Embed Size (px)
Citation preview
Vestibular Rehabilitation: Examination and Treatment in the Acute Setting
10/2021
Chara Booker, PT, DPT, NCSJulie Miller, PT, DPT, NCS, CBISNitin Saini, PT, DPTMichael Tran, PT, DPT

Course Objectives1. The course participants will understand anatomy and physiology
principles that are important for rehabilitation of
the vestibular system, including anatomy of the labyrinth and
otoliths, the triplanar model of the SSC and coplanar pairing.
2. The course participants will recognize the typical presentation of
acute vestibular syndrome (AVS) including BPPV and vestibular
hypofunction.
Course Objectives3. The course participants will identify the components of a bedside
vestibular examination performed in the Acute setting.
4. The course participants will select appropriate, evidence-based
vestibular physical therapy treatments for their patients based on
findings from examination.

Course Objectives5. The course participants will write appropriate “SMART” goals for
patients with acute vestibular syndrome with appropriate
timeframes for the acute setting with focus on appropriate
Referral/Disposition to next level of care and using DME, PRN.
6. The course participants will understand specific challenges to
vestibular treatments in the acute setting, including pharmacology,
polytrauma, and environmental considerations, and develop ways
to overcome them to deliver effective care for their patients.
Course Objectives7. The course participants will understand how to sequence and
incorporate vestibular examination and treatments in the context
of a medically-complex patient (with potentially peripheral
involvement from BPPV, UVH and central involvement concurrently
present) and will move to evaluation considering any needed
additional discharge planning and referral needs.
Inspiration for this Course
• Idea began when PT was covering weekend for Inpatient Rehab Unit
• Met a man who had fallen, developed a SDH and had been in hospital for 10 days with dizziness
• He had bilateral BPPV, PT treated him with bilat Epley CRM, he was discharged 2 days later with disposition to have further treatment in Outpatient department.
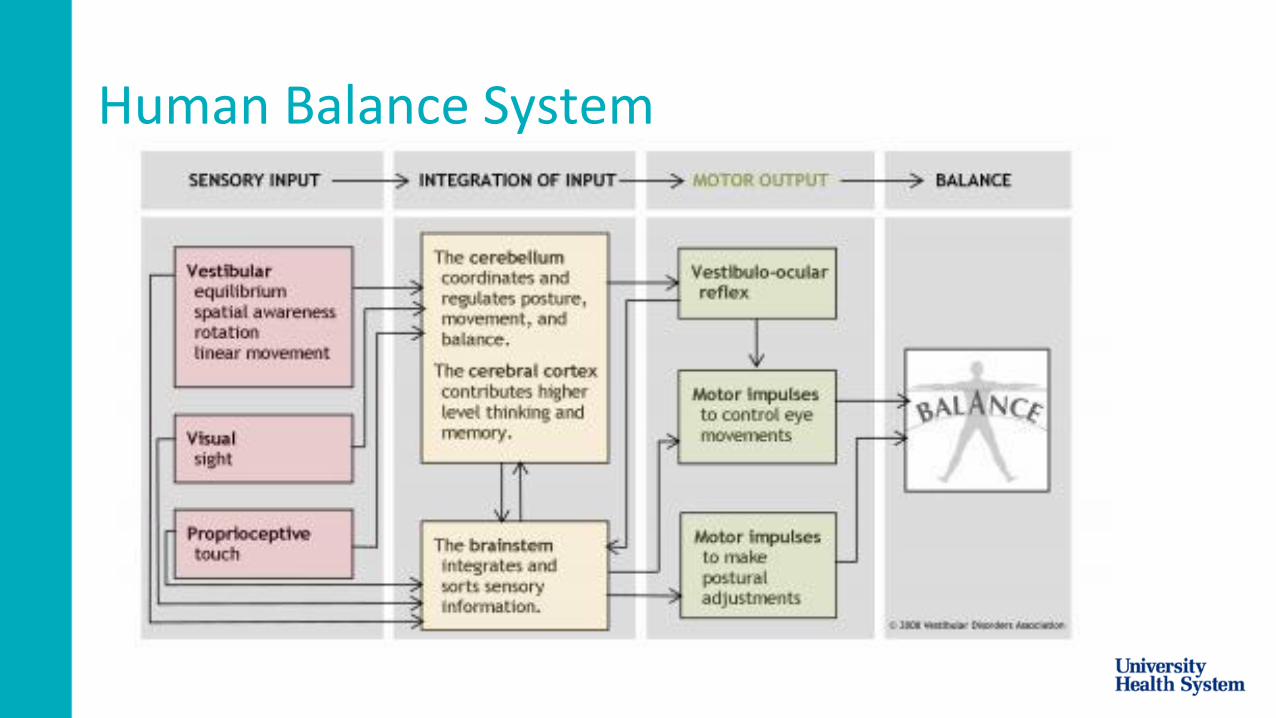
Human Balance System
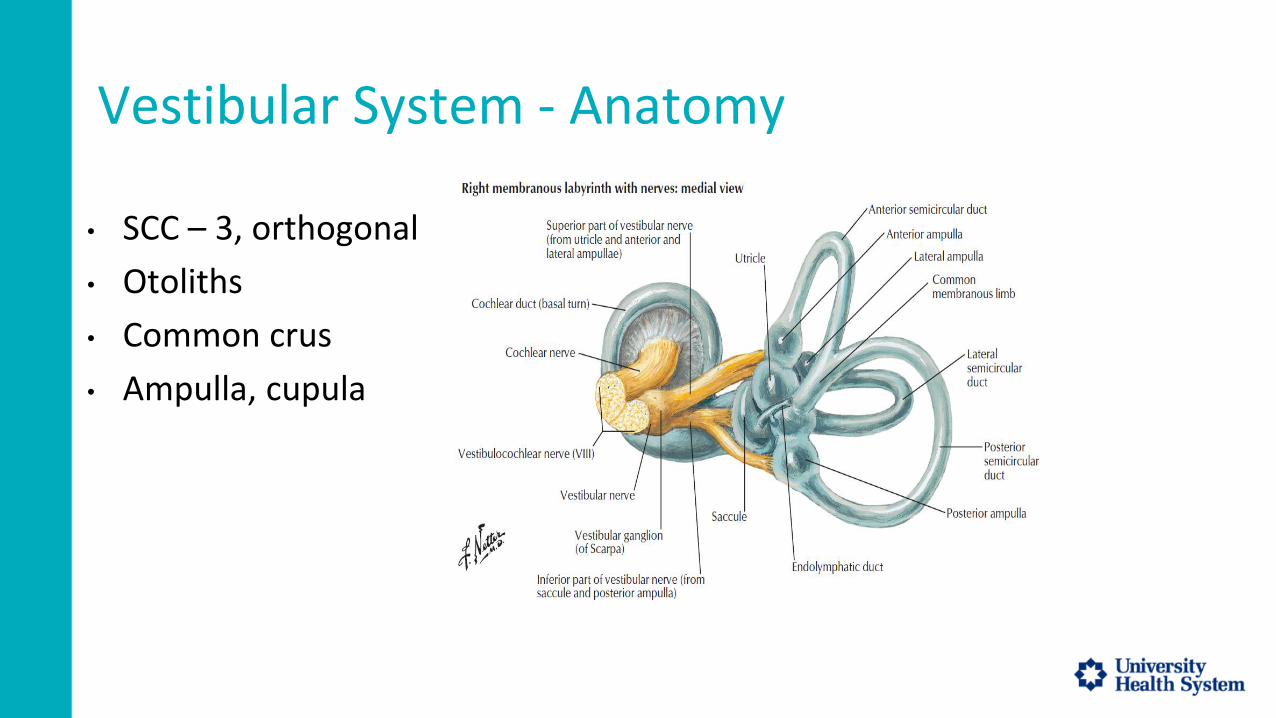
Vestibular System - Anatomy
• SCC – 3, orthogonal
• Otoliths
• Common crus
• Ampulla, cupula
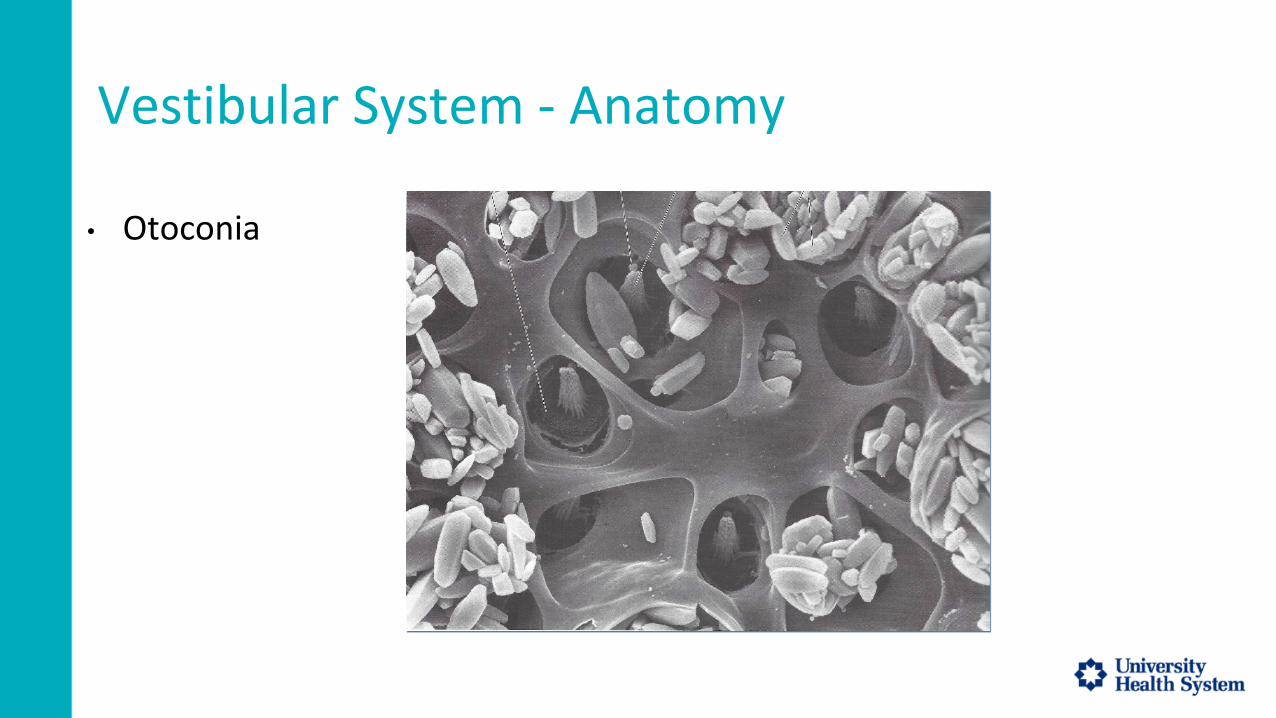
Vestibular System - Anatomy
• Otoconia
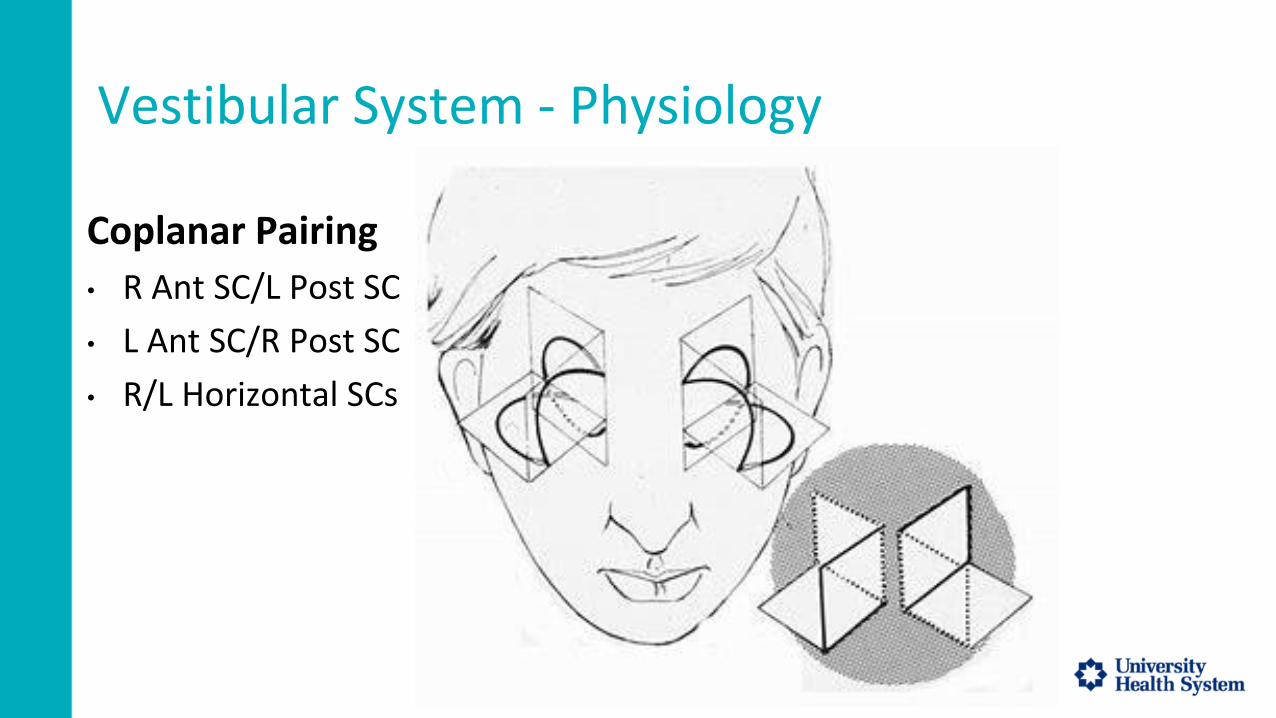
Vestibular System - Physiology
Coplanar Pairing
• R Ant SC/L Post SC
• L Ant SC/R Post SC
• R/L Horizontal SCs
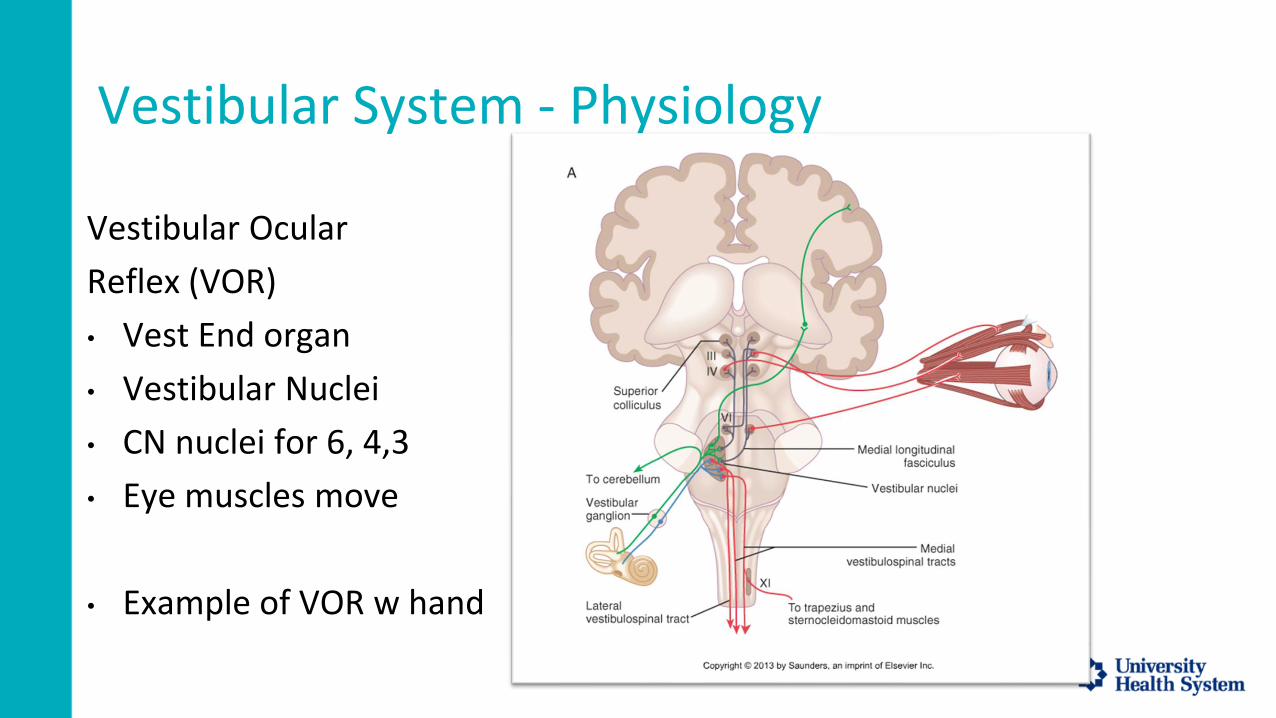
Vestibular System - Physiology
Vestibular Ocular
Reflex (VOR)
• Vest End organ
• Vestibular Nuclei
• CN nuclei for 6, 4,3
• Eye muscles move
• Example of VOR w hand

