Embed Size (px)
Citation preview

DOI: 10.1161/CIRCULATIONAHA.113.002863
1
Validation of Contrast-Enhanced MRI to Monitor Regenerative Efficacy after
Cell Therapy in a Porcine Model of Convalescent Myocardial Infarction
Running title: Malliaras et al.; Validation of MRI to assess cardiac regeneration
Konstantinos Malliaras, MD1; Rachel R. Smith, PhD1,2; Hideaki Kanazawa, MD, PhD1; Kristine
Yee, DVM, DACVIM1; Jeffrey Seinfeld, BS1; Eleni Tseliou, MD1; James F. Dawkins, DVM1;
Michelle Kreke, PhD2; Ke Cheng, PhD1; Daniel Luthringer, MD1; Chak-Sum Ho, PhD3; Agnieszka
Blusztajn, BS2; Ileana Valle, BS2; Supurna Chowdhury, MS1; Raj R. Makkar, MD1; Rohan
Dharmakumar, PhD4; Debiao Li, PhD4; Linda Marbán, PhD1,2; Eduardo Marbán, MD, PhD1
1Cedars-Sinai Heart Institute, Los Angeles, CA; 2Capricor Inc., Los Angeles, CA; 3Gift of Life
Michigan, Ann Arbor, MI; 4Cedars-Sinai Biomedical Imaging Research Institute, Los Angeles, CA
Address for Correspondence:
Eduardo Marbán, MD
Cedars-Sinai Heart Institute
8700 Beverly Blvd.
Los Angeles, CA 90048
Tel: 310-423-7557
Fax: 310-423-7637
E-mail: [email protected].
Journal Subject Code: Treatment:[27] Other treatment
Michelle Kreke, PhD2; Ke Cheng, PhD1; Daniel Luthringer, MD1; Chak-Sum Ho,, PPPhDhDhD333;; AgAgAgnininieseszzka
Blusztajn, BS2; Ileana Valle, BS2; Supurna Chowdhury, MS1; Raj R. Makkar, MD1; Rohan
DhDhDharararmamamakukukumamaar,r,, PPhD4; Debiao Li, PhD4; Linda a a MaMM rbán, PhD1,2; ; Eduauaarddrdo o Marbán, MD, PhD1
1CCeCedars-SSininnai HHeeartt Innnstiitutuuteee,,, LoL s s AnAnAnggeeless, CCCA;A; 2CCaCapprpricicicororr IInnc.,., LLLos AAAnnggelelleses,,, CACA;; 3GiGift oof LLLifffe
MiMiMichchchigigigananan,, AnAnAnnnn ArArArboboborr,r, MMMI;I;I; 4CeCeCedadadarsrsrs-SSSinininaiaiai BBBioioiomememedididicacacalll IIImamamagigigingngng RRReseseseaeaearcrcrchhh InInInssstitititutututetete,, LoLoLosss AnAnAngegegeleleless,s, CCCAAA
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from
by guest on Septem
ber 1, 2017http://circ.ahajournals.org/
Dow
nloaded from
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from
by guest on Septem
ber 1, 2017http://circ.ahajournals.org/
Dow
nloaded from
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from
by guest on Septem
ber 1, 2017http://circ.ahajournals.org/
Dow
nloaded from
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from
by guest on Septem
ber 1, 2017http://circ.ahajournals.org/
Dow
nloaded from
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from
by guest on Septem
ber 1, 2017http://circ.ahajournals.org/
Dow
nloaded from
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from
by guest on Septem
ber 1, 2017http://circ.ahajournals.org/
Dow
nloaded from
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from
by guest on Septem
ber 1, 2017http://circ.ahajournals.org/
Dow
nloaded from
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from
by guest on Septem
ber 1, 2017http://circ.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCULATIONAHA.113.002863
2
Abstract
Background—Magnetic Resonance Imaging (MRI) in the CADUCEUS trial revealed that
cardiosphere-derived cells (CDCs) decrease scar size and increase viable myocardium post-
myocardial infarction (MI), but MRI has not been validated as an index of regeneration after cell
therapy. We tested the validity of contrast-enhanced MRI in quantifying scarred and viable
myocardium after cell therapy in a porcine model of convalescent MI.
Methods and Results—Yucatan minipigs underwent induction of MI and 2-3 weeks later were
randomized to receive intracoronary infusion of 12.5x106 mismatched allogeneic CDCs or
vehicle. Allogeneic CDCs induced mild local mononuclear infiltration but no systemic
immunogenicity. MRI revealed that allogeneic CDCs attenuated remodeling, improved global
and regional function, decreased scar size and increased viable myocardium compared to placebo
2 months post-treatment. Extensive histological analysis validated quantitatively the MRI
measurements of scar size, scar mass and viable mass. CDCs neither altered gadolinium contrast
myocardial kinetics, nor induced changes in vascular density or architecture in viable and scarred
myocardium. Histology demonstrated that CDCs lead to cardiomyocyte hyperplasia in the border
zone, consistent with the observed stimulation of endogenous regenerative mechanisms
(cardiomyocyte cycling, upregulation of endogenous progenitors, angiogenesis).
Conclusions—Contrast-enhanced MRI accurately measures scarred and viable myocardium after
cell therapy in a porcine model of convalescent MI. MRI represents a useful tool for assessing
dynamic changes in the infarct and monitoring regenerative efficacy.
Key words: cardiosphere-derived cells, heart regeneration, allogeneic transplantation, magnetic resonance imaging
vehicle. Allogeneic CDCs induced mild local mononuclear infiltration but no syyssstemmmiicc
mmunogenicity. MRI revealed that allogeneic CDCs attenuated remodeling, improved global
annd d d rereregigigiononnalalal ffunnctctctiioion, decreased scar size and innncrcrc eeeased viable mmyoyy caardrdrdiiuium compared to placebo
22 mmomonths post-t-trtreaeaatmmeeent.t.t. EEExtxtxtenenensisivveve hhiisstoologggicccal aananaalyssisisss vavaaliidadatteedd ququaannttiitatatititivvevelyly ttthehehe MMMRIRIRI
memeeasasa urururememenenentstts oofff sscscarar sizizze,e, sscacac r r mamamasssss aaandndd vvviiaiablblbleee mmmaasasss.. CCCDCDCDCs s nenen iiti heheher r r aalalteeerered dd gagaadodoolililinnniumumm ccononntrrasasa t
myocardial kkinininetete iciccs,s,s, nnnororor indndnducucu ededd ccchahahangggeseses iin n n vavavascscsculululararar denenensisisitytyty ooor r r araa chchchitititececectututurerere iin nn viviv ababablelele and scarreedd
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from
DOI: 10.1161/CIRCULATIONAHA.113.002863
3
Cell therapy has emerged as a potential therapeutic strategy for ischemic cardiomyopathy. While
the paradigm of administering bone marrow-derived cells in the setting of acute or recent
myocardial infarctions (MIs) has proven to be safe, efficacy has been inconsistent1,2. Early
clinical experience with autologous heart-derived progenitor cells has been more encouraging3,4.
In the CADUCEUS trial, intracoronary infusion of autologous cardiosphere-derived cells
(CDCs)5 in post-MI patients with left ventricular (LV) dysfunction decreased scar size, increased
viable myocardium and improved regional function, as measured by contrast-enhanced magnetic
resonance imaging (MRI)3. Contrast-enhanced MRI has been extensively validated (and is
considered the “gold standard” imaging modality) for the quantification of necrotic/scarred and
viable myocardium in the setting of acute or chronic MI6-8. Thus, MRI represents a potentially
useful tool for monitoring regenerative efficacy, as it affords the unique ability to quantify,
rigorously and independently, scar mass and viable myocardial mass in human subjects before
and after cell therapy interventions9. However, its validity in characterizing tissue viability after
cell administration has been called into question10. Without evidence, concerns have been raised
that cell therapy may promote changes in vessel density or architecture (e.g., increase in wall
thickness or decrease in vascular permeability) that could affect gadolinium (Gd)-contrast
myocardial kinetics (in the form of accelerated contrast wash-out [a phenomenon that has been
described in non-cardiac tissues11] or decreased contrast extravasation, respectively), therefore
compromising the ability of contrast-enhanced MRI to distinguish scar from viable
myocardium10.
Here, we sought to test the validity of contrast-enhanced MRI to distinguish, and
accurately measure, scarred and viable myocardium after cell therapy. We used a porcine model
of intracoronary infusion of allogeneic CDCs, which enabled us to concurrently investigate the
viable myocardium in the setting of acute or chronic MI6-8 MRI representstss a ppoototennentititialalallylly . Thus,
useful tool for monitoring regenerative efficacy, as it affords the unique ability to quantify,
igogoorororouususlylyly aaandndn indndndeepependently, scar mass and viababablele myocardial mamamar ss iinn n hhuhuman subjects before
anndd d afa ter cell ttheheheraaapyy iintnttererrveveventntntioionsnsns999. HHoHowwevvverrr, itsss vvvalidddiitity y inini cchahaaraaactctererizizining g g tititissssueuee vviaiaiabibb liiitytty aaaftftter
ceellllll aaadmdmdmininisisistrtrtratatioioonn n hahass bbbeeeen ccac llllllededed iiintntooo quququesesestiiononon10100. WiWiWiththhouououtt t evevvididdenenncecece,, ccoconcncererernsnsns hhavavaveee bbeeeenn rraaaisseed d
hat cell therrapapapy y y mamamay yy prprpromommotototeee chchchanana gegeg s s ininin vvvesesessesesell dededensnsnsiti y y y ororor aaarcrcrchhhitititececctututurerere ((e.e.e g.g.g , ininincrcrcreaeaeasesese in wall
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.113.002863
4
safety and efficacy of allogeneic heart-derived cells without immunosuppression in a clinically-
relevant model of convalescent MI.
Methods
All animal studies were performed in an American Association for Accreditation of Laboratory
Animal Care accredited facility with approval from the Institutional Animal Care and Use
Committee of the Cedars-Sinai Medical Center (IACUC 3661). The experimental protocol is
depicted schematically in Figure 1. A total of 26 minipigs were studied: 3 completed the 24-hour
retention study (Fig 1A), 10 completed the validation study (Fig 1B), 5 completed the 2-month
engraftment study, 4 were excluded per protocol for procedural mortality, 3 were used for
allosensitization protocols, and 1 served as CDC donor.
Cell culture
Allogeneic CDCs were grown from a freshly-explanted heart obtained from one male Sinclair
minipig (Sinclair Bioresources) (for detailed methods see Online Supplement). For 24-hour
retention analysis, CDCs were transduced with an adenoviral vector carrying the firefly
luciferase gene 3 days prior to infusion.
