Embed Size (px)
Citation preview

Pemicu 4 blok GIT
Victoria (405080027)

Acute abdomen

•Neonate •2 months-2 years •2-5 years •>5 year s
•Colic •Dietary protein allergy •Volvulus •Necrotizing enterocolitis •Testicular torsion •Adhesions
•Gastroenteritis •Viral illness •Trauma (including inflicted injury) Incarcerated hernia •Intussusception •Urinary tract infection •Foreign body ingestion •Sickle cell syndrome vasoocclusive crisis •Dietary protein allergy •Tumor
•Gastroenteritis •Viral illness •Trauma (including inflicted injury) •Appendicitis •Pharyngitis •Constipation •Urinary tract infection •Pneumonia •Intussusception •Foreign body ingestion
•Gastroenteritis •Viral illness •Appendicitis •Trauma •Constipation •Pharyngitis •Pneumonia •Urinary tract infection •Diabetic ketoacidosis •Sickle cell syndrome vasoocclusive crisis •Henoch Schönlein purpura
Red life threatening Black common

•Neonate •2 months-2 years •2-5 years •>5 year s
•Hirschsprung•disease •Adhesions •Hemolytic uremic syndrome •Toxin •Meckel's diverticulum •Hepatitis
•Sickle cell syndrome vasoocclusive crisis •Henoch Schönlein purpura •Ovarian torsion •Intraabdominal abscess •Tumor •Adhesions •Hemolytic uremic syndrome •Hepatitis •Meckel's diverticulum •Toxin •Primary bacterial peritonitis
•Ovarian torsion •Testicular torsion •Inflammatory bowel disease •Intraabdominal abscess •Ruptured ovarian cyst •Cholecystitis •Pancreatitis •Urolithiasis •Hepatitis •Meckel's diverticulum •Perforated ulcer •Adhesions •Hemolytic uremic syndrome •Myocarditis, pericarditis •Primary bacterial peritonitis

life-threatening causes• Trauma • Appendicitis • Intussusception• Malrotation with midgut volvulus • Incarcerated inguinal hernia • Adhesions • Necrotizing enterocolitis • Peptic ulcer disease • Ruptured ovarian cyst • Ectopic pregnancy • Pelvic inflammatory disease • Foreign body ingestion

Uncommon life-threatening causes
• Diabetic ketoacidosis (DKA) is a life-threatening condition that can be associated with abdominal pain and vomiting.
• Hirschsprung associated enterocolitis (HAEC) is an uncommon, fulminant complication of Hirschsprung disease. Children typically have explosive diarrhea, fever, and abdominal pain. HAEC can occur prior to surgical intervention, in the immediate postoperative period, or more than two years after definitive repair.

• Hemolytic uremic syndrome (HUS) typically develops after an infection with Shiga toxin-producing enterohemorrhagic E. coli (EHEC) or Shigella .HUS has also been associated with pneumococcal infection, HIV, and genetic factors. Clinical features of HUS include hemolytic anemia, thrombocytopenia, and acute renal injury.
• Primary bacterial peritonitis, usually caused by Streptococcus pneumoniae or E. coli, is a life-threatening infectious complication of nephrotic syndrome.
• Myocarditis may cause abdominal pain as the result of passive hepatic congestion from heart failure. Pericarditis may cause referred abdominal pain.

Common cause
• Constipation • Gastrointestinal infection • Other infections – Urinary tract infections – Streptococcal pharyngitis – Pneumonia – Viral illnesses – Colic

Major Causes of Intestinal Obstruction
• Mechanical Obstruction • Adhesions • Hernias, internal or external • Volvulus• Intussusception • Tumors Inflammatory strictures • Obstructive gallstones, fecaliths, foreign bodies • Congenital strictures; atresias • Congenital bands • Meconium in mucoviscoidosis • Imperforate anus • Pseudo-obstruction• Paralytic ileus (e.g., postoperative) • Vascular—bowel infarction • Myopathies and neuropathies (e.g., Hirschsprung)


