Embed Size (px)
Citation preview

801
Review
www.expert-reviews.com ISSN 1477-9072© 2009 Expert Reviews Ltd 10.1586/ERC.09.69
Ventricular tachycardia & ventricular fibrillationVentricular tachycardia (VT) and ventricular fibrillation (VF) are the most important causes of sudden cardiac death (SCD), particularly in those with structural heart disease and reduced left ventricular function. The most common structural heart disease is chronic ischemic heart disease with a prior history of myo cardial infarc-tion (MI). Nonischemic cardio myopathy is an important group presenting, not infrequently, with life-threatening ventricular arrhythmia. Annually, 300,000 SCDs occur in the USA, accounting for 50% of cardio vascular mortality. Recent advances have facilitated management of these potentially lethal arrhythmias. Advances in the primary prevention of life-threatening ventricular arrhythmia in patients who are at risk but have not experienced an episode have been published [1]. VT may occur infrequently in a structurally normal heart. A structurally normal heart is defined as having a normal ECG, echocardiogram and coronary arterio-gram collectively. With a structurally nor-mal heart, monomorphic VTs are sometimes referred to as idiopathic VTs, with three com-monly cited syndromes:
• Repetitive monomorphic VT
• Paroxysmal sustained VT
• Idiopathic left ventricular VT
They are generally considered to have an excel-lent prognosis. With a structurally normal heart, polymorphic VT or VF may also infrequently occur. Catecholaminergic polymorphic VT hap-pens with a normal QT interval and typically begins in childhood or adolescence.
DefinitionsVentricular tachycardia may be re-entrant, auto-matic or triggered. It can either be monomor-phic or polymorphic. Monomorphic tachycar-dia is usually associated with myocardial scar or areas of conduction block. Polymorphic VT occurs in the presence of acute ischemia or QT prolongation. In the latter instance it is known as ‘torsades de pointes’.
Ventricular tachycardia is clinically divided based on the duration of an individual episode. Sustained VT lasts greater than 30 s, and non-sustained episodes less than that. Wide-QRS tachycardia in a patient with structural heart disease is most likely VT.
Differential diagnoses for wide-QRS tachycardia
• Ventricular tachycardia (most common)
• Supraventricular tachycardia with aberrant ventricular conduction (not uncommon)
• Supraventricular tachycardia with pre-existing bundle-branch block (uncommon)
• Pre-excited tachycardia (rare)
Komandoor Srivathsan, Daniel WC Ng and Farouk Mookadam†
†Author for correspondenceCardiovascular Diseases, Mayo Clinic, 13400 E Shea Blvd, Scottsdale, AZ 85255, USA [email protected]
Ventricular tachycardia and ventricular fibrillation are the most important causes of sudden cardiac death (SCD), particularly in those with structural heart disease and reduced left ventricular function. It is important to distinguish ventricular tachycardia from supraventricular tachycardia. A wide spectrum of ventricular arrhythmias exists, from those where the heart is structurally normal to those with structural heart disease. Each entity has a distinctive pathophysiology, treatment plan and prognostic outcome. Treatment modalities include simple b-blockade to implantation of implantable cardiac defibrillator and ablative approaches. In general, those ventricular arrhythmias associated with a structurally normal heart are more benign than those associated with structural heart disease.
Keywords: ablation • antiarrhythmic drug • implantable defibrillator • ischemic heart disease • nonischemic heart disease • structural heart disease • sudden cardiac death • ventricular tachycardia
Ventricular tachycardia and ventricular fibrillationExpert Rev. Cardiovasc. Ther. 7(7), 801–809 (2009)
For reprint orders, please contact [email protected]

Expert Rev. Cardiovasc. Ther. 7(7), (2009)802
Review Srivathsan, Ng & Mookadam
Diagnosis & initial evaluation of monomorphic VT & VFClinical history and examination are essential in the diagnosis of VT but less so in the diagnosis of VF. History of prior MI, congestive heart failure with systolic dysfunction (ejection frac-tion [EF] < 40%) or cardiomyopathy increase the likelihood VT in the clinical context of regular wide-QRS tachycardia. The observation of cannon ‘a’ waves and variable first heart sound are clinical hallmarks of atrioventricular (AV) dissociation and are highly suggestive of VT.
Hemodynamic stability should not be used to diagnose supra-VT (SVT). Whenever possible, a 12-lead ECG should be obtained for establishing the diagnosis. The criteria for diagnoses are listed in Table 1. The presence of fusion beats, capture beats and AV dissociation are the most important diagnostic criteria that are helpful in differentiating VT from SVT. Various case reports and studies described the proarrhythmia effects of adenosine. Hence, administration of intravenous adenosine to differentiate SVT from VT, thought to be a useful tool, needs to be considered with caution [2–5].
Once the acute situation has been adequately treated, investiga-tions are directed to establish the underlying substrate responsible for the arrhythmia and to identify triggers that led to the clinical presentation. These tests include an echocardiogram to assess the
EF, as well as exposing structural heart disease. Coronary angiog-raphy to evaluate the extent of ischemic heart disease and other noninvasive techniques, such as CT scanning or MRI, to identify myocardial dysplasia [6–9]. Tests are performed sequentially and further testing may be stopped if there is convincing evidence of an etiology. The influences of stunning on left ventricular function resulting from both tachycardia and or ischemia (either direct ischemia or secondary to hypoperfusion as a consequence of tachycardia) have to be considered before planning definitive treatment. Identifying triggers typically includes assessment of cardiac biomarkers and metabolic derangement. Myocardial injury is associated with automatic arrhythmia such as acceler-ated AV rhythm but if there is a pre-existing scar (from prior myocardial injury) the automatic arrhythmia may secondarily precipitate a re-entrant monomorphic VT [10,11].
