Microsoft Word - 6730822-file00Validation of the Hematopoietic Cell
Transplantation-Specific Comorbidity Index: a prospective,
multicenter GITMO study Roberto Raimondi1, Alberto Tosetto1, Rosi
Oneto2 , Riccardo Cavazzina1, Francesco Rodeghiero1, Andrea
Bacigalupo2 , Renato Fanin3, Alessandro Rambaldi4 and Alberto Bosi5
1 Department of Hematology, S. Bortolo Hospital, Vicenza, Italy; 2
Division of Hematology, Ospedale San Martino, Genova, Italy ; 3
Department of Hematology, Azienda Ospedaliera, Università di Udine,
Italy; 4 Hematology and Bone Marrow Unit, Ospedali Riuniti,
Bergamo, Italy; 5 Department of Hematology, Azienda Ospedaliera di
Careggi e Università di Firenze, Italy Correspondence to: Dr.
Roberto Raimondi, Hematology Department, S. Bortolo Hospital, Via
Rodolfi 37, 36100 Vicenza, Italy (phone: 0039-0444-753626; fax:
0039-0444-920708; e-mail:
[email protected])
Blood First Edition Paper, prepublished online June 27, 2012; DOI
10.1182/blood-2012-03-414573
Copyright © 2012 American Society of Hematology
For personal use only.on December 24, 2018. by guest
www.bloodjournal.orgFrom
decision. Recently, the Hematopoietic Cell Transplantation-Specific
Comorbidity Index (HCT-CI)
has been associated with increased NRM risk in several
retrospective studies, but its clinical utility
has never been demonstrated prospectively in an adequately sized
cohort. To this aim, we
prospectively evaluated a consecutive cohort of 1937 patients
receiving HSCT in Italy over two
years. HCT-CI was strongly correlated with both two-year NRM
(14.7%, 21.3% and 27.3% in
patients having an HCT-CI score of 0, 1-2, and ≥ 3 respectively)
and OS (56.4%, 54.5%, and 41.3%
respectively). There was an excellent calibration between the
predicted and observed two-year
NRM in patients having an HCT-CI score of 0 and 1-2, whereas in the
≥ 3 group the predicted
NRM overestimated the observed NRM (41% vs. 27.3%). HCT-CI alone
was the strongest
predictor of NRM in patients with lymphoma, myelodisplastic
syndrome, and acute myeloid
leukemia in first remission (c-statistics 0.66, 064 and 0.59
respectively). We confirm the clinical
utility of the HCT-CI score that could also identify patients at
low NRM risk possibly benefiting
from a HSCT-based treatment strategy.
For personal use only.on December 24, 2018. by guest
www.bloodjournal.orgFrom
and non-malignant hematological disorders. In the recent years,
novel approaches such as the
reduced-intensity conditioning regimens have expanded the use of
HSCT also to elderly patients or
to patients otherwise ineligible for conventional transplants. HSCT
still remains associated with a
significant mortality and morbidity although the Seattle team has
recently observed a substantial
reduction of nonrelapse mortality (NRM) and overall mortality in
the last years 1. Careful
assessment of risks and benefits prior to transplantation remains
however an essential issue. Three
major factors influence nonrelapse mortality and overall survival
(OS) after HSCT: the patient’s
disease, the type of transplant procedure and donor, and the
patient’s risk profile, which includes
age, performance status and presence of comorbidities. In an
attempt to improve quantification of
the patient’s risk profile, Sorror et al. recently proposed the
Hematopoietic Cell Transplantation-
Specific Comorbidity Index (HCT-CI) developed from a single-center
retrospective analysis and
internal validation 2. The HCT-CI demonstrated to capture more
pretransplant comorbidities than
the previously used Charlson Comorbidity Index and to provide
better assessment of NRM,
defining three risk groups, respectively with HCT-CI score of 0
(low-risk), 1-2 (intermediate risk)
and ≥ 3 (high-risk) showing linear predictions of NRM and OS.
On this premise, the HCT-CI score has been included as an
eligibility criterion in some clinical
trials, but it has never been externally validated by a large
multicenter longitudinal study.
Furthermore, it is not known how the clinical usefulness of the
HCT-CI applies to all the different
malignant hematologic diseases or if its use should be preferably
restricted to selected disorders. In
this study, we prospectively collected comorbidity data to compute
the HCT-CI score in a
consecutive series of patients undergoing allogeneic bone marrow
transplantation in Italy. The
primary aim of the study was to externally validate the HCT-CI in
terms of calibration and
discrimination in a multicenter, prospective study setting. As a
secondary aim, we evaluated the
usefulness of the HCT-CI in different patient subgroups.
For personal use only.on December 24, 2018. by guest
www.bloodjournal.orgFrom
and belonging to the national bone marrow transplantation network
(Gruppo Italiano Trapianto di
Midollo Osseo, GITMO) were asked to participate in this
prospective, multicenter observational
study. As it is mandatory for any GITMO center to enter information
for all their consecutive
transplants into the European Bone Marrow Transplantation (EBMT)
database (Promise, Project
Manager Internet Service, http://www.ebmt.org), we first updated
the Minimum Essential Data
section (MED-A) of the Promise database to include questions
specifically assessing the
presence/absence of all the comorbidities required to calculate the
HCT-CI score. Permission to
perform this study was obtained from the GITMO Clinical Studies
Board. All patients provided
informed consent in accordance with the Declaration of Helsinki for
the analysis of their clinical
data.