Pathophysiology
• Visceral pain• Somatic pain• Referred pain• Peritonitis

Pathophysiology
• Visceral pain comes from the abdominal viscera, which are innervated by autonomic nerve fibers and respond mainly to the sensations of distention and muscular contraction—not to cutting, tearing, or local irritation. Visceral pain is typically vague, dull, and nauseating. It is poorly localized and tends to be referred to areas corresponding to the embryonic origin of the affected structure. Foregut structures (stomach, duodenum, liver, and pancreas) cause upper abdominal pain. Midgut structures (small bowel, proximal colon, and appendix) cause periumbilical pain. Hindgut structures (distal colon and GU tract) cause lower abdominal pain.

Pathophysiology
• Somatic pain comes from the parietal peritoneum, which is innervated by somatic nerves, which respond to irritation from infectious, chemical, or other inflammatory processes. Somatic pain is sharp and well localized.
• Referred pain is pain perceived distant from its source and results from convergence of nerve fibers at the spinal cord. Common examples of referred pain are scapular pain due to biliary colic, groin pain due to renal colic, and shoulder pain due to blood or infection irritating the diaphragm.

Pathophysiology• Peritonitis:
– Peritonitis is inflammation of the peritoneal cavity. – The most serious cause is perforation of the GI tract, which produces
immediate chemical inflammation followed shortly by infection from intestinal organisms. Peritonitis can also result from any abdominal condition that produces marked inflammation (eg, appendicitis, diverticulitis, strangulating intestinal obstruction, pancreatitis, pelvic inflammatory disease, mesenteric ischemia).
– Intraperitoneal blood from any source (eg, ruptured aneurysm, trauma, surgery, ectopic pregnancy) is irritating and results in peritonitis.
– Barium causes severe peritonitis and should never be given to a patient with suspected GI tract perforation.

Pathophysiology• Peritonitis:
– Peritoneo-systemic shunts, drains, and dialysis catheters in the peritoneal cavity predispose a patient to infectious peritonitis, as does ascitic fluid.
– Rarely, spontaneous bacterial peritonitis occurs, in which the peritoneal cavity is infected by blood-borne bacteria.
– Peritonitis causes fluid shift into the peritoneal cavity and bowel, leading to severe dehydration and electrolyte disturbances.
– Adult respiratory distress syndrome can develop rapidly. – Kidney failure, liver failure, and disseminated intravascular coagulation
follow. – The patient's face becomes drawn into the masklike appearance
typical of hippocratic facies. – Death occurs within days.





History in Patients with Acute Abdominal Pain
Question Potential Responses and Indications
Where is the pain? See Fig. 1: Acute Abdomen and Surgical Gastroenterology: Location of abdominal pain and possible causes. What is the pain like? Acute waves of sharp constricting pain that “take the breath away” (renal or biliary colic)Waves of dull pain with vomiting (intestinal obstruction)Colicky pain that becomes steady (appendicitis, strangulating intestinal obstruction, mesenteric ischemia)Sharp, constant pain, worsened by movement (peritonitis)Tearing pain (dissecting aneurysm)Dull ache (appendicitis, diverticulitis, pyelonephritis)

Have you had it before? Yes suggests recurrent problems such as ulcer disease, gallstone colic, diverticulitis, or mittelschmerz
Was the onset sudden? Sudden: “like a light switching on” (perforated ulcer, renal stone, ruptured ectopic pregnancy, torsion of ovary or testis, some ruptured aneurysms)Less sudden: most other causes
How severe is the pain? Severe pain (perforated viscus, kidney stone, peritonitis, pancreatitis)Pain out of proportion to physical findings (mesenteric ischemia)
Does the pain travel to any other part of the body?
Right scapula (gallbladder pain)Left shoulder region (ruptured spleen, pancreatitis)Pubis or vagina (renal pain)Back (ruptured aortic aneurysm)
What relieves the pain? Antacids (peptic ulcer disease)Lying as quietly as possible (peritonitis)