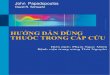
ECG in monomorphic ventricular tachycardiaThe morphologic criteria in support of VT largely depend on exclud-ing normal activation of the intact conducting bundle branch. In right bundle-branch block (RBBB), septal activation from left to right is preserved, and the resultant r-wave is small. If the initial R-wave is larger than R’ then it favors VT [12–14]. Similarly in a typi-cal RBBB, the s wave in V6 is small (Figure 1). If the S-wave is larger than the R-wave, it favors VT. The criteria in left bundle-branch block were also derived on extension of a similar idea.
In wide QRS tachycardia, VT should be the default diagnosis. SVT with aberrancy may be ruled in if specific criteria are met.
Acute managementCardioversion or defibrillation is the first line of management in VT and VF, respectively. Cardioversion for VT is carried out in patients who are hemodynamically unstable. If there is mild-to-moderate hypotension or normal blood pressure, intravenous amiodarone is the preferred drug for both out-of-hospital and in-hospital presentation (Table 2). Amiodarone is the only anti-arrhythmic medication that has been shown to improve survival to hospitalization in patients with out-of-hospital cardiac arrest [15]. The same trial did not have sufficient power to detect survival to hospital discharge. Once resuscitated, patients should undergo risk stratification and receive an implantable cardioverter defibrillator (ICD) if there is a substantial risk of recurrence [16].
Table 1. Criteria for diagnosis.
Criteria VT favored SVT favored
QRS > 140 ms Yes No
Atrioventricular dissociation Yes No
Positive QRS concordance Yes No
Right superior axis (-90° to +180°) Yes No
QRS morphology different from pre-existing bundle branch block
Yes No
History of structural heart disease Yes No
LBBB with right axis Yes No
RS interval in precordial lead > 100 ms
Yes No
LBBB: Left bundle-branch block; SVT: Supraventricular tachycardia; VT: Ventricular tachycardia.
LBBB pattern
R wave in V1 > 30 ms
QR or QSin V6
R to nadirof S wave> 60 ms
RBBB pattern
Amplitude R > R´ in V1
QS or RS(S > R) in V6
Initial deflectionin V1 differentfrom SR
Figure 1. QRS morphology criteria to recognize ventricular tachycardia. LBBB: Left bundle branch block; RBBB: Right bundle branch block.

www.expert-reviews.com 803
ReviewVentricular tachycardia & ventricular fibrillation
Secondary prevention of sudden cardiac deathSurvivors of cardiac arrest have a high risk of recurrence, with an incidence of 20–45% in the ensuing 2 years [17]. Therefore, many trials were conducted to identify whether ICD confers a survival benefit over con-ventional therapy with antiarrhythmic mediation and reduces overall mortality in this high-risk group. Based on the results of these studies, the American College of Cardiology (ACC)/American Heart Association (AHA)/European Society of Cardiology (ESC) guidelines state that sur-vivors of cardiac arrest, VF or sustained VT not caused by a reversible cause with a his-tory of structural heart disease should undergo implantation of an ICD [18]. The studies are outlined in Table 3. It is important to note that more than 80% of patients had coronary artery disease. The data are less than compelling in patients with an EF of more than 40%, but very few patients were randomized. In clinical practice, survivors of VF or cardiac arrest with preserved left ventricular function (EF > 40%) will receive an ICD in most instances. Patients with an ICD may still need antiarrhythmic therapy to control the number ICD shocks. In the Antiarrhythmics versus Implantable Defibrillators (AVID) trial, approximately 10% of patients were receiving amiodarone at 24 months after the ICD implantation. Although only 10% of the patients in the studies had nonischemic cardiomyopathy, these data are used widely in clinical practice to justify implantation of an ICD in survivors of cardiac arrest.
Antiarrhythmic medication in secondary preventionAntiarrhythmic drugs may not be beneficial when directly com-pared with device therapy, but frequently offer a complemen-tary role in the management of patients with an ICD. Drugs reduce the number of shocks by slowing the rate of VT there by
increasing the effectiveness of antitachycardia pacing, a func-tion present in all newer ICDs. Pooled data from European Myocardial Infarct Amiodarone Trial (EMIAT) and Canadian Amiodarone Myocardial Infarction Trial (CAMIAT) support adrenergic modulation with b-blockers and amiodarone, which confer a survival benefit particularly in patients with preserved left ventricular function [19,20]. Sotalol or dofetilide can be used to reduce ICD discharge if there is intolerance or side effects to amiodarone. There is compelling evidence not to use class I antiarrhythmic medication, particularly Ic drugs, such as fle-cainide, propafenone and moriczine, as they have been shown to increase mortality (The Cardiac Arrhythmia Suppression Trial [CAST]) [21,22].
Primary prevention of SCDPrimary prevention of SCD has evolved substantially over the last decade. Landmark trials have been outlined in Table 4. These stud-ies have guided clinical decision-making. The 2006 ACC/AHA/ESC guidelines provided a class I indication (level of evidence A) for prophylactic implantation of an ICD in patients who have post-infarct LV dysfunction and an EF less than or equal to 30–40%,
Table 2. Medication for ventricular tachycardia and fibrillation.
Medication Dosage Precautions
Amiodarone 150 mg intravenously over 10 min if blood pressure is normal or 300 mg (10 min) if mild-to-moderate hypotension is notedMaintenance after: 1 mg/min for 6 h followed by 0.5 mg/min for 18 h
Caution in cardiogenic shock.Use only with pacing if there is marked bradycardia, torsades de pointes is rare.