Eligibility criteria. Per protocol, we considered eligible for
analysis only those first transplants
performed from January 1st 2008 to February 1st 2011 on patients
> 18 years for malignant or non-
malignant hematological disease, and using peripheral blood stem
cells (PBSC) or bone marrow
(BM) as cell source (thus excluding cord blood cells). This
time-frame was chosen because from
preliminary analysis of previous enrollment data it was expected to
yield at least about 200 cases for
each of four pre-specified diagnoses (acute leukemias; non-Hodgkin
lymphomas; multiple
myeloma; myelodisplastic syndromes).
Definitions. According to the EBMT criteria 3, we considered as
myeloablative (MAC) any regimen
with a total busulfan dose > 8 mg/kg, or cyclophosphamide dose
> 120 mg/kg (or > 60 mg/kg if in
combination with other drugs) , or melphalan dose > 140 mg/m2 or
TBI dose > 6 Gy; reduced
intensity/non myeloablative conditioning regimens (RIC) were all
others regimens with dosages
below the above mentioned limits. According to the original paper
of Sorror et al., we defined acute
leukemia in first complete remission, chronic myeloid leukemia in
chronic phase and
myelodisplastic syndrome-refractory anemia as low risk diseases;
high risk diseases were all other
diagnoses 2.
Follow-up procedures. Nonrelapse mortality (NRM) was defined as
death from nonrelapse causes;
overall survival (OS) was defined as the time from transplantation
to death for any cause. Data was
censored at time of death or last available follow-up, as available
from the mandatory EBMT update
from each GITMO Center.
Statistical Methods. Multiple imputation was used to account for
sporadic missing values in
covariates other than those affecting the HCT-CI, to allow
multivariate analyses be carried in the
whole dataset, using the Stata mi impute procedure 4. Competing
risks analysis was used to
For personal use only.on December 24, 2018. by guest
www.bloodjournal.orgFrom
calculate the 12 and 24 months NRM cumulative incidence, using the
Gray’s test to test differences
between HCT-CI score groups 5,6. Overall Survival (OS) was
estimated using the Kaplan-Meier
method; hazard ratios were computed between subgroups using Cox
regression for OS and
competing risk regression for NRM, both stratified for centre.
Competing risk regression was used
to compute NRM cumulative incidence rates, considering
non-transplant mortality as the competing
event. The predictive ability of the HCT-CI score was assessed
using time-dependent receiver-operator
curves (ROC) analysis 7. All computations were performed using
Stata and the procedures cmprsk
and survivalROC of the R statistical package 8,9.
Results Patients. 44/46 (95.6%) of all GITMO centres performing
HSCTs in adult patients agreed to
participate in the study. From 3318 HSCTs performed during the
considered time-frame by the
enrolling Centres, 1937 were available for analysis. The reasons
for exclusion from the study were:
comorbidities not reported (n=1167), second or more transplants
(n=111), incomplete follow-up
data (n=55), non-hematologic diseases (n=31), lost to follow-up
(n=17). There were no material
differences in terms of OS and NRM between the 1937 evaluated
patients and the 1167 who were
excluded because of failure to report comorbidities (24 months OS,
53.9% [95% CI 50.8-56.8] vs.
56.6% [95% CI 52.5-60.5], p=0.23, respectively in the
evaluated/excluded groups; 24 months NRM
23.8% [95% CI 21.3-26.5] vs. 26.1% [95% CI 23.3-30.6], p=0.15 in
the evaluated/excluded
groups).
Table 1 reports the main characteristics and the prevalence of
comorbidities in the cohort, 1119
patients (58%) being classified as low risk (HCT-CI score=0), 441
(23%) as intermediate risk
(HCT-CI score=1-2) and 377 (19%) as high risk group (HCT-CI
score≥3).
Follow-up. Patient’s follow-up totalled 1681 patient-years with a
median time of 10.1 months from
transplant (range 0.03-38.77). During follow-up, 666 deaths were
observed in the cohort (332
NRM, 334 disease-related deaths). At multivariate analysis, HCT-CI
score, age above 50 years,
high-risk disease and unrelated donor were all associated with
increased NRM and decreased OS
(Table 2). HCT-CI score and high-risk disease were the strongest
predictors of both NRM and OS,
as apparent from multivariate analysis. Table 3 and Figure 1 report
the overall survival and NRM
for the low, intermediate and high risk HCT-CI score groups.
NRM prediction using the HCT-CI score. To validate the predictive
ability of the HCT-CI score, we
compared its performance in our dataset in terms of calibration and
discrimination 10,11. Two-year
For personal use only.on December 24, 2018. by guest
www.bloodjournal.orgFrom
NRM cumulative incidences, accounting for competing risks, and OS
were used to compare the
calibration of the HCT-CI model, and are presented in Figure 1 and
Figure 2 and stratified
according to different clinical conditions in Table 4. Figure 3
presents NRM and OS probabilities
stratified for reduced intensity or myeloablative conditioning
regimens and HCT-CI, after Cox (OS)
or competing-risk regression (NRM) adjustment for all the variables
presented in Table 2.
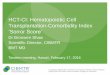
Increasing HCT-CI score confirmed to be associated with higher 1-
and 2-year probability of NRM
and with lower OS, with a double NRM and overall mortality risk in
those patients having a score ≥
3. However, while the Sorror’s two-year predicted NRM nearly
overlapped those observed in our
cohort for low and intermediate-risk HCT-CI scores, the HCT-CI
predicted two-year NRM did
overestimate the observed two-year NRM for the high-risk category
(41% vs. 27.3% respectively,
Figure 4).
