Embed Size (px)
Citation preview

1
Vestibular Rehabilitation: Vestibular Rehabilitation: Solutions to Common Solutions to Common
DysfunctionDysfunction
Nicole PrietoNicole Prieto--Lewis, MSPTLewis, MSPT
Dianna Saunders, MS, PTDianna Saunders, MS, PTGait and Balance ClinicGait and Balance Clinic
Gainesville VAMCGainesville VAMC
TopicsTopics Defining dizziness?Defining dizziness?
The Dizziness History The Dizziness History
Is this vestibular? (differential diagnosis)Is this vestibular? (differential diagnosis)
When to refer to MD?When to refer to MD?
The Clinical ExamThe Clinical ExamCentral ScreeningCentral Screening
Testing for BPPVTesting for BPPV
Testing VORTesting VOR
TreatmentTreatment
Lab sessionsLab sessions
““Dizziness ComplaintDizziness Complaint””
In the U.S., the primary complaint of In the U.S., the primary complaint of ““dizzinessdizziness”” results in nearly 7 million clinic results in nearly 7 million clinic visits per yearvisits per year
Vestibular disorders account for Vestibular disorders account for approximately 85% of these visitsapproximately 85% of these visits
90% of vertigo complaints in the over 65 90% of vertigo complaints in the over 65 crowd are due to peripheral vestibular crowd are due to peripheral vestibular impairmentsimpairments
““Dizziness ComplaintDizziness Complaint””
Dizziness/ Imbalance is the #1 reason that Dizziness/ Imbalance is the #1 reason that an elderly person consults a doctoran elderly person consults a doctor
BPPV accounts for 20BPPV accounts for 20--50% of vertigo 50% of vertigo complaints in those over 65complaints in those over 65
History of DizzinessHistory of Dizziness
Can be complex, as the complaint of Can be complex, as the complaint of ““dizzinessdizziness”” can be a very vague can be a very vague symptomsymptom
Key items for a good history:Key items for a good history:
Timing, Symptoms, ConditionsTiming, Symptoms, Conditions
Most important part of examMost important part of exam
TimingTiming
How long have you been dizzy?How long have you been dizzy? Is it an acute onset vs. chronicIs it an acute onset vs. chronic
Did event occur that immediately Did event occur that immediately precluded dizzinessprecluded dizziness
Frequency of Dizziness:Frequency of Dizziness: Is it constant (truly) or episodicIs it constant (truly) or episodic
Do symptoms last seconds, minutes , Do symptoms last seconds, minutes , hours or days?hours or days?

2
SymptomsSymptoms
What is meant by What is meant by ““dizzinessdizziness””?? Helps to distinguish between vertigo vs. Helps to distinguish between vertigo vs.
lightheadedlightheaded
Ask abo t related s mptomsAsk abo t related s mptoms Ask about related symptomsAsk about related symptoms nausea, hearing tinnitus, headache, nausea, hearing tinnitus, headache,
balance problems, etc.balance problems, etc.
Is there a true loss of consciousness?Is there a true loss of consciousness? if yes refer back to MDif yes refer back to MD
CircumstanceCircumstance
What brings on your symptoms? What brings on your symptoms?
What makes the dizziness worse?What makes the dizziness worse?
T l h th Di iT l h th Di i Tools such as the Dizziness Tools such as the Dizziness Handicap Inventory (DHI) may be Handicap Inventory (DHI) may be usefuluseful
Grade dizziness on a scale of 0Grade dizziness on a scale of 0--10.10.
Common Causes of Common Causes of ““DizzinessDizziness””
SystemSystem %%
Peripheral Vestibular (otologic)Peripheral Vestibular (otologic) 5656
Brainstem/Cerebellum (central)Brainstem/Cerebellum (central) 2222Brainstem/Cerebellum (central)Brainstem/Cerebellum (central) 2222
Proprioceptive (peripheral neuropathy)Proprioceptive (peripheral neuropathy) 77
VisualVisual 11
PsychologicalPsychological 33
UnknownUnknown 1414
NonNon--Vestibular DizzinessVestibular Dizziness
Anxiety Disorders/Panic DisordersAnxiety Disorders/Panic Disorders
Generalized Anxiety: persistent unrealistic Generalized Anxiety: persistent unrealistic worry with motor tension, autonomic worry with motor tension, autonomic hyperactivity apprehension for greaterhyperactivity apprehension for greaterhyperactivity, apprehension for greater hyperactivity, apprehension for greater than 6 monthsthan 6 months
Panic Attack: Discrete spells of intense Panic Attack: Discrete spells of intense fear or discomfort that develops abruptly fear or discomfort that develops abruptly and peaks in 10 minutesand peaks in 10 minutes
Orthostatic HypotensionOrthostatic Hypotension
Another cause of positional Another cause of positional ““dizzinessdizziness””
May be the only cause of positional May be the only cause of positional dizziness or may be acting in conjunction dizziness or may be acting in conjunction with BPPVwith BPPVwith BPPVwith BPPV
Requires measurement of blood pressure Requires measurement of blood pressure and heart rate, after: and heart rate, after:
at least 10 minutes supine restat least 10 minutes supine rest
immediately standing (not sitting)immediately standing (not sitting)
standing for 3 minutesstanding for 3 minutes
Cervicogenic DizzinessCervicogenic Dizziness Controversial diagnosisControversial diagnosis
Dizziness resulting from disruption or Dizziness resulting from disruption or alterations in cervical afferent signals to alterations in cervical afferent signals to vestibular nuclei (i.e. cervical vestibular nuclei (i.e. cervical ((proprioceptors)proprioceptors)
Suspected after cervical trauma, whiplash Suspected after cervical trauma, whiplash injuries.injuries.
Diagnosis made by exclusion: all other dx Diagnosis made by exclusion: all other dx ruled out first + clinical testsruled out first + clinical tests

3
Secondary ProblemsSecondary Problems
Cervical Dysfunction Cervical Dysfunction –– loss of ROM, loss of ROM, tension headaches, paintension headaches, pain
DeconditioningDeconditioning DeconditioningDeconditioning
AnxietyAnxiety
Loss of confidence/ social withdrawalLoss of confidence/ social withdrawal
Handicap:Handicap:Inability to perform ADL/IADLInability to perform ADL/IADL’’ss
Bathing and showeringBathing and showering
ShoppingShopping
Cleaning/ Household ChoresCleaning/ Household Chores
Dizziness QuestionnaireDizziness Questionnaire
Refer to handoutRefer to handout
Questions to PonderQuestions to Ponder
Is this vertigo?Is this vertigo?
Does this problem sound vestibular?Does this problem sound vestibular?
Could this be BPPV (Benign Could this be BPPV (Benign ParoxsysmalParoxsysmal Positional Vertigo)?Positional Vertigo)?
Should I refer to an MD ?Should I refer to an MD ?
Common Vestibular Common Vestibular ComplaintsComplaints
Vertigo or DizzinessVertigo or Dizziness
ImbalanceImbalance
Blurred visionBlurred vision
NauseaNausea
Hearing changesHearing changes
VertigoVertigo
The The illusionillusion of movement, of self or the of movement, of self or the world moving (can be rotational or linear)world moving (can be rotational or linear)
Often described as a spinning sensationOften described as a spinning sensation
C b d t l f f ti ( tib lC b d t l f f ti ( tib l Can be due to loss of function (vestibular Can be due to loss of function (vestibular neuronitis) or mechanical problems neuronitis) or mechanical problems (BPPV)(BPPV)
common in peripheral lesions, more rare in common in peripheral lesions, more rare in central lesionscentral lesions

