Embed Size (px)
Citation preview

European Heart Journal (1997) 18, 507-513
Accuracy and reproducibility of biplanetwo-dimensional echocardiographic measurements of
left ventricular dimensions and function
J. E. Otterstad*, G. Froeland*, M. St. John Suttonf and I. Holmet
* Division of Cardiology, Vestfold Central Hospital, Toensberg, Norway; ^Cardiovascular Division, Hospital of theUniversity of Pennsylvania, Philadelphia, U.S.A.; \Life Insurance Companies' Institute for Medical Statistics,
Ullevaal Hospital, Oslo, Norway
Objective To investigate sources of variability in serialechocardiographic recordings in a core laboratory we as-sessed the impact of repeated echo recordings, repeatedvideo measurements and measurements made by differentinvestigators.
Patients, methods Two investigators each recorded andanalysed two-dimensional echos in 12 individuals (n = 24 intotal) three times at one week intervals. Left ventricularend-diastolic and end-systolic volumes were measured usingthe biplane modified Simpson's rule. Ejection fraction wasderived from these volumes and left ventricular mass esti-mated using the area-length method. The left ventricularspherity index was expressed as the ratio of the short axisarea and the long axis area at end-diastole. A videorecording from each examination was reexamined twice byboth investigators.
Results Deviations between repeated echo recordings andrepeated video measurements ranged from — 5 to +5%
between investigators. A three-way repeated analysis ofvariance indicated a small, but systematic difference be-tween investigators. Reproducibility, measured by coef-ficients of variation, ranged from 3-9% for differentinvestigators, 3-6% for repeated video measurements and7-19% for repeated echo recordings across the differentvariables. The total variability of all three factors should beconsidered when the smallest detectable significant changein a variable is assessed. These ranged from 16-28% acrossthe five variables studied, when a 10% error of classificationwas accepted for a one-sided change in a variable.
Conclusion Repeated echo recordings were the dominantcomponent of variation. Two-dimensional echo measure-ments are reproducible and accurate, but the same investi-gator should follow the same patients.(Eur Heart J 1997; 18: 507-513)
Key Words: Two-dimensional echocardiography, leftventricular dimensions and function, reproducibility.
IntroductionTwo-dimensional echocardiography has been widelyused in clinical trials because it allows repeated non-invasive tomographic imaging of the heart withoutexposure to ionizing radiation. In a number of clinicaltrials the use of a core echo laboratory has beenadvocated to which different investigator sites send allecho videotapes'1"5'. The core laboratory serves twomajor functions: to maintain quality control of two-dimensional echo recordings and to minimize thevariability in echocardiographic measurements11'45'.However, there is little information regarding the accu-
Revision submitted 26 March 1996, and accepted 28 March 1996.
Correspondence: Dr Jan Erik Otterstad, MD, FESC, Divisionof Cardiology, Vestfold Central Hospital, N-3100 Toensberg,Norway.
racy or reproducibility of repeated echocardiographicmeasurements of left ventricular size and function inpost-infarction patients in whom such measurementsmay be confounded by the presence of left ventricularwall motion abnormalities.
The purpose of the present prospective study wasto assess the accuracy and reproducibility of biplanetwo-dimensional measurements of left ventricular vol-umes, ejection fraction, cavity shape and myocardialmass. In addition, we evaluated the impact upon thesemeasurements of three factors: repeated two-dimensional echo recordings made at examinations witha significant time interval between them, repeatedmeasurements made from the same video recordings,and the intra-observer and inter-observer variabilitywithin the echo core laboratory in normal subjectsand post-infarction patients with regional wall motionabnormalities.
0195-668X/97/030507+07 S18.00/0 1997 The European Society of Cardiology
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/18/3/507/498019 by guest on 27 D
ecember 2021

508 J. E. Otterstad et al.
Study population and methods
The study population was divided into two groups.Group 1 consisted of 12 healthy volunteers employedfull-time as anaesthesiologists in our hospital of whom11 were male and 1 was female and whose ages rangedfrom 30 to 57 (mean 43) years. All underwent a near-maximal bicycle ergometer test, without any symptomsor electrocardiographic evidence of myocardial ischae-mia. Their exercise capacity was normal and comparableto a previous study in healthy individuals'61.