Pathology - BPPV
2 Types of BPPV:
• Canalithiasis
• Cupulolithiasis

Pathology - BPPV
Canalithiasis
BPPV
BPPV accounted for 8% of individuals with moderate or severe dizziness/vertigo. The lifetime prevalence of BPPV was 2.4%, the 1 year prevalence was 1.6%Von Brevern et. Al, J Neurol Neurosurg Psychiatry. 2007 Jul; 78(7): 710–715.
Link to article: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2117684/
Types of BPPV
Of 122 patients, 110 had posterior canal involvement, 10 had horizontal canal involvement, and only 2 had the anterior canal variant.
(90% PC, 8% HC, 2% AC), Korres et. al, Otol Neurotol. 2002 Nov;23(6):926-32.
The incidence of posterior semicircular canal (PC) involvement is between 85% and 95% and lateral semicircular canal (LC) involvement is 5% to 15% of BPPV cases.1 The incidence of anterior semicircular canal (AC) involvement is low (3%). Galgon, A.K. et al. Agreement Between Physical Therapists in Diagnosing Benign Paroxysmal Positional Vertigo. JNPT. 2021; 45: 79-86.
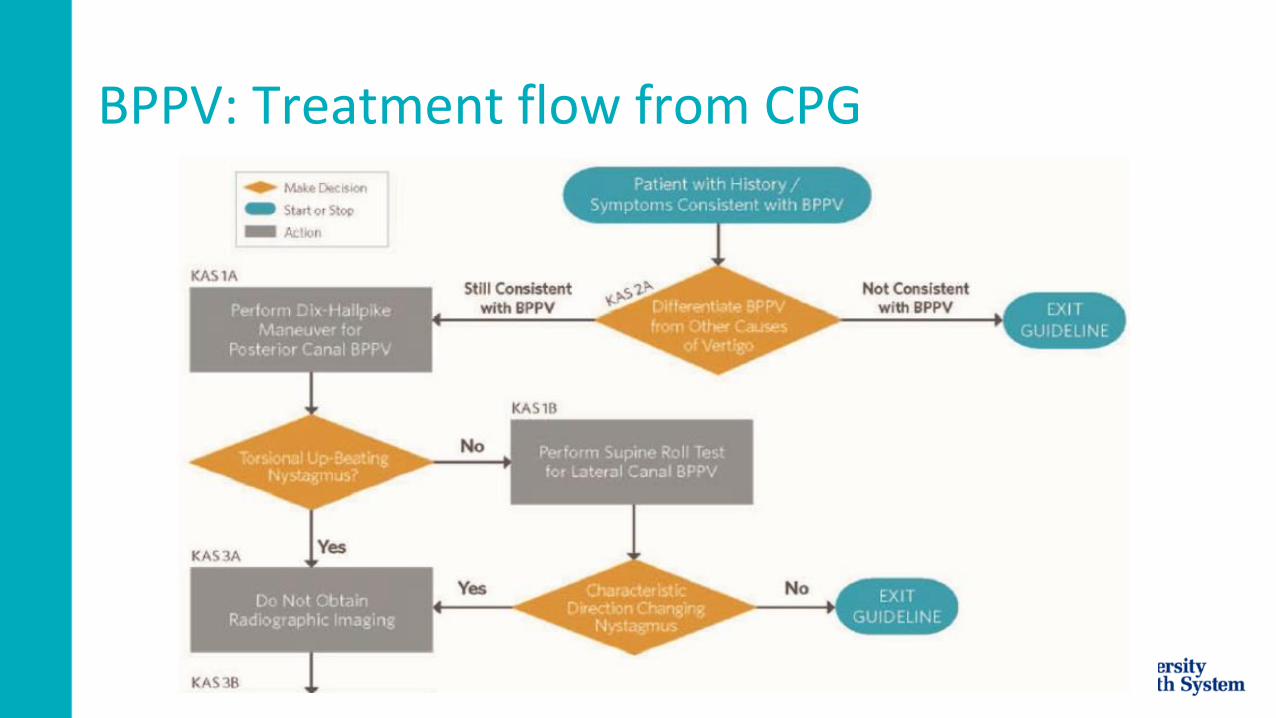
BPPV: Treatment flow from CPG
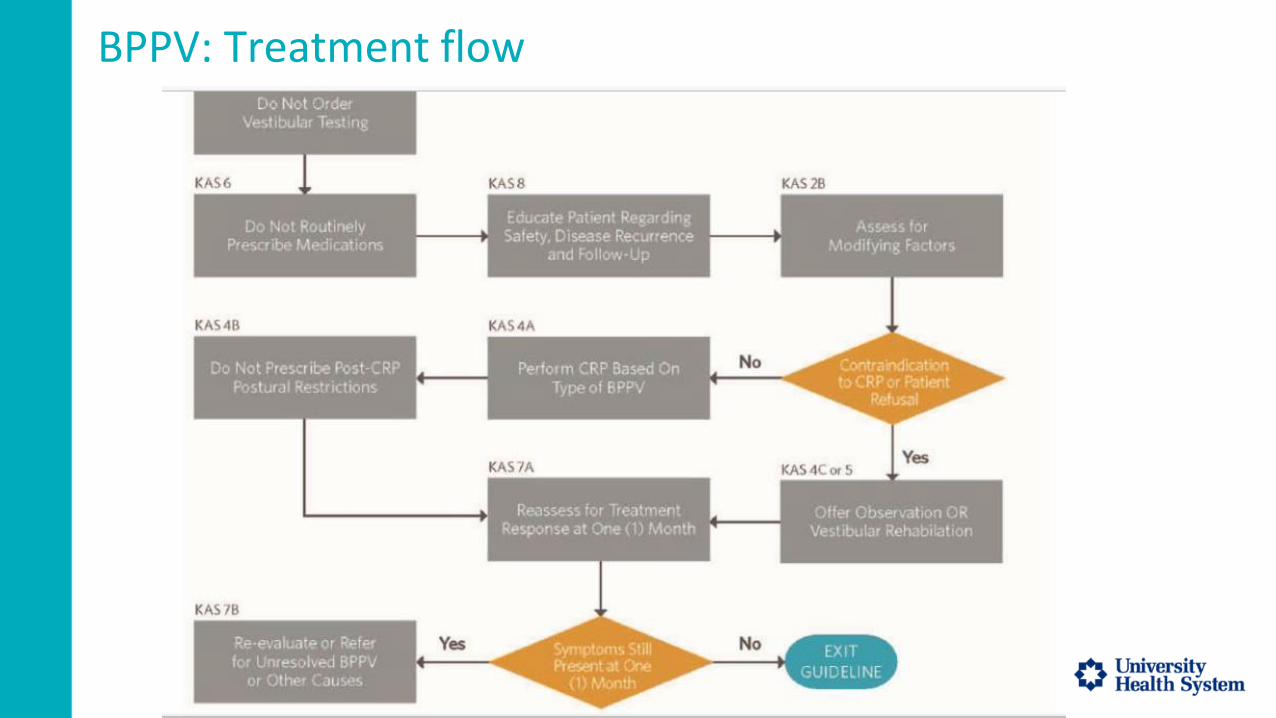
BPPV: Treatment flow

Unilateral Vestibular Hypofunction (UVH)
Uncompensated vestibular hypofunction results in postural instability, visual blurring with head movement, and subjective complaints of dizziness and/or imbalance.