What other symptoms occur with the pain?
Vomiting precedes pain and is followed by diarrhea (gastroenteritis)Delayed vomiting, absent bowel movement and flatus (acute intestinal obstruction; the delay increases with a lower site of obstruction)Severe vomiting precedes intense epigastric, left chest, or shoulder pain (emetic perforation of the intra-abdominal esophagus)
Red Flags
• Severe pain• Signs of shock (eg, tachycardia, hypotension,
diaphoresis, confusion)• Signs of peritonitis• Abdominal distention

Interpretation
• Distention, especially when surgical scars, tympany to percussion, and high-pitched peristalsis or borborygmi in rushes are present, strongly suggests bowel obstruction.
• Severe pain in a patient with a silent abdomen who is lying as still as possible suggests peritonitis; location of tenderness suggests etiology (eg, right upper quadrant suggests cholecystitis, right lower quadrant suggests appendicitis) but may not be diagnostic

• Back pain with shock suggests ruptured abdominal aortic aneurysm (AAA), particularly if there is a tender, pulsatile mass.
• Mild to moderate pain in the presence of active peristalsis of normal pitch suggests a nonsurgical disease (eg, gastroenteritis) but may also be the early manifestations of a more serious disorder

Testing: Tests are selected based on clinical suspicion.
• Urine pregnancy test for all women of childbearing age
• Selected imaging tests based on suspected diagnosi

Ileus
hypomotility of the gastrointestinal tract in the absence of mechanical
bowel obstruction
Epidemiology
• 20% of admissions due to acute abdominal pain are due to intestinal obstruction. Of these, approximately 80% have small intestinal obstruction
• 16% of colorectal malignancies present with obstruction

Etiology • Sepsis• Drugs (eg, opioids, antacids, warfarin, amitriptyline,
chlorpromazine)• Metabolic (eg, low potassium, magnesium, or sodium levels;
anemia; hyposmolality)• Myocardial infarction• Pneumonia• Trauma (eg, fractured ribs, fractured spine)• Biliary colic and renal colic• Head injury and neurosurgical procedures• Intra-abdominal inflammation and peritonitis • Retroperitoneal hematomas

Macam ileus Nyeri Usus Distensi Muntah borborigmi
Bising usus Ketegangan abdomen
Obstruksi simple tinggi
++ (kolik)
+ +++ Meningkat -
Obstruksi simple rendah
+++ (Kolik)
+++ + Lambat, fekal
Meningkat -
Obstruksi strangulasi
++++ (terus-
menerus, terlokalisir)
++ +++ Tak tentu biasanya
meningkat
+
Paralitik + ++++ + Menurun -
Oklusi vaskuler +++++ +++ +++ Menurun +