MI creation and CDC infusion
Infarcts were created in adult Yucatan minipigs by inflation of an angioplasty balloon in the mid-
left anterior descending artery (LAD) (distal to the 1st diagonal branch) for 2.5 h (for detailed
methods see Online Supplement). Two to 3 weeks later, pigs were randomized to receive 12.5
million CDCs (in 10 mls of CryostorTMCS10 containing 45 g/ml nitroglycerin and 180 U/ml
heparin) or vehicle. Intracoronary infusion was performed via an over-the-wire balloon catheter,
placed in the mid-LAD. CDCs or vehicle solution were infused in 3 cycles of intermittent
engraftment study, 4 were excluded per protocol for procedural mortality, 3 wereree usess dd d fofofor rr
allosensitization protocols, and 1 served as CDC donor.
CeCellllll cccululultututurerer
AAAllooogeg neic CDCDCCs wewererre gggroroownwnwn ffrromomom aa ffreeshllyy--expplalannteedd hheaeaartrtt oobtbbtaaiinen dd d frrromomm ooonene mmmalala ee SiSinncnclalalairrr
mimiininin pipipigg g (S(S(Sinininclcclaiairrr BBiBiororresessouourcceese ))) (f(f(fororor ddeetetaiaiaileleleddd mememeththhoodds seseeeee OnOnOnlililinenee SSSupupupppplememmenennt)t)t).. FoFoor r r 2424--h-hououo r r
etention analalysysysisis,, CDCDCDCsCC wwwerereree trtrtranana sdsdsducuccededed wwwititth h h anann aadeded nonoovivivirararal l vevevectcc ororor cccarararryryryinining g thththe e e fififirerereflf y
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.113.002863
5
balloon inflation12. Minipigs were euthanized either 24 hours post-infusion, to measure short-
term cardiac retention of administered cells (n=3), or 2 months later (n=15; 10 completed the
validation study, 5 completed the 2-month engraftment study).
In vivo cardiac MRI
Baseline (2-3 weeks post-MI, before intracoronary infusion) and endpoint (2 months post-
infusion) contrast-enhanced cardiac MRI was performed to measure scar mass, viable
myocardial mass (i.e., total mass minus scar mass), scar size (scar mass divided by total mass),
volumes, global function, and regional function of the LV.
All MRI studies were performed on a 3.0 T clinical MRI scanner (Siemens
MAGNETOM Verio®, Erlangen, Germany). Typical in-plane resolution was 1.3 x 1.3 mm, and
slice thickness was 6 mm, with no gaps. Global LV function, regional systolic thickening and
regional end-systolic thickness were assessed using ECG-gated and breath-held cine steady-state
free precession acquisitions13. Minipigs undergoing baseline MRI subsequently received an IV
injection of Gd-based contrast agent gadoversetamide (OptiMARK®, Covidien Imaging
Solutions, Hazelwood, MO, USA; 0.2 mmol/kg body weight), and, 8 minutes later, delayed
contrast-enhanced images were acquired with an ECG-gated, breath-hold, interleaved, 2D-Turbo
FLASH sequence14. The inversion time was adjusted by the scanner operator to null signal from
non-infarcted remote myocardium.
In minipigs undergoing endpoint MRI, once the cine acquisitions were completed, a
short-axis slice with significant regional hypokinesia was selected (after review of cine images)
to study Gd-contrast kinetics. Minipigs received an IV injection of Gd-contrast (0.1 mmol/kg
body weight) and a series of dynamic delayed contrast enhancement images were acquired (pre–
and 1, 2, 3, 4, 5, 6, 10, 12, 14, 16, 18 and 20 minutes post-contrast administration). An ECG-
MAGNETOM Verio®, Erlangen, Germany). Typical in-plane resolution was 1.3.33 xx 11.333 mmmm,m,m, aannd
lice thickness was 6 mm, with no gaps. Global LV function, regional systolic thickening and
eegigigionononalalal eeendndnd--ssysstototolilic thickness were assessed usssiiingngng ECG-gated aandnn bbrereeaatath-held cine steady-state
ffrreeee pprecessioon n aaacqququisisisiti ioioionsnsns13133.. MiMininin pipip gggs uunddderrrgoinnnggg baaaseseelilinnne MMRRIRI suubsbsbseqqqueueentntntlyly rreececeieieivveed d d anan IVVV
nnjejejectcttioioion n ofoff GGGd-d-bbabaseses d d cooontntraaststs aaagegegentntnt ggadadadovovoveeerseseetatat mimimidede ((OpOpOpttitiMAMAMARKRKRK®®,, CoCoCovividididienenn IImamamagiginnng
Solutions, HHazazzelele wowowoododod, MOMOMO,,, USUSUSA;A;A 000.2. mmmmomomol/l/l/kgkgkg bbbododody y y weweweigigghththt),),), aaandndn ,, , 8 8 8 mimim nununutetet s s lalalateteter,r,r, dddele ayed
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.113.002863
6
gated, breath-hold, interleaved 2D-Turbo FLASH sequence was used, and the inversion time was
kept constant at 270 ms15,16. Thirty minutes after the first contrast injection, a TI scout was
performed to ensure sufficient contrast clearance. Subsequently, minipigs received a second IV
injection of Gd-contrast (0.2 mmol/kg body weight) and 8 minutes later delayed contrast-
enhanced images were acquired to assess scar size as described above for baseline MRI. Thirty
minutes after the second contrast injection, a TI scout was performed to ensure sufficient contrast
clearance. Subsequently, minipigs received a third IV injection of Gd-contrast (0.2 mmol/kg
body weight) and were sacrificed 15 minutes later in order to perform ex vivo MRI of the heart.
All image analyses were performed using validated image processing software (QMass
MR®, Medis medical imaging systems). Global function and cardiac volumes were evaluated by
a researcher blinded to treatment allocation. To evaluate regional function, each short-axis slice
was divided into 6 segments, using the right ventricular insertion as a reference point. Scar size
from late Gd-enhanced cardiac MR images was defined based on the full-width half-max
(FWHM) criterion to delineate scarred myocardium7.
Ex vivo cardiac MRI & histology
Hearts from minipigs sacrificed 2 months post- infusion underwent ex vivo MRI. The heart was
removed ~30 minutes post Gd-DTPA administration, thoroughly rinsed in ice-cold saline to
remove any residual blood, and suspended by sutures in a plastic container filled with saline. 3D
Turbo FLASH images were acquired with a resolution of 1 x 1 x 1 mm 6. After image acquisition,
the heart was sectioned into 1 cm thick short-axis slices, which were incubated with 2% 2,3,5-
triphenyltetrazolium chloride (TTC) for 20 min at 37°C to stain viable myocardium. Each slice
was photographed with a digital camera and infarct size was determined as the percentage of LV
volume by manual tracing by a researcher blinded to treatment allocation (ImageJ, version 1.46,
MR®, Medis medical imaging systems). Global function and cardiac volumes wweeere ee evvvalalaluauauatetetedd byy
a researcher blinded to treatment allocation. To evaluate regional function, each short-axis slice
wawas s s dididivivividededed d d iinintoo 666 ssegments, using the right vennntrtrtricccular insertion n asaa aa rrrefefefere ence point. Scar size
ffrrommm late Gd-eenhnhnhaannceced d cacacardrdrdiaiaiaccc MRMRMR iimmamagges awaw s ddeefffineeed d babassesed d oonn tthehe fffululll-wiwiwidtddth h hahahalflflf-m-mmaxxx
FFWHWHWHM)M)M) cccririritteteririononon ttoo dedelilinneatatate scscscarararrreredd d mymymyoococararardidid umumum77.
Ex vivo carddiaiaiac c c MRMRMRI I I &&& hihihistststolologogogyy
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.113.002863
7
National Institutes of Health, Bethesda, MA, USA). Scar and viable myocardium volumes were
calculated by multiplying scar and viable area for each slice (in mm2) with the corresponding
slice thickness. Scar mass and viable myocardial mass were calculated by multiplying the scar
and viable myocardial volumes times a specific gravity of 1.05g/cm3.
Immune rejection in the heart was investigated by hematoxylin and eosin staining;
analysis was performed by an experienced cardiac pathologist blinded to treatment allocation
(DL), and rejection was graded according to the International Society for Heart & Lung
Transplantation (ISHLT) grading system, used in clinical practice to diagnose solid organ
transplant rejection. Morphometric analysis was performed with Masson’s trichrome staining.
Vascular density and architecture were investigated by fluorescent immunohistochemistry;
arterioles and arteries were defined as smooth-muscle-coated vessels with external vascular
diameter (lumen + vascular walls) <75 m and >75 m respectively. Myocyte cross-sectional
area was investigated by fluorescent immunohistochemistry; cardiomyocytes were accepted for
size measurement if they met the following criteria: (a) cellular cross-sections present (b) visible
nuclei located close to the cell center and (c) intact cell borders17. Cardiomyocyte cell-cycling
and activation of cardiac progenitors were investigated by fluorescent immunohistochemistry. In
all histological analyses, peri-infarct (border zone) area was defined as the region at the edges of
the scar (comprising areas of both viable and scarred myocardium). For detailed histological
methods see the Online Supplement.
Evaluation of 24-hour cardiac retention and 2-month cardiac engraftment
Evaluation of 24-hour cardiac retention was performed with the ex vivo luciferase assay12 (Supp
Fig 1a; for details see the Online Supplement). Two-month cardiac engraftment was investigated
by Fluorescence In Situ Hydridization (FISH) for the male Y chromosome (Supp Fig 2) 2
Vascular density and architecture were investigated by fluorescent immunohistococcheheemimistststryryry; ; ;
arterioles and arteries were defined as smooth-muscle-coated vessels with external vascular
diiamammeteteteerer (((lululummmen n +++ vav scular walls) <75 m and >7>7>755 m respectiveelylyl . MyMyMyooocyte cross-sectional
arreaaa was invesstitiiggagateteddd bybyy ffflluluorororeesesceceentntnt immmmmmunnohhhistooocchhemmmiisistrtryyy; ccararrdidiommyyyoccycytetees s wewererere aaacccceppptteted dd fofofor
iizezee mmmeaeae susuurererememennnt iif f ththheyeyy mmetetet tthehehe fofofolllllowowwinining g g crrritititereriaia:: (a(aa) ) cececellllllulullarara cccrrosososs-s-sssecctctioioonsnsn ppprereeseseentnt ((b)b)b) vviisisibbblel
nuclei locatededd ccclolol sesese ttooo thththe cececelllll cececentntn ererer aaandndnd (((c)c)c) iiintntn acacactt t cecec lll bbbororordededersrsrs171717.. CaCaCardrdrdioioiomymymyococcytytyte e e cececelllll -cycling
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.113.002863
8
months after sex-mismatch cell transplantation (male cells infused into infarcted female
recipients; for details see the Online Supplement).