On the basis of data from the National Health and Nutrition Examination Survey for 2001 to 2004, it is estimated that 35.4% of adults in the United States have vestibular dysfunction requiring medical attention and the incidence increases with age.Hall, et al. Vestibular Rehabilitation for Peripheral Vestibular Hypofunction: An Evidence-Based Clinical Practice Guideline. JNPT. 2016; 40: 124-155.
Unilateral Vestibular Hypofunction (UVH)
Appropriate treatment is critical because dizziness is a major risk factor for FALLS.
The incidence of falls is greater in individuals with vestibular hypofunction than in healthy individuals of the same age living in the community. Hall, et al. Vestibular Rehabilitation for Peripheral Vestibular Hypofunction: An Evidence-Based Clinical Practice Guideline. JNPT. 2016; 40: 124-155.
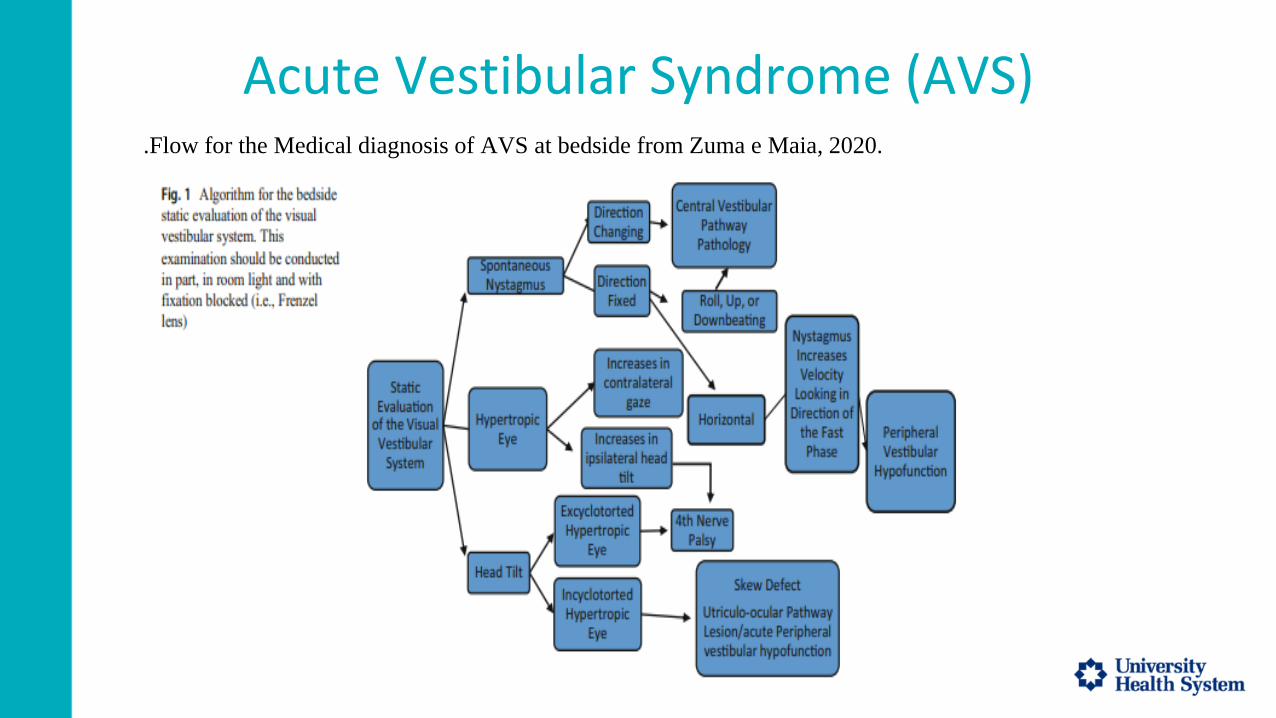
Acute Vestibular Syndrome (AVS).Flow for the Medical diagnosis of AVS at bedside from Zuma e Maia, 2020.
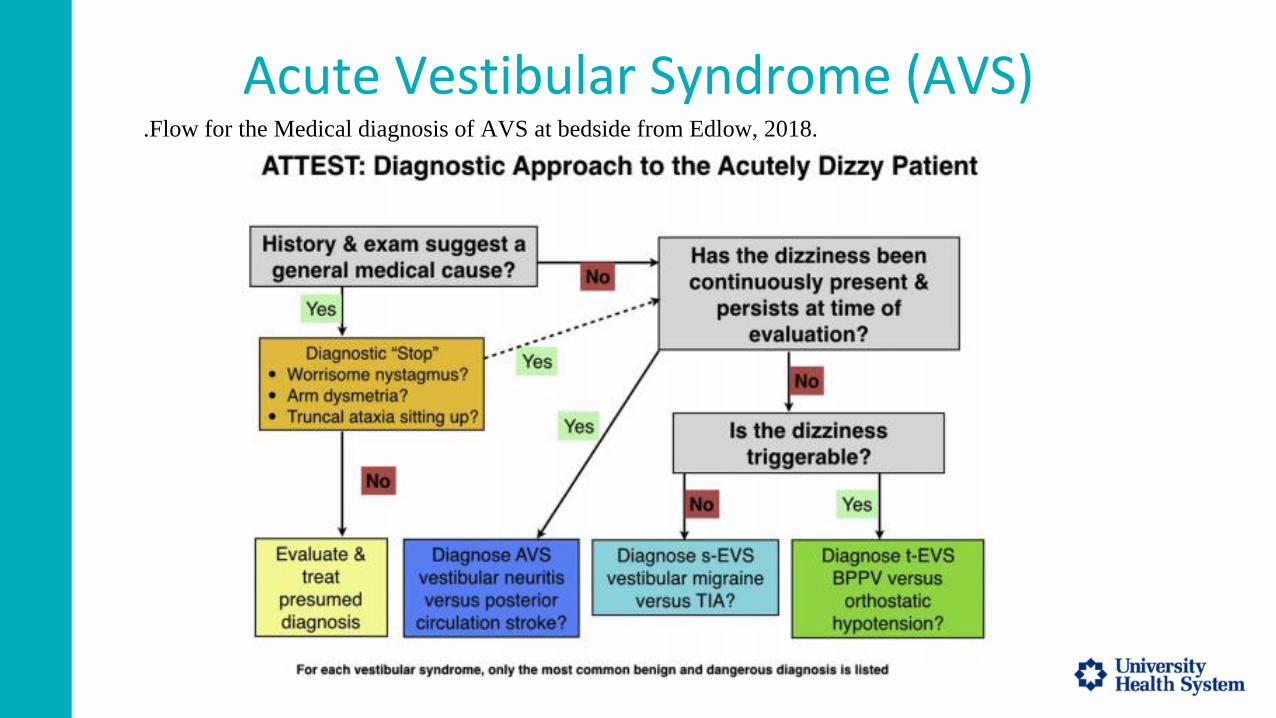
Acute Vestibular Syndrome (AVS).Flow for the Medical diagnosis of AVS at bedside from Edlow, 2018.
Acute Vestibular Syndrome (AVS).Flow for the Medical diagnosis of AVS at bedside from Edlow, 2018.
ATTEST:
A – Associated Symptoms
TT – Timing and Triggers (of dizziness)
ES – Examination Signs (Bedside exam)
T – Additional Testing (orthostatics)
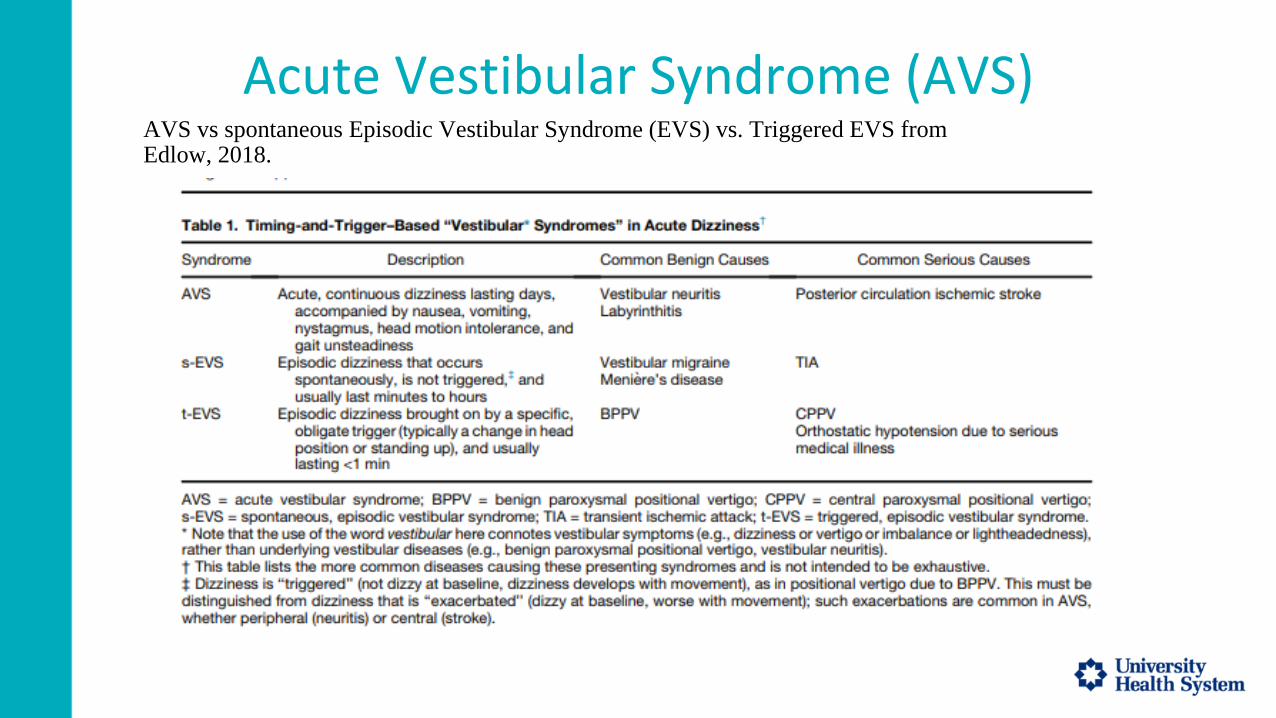
Acute Vestibular Syndrome (AVS)AVS vs spontaneous Episodic Vestibular Syndrome (EVS) vs. Triggered EVS from Edlow, 2018.