Lidocaine 1–3 mg/kg at 20–50 mg/min followed by maintenance at 1–4 mg/min depending on response
Reduce dose in heart failure, CNS side effects, such as delirium, paresthesia or seizures may occur.
Procainamide Loading dose: 17 mg/kgMaximum dose per min: 50 mg Maintenance: 1–4 mg/min
Avoid hypotension: if QRS prolongation is greater than 50%, hold medication.
Table 3. Studies of secondary prevention of sudden cardiac death.
Trial Strategy Patients Mean EF (%) Results Ref.
AVID ICD vs medication either amiodarone or sotalol
Total: 1016ICD: 507Medications (predominantly amiodarone): 509 (80% with ischemic heart disease)
32 (inclusion <40) Relative risk reduction:1-year: 39%2-year: 27%3-year: 31%(p = 0.02)
[17]
CIDS ICD vs amiodarone Total: 659ICD: 328Amiodarone: 331 (82% with ischemic heart disease)
<35 Relative risk reduction: 20%(p = 0.142)
[23]
CASH ICD vs amiodarone vs b-blocker
Total: 288 (74% with ischemic heart disease)ICD: 99Amiodarone: 92Metoprolol: 97
~45 Relative risk reduction at 5 years: 23% (p = 0.081)
[24]
AVID: Antiarrhythmics versus Implantable Defibrillators; CASH: Cardiac Arrest Study Hamburg; CIDS: Canadian Implantable Defibrillator Study; ICD: Implantable cardioverter defibrillator.

Expert Rev. Cardiovasc. Ther. 7(7), (2009)804
Review Srivathsan, Ng & Mookadam
Table 4. Trials of primary prevention of sudden cardiac death with implantable cardiac defibrillators.
Trial Strategy Patients EF (%) Outcome Ref.
MADIT I Conventional medical therapy vs ICD in patients with clinical NSVT and inducible VT during EPS that is not suppressible with procainamide
Medical therapy: 101ICD arm: 95
<35 54% RR reduction in mortality in favor of ICD; 95% CI: 0.26–0.82; p = 0.009
[25]
CABG-PATCH CAD patients undergoing CABG with abnormal signal averaged ECG randomized to ICD or control group
ICD epicardial: 446Control arm: 45 Total: 900
<36 No statistically significant reduction of mortality; hazard ratio: 1.07
[26]
MADIT II Patients with history of MI or wall motion abnormality, documented CAD and an EF < 30% (history of MI > 30days and revascularization > 90 days) randomized 3:2 to ICD vs conventional medical therapy
ICD: 42Conventional medical therapy: 490
<30 31% RR reduction in favor of ICD; 95% CI: 0.51–0.93; p = 0.16
[27]
AMIOVIRT Nonischemic dilated cardiomyopathy patients with nonsustained VT, randomized to ICD vs amiodarone
ICD: 51Amiodarone: 52Total: 103
<35 No significant difference in survival [28]
DEFINITE Nonischemic dilated cardiomyopathy patients with nonsustained VT, randomized to ICD vs standard medical therapy
Single-chamber ICD: 229Standard medical therapy: 229Total: 458
<36 Total mortality did not reach statistical significance; p = 0.08. Pre-specified secondary end point arrhythmic mortality showed in favor of ICD; p = 0.006
[29]
COMPANION Biventricular pacemaker with or without a defibrillator will reduce hospitalization and death in advanced heart failure and intraventricular conduction delay (QRS > 120 ms) in both ischemic and nonischemic causes
1520 randomized in 1:2:2 ratio to receive optimum pharmacological therapy, biventricular pacemaker alone or biventricular pacemaker defibrillator
<35 Combined end point of hospitalization and death reduced by the pacemaker alone 34% (p = 0.002) and pacemaker-ICD by 40% (p = 0.001). Secondary end point all cause mortality reduced by defibrillator by RR-36% (p = 0.003) but not by pacemaker alone. RR: 24% (p = 0.059)
[30]
DINAMIT Benefit of an ICD early after an MI within 6–40 days towards reduction of mortality when compared with medical therapy
ICD: 332Control: 342Total: 674
<35 62 deaths in the ICD group and 58 in the control group (p = 0.66; CI: 0.76–1.55). Arrhythmic causes were less in the ICD group but nonarrhythmic causes were significantly higher and thus overall mortality was not significantly different
[31]
SCD-HeFT To assess prognostic effect of ICD vs amiodarone vs placebo in class II and III heart failure regardless of etiology
Conventional therapy and placebo: 847Conventional therapy and amiodarone: 845Conventional therapy and single lead, shock only ICD: 829Total: 2521
<35 (ischemic etiology patients 52% and nonischemic etiology 48%)
Amiodarone and placebo outcome were comparable. ICD arm absolute risk reduction: 7.2% after 5 years;RR: 23% (p = 0.007)
[32]
AMIOVIRT: Amiodarone versus Implantable Defibrillator; CABG: Coronary artery bypass graft; CAD: Coronary artery disease; COMPANION: Comparison of Medical Therapy, Pacing, and Defibrillation in Heart Failure; DEFINITE: Defibrillators in Non-Ischemic Cardiomyopathy Treatment Evaluation; DINAMIT: Defibrillator in Acute Myocardial Infarction Trial; EF: Ejection fraction; EPS: Electrophysiology; ICD: Implantable cardiac defibrillator; MADIT: Multicenter Automatic Defibrillator Implantation Trial; MI: Myocardial infarction; NSVT: Nonsustained ventricular tachycardia; RR: Relative risk; SCD-HeFT: Sudden Cardiac Death in Heart Failure Trial; VT: Ventricular tachycardia.