Histocompatibility
To assess histocompatibility, low-resolution swine leukocyte antigen (SLA) typing was
performed on the donor and recipient minipigs as described in the Online Supplement.
Circulating donor-specific antibodies
To evaluate humoral immune response, recipient minipig serum samples (obtained at baseline, 1
day, 1 week, 2 weeks and 2 months post-infusion) were screened for circulating anti-donor IgG
antibodies by flow cytometry18.
An allosensitization protocol was performed to provide positive controls for the flow
cytometry assay. Peripheral bone marrow mononuclear cells (PBMNCs) were harvested from a
donor farm pig and injected intradermally and subcutaneously into the pinnae of recipient
Yucatan minipigs (n=2, 190 million PBMNCs injected per pig). Serum samples collected 2
weeks post PBMNC injection served as positive controls for allosensitization.
Statistical Analysis
Results are presented as mean ± SD in the text and as mean ± SEM in the figures. For continuous
measures, differences between 2 groups (controls, CDC-treated) were tested using independent
samples t-test. Comparisons of changes from baseline within groups were performed using
paired samples t-test. Histology data for grading of rejection were analyzed using a generalized
estimating equations (GEE) logistic regression model. Gd curves were analyzed with a linear
mixed effects model using random intercept to control for repeated measures and Tukey’s
adjustment for multiple comparisons. Serial Troponin I (TnI) measurements were analyzed using
a GEE model with an autoregressive correlation structure. Pearson correlations and the Bland-
An allosensitization protocol was performed to provide positive controls s foffor rr ththhe ee flflflowowow d
cytometry assay. Peripheral bone marrow mononuclear cells (PBMNCs) were harvested from a
doonononor r r fafafarmrmm ppiiig aaandndnd injected intradermally and suuubcbcb uutaneously inntotoo thee pppiininnae of recipient
YYuccacatan minipipiigggs ((n=n=2,2, 111909090 mmmililliliononon PPBMBMMNNCCsss injjeccctedd d ppeper r pipiig)g). SSeerurummm ssammpmplleles s cococollllllececteted dd 22
weweeekekeksss popopoststt PPPBMBMBMNNCNC iinnjecece tit ononn ssererervevevedd aasas ppposososiitivivvee ccoconntrrorolslss fffooor aaalllll oososenenensisitttizazaatitiononon.
Statistical AnAnnalalalysysysisisis
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from
DOI: 10.1161/CIRCULATIONAHA.113.002863
9
Altman analysis method were used to compare MRI measurements against postmortem
histological measurements. All tests were 2-sided. No multiplicity adjustment for multiple
comparisons was performed. A p value of <0.05 was considered statistically significant.
Results
Safety of CDC infusion, 24-hour retention and 2-month engraftment
Four of 22 minipigs (18%) died during creation of MI due to ventricular arrhythmias. There was
no further mortality (0%) in minipigs that survived the MI.
CDCs are ~20 m in diameter, so that microvascular occlusion is expected at escalating
doses12. We thus looked for any infusion-related impairment of coronary flow or increase in
ischemic biomarkers. No adverse events (sustained ventricular arrhythmias, unresolved ST-
segment elevations) occurred during cell infusion, and no impairment of TIMI flow was
observed after infusion (Supp Fig 3b). No difference in serum TnI was detected between the
CDC-treated and placebo groups at 1,7,14, or 60 days post-infusion (Supp Fig 3A). The mild
TnI elevations observed 1 day post-infusion in both groups are consistent with transient LAD
occlusion by the stop-flow infusion procedure.
To assess short-term cardiac retention of infused CDCs, 3 minipigs were infused with
luciferase-labeled allogeneic CDCs. Twenty-four hours later, the ex vivo luciferase assay (Supp
Fig 1A) revealed that cardiac retention of CDCs was 4.3±2.2% (Supp Fig 1B). Long-term
cardiac engraftment was investigated by FISH for the male Y chromosome (after infusion of
male CDCs into female recipients). While presence of infused cells in the recipient myocardium
could be verified at 2 weeks post-infusion (Supp Fig 2), no allogeneic (male) cells could be
detected at 2 months post-infusion (5 animals, 4782 nuclei analyzed)
doses12. We thus looked for any infusion-related impairment of coronary flow or r inincrcc eaeaeaseese iiin n n
schemic biomarkers. No adverse events (sustained ventricular arrhythmias, unresolved ST-
eegmgmgmenenenttt eleleleveve aatiooonsnsns) ) occurred during cell infusiononon, aaand no impairmmment t ofofof TTIMI flow was
obbseeservr ed afterr iiinfnn uuusioionn (((SuSuSupppppp FFigigg 333bb)). NNNo dddiffffereenencce iiinn seserrurum m TTnTnII wawas ddedeteteectctcteded bbbetetetweweeennn ttheheh
CDCDDC-C-C-trtrtreaeateteed d d ananddd plplplacacebebbo o grg oououpspsps aaat t t 1,1,77,7,141414,, ororo 66600 dadadaysysy ppososost-t-t-innnfufufusssiononon ((SSSuppppp FFFigigg 33AAA)).). TThehehe mmililld
TnI elevationsnss ooobsbsserererveveed d d 1 dadaday yy popopoststs -i-iinfnffususu ioioion n n ininin boboboththh gggrorooupupupsss arara ee e cococ nsnsnsisisstetetentntnt wwwitith h h trtrtrananansisisiene t LAD
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from
DOI: 10.1161/CIRCULATIONAHA.113.002863
10
Immune reaction to allogeneic CDCs
Low-resolution SLA genotyping revealed complete Class I (SLA-1, SLA-2, SLA-3) and Class II
(DRB1, DQB1, DQA) mismatches between the donor minipig and CDC recipients (Supp Fig 4).
Cardiac histology demonstrated a marginally significant increase in focal lymphoplasmacytic
infiltration (deemed to be unrelated to the natural inflammatory response to the ischemic insult)
in the peri-infarct area of CDC-treated minipigs compared to placebo (p=0.058 between groups,
Odds Ratio=8.61 [95% CI: 0.93-79.52]). (Supp Fig 5A). The infiltrating cells were localized
within interstitial and perivascular spaces (Grade 1R according to the ISHLT grading system)
(Supp Fig 5B); importantly, no foci of rejection-associated myocyte damage were detected. The
remote myocardium was consistently clear of inflammatory infiltrates. No circulating
alloreactive antibodies were detected in any recipients of allogeneic CDCs at any time point. In
contrast, in minipigs that were allosensitized by intradermal and subcutaneous PBMNC
injections, high titers of circulating alloreactive IgG antibodies were detected 2 weeks post-
injection (Supp Figure 5C,D).
Functional and structural benefits after infusion of allogeneic CDCs
To assess efficacy of allogeneic CDCs, minipigs underwent cardiac MRI before infusion (2-3
weeks post MI) and 2 months later. Allogeneic CDCs resulted in preservation of LVEF ( :-
0.5±3.2, p=0.73 within group), while LVEF decreased in control animals ( :-9.9±1.3%, p<0.001
within group, p<0.001 between groups) (Fig 2A-C, Supplemental Videos 1-4). In addition,
allogeneic CDCs attenuated LV remodeling: CDC-treated animals exhibited a smaller increase in
ESV ( :10.9±7.4ml) compared to controls ( :26.6±13.2ml, p=0.048 between groups) (Fig 2E).
EDV increased in both CDC-treated animals ( :17.7±10.5ml, p=0.020 within group) and
controls ( :30.5±19.8ml, p=0.026 within group, p=0.24 between groups) (Fig 2D).
emote myocardium was consistently clear of inflammatory infiltrates. No circululataatininng gf
alloreactive antibodies were detected in any recipients of allogened ic CDCs at any time point. In
coontntntrararaststst, ininin mmminipippigigigss that were allosensitized by y iininttrradermal and sususubccutututanananeous PBMNC
nnjeeecctions, highghh tttitererss ofof ccirirircculululaatatininngg g aallloorrreacttit vvve IgGgGgG anntntiibibododdiieess wwweeere e dededeteeectctededed 22 wwweeeeeeksksks poosost-t-
nnjejejectcttioioionn (((SuSuSupppp FFigigigururre 5C5C,DDD).).).
Functional aandndnd sstrtrtrucucuctututuraaalll bbbenennefefefitittss s affftetet rr r inininfufufusisisiononon ooof f alalallolologegegeneneneicicic CCCDCDCDCsss
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.113.002863
11
Regional function was assessed in infarcted and non-infarcted myocardial segments, after visual
inspection of corresponding late Gd-enhanced images. Two months post-infusion, CDC-treated
infarcted myocardial segments displayed increased systolic thickening (p<0.001 between
groups), and increased end-systolic thickness (p=0.025 between groups), compared to infarcted
segments from placebo-treated animals (Fig 2F,G). In addition, regional function in the non-
infarcted myocardial segments was improved in CDC-treated animals compared to controls,
consistent with attenuation of LV remodeling (Fig 2F,G).
Fig. 3A shows representative late Gd-enhanced MRI acquisitions of hearts in short-axis
section at end-diastole. Gd-contrast agent accumulates in the infarct scar (as a result of a larger
distribution volume due to increased extracellular space in the scar compared with normal
myocardium19.20). In the CDC-treated minipig, the infarcted wall thickness was preserved 2
months post-infusion; importantly, the scar decreased in transmurality, while viable myocardial
mass increased. In contrast, the placebo-treated minipig was characterized by infarct thinning
and expansion, with no evidence of an increase in viable myocardium over the same time period
(Fig. 3A).
Two months post-infusion, MRI analysis revealed that scar size remained unchanged in
controls ( :0.4±0.9%, p=0.33 within group) but decreased in CDC-treated animals ( : -3.6
±2.4%, p=0.026 within group, p=0.007 between groups) (Fig 3B), resulting in significantly
smaller scar size in CDC-treated animals (9.2±0.8%) compared to controls (14.6±3.2%, p=0.006
between groups), despite similar scar size at baseline (12.8±2.8% [CDCs] vs 14.1±2.8%
[controls], p=0.48 between groups) (Fig 3E). While scar size is a conventional measure of
myocardial viability, cardiac MRI can quantify independently the individual components of scar
mass and viable myocardial mass9, enabling more discriminating insight into mechanism. Scar
distribution volume due to increased extracellular space in the scar compared wiwiththth nnnorrrmamamal ll
myocardium19.20). In the CDC-treated minipig, the infarcted wall thickness was preserved 2
momontntnthshshs ppososost-tt-iiinfufuusisisiono ; importantly, the scar decrerereasaseed in transmururrala ity,y, wwwhih le viable myocardial
mmasssss increaseded. InInIn cononntrrrasasastt,t, ttthehehe pplalalaccecebbo--treaaateeed mmminnnipiiig g g wawaas chchaaaraacteteriririzeeed d bybyby iinfnffaaarctctct tthhih nnnnninning
anndd d exexexpapapansnssioioion,n, wwwittth h nonno eeevividedeencncceee ofofof aan n innncrcrcreeeasesese iinnn vvviai bblbleee mymymyocococararrdidiiumumum oovvever r ththt e ee sasaamememe tiimime e e pepeeriiodod
Fig. 3A).