Paralytic (adynamic)
ileus • is due to functional failure
of normal intestinal peristalsis
• It commonly occurs post-operatively following abdominal surgery
• It may also occur in patients with acute pancreatitis, ischaemic gastrointestinal disease, choledocholithiasis, peritonitis and external trauma, or may be induced by ganglion-blocking antihypertensive drugs
• Numerous air-fluid level
Mechanical ileus
• Is mechanical or organic obstruction of the small intestine or colon and maybe complete or partial (subacute obstruction)
• It’s commonly caused by fibrous bands and adhesion, hernias, malignant disease, impacted faeces or inflammatory bowel disease
• In the short duration of obstruction some gas may be seen in loops of intestine distal to the site
• In the long duration of obstruction no gas in the distal obstruction
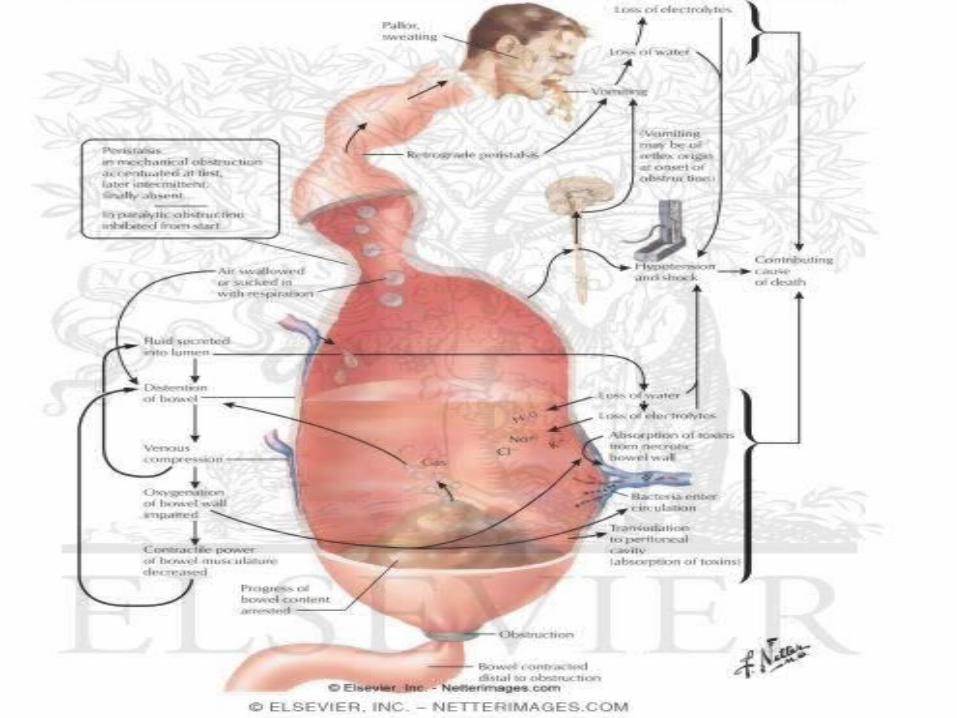

• Distention of the intestine is caused by the accumulation of gas and fluid proximal to and within the obstructed segment. Between 70 and 80% of intestinal gas consists of swallowed air, and because this is composed mainly of nitrogen, which is poorly absorbed from the intestinal lumen, removal of air by continuous gastric suction is a useful adjunct in the treatment of intestinal distention. The accumulation of fluid proximal to the obstructing mechanism results not only from ingested fluid, swallowed saliva, gastric juice, and biliary and pancreatic secretions but also from interference with normal sodium and water transport. During the first 12–24 h of obstruction, a marked depression of flux from lumen to blood occurs of sodium and consequently water in the distended proximal intestine. After 24 h, sodium and water move into the lumen, contributing further to the distention and fluid losses. Intraluminal pressure rises from a normal of 2–4 cmH2O to 8–10 cmH2O. The loss of fluids and electrolytes may be extreme, and unless replacement is prompt, hypovolemia, renal insufficiency, and shock may result. Vomiting, accumulation of fluids within the lumen, and the sequestration of fluid into the edematous intestinal wall and peritoneal cavity as a result of impairment of venous return from the intestine all contribute to massive loss of fluid and electrolytes.

• The most feared complication of acute intestinal obstruction is the presence of a "closed loop." Closed-loop obstruction of the small intestine results when the lumen is occluded at two points by a single mechanism such as a fascial hernia or adhesive band, thus producing a closed loop whose blood supply is often occluded by the hernia or band as well. During peristalsis, when a "closed loop" is present, pressures reach 30–60 cmH2O. Strangulation of the closed loop is common in association with marked distention proximal to the involved loop. A form of closed-loop obstruction is encountered when complete obstruction of the colon exists in the presence of a competent ileocecal valve (85% of individuals). Although the blood supply of the colon is not entrapped within the obstructing mechanism, distention of the cecum is extreme because of its greater diameter (Laplace's law), and impairment of the intramural blood supply is considerable, with consequent gangrene of the cecal wall. Once impairment of blood supply to the gastrointestinal tract occurs, bacterial invasion supervenes, and peritonitis develops. The systemic effects of extreme distention include elevation of the diaphragm with restricted ventilation and subsequent atelectasis. Venous return via the inferior vena cava may also be impaired.