Group 2 consisted of 12 patients all of whomwere male, who ranged in age from 52 to 73 (mean 65)years and who were recruited consecutively from ouroutpatient clinic. All had sustained a transmural acutemyocardial infarction more than one year previously,but were clinically stable, in sinus rhythm, not in con-gestive heart failure and whose medications did notchange throughout the study period. No patient wasexcluded on account of a technically unsatisfactorytwo-dimensional echocardiogram.
Two investigators, both experienced echocardi-ographers (J.E.O. and G.F.), each obtained two-dimensional echos in 12 subjects, six in Group 1 and sixin Group 2, i.e. 24 subjects in total. All subjects hadthree echocardiograms obtained at weekly intervals.Each two-dimensional echo required a left parasternalview of the short axis of the left ventricle at themid-papillary muscle level; apical four-chamber andapical long axis views were all obtained during breath-held expiration. Two-dimensional echo recordings wereacquired for at least 1 min in each view, while electro-cardiograms were recorded simultaneously on superVHS videotape using a Hewlett Packard (HP) Sonos1500 and commercially available analysis software. Allvideo recordings were reexamined twice by both investi-gators, with an interval of over a week between the twoexaminations. Thus, each investigator performed threerepeated two-dimensional echo recordings, and accord-ingly 12 repeated video measurements per subject werestudied. All two-dimensional echos were obtained withthe subject in the left lateral recumbent position. Theintercostal space and the distance of the transducerfootprint from the mid sternum was noted at baselineand used as a reference for repeated video recordings.
Left ventricular volumes and ejectionfraction
The endocardial surfaces of the apical four-chamber andapical long axis echocardiographic images were digitizedat end-diastole and end-systole from a minimum of threecardiac cycles in breath-held expiration to obtain leftventricular areas. End-diastolic areas were digitizedfrom apical biplane echo images coincident with thebeginning of the Q-wave on the electrocardiogram.End-systolic areas were digitized from video frames nearthe end of the T-wave with the maximum inward motionof the left ventricular walls. An example of endocardial
Figure 1 Apical four-chamber view from a patient inGroup 2 (post-myocardial infarction) with endocardialtracings and left ventricular long axis. Top: end-diastole;bottom: end-systole.
tracings in the apical four-chamber view is shown inFig. 1 (top: end-diastole; bottom: end-systole). Figure 2presents an example of such tracings in the apical longaxis view (top: end-diastole; bottom: end-systole). Whiledigitizing the endocardial borders, minor irregularitiesdue to decreased integrity of the left ventricular endo-cardium were interpolated by reviewing the previous andsubsequent echo frames in real-time, in slow motion, orin single frame advance mode. The papillary muscleswere excluded from the endocardial tracings and re-garded as left ventricular cavity similar to quantitativeangiography. The lengths of the long axis of the leftventricular cavity were measured from the apex to themid-point of the mitral plane in both apical views (Figs1 and 2), in order to minimize foreshortening of thecavity. Left ventricular volumes were calculated at end-diastole and end-systole on HP Sonos 1500 softwareusing the modified Simpson's rule from biplane pairedechocardiographic apical images in the four-chamberand long axis views, as recommended by the AmericanSociety of Echocardiography'71. Mean values for end-diastolic and end-systolic volumes were calculated from
Eur Heart J. Vol. 18, March 1997
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/18/3/507/498019 by guest on 27 D
ecember 2021

Biplane 2-D echocardiography of L V function 509
Figure 2 Apical long axis view from a healthy subject(Group 1) with endocardial tracings and left ventricularlong axis. Top: end-diastole; bottom: end-systole.
the three cardiac cycles analysed. In order to optimizerepeated echo recordings and repeated video measure-ment, each investigator had access to 'stop-frames' ofthe endocardial tracings at end-diastole and end-systolefrom baseline recordings. Left ventricular ejection frac-tion was derived from the biplane volumes as thedifference between end-diastolic and end-systolic vol-umes expressed as a percentage of end-diastolic volume.