4
Peripheral vs. Central VertigoPeripheral vs. Central Vertigo
PeripheralPeripheral CentralCentral
OnsetOnset SuddenSudden Slow, gradualSlow, gradualIntensityIntensity SevereSevere Ill definedIll definedDurationDuration ParoxysmalParoxysmal ConstantConstantNausea/DiaphoresisNausea/Diaphoresis FrequentFrequent InfrequentInfrequent
CNS signsCNS signs AbsentAbsent Usually presentUsually presentTinnitus/hearing lossTinnitus/hearing loss Can be presentCan be present AbsentAbsent
NystagmusNystagmus Torsional/horizontalTorsional/horizontal VerticalVerticalNystagmusNystagmus FatigableFatigable NonNon--fatigablefatigable
Watch out for Atypical Watch out for Atypical ComplaintsComplaints
““II’’m feeling like Im feeling like I’’m going to pass outm going to pass out””
““II’’m not dizzy just nauseated when I lie m not dizzy just nauseated when I lie down on my left sidedown on my left side””
““I feel swimmy headed…heavy I feel swimmy headed…heavy headed...lightheaded…hung overheaded...lightheaded…hung over””
““I get this pressure in the back of my I get this pressure in the back of my headhead””
““ I fall when I try to get upI fall when I try to get up””
Nausea and VomitingNausea and Vomiting
Usually accompanies vertigoUsually accompanies vertigo
Due to stimulation of the medulla Due to stimulation of the medulla (autonomic centers)(autonomic centers)(autonomic centers)(autonomic centers)
Usually mild in peripheral lesions and Usually mild in peripheral lesions and in proportion to the degree of vertigo in proportion to the degree of vertigo (symptoms vary in central lesions)(symptoms vary in central lesions)
DysequilibriumDysequilibrium
Imbalance or unsteadiness while Imbalance or unsteadiness while standing or walking standing or walking can be due to many factors perceptual, can be due to many factors perceptual,
sensory and/or motor dysfunctionsensory and/or motor dysfunction
Commonly mistaken for or referred to Commonly mistaken for or referred to as as ““dizzinessdizziness””
OscillopsiaOscillopsia
Blurred visionBlurred vision happens when having nystagmus or happens when having nystagmus or
with head motions (retinal slip) due to with head motions (retinal slip) due to l i i d VOR (i bil t ll i i d VOR (i bil t lseverely impaired VOR (i.e. bilateral severely impaired VOR (i.e. bilateral
vestibular loss)vestibular loss)
Oscillopsia is a subjective illusion of Oscillopsia is a subjective illusion of visual motion (occurs with eyes open visual motion (occurs with eyes open not closed)not closed)
Motion SensitivityMotion Sensitivity
Abnormal or increased sensitivity to Abnormal or increased sensitivity to motion (head/body or visual motion) motion (head/body or visual motion) leading to vertigo, leading to vertigo, ““dizzinessdizziness””, , nauseanausea
Common after acute peripheral Common after acute peripheral lesions (may persist)lesions (may persist)
Common in central lesionsCommon in central lesions

5
Most Common Vestibular Most Common Vestibular DisorderDisorder
BPPVBPPVBPPVBPPV
A Mechanical ProblemA Mechanical Problem
Benign Paroxysmal Benign Paroxysmal Positional VertigoPositional Vertigo
The The most commonmost common cause of cause of vertigo due to a peripheral disordervertigo due to a peripheral disorder
Dissecting BPPVDissecting BPPV
BenignBenign having no significant effect having no significant effect
yet for those who suffer from BPPV it yet for those who suffer from BPPV it can be severe frightening and disablingcan be severe frightening and disablingcan be severe, frightening and disablingcan be severe, frightening and disabling
ParoxysmalParoxysmal a sudden attack of symptomsa sudden attack of symptoms
episodes of vertigo due to BPPV tend to episodes of vertigo due to BPPV tend to be very brief, <60 secondsbe very brief, <60 seconds
Dissecting BPPVDissecting BPPV
PositionalPositional occurs with change in head occurs with change in head
position s ch asposition s ch asposition, such as:position, such as:
Lying downLying down Rolling overRolling over
Bending overBending over Looking up or downLooking up or down
Turning head right or leftTurning head right or left
Dissecting BPPVDissecting BPPV
VertigoVertigo an illusion of motionan illusion of motion
““The room is spinningThe room is spinning””
Many Other DescriptionsMany Other Descriptions
RockingRocking TiltingTilting
Somersaulting Somersaulting Imbalance or fallingImbalance or fallingNauseaNausea Riding an elevator Riding an elevator
down down
Clinical Presentation of BPPVClinical Presentation of BPPV
Classically, symptoms are:Classically, symptoms are:
Sudden in onsetSudden in onset
Typically brief but intense, lasting only Typically brief but intense, lasting only
secondsseconds
Triggered by rapid head movementTriggered by rapid head movement
Often associated with nausea, possibly Often associated with nausea, possibly
vomiting vomiting
Often result in self limiting activitiesOften result in self limiting activities

6
Clinical Presentation of BPPVClinical Presentation of BPPV
Commonly described triggers include:Commonly described triggers include:
lying down or rolling in bed, sitting up lying down or rolling in bed, sitting up
from supine, bending over, turning head from supine, bending over, turning head
d l kid l kiand looking upand looking up
Sense of light headedness and Sense of light headedness and
imbalance may persist after vertigoimbalance may persist after vertigo
Clinical Presentation of BPPVClinical Presentation of BPPV
Between attacks patient may have no Between attacks patient may have no symptoms, if there is no other symptoms, if there is no other vestibular pathologyvestibular pathology
Attacks often occur in clusters that Attacks often occur in clusters that may take placer over several days to may take placer over several days to monthsmonths
Benign Paroxysmal Positional Benign Paroxysmal Positional VertigoVertigo
CANALITHIASIS CANALITHIASIS (most common)(most common)
Degenerative debris from the utricle Degenerative debris from the utricle breaks off and isbreaks off and is freefree--floatingfloating in thein thebreaks off and is breaks off and is freefree--floatingfloating in the in the SCCSCC
Debris moves to the dependent part of Debris moves to the dependent part of the canal, moves the the canal, moves the endolymphendolymph and and causes causes cupularcupular deflectiondeflection
Benign Paroxysmal Positional Benign Paroxysmal Positional VertigoVertigo
CANALITHIASISCANALITHIASIS Vertigo/ NystagmusVertigo/ Nystagmus
latency to onset 1latency to onset 1--40 seconds40 seconds
disappears within 60 secondsdisappears within 60 seconds
Posterior canal BPPV is by far the most Posterior canal BPPV is by far the most common variantcommon variant
Benign Paroxysmal Positional Benign Paroxysmal Positional VertigoVertigo
CUPULOLITHIASISCUPULOLITHIASIS
cellular debris adheres to the cupula of the cellular debris adheres to the cupula of the posterior (or other canal)posterior (or other canal)posterior (or other canal)posterior (or other canal)
Makes the cupula Makes the cupula ““heavyheavy””, causing , causing cupular deflection and persistent vertigo, cupular deflection and persistent vertigo, in certain head positions. in certain head positions.
Mechanism of BPPVMechanism of BPPV

7
PhysiologyPhysiology
In a normal situation:In a normal situation:
head turns right head turns right →→ endolymph moves endolymph moves →→
SCC receptors fire SCC receptors fire ►►head is turning righthead is turning right
head stops head stops →→ endolymph stops endolymph stops →→ SCC SCC
receptors stop receptors stop ►►head has stoppedhead has stopped
Pathophysiology of BPPVPathophysiology of BPPV
stop turning head stop turning head →→ otoliths keep moving otoliths keep moving
→→ endolymph keeps moving endolymph keeps moving →→ receptors receptors
keep firing keep firing ►► head STILL movinghead STILL moving
eyes eyes ►► head is NOT movinghead is NOT moving
brain brain ►► room MUST be spinningroom MUST be spinning
Risk Factors for BPPVRisk Factors for BPPV
Increased age (idiopathic)Increased age (idiopathic)
Head trauma (young)Head trauma (young) Head trauma (young)Head trauma (young)
Preceding viral infectionPreceding viral infection
Post surgicalPost surgical
Variations of BPPVVariations of BPPV
Posterior CanalPosterior Canal
Lateral CanalLateral Canal atypical, accounting atypical, accounting yp , gyp , g
for about 3for about 3--12 12 percentpercent
Anterior CanalAnterior Canal rare, accounting for rare, accounting for
only about 2%only about 2%
DixDix--Hallpike TestHallpike Test
Upbeating Torsional NystagmusUpbeating Torsional Nystagmus