Pharmacological Management of Acute VertigoLatest Trends

Clinical Practice Guideline- BPPVBhattacharya et al (2017)
• Vestibular Physical Therapy referral
• Canalith Repositioning Maneuver indicated
• No further imaging/investigations necessary if post testing negative
• No vestibular suppressants indicated
• Exception; use vestibular suppressants if patient not able to tolerate treatment/ vestibular assessment

Acute Peripheral Vestibulopathy
• Unilateral vestibular hypofunction, resulting from varying pathological processes, most common-inflammatory.
• Steroid therapy is debated with no supportive evidence found in recent investigations (Yoo et al. 2017).
• Vestibular suppressants indicated to manage acute symptoms but must be discontinued in 7 days to allow vestibular compensation. (Chabbert, 2016)
• No evidence has been found in support of Antiviral Therapy (Strupp et al. 2004)
• Physical Therapy Clinical practice guideline with research evidence to support VRT in unilateral, bilateral Vestibulopathy (Hall et al, 2016)
Central Vertigo
• Brain Stem or cerebellar stroke
• Invisible Brain stem infarctions have been documented (Tsuyusaki et al. 2014)
• Clinical correlation is warranted
• Vestibular suppressants indicated
• Physical Therapy is indicated
Vestibular Suppressants
• Antihistamines- Meclizine, Cyclizine and promethazine
• Anticholinergics- Scopolamine transcutaneous patch.
• Benzodiazepines- Specially if severe anxiety is associated with vertigo
• Calcium channel antagonists-Cinarazine and flunarzine showing benefit in managing Vestibular Migraine. (Lepcha et al, 2014).

Comparing Vestibular suppressants
• Dornhoffer, Chelonis and Blake (2004) compared effectiveness of Vestibular suppressants in managing over vestibular stimulation in space motion sickness. From most effective to least, scopolamine > promethazine > placebo > meclizine > lorazepam
• Promethazine was found to be more effective in treating Acute vertigo in ED as compared to Lorezapam. (Amini et al. 2014)

Antiemetics
• Onadansetron has been found to be more effective than Promethazine alone to manage Nausea in patients with vertigo (Saberi et al. 2019).
• In addition to being an Antiemetic, Onadansetron may also have vestibulo-protective effect during an excitotoxic neuroinflammatory condition such as Vestibular neuritis resulting in decreased functional limitations (Dyhrfjeld-Johnsen et al. 2013).
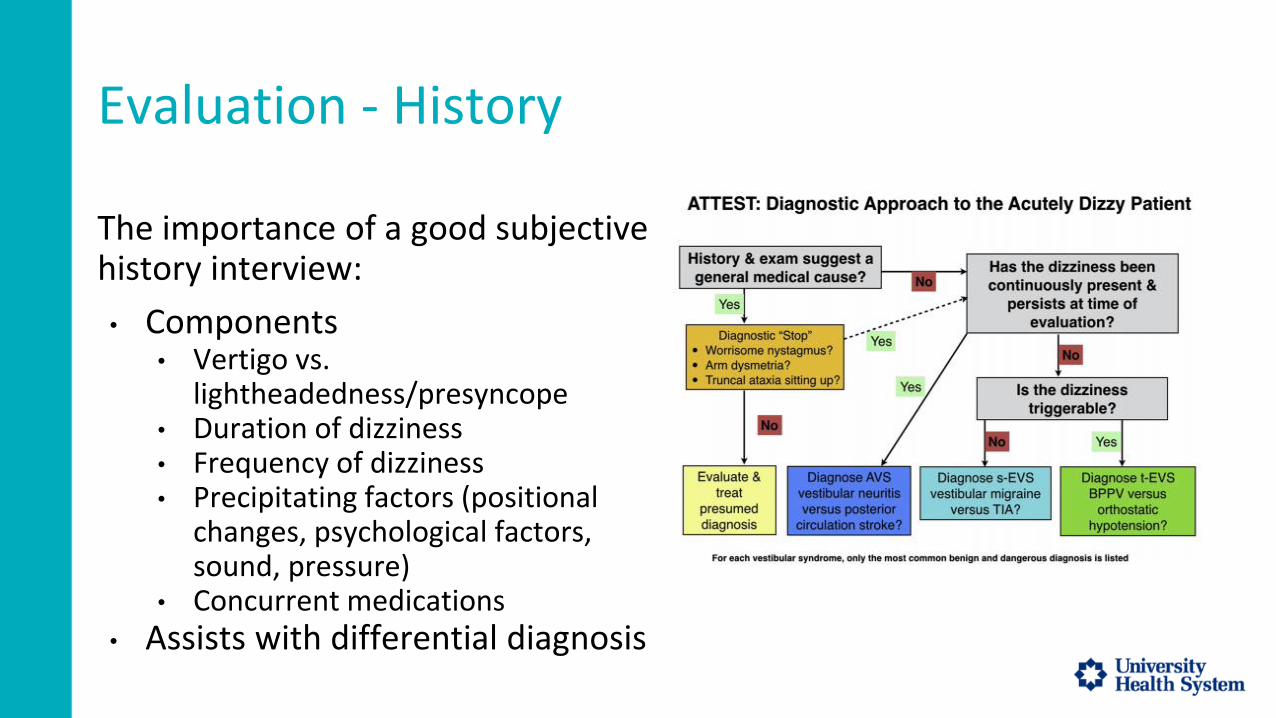
Evaluation - History
The importance of a good subjective history interview:
• Components• Vertigo vs.
lightheadedness/presyncope• Duration of dizziness• Frequency of dizziness• Precipitating factors (positional
changes, psychological factors, sound, pressure)
• Concurrent medications• Assists with differential diagnosis

