 Mar;85(3):263-76.
Kusek, J. Z. et al. (2013) Fail-safe management: 5 rules to avoid project failure. Washington: The World Bank
Lehmann, U., Gilson, L. (2013) Actor interfaces and practices of power in a community health worker programme: a South African study of unintended policy outcomes. Health Policy Plan. 2013 Jul; 28(4):358-66.
Meuwissen, L. E. (2002). Problems of cost recovery implementation in district health care: a case study from Niger. Health Policy and Planning. Sept: 17(3): 304 – 13
Mounier-Jack, S. et al. (2014). Measuring the health systems impact of disease control programmes: a critical reflection on the WHO building blocks framework. BMC public health, 14(1), p.278.
Mumtaz, Z. et al. (2003). Gender based barriers to health care provision in Pakistan: the experience of female providers. Health Policy and Planning. 18(3): 261-269
Penn-Kekana, L. et al. (2004). ‘It makes me want to run away to Saudi Arabia.’: management and implementation challenges for public finance reforms from a maternity ward perspective. Health Policy and Planning. 19 (suppl 1): i71-i77.
Smith, R. & Hanson, K. eds. (2012). Health systems in low- and middle-income countries: an economic and policy perspective. Oxford: Oxford University Press.
Rwashana, A.S., et al. (2009). System dynamics approach to immunization healthcare issues in developing countries: a case study of Uganda. Health informatics journal, 15(2), pp.95–107.
Sheikh K., et al. (2011) Building the Field of Health Policy and Systems Research: Framing the Questions. PLoS Med 8(8): e1001073. http://www.plosmedicine.org/article/info:doi/10.1371/journal.pmed.1001073
Sheikh, K., et al. (2014). People-centred science: strengthening the practice of health policy and systems research. Health research policy and systems. 12:19. http://www.health-policy-systems.com/content/12/1/19.
Scott, V. et al. (2012). Constraints to implementing an equity-promoting staff allocation policy: understanding mid-level managers’ and nurses’ perspectives affecting implementation in South Africa. Health Policy and Planning. 27(2): 138-146.
Svitone, E. C. (2000). Primary health care lessons from the Northeast of Brazil: the Agentes de Saúde Program. Rev Panam Salud Publica/Pan Am J Public Health 7(5): 293-302 http://www.scielosp.org/pdf/rpsp/v7n5/2361.pdf
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 64
Topp, S.M., et al. (2014) Understanding the dynamic interactions driving Zambian health centre performance: a case-based health systems analysis. Health policy and planning, (advance access) http://heapol.oxfordjournals.org/content/early/2014/05/14/heapol.czu029.full.pdf+html
Van Olmen, J. et al., (2012). The Health System Dynamics Framework: The introduction of an analytical model for health system analysis and its application to two case-studies. Health, Culture and Society, 2(1), pp.0–21. url: http://hcs.pitt.edu/ojs/index.php/hcs/article/view/71/96
Van Olmen, J. et al. (2012) Health systems frameworks in their political context: framing divergent agendas. BMC Public Health 12:774 doi:10.1186/1471-2458-12-774
WHO. (2007). Everybody’s business: Strengthening health systems to improve health outcomes: WHO’s framework for action. Geneva: World Health Organization. http://www.who.int/entity/healthsystems/strategy/everybodys_business.pdf
WHO (2000) World Health Report 2000 – Health systems: improving performance. Geneva: WHO
Wibulpolprasert, S., Pengpaibon, P. (2003). Integrated strategies to tackle inequitable distribution of doctors in Thailand: four decades of experience. Human Resources for Health. 1(12). http://www.human-resources-health.com/content/1/1/12
CHEPSAA: Introduction to Complex Health Systems: Facilitators’ Guide 65





























