Embed Size (px)
Citation preview

http://vmj.sagepub.com/Vascular Medicine
http://vmj.sagepub.com/content/early/2014/08/31/1358863X14547561The online version of this article can be found at:
DOI: 10.1177/1358863X14547561
published online 1 September 2014Vasc MedAlexandrov and Sandra L Katanick
Bendick, Naomi M Hamburg, Joann M Lohr, Lucy LaPerna, Steven A Leers, Michael P Lilly, Charles Tegeler, Andrei V.Marge Hutchisson, Laurence Needleman, James F Benenati, Michael R Jaff, George H Meier, Susana Perese, Phillip Tatjana Rundek, Scott C Brown, Kefeng Wang, Chuanhui Dong, Mary Beth Farrell, Gary V Heller, Heather L Gornik,
beneficiaries: The VALUE (Vascular Accreditation, Location & Utilization Evaluation) StudyAccreditation status and geographic location of outpatient vascular testing facilities among Medicare
Published by:
http://www.sagepublications.com
On behalf of:
Society for Vascular Medicine
can be found at:Vascular MedicineAdditional services and information for
http://vmj.sagepub.com/cgi/alertsEmail Alerts:
http://vmj.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
What is This?
- Sep 1, 2014OnlineFirst Version of Record >>
by guest on September 2, 2014vmj.sagepub.comDownloaded from by guest on September 2, 2014vmj.sagepub.comDownloaded from

Vascular Medicine 1 –9
© The Author(s) 2014Reprints and permissions:
sagepub.co.uk/journalsPermissions.navDOI: 10.1177/1358863X14547561
vmj.sagepub.com
Accreditation status and geographic location of outpatient vascular testing facilities among Medicare beneficiaries: The VALUE (Vascular Accreditation, Location & Utilization Evaluation) Study
Tatjana Rundek1,2, Scott C Brown2, Kefeng Wang2, Chuanhui Dong1, Mary Beth Farrell3, Gary V Heller3, Heather L Gornik4, Marge Hutchisson3, Laurence Needleman5, James F Benenati6, Michael R Jaff7, George H Meier8, Susana Perese9, Phillip Bendick10, Naomi M Hamburg11, Joann M Lohr12, Lucy LaPerna13, Steven A Leers14, Michael P Lilly15, Charles Tegeler16, Andrei V. Alexandrov17 and Sandra L Katanick3
AbstractObjective: There is limited information on the accreditation status and geographic distribution of vascular testing facilities in the US. The Centers for Medicare & Medicaid Services (CMS) provide reimbursement to facilities regardless of accreditation status. The aims were to: (1) identify the proportion of Intersocietal Accreditation Commission (IAC) accredited vascular testing facilities in a 5% random national sample of Medicare beneficiaries receiving outpatient vascular testing services; (2) describe the geographic distribution of these facilities.Methods: The VALUE (Vascular Accreditation, Location & Utilization Evaluation) Study examines the proportion of IAC accredited facilities providing vascular testing procedures nationally, and the geographic distribution and utilization of these facilities. The data set containing all facilities that billed Medicare for outpatient vascular testing services in 2011 (5% CMS Outpatient Limited Data Set (LDS) file) was examined, and locations of outpatient vascular testing facilities were obtained from the 2011 CMS/Medicare Provider of Services (POS) file.Results: Of 13,462 total vascular testing facilities billing Medicare for vascular testing procedures in a 5% random Outpatient LDS for the US in 2011, 13% (n=1730) of facilities were IAC accredited. The percentage of IAC accredited vascular testing facilities in the LDS file varied significantly by US region, p<0.0001: 26%, 12%, 11%, and 7% for the Northeast, South, Midwest, and Western regions, respectively.Conclusions: Findings suggest that the proportion of outpatient vascular testing facilities that are IAC accredited is low and varies by region. Increasing the number of accredited vascular testing facilities to improve test quality is a hypothesis that should be tested in future research.