In terms of discriminatory capability, the HCT-CI score showed a
c-value of 0.60 and 0.54 for
NRM and OS, respectively. Pre-specified subgroup analysis disclosed
significant differences in
NRM prediction by the HCT-CI score, being higher in patients
undergoing transplantation for
lymphoma, myelodisplastic syndrome, and acute myeloid leukemia in
first remission (Table 4). In
contrast, in patients with multiple myeloma the predictive ability
was lower, with no clear NRM
gradient between the three HCT-CI score groups and the lowest
observed c-value.
Finally, we assessed the accuracy of data collected for HCT-CI
scoring on a random set of 244
patients. These audits were made at the participating sites by
researchers independent from the
original abstractors, who recalculated from the patient charts the
HCT-CI score completely blinded
from the previous results. Discrepant results were observed in
26/244 patients, resulting in a shift of
the HCT-CI score group in 9.8% of the audited sample: 13/26 had an
increased HCT-CI score,
11/26 a decreased score and in two cases the score remained
unchanged (though with different
individual comorbidities). However, there were no differences
between the original and recalculated
mean HCT-CI score (1.58 vs. 1.60, p=0.66), and there were no
differences in terms of NRM
predictive ability between the original and recalculated HCT-CI, (c
statistic 0.699 vs. 0.700,
p=0.911; both adjusted for age, sex, high-risk disease, donor type,
stem cell source).
Discussion
In this study we primarily aimed at externally validate the
Hematopoietic Cell Transplantation-
Specific Comorbidity Index (HCT-CI), a widely used prognostic index
originally proposed in 2005 2 whose usefulness has been
subsequently reported only in studies based on limited,
retrospective
and mostly single-center patient series 12-46. To this aim, we
prospectively enrolled a wide cohort of
unselected patients consecutively undergoing allogeneic bone marrow
transplantation in Italy, and
For personal use only.on December 24, 2018. by guest
www.bloodjournal.orgFrom
evaluated the NRM and OS predictive ability of the HCT-CI applying
the same selection criteria
originally used by Sorror et al. 2. At our knowledge, this is the
first study aimed to validate the
HCT-CI in a prospective large cohort analysis using a multicentre
national registry.
As a first result, we were able to confirm that the HCT-CI is an
independent predictor of both NRM
and OS. However, while we observed a very good linear correlation
between the predicted and the
observed NRM in patients having a HCT-CI score of 0 and 1-2, the
observed NRM were
considerably lower in patients having a HCT-CI score greater than
2. This finding therefore reduces
the overall predictive value of the HCT-CI score, as indicated by a
lower discriminatory c-value in
our study (0.60 vs. 0.65 reported by Sorror et al 2) and could be
partly explained by an overfitting of
the original regression model, a well-known statistical artifact
that justifies the need for validation
in external cohorts 11. The reliability of the HCT-CI scoring is
another important issue, particularly
in multicenter studies, in which exposure misclassification could
be a consequence both of intra and
between-Centers variability, and reduces the degree of association
between HCT-CI and NRM. To
assess the degree of intra-Centers data accuracy, we performed an
audit on about 12% of patient
charts, finding only minimal changes in HCT-CI score that did not
affect the final results of our
study. Between-Centers variability could not be formally evaluated
in our study, but we tackle this
issue by stratifying our analyses for centers. Finally, another
possible explanation of the different
predictive capability of the HCT-CI score could well be the higher
percentage of patients
transplanted for myelodisplastic syndrome and chronic myeloid
leukemia in the Sorror’s cohort. In
these two disease subgroups, our analysis disclosed that the NRM is
remarkably high in those
patients having a HCT-CI score ≥ 3. Therefore, an additional
explanation of the reduced observed
NRM in patients with an HCT-CI score ≥ 3 could therefore lie in the
different sample composition
of our cohort.
Additional major differences exist between our study population and
the population of the original
study of Sorror et al. First, we analysed only adult patients.
Second, our cohort had a different
composition in terms of a higher percentage of high risk diseases
(69% vs. 41%) and of unrelated
donors (50% vs. 42%), more infections (11% vs. 4%) but less
psychiatric (3% vs. 9%), mild hepatic
(5% vs. 16%) and mild pulmonary (10% vs. 24%) comorbidities. Our
cohort showed a higher
proportion of patients having an HCT-CI score of 0. It is however
worthwhile to note that in our
cohort the baseline two-year NRM risk in patients with a HCT-CI
score of 0 was 14.7%, a figure
that nearly overlaps the Sorror’s predicted NRM (14%). Therefore,
despite the unavoidable
differences in patient composition and the different (prospective)
design of our study, the
For personal use only.on December 24, 2018. by guest
www.bloodjournal.orgFrom
and the generalizability of the HCT-CI.
Pre-specified subgroup analyses showed that in patients having a
HCT-CI score equal to 0 the NRM
was similar for myeloablative and
reduced-intensity/non-myeloablative conditioning regimens,
while in patients having a HCT-CI score ≥ 1 the use of
reduced-intensity/non-myeloablative
conditioning regimens was correlated with lower NRM rates during
the first year. After the first
year, however, the myeloablative group reaches a plateau whereas in
the reduced-intensity/non-
myeloablative conditioning regimen group, NRM continues to
increase. The advantage of related
donor compared with unrelated donor is evident across all the
HCT-CI risk groups, but in the
setting of transplant from related donor the absence (HCT-CI score
= 0) or presence (HCT-CI score
≥ 1) of comorbidities show a significant impact on NRM.