8
Upbeating Torsional NystagmusUpbeating Torsional Nystagmus
Downbeating Torsional NystagmusDownbeating Torsional Nystagmus
Horizontal NystagmusHorizontal Nystagmus
Horizontal NystagmusHorizontal Nystagmus
““So, YouSo, You’’ve Got Rocks in Your ve Got Rocks in Your HeadHead””
Treatment of BPPVTreatment of BPPV

9
Canalith Repositioning Canalith Repositioning TechniquesTechniques
Easy to performEasy to perform
High success rate in one treatmentHigh success rate in one treatment
Traditionally postTraditionally post--maneuver instructions maneuver instructions were given, latest research suggests not were given, latest research suggests not necessary.necessary.
Canalith Repositioning Canalith Repositioning TechniquesTechniques
A specific maneuvers used to treat BPPV A specific maneuvers used to treat BPPV by moving the debris back into the utricle by moving the debris back into the utricle by placing the patient head through a by placing the patient head through a series of positions.series of positions.
Different maneuvers exist for different Different maneuvers exist for different canalscanals
Different maneuvers depending on type of Different maneuvers depending on type of BPPV: canalithiasis vs cupulolithiasis.BPPV: canalithiasis vs cupulolithiasis.
Canalith Repositioning Canalith Repositioning TreatmentTreatment
Canalith Repositioning Canalith Repositioning ManeuverManeuver
Canalith Repositioning Canalith Repositioning TreatmentTreatment
Contraindications/ PrecautionsContraindications/ Precautions ::
known vertebrobasilar insufficiencyknown vertebrobasilar insufficiency
severe cervical / lumbar disease or traumasevere cervical / lumbar disease or trauma
history of rheumatoid arthritishistory of rheumatoid arthritis
unstable heart diseaseunstable heart disease
high grade carotid stenosishigh grade carotid stenosis
active neurological signs (TIA/stroke)active neurological signs (TIA/stroke)
Other Treatment OptionsOther Treatment Options
Semont (Liberatory)Semont (Liberatory)
Liberatory for Horizontal Canal Liberatory for Horizontal Canal yy((CanalithiasisCanalithiasis))
Modified Semont for Horizontal Canal Modified Semont for Horizontal Canal (Cupulolithiasis)(Cupulolithiasis)

10
Common Dysfunction # 2Common Dysfunction # 2
VESTIBULAR VESTIBULAR HYPOFUNCTIONHYPOFUNCTIONHYPOFUNCTIONHYPOFUNCTION
Peripheral LesionsPeripheral Lesions
Loss of FunctionLoss of Function
1) Acute1) Acute-- unilateral( UVL) unilateral( UVL)
bilateral( BVL)bilateral( BVL)
2) Progressive2) Progressive-- ( UVL) ( UVL)
( BVL)( BVL)
3) Episodic 3) Episodic
Specific Vestibular LesionsSpecific Vestibular Lesions
2 Main Divisions: Peripheral and Central2 Main Divisions: Peripheral and Central
Peripheral: membranous labyrinth and Peripheral: membranous labyrinth and vestibular nerve.vestibular nerve.
C t l b i t ( tib l l i)C t l b i t ( tib l l i) Central: brainstem( vestibular nuclei), Central: brainstem( vestibular nuclei), cerebellum and vestibular cortexcerebellum and vestibular cortex
Peripheral vs CentralPeripheral vs Central
Peripheral VestibularPeripheral Vestibular Central VestibularCentral Vestibular
BPPVBPPV MigraineMigraine
MeniereMeniere’’s diseases disease CVA/TIACVA/TIA
Ototoxicity Ototoxicity TBITBI
Vestibular neuronitisVestibular neuronitis Multiple sclerosis Multiple sclerosis
Acoustic neuromaAcoustic neuroma
General CharacteristicsGeneral Characteristics
PERIPHERALPERIPHERAL: nystagmus,vertigo, n&v : nystagmus,vertigo, n&v (mild to mod),dysequilibrium(acutely). (mild to mod),dysequilibrium(acutely). After several weeks: dysequilibrium, After several weeks: dysequilibrium,
ti iti it ill i ith f tti iti it ill i ith f tmotion sensitivity,oscillopsia with fast motion sensitivity,oscillopsia with fast head motion.head motion.
CENTRALCENTRAL: may/may not have vertigo, : may/may not have vertigo, nystagmus, lateropulsion/tilt, oculomotor nystagmus, lateropulsion/tilt, oculomotor abnormalities, motion sensitivity( may abnormalities, motion sensitivity( may be severe)be severe)
Peripheral Lesions (Unilateral)Peripheral Lesions (Unilateral)ACUTE LOSS OF FUNCTION (UVL)ACUTE LOSS OF FUNCTION (UVL)
Vestibular neuritis/Vestibular neuritis/labyrinthitislabyrinthitis: : infection( viral or bacterial) resulting in infection( viral or bacterial) resulting in vertigo, vertigo, N&V,severeN&V,severe symptoms last 3symptoms last 3--4 4
daysdaysdaysdays
gradual resolution of symptoms( several gradual resolution of symptoms( several weeks) May c/o dizziness/vertigo with weeks) May c/o dizziness/vertigo with head movement, head movement, dysequilibriumdysequilibrium, motion , motion sensitivitysensitivity

11
Peripheral Lesion (Bilateral)Peripheral Lesion (Bilateral)ACUTE LOSS OF FUNCTION (BVL)ACUTE LOSS OF FUNCTION (BVL)
Bilateral Vestibular Loss (Ototoxicity):Bilateral Vestibular Loss (Ototoxicity):Complete loss of vestibular function, Complete loss of vestibular function, complete destruction of hair cells due to complete destruction of hair cells due to pptreatment with certain antibiotics that treatment with certain antibiotics that are ototoxic Ex: gentamicin, are ototoxic Ex: gentamicin, streptomicinstreptomicin
No vertigo, but severe dysequilibrium, No vertigo, but severe dysequilibrium, oscillopsia, gait dysfunction.oscillopsia, gait dysfunction.
Peripheral Lesions (Unilateral)Peripheral Lesions (Unilateral)PROGRESSIVE LOSS PROGRESSIVE LOSS
Acoustic NeuromaAcoustic Neuroma: progressive : progressive unilateral hearing loss, tinnitus and unilateral hearing loss, tinnitus and
mild dysequilibrium (vertigo in <20 % of mild dysequilibrium (vertigo in <20 % of ))cases) cases)
Usually benign tumor (schwann cells) Usually benign tumor (schwann cells) arising from vestibular nerve. If not arising from vestibular nerve. If not discovered may encroach on the discovered may encroach on the brainstem/cerebellum (central lesion)brainstem/cerebellum (central lesion)
Peripheral Lesions (Bilateral)Peripheral Lesions (Bilateral)PROGRESSIVE LOSSPROGRESSIVE LOSS
IdiopathicIdiopathic: Unknown cause: Unknown cause
Sequential unilateral lossSequential unilateral loss: had UVL in : had UVL in the past and now have the other ear the past and now have the other ear affectedaffectedaffected.affected.
Progressive dysequilibrium and severe Progressive dysequilibrium and severe oscillopsia, gait dysfunction.oscillopsia, gait dysfunction.
Peripheral Lesions( Unilateral)Peripheral Lesions( Unilateral)EPISODIC VESTIBULAR LOSSEPISODIC VESTIBULAR LOSS
Meniere's DiseaseMeniere's Disease: spells of aural : spells of aural fullness, fluctuating hearing loss, fullness, fluctuating hearing loss, tinnitus and vertigo lasting minutes to tinnitus and vertigo lasting minutes to hourshourshours.hours.
Increased volume of endolymph, Increased volume of endolymph, rupture of membranes separating rupture of membranes separating endolymph from perilymph.endolymph from perilymph.
PatientPatient’’s are usually asymptomatic s are usually asymptomatic between spells, in later stages may between spells, in later stages may present with UVLpresent with UVL
Peripheral Lesions (Unilateral)Peripheral Lesions (Unilateral)EPISODIC VESTIBULAR LOSSEPISODIC VESTIBULAR LOSS
PerilymphaticPerilymphatic FistulaFistula: spells of vertigo, : spells of vertigo, dysequilibriumdysequilibrium and hearing loss brought and hearing loss brought on by straining/exertion and loud on by straining/exertion and loud noises. noises.
Associated with Associated with barotraumabarotrauma, head , head trauma. May have residual trauma. May have residual dysequilibriumdysequilibrium and motion sensitivity.and motion sensitivity.
Controversial diagnosis: leak of Controversial diagnosis: leak of perilymphperilymph into the middle earinto the middle ear
RememberRemember
The ONLY type of episodic vertigo we can The ONLY type of episodic vertigo we can t t i BPPVt t i BPPVtreat is BPPV.treat is BPPV.