Evaluation - HINTS (and HINTS+) Exam
• Quick exam to differentiate AVS from possible posterior circulation CVA
• Head Impulse, Nystagmus, and Test of Skew tests
• Possible stroke (or central pathology) includes:• NORMAL Head Impulse test• DIRECTION-CHANGING nystagmus• PRESENCE of skew deviation
Evaluation - Diagnostic Maneuvers
• Dix Hallpike• Modified Dix Hallpike• Supine Roll Test• Sit to Supine Test
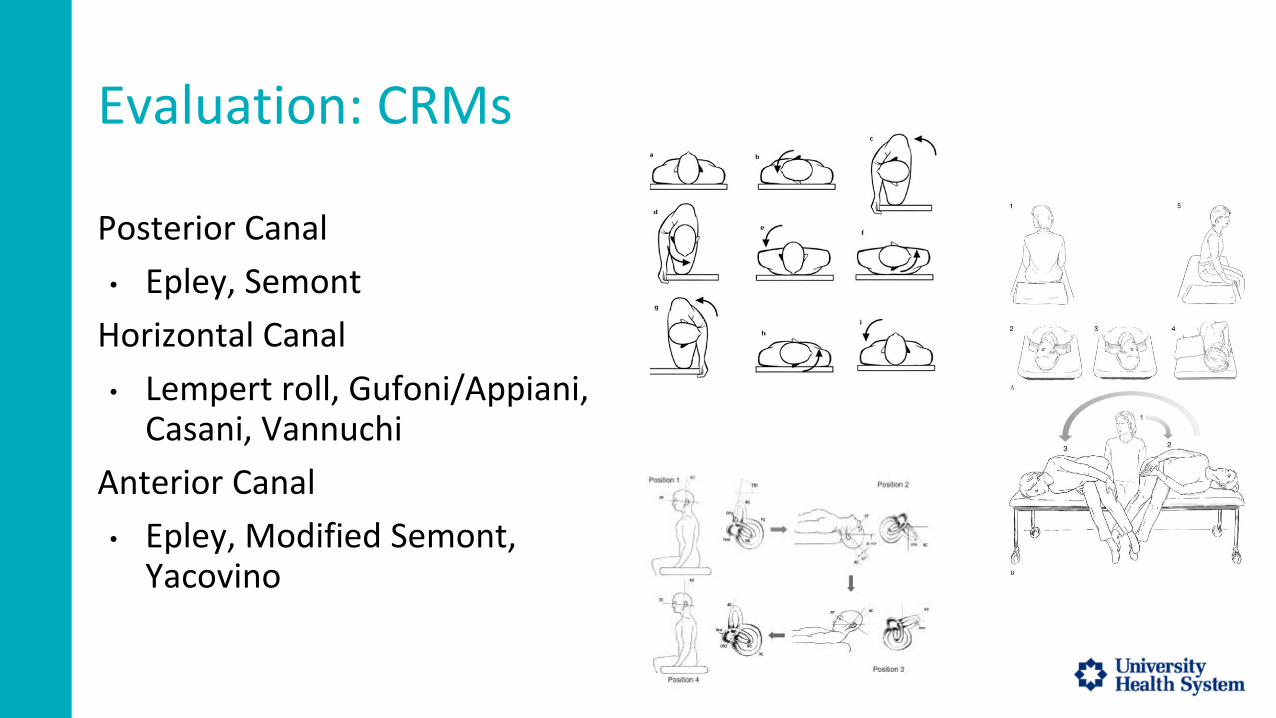
Evaluation: CRMs
Posterior Canal
• Epley, Semont
Horizontal Canal
• Lempert roll, Gufoni/Appiani, Casani, Vannuchi
Anterior Canal
• Epley, Modified Semont, Yacovino
Outcome Measures
Why Use Outcome Measures?
• Quantify observations is meaningful way• Consistency between therapists• Consistency between settings (acute - IP - OP)• Justification of therapy needs• Easier documentation
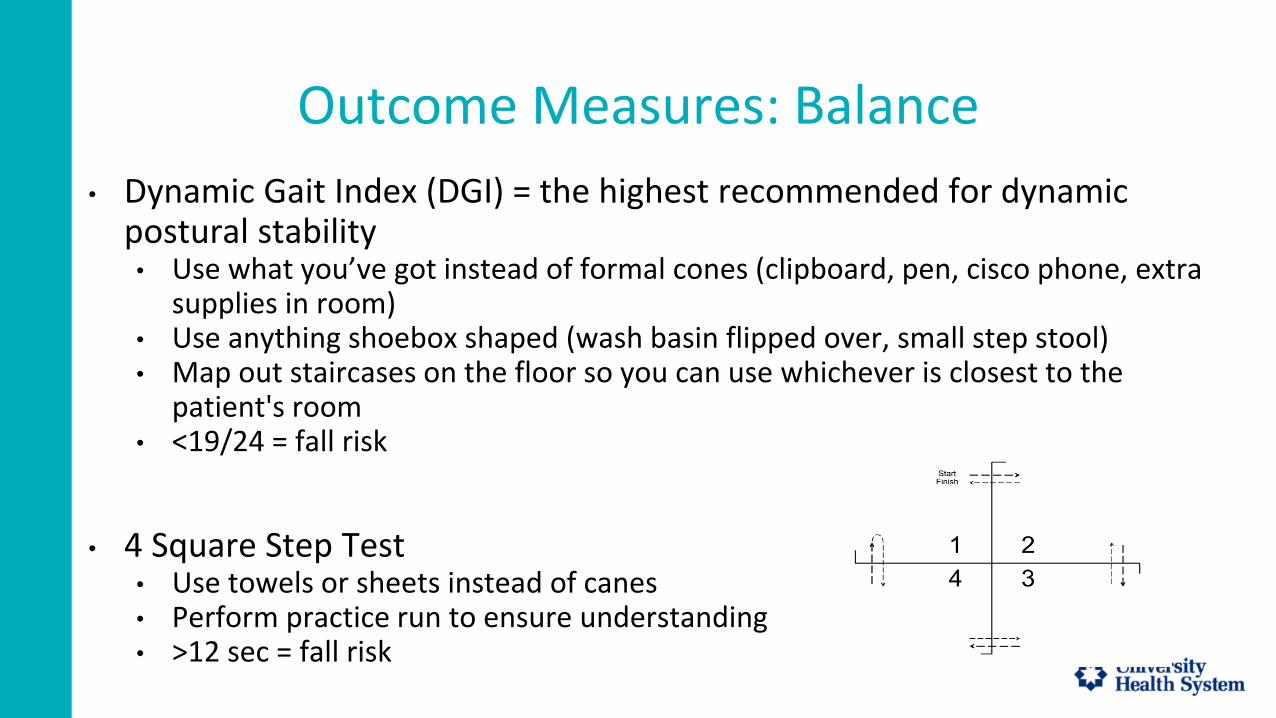
Outcome Measures: Balance
• Dynamic Gait Index (DGI) = the highest recommended for dynamic postural stability • Use what you’ve got instead of formal cones (clipboard, pen, cisco phone, extra
supplies in room)• Use anything shoebox shaped (wash basin flipped over, small step stool)• Map out staircases on the floor so you can use whichever is closest to the
patient's room• <19/24 = fall risk
• 4 Square Step Test• Use towels or sheets instead of canes• Perform practice run to ensure understanding• >12 sec = fall risk

Outcome Measures: Other Domains
• Gaze Stabilization: Head Impulse Test*
• Positional: Dix Hallpike*
• *Note this is more diagnostic than traditional outcome measure
• Function/ Participation: Dizziness Handicap Inventory