As a secondary finding, we demonstrated that the predictive ability
of HCT-CI was higher in
patients having lymphoma, as already reported, 21,26,27 or
myelodisplastic syndrome (MDS), as
already reported, 14,15,18,28,29 and in those receiving PBSCs as
stem cell source. On the other hand,
the predictive value was much lower in patients having acute
leukemias. However, since the
decision to offer elective HSCT in patients with acute myeloid
leukemia (AML) in first complete
remission without high-risk characteristics is controversial, we
analysed separately the 413 AML
patients who received HSCT in first remission. In these patients,
the 2-year NRM was 9.1%, 11.4%,
and 19.4% for the HCT-CI score groups 0, 1-2, ≥3 respectively.
Although these findings should be
taken very cautiously given the lack of randomization to HSCT in
our cohort, they nonetheless
suggest that the NRM risk in selected patients with no or few
comorbidities could be very limited,
and below the reported rate of death attributable to disease
relapse even in patients with AML at
low risk of relapse (estimated to be around 20% 47). The same
reasoning may be applied to patients
with lymphoma or myelodisplastic syndrome, since the NRM risk is
increased more than two-folds
in patients having an HCT-CI ≥3 as compared with those having a
score equal to 0. Therefore, our
study further support the need for appropriately designed studies
investigating HSCT transplant in
those patients having a low HCT-CI score predicting a low NRM
risk.
In an additional subgroup analysis, we evaluated the predictive
role of HCT-CI in patients
undergoing reduced-intensity or myeloablative conditioning
regimens. Given the observational
nature of our study, we used a multivariate approach to weight the
reciprocal contributions of HCT-
CI and conditioning regimens to overall survival and transplant
related mortality, adjusted for high-
risk disease, age and donor type. In this analysis, HCT-CI was a
determinant of both OS and NRM,
For personal use only.on December 24, 2018. by guest
www.bloodjournal.orgFrom
while type of conditioning was related to OS but not with NRM, a
finding that seems in keeping
with a previously published report in a smaller series 19. Our
results support the hypothesis that
HCT-CI score groups and myeloablative conditioning have an
apparently additive effect in
predicting survival: for instance, two-years survival is similarly
reduced by an HCT-CI score 1- 2 in
patients receiving RIC or by an HCT-CI score 0 in patients
receiving MAC.
A possible limitation of the present study is the unavailability of
the HCT-CI in a relevant fraction
of all potentially eligible patients, since 1167/3318 (35%) were
excluded from analysis because,
despite that the study formally started on January 1st 2008, some
GITMO Centres started to
prospectively enter comorbidity data into the MEDAB database with
some delay. This explains why
several patients (potentially eligible for study, since they
received BMT in the per-protocol time-
frame) were considered as missing. However, we did not observed any
difference both in terms of
OS and NRM between those patients in whom comorbidities were
reported and those without,
supporting the validity of our study and the absence of a relevant
selection bias.
To summarize, in the largest recent cohort of unselected patients
undergoing HSCT so far
described, we were able to confirm the clinical utility of the
HCT-CI score, although with a slightly
reduced discriminant capability. Furthermore, our findings suggest
that the HCT-CI could have the
potential to identify patients at low NRM risk that could benefit
from a more intensive, transplant-
based treatment strategy in selected disease subgroups. This latter
finding needs to be further
explored by appropriately designed randomized clinical
trials.
For personal use only.on December 24, 2018. by guest
www.bloodjournal.orgFrom
Contributions: R.R., A. Bosi, and R.F. designed the research; R.R.
and R.O. collected data; R.R., A.T., F.R., R.F., A.R.,
A. Bosi, A. Bacigalupo analyzed and interpreted data; R.C.
performed statistical analysis; R.R and A.T. wrote the
paper.
Acknowledgments
This work was supported in part by grants from Fondazione Progetto
Ematologia (Hematology Project Foundation,
Vicenza, Italy) and AViLL/AIL (Associazione Vicentina per le
Leucemie, i Linfomi e il Mieloma/Associazione Italiana
Leucemie, Vicenza, Italy).
R.R. thanks Michela Trentin for her support in data
collection.
The Authors thank Caterina Micò, Irene Donnini, Alessandra Sperotto
and Carlo Borghero for the audit re-evaluation of
patients’ charts.
Appendix
The authors wish to thank the colleagues of the following
institutions (GITMO centers) in Italy that contributed to the
study: Department of Hematology; Nuovo Ospedale Torrette, Ancona
(P. Leoni); Division of Hematology, Ospedale
S.G. Moscati, Ascoli Piceno (P. Galieni); Division of Hematology,
Ospedale “S. S. Antonio e Biagio” Alessandria (A.
Levis); Division of Hematology, University of Bari, Bari (G.
Specchia); Division of Hematology, Ospedali Riuniti,
Bergamo (A. Rambaldi); Institute of Hematology and Clinical
Oncology “L. A. Seragnoli,” Ospedale “S. Orsola-
Malpighi,” University of Bologna, Bologna (G. Bandini, M.
Baccarani); Department of Hematology, Ospedale
Regionale, Bolzano (M. Casini, S. Cortelazzo); Bone Marrow
Transplant Center, Spedali Civili, Brescia (D. Russo);
Division of Hematology and Bone Marrow Transplant Center, Ospedale
Oncologico “A. Businco,” Cagliari (E.