1 Department of Neurology, University of Miami Miller School of Medicine, Miami, FL, USA
2 Department of Public Health Sciences, University of Miami Miller School of Medicine, Miami, FL, USA
3Intersocietal Accreditation Commission (IAC), Ellicott City, MD, USA4 Department of Vascular Medicine, Cleveland Clinic, Cleveland, OH, USA5 Department of Radiology, Thomas Jefferson University, Jefferson Medical College, Philadelphia, PA, USA
6 Baptist Cardiac & Vascular Institute, Baptist Hospital of Miami, Miami, FL, USA
7 Department of Medicine, Harvard Medical School, Massachusetts General Hospital, Boston, MA, USA
8 Department of Vascular Surgery, University of Cincinnati Academic Health Center, Cincinnati, OH, USA
9 Department of Vascular Surgery, University of Southern California, Keck School of Medicine, Los Angeles, CA, USA
10Vascular Laboratory, William Beaumont Hospital, Royal Oak, MI, USA11 Whitaker Cardiovascular Institute, Boston University School of
Medicine, Boston, MA, USA
547561 VMJ0010.1177/1358863X14547561Vascular MedicineRundek et al.research-article2014
Original Article
12Good Samaritan Outpatient Center, Cincinnati, OH, USA13Riverside Radiology Associates, Columbus, OH, USA14University of Pittsburgh Medical Center, Pittsburgh, PA, USA15 University of Maryland School of Medicine, Vascular Laboratory,
Baltimore, MD, USA16Wake Forest Baptist Health, Winston-Salem, NC, USA17 University of Tennessee Health Science Center, Memphis, TN, USA
Dr Jeffrey Olin was the guest editor for this article.
Corresponding author:Scott C BrownDepartment of Public Health SciencesUniversity of Miami Miller School of Medicine1120 NW 14th StClinical Research Building (CRB) Rm. 1065Miami, FL 33136USAE-mail: [email protected]
by guest on September 2, 2014vmj.sagepub.comDownloaded from

2 Vascular Medicine
KeywordsGeographic disparities, Intersocietal Accreditation Commission (IAC), Medicare beneficiaries, Vascular Accreditation, Location & Utilization Evaluation (VALUE) Study, Vascular laboratory testing accreditation, Vascular testing
Introduction
There is limited information regarding the utilization of vascular testing in the US with respect to accreditation sta-tus of vascular testing facilities. The Medicare Payment Advisory Commission (MedPAC), and ultrasound-related professional organizations, support the requirements for sonographers to either have an appropriate certification cre-dential or to operate in facilities that are accredited, to help assure that quality standards are maintained.1 Accreditation, except in selected states, does not affect reimbursement. The Centers for Medicare and Medicaid Services (CMS) equally reimburse for services provided by accredited and non-accredited facilities. Monitoring the status of accred-ited vascular facilities, including the number of accredited facilities and the quality of services that accredited vascular testing facilities provide, is relatively well documented;2–6 however, non-accredited vascular testing facilities perform services of unknown volume.
Prior evidence suggests that the accreditation of vascu-lar testing facilities may be associated with optimal clinical outcomes. For example, a high degree of diagnostic accu-racy in assessing internal carotid artery stenosis has been reported for accredited vascular testing laboratories.2 Moreover, there is comparative data on the quality of test-ing between accredited and non-accredited laboratories in performing carotid duplex ultrasound scanning. These data suggest results from non-accredited laboratories do not appear to be reliable in planning management of carotid atherosclerotic disease and results from non-accredited laboratories should be used with caution.7
The Intersocietal Accreditation Commission (IAC), a multi-specialty accreditation organization, is one of the few CMS-deemed8 organizations for accreditation of facilities performing imaging, along with the American College of Radiology (ACR) and the Joint Commission (through its Ambulatory Care program).1,4,9,10 The IAC has developed high standards with uniform guidelines for vascular testing and accreditation.3–5,11,12 The mission of the IAC is ‘Improving Health Care Through Accreditation’ with the goal ‘to ensure high quality patient care and to promote health care by providing a mechanism to encourage and recognize the provision of quality imaging diagnostic eval-uations by a process of accreditation’.5 Although the IAC currently maintains an up-to-date list of all IAC accredited outpatient vascular facilities in the US,6 the number and locations of non-IAC accredited vascular testing facilities that receive reimbursement from CMS is unknown. Accreditation status of the vascular testing facility may be one determinant of the quality of health care services and outcomes2,7 in Medicare beneficiaries and other at-risk populations. The number and geographic locations of IAC accredited and non-IAC accredited facilities may be impor-tant information to determine whether a potential source of quality differences in vascular testing services exists. Given
that many vascular diseases occur in older populations, the Medicare database is an appropriate source for this information.
The main aims of the present study were therefore: (1) to identify the proportion of IAC accredited vascular testing facilities in a 5% random national sample of Medicare ben-eficiaries receiving outpatient vascular testing services in 2011; and (2) to describe the geographical distribution of these facilities. An additional aim was to identify variation in the types and volumes of outpatient procedures per-formed by IAC versus non-IAC facilities.