12
Another Look at NystagmusAnother Look at Nystagmus
Pathological NystagmusPathological Nystagmus
Can appear Can appear ““spontaneouslyspontaneously”” with a with a sudden loss of vestibular activity from one sudden loss of vestibular activity from one side .side .
can be induced in patients with gaze( can be induced in patients with gaze( gaze gaze --evoked) or head position( positional evoked) or head position( positional nystagmus).nystagmus).
Pathological NystagmusPathological Nystagmus
Named by the quick phase( although the Named by the quick phase( although the vestibular system drives the slow phase of vestibular system drives the slow phase of nystagmus)nystagmus)
Can be upbeating downbeating rightCan be upbeating downbeating right Can be upbeating, downbeating, right Can be upbeating, downbeating, right beating, left beating, torsional etc…beating, left beating, torsional etc…
EX: right vestibular lesion EX: right vestibular lesion
seen in both peripheral and central lesionsseen in both peripheral and central lesions
Horizontal NystagmusHorizontal Nystagmus
Properties of Peripheral Properties of Peripheral Vestibular NystagmusVestibular Nystagmus
Increases with visual fixation blocked ( Increases with visual fixation blocked ( Frenzel lenses)Frenzel lenses)
B t f th l i ( R l i LB t f th l i ( R l i L Beats away from the lesion ( R lesion = L Beats away from the lesion ( R lesion = L beating nystagmus), increases when beating nystagmus), increases when looking away from lesion side. 3) looking away from lesion side. 3) Disappears within 24 hoursDisappears within 24 hours
Central NystagmusCentral Nystagmus
Persists, not increased with visual fixation Persists, not increased with visual fixation blocked ( Frenzel lenses on)blocked ( Frenzel lenses on)
Often vertical ( persistent down beating)Often vertical ( persistent down beating)
If iti l ill t f tiIf iti l ill t f ti If positional will not fatigueIf positional will not fatigue
13
Upbeating NystagmusUpbeating Nystagmus
Downbeating NystagmusDownbeating Nystagmus
VOR ImpairmentVOR Impairment
Oscillopsia in some patients can Oscillopsia in some patients can be attributed to a failure of the be attributed to a failure of the vestibulovestibulo--ocular reflex (VOR) to ocular reflex (VOR) to compensate for head movements compensate for head movements
Without the stabilizing effect of Without the stabilizing effect of the VOR, head perturbations can the VOR, head perturbations can result in retinal slip, which result in retinal slip, which significantly alters visual acuitysignificantly alters visual acuity
How The World Would Appear How The World Would Appear Without VOR Function Without VOR Function
VOR TestingVOR Testing
2 Quick Tests for VOR:2 Quick Tests for VOR:
Head ThrustHead Thrust: Positive test(+) is a : Positive test(+) is a refixationrefixation of eyes after head thrust(of eyes after head thrust(refixationrefixation of eyes after head thrust( of eyes after head thrust( corrective saccade). Indicates corrective saccade). Indicates decreased VOR on the side that this decreased VOR on the side that this occurs. occurs.
VOR TestingVOR Testing
DVA (Dynamic Visual Acuity) TestDVA (Dynamic Visual Acuity) Test: :
tests the difference between static and tests the difference between static and dynamic visual acuity. dynamic visual acuity.
t t i h d i l itt t i h d i l it + test is when a person drops visual acuity + test is when a person drops visual acuity with head moving at 2 Hz (2 cycles per with head moving at 2 Hz (2 cycles per second)second)
22--3 lines (unilateral vestibular deficit) 3 lines (unilateral vestibular deficit)
5 lines or more (bilateral vestibular deficit)5 lines or more (bilateral vestibular deficit)