Angelucci, D. Baronciani); Bone Marrow Transplantation Unit,
Ospedale “R. Binaghi,” University of Cagliari, Cagliari
(G. La Nasa); Division of Hematology and Bone Marrow
Transplantation, Ospedale “Ferrarotto,” Catania (G. Milone);
Division of Hematology, Ospedale “S. Croce e Carlo,” Cuneo (N.
Mordini); Department of Hematology, Ospedale
“Careggi,” University of Florence, Firenze (A. Bosi, S. Guidi);
Division of Hematology, Ospedale “S. Martino,”
Genova (A. Bacigalupo, M. T. Van Lint); Hematology–Bone Marrow
Transplantation Unit, Istituto Nazionale dei
Tumori, University of Milano, Milano (P. Corradini); Istituto
Europeo di Oncologia, Milano (G. Martinelli);
Division of Hematology Ospedale “Cà Granda” Niguarda, Milano (E.
Morra, P. Marenco); Department of Hematology,
Fondazione IRCCS Ospedale Maggiore Policlinico, Mangiagalli e
Regina Elena, Milano (G. Lambretenghi Deliliers, F.
Onida); Hematology and Bone Marrow Transplantation Unit, S.
Raffaele Scientific Institute, Milano (F. Ciceri, J.
Peccatori); Transplantation Unit Department of Oncology-Hematology,
IRCCS Clinica Humanitas, Rozzano (L.
Castagna); Department of Oncology and Hematology University of
Modena and Reggio Emilia, Modena (F. Narni);
Division of Hematology and Transplant Unit, Ospedale “S. Gerardo,”
University of Milano-Bicocca, Monza (P.
Pioltelli); Division of Hematology, University of Napoli “Federico
II” Medical School, Napoli (C. Selleri); Division of
Hematology and Transplant Unit, Ospedale “V. Cervello,” Palermo (R.
Scimè); Department of Oncology, Hematology
Unit, Ospedale “La Maddalena,” Palermo (M. Musso); Division of
Hematology, University of Pavia, Fondazione
For personal use only.on December 24, 2018. by guest
www.bloodjournal.orgFrom
Salvatore,” Pesaro (G. Visani); Department of Hematology, Ospedale
Civile, Pescara (P. Di Bartolomeo); Oncology
and Hematology Department, Ospedale “Guglielmo da Saliceto,”
Piacenza (D. Vallisa, L. Cavanna); Division of
Hematology, Univeristy of Pisa, Pisa (M. Petrini, F. Papineschi);
Transplant Unit “A. Neri,” Ospedale “Bianchi-
Melacrino-Morelli,” Reggio Calabria (P. Iacopino, G. Messina);
Hematology Unit, Arcispedale “S. Maria Nuova,”
Reggio Emilia (F. Merli, L. Gugliotta); Division of Hematology,
Department of Cellular Biotechnologies and
Hematology, University “La Sapienza” (A. P. Iori, R. Foà);
Hematology and Stem Cell Transplantation Unit Ospedale
“S. Camillo,” Roma (A. Locasciulli, I. Majolino); Division of
Hematology, University “Cattolica S. Cuore”, Roma (G.
Leone, S. Sica); Hemato-Oncology Transplant Unit, University “Tor
Vergata,” Transplant Network, Roma (W.
Arcese); Unit of Hematology and Bone Marrow Transplantation, IRCCS,
“Casa Sollievo della Sofferenza,” S. Giovanni
Rotondo (A. M. Carella, N. Cascavilla); Division of Hematology and
Bone Marrow Unit, Azienda Ospedaliera
Universitaria Senese “S. Maria alle Scotte”, Siena (G. Marotta);
Institute of Hematology, Ospedale “San Giusepppe
Moscati”, Taranto (P. Mazza); Division of Hematology, Ospedale “S.
Giovanni Battista,” Torino (M. Falda, B. Bruno);
Division of Hematology, Ospedale “C. Panico”, Tricase (V. Pavone);
Division of Hematology and Bone Marrow
Transplantation, University of Udine, Udine (R. Fanin, F.
Patriarca); Division of Hematology and Bone Marrow Unit,
Policlinico “G.B. Rossi”, Verona (G. Pizzolo, F. Benedetti);
Department of Hematology, Ospedale “S. Bortolo,”
Vicenza (F. Rodeghiero, R. Raimondi).
For personal use only.on December 24, 2018. by guest
www.bloodjournal.orgFrom
1. Gooley TA, Chien JW, Pergam SA, et al. Reduced mortality after
allogeneic hematopoietic- cell transplantation. N Engl J Med.
2010;363(22): 2091-2101.
2. Sorror ML, Maris MB, Storb R, et al. Hematopoietic cell
transplantation (HCT)-specific comorbidity index: a new tool for
risk assessment before allogeneic HCT. Blood. 2005;106(8):
2912-2919.
3. MED-AB FORMS MANUAL. http://www.ebmt.org/Contents/Data-
Management/Registrystructure/MED-ABdatacollectionforms/Documents/MED-
ABFormsManual.pdf . Accessed 24 Feb 2012.
4. Steyerberg E. Clinical Prediction Models: Springer-Verlag;
2010.
5. Prentice RL, Kalbfleisch JD, Peterson AV, Flournoy N, Farewell
VT, Breslow NE. The Analysis of Failure Times in the Presence of
Competing Risks. Biometrics . 1978;34(4): 541-554.