Left ventricular mass
To calculate left ventricular mass (LVM), the endocar-dial and epicardial boundaries of the left ventricularshort axis images from the left parasternal region weredigitized at end-diastole to obtain endocardial (cavity)area — Aend and epicardial (total) area — Aepi (Fig. 3).The apical epicardial and endocardial left ventricularlong axis length (Lepi and Lend) were measured in theapical four-chamber view (Fig. 1 (top)) and left ventricu-lar mass was calculated using the 5/6 (area x length)method previously described181:
Figure 3 Parasternal short-axis view at mid-papillarymuscle level from a healthy subject (Group 1) — end-diastole. Endocardial and epicardial tracings are shown.The average distance between the two circles is taken asleft ventricular wall thickness.
LVM = 105 x 5/6 (Aepi x LAepi - Aend x LAend).
1 -05 is the density of myocardium.
Left ventricular cavity shape
Left ventricular cavity shape was defined in terms of aspherity index (SI), and calculated as the ratio of end-diastolic short axis area (EDASa) and the mean longaxis cavity area (EDAav) from the two apical views:
SI = EDASa/EDAav
A spherity index (SI) of unity represents a sphere.
Statistical methods
The accuracy of repeated video measurement and re-peated echo recordings were first assessed by calculatingpercentage deviation of means from baseline to eachrepeated video measurement per echo recording andper investigator. A three-way factorial (repeated)measurements design analysis of variance (ANOVA)was performed to determine whether any interaction waspresent between the factors: repeated video measure-ments, repeated echo recordings and observer, and ifnot, did any of these factors show a systematic vari-ation with the relevant variable to be analysed. Acheck of interaction with patient type (sustained acutemyocardial infarction or not) was also performed.
Reproducibility was assessed from the three-wayANOVA model using estimates of within-subject vari-ance components for each factor. Coefficients of vari-ance were used as statistics to estimate reproducibility.The total variability (standard deviation) within subjects
Eur Heart J, Vol. 18, March 1997
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/18/3/507/498019 by guest on 27 D
ecember 2021
510 J. E. Otterstad et al.
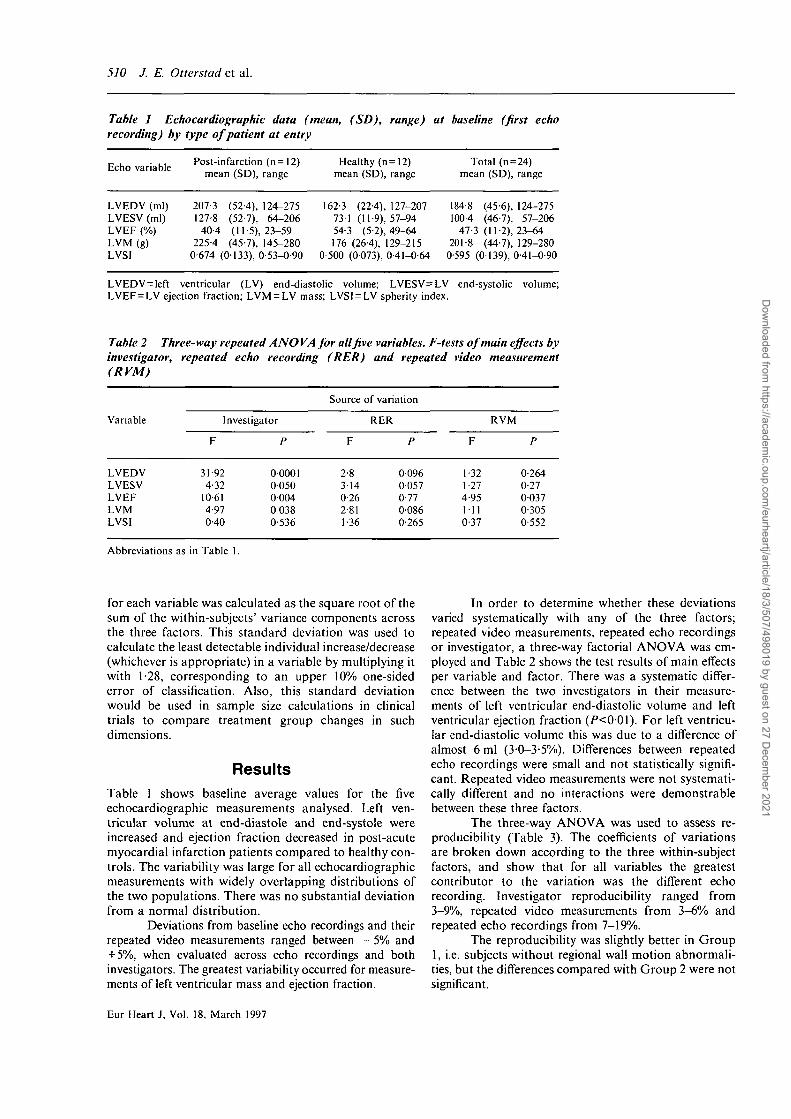
Table 1 Echocardiographic data (mean, (SD), range) at baseline (first echorecording) by type of patient at entry
Echo variablePost-infarction (n=12)
mean (SD), rangeHealthy (n= 12)
mean (SD), rangeTotal (n = 24)
mean (SD), range
LVEDV (ml)LVESV (ml)LVEF (%)LVM (g)LVSI
207-3 (52-4), 124-275127-8 (52-7), 64-206
40-4 (11-5), 23-59225-4 (45-7), 145-280
0-674 (0133), 0-53-O-90
162-3 (22-4), 127-207731 (11-9), 57-9454-3 (5-2), 49-64176 (26-4), 129-215
0-500 (0073), 0-41-0-64
184-8 (45-6), 124-275100-4 (46-7), 57-206
47-3 (11-2), 23-64201-8 (44-7), 129-280
0-595 (0139), 0-41-0-90
LVEDV = left ventricular (LV) end-diastolic volume; LVESV=LV end-systolic volume;LVEF=LV ejection fraction; LVM = LV mass; LVSI = LV spherity index.