14
Arriving at a PT DiagnosisArriving at a PT Diagnosis
Diagnosis by ImpairmentDiagnosis by Impairment
VOR hypofunction: gaze stabilization VOR hypofunction: gaze stabilization problemproblem
M h i l P bl ( BPPV)M h i l P bl ( BPPV) Mechanical Problem ( BPPV)Mechanical Problem ( BPPV)
Balance DeficitBalance Deficit
TreatmentTreatment
Components of Vestibular Rehabilitation Components of Vestibular Rehabilitation Common Peripheral Vestibular DisordersCommon Peripheral Vestibular Disorders
1) Canalith repositioning1) Canalith repositioning-- for BPPVfor BPPV
2) V tib l Ad t ti2) V tib l Ad t ti f i i d VORf i i d VOR2) Vestibular Adaptation2) Vestibular Adaptation-- for impaired VORfor impaired VOR
3) Compensation/ Substitution3) Compensation/ Substitution-- for bilateral for bilateral lossloss
4) Balance Training4) Balance Training-- for balance deficitfor balance deficit
AdaptationAdaptationADAPTATIONADAPTATION
Def:LongDef:Long-- term term change within neuronschange within neuronsin response to an input.in response to an input.
Exercises that improve gaze Exercises that improve gaze p gp gstabilization by improving the VOR ( stabilization by improving the VOR ( VOR Gain)VOR Gain)
Research shows that after a unilateral Research shows that after a unilateral vestibular loss there is some limited vestibular loss there is some limited cellular recovery but adaptation must cellular recovery but adaptation must occur.occur.
AdaptationAdaptation
Stimulus to induce adaptation is called Stimulus to induce adaptation is called ““retinal slip.retinal slip.””
Cerebellum : important role in adaptation.Cerebellum : important role in adaptation.
Detects the error signal ( retinal slip) and Detects the error signal ( retinal slip) and adjusts the gain of the VOR.adjusts the gain of the VOR.
AdaptationAdaptation
Adaptation is context specific: speed Adaptation is context specific: speed dependent and position dependent.dependent and position dependent.
Research indicates that it takes at least Research indicates that it takes at least 1 5 minutes of movement with sufficient1 5 minutes of movement with sufficient1.5 minutes of movement with sufficient 1.5 minutes of movement with sufficient head speed in order for adaptation head speed in order for adaptation exercises to work.exercises to work.
Example: VORX1Example: VORX1
VORX2VORX2
Indications for Adaptation Indications for Adaptation ExerciseExercise
IndicationsIndications
1) + complaints of blurred vision/ oscillopsia1) + complaints of blurred vision/ oscillopsia
2) + DVA test 2) + DVA test
3) + head thrust test3) + head thrust test
4) + motion sensitivity to horizontal/vertical 4) + motion sensitivity to horizontal/vertical head rotation.head rotation.
5) UVL>BVL>CENTRAL5) UVL>BVL>CENTRAL
15
Contraindications for Adaptation Contraindications for Adaptation ExerciseExercise
1) Poor vision/ blindness1) Poor vision/ blindness
2) Severe cervical dysfunction or c/o pain 2) Severe cervical dysfunction or c/o pain d it difi tid it difi tidespite modifications.despite modifications.
Compensation/Substitution Compensation/Substitution ExercisesExercises
Def: promoting the use of an alternative Def: promoting the use of an alternative strategy or compensation for deficits that strategy or compensation for deficits that are irreversible.are irreversible.I di d i bil l l i hI di d i bil l l i h Indicated in severe bilateral loss with no Indicated in severe bilateral loss with no remaining vestibular function.remaining vestibular function.
Exercises to promote use of cervical Exercises to promote use of cervical ocular reflexes, eye and head movements, ocular reflexes, eye and head movements, imaginary targets .imaginary targets .
Balance exercises/Education Balance exercises/Education
Expected Outcomes: Unilateral Expected Outcomes: Unilateral Vestibular LesionsVestibular Lesions
After full compensation ( vestibular rehab )After full compensation ( vestibular rehab ) 90 % of patient rate themselves as no 90 % of patient rate themselves as no
disability or mild disability.disability or mild disability. May have persistent gaze stability problemMay have persistent gaze stability problem May have persistent gaze stability problem May have persistent gaze stability problem
( VOR to rapid head movements( VOR to rapid head movements Expect near normal balance and gait.Expect near normal balance and gait. Minor residual symptoms, full recovery 3Minor residual symptoms, full recovery 3--6 6
months.months.
Expected Outcomes: Bilateral Expected Outcomes: Bilateral Vestibular LesionsVestibular Lesions
Expect a considerable amount of Expect a considerable amount of improvement but will recover more slowly.improvement but will recover more slowly.
Will always have some deficits: slower Will always have some deficits: slower gait risk for fallsgait risk for fallsgait, risk for falls.gait, risk for falls.
Bad prognosis if other sensory systems Bad prognosis if other sensory systems are affected( vision, somatosensory)are affected( vision, somatosensory)
Expected Outcomes: Central Expected Outcomes: Central LesionsLesions
Variable results with vestibular rehab Variable results with vestibular rehab depending on areas involved.depending on areas involved.
L tiL ti Longer recovery time Longer recovery time
VESTIBULAR LABVESTIBULAR LAB
16
Essential Components of Essential Components of Clinical ExamClinical Exam
DIZZINESS HISTORYDIZZINESS HISTORY
CENTRAL SCREENINGCENTRAL SCREENING
RULE OUT BPPVRULE OUT BPPV
TEST FOR VOR FUNCTIONTEST FOR VOR FUNCTION
LAB # 1LAB # 1
OcculomotorOcculomotor Exam/ Central ScreeningExam/ Central Screening
Observe for nystagmusObserve for nystagmus
Smooth pursuit testSmooth pursuit test
Saccade TestSaccade Test
VBI TestVBI Test
OcculomotorOcculomotor Exam (Central Exam (Central Screening Tests)Screening Tests)
Screening for central vestibular problems Screening for central vestibular problems such as lesions in the:such as lesions in the: CerebellumCerebellum ParietoParieto--occipital cortexoccipital cortexpp PonsPons
Smooth Pursuit Smooth Pursuit Saccade TestSaccade Test
Clinical ExamClinical Exam
OcculomotorOcculomotor Exam:Exam:
Observe for spontaneous nystagmus, Observe for spontaneous nystagmus, gaze holding nystagmus.gaze holding nystagmus.
PRACTICEPRACTICE PRACTICE PRACTICE
Smooth PursuitSmooth Pursuit
Smooth PursuitSmooth Pursuit: Ask patient to follow : Ask patient to follow your finger with their eyes.your finger with their eyes.
*Abnormal test would be saccadic eye *Abnormal test would be saccadic eye movements ( nonmovements ( non fluid jerky eyefluid jerky eyemovements ( nonmovements ( non--fluid jerky eye fluid jerky eye movements, eyes trying to catch up)movements, eyes trying to catch up)
SaccadeTestSaccadeTest
Hold target about 9Hold target about 9--12 inches apart12 inches apart
Vertical , horizontal, and diagonalVertical , horizontal, and diagonal
Note if patient overshoots or undershoots Note if patient overshoots or undershoots th t t d i t th 2th t t d i t th 2the target and requires greater than 2 eye the target and requires greater than 2 eye movements to reach target.movements to reach target.
17
Video #1Video #1
NORMAL SMOOTH PURSUITNORMAL SMOOTH PURSUIT
ABNORMAL SMOOTH PURSUIT: ABNORMAL SMOOTH PURSUIT: Indicates a possible central lesion Indicates a possible central lesion (cerebellum, brainstem, Parkinson’s (cerebellum, brainstem, Parkinson’s disease)disease)
Normal Smooth PursuitNormal Smooth Pursuit
Saccadic Intrusions and Saccadic Intrusions and Abnormal PursuitAbnormal Pursuit
Perform VBI Test/ cervical ROMPerform VBI Test/ cervical ROM
Active then passive cervical ROM testActive then passive cervical ROM test
Quadrant testingQuadrant testing
+ Test for VBI would be dizziness, + Test for VBI would be dizziness, tt d th id th i bl d i ibl d i inystagmus, nystagmus, dysarthriadysarthria, blurred vision., blurred vision.
Liability Issues. Liability Issues.
LAB # 2LAB # 2
BPPV TESTINGBPPV TESTING
Dix Dix -- HallpikeHallpike
Roll TestRoll Test
ModifiedModified--Hallpike (Semont position)Hallpike (Semont position)
HallpikeHallpike--Dix Test for BPPVDix Test for BPPV
Can be done with or without Frenzel LensesCan be done with or without Frenzel Lenses
Patient long sitting on mat, head turned 45 Patient long sitting on mat, head turned 45 toward test eartoward test ear
P ti t i kl d t i ith h dP ti t i kl d t i ith h d Patient quickly moved to supine with head Patient quickly moved to supine with head hanging 20hanging 20--30 degrees in cervical extension30 degrees in cervical extension
Positive test usually includes nystagmus Positive test usually includes nystagmus and patientand patient’’s report of vertigos report of vertigo

18
DixDix--HallpikeHallpike
Roll TestRoll Test Patient is lying on mat with head flexed Patient is lying on mat with head flexed
2020--30 degrees30 degrees
Patient turns head 45 degrees to the right Patient turns head 45 degrees to the right while maintaining flexionwhile maintaining flexion
P iti i h ld f t l t 30 dP iti i h ld f t l t 30 d Position is held for at least 30 secondsPosition is held for at least 30 seconds
Same is repeated with head turned to the Same is repeated with head turned to the leftleft
Positive test presents with horizontal Positive test presents with horizontal nystagmus (usually bilateral) and patientnystagmus (usually bilateral) and patient’’s s report of dizzinessreport of dizziness
Video DemonstrationVideo Demonstration
Positive HallpikePositive Hallpike--DixDix
Upbeating or downbeating nystagmus with Upbeating or downbeating nystagmus with
i li ltorsionaltorsional
Positive Roll TestPositive Roll Test Horizontal nystagmus Horizontal nystagmus –– geotropic vs. geotropic vs.
ageotropicageotropic
VIDEOSVIDEOS
Name that nystagmus?Name that nystagmus?
Upbeating or downbeatingUpbeating or downbeating
right or left horizontalright or left horizontal
geotropic/geotropic/ageotropicageotropic
direction of torsiondirection of torsion
Upbeating Torsional NystagmusUpbeating Torsional Nystagmus
Upbeating Torsional NystagmusUpbeating Torsional Nystagmus

19
Downbeating Torsional NystagmusDownbeating Torsional Nystagmus
Horizontal NystagmusHorizontal Nystagmus
Horizontal NystagmusHorizontal Nystagmus
LAB # 2LAB # 2
BPPV TREATMENTBPPV TREATMENT
Posterior / Anterior CanalsPosterior / Anterior Canals Canalith Repositioning Maneuver Canalith Repositioning Maneuver gg
(Epley)(Epley)
Semont ManeuversSemont Maneuvers
Horizontal CanalHorizontal Canal GufoniGufoni ManeuversManeuvers
Canalith Repositioning Canalith Repositioning TreatmentTreatment
Demonstrations of Treatment Demonstrations of Treatment TechniquesTechniques
Posterior / Anterior CanalsPosterior / Anterior Canals Canalith Repositioning Maneuver Canalith Repositioning Maneuver
(E l )(E l )(Epley)(Epley)
Semont ManeuversSemont Maneuvers
Horizontal CanalHorizontal Canal GufoniGufoni ManeuversManeuvers