www.expert-reviews.com 805
ReviewVentricular tachycardia & ventricular fibrillation
who are at least 40 days after an MI and are New York Heart Association (NYHA) class II or III. The class I indication for those with nonischemic cardiomyopathy is also similar with the EF less or equal to 30–35%. In patients who are NYHA class I with EF equal or less than 35%, it is a class IIa indication for prophylactic implantation of an ICD but a class IIb indication for those with nonischemic cardiomyopathy. Biventricular pacing in the absence of ICD therapy in patients with NYHA III or IV heart failure, EF less than 35%, QRS equal to or wider than 160 ms or 120 ms (with other evidence of ventricular dyssynchrony). However, deploying clinical judgment prior to recommending device implantation is always necessary. If the patient is terminally ill from other causes, such as cancer, with less than 1 year of life expectancy, then it may be reasonable to withhold device implantation [18].
VT ablation therapyAlthough the repeated studies have showed that the ICD is superior to no treatment or antiarrhythmic drug treatment in the prevention of sudden death, substantial evidence has accu-mulated, suggesting that the risk of cardiac and sudden death increases with the number of shock treatments. Furthermore, the occurrence of arrhythmia storm (the occurrence of more than three distinct VT episodes, requiring ICD treatment within a 24-h period) is an independent predictor of cardiac mortality. Adjunctive catheter ablation in this setting appears to substan-tially decrease the number of appropriate ICD interventions and to reduce the incidence of cardiac death [33,34]. Radiofrequency ablation therapy is considered a class I recommendation under the following circumstances [18]:
• Frequent shocks from an ICD secondary to VT despite adequate antiarrhythmic therapy
• Patient intolerant of effective antiarrhythmic medication
• Mappable VT and the patient does not want to take medication
With novel imaging modalities and advances in radiofrequency ablation technology, the success rate of radiofrequency ablation VT in large series is 70% with approximately 7% risk of major complications [35,36]. Based on these data, radiofrequency abla-tion is reserved for intractable cases. With introduction of novel mapping approaches and techniques, one may expect improved success rate and a decrease in procedure time [37,38]. Cost–effec-tiveness of catheter ablation in patients with VT with ischemic coronary disease was reviewed and deemed economically attrac-tive (cost–effectiveness ratio of approximately US$21,000 per quality-adjusted life-year) [39].
Bundle branch re-entrant VTThis is a special-type rapid VT, usually with left bundle-branch block morphology that generally occurs with advanced dilated car-diomyopathy, both ischemic and nonischemic [40–43]. In referral centers the reported incidence is 8% of the cases referred for abla-tion [44]. This tachycardia may also occur in valvular cardiomyopa-thy and cardiomyopathy associated with myotonic dystrophy [45,46]. Prolonged HV interval in sinus rhythm is observed in majority of
patients with bundle branch re-entrant VT. This tachycardia is usu-ally due to re-entry within the His–Purkinje conduction system, the vast majority being retrograde over the left bundle branch and ante-grade conduction over right bundle branch [40–43,45]. Characteristics of this arrhythmia include an HV interval during the tachycardia is usually longer than the HV interval during sinus rhythm. It is important to recognize that the differential diagnosis of bundle branch re-entry VT include other types of VTs and various types of SVT with conduction aberrancy. The differential diagnosis can be based on the diagnostic criteria of VT, as well as SVT [47]. In general, pharmacologic therapies are not effective. Radiofrequency catheter ablation of a bundle branch can be curative and considered the therapy of choice. The technique of choice is ablation of the right bundle [41–43]. Long-term prognosis of patients with bundle branch reentry VT depends on their underlying cardiac diseases. Many of these patients have advanced heart failure and ought to be considered for ICD implantation with or without cardiac resynchronization therapy even after successful ablation [7–11].
Idiopathic VTVentricular tachycardia may occur in the absence of structural heart disease (i.e., when the ECG, echocardiogram and coronary angiography are all normal). The common types are right ventric-ular outflow-tract tachycardia and idiopathic verapamil-sensitive left VT. This group of tachycardias may be caused by triggered activity (right ventricular outflow tract tachycardia) or re-entry (left VT) [48]. The most common is right ventricular outflow-tract tachycardia (90%) and is recognized by a left bundle-branch block pattern with an inferior axis during VT [49]. These tachycardias are usually monomorphic in morphology. Isolated recurrent ven-tricular extrasystole may be a manifestation of right ventricular outflow-tract tachycardia [47]. Triggered outflow-tract tachycardias are dependent on cyclic adenosine monophosphate and respond to intravenous adenosine [48,50,51]. Overall, the arrhythmia carries a benign prognosis. Sudden death is rare and ICD is usually not required. Patients usually present with palpitations, presyncope or frank syncope. Physical examination and echocardiography reveal a structurally normal heart. The initial treatment is either b-blockers or verapamil. Although other membrane-active drugs may be useful in an occasional case, radiofrequency ablation is curative in over 90% of cases [52–57]. VT following tetralogy of Fallot repair or mahaim tachycardia and tachycardia secondary to arrhythmogenic right ventricular dysplasia should be considered in the differential diagnosis.
Brugada syndromeBrugada syndrome is a life-threatening cardiac arrhythmia (VF and polymorphic VT) with no demonstrable structural cardiac disease [58]. Young males and adolescents are affected most often. This syndrome is familial and a mutation in chromosome 3 has been identified. The mutation affects a sodium channel (SCN5A) and leads to loss of function of the channel [59–61].