Materials and methods
Overview of materials and methods
Study design. The VALUE (Vascular Accreditation, Loca-tion & Utilization Evaluation) Study was conducted to identify the proportion of IAC accredited vascular testing facilities among those Medicare beneficiaries receiving vascular testing services in ambulatory settings, as well as to identify utilization and geographic variation in the locations of IAC accredited versus non-IAC accredited vascular testing facilities which receive reimbursement from CMS.
The present analyses examined the proportion of IAC accredited facilities in a 5% CMS random Outpatient Limited Data Set (LDS) who billed CMS (Medicare) for vascular testing services in 2011. The geographic distribu-tion of these facilities and the types and volumes of vascu-lar testing procedures across IAC versus non-IAC accredited facilities were collected. The list of all testing facilities that billed Medicare for vascular testing services from the CMS 2011 5% Medicare Outpatient LDS file was examined, and locations of outpatient vascular testing facil-ities were obtained from the 2011 Medicare Provider of Services (POS) file. The list of the names and locations of all IAC accredited vascular testing facilities in 2011 was obtained from the IAC.
CMS data sources
The following CMS data sets were obtained. (1) The 2011 CMS Outpatient LDS file, 5% national file (ResDAC, www.resdac.org), which contains final action, fee-for-ser-vice claims data submitted by institutional outpatient pro-viders, including vascular testing facilities. The 2011 CMS Outpatient LDS data was released in March of 2013, and the 5% sample was selected at random based on health insurance claim (HIC) numbers for all outpatient Medicare billing records in 2011. This file also contained both a CMS provider number, as well as a listing of the procedures (Current Procedural Terminology (CPT) code) performed by each facility. (2) The 2011 Medicare POS file, which was the list of all providers/facilities that billed Medicare
by guest on September 2, 2014vmj.sagepub.comDownloaded from

Rundek et al. 3
for patient services in 2011. Included in the POS file were a listing of all facilities (including vascular testing facilities) that billed Medicare/CMS – and a billing address for each facility. Specifically, the present analyses used the ‘Provider of Services (POS) – Other Facilities’ data file (which included those facilities billing CMS for vascular testing facilities on an outpatient and/or inpatient basis). Thus, this file contained provider numbers and provider geographical information for all Medicare-approved providers billing for outpatient services in 2011, which served as the denomina-tor for the present analyses. A second segment of the POS file Clinical Laboratory Improvement Amendments (CLIA) that contained only labs, which would correspond more closely to the CMS’s carrier files, but that provided a low match (~5%) to the list and locations of IAC accredited facilities, was not used in the present analyses.
IAC data
IAC data included a listing of all 1765 non-duplicated IAC accredited vascular testing facilities, with their street address, and was received by the research team from IAC in June 2013. This data file contained the names and loca-tions of all IAC accredited vascular testing facilities, which served to determine the numerator for the present analyses, and which was needed for merging with the CMS data files (which contained data on all vascular testing facilities reimbursed by Medicare in 2011).
Procedures
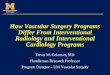
Figure 1 schematically represents an overview of the data merge process conducted for this study. Given that the pre-sent analyses focus on outpatient vascular testing services, the listing of all CMS Outpatient LDS records in the 5% national data file for 2011 were restricted to those claims using one of 20 CPT vascular testing codes, including both cerebrovascular CPTs (eight CPT codes) and non-cerebro-vascular CPTs (12 CPT codes) – Cerebrovascular testing: 93875 (non-invasive physiologic studies of extracranial arteries, complete bilateral study), 93880 (carotid duplex), 93882 (limited), 93886 (transcranial Doppler, TCD), 93888 (limited), 93890 (vasoreactivity), 93892 (emboli detection without intravenous microbubble injection), 93893 (emboli detection with intravenous microbubble injection); Extremity arterial (duplex and physiological testing): 93922, 93923, 93931, 93924, 93925, 93926; Extremity venous: 93970, 93971; Visceral vascular: 93976, 93978, 93979; and Hemodialysis access: 93990.
A two-step solution was devised for data merging among the IAC file, CMS POS file, and CMS Outpatient LDS file because of a lack of unique identifiers across all data file types (Figure 1). In the first step, the CMS POS file was merged with the CMS Outpatient file to find the addresses for all providers with outpatient vascular testing proce-dures. In the second step, these addresses were matched to the addresses of the IAC facilities.