Sign & symptomps
• In adynamic ileus as well as colonic pseudo-obstruction,
• colicky pain is absent and only discomfort from distention is evident.
• Vomiting may be frequent but is rarely profuse.
• Complete obstipation may or may not occur. • Singultus (hiccups) is common

History• Diffuse, central abdominal pain of a colicky nature. Pain is less or absent in
paralytic ileus but there may be a history to suggest causes.• Vomiting tends to be early in high level obstruction. Faeculent vomiting is
extremely unpleasant and is limited to low obstruction• Abdominal distension: the lower the level of obstruction• Absolute constipation is early in low obstruction and late in high-level
obstruction. In paralytic ileus there is no bowel movement and no flatus.• In sigmoid volvulus the picture is rather like large bowel obstruction with
pain, constipation, late vomiting and a very marked degree of abdominal distension. Half of such patients will have had a previous episode.
• Severe pain and tenderness suggests ischaemia or perforation.
Presentation

Examination
• Look for signs of dehydration such as poor peripheral perfusion, tachycardia and hypotension.
• Abdominal distension will be apparent. Massive peristalsis may even by visible.
• Distended bowel is very resonant on percussion• If strangulation or perforation occurs there will be features of
an acute abdomen with peritonism.• Check hernial orifices• Bowel sounds
– In obstruction very active and tinkling – In ileus silent or nearly so
• The patient may be generally toxic and unwell because ischaemia of the bowel allows bacteria and toxins to enter the circulation.

Workup
• Fluid charts – are required to monitor intake and output, especially as an intravenous
infusion is almost certainly required, a nasogastric tube may be passed and oliguria is an important sign of early dehydration
• Plain abdominal X-ray – Sensitivity is 50-66%– Films are taken supine and erect– Obstruction of the small bowel shows ladder-like series of small bowel
loops but this also occurs with an obstruction of the proximal colon– Fluid levels will also be seen in paralytic ileus and the small bowel is
distended throughout its length– Multiple fluid levels and distension of the bowel is abnormal– Gas under the diaphragm suggests perforation.

• Blood should be taken for full blood count, urea, electrolytes and creatinine. Glucose may be slightly elevated by stress but very high levels are a cause for concern.
• Water-soluble contrast may also be helpful in small bowel obstruction due to adhesions.
• CT scanning – To predict the need for surgery in small bowel obstruction– Patients with peritoneal fluid evident on CT scan are three times more likely to
require surgical intervention than those who do not have this sign– Partial obstruction may not be detected on CT and suspicion should remain
high if the clinical picture suggests obstruction despite a normal scan
• MRI and ultrasound have been found useful in the diagnosis of small bowel obstruction

Laboratory and X-Ray Findings• Leukocytosis, with shift to the left, usually occurs when strangulation is
present, but a normal white blood cell count does not exclude strangulation.
• Elevation of the serum amylase level is encountered occasionally in all forms of intestinal obstruction. R
• oentgenographic images demonstrating distention of fluid- and gas-filled loops of small intestine usually arranged in a "stepladder" pattern with air-fluid levels and an absence or paucity of colonic gas are pathognomonic for small-bowel obstruction.
• Complete obstruction is suggested when passage of gas or stool per rectum has ceased and when gas is absent in the distal intestine by x-ray.
• A general haze due to peritoneal fluid and sometimes a "coffee bean"–shaped mass are seen in strangulating closed loop obstruction.

• A thin barium upper gastrointestinal series may help to differentiate partial from complete obstruction.
• However, thick barium given by mouth should be avoided when the obstruction is considered to be high grade or complete since retained barium sulfate may become inspissated.
• CT is the most commonly used modality to evaluate postoperative patients for intestinal obstruction because of its ability in differentiating adynamic ileus, partial obstruction, and complete obstruction (Fig. 293-1).
• However, the sensitivity and specificity of CT for strangulating obstruction are low (50 and 80%, respectively