An ECG is helpful in the diagnosis and the typical findings are RBBB with ST elevation in V1–V3 (V2 always present) [59,62]. The QT interval is normal. Flecainide or procainamide may be used to

Expert Rev. Cardiovasc. Ther. 7(7), (2009)806
Review Srivathsan, Ng & Mookadam
unmask the ECG changes. Some patients remain asymptomatic despite Brugada-type ECG. An ICD is needed for patients with life-threatening arrhythmia. Asymptomatic patients with abnormal ECG at baseline may benefit from electrophysiologic studies; if sustained ventricular arrhythmia is inducible, an implantable car-dioverter defibrillator is usually implanted. There is, however, no evidence from prospective studies that programmed stimulation is a reliable predictive of subsequent arrhythmic events. Asymptomatic patients with normal baseline ECG require no further testing [59,63].
Long QT syndromeFamily history of SCD, QT prolongation on the ECG and bilateral neural deafness with autosomal recessive pattern of inheritance affecting several children in a family was first reported (Jervell and Lange–Nielsen syndrome) [64]. Family history of SCD, QT prolongation and autosomal dominant pattern of inheritance was subsequently identified (Romano–Ward syndrome). Romano–Ward syndrome is more common than Jervell and Lange–Nielsen syndrome. QTc interval is over 480 ms. Mutations in seven LQTS (LQTS1–7) genes have been identified so far. The fundamental abnormality is prolongation of the action potential secondary to abnormality of transmembrane ion transport. Most mutations
affect the potassium channel except in LQT3 and probably in LQT4 where a sodium channel is affected. In patients with LQT1 subtype, exercise seems to precipitate clinical events. In those with LQT2, acute arousal, such as a sudden loud noise, tends to be a precipitating factor. In patients with LQT3, clinical events occur at rest or during sleep. The risk of cardiac events is higher with certain genotypes; patients with LQT1 and LQT2 have higher risk of events than do those with LQT3. The risk of events also is higher during adulthood in females and during adolescence (before puberty) in males. Increase in the length of the QTc interval and a high number of mutations also increases the risk. Once a clinical event occurs (syncope or survival after SCD), recurrence is frequent.
ManagementAdrenergic modulation with b-blockers is the most useful therapy in both symptomatic and asymptomatic patients, even though b-blockers do not alter QTc interval. Surgical sympathectomy is an adjuvant treatment and has been done rarely since the intro-duction of b-blockers. Oral potassium may be useful in certain genotypes. ICD placement, along with b-blocker therapy, offers the best protection in high-risk patients (survivors of sudden death and those with recurrent syncope).
Torsades de pointesAcquired prolongation of QT interval and pause-dependent, early-after-depolarization-mediated torsades de pointes is most often caused by medication and, occasionally, is caused by metabolic derangement (hypokalemia and hypomagnesemia). Correction of electrolyte abnormalities and discontinuation of precipitating drugs usually leads to amelioration of the arrhythmia. The list of medications that can cause QT prolongation is listed in box 1. Although it may not have an effect on QT interval, intravenous magnesium is highly effective at suppressing torsades de pointes. Occasionally, a temporary transvenous pacemaker or isoprenaline may be needed for effective management.
VT in hypertrophic cardiomyopathySudden cardiac death may be a manifestation of hypertrophic cardio myopathy and is the most common cause of SCD in young athletes. Survivors of SCD require ICD implantation. Primary prevention with an ICD is also used in high-risk patients. Criteria identifying high-risk patients include family history of SCD, exer-cise-induced hypotension, left ventricular hypertrophy with a wall thickness of more than 30 mm and recurrent syncope (particularly when exertional and nonsustained VT on ECG monitoring if fre-quent, repetitive and prolonged). Electrophysiological studies to risk stratify patients have been disappointing. Prophylactic therapy with b-blockers and calcium channel blockers has not been established to prevent SCD, although frequently used. Amiodarone is reportedly useful in this regard, based on an observational study.
VT in arrhythmogenic right ventricular dysplasiaArrhythmogenic right ventricular dysplasia is an important cause of VT and SCD in a small group of patients. Drug therapy is often used, although it is frequently ineffective. ICDs are frequently
Box 1. Drugs associated with QT prolongation.
Antiarrhythmics• Quinidine
• Procainamide
• Disopyramide
• Amiodarone
• Sotalol
• Dofetilide
• Ibutilide
Antihistamines• Astemizole
• Terfenadine
Antimalarials• Chloroquine
• Quinine
Antibiotics• Erythromycin
• Clarithromycin
• Co-trimoxazole
• Ketoconazole
• Grepafloxacin
• Sparfloxacin
Psychiatric drugs• Amitriptyline
• Lithium
• Chlorpromazine
• Haloperidol
• Thioridazine
Miscellaneous• Terodiline
• Cisapride

www.expert-reviews.com 807
ReviewVentricular tachycardia & ventricular fibrillation
Key issues
• Ventricular tachycardia and ventricular fibrillation are the most notable causes of sudden cardiac death.
• Each ventricular arrhythmia has a distinctive pathophysiology, treatment plan and prognosis.
• It is important to distinguish supraventricular tachycardia with aberrancy from ventricular tachycardia.
• In general, those ventricular arrhythmias associated with structurally normal heart are more benign than those associated with structural heart disease.
• Implantable cardiac defibrillators play a pivotal role in both primary and secondary prevention of sudden cardiac death in both ischemic and nonischemic heart diseases.
• b-blockers will usually be the first line of treatment in the majority of types of ventricular tachycardia, ischemic and nonischemic.
• Antiarrhythmic drugs may not be beneficial when directly compared with device therapy but frequently offer a complementary role in the management of patients with an implantable cardiac defibrillator.
• Catheter-based ablation should be considered in patients with the appropriate clinical profiles.
References1 Myerburg RJ, Kessler KM, Castellanos A.
Sudden cardiac death: epidemiology, transient risk, and intervention assessment. Ann. Intern. Med. 119(12), 1187–1197 (1993).