Spa�al join using ArcGIS
Outpa�ent Vascular Tes�ngProviders in USA
(n = 13462)
Original Accredited Facili�esFile from IAC (n = 2297)
Non-duplicated IAC Facili�es(n = 1765)
Deduplica�on by LaboratoryNumber
IAC lab addresses linked withprovider addresses
(n = 1765)
IAC lab addresses in USA linked with provider
addresses(n = 1730)
Exclude Canada loca�ons,U.S. Territories and USFacili�es with distancegreater than 10 miles
Geocode IAC AddressesGeocode IAC Addresses
Figure 1. Flow diagram indicating data processing steps for merging CMS Medicare data sets (POS and Outpatient 5% LDS) with Intersocietal Accreditation Commission (IAC) data on IAC accredited facilities and locations.
by guest on September 2, 2014vmj.sagepub.comDownloaded from

4 Vascular Medicine
Geographic information system (GIS)
Facilities were geocoded using ArcGIS software version 10 (ESRI, Redlands, CA, USA). Geocoding was used to merge facility addresses from the IAC and CMS POS data files. Prior to geocoding, the facility addresses were standardized from both the IAC and CMS POS files. In most instances the exact characters (including spelling, abbreviations, etc.) for a 100% address overlap between the files did not exist and the automatic program could not perform merging (e.g. without this, ‘St.’ and ‘Street’ did not match). Therefore, it was necessary to relax the merging rules to permit a mini-mum match score of 80% or more of address characters between the two files. A separate file was then created using standardized facility addresses. For example, using this 80% match rule, ‘1120 NW 14 Street, Miami, Florida 33136’ might be standardized to read, ‘1120 NW 14th St., Miami, FL’. After sorting the spatial-join result by descend-ing distance, a manual standardization was performed to merge the IAC facility addresses to POS provider addresses, in which the top 5% of records with the greatest distances between the IAC address and the nearest/corresponding POS address were manually checked to verify the accuracy of the matching processing. The facility address is not nec-essarily the same address as the billing address for the pro-vider that bills Medicare for vascular testing services. Therefore, a case-by-case examination was conducted to see what tolerance/maximum distance resulted in an accu-rate match between the addresses in the POS and IAC files. After excluding those IAC facilities located in US territo-ries or Canada, as well as those facilities where the distance between the IAC address and nearest POS billing address was more than 10 miles, approximately 98% of IAC accred-ited facilities (n=1730 out of 1765) were successfully geo-coded and matched to CMS POS addresses.
In summary, over 98% (n=1730) of the IAC accredited facilities were matched to a CMS provider in the US, each of which billed Medicare for outpatient vascular testing services. Following geocoding, facilities were assigned to their corresponding state, and to one of four US Census-defined regions of the US: Northeast, South, Midwest, and West.13
Statistical analyses
Descriptive and associational analyses were conducted using SAS version 9 software (Cary, NC, USA). A chi-squared test was conducted to test for regional variation in the proportion of IAC accredited facilities across the four Census-defined regions of the US.13
Results
Figure 1 shows that, of the 13,462 total facilities billing Medicare for vascular testing procedures in a 5% random Outpatient LDS for the US in 2011, only 13% (n=1730) were IAC accredited. The remaining 11,732 (87%) facili-ties (assuming one facility per provider) were considered non-IAC accredited because they could not be matched by name or location with the 1730 IAC accredited facili-ties that were geocoded within the US. Of the total of
1730 IAC accredited facilities that could be geocoded from the list of IAC facilities, these were distributed across all US regions, with 30% (n=526) in the Northeast, 36% (n=619) in the South, 25% (n=424) in the Midwest, and 9% (n=161) in the West region, respectively (not shown in Figure 1).
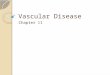
Figure 2 shows the distribution of all POS vascular test-ing facilities and all IAC accredited facilities across the US. Figure 3 shows the percentage of facilities that billed CMS for outpatient vascular testing services that were IAC accredited, by region. When examining the percentage of IAC accredited facilities within each region, the percentage of vascular facilities in the 5% Outpatient LDS file that were IAC accredited varied significantly across all four US regions (χ2[3]=397.6, p<0.0001): 26%, 12%, 11% and 7% of facilities were IAC accredited within each of the Northeast, South, Midwest, and West regions, respectively (Figure 2). The five states and locations with the highest percentages of IAC accredited facilities, in descending order, were NY, NJ, MD, MA, and DE, each having over 25% of facilities accredited by the IAC. (See Figures 4a and 4b for the absolute number and percentage of IAC accredited facilities for each state/location, respectively.)