Table 2 Three-way repeated ANOVA for all five variables. F-tests of main effects byinvestigator, repeated echo recording (RER) and repeated video measurement(RVM)
Variable
LVEDVLVESVLVEFLVMLVSI
Investigator
F
31-924-32
10-614-970-40
P
00001005000040 0380-536
Source
F
2-83140-262-811-36
of variation
RER
P
0-0960-0570-770-0860-265
F
1-321-274-951110-37
RVM
P
0-2640-2700370-3050-552
Abbreviations as in Table 1.
for each variable was calculated as the square root of thesum of the within-subjects' variance components acrossthe three factors. This standard deviation was used tocalculate the least detectable individual increase/decrease(whichever is appropriate) in a variable by multiplying itwith 1-28, corresponding to an upper 10% one-sidederror of classification. Also, this standard deviationwould be used in sample size calculations in clinicaltrials to compare treatment group changes in suchdimensions.
ResultsTable 1 shows baseline average values for the fiveechocardiographic measurements analysed. Left ven-tricular volume at end-diastole and end-systole wereincreased and ejection fraction decreased in post-acutemyocardial infarction patients compared to healthy con-trols. The variability was large for all echocardiographicmeasurements with widely overlapping distributions ofthe two populations. There was no substantial deviationfrom a normal distribution.
Deviations from baseline echo recordings and theirrepeated video measurements ranged between — 5% and+ 5%, when evaluated across echo recordings and bothinvestigators. The greatest variability occurred for measure-ments of left ventricular mass and ejection fraction.
In order to determine whether these deviationsvaried systematically with any of the three factors;repeated video measurements, repeated echo recordingsor investigator, a three-way factorial ANOVA was em-ployed and Table 2 shows the test results of main effectsper variable and factor. There was a systematic differ-ence between the two investigators in their measure-ments of left ventricular end-diastolic volume and leftventricular ejection fraction (/)<001). For left ventricu-lar end-diastolic volume this was due to a difference ofalmost 6 ml (3-0-3-5%). Differences between repeatedecho recordings were small and not statistically signifi-cant. Repeated video measurements were not systemati-cally different and no interactions were demonstrablebetween these three factors.
The three-way ANOVA was used to assess re-producibility (Table 3). The coefficients of variationsare broken down according to the three within-subjectfactors, and show that for all variables the greatestcontributor to the variation was the different echorecording. Investigator reproducibility ranged from3-9%, repeated video measurements from 3-6% andrepeated echo recordings from 7-19%.
The reproducibility was slightly better in Group1, i.e. subjects without regional wall motion abnormali-ties, but the differences compared with Group 2 were notsignificant.