2 Knight BP, Zivin A, Souza J et al. Use of adenosine in patients hospitalized in a university medical center. Am. J. Med. 105, 275–280 (1998).
3 Ertan C, Atar I, Gulmez O et al. Adenosine-induced ventricular arrhythmias in patients with supraventricular tachycardias. Ann. Noninvasive Electrocardiol. 13(4), 386–390 (2008).
4 Romer M, Candinas R. Adenosine-induced non-sustained polymorphic ventricular tachycardia. Eur. Heart J. 15(2), 281–282 (1994).
5 Tan HL, Spekhorst HH, Peters RJ, Wilde AA. Adenosine induced ventricular arrhythmias in the emergency room. Pacing Clin. Electrophysiol. 24(4 Pt 1), 450–455 (2001).
6 Mahnken, AH, Koos R, Katoh M et al. Assessment of myocardial viability in reperfused acute myocardial infarction using 16-slice computed tomography in comparison to magnetic resonance imaging. J. Am. Coll. Cardiol. 45(12), 2042–2047 (2005).
7 Choe Y, Choo K, Jeon E, Gwon H, Choi JH, Park J. Comparison of MDCT and MRI in the detection and sizing of acute and chronic myocardial infarcts. Eur. J. Radiol. 66(2), 292–299 (2008).
8 Ichikawa Y, Sakuma H, Suzawa N. Late gadolinium-enhanced magnetic resonance imaging in acute and chronic myocardial
infarction. Improved prediction of regional myocardial contraction in the chronic state by measuring thickness of nonenhanced myocardium. J. Am. Coll. Cardiol. 45(6), 901–909 (2005).
9 Kwong RY, Korlakunta H. Diagnostic and prognostic value of cardiac magnetic resonance imaging in assessing myocardial viability. Top. Magn. Reson. Imaging 19(1), 15–24 (2008).
10 Campbell RW, Murray A, Julian DG. Ventricular arrhythmias in first 12 hours of acute myocardial infarction. Natural history study. Br. Heart J. 46(4), 351–357 (1981).
11 Northover BJ. Ventricular tachycardia during the first 72 hours after acute myocardial infarction. Cardiology 69(3), 149–156 (1982).
implanted in this group of patients. Radiofrequency ablation or surgical disarticulation techniques may be tried if arrhythmia is frequent and leads to multiple shocks.
ConclusionVentricular tachycardia and VF as a cause of death in ischemic heart disease has substantially increased as revascularization techniques have become widely available. The pathogenesis and management of this preventable cause of death is better under-stood from multiple randomized trial data. ICD is the mainstay in secondary and primary prevention. A benefit of adrenergic modu-lation, particularly with b-blocker therapy, is increasingly recog-nized. Appropriate diagnosis, management of reversible causes and triggers has led to improvement in both mortality and morbidity.
Expert commentary & five-year viewRecognition of VT and VF is on the increase as a result of improved survival from revascularization and heart failure man-agement along with ever-increasing utility of ICDs. In the future, ICDs are likely to become smaller and provide antitachycardia pacing from both left ventricular and right ventricular leads to
prevent shocks. Longevity of ICDs will be better and ICDs will play an integral role in heart failure management in monitoring several parameters that will lead to alteration of tailored medical therapy. Leadless ICD is perhaps several years away and, when developed along with leadless pacing targeting specific regions of the myocardium, will afford this therapy a wider appeal with minimal risk. Endocardial and epicardial radiofrequency and cryoablations will be offered early to prevent ICD shocks, likely in a preventive fashion. Newer antiarrhythmic drugs may target specific ion channels to prevent VT and VF without proarrhyth-mia. Overall, VT and VF as causes of cardio vascular death is likely to decline, perhaps replaced by pump failure as a major cause of death.
Financial & competing interests disclosureThe authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.

Expert Rev. Cardiovasc. Ther. 7(7), (2009)808
Review Srivathsan, Ng & Mookadam
12 Brugada P, Brugada J, Mont L, Smeets J, Andries EW. A new approach to the differential diagnosis of a regular tachycardia with a wide QRS complex. Circulation 83(5), 1649–1659 (1991).
13 Lau EW, Ng GA. The reliable electrocardiographic diagnosis of regular broad complex tachycardia: a holy grail that will forever elude the clinician’s grasp? Pacing Clin. Electrophysiol. 25(12), 1756–1761 (2002).
14 Wellens HJ. Electrophysiology: ventricular tachycardia: diagnosis of broad QRS complex tachycardia. Heart 86(5), 579–585 (2001).
15 Kudenchuk PJ, Cobb LA, Copass MK et al. Amiodarone for resuscitation after out-of-hospital cardiac arrest due to ventricular fibrillation. N. Engl. J. Med. 341(12), 871–878 (1999).
16 Goldberger JJ, Cain ME, Hohnloser S et al. American Heart Association/american College of Cardiology Foundation/heart Rhythm Society scientific statement on noninvasive risk stratification techniques for identifying patients at risk for sudden cardiac death: a scientific statement from the American Heart Association Council on Clinical Cardiology Committee on Electrocardiography and Arrhythmias and Council on Epidemiology and Prevention. Heart Rhythm 5(10), E1–E21 (2008).
17 No authors listed. A comparison of antiarrhythmic-drug therapy with implantable defibrillators in patients resuscitated from near-fatal ventricular arrhythmias. The Antiarrhythmics versus Implantable Defibrillators (AVID) Investigators. N. Engl. J. Med. 337(22), 1576–1583 (1997).
18 Zipes DP, Camm AJ, Borggrefe M et al. ACC/AHA/ESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: a report of the American College of Cardiology/American Heart Association Task Force and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Develop Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death). J. Am. Coll. Cardiol. 48(5), E247–E346 (2006).