Table 1 shows the percentage of outpatient vascular test-ing procedures that were conducted at IAC versus non-IAC facilities, by test type. Overall, 37% of all outpatient vascu-lar testing procedures by volume were conducted in IAC accredited facilities. There was significant variation in the percentage of procedures that were conducted by IAC facil-ities by test type (χ2[4]=325.0, p<0.0001): 35%, 37%, 39%, 46% and 26% of procedures were performed in IAC accred-ited facilities for extremity venous, cerebrovascular, extremity arterial, visceral vascular, and hemodialysis access, respectively (Table 1). This result reflects the fact that the percentage of IAC accredited procedures was approximately the same (~37%) across the first three test types (extremity venous, cerebrovascular, and extremity arterial), but that a relatively high percentage (46%) of vis-ceral vascular tests were performed in IAC accredited facil-ities, and that a much lower percentage (26%) of hemodialysis access procedures were performed in IAC accredited facilities.
Further analyses examined whether the proportion of vascular testing procedures that were conducted in IAC accredited facilities varied by region: When considering whether there was geographic variation in the proportion of all vascular testing procedures in a region that were con-ducted in IAC accredited facilities, there were statistically significant differences in the percentage of procedures that were conducted in IAC facilities by region: 47% of all vas-cular testing procedures that were conducted in the Northeast were performed by IAC accredited facilities in that region, compared to 36% in the South, 38% in the Midwest, and 22% in the West (χ2[3] = 2577.11, p<0.0001).
Discussion
This is the first study to suggest that the proportion of IAC accredited facilities appears to be low (13%) among those facilities billing CMS for outpatient vascular testing
by guest on September 2, 2014vmj.sagepub.comDownloaded from

Rundek et al. 5
services. However, IAC accredited facilities produced more examinations per facility than did non-IAC accredited facilities: 37% of testing procedures were done in IAC accredited facilities, despite the fact that only 13% of facilities were IAC accredited. With regard to the specific
procedures performed by accreditation status, the low per-centage of hemodialysis procedures that were performed in IAC accredited facilities may reflect the fact that the IAC does not specifically accredit hemodialysis access procedures.
Figure 2. Overlay of geocoding of vascular testing facilities in the CMS 2011 Provider of Services (POS) file with IAC data on locations of IAC accredited facilities in the US.
Figure 3. Comparison of percentage IAC accredited versus non-IAC accredited vascular testing facilities within each US region.
by guest on September 2, 2014vmj.sagepub.comDownloaded from

6 Vascular Medicine
Fig
ure
4. C
ompa
riso
n of
(a)
num
ber
of IA
C a
ccre
dite
d va
scul
ar t
estin
g fa
cilit
ies
by U
S st
ate
or lo
catio
n; (
b) p
erce
ntag
e of
IAC
acc
redi
ted
vasc
ular
tes
ting
faci
litie
s by
US
stat
e or
loca
tion.
by guest on September 2, 2014vmj.sagepub.comDownloaded from

Rundek et al. 7
There is substantial variation in IAC accreditation rates across the US. These results suggest that geographically focused outreach efforts may increase the number of accredited vascular testing facilities nationwide: this is par-ticularly true in the South, Midwest, and Western regions, which had the lowest percentages of IAC accredited facili-ties (i.e. 12%, 11% and 7%, respectively) among those facilities billing CMS/Medicare for outpatient vascular testing services in 2011. Interestingly, as of 2011, there were two states that had passed a bill requiring the licensure of ultrasound technologists: New Mexico (April 2009) and Oregon (July 2009),14 which had IAC accreditation rates of 8% and 9%, respectively, in 2011. This result suggests that accreditation rates, although low for these two states, were comparable to other states in the Western region, and that further time may be needed to ascertain whether practition-ers embrace licensure over accreditation, or vice versa, in states mandating licensure. Interestingly, although no infor-mation was available for this study on the proportion of non-IAC accredited facilities that employ credentialed sonographers, additional data suggest that over 98% of IAC accredited vascular testing facilities had at least one cre-dentialed staff member in 2011 and, on average, a high per-centage (M=78.3%; SD=25.9%) of technical staff members were credentialed within each IAC facility (Personal Communication, MB Farrell, IAC, June 2014).