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from
DOI: 10.1161/CIRCULATIONAHA.113.002863
12
mass decreased in CDC-treated animals ( :-1.4±1.4g), but not in controls ( :0.8±0.6g, p=0.012
between groups) (Fig 3C), resulting in a trend towards smaller endpoint scar mass in CDC-
treated animals (6.6±0.7g) compared to controls (9.7.3±3.5g, p:0.093 between groups) (Fig 3F).
In addition, CDC-treated animals exhibited significant increases in viable myocardial mass
( :10.7±3.6g) compared to controls ( :2.7±2.1g, p=0.003 between groups) over 2 months (Fig
3D), resulting in greater endpoint viable mass (65.8.9±4.5g) compared to controls (55.5±5.0g,
p=0.010 between groups) (Fig 3G). A complete list of MRI-measured parameters for each
experimental animal is provided in Supp Table 1.
Comparison of cardiac MRI with histology for assessment of scarred and viable
myocardium after cell therapy
Post-mortem histological analysis confirmed the MRI results, not just qualitatively but also with
quantitative accuracy. Fig 4A shows representative short-axis cardiac slices after incubation with
TTC, while Fig 4B shows representative sections from the infarcted wall stained with Masson’s
trichrome. CDC-treated hearts consistently exhibited significant amounts of viable myocardium
in the infarcted wall, most often in the form of endocardial and epicardial muscular layers
surrounding the scar but also in the form of islets of viable myocardial tissue interspersed
between the collagen fibers. In contrast, in control minipigs the scar was homogeneous and
largely transmural (Fig 4A,B,F). The increased amount of viable myocardium in the infarct
region after cell therapy is consistent with the improved regional contractility of infarcted
segments in CDC-treated animals compared to controls (Fig 2F,G). Histological measurement of
scar and viable myocardium demonstrated decreased scar transmurality in CDC-treated animals
(44.1±21.3% vs 79.3±25.2%, p=0.044), smaller scar size (9.1±1.2% vs 14.0±2.9%, p=0.009) and
increased viable myocardial mass (68.7±4.7g vs 55.2±4.9g, p=0.002) in CDC-treated animals
myocardium after cell therapy
Post-mortem histological analysis confirmed the MRI results, not just qualitatively but also with
ququananantitititatatatititiveveve aaaccurururaacacy. Fig 4A shows representatttivivivee short-axis cardrddiac c slslsliicices after incubation with
TTTCCC, while Fiig g 4B4B4B sshohoh wswsws rrreepeprrereseseentntntata iivveee seccctiiionss ffrrrommm tththe e innnfafarrccteed d wwallll sstataaininneded wwwititith hh MaMaMassssononon’s
rricicchrhrhromomome.e. CCCDCDDC---trreeatateeded hheeartrtrts s cococonsnsnsiisisteteentnttlylyly eeexhxhxhibibiiiteeded sssigiggnininiffificacaantntn aamomomoununntstss oof f f viviiababa lelele mmmyyoyoccacardrddiuiumm m
n the infarcttededed wwwalala ll,l, mmmosoo t t ofofoftett n n n ininin ttthehh ffforororm m m ofofof eeendndndococcarardididialalal aaandndnd eeepipicacacarrrdididialalal mmmususscucuculalalarr r lalalayers
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.113.002863
13
compared to infarcted controls (Fig 4C-F), yielding virtually identical results to those obtained
from contrast-enhanced MRI (Fig 3E-G). A complete list of histological measurements of scar
size, scar mass and viable mass for each experimental animal is provided in Supp Table 2.
To further evaluate the ability of contrast-enhanced MRI to accurately measure scarred
and viable myocardium after cell therapy, all TTC-stained cardiac slices were matched with their
corresponding late Gd-enhanced images (from both the in vivo and ex vivo MRI datasets). Fig
5A provides representative examples of this analysis for a CDC-treated and a control minipig. In
both cases, areas of hyperenhancement in cardiac MRIs correspond faithfully to regions of
scarred myocardium in histological slices. Importantly, MRI reveals significant amounts of
viable myocardium within the infarct region of the CDC-treated heart, a finding that is confirmed
by cardiac histology: the endocardial and epicardial rims of non-hyperenhanced tissue in the
infarcted wall in contrast-enhanced MRIs are virtually identical to the endocardial and epicardial
TTC-positive muscular layers surrounding the scar in histological slices. In contrast, the control
heart is characterized by a dense transmural scar, and no viable myocardium can be detected in
the infarct area by either MRI or histology. Figs 5B-D show quantitative correlation analysis
between the various MRI parameters and the corresponding histological values; the measures of
scar size (as % of isolated cardiac slices and as % of the LV), LV scar mass and LV viable mass
all correlate strongly, with a slope close to the line of identity. Bland-Altman analysis
demonstrated excellent agreement between MRI and post-mortem histology (Supp Fig 6).
MR imaging of Gd-contrast kinetics in cell-treated myocardium
To assess whether cell therapy fundamentally alters myocardial contrast uptake and/or wash-out,
we compared Gd-contrast kinetics in various regions infused with cells to the kinetics in the
remote (non-infarcted, non-cell treated) myocardium. A series of dynamic late Gd-enhanced
viable myocardium within the infarct region of the CDC-treated heart, a finding ttthahahatt isiss cconononfififirmrmed
by cardiac histology: the endocardial and epicardial rims of non-hyperenhanced tissue in the
nnfafaarcrcrcteteteddd wawaw lllll in n cococontn rast-enhanced MRIs are viirtrtrtuauaally identical totoo thee eeenndndocardial and epicardiald
TTTCCC-positive mmuususcuculalalar lalalayeyerrsrs ssururrororoununu didinng tthehee scaaar r in hhhiisistotolologigiccaal slsliciceees.. InIn ccoonontrtrasasa t,t,t ttheheh cccononntrrrol
heheararart t isisis cchahaarararactctererrizzzeded bby y y a a dedeensnseee trtrtranaansmsmmurururalalal scacacarr,,, annnd nonono vvviiaiablblblee e mymymyococo aararddidiumumm cccanana bbbee e deeetetectctc ededd iinnn
he infarct arreaeaea bbbyyy eieieiththhererer MMMRIRIRI ooor r r hihih stststolologogogy.y.y FiFiFigsgsgs 555B-B-B DD ssshohohow w w quququananantiiitatatatititiveveve cccororo rereelalaatititiononon aanalysis
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from
DOI: 10.1161/CIRCULATIONAHA.113.002863
14
images were acquired with a fixed TI (Fig 6A)15,16, and signal intensity of specific areas
(collagenous scar, viable myocardium in the infarcted region, viable myocardium at the border
zone, remote myocardium) was measured at various timepoints following contrast administration,
resulting in the generation of site-specific Gd-contrast curves (Fig 6B; pooled data from all
CDC-treated minipigs). Analysis using a linear mixed effects model demonstrated that the only
site in which Gd kinetics were (predictably) different compared to remote healthy myocardium
was the infarct scar. Importantly, Gd-contrast kinetics were virtually identical in cell-treated
viable (non-hyperenhanced) areas and in the remote non-cell treated healthy myocardium.
Vascular density and architecture
To investigate whether cell therapy with CDCs can induce vascular changes in the treated
(scarred or viable) myocardium, we studied vessel density and architecture in the collagenous
scar, in viable myocardium in the infarcted wall and in the remote (non-infarcted, non-cell
treated) myocardium. As expected21,22, capillary density was low in the collagenous scar
(117.7±32.9 vessels/mm2) and in the border zone (525.3±274.3 vessels/mm2) as compared to
remote myocardium (1344.4±356.5 vessels/mm2). While total capillary density was increased in
the border zone (defined as the region at the edges of the scar comprising areas of both scarred
and viable myocardium) of CDC-treated hearts (721.9±192.5 vessels/mm2 vs 328.8±188.8
vessels/mm2, p=0.012) (Fig 7B), no differences in capillary, arteriolar or arterial density in
scarred or viable myocardium could be detected between CDC-treated animals and controls (Fig
7C). Thus, the increased total capillary density in the border zone of CDC-treated hearts is a
result of the increased viable mass and decreased scar mass observed in the infarct border zone
after CDC therapy, and cannot be attributed to differences in vascular density of scarred or viable
myocardium between CDC-treated hearts and controls. Vessel architecture (as quantified by
To investigate whether cell therapy with CDCs can induce vascular changes in ththhe trtrt eaateteted d d
scarred or viable) myocardium, we studied vessel density and architecture in the collagenous
ccararr, ininin vviaiaiablblbleee mymyyoococardium in the infarcted walll aaanndd in the remotetee (nononn-i-i-innfarcted, non-cell
rreaaateted) myocacardrdrdiuuum.m. AAss s exeexpepepectctededd2121,1,22222,, cccapiillll aaary ddedennsitttyy y wawaas lolowww iinn thehehe cccolollalalaggegenonooususus ssccar r r
11171717.7.77±3±3± 2.2..99 9 vevesssssellls/s/mmmmmm2) ) annnd d ininin ttthehehe bbbororrdedederr r zooonenen (55252555.3±3±3±227274.4.4 333 vvevesssssselelsss/mmmmm22))) asasa cccomomompapapareeed d totoo
emote myocacaardrdrdiuiuum m m (1(113433 4.4.4.4±4±4±35556.6.6 55 vevev sssssselelels/s//mmmmmm222).).) WhWhW ililile ee totototatatalll cacacapipiilllll ararary yy dededensnsn ititity y y wawawas s s ini creased innn
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.113.002863
15
lumen diameter [Fig 7D], wall thickness, endothelial layer thickness, smooth muscle layer
thickness [Fig 7E] and lumen/wall ratio [7F]) was similar in CDC-treated and control hearts.
Stimulation of endogenous cardiac regeneration by allogeneic CDCs
To investigate whether the increased viable myocardium observed after CDC-therapy was a
result of myocyte hypertrophy, we measured cardiomyocyte cross-sectional area in the infarct
and peri-infarct area. Myocyte size was significantly smaller in CDC-treated animals compared
to controls (Fig 8A), thus excluding myocyte hypertrophy as a contributor to the increase in
viable myocardium. The conjunction of increased viable mass and smaller myocyte size are
indicative of cardiomyocyte hyperplasia after cell therapy. With regard to the latter, we found
that transplantation of CDCs upregulated cardiomyocyte cycling (Fig 8B) and increased the
number of small round TnI+ cells (previously defined as putative myocyte progenitors22,23) in the
infarct and peri-infarct area (Fig 8C), confirming previous reports18,24. While cardiomyogenesis
is likely to play a role in the reduction of cardiomyocyte area, attenuation of adverse remodeling
(which involves cardiomyocyte hypertrophy) may potentiate the reduction in myocyte size in the
infarct and peri-infarct area of CDC-treated animals. Supporting this conjecture, myocyte cross-
sectional area in the remote myocardium tended to be lower as well (consistent with relief of
wall stress), although the differences did not reach statistical significance (Supp Fig 7).
