Embed Size (px)
Citation preview

Victor Bowers , M.D, FACS
Current Issues And Future Directions In Renal Transplantation

DisclosuresI HAVE NO FINANCIAL
RELATIONSHIP(S) RELEVANT TO THE CONTENT OF THIS
CME ACTIVITY.

Disclosures
I WILL NOT DISCUSS OFF-LABEL USE OF MEDICATIONS.

Renal Transplantation
• True or False-The Number of kidney transplants performed in 2013 was greater than
the entire kidney transplant waiting list in June of 1989.

UNOS Patient Waiting ListThe UNOS national patient waiting list for organ transplant contains
more than 17,000 names.*
ORGAN NUMBER
Kidney 15,045
Kidney/Pancreas 267
Heart 1,216
Liver 763
TOTAL 17,291
UNOS 6/1989

Recent Facts
2003 2008 2010 2013
Deceased Donors
5,752 7,188 7,241 7,547
Deceased Donor Transplant
8,668 10,553 10,622 11,163
Living Donors
6,470* 5,968 6,278 5,732
Total Renal Transplants
15,138 16,521 16,900 16,895

Chronic Kidney Disease
Any Condition That Causes Reduced Kidney Function, GFR Less 60 Ml/Min For More Than 3 Months or When a
Patients Urine Albumin-to- Creatinine Ratio Over 30mg of Albumin to Each
Gram of Creatinine.
One In 10 American Adults Have a Diagnosis of CKD.
(CKD)

Chronic Kidney Disease
Stages 1- GFR > 90 Ml/Min (per 1.73m2) 2- GFR 60-89 Ml/Min (per 1.73m2) 3a-GFR 45-59 Ml/Min 3b-GFR 30-44 Ml/Min 4- GFR 15-29 Ml/Min 5- GFR <15Ml/Min or Treatment on
Dialysis

Adjusted Incident Rates Of ESRD & Annual Change

USRD 2013

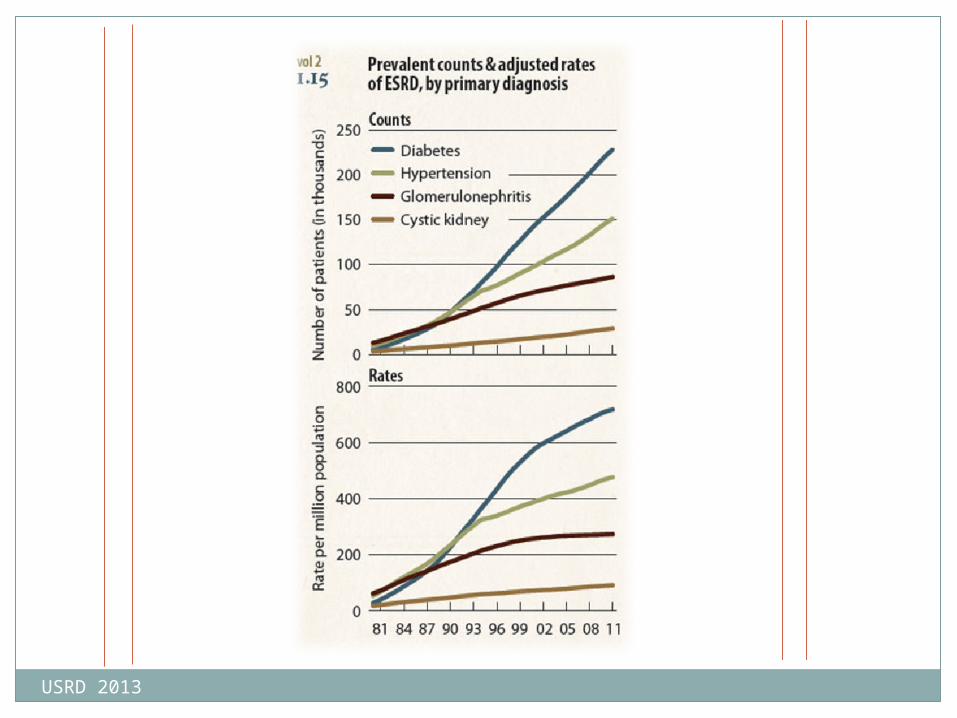
Adjusted Prevalent Rates of ESRD & Annual Percent Change
USRD 2013
USRD 2013

USRD 2013

Incident & prevalent patient counts (USRDS), by modality
USRDS 2013
Figure 1.1 (Volume 2)