19 Julian DG, Camm AJ, Frangin G et al. Randomised trial of effect of amiodarone on mortality in patients with left-ventricular dysfunction after recent myocardial infarction: EMIAT. European
Myocardial Infarct Amiodarone Trial Investigators. Lancet 349(9053), 667–674 (1997).
20 Cairns JA, Connolly SJ, Roberts R, Gent M. Randomised trial of outcome after myocardial infarction in patients with frequent or repetitive ventricular premature depolarisations: CAMIAT. Canadian Amiodarone Myocardial Infarction Arrhythmia Trial Investigators. Lancet 349(9053), 675–682 (1997).
21 Echt DS, Liebson PR, Mitchell LB et al. Mortality and morbidity in patients receiving encainide, flecainide, or placebo. The Cardiac Arrhythmia Suppression Trial. N. Engl. J. Med. 324(12), 781–788 (1991).
22 Effect of the antiarrhythmic agent moricizine on survival after myocardial infarction. The Cardiac Arrhythmia Suppression Trial II Investigators. N. Engl. J. Med. 327(4), 227–233 (1992).
23 Connolly SJ, Gent M, Roberts RS et al. Canadian implantable defibrillator study (CIDS) : a randomized trial of the implantable cardioverter defibrillator against amiodarone. Circulation 101, 1297–1302 (2000).
24 Kuck KH, Cappato R, Siebels J, Ruppel R. Randomized comparison of antiarrhythmic drug therapy with implantable defibrillators in patients resuscitated from cardiac arrest: the Cardiac Arrest Study Hamburg (CASH). Circulation 102, 748–754 (2000).
25 Moss AJ, Hall WJ, Cannom DS et al. Improved survival with an implanted defibrillator in patients with coronary disease at high risk for ventricular arrhythmia. Multicenter Automatic Defibrillator Implantation Trial Investigators. N. Engl. J. Med. 335, 1933–1940 (1996).
26 Bigger JT Jr. Prophylactic use of implanted cardiac defibrillators in patients at high risk for ventricular arrhythmias after coronary-artery bypass graft surgery. Coronary Artery Bypass Graft (CABG) Patch Trial Investigators. N. Engl. J. Med. 337, 1569–1575 (1997).
27 Moss AJ, Zareba W, Hall WJ et al. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. Multicenter Automatic Defibrillator Implantation Trial II Investigators. N. Engl. J. Med. 346, 877–883 (2002).
28 Strickberger SA, Hummel JD, Bartlett TG et al. Amiodarone versus implantable cardioverter-defibrillator: randomized trial in patients with nonischemic dilated
cardiomyopathy and asymptomatic nonsustained ventricular tachycardia – AMIOVIRT. AMIOVIRT Investigators. J. Am. Coll. Cardiol. 41, 1707–1712 (2003).
29 Kadish A, Dyer A, Daubert JP et al. Defibrillators in Non-Ischemic Cardiomyopathy Treatment Evaluation (DEFINITE) Investigators. N. Engl. J. Med. 350, 2151–2158 (2004).
30 Bristow MR, Saxon LA, Boehmer J et al. Cardiac-resynchronization therapy with or without an implantable defibrillator in advanced chronic heart failure. Comparison of Medical Therapy, Pacing, and Defibrillation in Heart Failure (COMPANION) Investigators. N. Engl. J. Med. 350, 2140–2150 (2004).
31 Hohnloser SH, Kuck KH, Dorian P et al. Prophylactic use of an implantable cardioverter-defibrillator after acute myocardial infarction. N. Engl. J. Med. 351, 2481–2488 (2004).
32 Bardy GH, Lee KL, Mark DB et al. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. Sudden Cardiac Death in Heart Failure Trial (SCD-HeFT) Investigators. N. Engl. J. Med. 352, 225–237 (2005).
33 Reddy VY, Reynolds MR, Neuzil P et al. Prophylactic catheter ablation for the prevention of defibrillator therapy. N. Engl. J. Med. 357, 2657–2665 (2007).
34 Carbucicchio C, Santamaria M, Trevisi N et al. Catheter ablation for the treatment of electrical storm in patients with implantable cardioverter-defibrillators: short- and long-term outcomes in a prospective single-center study. Circulation 117, 462–469 (2008).
35 O’Donnell D, Bourke JP, Anilkumar R, Simeonidou E, Furniss SS. Radiofrequency ablation for post infarction ventricular tachycardia. Report of a single centre experience of 112 cases. Eur. Heart J. 23(21), 1699–1705 (2002).
36 Calkins H, Epstein A, Packer D et al. Catheter ablation of ventricular tachycardia in patients with structural heart disease using cooled radiofrequency energy: results of a prospective multicenter study. Cooled RF Multi Center Investigators Group. J. Am. Coll. Cardiol. 35(7), 1905–1914 (2000).
37 Fahmy TS, Wazni OM, Jaber WA et al. Integration of positron emission tomography/computed tomography with electroanatomical mapping: a novel approach for ablation of scar-related ventricular tachycardia. Heart Rhythm 5(11), 1538–1545 (2008).

www.expert-reviews.com 809
ReviewVentricular tachycardia & ventricular fibrillation
38 Klemm HU, Ventura R, Steven D et al. Catheter ablation of multiple ventricular tachycardias after myocardial infarction guided by combined contact and noncontact mapping. Circulation 115(21), 2697–2704 (2007).
39 Marshall DA, O’Brien BJ, Nichol G. Review of economic evaluations of radiofrequency catheter ablation for cardiac arrhythmias. Can. J. Cardiol. 19(11), 1285–1304 (2003).
40 Caceres J, Jazayeri M, McKinnie J et al. Sustained bundle branch reentry as a mechanism of clinical tachycardia. Circulation 79(2), 256–270 (1989).