Discussion
Heart-derived cells are particularly promising for cardiac repair and regeneration. In the
CADUCEUS trial, intracoronary infusion of autologous CDCs decreased scar size, increased
viable myocardium and improved regional myocardial function, as measured by MRI3. An
interim MRI analysis of the still-ongoing SCIPIO trial (where MRI was performed only in
hat transplantation of CDCs upregulated cardiomyocyte cycling (Fig 8B) and inncccreaee sseedd d thththe e e
number of small round TnI+ cells (previously defined as putative myocyte progenitors22,23) in the
a (nnfafaarcrcrcttt anandd d pepeperi-i-iinfnfnfara ct area Fig 8C), confirminnng gg pprrevious reportstss18,244.. WWWhile cardiomyogenesis
ss liikikely to plaay y aaa rrrolele in n n thththeee rerereduducctctioioionn ooff carrrddiiommyoocyyytetee aarreeaa,a, aatttteennuauatititionn oof ff aadadveveersrsr e e e rereemmomodededeliiingn
wwhihih chchch iinvnvvolololveves s caaardrdiioommymyococytyty ee hyhyhypeppertrttroroophphphyyy) mmmayayay pppotttenenntititiatatate thththee e rereedudud cccttioonon iiin nn mymymyocococyytyte e siiizeze iiinn ththt e
nfarct and pepeperirir -i-infnfnfarararctctt aaareea a a ofofo CCCDCDCDC-t-treeeatatatededed aaannnimimimalalls.s.. SSupupuppopoportrtr ininng g g ththhisisis ccconononjejejectctc ururre,e,e, mmmyoyoyocyc te cross-
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.113.002863
16
treated, primarily non-randomized patients) showed similar results4. Although late Gd-enhanced
cardiac MRI has been extensively validated for the quantification of necrotic/fibrotic and viable
myocardium in acute/chronic MI6-8, its validity to accurately characterize tissue viability after
cell therapy has been questioned10: cell administration may increase vascular wall thickness,
resulting in decreased vessel permeability and attenuation of Gd-contrast extravasation in cell-
treated myocardial regions, or stimulate angiogenesis, leading to enhanced drainage of Gd-
contrast from the cell-treated myocardium (a phenomenon that has been described in
hypervascular hepatocellular carcinomas11). Any of these confounding factors, if operative,
would result in altered Gd-contrast myocardial kinetics (in the form of decreased contrast
extravasation or accelerated wash-out) that could compromise the fidelity of contrast-enhanced
MRI10.
We sought to validate experimentally the ability of contrast-enhanced MRI to distinguish
and accurately measure scarred from viable myocardium after cell therapy. We find that CDC
infusion does not change vascular density or architecture in scarred and viable myocardium,
neither does it result in altered Gd-contrast myocardial tissue kinetics. Importantly, using post-
mortem histology as the gold standard, we demonstrate that contrast-enhanced MRI readily
distinguishes viable and scarred myocardium and provides accurate measurements of scar size,
scar mass and viable myocardial mass in cell-treated hearts.
The present work differs from previous human3 and porcine12 studies of CDCs in that the
prior studies used autologous cells. The effects of allogeneic CDC therapy reported here are
qualitatively similar, and at least as impressive quantitatively in terms of regenerative and
functional efficacy; however, a head-to-head comparison of allogeneic versus autologous cells
was beyond the scope of this study. The greater increase in EF observed in this study may be
extravasation or accelerated wash-out) that could compromise the fidelity of contnttraraststs -eenhnhnhananancecec dd
MRI10.
WeWeWe ssoooughghhttt toto validate experimentally theee aabbbility of contrasasst-ennhahahannced MRI to distinguish
anndd d aca curatelyy mmmeaasusurrre ssscacacarrrrrededed ffrororommm vvviaaable mmmyocccarrrdiuuummm afaffteeer r ceceelll ttheherrrappypy.. WeWeW ffinininddd thththatat CCCDCDCDC
nnfufufusisiionono ddoeoeoesss nonott cchchananngegee vvasscucuc lalalarrr deded nsnssitttyy y ororor aaarrrchchchiiteeectutuureree iiinnn scsccarara rerer ddd aaanndnd vvviaiabblble ee mymymyoococarrrdidiumumu ,,,
neither does iit t t rereresusuultltlt in nn alaa teeererered dd GdGdGd-c-cconono trtrtrasasast t mmmyoyoyocacac rdrdrdiaiai l tititissssssueueue kkkininineteticicicsss.. ImImImpopoportrtananantltltly,y,y, uuusis ng post-
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.113.002863
17
attributable to one of several factors: 1) increased efficacy of allogeneic cells (not evident in
previous rat studies, which showed equivalence of intramyocardially-injected allogeneic and
syngeneic CDCs18 or cardiospheres25); 2) the earlier administration of CDCs here (2-3 weeks
post-MI, versus 4-5 weeks in our autologous porcine study12 or 1.5-3 months post-MI in
humans3). A comparison of EF values in the present study versus our previous porcine study12
reveals higher baseline EF values in both groups (a finding consistent with the earlier timepoint
of baseline imaging) and a larger decrease in EF in the control group over the period of 2 months
in the present study; EF of the treated group is preserved over time in both studies. These data
may hint that administration of CDCs earlier in the remodeling process may offer increased
functional benefit; and 3) the absence of concomitant anti-remodeling therapies (which in the
human setting leave little room for EF improvement). Allogeneic CDCs induced a mild local
immune reaction in the heart with no signs of immune-related myocardial damage. Importantly,
no circulating anti-donor antibodies could be detected, predicting that no development of panel
reactive antibodies would occur in the human setting (at least after a single administration of
allogeneic cells). The efficacy of allogeneic cells is rationalized by their indirect mechanism of
benefit18, which relies on activation of endogenous reparative and regenerative pathways
(increased cardiomyocyte cycling, upregulation of endogenous progenitors, angiogenesis), rather
than long-term engraftment and differentiation of transplanted cells (no donor cells could be
detected in the recipient myocardium 2 months post-administration).
While cardiac MRI cannot distinguish cardiac hypertrophy from hyperplasia, post-
mortem histological analysis ruled out myocyte hypertrophy as a contributor to the increase in
viable myocardium observed after CDC therapy; myocyte size was actually smaller in the infarct
and peri-infarct area of CDC-treated animals compared to controls, a finding consistent with
functional benefit; and 3) the absence of concomitant anti-remodeling therapies (w(w(whihih chchch iinn n thththe e
human setting leave little room for EF improvement). Allogeneic CDCs induced a mild local
mmmumumunnene rreaeaeactctctionnn ininin the heart with no signs of immmmmmuuune-related myyyoco arrdididiaalal damage. Importantly, f
nno ccciri culatingg aannnti--dodonnonorr r ananantititibobbodidieseses ccoououlld bbee ddeteeecttted, , , pprprededdiccctitinngg tthahatt nonono ddeeveveelelopoppmemementntt oof ff papaaneneel
eeacacactitiivevev aantntntibibibododiieiesss wowooululld d ococcucuc rrr ininin ttthehe hhumumumaanan sssetettttingngng (((atatt llleeaeasttt aaaffnn ttter rr a a a sisiingngglele aaadmdmdmininnisissttratattiooon n ooff ffff
allogeneic celelllslsl ).).). TTTheheh eeeffff icccacacacy yy ofofof aaalllllogogo eneneneieieiccc cececelllll ss s isiss rrrata ioioonananalililizezezed d d bybyby tttheheheiririr iiindndndirirececect t t mememechchc anism of
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.113.002863
18
attenuation of remodeling-associated cardiomyocyte hypertrophy and birth of new (smaller)
myocytes after cell therapy. The latter likely occurs through differentiation of endogenous
progenitors (visualized here as small round TnI+ cells) and induction of resident cardiomyocyte
proliferation in the border zone, in agreement with results from fate-mapping studies24.
Limitations
Our study has several limitations. First, delayed contrast enhancement images were acquired 8
minutes post-Gd administration. Even though the FWHM technique (used here) has been shown
to provide accurate measurement of infarct size as early as 6 minutes post contrast
administration7, standardized protocols issued by the Society for Cardiovascular Magnetic
Resonance advocate waiting at least 10 minutes26 before acquisition of delayed contrast
enhancement images. Second, allogeneic CDCs were derived from a single healthy donor
minipig; we did not investigate inter-donor variability in cell immunogenicity or potency. Finally,
we did not investigate the safety and efficacy of repeat administrations of allogeneic CDCs.
Careful preclinical studies of safety and efficacy will be required before repeat dosing with
allogeneic cells can be contemplated.
Conclusions
In conclusion, we validate the ability of late Gd enhancement MRI to accurately measure scarred
and viable myocardium after cell therapy, supporting the utility of contrast-enhanced MRI for
assessing dynamic changes in the infarct and monitoring therapeutic regenerative efficacy. We
also demonstrate that intracoronary infusion of allogeneic CDCs without immunosuppression is
safe, improves heart function and indirectly promotes cardiac regeneration in a clinically-
relevant porcine model of convalescent MI. The safety and efficacy of allogeneic CDCs in
Resonance advocate waiting at least 10 minutes26 before acquisition of delayed ccononontrtrt asasst tt
enhancement images. Second, allogeneic CDCs were derived from a single healthy donor
miminininipipipigg;g; wwwe e e dddid d nononot t investigate inter-donor variabababillity in cell immumum noogegegennnicity or potency. Finally
wwe ddid not invvesestit ggagatetee thehehe sssafafafetetety y ananand d d eeffffiicaccyy of rrepeppeatt t aadadmmminniniststraratitiononsss ooff aalllllloogogenenneieieic c c CDCDC CsCCs. f
CaCaarerer fufufull prprp ecececlillininicccall l ststuuudiieies s ofoff safafafetetety yy anannd d efefeffifificaaacycyc wwwiilill bebebe rrreqeqequiuiuirerer ddd bebebefofof rrre rrepeppeaeaeatt t dodoosisiingng wwwitith h
allogeneic celelllslsl ccananan bbe e e cocc ntntntemememplplplatata ededd.
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.113.002863
19
human subjects with LV dysfunction post-MI is currently being tested in the phase 1/2
randomized double-blind, placebo-controlled ALLSTAR trial, (ALLogeneic heart STem Cells to
achieve myocArdial Regeneration, NCT01458405)27, which uses infarct size assessed by MRI as
its primary efficacy endpoint.