Eur Heart J, Vol. 18, March 1997
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/18/3/507/498019 by guest on 27 D
ecember 2021

Biplane 2-D echocardiography of LVfunction 511
Table 3 Coefficients of variation (%) from model-basedthree-way repeated ANOVA calculations of within-subjectvariability according to the three factors: investigator,repeated echo recording (RER) and repeated videomeasurement (RVM)
Table 5 Differences in average changes to be detectedwith 80% or 90% statistical power during a randomizedtrial. Comparison of changes in echocardiographic vari-ables between two groups (n=250 or n=500 per group)
Variable
LVEDVLVESVLVEFLVMLVSI
Investigator
4-883195-658-32903
RER
11-567-54
121714-8618-80
RVM
2-824-505-655-855-23
Total
12-869-34
14-56180121-50
Abbreviations as in Table 1.
Table 4 Clinical limits for individual increases/decreasesbased on 10% one-sided classification error (Za=l-28)due to random variation, accounting for the threefactors: repeated video measurement (RVM), repeatedecho recording (RER) and Investigator (INV). Method:SD=~4MSR VM+MSRER+MS/Ny, where MSs are calcu-lated mean squares within subjects from three-way re-peated A NOVA. Upper cut-off limits for individualchanges to be of clinical significance are shown
Variable
LVEDVLVESVLVEFLVMLVSI
S D x 1-28
30-4 ml20-2 ml
8-5%46-6 g
0167
% (of mean)
16-320018123-327-6
Abbreviations as in Table 1.
Individual increases or decreases in the echocar-diographic measurements over time should not be re-garded as clinically significant unless they exceed the90% one-sided percentage point in the normal distribu-tion, with a standard deviation equal to the total within-subject standard deviation calculated from the ANOVAtable, i.e. 1 -28 x SD. This means that the least significantdetectable increase/decrease will lie in the range of16-28% for the five variables studied (Table 4), with16-3% for left ventricular end-diastolic volume, 200%for left ventricular end-systolic volume and 181% forleft ventricular ejection fraction. These percentagescould then be used as individual cut-off limits to define aclinically significant increase/decrease in any of theseechocardiographic measurements. Sometimes it is neces-sary to detect both a decrease and an increase, so atwo-sided approach may be desirable. In these cases theupper 5 percentage points in the normal distributionmay be more appropriate. If so, then 1 -65 x SD shouldreplace 1-28 x SD.
This within-patient standard deviation may alsobe used to find the smallest average change necessary toobtain a predefined statistical power for a given samplesize in a clinical trial. Table 5 gives an example of a
Variable
LVEDV (ml)LVESV (ml)LVEF (%)LVM (g)LVSI
80%
n = 250
8-35-52-33
12-70-045
Statistical
n = 500
5-940110910033
power
90%
n = 250
9-86-52-7
1500054
n = 500
6-94-71-94
10 60-038
Method: a=j2 x SD; a=005 (two-sided). SD = within-patient totalstandard deviation from three way repeated ANOVA.Abbreviations as in Table 1.
500-patient or a 1000-patient randomized trial with halfthe patients allocated to a treatment and half to aplacebo group. The table shows that the net difference inthe average changes of left ventricular end-diastolicvolume has to be about 6 ml to have 80% power with asample size of 500 patients per group. A similar differ-ence for left ventricular ejection fraction would have tobe 11%.
Discussion
The accuracy of left ventricular volumes and functionwith two-dimensional echocardiography in the presentstudy was reflected by minor deviations of measurementby both investigators (Table 2). In an echocardiographiccore laboratory in a multi-centre study, at least twoexaminers should be operative in order to ensure qualitycontrol and immediate response to all videotapes re-ferred from investigator sites. Although there was closeagreement between the two investigators for most of theechocardiographic measurements, significant differenceswere noted in left ventricular end-diastolic volumes andleft ventricular ejection fractions. Before initiation ofthis study, consensus was reached regarding the princi-pal guidelines on how to identify and digitize the leftventricular endocardium. The left ventricular apex wasregarded as dome-shaped, and the endocardium ident-ified by important internal landmarks, such as theinsertions of mitral valve and papillary muscles.