The present findings are an important first step to under-stand the nationwide impact of voluntary accreditation. Non-accredited vascular testing facilities perform vascular ultrasound services of unknown volume and quality, while equally reimbursed for their performance. In the GAO report to Congressional committees in 2007,1 most ultra-sound procedures provided to Medicare beneficiaries in any setting were either echocardiograms or non-invasive vascular procedures, accounting for 53% of the 41 million procedures provided to nearly 12.4 million Medicare ben-eficiaries in any setting and 49% of the US$3.2 billion in Medicare Part B payments for ultrasound procedures. In addition, the GAO report1 has suggested that CMS consider establishing credentialing or other qualification require-ments for sonographers as their skills are critical for its use. Findings from several peer-reviewed studies, the MedPAC, and ultrasound-related professional organizations support the requirements for sonographers to either have creden-tials or to operate in facilities that are accredited, whereby specific quality standards are maintained.1 CMS has stated that it would consider a nationwide recommendation, but it would rather have states engage their own licensing bodies
in implementing sonographer licensure programs that address competency and qualification issues because a national policy would not take into account regional varia-tion in factors such as access to care and state licensing requirements.1 Unfortunately, few states require diagnostic medical sonographers to be licensed. This study indicates that since one of only a few voluntary accreditation pro-grams is not widely used, voluntary accreditation has also not been a solution for the issues the MedPAC has raised. The quality of nationwide vascular testing services is not consistent or standardized by either licensure or accreditation.
In some settings, CMS or its contractors have required or recommended that sonographers either be credentialed or work in an accredited facility.15 Medicare’s inconsistent requirements for accreditation of facilities undermine assurance that beneficiaries are receiving high-quality ser-vices across the country.
The different IAC accreditation rates by state and region of outpatient vascular testing facilities and their utilization among Medicare beneficiaries within the present study provide high-impact data to develop geographically focused outreach efforts to increase the number of accred-ited vascular testing facilities. Interestingly, although only 13% of the facilities in the sample were IAC accredited, a disproportionately larger proportion (37%) of the vascular testing procedures were conducted by IAC facilities rela-tive to the number of IAC accredited facilities. Similar to the finding that there was geographic variation in the per-centage of facilities that are IAC accredited within each region, there was substantial geographic variation in the percentage of vascular testing procedures that were con-ducted in IAC facilities in each region, with the finding that 47% of all vascular testing procedures that were con-ducted in the Northeast were performed by IAC facilities in that region, versus lower percentages of vascular testing procedures conducted by IAC facilities in the other regions of the US (i.e. 36%, 38%, and 22% of vascular testing pro-cedures were conducted in IAC facilities in the South, Midwest, and Western regions, respectively). This finding suggests that both the availability and utilization of IAC facilities vary substantially by region, with the greatest proportion of IAC accredited facilities as well as the great-est proportion of vascular testing procedures performed in IAC facilities occurring in the Northeast, and with the smallest proportions of IAC accredited facilities and pro-cedures performed in IAC accredited facilities occurring in the West.
Table 1. Vascular testing procedures by facility type.
Test Total vascular procedures IAC accredited procedures Non-IAC accredited procedures
n=124,184 (%) n=45,470 (37%) n=78,714 (63%)
Extremity venous 52,717 (42) 18,370 (35) 34,347 (65)Cerebrovascular 38,529 (31) 14,139 (37) 24,390 (63)Extremity arterial 27,379 (22) 10,554 (39) 16,825 (61)Visceral vascular 4,846 (4) 2,220 (46) 2,626 (54)Hemodialysis access 713 (1) 187 (26) 526 (74)
by guest on September 2, 2014vmj.sagepub.comDownloaded from

8 Vascular Medicine
Strengths
There are multiple strengths to the study. This is the first study to examine IAC accreditation status (i.e. the propor-tion of IAC accredited versus non-IAC accredited facili-ties) among a sample of Medicare beneficiaries who are undergoing vascular testing at outpatient vascular testing facilities. Prior to this work, there had not been an adequate characterization of accreditation status for vascular testing. The finding of substantial geographic variation in IAC accreditation status of vascular testing facilities, as well as in the proportion of vascular testing procedures that are performed by IAC accredited facilities in each region, sug-gest that there may be geographic/health disparities in the types/quality of health care that may be available by state and by region, which could differentially impact on health care outcomes (and possibly associated health care costs). These characterizations of health care access and quality are of growing importance, given the current implementa-tion of the Affordable Health Care Act, and growing inter-est by the US Government as well as the general public to conduct research to provide information about the best available evidence to help patients and their health care providers make more informed decisions (e.g. Patient-Centered Outcomes Research Institute (PCORI)). Thus, the present study findings may help inform policy makers as well as the general public to make the best possible deci-sions about their health care options, in ways that maximize individual and public health outcomes and that are most cost-effective for society.