20
Lab # 4Lab # 4
VOR TESTINGVOR TESTING
Head Thrust TestHead Thrust Test
Dynamic Visual Acuity Test ( DVA Test)Dynamic Visual Acuity Test ( DVA Test)
VOR TestingVOR Testing
2 Quick TESTS for VOR:2 Quick TESTS for VOR:
Head ThrustHead Thrust: Positive test(+) is a : Positive test(+) is a refixationrefixation of eyes after head thrust(of eyes after head thrust(refixationrefixation of eyes after head thrust( of eyes after head thrust( corrective saccade). Indicates corrective saccade). Indicates decreased VOR on the side that this decreased VOR on the side that this occurs. occurs.
VOR TestingVOR Testing
DVA (Dynamic Visual Acuity) TestDVA (Dynamic Visual Acuity) Test: :
tests the difference between static and tests the difference between static and dynamic visual acuity. dynamic visual acuity.
t t i h d i l itt t i h d i l it + test is when a person drops visual acuity + test is when a person drops visual acuity with head moving at 2 Hz (2 cycles per with head moving at 2 Hz (2 cycles per second)second)
22--3 lines (unilateral vestibular deficit) 3 lines (unilateral vestibular deficit)
5 lines or more (bilateral vestibular deficit)5 lines or more (bilateral vestibular deficit)
Practice Head ThrustPractice Head Thrust
Slow then FastSlow then Fast
By now you should have a good feel for By now you should have a good feel for patientpatient’’s cervical ROM and any limitations s cervical ROM and any limitations and pain that exists BE CAREFUL!and pain that exists BE CAREFUL!and pain that exists. BE CAREFUL!and pain that exists. BE CAREFUL!
Abnormal Head ThrustAbnormal Head Thrust
Practice DVAPractice DVA

21
LAB #5LAB #5
VOR Adaptation : VOR x 1, VOR x2VOR Adaptation : VOR x 1, VOR x2
Compensation/Substitution ExercisesCompensation/Substitution Exercises
Balance trainingBalance training
Example of Adaptation Example of Adaptation ExercisesExercises
VOR x1VOR x1
VOR x 2VOR x 2
Progression Hints:Progression Hints: Increase time FIRST (up to 90 seconds) then Increase time FIRST (up to 90 seconds) then
increase speed.increase speed.
Sitting Sitting --standingstanding-- during balance activitiesduring balance activities
Plain to busy backgroundsPlain to busy backgrounds
Practice VOR AdaptationPractice VOR Adaptation
VOR x 1VOR x 1
VOR x 2VOR x 2
Balance ScreeningBalance Screening
Berg Balance ScaleBerg Balance Scale
Dynamic Gait Index Dynamic Gait Index
Gait observationGait observation
CTSIB (Clinical Test for Sensory CTSIB (Clinical Test for Sensory Interaction and Balance) Interaction and Balance) ““foam and foam and domedome””
Case StudiesCase Studies
BPPV Case 1BPPV Case 1 Mr. SmithMr. Smith 56 yo56 yo malemale
PMHx: HTN, CABGx1, diabetes, CVA 15 PMHx: HTN, CABGx1, diabetes, CVA 15 yrs agoyrs ago
Patient presents to clinic with c/o episodic Patient presents to clinic with c/o episodic ““dizzinessdizziness”” for past weekfor past week
Last Sunday, patient got out of bed and the Last Sunday, patient got out of bed and the room started spinningroom started spinning
Since then he c/o lightheadedness, off Since then he c/o lightheadedness, off balance, and balance, and ““dizzinessdizziness”” when he gets up, when he gets up, turns or tries to work under his truckturns or tries to work under his truck

22
BPPV Case 1BPPV Case 1
Based on simple hx, what do you suspect?Based on simple hx, what do you suspect?
Mr. Smith is not orthostatic, no central Mr. Smith is not orthostatic, no central signs noted, normal smooth pursuit, signs noted, normal smooth pursuit,
ti h d th tti h d th tnegative head thrustnegative head thrust
DixDix--Hallike: left side: no nystagmus or sx Hallike: left side: no nystagmus or sx complaint; right side: upbeating, right complaint; right side: upbeating, right torsional nystagmus observed, significant torsional nystagmus observed, significant c/o dizziness from patientc/o dizziness from patient
BPPV Case 1BPPV Case 1
Diagnosis: BPPV, right posterior canalDiagnosis: BPPV, right posterior canal
Mr. Smith was treated with Canalith Mr. Smith was treated with Canalith Repositioning ManeuverRepositioning Maneuver
ReRe--test right Hallpike: Mr. Smith reprtos test right Hallpike: Mr. Smith reprtos increase symptom complaint, extremely increase symptom complaint, extremely vertiginous, horizontal nystagmus notedvertiginous, horizontal nystagmus noted
Now what?Now what?
BPPV Case 2BPPV Case 2
Mrs. JonesMrs. Jones 88 yo88 yo FemaleFemale
Reports h/o Reports h/o ““dizzinessdizziness”” for past 20 years, for past 20 years,
ever since her first CVAever since her first CVA
PMHx: h/o CVA, ParkinsonPMHx: h/o CVA, Parkinson’’s disease, s disease,
orthostatic hypotensionorthostatic hypotension
Patient c/o lightheadedness, floating Patient c/o lightheadedness, floating
feeling, especially when she gets up from feeling, especially when she gets up from
bedbed
BPPV Case 2BPPV Case 2
She denies sense of spinning, but reports She denies sense of spinning, but reports nausea when shenausea when she’’s lightheaded, and s lightheaded, and occasionally fallsoccasionally falls
BERG: 41/56BERG: 41/56 DGI: 18/2DGI: 18/2 BERG: 41/56BERG: 41/56 DGI: 18/2DGI: 18/2
Orthostatic measures:Orthostatic measures: BPBP HRHR
supinesupine 118/69118/69 8181
standingstanding 92/5892/58 9090
after 3 minutesafter 3 minutes 90/5290/52 9292
BPPV Case 2BPPV Case 2
Is it BPPV?Is it BPPV?
DixDix--HallpikeHallpike
Right side: no Right side: no nystagmusnystagmus observed, no observed, no gg y gy g ,,c/o vertigoc/o vertigo
Left side: no Left side: no nystagmusnystagmus observed, no observed, no vertigo, but c/o nauseavertigo, but c/o nausea
Should you treat for BPPV or not? Or Should you treat for BPPV or not? Or is it just is it just orthostasisorthostasis??
Case Study #3Case Study #3
56 y/o wm with hx of sudden onset of 56 y/o wm with hx of sudden onset of vertigo with severe nausea and vomiting vertigo with severe nausea and vomiting lasting 3 days. Symptoms gradually lasting 3 days. Symptoms gradually resolved but still dizzy( constant) and offresolved but still dizzy( constant) and offresolved but still dizzy( constant) and off resolved but still dizzy( constant) and off balance.balance.
What is history telling us?What is history telling us?