6. Fine J, Gray R. A Proportional Hazards Model for the
Subdistribution of a Competing Risk. J Am Stat Assoc. 1999;94(446):
496-509.
7. Heagerty PJ, Lumley T, Pepe MS. Time-dependent ROC curves for
censored survival data and a diagnostic marker. Biometrics.
2000;56(2): 337-344.
8. StataCorp. Stata Statistical Software: Release 11.0. College
Station, TX: Stata Corporation; 2010.
9. Team RD. R: A language and environment for statistical
computing. Vienna: R Foundation for Statistical Computing;
2011.
10. Moons KGM, Altman DG, Vergouwe Y, Royston P. Prognosis and
prognostic research: application and impact of prognostic models in
clinical practice. BMJ 2009;338:b606
11. Moons KGM, Royston P, Vergouwe Y, Grobbee DE, Altman DG.
Prognosis and prognostic research: what, why, and how? BMJ
2009;338:b375.
12. Kerbauy DMB, Chyou F, Gooley T, et al. Allogeneic hematopoietic
cell transplantation for chronic myelomonocytic leukemia. Biol
Blood Marrow Transplant. 2005;11(9): 713-720.
13. Baron F, Storb R, Storer B, et al. Factors associated with
outcomes in allogeneic hematopoietic cell transplantation with
nonmyeloablative conditioning after failed myeloablative
hematopoietic cell transplantation. J Clin Oncol. 2006;24(25):
4150-57.
14. Martino R, Valcaircel D, Brunet S, Sureda A, Sierra J.
Comparable non-relapse mortality and survival after HLA-identical
sibling blood stem cell transplantation with reduced or
conventional-intensity preparative regimens for high-risk
myelodysplasia or acute myeloid leukemia in first remission. Bone
Marrow Transplant. 2008;41(1): 33-38.
15. Boehm A, Sperr WR, Leitner G, et al. Comorbidity predicts
survival in myelodysplastic syndromes or secondary acute myeloid
leukaemia after allogeneic stem cell transplantation. Eur J Clin
Invest 2008;38(12): 945-52.
For personal use only.on December 24, 2018. by guest
www.bloodjournal.orgFrom
18. Sorror ML, Sandmaier BM, Storer B, et al. Comorbidity and
disease status based risk stratification of outcomes among patients
with acute myeloid leukemia or myelodysplasia receiving allogeneic
hematopoietic cell transplantation. J Clin Oncol. 2007;25(27):
4246-54 .
19. Majhail NS, Brunstein CG, McAvoy S, et al. Does the
hematopoietic cell transplantation specific comorbidity index
predict transplant outcomes? A validation study in a large cohort
of umbilical cord blood and matched related donor transplants. Biol
Blood Marrow Transplant. 2008;14(9): 985-992.
20. Xhaard A, Porcher R, Chien JW, et al. Impact of comorbidity
indexes on non-relapse mortality. Leukemia. 2008;22(11):
2062-2069.
21. Sorror ML, Storer B, Maloney D, Sandmaier BM, Martin PJ, Storb
R. Outcomes after allogeneic hematopoietic cell transplantation
with nonmyeloablative or myeloablative conditioning regimens for
treatment of lymphoma and chronic lymphocytic leukemia. Blood.
2008;111(1): 446- 452.
22. Sorror ML, Storer B, Sandmaier BM, et al. Five-year follow-up
of patients with advanced chronic lymphocytic leukemia treated with
allogeneic hematopoietic cell transplantation after
nonmyeloablative conditioning. J Clin Oncol. 2008;26(30):
4912-4920.
23. Mohty M, M. L, Basara N. Association Between the Hematopoietic
Cell Transplantation- Specific Comorbidity Index (CI) and
Non-Relapse Mortality (NRM) after reduced intensity conditioning
(RIC) allogeneic Stem Cell transplantation (allo-SCT) for Acute
Myeloid Leukemia (AML) in. Blood (ASH Annual Meeting).
2009;114:Abstract 650.
24. Guilfoyle R, Demers A, Bredeson C, et al. Performance status,
but not the hematopoietic cell transplantation comorbidity index
(HCT-CI), predicts mortality at a Canadian transplant center. Bone
Marrow Transplant. 2009;43(2): 133-139.
25. Sorror ML, Storer B, Sandmaier BM, et al. Hematopoietic cell
transplantation-comorbidity index and Karnofsky performance status
are independent predictors of morbidity and mortality after
allogeneic nonmyeloablative hematopoietic cell transplantation.
Cancer. 2008;112(9): 1992-2001.
26. Farina L, Bruno B, Patriarca F, et al. The hematopoietic cell
transplantation comorbidity index (HCT-CI) predicts clinical
outcomes in lymphoma and myeloma patients after reduced- intensity
or non-myeloablative allogeneic stem cell transplantation.
Leukemia. 2009;23(6): 1131- 1138.
27. Pollack S, Steinberg S, Odom J, Dean R, Fowler D, Bishop M.
Assessment of the hematopoietic cell transplantation comorbidity
index in non-Hodgkin lymphoma patients receiving reduced-intensity
allogeneic hematopoietic stem cell transplantation. Biol Blood
Marrow Transplant. 2009;15(2): 223-230.
For personal use only.on December 24, 2018. by guest
www.bloodjournal.orgFrom
29. Lee JH, Lee JH, Lim SN, et al. Allogeneic hematopoietic cell
transplantation for myelodysplastic syndrome: prognostic
significance of pre-transplant IPSS score and comorbidity. Bone
Marrow Transplant. 2010;45(3): 450-457.