Barriers to Vestibular Care in the Acute Setting
• Traumatic injuries• vertebral artery screen, neck issues, orthopedic injuries that prevent
maneuvers• Cognitive issues• Acute brain injury• Post-surgical precautions• Vitals• Electrolyte imbalances• Potential for worsening acute status
Barriers to Vestibular Care in the Acute Setting
Other acute disorders may mimic BPPV e.g. migraines, vertebral artery occlusions, tumors, hydrocephalus, psychogenic disorders
Equipment?
• Plinths often not available in the acute care setting• Appropriateness for plinth?
• Time, stability, endurance to transport to gym• Hospital bed modification
• For Dix Hallpike/Epley - two pillows underneath lumbar/thoracic area• Trendelenburg position with bed or tilt table if patient lacks neck extension
• Check for contraindications of back extension with acute injuries
Physical Therapy in ED (Kim et al. 2018)
As the ED patient volumes continue to increase, there is a need for ED initiated Physical Therapy
ED physicians are often unable to complete a detailed evaluation as is needed for Peripheral Vertigo (Chrisholm et al. 2008)
Peripheral Vertigo assessment and treatment by ED PT has potential to decrease length of stay and unnecessary imaging/tests
An effective communication and collaboration with stake holders such as ED physicians, ED administration is necessary
What interventions do we choose ?
SYMPTOMS DIAGNOSIS FUNCTION DIZZINESS OF NON
VESTIBULAR ORIGIN
Positional Vertigo
Impaired Gaze stability
Non-Positional Vertigo
Dizziness
Vertigo
Gait dysfunction
Falls
Bed mobility
Transfers
Gait
Balance
ADLs
Postural Hypotension
Pulmonary pathology
Cardiac conditions
Migraine
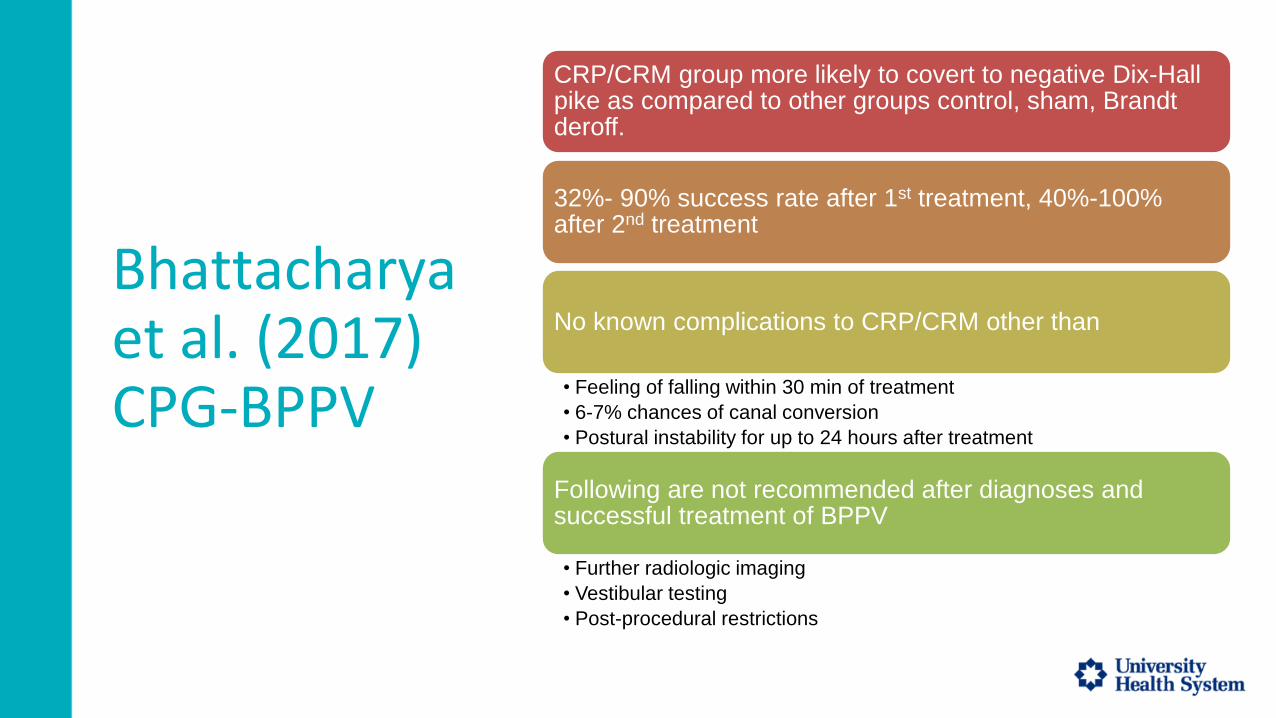
Bhattacharya et al. (2017) CPG-BPPV
CRP/CRM group more likely to covert to negative Dix-Hall pike as compared to other groups control, sham, Brandt deroff.
32%- 90% success rate after 1st treatment, 40%-100% after 2nd treatment
No known complications to CRP/CRM other than
• Feeling of falling within 30 min of treatment
• 6-7% chances of canal conversion
• Postural instability for up to 24 hours after treatment
Following are not recommended after diagnoses and successful treatment of BPPV
• Further radiologic imaging
• Vestibular testing
• Post-procedural restrictions

BPPV: Treatment flow from CPG

BPPV: Treatment flow
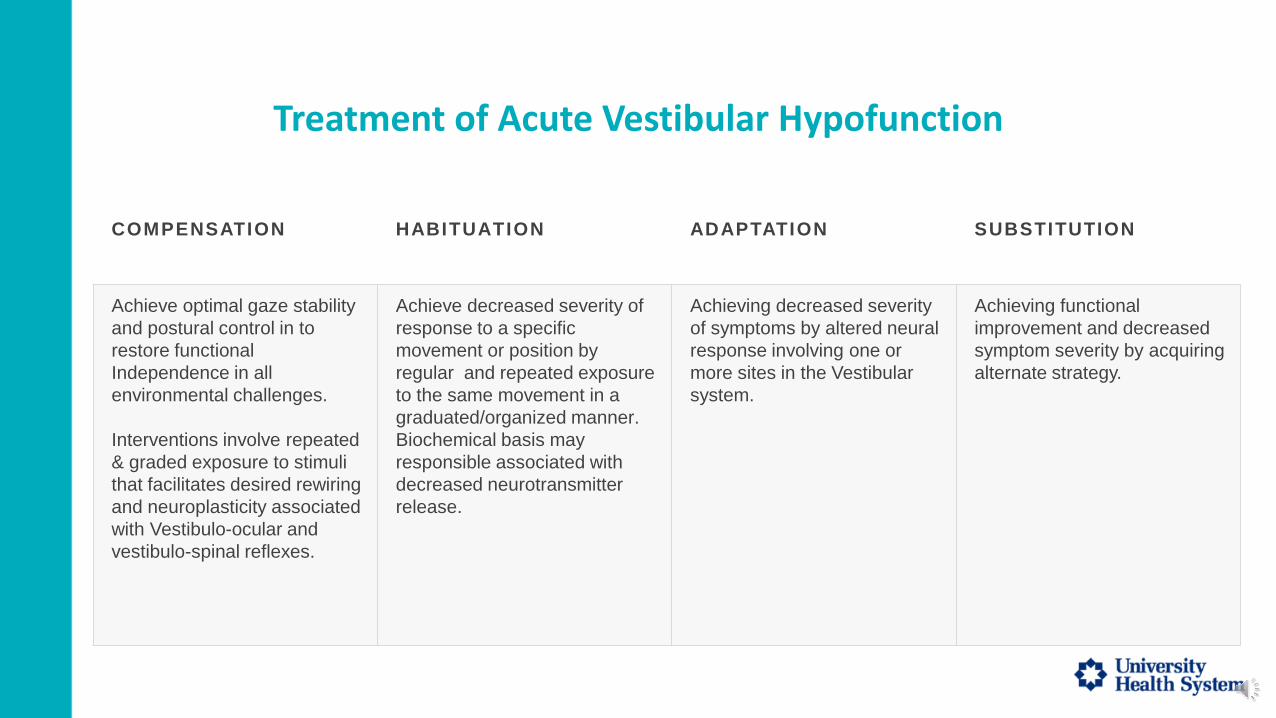
Treatment of Acute Vestibular Hypofunction
COMPENSATION HABITUATION ADAPTATION SUBSTITUTION
Achieve optimal gaze stability
and postural control in to
restore functional
Independence in all
environmental challenges.
Interventions involve repeated
& graded exposure to stimuli
that facilitates desired rewiring
and neuroplasticity associated
with Vestibulo-ocular and
vestibulo-spinal reflexes.
Achieve decreased severity of
response to a specific
movement or position by
regular and repeated exposure
to the same movement in a
graduated/organized manner.
Biochemical basis may
responsible associated with
decreased neurotransmitter
release.
Achieving decreased severity
of symptoms by altered neural
response involving one or
more sites in the Vestibular
system.
Achieving functional
improvement and decreased
symptom severity by acquiring
alternate strategy.
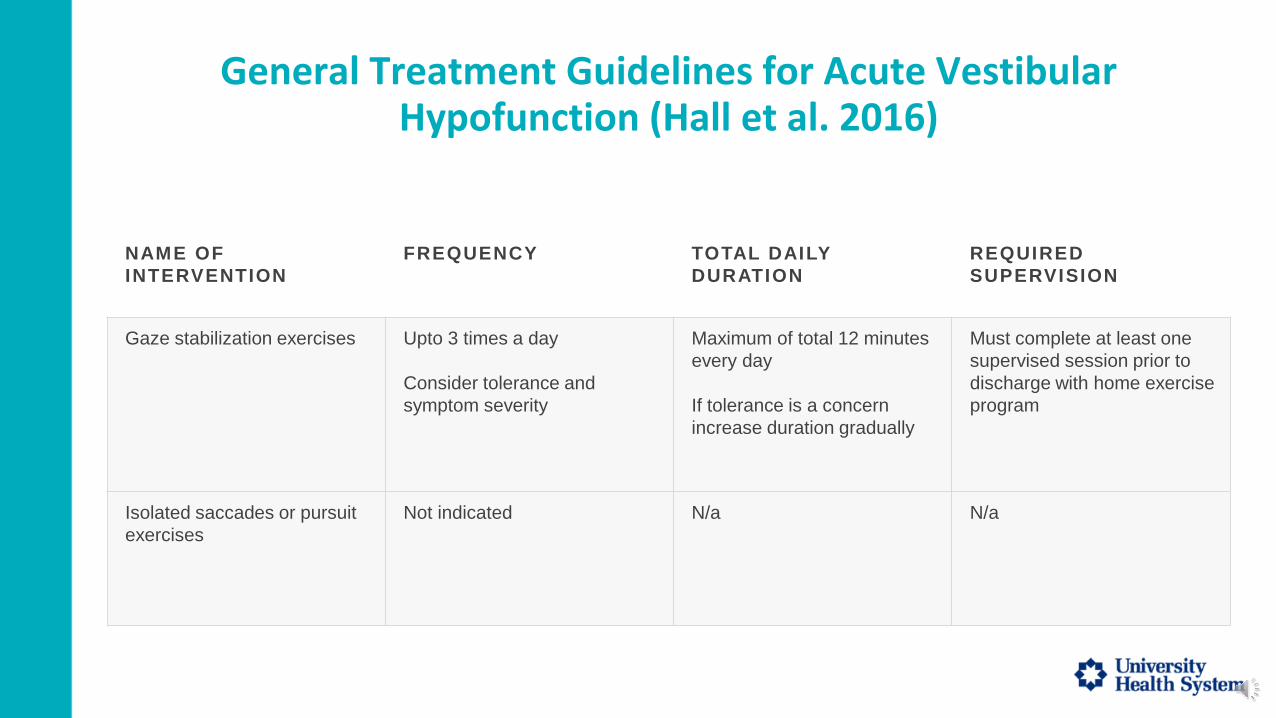
General Treatment Guidelines for Acute Vestibular Hypofunction (Hall et al. 2016)
NAME OF
INTERVENTION
FREQUENCY TOTAL DAILY
DURATION
REQUIRED
SUPERVISION
Gaze stabilization exercises Upto 3 times a day
Consider tolerance and
symptom severity
Maximum of total 12 minutes
every day
If tolerance is a concern
increase duration gradually
Must complete at least one
supervised session prior to
discharge with home exercise
program
Isolated saccades or pursuit
exercises
Not indicated N/a N/a