Renal Transplant OutcomesProbability of Graft Survival
Adult
1 Year 3 Year
TGH 94.9 90.3
Nat’l Expected 94.9 87.1
SRTR 03/20/2014
Deceased t ½ 9.5 yearsLiving t ½ 12.4 years

Adjusted all-cause mortality in the ESRD & general populations, by age, 2011
USRDS 2013
Figure 5.2 (Volume 2)

(PER 1 ,000 PATIENT YEARS AT RISK)
Adjusted All- Cause Mortality in the ESRD & General
Populations,2011
USRD 2013

Total Medicare Expenditures per person/year
Hemodialysis $87,945
Peritoneal Dialysis $71,630
Transplant $32,922

Wait Listed Patients Receiving a Deceased Donor Transplant in 3 years - Listing (2010)
Blood Type %TGH
%Nat’l
“O” 43 21.1
“A” 57.7 33.0
“B” 56.9 20.8
“AB” 65.8 45.8
USRDS 2013


Kidney Transplant:Supply and Demand
Kidney Transplant is Routinely successfulCost EfficientImproves Patient Survival and Quality of LifeLimited Only by donor Availability

Medicare Act Signed into Law July 30, 1965

ESRD Act Signed into Law 1972

10 ,000 NEW PATIENTS PER YEARTOTAL BENEFICIARIES WILL LEVEL AT 35 ,000
Estimated ESRD Program(Klar 1972)
Reality
1978- 14,000
1986- 32,000
1998- 75,000
2011- 115,643

US Healthcare Cost $• 2.8 Trillion Dollars
• 18% GDP (15.1 Trillion)
• Projected to 21% by 2020
• Distinct Threat to our Government’s Fiscal Stability



Institute of Medicine Report
September 6th, 2012
“It’s A Mess”
US Healthcare

30 % Healthcare Spending is WASTED (750 Billion)
Unnecessary Services Defensive Medicine/ Futile Care
Excess Administrative Costs
Fraud
Contractual Value Clinical
Medical Devices
US Healthcare

Single Largest Payer-Medicare Uncapped Entitlement
Fee for Service
Accelerate Use of Alternatives to Fee for Service Comprehensive “Fee for Event”
“Bundled Payments”
Payment/ Health Reform

Transplant Centers
Multidisciplinary Approach• All Facets of Care-“Under One Roof”• Identify Processes for Improving Communication• Protocols for All Areas of Care Including
Community Physicians• Dedicated Specialists • Physician Extenders
Survival Guide

David and Goliath

Waitlist vs. TransplantedNational
2014 2013 2003 1989
Waitlist 108,314 103,131 59,080 15,045
Transplanted
2,676* 16,894 15,138 8,656
*As of May 30, 2014 OPTN

Kidney
Donor
Profile
Index
KDPI
Score is Associated with How Long Kidney is Likely to Function Compared to Other KidneysRange 0 to 100

KDPI ScoreAgeHeightWeightEthnicityDid Donor Die Due To
Loss of Heart or Brain Function
CVA Cause of DeathHistory of
HypertensionHistory of DiabetesPositive Serology for
Hepatitis CSerum Creatinine

KDPI: Kidney Donor Profile Index

Estimated Graft Half Lives (Years)

Score of 20 Means That The Kidney is
Likely to Function Longer Than 80%
of
“Available Kidneys”
Score of 60 Means That This Kidney is
Likely to Function Longer Than 40%
of “Available Kidneys”

Estimated
Post
Transplant
Survival
EPTS
Each Kidney Transplant Candidate Will Get An Individual ScoreRange 0 to 100

EPTS Score
Calculated on 4 Variables Age Length of Time On Dialysis Having a Previous Transplant
(Of any Organ) Current Diagnosis of Diabetes

EPTS of 20% Indicates That You Will Need a
Kidney Longer Than 80% of the Other
Candidates
EPTS of 55 Means That One Will Need A
Kidney Longer Than 45% of Other
Candidates

KDPI/EPTSAllocation
KDPI- Score Of 20 or Less Will First Be Off ered to Patients Likely to Need A Transplant The
Longest-Those With An EPTS Score of 20 or Less.
If Not Accepted by One of These Individuals, It ’s Off ered to Any Other Person Who Would Match on
the Transplant List.