41 Cohen TJ, Chien WW, Lurie KG et al. Radiofrequency catheter ablation for treatment of bundle branch reentrant ventricular tachycardia: results and long-term follow-up. J. Am. Coll. Cardiol. 18(7), 1767–1773 (1991).
42 Blank Z, Dhala A, Deshpande S et al. Bundle branch reentrant ventricular tachycardia: cumulative experience in 48 patients. J. Cardiovasc. Electrophysiol. 4(3), 253–262 (1993).
43 Mehdirad AA, Keim S, Rist K, Tchou P et al. Long-term clinical outcome of right bundle branch radiofrequency catheter ablation for treatment of bundle branch reentrant ventricular tachycardia. Pacing Clin. Electrophysiol. 18(12 Pt 1), 2135–2143 (1995).
44 Lopera G, Stevenson WG, Soejima K et al. Identification and ablation of three types of ventricular tachycardia involving the His–Purkinje system in patients with heart disease. J. Cardiovasc. Electrophysiol. 15(1), 52–58 (2004).
45 Narasimhan C, Jazayeri MR, Sra J et al. Ventricular tachycardia in valvular heart disease: facilitation of sustained bundle-branch reentry by valve surgery. Circulation 96(12), 4307–4313 (1997).
46 Merino JL, Carmona JR, Fernández-Lozano I, Peinado R, Basterra N, Sobrino JA. Mechanisms of sustained ventricular tachycardia in myotonic dystrophy: implications for catheter ablation. Circulation 98(6), 541–546 (1998).
47 Josephson M. Clinical Cardiac Electrophysiology: Techniques and Interpretations (4th Edition). Lippincott Williams & Wilkins, OA, USA (2008).
48 Zipes D. Cardiac Electrophysiology: From Cell to Bedside (4th Edition). WB Sauders Company, PA, USA (2004).
49 Latif S, Dixit S, Callans DJ. Ventricular arrhythmias in normal hearts. Cardiol. Clin. 18(2), 265–291 (2000).
50 Lerman BB, Stein K, Engelstein ED et al. Mechanism of repetitive monomorphic ventricular tachycardia. Circulation 92(3), 421–429 (1995).
51 Lerman BB, Belardinelli L, West GA et al. Adenosine-sensitive ventricular tachycardia: evidence suggesting cyclic AMP-mediated triggered activity. Circulation 74(2), 270–280 (1986).
52 Coggins DL, Lee RJ, Sweeney J et al. Radiofrequency catheter ablation as a cure for idiopathic tachycardia of both left and right ventricular origin. J. Am. Coll. Cardiol. 23(6), 1333–1341 (1994).
53 Klein LS, Shih HT, Hackett FK, Zipes DP, Miles WM. Radiofrequency catheter ablation of ventricular tachycardia in patients without structural heart disease. Circulation 85(5), 1666–1674 (1992).
54 Calkins H, Kalbfleisch SJ, el-Atassi R et al. Relation between efficacy of radiofrequency catheter ablation and site of origin of idiopathic ventricular tachycardia. Am. J. Cardiol. 71(10), 827–833 (1993).
55 Wilber DJ, Baerman J, Olshansky B, Kall J, Kopp D. Adenosine-sensitive ventricular tachycardia. Clinical characteristics and response to catheter ablation. Circulation 87(1), 126–134 (1993).
56 Timmermans C, Rodriguez LM, Crijns HJ, Moorman AF, Wellens HJ. Idiopathic left bundle-branch block-shaped ventricular tachycardia may originate above the pulmonary valve. Circulation 108(16), 1960–1967 (2003).
57 Rodriguez LM, Smeets JL, Timmermans C, Wellens HJ. Predictors for successful ablation of right- and left-sided idiopathic ventricular tachycardia. Am. J. Cardiol. 79(3), 309–314 (1997).
58 Antzelevitch C, Brugada P, Brugada J. Brugada syndrome: a decade of progress. Circ. Res. 91(12), 1114–1118 (2002).
59 Antzelevitch C, Brugada P, Borggrefe M. Brugada syndrome: report of the second consensus conference: endorsed by the Heart Rhythm Society and the European Heart Rhythm Association. Circulation 111(5), 659–670 (2005).
60 Weiss R, Barmada MM, Nguyen T et al. Clinical and molecular heterogeneity in the Brugada syndrome: a novel gene locus on chromosome 3. Circulation 105(6), 707–713 (2002).
61 Chen Q, Kirsch GE, Zhang D et al. Genetic basis and molecular mechanism for idiopathic ventricular fibrillation. Nature 392(6673), 293–296 (1998).
62 Wilde AA, Antzelevitch C, Borggrefe M et al. Proposed diagnostic criteria for the Brugada syndrome. Eur. Heart J. 23(21), 1648–1654 (2002).
63 Sacher F, Probst V, Iesaka Y et al. Outcome after implantation of a cardioverter-defibrillator in patients with Brugada syndrome: a multicenter study. Circulation 114(22), 2317–2324 (2006).
64 Moss AJ. Long QT syndrome. JAMA 289(16), 2041–2044 (2003).
Affiliations• Komandoor Srivathsan, MD, FACC
Cardiovascular Diseases, Mayo Clinic, 13400 E Shea Boulevard, Scottsdale, AZ 85255, USA
• Daniel WC Ng, MD Cardiovascular Diseases, Mayo Clinic, 13400 E Shea Boulevard, Scottsdale, AZ 85255, USA
• Farouk Mookadam, MD, FACC Cardiovascular Diseases, Mayo Clinic, 13400 E Shea Boulevard, Scottsdale, AZ 85255, USA [email protected]