23
Case Study # 3Case Study # 3
What tests would you perform?What tests would you perform?
Case Study # 3Case Study # 3
Test Results :Test Results :
What treatments would you choose?What treatments would you choose?
Case Study # 4Case Study # 4
82 y/o wm with hx of DM and peripheral 82 y/o wm with hx of DM and peripheral neuropathy with progressive imbalance neuropathy with progressive imbalance and falls. No dizziness or vertigo. Afraid to and falls. No dizziness or vertigo. Afraid to walk deconditionedwalk deconditionedwalk, deconditioned.walk, deconditioned.
What does the history imply?What does the history imply?
Case Study # 4Case Study # 4
What tests should you perform?What tests should you perform?
Test Results:Test Results:
Case Study # 4Case Study # 4
What treatment would be a priority for this What treatment would be a priority for this patient ?patient ?
Sample goals ( STG & LTG)Sample goals ( STG & LTG)
Billing codesBilling codes
Thank You !Thank You !
DICUSSIONDICUSSIONDICUSSIONDICUSSION

9/13/2011
1
Vestibular Rehabilitation: Vestibular Rehabilitation: Solutions to CommonSolutions to CommonSolutions to Common Solutions to Common
Dysfunctions Dysfunctions FPTA Annual Conference 2011FPTA Annual Conference 2011
Nicole PrietoNicole Prieto--Lewis MSPT, Dianna Saunders MS, PT, Jodi Lewis MSPT, Dianna Saunders MS, PT, Jodi Liphart PT, DHSc, NCS, Kathy Swanick PT, DPT, OCSLiphart PT, DHSc, NCS, Kathy Swanick PT, DPT, OCS
What’s is like to be dizzyWhat’s is like to be dizzy
www.vestibular.org VEDA
Topics of DiscussionTopics of Discussion
Anatomy, Anatomy, PathophysiologyPathophysiology and Function of and Function of the Vestibular Systemthe Vestibular System Vestibular ComplaintsVestibular Complaints Vestibular ComplaintsVestibular Complaints Vestibular Examination and treatment for Vestibular Examination and treatment for
BPPV and BPPV and HypofunctionHypofunction Interpretation of Interpretation of NystagmusNystagmus Case StudiesCase Studies
9/13/2011
2
Functions of the Vestibular Functions of the Vestibular SystemSystem
Gaze stabilizationGaze stabilization
Postural stabilityPostural stability
Orientation in spaceOrientation in space
The vestibular system is both a sensory and The vestibular system is both a sensory and motor systemmotor system
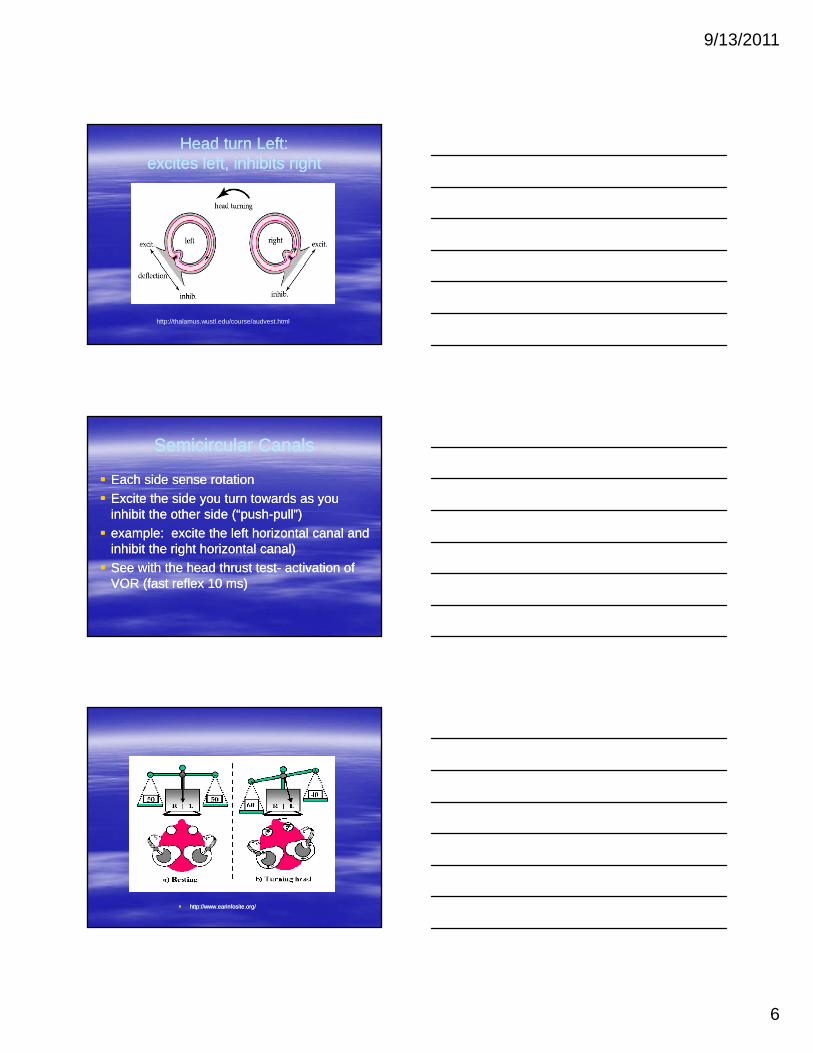
Vestibular System: One Component of the Vestibular System: One Component of the Balance SystemBalance System
http://www.earinfosite.orghttp://www.earinfosite.org
Role of the Vestibular SystemRole of the Vestibular System
4 important roles of vestibular system as it 4 important roles of vestibular system as it relates to postural control/Balance:relates to postural control/Balance:–– Sensation and perception of position and Sensation and perception of position and
motionmotionmotionmotion
–– Role in orienting the head and body to verticalRole in orienting the head and body to vertical
–– Role in controlling position of the body’s COMRole in controlling position of the body’s COM
–– Role in stabilizing head during movementRole in stabilizing head during movement

9/13/2011
3
Structures of the Vestibular Structures of the Vestibular SystemSystem
P i h l S A t (SCCP i h l S A t (SCC Peripheral Sensory Apparatus (SCC, Peripheral Sensory Apparatus (SCC, Otoliths)Otoliths)
Central Processor (vestibular nuclei)Central Processor (vestibular nuclei)
Mechanisms for Motor Output (VOR, VSR)Mechanisms for Motor Output (VOR, VSR)
Peripheral Sensory Peripheral Sensory ApparatusApparatus
3 Semicircular Canals3 Semicircular CanalsB L b i th (fill d ith il h)B L b i th (fill d ith il h)–– Bony Labyrinth (filled with perilymph)Bony Labyrinth (filled with perilymph)
–– Membranous Labyrinth (filled with endolymph)Membranous Labyrinth (filled with endolymph)
2 Otolith Organs2 Otolith Organs–– Saccule (linear acceleration)Saccule (linear acceleration)
–– Utricle (horizontal linear acceleration)Utricle (horizontal linear acceleration)
Hair CellsHair Cells
Herdman, S. Vestibular Rehabilitation FA Davis Co. 1994 p. 5

9/13/2011
4
Semicircular CanalsSemicircular Canals
Herdman, S. Vestibular Rehabilitation FA Davis Co. 1994 p. 5
Semicircular CanalsSemicircular Canals
Detect rotational movement (angular velocity)Detect rotational movement (angular velocity) Most sensitive to faster head movementsMost sensitive to faster head movements Canals are oriented 90 degrees to each otherCanals are oriented 90 degrees to each other The horizontal canal is tilted up 30 degreesThe horizontal canal is tilted up 30 degreesThe horizontal canal is tilted up 30 degreesThe horizontal canal is tilted up 30 degrees “Push“Push--Pull” relationshipPull” relationship The Cupula (gelatinous “sailThe Cupula (gelatinous “sail--like” structure) is like” structure) is
found in the ampulla of each SCCfound in the ampulla of each SCC Hair cells stick up from the Crista ampullaris into Hair cells stick up from the Crista ampullaris into
the Cupula the Cupula
Canal OrientationCanal Orientation