Gaze Stabilization Exercises x1
INTERVENTION &
PROGRESSION
MECHANISM
X1 viewing exercise
Progression by using a
metronome
Progression by increasing
postural challenge
a. sitting unsupported
b. standing with optimal BOS
c. Standing narrow BOS
VOR adaption/compensation

Gaze Stabilization Exercises x2
NAME OF
INTERVENTION
MECHANISM
X2 viewing exercise
Progression by using a
metronome
Progression by increasing
postural challenge
a. Sitting unsupported
b. Standing with optimal
BOS
c. Standing narrow BOS
VOR adaption/compensation
Treatment of Acute UVH in ED
• During Acute phase patient likely to be in a lot of distress/anxiety
• Consider severity of symptoms before starting viewing exercises
• Consider recommending Vestibular suppressants to manage acute symptoms.
• In most cases vestibular suppressants must be discontinued 7 days after onset to ensure compensation
• Once diagnosed with Acute UVH and all other pathologies ruled out, education and reassurance about prognosis can be beneficial.
Time Frames
Patients with BPPV, resolved (negative post testing)
• Can go home from ED if no other unrelated medica/surgical needs
• Document pre/post testing and subjective reports
• Document pre/post treatment changes in mobility
• Outcome reports
Patients with Acute UVH
• May go to the floor
• 3-5 days in hospital based on severity
• Likely get put on steroids if inflammatory process suspected
• Document functional/ADL limitations, barriers for safe discharge to support rehab (if needed)

Discharge Disposition
BPPV-IF RESOLVED
AFTER TREATMENT
BPPV- IF NOT
RESOLVED AFTER
TREATMENT
ACUTE UVH THAT IS
NOT RESOLVED
COMPLETELY
ACUTE UVH THAT IS
PARTIALLY RESOLVED
WITH MINIMAL
SYMPTOMS
Home with no follow up
needed if no other barriers
exist
No Assistive device
indicated unless indicated
for another
diagnosis/limitation
No vestibular suppressants
indicated
Home with follow up with
recommendations to follow up
with a specialist
No Assistive device indicated
unless indicated for another
diagnosis/limitation
No Vestibular Suppressants
indicated
Based on mobility and
homeset up any where from
Rehab to Home with Home
health
Assistive device
recommendations to be made
considering symptoms usually
resolve in weeks/days
Vestibular suppressants
usually discontinued 7 days
from onset unless indicated
otherwise
Home with recommendations
to follow up with a vestibular
specialist.
Assistive device
recommendations to be made
considering symptoms usually
resolve in weeks/days
Vestibular suppressants
usually discontinued 7 days
from onset unless indicated
otherwise
Does Physical Therapy work
for these patients?
• Expanding literature supporting Vestibular rehab in vestibular disorders of central and peripheral orgin (Dunlap, Holmberg & Whitney, 2019).
• Canalolith Repositioning Maneuvers can relieve disabling symptoms of BPPV, eliminating need of further imaging (Bhattacharya et al. 2008).
• Corticosteroid therapy and vestibular Rehabilitation therapy have been found to be equally effective in Vestibular Neuritis (Ismail, Morgan & Abdel Rehman, 2018)
• Early intervention can be a game changer in improving outcomes of unilateral vestibular hypofunction (Michael, Laurent & Alain, 2020)
Relevant Practice Patterns
• Pattern 5A: Primary Prevention/Risk Reduction for Loss of
Balance and Falling
• Pattern 5F: Impaired Peripheral Nerve Integrity and Muscle
Performance Associated With Peripheral Nerve Injury
References• Asprella Libonati G. Diagnostic and treatment strategy of lateral semicircular canal canalolithiasis. Acta Otorhinolaryngol Ital. 2005 Oct;25(5):277-83. PMID:
16602326; PMCID: PMC2639908.
• Bhattacharyya, N., Gubbels, S. P., Schwartz, S. R., Edlow, J. A., El-Kashlan, H., Fife, T., Holmberg, J. M., Mahoney, K., Hollingsworth, D. B., Roberts, R., Seidman, M. D., Steiner, R. W., Do, B. T., Voelker, C. C., Waguespack, R. W., & Corrigan, M. D. (2017). Clinical Practice Guideline: Benign Paroxysmal Positional Vertigo (Update). Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery, 156(3_suppl), S1–S47. https://doi.org/10.1177/0194599816689667
• Emergency Department Workplace Interruptions Are Emergency Physicians “Interrupt-driven” and “Multitasking”? Carey D. Chisholm MD, Edgar K. Collison BA, David R. Nelson MS, William H. Cordell MD
• Four square step test2. Shirley Ryan AbilityLab. (n.d.). Retrieved, from https://www.sralab.org/rehabilitation-measures/four-square-step-test.
• Head impulse test / head thrust test. Shirley Ryan AbilityLab. (n.d.). Retrieved, from https://www.sralab.org/rehabilitation-measures/head-impulse-test-head-thrust-test#vestibular-disorders.
• Herdman, S. J., & Clendaniel, R. (2014). Vestibular rehabilitation. F.A. Davis.
• Kattah, J., Talkad, A., Wang, D., Hsieh, Y. and Newman-Toker, D., 2009. HINTS to Diagnose Stroke in the Acute Vestibular Syndrome. Stroke, 40(11), pp.3504-3510.
• Lempert, T. and Tiel-Wilck, K. (1996), A Positional Maneuver for Treatment of Horizontal-Canal Benign Positional Vertigo. The Laryngoscope, 106: 476-478.
• Mandalà, M., Pepponi, E., Santoro, G.P., Cambi, J., Casani, A., Faralli, M., Giannoni, B., Gufoni, M., Marcelli, V., Trabalzini, F., Vannucchi, P. and Nuti, D. (2013), Double-blind randomized trial on the efficacy of the Gufoni maneuver for treatment of lateral canal BPPV. The Laryngoscope, 123: 1782-1786.
• Parnes, L., Agrawal, S. and Atlas, J., 2021. Diagnosis and management of benign paroxysmal positional vertigo (BPPV). [online] CMAJ.
• Vestibular UVH Clinical Practice Guideline - neuropt.org. Academy of Neurologic Physical Therapy. (n.d.). Retrieved, from https://www.neuropt.org/docs/default-source/cpgs/vestibular-uvh-clinical-practice-guideline.pdf?sfvrsn=2&sfvrsn=2.
• Yacovino DA, Hain TC, Gualtieri F. New therapeutic maneuver for anterior canal benign paroxysmal positional vertigo. J Neurol. 2009 Nov;256(11):1851-5. doi: 10.1007/s00415-009-5208-1. Epub 2009 Jun 18. PMID: 19536580.
References
• Amini, A., Heidari, K., Asadollahi, S., Habibi, T., Shahrami, A., Mansouri, B., & Kariman, H. (2014). Intravenous promethazine versus lorazepam for the treatment of peripheral vertigo in the emergency department: A double blind, randomized clinical trial of efficacy and safety. Journal of vestibular research : equilibrium & orientation, 24(1), 39–47. https://doi.org/10.3233/VES-130506
• Antor, M. A., Uribe, A. A., Erminy-Falcon, N., Werner, J. G., Candiotti, K. A., Pergolizzi, J. V., & Bergese, S. D. (2014). The effect of transdermal scopolamine for the prevention of postoperative nausea and vomiting. Frontiers in pharmacology, 5, 55. https://doi.org/10.3389/fphar.2014.00055
• Bhattacharyya, N., Baugh, R. F., Orvidas, L., Barrs, D., Bronston, L. J., Cass, S., Chalian, A. A., Desmond, A. L., Earll, J. M., Fife, T. D., Fuller, D. C., Judge, J. O., Mann, N. R., Rosenfeld, R. M., Schuring, L. T., Steiner, R. W., Whitney, S. L., Haidari, J., & American Academy of Otolaryngology-Head and Neck Surgery Foundation (2008). Clinical practice guideline: benign paroxysmal positional vertigo. Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery, 139(5 Suppl 4), S47–S81. https://doi.org/10.1016/j.otohns.2008.08.022
• Carmeli E. (2015). Anxiety in the Elderly Can be a Vestibular Problem. Frontiers in public health, 3, 216. https://doi.org/10.3389/fpubh.2015.00216
• Chabbert C. (2016). Principles of vestibular pharmacotherapy. Handbook of clinical neurology, 137, 207–218. https://doi.org/10.1016/B978-0-444-63437-5.00014-5
• Dhaliwal JS, Rosani A, Saadabadi A. Diazepam. [Updated 2020 Aug 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537022/
• Dornhoffer, J., Chelonis, J. J., & Blake, D. (2004). Stimulation of the semicircular canals via the rotary chair as a means to test pharmacologic countermeasures for space motion sickness. Otology & neurotology : official publication of the American Otological Society, American Neurotology Society [and] European Academy of Otology and Neurotology, 25(5), 740–745. https://doi.org/10.1097/00129492-200409000-00016
• Dunlap, P. M., Holmberg, J. M., & Whitney, S. L. (2019). Vestibular rehabilitation: advances in peripheral and central vestibular disorders. Current opinion in neurology, 32(1), 137–144. https://doi.org/10.1097/WCO.0000000000000632
• Dyhrfjeld-Johnsen, J., Gaboyard-Niay, S., Broussy, A., Saleur, A., Brugeaud, A., & Chabbert, C. (2013). Ondansetron reduces lasting vestibular deficits in a model of severe peripheral excitotoxic injury. Journal of vestibular research : equilibrium & orientation, 23(3), 177–186. https://doi.org/10.3233/VES-130483
• Gurvich, C., Maller, J. J., Lithgow, B., Haghgooie, S., & Kulkarni, J. (2013). Vestibular insights into cognition and psychiatry. Brain research, 1537, 244–259. https://doi.org/10.1016/j.brainres.2013.08.058
• Hall, C. D., Herdman, S. J., Whitney, S. L., Cass, S. P., Clendaniel, R. A., Fife, T. D., Furman, J. M., Getchius, T. S., Goebel, J. A., Shepard, N. T., & Woodhouse, S. N. (2016). Vestibular Rehabilitation for Peripheral Vestibular Hypofunction: An Evidence-Based Clinical Practice Guideline: FROM THE AMERICAN PHYSICAL THERAPY ASSOCIATION NEUROLOGY SECTION. Journal of neurologic physical therapy : JNPT, 40(2), 124–155. https://doi.org/10.1097/NPT.0000000000000120
• Han, B. I., Song, H. S., & Kim, J. S. (2011). Vestibular rehabilitation therapy: review of indications, mechanisms, and key exercises. Journal of clinical neurology (Seoul, Korea), 7(4), 184–196. https://doi.org/10.3988/jcn.2011.7.4.184
• Heiss WD, Zeiler K. Medikamentöse Beeinflussung der Hirndurchblutung [The influence on drugs on cerebral blood flow] Pharmakotherapie. 1978;1(3):137–144
• Huang, S. Y., Jeng, C., Kao, S. C., Yu, J. J., & Liu, D. Z. (2004). Improved haemorrheological properties by Ginkgo biloba extract (Egb 761) in type 2 diabetes mellitus complicated with retinopathy. Clinical nutrition (Edinburgh, Scotland), 23(4), 615–621. https://doi.org/10.1016/j.clnu.2003.10.010
Reference• Ismail, E. I., Morgan, A. E., & Abdel Rahman, A. M. (2018). Corticosteroids versus vestibular rehabilitation in long-term outcomes in vestibular neuritis. Journal of vestibular research : equilibrium &
orientation, 28(5-6), 417–424. https://doi.org/10.3233/VES-180645
• Lepcha, A., Amalanathan, S., Augustine, A.M. et al. Flunarizine in the prophylaxis of migrainous vertigo: a randomized controlled trial. Eur Arch Otorhinolaryngol 271, 2931–2936 (2014). https://doi.org/10.1007/s00405-013-2786-4
• Lin, E., & Aligene, K. (2013). Pharmacology of balance and dizziness. NeuroRehabilitation, 32(3), 529-542. doi:10.3233/nre-130875
• Maass B, Silberzahn J, Simon R. Zur Wirkung von Ginkgo-biloba—Extrakt (Tebonin) auf die Wasserstoff-Auswaschvorgänge an der Cochleabasis unter hypotensiver Ischämie. Extracta Otorhinolaryngologica. 1987
• Maass B, Silberzahn J, Simon R. Zur Wirkung von Ginkgo-biloba—Extrakt (Tebonin) auf die Wasserstoff-Auswaschvorgänge an der Cochleabasis unter hypotensiver Ischämie. Extracta Otorhinolaryngologica. 1987
• Michel, L., Laurent, T., & Alain, T. (2020). Rehabilitation of dynamic visual acuity in patients with unilateral vestibular hypofunction: earlier is better. European archives of oto-rhino-laryngology : official journal of the European Federation of Oto-Rhino-Laryngological Societies (EUFOS) : affiliated with the German Society for Oto-Rhino-Laryngology - Head and Neck Surgery, 277(1), 103–113. https://doi.org/10.1007/s00405-019-05690-4
• Nagaratnam, N., Ip, J., & Bou-Haidar, P. (2005). The vestibular dysfunction and anxiety disorder interface: a descriptive study with special reference to the elderly. Archives of gerontology and geriatrics, 40(3), 253–264. https://doi.org/10.1016/j.archger.2004.09.006
• Newman-Toker, D. E., Camargo, C. A., Jr, Hsieh, Y. H., Pelletier, A. J., & Edlow, J. A. (2009). Disconnect between charted vestibular diagnoses and emergency department management decisions: a cross-sectionalanalysis from a nationally representative sample. Academic emergency medicine : official journal of the Society for Academic Emergency Medicine, 16(10), 970–977. https://doi.org/10.1111/j.1553-2712.2009.00523.x
• Rutka J. (2019). Aminoglycoside Vestibulotoxicity. Advances in oto-rhino-laryngology, 82, 101–110. https://doi.org/10.1159/000490277
• Saberi, A., Pourshafie, S. H., Kazemnejad-Leili, E., Nemati, S., Sutohian, S., & Sayad-Fathi, S. (2019). Ondansetron or promethazine: Which one is better for the treatment of acute peripheral vertigo?. American journal of otolaryngology, 40(1), 10–15. https://doi.org/10.1016/j.amjoto.2018.09.010
• Schmitt, L. G., & Shaw, J. E. (1986). Alleviation of induced vertigo. Therapy with transdermal scopolamine and oral meclizine. Archives of otolaryngology--head & neck surgery, 112(1), 88–91. https://doi.org/10.1001/archotol.1986.03780010090017
• Strupp, M., Zingler, V. C., Arbusow, V., Niklas, D., Maag, K. P., Dieterich, M., Bense, S., Theil, D., Jahn, K., & Brandt, T. (2004). Methylprednisolone, valacyclovir, or the combination for vestibular neuritis. The New England Journal of Medicine, 351(4), 354–361.
• Sokolova, L., Hoerr, R., & Mishchenko, T. (2014). Treatment of Vertigo: A Randomized, Double-Blind Trial Comparing Efficacy and Safety of Ginkgo biloba Extract EGb 761 and Betahistine. International journal of otolaryngology, 2014, 682439. https://doi.org/10.1155/2014/682439
• Tsuyusaki, Y., Sakakibara, R., Kishi, M., Tateno, F., Aiba, Y., Ogata, T., Nagao, T., Terada, H., & Inaoka, T. (2014). "Invisible" brain stem infarction at the first day. Journal of stroke and cerebrovascular diseases : the official journal of National Stroke Association, 23(7), 1903–1907. https://doi.org/10.1016/j.jstrokecerebrovasdis.2014.02.010
• Weerts, A. P., De Meyer, G., Pauwels, G., Vanspauwen, R., Dornhoffer, J. L., Van de Heyning, P. H., & Wuyts, F. L. (2012). Pharmaceutical countermeasures have opposite effects on the utricles and semicircular canals in man. Audiology & neuro-otology, 17(4), 235–242. https://doi.org/10.1159/000337273
• Yoo, M. H., Yang, C. J., Kim, S. A., Park, M. J., Ahn, J. H., Chung, J. W., & Park, H. J. (2017). Efficacy of steroid therapy based on symptomatic and functional improvement in patients with vestibular neuritis: a prospective randomized controlled trial. European Archives of Oto-Rhino-Laryngology : Official Journal of the European Federation of Oto-Rhino-Laryngological Societies (EUFOS) : Affiliated with the German Society for Oto-Rhino-Laryngology - Head and Neck Surgery, 274(6), 2443–2451. https://doi-org.akin.css.edu/10.1007/s00405-017-4556-1