30. DeFor TE, Majhail NS, Weisdorf DJ, et al. A modified
comorbidity index for hematopoietic cell transplantation. Bone
Marrow Transplant. 2010;45(5): 933-938.
31. Kataoka K, Nannya Y, Ueda K, Kumano K, Takahashi T, Kurokawa M.
Differential prognostic impact of pretransplant comorbidity on
transplant outcomes by disease status and time from transplant: a
single Japanese transplant centre study. Bone Marrow Transplant.
2010;45(3): 513-520.
32. Terwey T, Hemmati P, Martus P, et al. A modified EBMT risk
score and the hematopoietic cell transplantation-specific
comorbidity index for pre-transplant risk assessment in adult acute
lymphoblastic leukemia. Haematologica. 2010;95(5): 810-818.
33. Barba P, Pinana JL, Martino R, et al. Comparison of two
pretransplant predictive models and a flexible HCT-CI using
different cut off points to determine low-, intermediate-, and
high-risk groups: the flexible HCT-CI Is the best predictor of NRM
and OS in a population of patients undergo. Biol Blood Marrow
Transplant. 2010;16(3): 413-420.
34. Pavlu J, Kew A, Taylor-Roberts B, et al. Optimizing patient
selection for myeloablative allogeneic hematopoietic cell
transplantation in chronic myeloid leukemia in chronic phase.
Blood. 2010;115(20): 4018-4020.
35. Gyurkocza B, Storb R, Storer B, et al. Nonmyeloablative
allogeneic hematopoietic cell transplantation in patients with
acute myeloid leukemia. J Clin Oncol. 2010;28(17): 2859-2867.
36. Patel P, Sweiss K, Nimmagadda S, Gao W, Rondelli D. Comorbidity
index does not predict outcome in allogeneic myeloablative
transplants conditioned with fludarabine/i.v. busulfan (FluBu4).
Bone Marrow Transplant. 2011;46(10): 1326-1330.
37. Warlick E, Tomblyn M, Cao Q, et al. Reduced-intensity
conditioning followed by related allografts in hematologic
malignancies: long-term outcomes most successful in indolent and
aggressive non-Hodgkin lymphomas. Biol Blood Marrow Transplant.
2011;17(7): 1025-1032.
38. Eissa H, Gooley TA, Sorror ML, et al. Allogeneic hematopoietic
cell transplantation for chronic myelomonocytic leukemia:
relapse-free survival is determined by karyotype and comorbidities.
Biol Blood Marrow Transplant. 2011;17(6): 908-915.
39. Castagna L, Furst M, Marchetti N, et al. Retrospective analysis
of common scoring systems and outcome in patients older than 60
years treated with reduced-intensity conditioning regimen and
alloSCT. Bone Marrow Transplant. 2011;46(7): 1000-1005.
40. El Kourashy S, Williamson T, Chaudhry MA, et al. Influence of
comorbidities on transplant outcomes in patients aged 50 years or
more after myeloablative conditioning incorporating fludarabine, BU
and ATG. Bone Marrow Transplant. 2011;46(8): 1077-1083.
For personal use only.on December 24, 2018. by guest
www.bloodjournal.orgFrom
42. McCormack S, Cao Q, Oran B, Weisdorf D, Warlick E.
Pre-transplant consolidation chemotherapy may not improve outcomes
after reduced intensity conditioning hematopoietic stem cell
transplantation for acute myeloid leukemia in first complete
remission. Leuk Res. 2011;35(6): 757-761.
43. Smith A, Majhail NS, MacMillan M, et al. Hematopoietic cell
transplantation comorbidity index predicts transplantation outcomes
in pediatric patients. Blood. 2011;117(9): 2728-2734.
44. Kagoya Y, Kataoka K, Nannya Y, Kurokawa M. Pretransplant
predictors and posttransplant sequels of acute kidney injury after
allogeneic stem cell transplantation. Biol Blood Marrow Transplant.
2011;17(3): 394-400.
45. Bokhari SW, Watson L, Nagra S, et al. Role of HCT-comorbidity
index, age and disease status at transplantation in predicting
survival and non-relapse mortality in patients with myelodysplasia
and leukemia undergoing reduced-intensity-conditioning hemopoeitic
progenitor cell transplantation. Bone Marrow Transplant.
2012;47(4): 528-34.
46. Birninger N, Bornhauser M, Schaich M, Ehninger G, Schetelig J.
The hematopoietic cell transplantation-specific comorbidity index
fails to predict outcomes in high-risk AML patients undergoing
allogeneic transplantation--investigation of potential limitations
of the index. Biol Blood Marrow Transplant. 2011;17(12):
1822-1832.
47. Cornelissen JJ, van Putten WL, Verdonck LF, et al. Results of a
HOVON/SAKK donor versus no-donor analysis of myeloablative
HLA-identical sibling stem cell transplantation in first remission
acute myeloid leukemia in young and middle-aged adults: benefits
for whom? Blood. 2007;109(9): 3658-3666.