The major component of the random variationin left ventricular volumes and function was repeatedecho recordings. By contrast, repeated video measure-ments and inter-observer variability did not have suchan important impact. Small differences in angulationand placement of the transducer during serial echorecordings may influence measurements of left ventricu-lar dimensions. To reduce this effect, still video framesfrom the baseline recordings were used for optimalreconstruction of left ventricular long and short axes. Arelatively high gain setting was used to obtain good
Eur Heart J, Vol. 18, March 1997
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/18/3/507/498019 by guest on 27 D
ecember 2021

512 J. E. Otterstad et al.
endocardial echoes. To further improve reproducibilityof serial examinations, still frames of baseline endocar-dial tracings were used during repeated examinations,but numerical values were not available. This use ofbaseline stop-frame images and endocardial outlines did,however, eliminate true 'blinding' of the measurements.
In addition to methodological pitfalls, biologicalfactors may cause variations in left ventricular dimen-sions and function. Thus, loading conditions may differdue to several factors including variations in intravascu-lar volume, adrenergic drive, or in the post-absorptionalstate after a meal. Biological factors may account for asmuch as 50% of the total variability encountered inrepeated echo examinations (R. B. Devereux, personalcommunication). The findings in the present study con-firm that a substantial component of the total variabilityobserved may be related to biological factors, since thecombined variability of repeated video measurementsand more than one investigator was only 40% of thevariability related to repeated echo recordings (Table 4).However, the study did not address to what extentbiological factors are responsible for the variability inrepeated echo recordings.
Hitherto, most studies on the reproducibility oftwo-dimensional echo measurements have not incorpor-ated the influence of repeated echo recordings. In theecho substudy of SAVE[I], 50 video recordings werereexamined three times by the same investigator, withstandard deviations of 3-5% for diastolic cavity area and2-9% for systolic cavity area. These findings are similarto those in the present study as regards repeated videomeasurements of left ventricular end-diastolic and leftventricular end-systolic volumes (Table 4). Senior et alP]
reexamined video recordings and evaluated inter-observer variability in post-acute myocardial infarctionpatients, and found similar reproducibility for repeatedvideo measurement and investigator, but did not incor-porate repeated echo recordings in their study. However,these studies'191 used video recordings from post-acutemyocardial infarction patients. Gordon et al.[io] per-formed repeated echo recordings at 2-4 day intervalsand found lower standard deviations for left ventricularvolumes and ejection fraction when compared to thepresent study. These studies are not strictly comparable,however, because Gordon et a/.[10' used a single planefour-chamber view for left ventricular volume calcu-lations according to the area-length method of Sandierand Dodge1"'. According to Albin and Rakho'12', apicalbiplane images using Simpson's rule, as used in thepresent study, is the most accurate of various formulaetested against radionuclide left ventricular volume andejection fraction measurements.
The reproducibility data obtained in an estab-lished core laboratory with two experienced investi-gators may not represent the average standard at each ofthe investigator sites participating in a multicentre study.Not all investigators will be experienced echocardiogra-phers, and the quality of the echo equipment at somesites may differ from that of the core laboratory. Thus,the overall variability in a multicentre study may be
greater than that observed in a core laboratory. On theother hand, the subjects in the present study were notselected in any way, but were recruited consecutivelyfrom the anaesthesiology department and outpatientclinic, respectively. In the echo substudy of SAVE only66% of baseline video studies were accepted for analy-sis1'1. In the DEFIANT-I and -II trials, a prerequisite forinclusion was that patients were 'echogenic'[4'5]. Thus,inclusion bias in multicentre studies may tend tocounteract the possible negative influence on variabilityrelated to different investigators and echocardiographicequipment.
In many clinical studies, changes in indices of adisease are used to classify patients into groups accord-ing to progression/no progression or regression/no re-gression of the disease index. To avoid classificationerrors, changes have to exceed certain cut-off limits toallow for random variation. Thus, it is essential toidentify the sources of individual random variationinvolved, estimate their magnitude singly and combined,and use the estimate of total within-patient variability inorder to define the cut-off points for individual changesabove or below which disease progression/regression hasoccurred. Usually, upper fractions of the normal distri-bution are used for this purpose, i.e. 1-28 or 1-64(Z-values) times the global standard deviation ofchange, including all sources of variation. This corre-sponds to an upper 10% or 5% classification error raterespectively.