Acknowledgments: We thank Adrian Glenn, Hao Zeng, Miguel Huerta, Claudia Anchante, Julie
Avalos and Stephen Taylor for their technical and surgical support, Laura Smith for performing
the MRI scans and analyzing MRIs, Nina Duong for blood processing, and David Elashoff and
Tristan Grogan for statistical consulting.
Funding Sources: This work was supported by a grant to RRS from the NIH (HL103356), and
by a grant to EM from the California Institute for Regenerative Medicine. Statistical analysis was
supported by NIH/National Center for Advancing Translational Science (NCATS) UCLA CTSI
Grant Number UL1TR000124.General laboratory support was provided by the Cedars-Sinai
Board of Governors Heart Stem Cell Center.
Conflict of Interest Disclosures: EM and LM own equity in Capricor, Inc. KM is a consultant
for Capricor, Inc. Other authors have no relationships to disclose.
References:
1. Dauwe DF, Janssens SP. Stem cell therapy for the treatment of myocardial infarction. CurrPharm Des. 2011;17:3328-3340.
2. Malliaras K, Marbán E. Cardiac cell therapy: where we've been, where we are, and where we should be headed. Br Med Bull. 2011;98:161-185.
3. Makkar RR, Smith RR, Cheng K, Malliaras K, Thomson LE, Berman D, Czer LS, Marbán L, Mendizabal A, Johnston PV, Russell SD, Schuleri KH, Lardo AC, Gerstenblith G, Marbán E. Intracoronary cardiosphere-derived cells for heart regeneration after myocardial infarction (CADUCEUS): a prospective, randomised phase 1 trial. Lancet. 2012;379:895-904.
4. Chugh AR, Beache GM, Loughran JH, Mewton N, Elmore JB, Kajstura J, Pappas P, Tatooles A, Stoddard MF, Lima JA, Slaughter MS, Anversa P, Bolli R. Administration of cardiac stem
Funding Sources: This work was supported by a grant to RRS from the NIH (HHL1L1L10303033535356)6)6), , ananand
by a grant to EM from the California Institute for Regenerative Mer dicine. Statistiticacaalll anannalalalyssysisisis wwaaa
upported by NIH/National Center for Advancing Translational Science (NCATS) UCLA CTSI
GrGrananant t t NuNuNumbmbmbeeer UUULL1L1TR000124.General laboratororry yy ssupport was prrovoo iddededed bby the Cedars-Sinai
BBBoaarard of Govovererrnnonorsrs HHHeaaartrt SSSteteem m m CeCeCellllll CCCeennteteer.r.r
CoConfnfnflililictctct ooofff InInteteererereststst DDDisisisclclc oso ururreseses::: EEMEM aaandndnd LLLMM M owowownnn eqeqequiuiuitytyty iiinn n CCaCaprprpricicicororor, InInInc.c KKKMM M isisis aa ccconononsususultltltananant t t
for Capricor, , InInInc.c.c OOOththt ererer autututhohohorsss hhhaaveveve nnno oo rererelalalatititionono shshshipipips s tooo dddisisisclcc ososose.ee
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.113.002863
20
cells in patients with ischemic cardiomyopathy: the SCIPIO trial: surgical aspects and interim analysis of myocardial function and viability by magnetic resonance. Circulation. 2012;126(11 Suppl 1):S54-64.
5. Smith RR, Barile L, Cho HC, Leppo MK, Hare JM, Messina E, Giacomello A, Abraham MR, Marbán E. Regenerative potential of cardiosphere-derived cells expanded from percutaneous endomyocardial biopsy specimens. Circulation. 2007;115:896-908.
6. Kim RJ, Fieno DS, Parrish TB, Harris K, Chen EL, Simonetti O, Bundy J, Finn JP, Klocke FJ, Judd RM. Relationship of MRI delayed contrast enhancement to irreversible injury, infarct age, and contractile function. Circulation. 1999;100:1992-2002.
7. Amado LC, Gerber BL, Gupta SN, Rettmann DW, Szarf G, Schock R, Nasir K, Kraitchman DL, Lima JA.. Accurate and objective infarct sizing by contrast enhanced magnetic resonance imaging in a canine myocardial infarction model. J Am Coll Cardiol. 2004;44:2383-2389.
8. Schelbert EB, Hsu LY, Anderson SA, Mohanty BD, Karim SM, Kellman P, Aletras AH, Arai AE. Late gadolinium-enhancement cardiac magnetic resonance identifies postinfarction myocardial fibrosis and the border zone at the near cellular level in ex vivo rat heart. CircCardiovasc Imaging. 2010;3:743-752.
9. Malliaras K, Kreke M, Marbán E. The stuttering progress of cell therapy for heart disease. Clin Pharmacol Ther. 2011;90:532-541.
10. Chin MT, Murry CE. Is it possible to transform cardiac scar tissue into beating heart muscle in humans? Regen Med. 2012;7:623-625.
11. Yu JS, Chung JJ, Kim JH, Kim KW. Small hypervascular hepatocellular carcinomas: value of "washout" on gadolinium-enhanced dynamic MR imaging compared to superparamagnetic iron oxide-enhanced imaging. Eur Radiol. 2009;19:2614-2622.
12. Johnston PV, Sasano T, Mills K, Evers R, Lee ST, Smith RR, Lardo AC, Lai S, Steenbergen C, Gerstenblith G, Lange R, Marbán E. Engraftment, differentiation, and functional benefits of autologous cardiosphere-derived cells in porcine ischemic cardiomyopathy. Circulation.2009;120:1075-1083.
13. Carr JC, Simonetti O, Bundy J, Li D, Pereles S, Finn JP. Cine MR angiography of the heart with segmented true fast imaging with steady-state precession. Radiology. 2001;219:828-834.
14. Simonetti OP, Kim RJ, Fieno DS, Hillenbrand HB, Wu E, Bundy JM, Finn JP, Judd RM. An improved MR imaging technique for the visualization of myocardial infarction. Radiology. 2001;218:215-223.
15. Wagner A, Mahrholdt H, Thomson L, Hager S, Meinhardt G, Rehwald W, Parker M, Shah D, Sechtem U, Kim RJ, Judd RM. Effects of time, dose, and inversion time for acute myocardial infarct size measurements based on magnetic resonance imaging-delayed contrast enhancement.
AE. Late gadolinium-enhancement cardiac magnetic resonance identifies postinfaarcrcctitit onon myocardial fibrosis and the border zone at the near cellular level in ex vivo rat hheeeartrtt. CiCiCircrccCardiovasc Imaging. 2010;3:743-752.
9. Malliaras K, Kreke M, Marbán E. The stutteringg progress of cell therapapy for heart disease. ClClininn PPPhahaharmrmrmacaccoll TTThheher. 2011;90:532-541.
1100. CChin MT, MMMururrryy CCCE.E.E. IIIsss ititit ppposossisis blblb ee too traaansssforrm m caardrdrdiaiacc sccarar tisssusuee inntoto bbbeeaeatitingngng hhheaeaartt mmmuuuscccle nnn hhuumu ans? ReRegeeenn Meedd. 2010112;;;7:626 3-3-3 6622555.
11. YuYu JJS,S, CChuhungn JJJ,J, KKimm JH,H KKimim KW.W SSmamallll hhypervrvasascuculalar r heh papatotocecellulular r cacarcr ini omomass:: vavalul e e aof "washout" ooon nn gagagadodod lilil ninn umumm-e-eenhnhhanana cececed d dydydynananamimim ccc MRMRMR iimamamagigigingngng cccomomompapaparerered d d tototo sssupupperererpapaparararamamm gnetic RRRrronon ooxixidede e-enhnhanancecedd imimagaginingg EuEurr RaRadidiolol 20200909;1;19:9:26261414 2-2626222
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.113.002863
21
J Am Coll Cardiol. 2006;47:2027-2033.
16. Knowles BR, Batchelor PG, Parish V, Ginks M, Plein S, Razavi R, Schaeffter T. Pharmacokinetic modeling of delayed gadolinium enhancement in the myocardium. Magn Reson Med. 2008;60:1524-1530.
17. Drakos SG, Kfoury AG, Hammond EH, Reid BB, Revelo MP, Rasmusson BY, Whitehead KJ, Salama ME, Selzman CH, Stehlik J, Clayson SE, Bristow MR, Renlund DG, Li DY. Impact of mechanical unloading on microvasculature and associated central remodeling features of the failing human heart. J Am Coll Cardiol. 2010;56:382-391.
18. Malliaras K, Li TS, Luthringer D, Terrovitis J, Cheng K, Chakravarty T, Galang G, Zhang Y, Schoenhoff F, Van Eyk J, Marbán L, Marbán E. Safety and efficacy of allogeneic cell therapy in infarcted rats transplanted with mismatched cardiosphere-derived cells. Circulation. 2012;125:100-112.
19. Ordovas KG, Higgins CB. Delayed contrast enhancement on MR images of myocardium: past, present, future. Radiology. 2011;261:358-374.
20. Arai AE. The cardiac magnetic resonance (CMR) approach to assessing myocardial viability. J Nucl Cardiol. 2011;18:1095-1102.
21. Dubois C, Liu X, Claus P, Marsboom G, Pokreisz P, Vandenwijngaert S, Dépelteau H, Streb W, Chaothawee L, Maes F, Gheysens O, Debyser Z, Gillijns H, Pellens M, Vandendriessche T, Chuah M, Collen D, Verbeken E, Belmans A, Van de Werf F, Bogaert J, Janssens S. Differential effects of progenitor cell populations on left ventricular remodeling and myocardial neovascularization after myocardial infarction. J Am Coll Cardiol. 2010;55:2232-2243.
22. Lin YD, Luo CY, Hu YN, Yeh ML, Hsueh YC, Chang MY, Tsai DC, Wang JN, Tang MJ, Wei EI, Springer ML, Hsieh PC. Instructive nanofiber scaffolds with VEGF create a microenvironment for arteriogenesis and cardiac repair. Sci Transl Med. 2012 8;4:146ra109.
23. Davis ME, Motion JP, Narmoneva DA, Takahashi T, Hakuno D, Kamm RD, Zhang S, Lee RT. Injectable self-assembling peptide nanofibers create intramyocardial microenvironments for endothelial cells. Circulation. 2005;111:442-450.
24. Malliaras K, Zhang Y, Seinfeld J, Galang G, Tseliou E, Cheng K, Sun B, Aminzadeh M, Marbán E. Cardiomyocyte proliferation and progenitor cell recruitment underlie therapeutic regeneration after myocardial infarction in the adult mouse heart. EMBO Mol Med. 2013;5:191-209.