9/13/2011
5
Semicircular Canals:Push/PullSemicircular Canals:Push/Pull
The canals function as coplanar pairs:The canals function as coplanar pairs:–– Right and Left Lateral (horizontal) canalsRight and Left Lateral (horizontal) canals
–– Left Anterior and Right PosteriorLeft Anterior and Right Posterior
L ft P t i d Ri ht A t iL ft P t i d Ri ht A t i–– Left Posterior and Right AnteriorLeft Posterior and Right Anterior
Similar planes to the extraocular musclesSimilar planes to the extraocular muscles
PairingPairing——provides sensory redundancyprovides sensory redundancy
1997 Encyclopaedia Britannica, Inc
Herdman, S. Vestibular Rehabilitation FA Davis Co. 1994 p.6
9/13/2011
6
Head turn Left: Head turn Left: excites left, inhibits right excites left, inhibits right
http://thalamus.wustl.edu/course/audvest.html
Semicircular CanalsSemicircular Canals
Each side sense rotationEach side sense rotation
Excite the side you turn towards as you Excite the side you turn towards as you inhibit the other side (“pushinhibit the other side (“push--pull”)pull”)
example: excite the left horizontal canal and example: excite the left horizontal canal and inhibit the right horizontal canal)inhibit the right horizontal canal)
See with the head thrust testSee with the head thrust test-- activation of activation of VOR (fast reflex 10 ms)VOR (fast reflex 10 ms)
http://www.earinfosite.org/http://www.earinfosite.org/

9/13/2011
7
OtolithsOtoliths
Respond to linear acceleration/gravityRespond to linear acceleration/gravity
Hair cells arise from the Macula and project Hair cells arise from the Macula and project up into the otolithic membraneup into the otolithic membrane
S lS l ti ll i t d d tti ll i t d d t SacculeSaccule: vertically oriented, responds to : vertically oriented, responds to up/down head translationsup/down head translations
UtricleUtricle: horizontally oriented, responds to : horizontally oriented, responds to fore/aft tiltsfore/aft tilts
Curved structures so they respond to linear Curved structures so they respond to linear acceleration in any directionacceleration in any direction
OtoconiaOtoconia
http://www.ncbi.nlm.nih.gov/books/NBK10792/

9/13/2011
8
1997 Encyclopaedia Britannica, Inc
http://weboflife.nasa.gov/currentResearch/currentResearchFlight/adfFlight.htm
http://vestibular.wustl.edu/primer3.html
9/13/2011
9
Central ProcessorCentral Processor
Vestibular Nuclear ComplexVestibular Nuclear Complex
CerebellumCerebellum
Lots of connections!! Vestibular sensory info Lots of connections!! Vestibular sensory info is processed with somatosensory and visual is processed with somatosensory and visual inputinput
Vestibular NucleiVestibular Nuclei
Vestibular Nuclear ComplexVestibular Nuclear Complex
9/13/2011
10
Mechanisms for Motor OutputMechanisms for Motor Output
Output for the VOROutput for the VOR–– ocular motor nucleiocular motor nuclei
Output for the VSROutput for the VSR–– Medial and Lateral vestibulospinal tracts, Medial and Lateral vestibulospinal tracts,
Reticulospinal tractReticulospinal tract
VORVOR
Purpose: maintain stable vision while your Purpose: maintain stable vision while your head in movinghead in moving The The extraocularextraocular muscles are paired with the muscles are paired with the
semicircular canalssemicircular canalssemicircular canalssemicircular canals When you stimulate one canal the eye When you stimulate one canal the eye
movement will be in the same plane as that movement will be in the same plane as that canal: (move head back and to the right will canal: (move head back and to the right will stimulate the right posterior canal and the stimulate the right posterior canal and the eyes depress and rotate left)eyes depress and rotate left) Gain of the VORGain of the VOR
VSRVSR
Maintain/stabilize body postureMaintain/stabilize body posture–– Medial and Lateral Vestibulospinal tractsMedial and Lateral Vestibulospinal tracts To motor neurons in the cervical and lumbar spinal To motor neurons in the cervical and lumbar spinal
cordcordcordcord

9/13/2011
11
CerebellumCerebellum
The adaptive processorThe adaptive processor
Adjusts and maintains the gain of the VORAdjusts and maintains the gain of the VOR
Vascular SupplyVascular Supply
Vascular SupplyVascular Supply
Labyrinth Artery: comes off AICA or BasilarLabyrinth Artery: comes off AICA or Basilar–– Branches into Anterior Vestibular Artery and Branches into Anterior Vestibular Artery and
Posterior Vestibular ArteryPosterior Vestibular Artery
Anterior supplies anterior and lateral SCC andAnterior supplies anterior and lateral SCC and–– Anterior supplies anterior and lateral SCC and Anterior supplies anterior and lateral SCC and utricleutricle
–– Posterior supplies posterior SCC, saccule and Posterior supplies posterior SCC, saccule and part of cochleapart of cochlea

9/13/2011
12
InnervationInnervation
Vestibular Nerve (CN 8)Vestibular Nerve (CN 8)–– 2 Branches2 Branches Superior division: anterior and lateral SCC and utricleSuperior division: anterior and lateral SCC and utricle
Inferior division: posterior SCC and sacculeInferior division: posterior SCC and saccule Inferior division: posterior SCC and sacculeInferior division: posterior SCC and saccule
Vestibular ComplaintsVestibular Complaints
DizzinessDizziness–– Vague term, many causesVague term, many causes
Common symptoms of vestibular disorders: Common symptoms of vestibular disorders: vertigo, imbalance, tilt, nausea/vomiting, vertigo, imbalance, tilt, nausea/vomiting, hearing loss, oscillopsiahearing loss, oscillopsia
Incidence of DizzinessIncidence of Dizziness
Dizziness as reason to see MD:Dizziness as reason to see MD:
1.3% 1.3% age 45age 45--6464
2.9%2.9% age 65 age 65 ––7575
3 83 8 %% age 75 and overage 75 and over 3.83.8 %% age 75 and overage 75 and over
45% due to vestibular disorders45% due to vestibular disorders 1 year prevalence of dizziness as reason to see Family 1 year prevalence of dizziness as reason to see Family
Practice MD for patients 65 and older was 8.3% (increased Practice MD for patients 65 and older was 8.3% (increased with age, women more than men) Maarsingh et al 2010with age, women more than men) Maarsingh et al 2010
9/13/2011
13
Vestibular system and agingVestibular system and aging
Decrease in hair cellsDecrease in hair cells Decrease in vestibular neuronsDecrease in vestibular neurons VOR gain decreasesVOR gain decreases
Thi lt i t ti l li dThi lt i t ti l li d This results in greater retinal slip and poorer This results in greater retinal slip and poorer visual acuity during head movementvisual acuity during head movement Degeneration in otoconia (higher incidence Degeneration in otoconia (higher incidence
of BPPV)of BPPV)
Other systems affected with Other systems affected with agingaging
Visual deficits:Visual deficits:–– Visual acuity, accomodation, smooth pursuits all Visual acuity, accomodation, smooth pursuits all
decrease with agedecrease with age–– Inability to adapt to darkInability to adapt to darky py p
Somatosensory Changes:Somatosensory Changes:–– Decrease in vibration senseDecrease in vibration sense–– Decrease in proprioception of feetDecrease in proprioception of feet–– Increase LE reaction timesIncrease LE reaction times
Older adultOlder adult
Changes in vestibular function is similar to Changes in vestibular function is similar to bilateral vestibular deficit (c/o disequilibrium, bilateral vestibular deficit (c/o disequilibrium, gait ataxia, without vertigogait ataxia, without vertigo More likely to need an assistive deviceMore likely to need an assistive deviceMore likely to need an assistive deviceMore likely to need an assistive device More likely to have difficulty walking in the More likely to have difficulty walking in the
dark (need to increase lighting: use dark (need to increase lighting: use nightlights, flashlights)nightlights, flashlights)

9/13/2011
14
Peripheral Vs. CentralPeripheral Vs. Central
Vestibular Disorder can come from Vestibular Disorder can come from peripheral or central sources peripheral or central sources
Peripheral: dysfunction of the SCC or Peripheral: dysfunction of the SCC or Ot lithOt lith it t l b kit t l b kOtolithsOtoliths or nerve as it travels backor nerve as it travels back
Central: dysfunction of vestibular nuclei, Central: dysfunction of vestibular nuclei, cerebellum or their outputscerebellum or their outputs
The signs and symptoms are differentThe signs and symptoms are different
You made it through the You made it through the Anatomy!Anatomy!
SummarySummary
Now to the “Now to the “good stuff” good stuff”





