Limitations
There are several limitations to this study. The present study used a 5% Outpatient LDS national sample claims data file from CMS to examine the proportion of IAC accredited versus non-IAC accredited facilities, which billed CMS/Medicare for outpatient vascular testing ser-vices in 2011. Although the present study did not use a 100% LDS data file of all outpatient facilities billing CMS, over 95% of the accredited facilities provided to us by the IAC were located within the Outpatient LDS file. This result suggests that, despite this being a small subset of out-patient records, it captured most IAC accredited vascular testing facilities in the US. A second limitation is that the proportion of non-accredited vascular testing facilities was estimated based on the number of providers which bill CMS for vascular testing: This approach may have resulted in an underestimation of the true number of non-accredited facilities (given the possibility of some providers having multiple satellite labs or facilities, but with one POS billing address). If this were to be the case, the true percentage of IAC accredited facilities (out of all facilities that bill CMS for vascular testing, both accredited and non-accredited) may actually be even lower than 13% (i.e. if there are even more non-accredited facilities than providers). Unfortunately, the CMS POS file does not provide the true number of non-accredited facilities (only the number of providers), limiting these data. Therefore, this is a conserv-ative analysis, which may even overestimate the proportion
of IAC accredited facilities out of those facilities that bill CMS for vascular testing. A further limitation is that Inpatient LDS data were not employed in the present analy-ses: Future research should examine the accreditation status of inpatient, as well as outpatient, vascular testing facilities. Moreover, the study focused on Medicare beneficiaries, who comprise the largest group of insured over the age of 65 in the US. Future work should investigate the accredita-tion status of vascular testing facilities among other popula-tions who may not qualify for Medicare but who are in need of vascular testing services, as well as the accreditation sta-tus of facilities who do not accept reimbursement from Medicare/CMS. A further limitation is that data were not available on the credentialing status of non-IAC accredited facilities; however, almost all (over 98% of) IAC facilities had at least one credentialed staff member in 2011 and, on average, more than three-quarters (78%) of technical staff members are credentialed in each IAC facility (Personal Communication, MB Farrell, IAC, June 2014). Although the present analyses identified that 37% of vascular testing procedures were conducted by IAC facilities nationally, future work should examine variation in the volume of the specific vascular testing procedures (CPTs) performed as well as in related diagnoses and health-care costs across IAC accredited versus non-IAC accredited facilities. Finally, the focus of the present study was on IAC accred-ited facilities only, which is an important limitation. Other organizations provide outpatient vascular accreditation (e.g. American College of Radiology (ACR); Joint Commission on Accreditation of Healthcare Organizations (JCAHO), etc.),1,4,9,10 and an important future direction is to determine whether these results exist for other accreditation pathways. Unfortunately, at the time of the present study, it was not possible to obtain data on the proportion of vascu-lar testing facilities that received accreditation from organi-zations other than IAC (e.g. ACR). Future research should therefore investigate these other accreditation organiza-tions for vascular testing, and how these accreditation pro-grams vary as a proportion of all CMS-reimbursed vascular testing facilities by region. The present findings on IAC, as well as those on other accreditation agencies, may help to develop outreach efforts by geographic region and to increase the number of accredited vascular testing facilities nationally and potentially enhance patient safety, quality and utilization control (costs).
Conclusion
The present study identified a low (13%) level of IAC accreditation among all outpatient vascular testing facilities appearing in a 5% national Outpatient Limited Data Set (LDS) of Medicare beneficiaries receiving vascular testing services throughout the US in 2011. Only 37% of all outpa-tient vascular testing procedures identified in this data set were conducted by IAC accredited facilities. Additionally, there was substantial geographic variation in the proportion of IAC accredited facilities among those outpatient vascu-lar testing facilities appearing in this data set. The range of IAC accredited facilities varied significantly by US state
by guest on September 2, 2014vmj.sagepub.comDownloaded from

Rundek et al. 9
and by region, with the greatest proportion of IAC accred-ited outpatient vascular testing facilities in the Northeast (26%) and the smallest proportion in the West (7%). These findings may help develop geographically focused out-reach efforts to increase the number of accredited vascular testing facilities nationwide and therefore potentially improve the quality of their services and improve outcomes for patients, given the high percentage of credentialed tech-nical staff identified within IAC accredited facilities. Increasing the number of accredited vascular testing facili-ties to improve test quality is a hypothesis that should be tested in future research.
Declaration of conflicting interest
T Rundek, SC Brown, K Wang, and C Dong received partial salary support from an IAC Grant (PI: T Rundek). MB Farrell, GV Heller, M Hutchisson, and SL Katanick are paid employees of the IAC. T Rundek, HL Gornik, JF Benenati, MR Jaff, NM Hamburg, MP Lilly, and L Needleman are members of the IAC Vascular Testing Board of Directors. MR Jaff is a Member of the Board of Trustees of VIVA Physicians, a 501(c)(3) not-for-profit education and research organi-zation. MP Lilly is a member of the Board of Directors of the American Registry for Diagnostic Medical Sonography. No other financial disclosures have been reported by the authors of this paper.