25. Tseliou E, Pollan S, Malliaras K, Terrovitis J, Sun B, Galang G, Marbán L, Luthringer D, Marbán E. Allogeneic cardiospheres safely boost cardiac function and attenuate adverse remodeling post-myocardial infarction in immunologically-mismatched rat strains. J Am Coll Cardiol. 2013;61:1108-1119.
past, present, future. Radiology. 2011;261:358-374.
20. Arai AE. The cardiac magnetic resonance (CMR) approach to assessingRR myococarararddidialalal vviaiaiabibibilililityttyJ Nucl Cardiol. 2011;18:1095-1102.
211. . DuDuDuboboboisisis CCC,, LiLiiuu u XX, Claus P, Marsboom G, Pookkrkreeiisz P, Vandennwiww jnngagaaeerert S, Dépelteau H, StrebWW,W, CCChah othahaweww e e L,L,L MMaeaees s F,F,F, GGheheeysysysenenss O,O, DDebebysyserrr ZZZ, GiGillllllijijijnsnsn HH,,, PePeP llllenenss s M,M VVananandeded ndndririesesesscscchehehe TT,rCCChuuauah M, Colllelennn DD,D, VVVererrbebebekekekennn E,E, BBBele mamamans AAA,, Vaann dde WWWererff f FF,F, BBBogggaeaertrtt JJ,, JaJaansnsnssesensnss SSS.. DiDD ffffffererenenenttialefefffeectc s of prorogegg nnnittoor ccellll popoppuululattionsnsn ooonn lefttt vvventrrricccululararar rrremememooodelllinng annd mymyyooccara diiaala tneneoovovasasascuculalaariririzazatitiononon aaftftterer mmyooocacardrdrdiaiaialll ininnfafafarcrcrctititiononn.. J J AmAmAm CCCololollll CaCaCardrdrdioiooll. . 20202 1110;5;5;55:5::2222223232-2-2-22224333.
22. Lin YD, , LuLuLuooo CYCYCY, , HuHuH YYYN,N,N YYYeheheh MMML,L,L, HHHsusuueheheh YCYCYC,, ChChC ananangg g MYMYMY, ,, TsTssaiaia DDDC,C,C, WWWananang g g JNJNJN,,, TaT ng MJ, WeWeii EIEI SpSpriringngerer MMLL HHsisieheh PPCC IInsnstrtrucuctitiveve nananonofifibeberr scscafaffofoldldss wiwithth VVEGEGFF crcreaeatete aa
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.113.002863
22
26. Kramer CM, Barkhausen J, Flamm SD, Kim RJ, Nagel E; Society for Cardiovascular Magnetic Resonance Board of Trustees Task Force on Standardized Protocols. Standardized cardiovascular magnetic resonance imaging (CMR) protocols, society for cardiovascular magnetic resonance: board of trustees task force on standardized protocols. J Cardiovasc Magn Reson. 2008;10:35.
27. Allogeneic Heart Stem Cells to Achieve Myocardial Regeneration (ALLSTAR) (NCT01458405). Available at: http://clinicaltrials.gov/ct2/show/NCT01458405?term=allstar&rank=1. Accessed February 28, 2013.
Figure Legends:
Figure 1. Study protocol. Schematic depiction of the 24-hour retention study (A) and the
validation study (B).
Figure 2. Allogeneic CDCs attenuate adverse remodeling and improve global and regional
function compared to controls. A,B: Matched cine short-axis images (at end-diastole [ED] and
end-systole [ES]) at baseline and 2 months (videos of the cine acquisitions are provided in the
Online Supplement) for a minipig treated with allogeneic CDCs (A) and a control minipig (B).
Images were obtained at similar levels (note the similar morphology of papillary muscles).
Changes in ejection fraction (C), end-diastolic volume (D) and end-systolic volume (E) from
baseline to 2 months in controls and CDC-treated minipigs. Systolic thickening (F) and end-
systolic thickness (G) in infarcted (infarct) and non-infarcted (remote) segments at 2 months
post-infusion in controls and CDC-treated minipigs (* p<0.05 vs CDC-treated group).
Figure 3. Allogeneic CDCs decrease scar size, decrease scar mass and increase viable
Figure 1. Study protocol. Schematic depiction of the 24-hour retention study (AA) ) anananddd ththheee
validation study ((B)).
FFiFiguuure 2. AlAllologeeenneeic CCDDCDCss atatttet nun atatatee adaddverrssee remomomodedelililingngng aaanndd impmpmproveee ggglolobabaall ana dd d reeegigiionnnal
funcnctitiono ccomompaparred d toto conntrtrolls.s. AA,BB: Maatctchehedd cicinen shohortrt-a-axixiss imimagageses ((ata eendnd-d-diaiaststole e [E[ D]D] aandnd
enendd-sysyststololee [E[ES]S])) atat bbasaselelininee anandd 22 momontnthshs ((vividedeosos ooff ththee cicinene aaccququisisititioionsns aarere pprorovividededd inin tthehe
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from
DOI: 10.1161/CIRCULATIONAHA.113.002863
23
myocardial mass compared to controls, as assessed by MRI. A: Representative delayed contrast-
enhanced MRI acquisitions of hearts in short-axis section at end-diastole. Scarred myocardium
appears white while viable myocardium appears black. In the CDC-treated minipig the scar
decreased in transmurality and viable myocardial mass increased over the period of 2 months
after CDC infusion. The control minipig was characterized by scar thinning and scar expansion,
with no evidence of increase in viable myocardium over the same time period. Changes in scar
size (B), scar mass (C) and viable mass (D) from baseline to 2 months in controls and CDC-
treated minipigs. E: Scar size at baseline and at months post-infusion in control and CDC-treated
minipigs. Scar mass (F) and viable mass (G) at 2 months post-infusion in controls and CDC-
treated minipigs (* p<0.05 vs CDC-treated group, # p<0.05 vs baseline).
Figure 4. Allogeneic CDCs decrease scar size and increase viable myocardial mass compared to
controls, as assessed by post-mortem histology. A: Representative short-axis cardiac slices of 2
CDC-treated and 2 control minipigs at 2 months post-infusion after incubation with TTC. Slices
were obtained at similar levels (note the similar morphology of papillary muscles). Viable
myocardium stains brick-red, while scarred myocardium appears white (unstained). B:
Representative sections from the infarcted wall of a treated and a control minipig stained with
Masson’s trichrome. Viable myocardium stains red, while collagenous scar stains blue. CDC-
treated hearts exhibited significant amounts of viable myocardium in the infarcted wall, in the
form of endocardial and epicardial muscular layers surrounding the scar and in the form of islets
of viable myocardial tissue dispersed in-between the collagen fibers. In control minipigs the scar
was largely transmural. Scar size (C), scar mass (D), viable mass (E) and scar transmurality (F)
at 2 months post-infusion in controls and CDC-treated minipigs, as assessed by post-mortem
reated minipigs (* p<0.05 vs CDC-treated group, # p<0.05 vs baseline).
Fiigugugurerere 444. AlAlAllllogegeeneneneici CDCs decrease scar size aaanndnd iincrease viablleee myyocococaaardial mass compared to
coonntntror ls, as assssesessseed d bybyb popopoststst-m-m-morortetetemmm hhhissstoloogogyy. AAA: Repepprrereseseennttatatiivvee shshoorrt---axaxisisis ccarardidid acacc sslil cececes s ofofof 2
CDCDDC-C-C-trtrtreaeateteed d d ananddd 22 2 cocontntroror l l mmiminininipipipigsgsgs aatt t 22 momomonttthshsh popoposts --iinfnffusususioion nn afaffteeerrr inini ccucubbabatitiiononon wwititithh h TTTTCC.C. SSllliccees
were obtaineed d d atata sssimimimilillararar levevvelelels (n(n(nototo eee thhhee e sisisimimim lalalar r r momomorprprphohoololologygygy ooof f f papp pipipilllllararary y y mumumuscscclelees)s)s).. ViViV able
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.113.002863
24
histology (* p<0.05 vs CDC-treated group).
Figure 5. Comparison of cardiac MRI with histology for assessment of scarred and viable
myocardium after cell therapy. A: TTC-stained cardiac slices matched with their corresponding
delayed contrast-enhanced MRI images (from both the in vivo and ex vivo MRI datasets) for a
CDC-treated and a control minipig. Areas of hyperenhancement in cardiac MRIs correspond
excellently to regions of scarred myocardium in histological slices. The treated minipig MRI
demonstrates endocardial and epicardial rims of non-hyperenhanced tissue in the infarcted wall
which correspond excellently to endocardial and epicardial TTC-positive muscular layers
surrounding the scar in histological slices. The control heart is characterized by a transmural
scar, and no viable myocardium can be detected in the infarct area by either MRI or histology.
Correlation of MRI measurements of scar size as % of isolated cardiac slices (for in vivo [B] and
ex vivo [C] MRI), scar size as % of LV, LV scar mass and LV viable mass (D) with the
corresponding histological measurements.
Figure 6. Gd-contrast myocardial kinetics in cell-treated hearts. A: A series of dynamic delayed
contrast enhancement images with a fixed T1 were acquired and signal intensity of specific areas
(collagenous scar, viable myocardium in the infarcted region, viable myocardium at the border
zone, remote myocardium) was measured at various timepoints following contrast administration,
resulting in the generation of site-specific Gd-contrast curves in all cell-treated minipigs. B: Gd-
contrast kinetics pooled data from all treated minipigs. Analysis using a linear mixed effects
model demonstrated that Gd-contrast kinetics were identical in cell-treated viable (non-
hyperenhanced) areas and in the remote non-cell treated healthy myocardium. Image on the right
urrounding the scar in histological slices. The control heart is characterized by a aa trranaa smsmsmurururalalal
car, and no viable myocardium can be detected in the infarct area by either MRI or histology. d
CoCorrrrrrelelelatatatioioionn n ofofo MMMRRIRI measurements of scar size aaasss %%% of isolated cararardiacacc sssllilices (for in vivo [B] and
exx vvvivi o [C] MRMRI)II ,, sccaarar sssiizizeee asasas %% oooff f LVLVV,, LVVV ssccar mmassss aaandnd LLV V vvviaabablele mmmaasass s (((DDD) ) wiwiwiththh tthheh
coorrrrrresesspopopondnddinining g hihiistttolologoogiciccalal mmmeaeasususurererememementnttss.s.
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.113.002863
25
in A is the corresponding histological section stained with Masson’s trichrome of the inset in the
MRI acquisitions.
Figure 7. Vessel density and architecture. A: Vascular density and architecture were evaluated
by immunostaining for -sarcomeric actinin, -smooth muscle actin and isolectin. Image on the
right is a high-power image of inset on left. B: Vessel density in the border zone (defined as the
region at the edges of the scar comprising areas of both scarred and viable myocardium). Vessel
density (C), lumen diameter (D), total wall thickness, endothelial layer thickness, smooth muscle
layer thickness (E) and lumen to wall ratio (F) in viable myocardium in the infarcted wall
(viable), in the collagenous scar (scar) and in the remote non-infarcted myocardium (remote) (*
p<0.05 vs CDC-treated group).