Break out into 3 groups for case studies
When return to large group will need:
Brief Summary of discussion from one group member (~3 mins or less)
• Treatment chosen
• Goals for patient
• Discharge Planning/Disposition
Case Study #1: Man Who Hates Movement
Order to see patient for PT evaluation for dizziness, being worked up for CVA
• Came in after fall at home because he was so dizzy, he got up and had to hold onto the wall to make it to the bathroom to vomit, family called 911
• CT was negative, pending MRI
Walk in the room, patient is in bed, doesn’t turn to look at you just keeps looking straight ahead, not happy to see you for PT because he don’t want to get up because he get dizzy and nauseous
• No lights on, blinds drawn

Case Study #1: Man Who Hates Movement
First Part of Exam = mobility basics
• Seems to be doing well with no immediately noticeable balance issues• DGI of 21/24, few points off for head turns
Second Part of Exam = vestibular portion
• Dix Hallpike is negative• HINTS
• + Head Impulse on R• - Direction Changing Nystagmus• + Test of Skew on R
• Symptomatic with smooth pursuits, saccades, gaze conjugation (also noted to have corrective saccades on R)

Case Study #1: Man Who Hates Movement
What tests would you do?
What diagnose(s) does the patient have?
What treatment would you do first?
What is a good (“SMART”) goal for the patient?
Where would you send him next/disposition?
Case Study #2: M.D.
Pt is a 70 yo man who fell at home, hitting his head posteriolaterally. He was admitted from ED after MRI showed he had a small SDH in occipitoparietal region on right. On Neuro floor, he complains of dizziness and is unsteady with walking, needing HH support or to use a RW with CGA to ambulate. He has dizziness with moving in/out of bed and needs to sit at bedside for about 30 secs before he can do a sit to stand or bed to WC transfer. He denies hearing loss or tinnitus. He reports dizziness when he moves his head or turns to quickly.

Case Study #2: M.D.
What tests would you do?
What diagnose(s) does M.D. have?
What treatment would you do first?
What is a good (“SMART”) goal for M.D.?
Where would you send him next/disposition?

Return to Large Group
Brief Summary from one group member (~3 mins or less)
• Treatment chosen
• Goals for pt
• DC planning/Disposition
Questions?
Any Questions?
Chara Booker, PT, DPT, NCS, Herdman-certified Vestibular Rehab specialist
Julie Miller, PT, DPT, NCS, CBIS
Reeves Rehab Center at University Health, San Antonio, TX
Nitin Saini, PT, DPT – Methodist Hospital, San Antonio, TX
Michael Tran, PT, DPT – Dell Seton Medical Center, Austin, TX
Thank You!!
.





