In conclusion, serial measurements of left ven-tricular volumes, mass, shape and function by biplanetwo-dimensional echocardiography are accurate andfairly reproducible. The major component of variabilityis related to repeated echo examinations and not somuch to repeated measurements on a videotape from thesame echo recording, or to measurements made bydifferent investigators. The present study indicates thatboth methodological and biological factors are respon-sible for the variability of serial echo measurements, butthese are small. In assessing clinical limits for individualchanges in left ventricular volume and function andcalculating statistical power for detecting differences intwo patient groups followed over time, all three factors:repeated echo examinations, repeated video measure-ments of the same echo examination and differentinvestigators must be taken into account.
This work was supported by a grant from Bristol-Myers Squibb,Norway. The assistance and support of Bjorn Graving is highlyappreciated.
References
[1] St. John Sutton M. Pfeffer MA, Plappert T et al. Quantitativetwo-dimensional echocardiographic measurements are majorpredictors of adverse cardiovascular events after acutemyocardial infarction. The protective effect of captopril.Circulation 1994; 89: 68-75.
[2] Kingma JH, van Gilst WH, Peels CH et al. Acute interventionwith captopril during thrombolysis in patients with firstanterior myocardial infarction. Eur Heart J 1994; 15: 898-907.
Eur Heart J. Vol. 18. March 1997
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/18/3/507/498019 by guest on 27 D
ecember 2021
Biplane 2-D echocardiography of L V function 513
[3] Nicolosi GI, Ascione L, Badano E et al. Time course offunctional improvement of regional wall motion abnormalitiesafter transmural myocardial infarction. Influence of theextent of acute abnormal wall motion, and of early lisinopriland nitrate therapy. Preliminary data from the Gissi-3 echosubstudy. Eur Heart J 1995; 16 (Abstr Suppl): 342.
[4] The DEFIANT Research Group (Doppler Flow and Echocar-diography in Functional cardiac Insufficiency; assessment ofNisoldipine Therapy): Improved diastolic function with thecalcium antagonist nisoldipine (coat-core) in patients postmyocardial infarction: results of the DEFIANT study. EurHeart J 1992; 13 1496-1505.
[5] MacNeill AB, St. John Sutton M, Poole-Wilson PA, Lubsen J,on behalf of the DEFIANT-II Research Group. Doppler flow,Echocardiography and Functional Improvement: assessmentof nisoldepine Therapy (Defiant-II study). Objectives anddesign. Clin Trials and Meta-Analysis 1993; 28: 267-80.
[6] Michelsen S, Otterstad JE. Blood pressure response duringmaximal exercise in apparently healthy men and women.J Intern Med 1990; 227: 157-63.
[7] Schiller NB, Shah PM, Crawford M et al. Recommendationsfor quantitation of the left ventricle by two-dimensionalechocardiography. Am J Soc Echocard 1989; 2: 358-68.
[8] Reichek N, Helak J. Plappert T, St. John Sutton M, WeberKT. Anatomic validation of left ventricular mass estimatesfrom clinical two-dimensional echocardiography: initialresults. Circulation 1983; 67: 348-52.
[9] Senior R, Sridhara BS, Basu S et al. Comparison of radio-nuclide ventnculography and 2D echocardiography forthe measurement of left ventricular ejection fraction follow-ing acute myocardial infarction. Eur Heart J 1994; 15:1235-9.
[10] Gordon EP, Schnittger I, Fitzgerald PJ, Williams P, Popp RL.Reproducibility of left ventricular volumes by two-dimensional echocardiography. J Am Coll Cardiol 1983; 2:506-13.
[11] Sandier H, Dodge HT. The use of single plane angiocardio-grams for the calculation of left ventricular volume in man.Am Heart J 1968; 75: 325-34.
[12] Albin G, Rahko PS. Comparison of echocardiographic quan-titation of left ventricular ejection fraction to radionucleideangiography in patients with regional wall motion abnormali-ties. Am J Cardiol 1990; 65: 1031-2.
Eur Heart J. Vol. 18, March 1997
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/18/3/507/498019 by guest on 27 D
ecember 2021





