Treatment • NGT• IV fluids
• Treatment involves continuous nasogastric suction, npo status, IV fluids and electrolytes, a minimal amount of sedatives, and avoidance of opioids and anticholinergic drugs. Maintaining an adequate serum K level (> 4 mEq/L [> 4 mmol/L]) is especially important. Ileus persisting > 1 wk probably has a mechanical obstructive cause, and laparotomy should be considered. Sometimes colonic ileus can be relieved by colonoscopic decompression; rarely, cecostomy is required. Colonoscopic decompression is helpful in treating pseudo-obstruction (Ogilvie's syndrome), which consists of apparent obstruction at the splenic flexure, although no cause can be found by contrast enema or colonoscopy for the failure of gas and feces to pass this poin

Treatment• Paralytic ileus
– Is usually self-limiting and is initially treated conservatively– Recovery may be expedited with intravenous fluid replacement and gastric aspiration
• Mechanical ileus– Is treated similarly but surgery should be carried out as soon as the patient’s condition
allows• Strangulation or infarction surgery• Peritonitis antibacterial drugs • Nasogastric decompression abdominal distention associated with pain or to relieve
recurrent vomiting• Ileus after abdominal surgical procedures usually results in return of normal intestinal
motility within 24-72 hr. • Prokinetic agents may stimulate the return of normal bowel motility and be of assistance
to children with prolonged ileus. – metoclopramide – erythromycin

DD Ileus


Ileus Pseudo-obstruction Mechanical Obstruction (Simple)
Symptoms Mild abdominal pain, bloating, nausea, vomiting, obstipation, constipation
Crampy abdominal pain, constipation, obstipation, nausea, vomiting, anorexia
Crampy abdominal pain, constipation, obstipation, nausea, vomiting, anorexia
Physical Examination Findings
Silent abdomen, distention, tympanic
Borborygmi, tympanic, peristaltic waves, hypoactive or hyperactive bowel sounds, distention, localized tenderness
Borborygmi, peristaltic waves, high-pitched bowel sounds, rushes, distention, localized tenderness
Plain Radiographs Large and small bowel dilatation, diaphragm elevated
Isolated large bowel dilatation, diaphragm elevated
Bow-shaped loops in ladder pattern, paucity of colonic gas distal to lesion, diaphragm mildly elevated, air-fluid levels

Differential diagnosis
• Ischaemia of the gut• Acute pancreatitis• Perforation of the gut• Intussusception• Tuberculosis• Non-gastrointestinal conditions

Complication
• Strangulation or infarction• Leading to gangrene• Perforation• peritonitis

Prognosis
• In patients with small bowel obstruction, the mortality is 25% if surgery is delayed beyond 36 hours; under 36 hours this drops to 8%
• 50% of sigmoid volvulus will recur in the next 2 years• 60% of stomas are never reversed• Older patients, patients with hypoalbuminaemia and those in
whom the primary tumour is not gastrointestinal in origin are less able to withstand the rigours of major surgery

Mechanical intestinal obstruction• is characterized by cramping midabdominal pain, which tends to be more severe the
higher the obstruction. The pain occurs in paroxysms, and the patient is relatively comfortable in the intervals between the pains. Audible borborygmi are often noted by the patient simultaneously with the paroxysms of pain. The pain may become less severe as distention progresses, probably because motility is impaired in the edematous intestine. When strangulation is present, the pain is usually more localized and may be steady and severe without a colicky component, a fact that often causes delay in diagnosis of obstruction. Vomiting is almost invariable, and it is earlier and more profuse the higher the obstruction. The vomitus initially contains bile and mucus and remains as such if the obstruction is high in the intestine. With low ileal obstruction, the vomitus becomes feculent, i.e., orange-brown in color with a foul odor, which results from the overgrowth of bacteria proximal to the obstruction. Hiccups (singultus) are common. Obstipation and failure to pass gas by rectum are invariably present when the obstruction is complete, although some stool and gas may be passed spontaneously or after an enema shortly after onset of the complete obstruction. Diarrhea is occasionally observed in partial obstruction. Blood in the stool is rare but does occur in cases of intussusception.