For personal use only.on December 24, 2018. by guest
www.bloodjournal.orgFrom
For personal use only.on December 24, 2018. by guest
www.bloodjournal.orgFrom
Predictor (n) NRM OS
HR p HR p
1-2 (n=441) 1.54 <0.001 1.29 0.009
≥ 3 (n=377) 1.90 < 0.000 1.93 < 0.000
High risk disease (n=1355) vs. low-risk 1.62 < 0.000 1.75 <
0.000
Age >50 years (n=824) 1.33 0.008 1.25 0.004
Myeloablative regimen (n=1083) vs. RIC 1.04 0.675 1.33 0.002
PBSC (n=1466) vs. bone marrow 1.03 0.813 0.98 0.910
Male gender (n=1108) vs. female 0.87 0.234 1.00 0.925
Unrelated donor (n=979) vs. related 2.01 < 0.000 1.38 <
0.000
Female donor/Male recipient (n=390) vs. other 1.07 0.571 1.00
0.952
CMV serostatus Donor -/Recipient - (n=192) vs. other 0.92 0.592
0.86 0.171
RIC: reduced-intensity/non-myeloablative conditioning regimens,
PBSC: peripheral blood stem cells.
For personal use only.on December 24, 2018. by guest
www.bloodjournal.orgFrom
OS NRM OS NRM
For personal use only.on December 24, 2018. by guest
www.bloodjournal.orgFrom
Predictor HCT-CI Score
Related Donor 8.9 (6.2-12.3) 20.8* (13.7-28.9) 22.0+ (14.2-31.0)
< 0.001 0.63
Unrelated Donor 22.4 (18.3-26.6) 24.9 (18.2-32.2) 27.3 (19.6-34.9)
0.23 0.53
Bone marrow (BM) 20.2 (15.2-25.8) 17.7 (9.8-27.3) 26.29
(16.58-37.02) 0.23 0.53
PBSC 15.5 (12.4-18.3) 26.9*(21.4-32.9) 32.3+ (25.70-39.10) <
0.001 0.61
RIC 17.9 (13.4-22.9) 29.2*(21.2-37.6) 33.1+(25.2-41.0) <0.001
0.59
Myeloablative Conditioning 16.0 (12.9-19.2) 20.9 (15.1-27.0) 29.6+
(21.6-37.3) < 0.001 0.58
Disease:
Acute leukemia 15.7 (12.4-19.4) 18.3 (13.0-24.4) 22.0 (15.4-29.1)
0.12 0.54
Acute myeloid leukemia 13.4 (10.2-16.9) 13.7 (9.0-19.4) 20.7
(14.4-27.8) 0.08 0.54
Acute myeloid leukemia, 1st remission 9.1 (5.9-13-1) 11.4
(6.2-18.3) 19.4 (10.9-29.7) 0.03 0.59
Multiple myeloma 21.5 (13.6-30.7) 34.3 (18.2-51.2) 26.1 (9.0-45.9)
0.31 0.57
Lymphoma (Hodgkin and non-Hodgkin) 12.3 (8.2-17.3) 23.4*(14.5-33.4)
30.1+ (20.0-40.9) <0.001 0.66
Myelodisplastic syndrome 18.9 (12.7-26.1) 30.6*(19.6-42.4)
47.4+(34.1-59.7) <0.001 0.64
Chronic myeloid leukemia 16.9 (8.2-28.3) 15.3 (2.1-39.9) 42.8
(7.1-76.1) 0.22 0.60
All diseases 14.7 (12.7-16.8) 21.3* (17.6-25.2) 27.3 (22.9-31.8)
<0.001 0.60
* comparison group 0 vs. group 1-2: P-value < 0.05; + comparison
group 0 vs. group ≥ 3: P-value < 0.05
RIC: reduced-intensity/non-myeloablative conditioning regimens,
PBSC: peripheral blood stem cells.
F or personal use only.
on D ecem
w w
w .bloodjournal.org
F rom
For personal use only.on December 24, 2018. by guest
www.bloodjournal.orgFrom
0 4 8 12 16 20 24 28 32 36
Months
on D ecem
w w
w .bloodjournal.org
F rom
0 4 8 12 16 20 24 28 32 36
Months
on D ecem
w w
w .bloodjournal.org
F rom
0 4 8 12 16 20 24 28 32 36
Months
0 4 8 12 16 20 24 28 32 36
Months
For personal use only.on December 24, 2018. by guest
www.bloodjournal.orgFrom
HCT-CI Predicted 2 years NRM (%)
Figure 4
on D ecem
w w
w .bloodjournal.org
F rom
Bacigalupo, Renato Fanin, Alessandro Rambaldi and Alberto Bosi
Roberto Raimondi, Alberto Tosetto, Rosi Oneto, Riccardo Cavazzina,
Francesco Rodeghiero, Andrea Index: a prospective,
multicenter GITMO study Validation of the Hematopoietic Cell
Transplantation-Specific Comorbidity
http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests
Information about reproducing this article in parts or in its
entirety may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#reprints
Information about ordering reprints may be found online at:
http://www.bloodjournal.org/site/subscriptions/index.xhtml
Information about subscriptions and ASH membership may be found
online at:
digital object identifier (DOIs) and
date of initial publication. indexed by PubMed from initial
publication. Citations to Advance online articles must include
final publication). Advance online articles are citable and
establish publication priority; they are appeared in the paper
journal (edited, typeset versions may be posted when available
prior to Advance online articles have been peer reviewed and
accepted for publication but have not yet
Copyright 2011 by The American Society of Hematology; all
rights reserved. Hematology, 2021 L St, NW, Suite 900, Washington
DC 20036. Blood (print ISSN 0006-4971, online ISSN 1528-0020), is
published weekly by the American Society of
For personal use only.on December 24, 2018. by guest
www.bloodjournal.orgFrom