Funding
This project was supported by a grant from the Intersocietal Accreditation Commission, ‘Utilization of Vascular Testing in Medicare Beneficiaries: The Role of Ultrasound Laboratory Accreditation’, awarded to Dr Tatjana Rundek (PI). Its contents are solely the responsibility of the authors and do not necessarily represent the views of the IAC. Dr Rundek has been supported by the NINDS K24 NS 062737 award that allowed for protected time for this research.
FundRef Funding Sources: National Institute of Neurological Disorders and Stroke (Grant / Award Number: ‘K24 NS 062737’) Intersocietal Accreditation Commission (Grant / Award Number: ‘Utilization of Vascular Testing in Medicare Beneficiaries: The Role of Ultrasound Laboratory Accreditation’).
References
1. US Government Accountability Office (GAO). Medicare ultrasound procedures: consideration of payment reforms and technician qualification requirements. Report no. GAO-07–734, 28 June 2007, http://www.gao.gov/products/GAO-07–734 (2007, accessed 14 May 2014).
2. Gornik HL, Hutchisson M, Khan M, et al. Diagnostic cri-teria for ultrasound diagnosis of internal carotid artery stenosis vary widely among accredited vascular testing
laboratories. A survey from the Intersocietal Commission for the Accreditation of Vascular Laboratories (ICAVL). Circulation 2011; 124(Suppl 1): A8918.
3. Gornik HL, Needleman N, Benenati J, et al. Support for standardization of duplex ultrasound diagnostic criteria for internal carotid artery stenosis: a survey from the Intersocietal Accreditation Commission (IAC). J Am Coll Cardiol 2013; 61(10_S): E2020. doi:10.1016/S0735-1097(13)62020-3.
4. Heller GV, Katanick SL, Sloper T, et al. Accreditation for cardiovascular imaging: setting quality standards for patient care. JACC: Cardiovascular Imaging 2008; 1: 390–397.
5. Intersocietal Accreditation Commission (IAC). What is IAC accreditation? www.intersocietal.org/iac/accreditation/wha-tisaccreditation.htm (2014, accessed 14 May 2014).
6. Intersocietal Accreditation Commission (IAC). Directory of IAC accredited facilities. www.intersocietal.org/iac/helpful-resources/lab_list.htm (2014, accessed 14 May 2014).
7. Brown OW, Bendick PJ, Bove PG, et al. Reliability of extracranial carotid artery duplex ultrasound scanning: value of vascular laboratory accreditation. J Vasc Surg 2004; 39: 366–371.
8. Intersocietal Commission for the Accreditation of Computed Tomography Laboratories (ICACTL). ICACTL: a division of the Intersocietal Accreditation Commission. www.entnet.org/Practice/upload/ICACTL-Overview.ppt (accessed 14 May 2014).
9. American College of Radiology (ACR). Ultrasound accred-itation program requirements, updated 10 April 2014, www.acr.org/~/media/ACR/Documents/Accreditation/US/Requirements.pdf (2014, accessed 7 July 2014).
10. The Joint Commission. 2014 Ambulatory care overview: a snapshot of the accreditation process. www.jointcommis-sion.org/assets/1/6/2014_AHC_Overview_Guide.pdf (2014, accessed 7 July 2014).
11. Intersocietal Accreditation Commission (IAC). IAC stand-ards and guidelines for vascular testing accreditation, updated 15 June 2013, www.intersocietal.org/vascular/stand-ards/IACVascularTestingStandards2013.pdf (2013, accessed 14 May 2014).
12. Intersocietal Accreditation Commission (IAC). About the IAC. http://intersocietal.org/vascular/ (2014, accessed 14 May 2014).
13. US Census Bureau. Census regions and divisions of the United States. www.census.gov/geo/maps-data/maps/pdfs/reference/us_regdiv.pdf (2013, accessed 14 May 2014).
14. American Society of Echocardiology (ASECHO). Sonography licensure FAQS. www.asecho.org/sonographyl-icensurefaqs/ (2014, accessed 14 May 2014).
15. Intersocietal Accreditation Commission (IAC). CMS pay-ment policies (by state), updated 15 April 2014, www.intersocietal.org/iac/reimbursement/policies/IACVascular_CMSPaymentPolicies.pdf (2014, accessed 14 May 2014).
by guest on September 2, 2014vmj.sagepub.comDownloaded from