KDPI/EPTSAllocation
Children & Teenagers(Age <18) Will Receive Priority for Kidneys With a KDPI Score of 35% or Lower
Blood Group A2 B
Highly Sensitized Candidates Also get Priority (> 98% PRA)

Current Renal Allocation
Deceased Donor 21 year old male MVA passenger Multi-organ Donor
Recipient Profile No pediatric compatible recipients 72 year old male Dialysis 2 years Type II DM, HTN

PROPOSEDEPTS CALCULATION
45 years old 2 years dialysis No diabetes No previous
transplants
EPTS Score 16%
70 years old Pre-emptive No diabetes No previous
transplants
EPTS Score 55%

Proposed EPTS Calculation
65 years oldDialysis 5 yearsType II diabetes1 previous transplant
EPTS Score 97%
30 years oldPre-emptiveNo history of diabetesNo previous
transplants
EPTS Score 2%*

TRIVIA
Which event(s) took place in 1996?a) Derek Jeter named rookie of the yearb) Winter Olympics held in Lillehammer, Norwayc) “dolly” the sheep clonedd) Monica Lewinsky signs affidavit denying affair with
President Clintone) First crew arrives at the International Space
Station

We can’t solve problems by using the same kind
of thinking we used when we created them.Albert Einstein
Quote…


THE PAST 30 YEARS HAS SEEN THE EMERGENCE OF AN ENDEAVOR CALLED REGENERATIVE MEDICINE AND TISSUE
ENGINEERING. SCIENTISTS, ENGINEERS, AND PHYSICIANS APPLY BIOLOGICAL SUBSTITUTES
THAT CAN REPLACE OR HELP REGENERATE DISEASED OR INJURED TISSUES.
Regenerative Medicine/Tissue Engineering

REGENERATIVE MEDICINE IS OFTEN USED SYNONYMOUSLY WITH TISSUE ENGINEERING,
ALTHOUGH THOSE INVOLVED IN REGENERATIVE MEDICINE PLACE MORE
EMPHASIS ON THE USE OF STEM CELLS TO PRODUCE REPAIR TISSUE.
Regenerative Medicine

Regenerative
Medicine

TISSUE ENGINEERING IS THE USE OF A COMBINATION OF CELLS, ENGINEERING AND
MATERIAL METHODS, AND SUITABLE BIOCHEMICAL AND PHYSIO-CHEMICAL
FACTORS TO IMPROVE OR REPLACE BIOLOGICAL FUNCTIONS.
Tissue Engineering

Mammalian Development
ZygoteBlastomere (32-64 cell stage)MorulaBlastocyst
TrophoblastInner Cell Mass (Gastrula)

GASTRULA“GERM LAYERS”
3 Layers are responsible for all tissue within the human body.EndodermMesodermEctoderm

CAPABLE OF SELF-RENEWAL ABILITY OF CELLS TO PROLIFERATE WITHOUT LOSS OF DIFFERENTIATION WITHOUT
UNDERGOING SENESCENCE
CAPABILITY TO DIFFERENTIATE SYMMETRICAL OR ASYMMETRICAL (SELF GENERATION) OR
(DIFFERENTIATED CELL TYPES)
Stem Cells

Stem Cells
Pluripotent Cells – can make all cells of the embryo (can make any cell type of the body)
Multipotent Cells - Can only make cells from within a given germ layer.
Unipotent Cells – Can make cells of a single cell type within a specific germ layer

Stem Cells
Pluripotent cells were thought to be limited to cells derived from the inner cell mass of the blastocyst (7-10 days)
Cells cultured and cell lines established from these structures are called embryonic stem cells (ES)

Induced Pluripotent Stem Cells(iPSCs)
2006 Yamanaka Took genes of pluripotent ES cells and
introduced them into “mature cells”. A small number of mature cells reverted
back to a highly immature cell state that resembled an ES cell “reprogramming”.
Induced a pluripotent state in a previously differentiated cell type. (“Re-Programmed”)
“Unprecedented Opportunities”

CAN BE DIFFERENTIATED INTO MANY TISSUES
Hematopoietic precursorsOsteoclassPancreatic B-CellsCardiomyocytesHepatocytes and Biliary Epithelium
Human iPSCs

TWO METHODS OF “BUILDING”ORGANS/TISSUES
Utilization Tissue Scaffolds High porosity, pore size to facilitate
seeing/nutrition/waste removal “ghost organs”
Bioprinting Computer program is created, rather than
ink, cells are utilized

TISSUE INTEGRATION:
How effectively will these cells integrate into surrounding tissue and achieve physiologic function
ONCOGENESIS:
Pluripotent cells in vivo may form teratomas (neoplastic tumors with all three germ lines)
DIRECTED DIFFERENTIATION
Challenges in Clinical Use of Stem Cells


BIO PRINTER

Ghost Organ

Thank you!






