Figure 8. Allogeneic CDCs attenuate myocyte hypertrophy and promote endogenous
regeneration in the infarct and peri-infarct area. A: Cardiomyocyte cross-sectional area in the
infarct and peri-infarct area. B: Cycling cardiomyocytes (arrows) in the infarct and peri-infarct
area. C: Small TnI+ cells (arrows; image on the right is a magnification of the inset on left) in
the infarct and peri-infarct area (* p<0.05 vs CDC-treated group).
viable), in the collagenous scar (scar) and in the remote non-infarcted myocarddiuiuum mm (r(rrememmototote)e)e) ((*
p<0.05 vs CDC-treated group).
FFiguugure 8. Alloogegeenneeicc CCDCDCDCs s atatatttetenunuuaatate e mymyoc ytytee hyyyppeertrroropphphyyy aanandd prromomoooteee enenndododogegennonoususu
eegegegenenenerarar titiononon iin n tthhee e ininfffarrcrct t annnd dd pepepeririri-i-i-infnffarara ctctct aaarerea.aa. AAA: CaCaardrddioioiomymymyococo yyyteee crcrc ooosss--sesectctc ioioionanaall l aaareaeaa iinn n ththhe
nfarct and pepeperirir -i-infnfnfarararctctt aaareea.a.a BBB: CyCyCyclclcliningg g cacacardrdrdioioiomymymyocococytyty esess ((arararroror wswsws)) innn t ttthehehe iiinfnfnfarara ctctct aaandndnd pppere i-infarct
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from

Figure 1
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from

Figure 2
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from

Figure 3
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from

Figure 4
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from

Figure 5
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from

Figure 6
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from

Figure 7
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from

Figure 8
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from

Marbán and Eduardo MarbánBlusztajn, Ileana Valle, Supurna Chowdhury, Raj R. Makkar, Rohan Dharmakumar, Debiao Li, LindaTseliou, James F. Dawkins, Michelle Kreke, Ke Cheng, Daniel Luthringer, Chak-Sum Ho, Agnieszka
Konstantinos Malliaras, Rachel R. Smith, Hideaki Kanazawa, Kristine Yee, Jeffrey Seinfeld, Elenia Porcine Model of Convalescent Myocardial Infarction
Validation of Contrast-Enhanced MRI to Monitor Regenerative Efficacy after Cell Therapy in
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 2013 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation published online September 23, 2013;Circulation.
http://circ.ahajournals.org/content/early/2013/09/23/CIRCULATIONAHA.113.002863World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circ.ahajournals.org/content/suppl/2013/09/23/CIRCULATIONAHA.113.002863.DC1Data Supplement (unedited) at:
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer available in the
Permissions in the middle column of the Web page under Services. Further information about this process isOnce the online version of the published article for which permission is being requested is located, click Request
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Circulation Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from

SUPPLEMENTAL MATERIAL
SUPPLEMENTAL METHODS
Culture of porcine CDCs
A Sinclair mini-pig heart from a ~4 months old male was obtained from Sinclair BioResources to create
a master cell bank (MCB). The heart arrived on ice submerged in cardioplegic solution. Hearts were grossly
dissected and biopsy-sized pieces (~25mg) were seeded to create explant derived cells (EDCs). After ~14
days, the EDCs were harvested to create a MCB. MCB vials were thawed and cultured as cardiospheres
(CSps) in suspension culture. CDCs were grown by seeding CSps on tissue culture treated flasks, and
passaged when confluent. Passage 5 CDCs were resuspended in CryoStor™CS10 (BioLife Solutions) with
100 U/mL heparin in cryobags (for a total dose of 12.5 M cells/10 mL), placed directly in a CryoMed controlled-
rate freezer, and then transferred to liquid nitrogen. CDCs were thawed at the day of the infusion. Upon
thawing, 100 U/mL heparin and 50 µg/mL nitroglycerin were added as excipients to each 10 mL dose.
MI creation and CDC infusion
On day 0, animals were premedicated with ketamine 20mg/kg IM, atropine 0.05mg/kg IM, and
acepromazine 0.25mg/kg IM. Animals were subsequently induced with propofol 2-4mg/kg IV to effect,
intubated, and maintained on isoflurane 2-3%. Amiodarone 10mg/kg IV loading dose, then 0.5mg/kg IV as
needed and lidocaine 0.03µg/kg/min were given for ventricular arrhythmias. Heparin 100IU/kg IV was given for
anticoagulation. Minipigs were subjected to an anteroseptal MI by inflation of an angioplasty balloon in the mid-
left anterior descending artery (LAD) (distal to the 1st diagonal brach) for 2.5 h., followed by coronary
reperfusion. Two to 3 weeks after MI creation, infarcted minipigs were re-anesthetised using the same protocol
and drug regimen. Pigs were randomized to receive 12.5 million CDCs (in 10 mls of CryostorTMCS10
containing 45 μg/ml nitroglycerin and 180 U/ml heparin) or vehicle. Intracoronary infusion was performed via
an over-the-wire balloon catheter, placed in the mid LAD. CDCs or vehicle solution were infused in 3 cycles of
intermittent balloon inflation. Minipigs were euthanized either 24 hours post-infusion, to measure short-term
cardiac retention of administered cells, or 2 months later.

Histocompatibility
To assess histocompatibility, low-resolution swine leukocyte antigen (SLA) typing was performed on the
donor Sinclair minipig and all recipient Yucatan minipigs as described elsewhere (1,2). Divergent pig strains
were used to simulate the typical allogeneic conditions in human transplantation where donor and recipient are
frequently mismatched with regard to human leukocyte antigen. Complete SLA mismatch was confirmed if
there was at least one class I and one class II antigen mismatch at the allele group level between donor and
recipient.
Ex vivo luciferase assay
The ex vivo luciferase assay, a method with high sensitivity and reproducibility (3) (depicted
schematically in Supplemental Figure 1a) was performed as described (4). In brief, CDCs were transduced
with an adenoviral vector carrying the firefly luciferase gene 3 days prior to infusion. For each animal a
separate standard curve was constructed, as transduction efficiency and transgene copy number per cell vary
by experiment. Specifically, once the cell dose was allocated for infusion, an aliquot of cells (from the same
batch of adenovirally-transduced cells) was cultured for an additional 24 hours. Twenty-four hours after cell
delivery, the explanted LV was cut into 1g samples that were subsequently homogenized and analyzed for
luciferase signal. The animal-specific standard curve was prepared by measuring the luciferase signal from pig
myocardial samples from the left atrium (not infused with cells) spiked with known numbers of transduced
CDCs.
Histology
To evaluate immune rejection in the heart, hematoxylin and eosin-stained sections from myocardial
samples (fixed in 10% formalin, paraffin-embedded [FFPE]) obtained from the infarct and peri-infarct area
(n=4-6 slides/heart) and the remote myocardium (n=2 slides/heart) were analyzed by an experienced cardiac
pathologist blinded to treatment allocation (DL). Analysis was graded according to the International Society for
Heart & Lung Transplantation (ISHLT) grading system, used in clinical practice to diagnose solid organ
transplant rejection. Morphometric analysis with Masson’s trichrome staining was performed on 8 μm sections
from myocardial samples (FFPE) extending from the viable myocardium at the edges of the scar to the core of
the collagenous scar (n=4 slides/heart). To study vascular density and architecture, 8 μm sections from
samples (FFPE) obtained from the infarct, peri-infarct (n=4-6 slides/heart) and remote (n=2 slides/heart) areas
underwent immunostaining for α-sarcomeric actinin (Sigma), α-smooth muscle actin (Abcam) and isolectin
(Molecular probes). Arterioles and arteries were defined as smooth-muscle-coated vessels with external
vascular diameter (lumen + vascular walls) <75 μm and >75μm respectively. To measure myocyte cross-
sectional area, 8 μm sections from myocardial samples (FFPE) obtained from the infarct, peri-infarct (n=4-6
slides/heart) and remote (n=2 slides/heart) areas underwent immunostaining for α-sarcomeric actinin and
wheat-germ agglutinin (Molecular probes) (to visualize cell borders). Cardiomyocytes were accepted for size
measurement if they met the following criteria: (a) cellular cross-sections present (b) visible nuclei located
close to the cell center and (c) intact cell borders (17). To measure cardiomyocyte cell-cycling, 8 μm sections
from myocardial samples (FFPE) obtained from the infarct and peri-infarct area (n=4-6 slides/heart) underwent
immunostaining for α-sarcomeric actinin and Ki67 (Thermo). To visualize myocyte progenitors, 8 μm sections
from myocardial samples (FFPE) obtained from the infarct & peri-infarct area (n=4-6 slides/heart) underwent
immunostaining for Troponin I (Sigma). Alexa Fluor-conjugated secondary antibodies (Molecular probes) were
used and slides were counterstained for DAPI (Molecular probes). Sections were imaged using a confocal
laser scan microscope (Leica Microsystems) and images were processed by Leica Application Suite software.
Peri-infarct (border zone) area was defined as the region at the edges of the scar (comprising areas of both
viable and scarred myocardium).
Fluorescence In Situ Hybridization
Two to 3 weeks post-MI infarcted female mini-pigs were intracoronarily infused with allogeneic CDCs
derived from a male mini-pig donor to enable cell detection Fluorescence In Situ Hydridization (FISH).
ZytoLight porcine X/Y Dual Color Probe and ZytoLight FISH-Tissue Implementation Kit (ZytoVision GmbH)
were used to prepare slides and test for the porcine Y and X chromosomes. Sections obtained from 3 sites
were used for FISH analysis: central infarct region, infarct border zone and normal myocardium Three to 6

slides (1 or 2 from each of the 3 sites) were selected for each of the animals for analysis. A simple preparation
of male CDCs served as a positive control for the method (Supp Fig 2A).
On day one, slides were incubated for 10 minutes on a hot plate (VWR, Digital Heatblock) at 70°C,
followed by two 10 minute incubations in xylene (Sigma). Next, the slides were incubated for 5 minutes each in
100%, 100%, 90%, and 70% ethanol. In order to keep the Heat Pretreatment Solution Citric Solution at 98°C, a
coplin jar was kept in a hot water bath at boiling temperature. Immediately before placing slides in the jar, the
Heat Pretreatment Solution Citric Solution was brought up to boiling temperatures in a microwave. The solution
was placed inside the warmed up coplin jar along with the slides, slides were incubated at 98°C for 15 minutes.
Slides were then washed twice for 2 minutes in deionized water and then water was blotted off. Pepsin solution
was added drop-wise to slides and incubated for 10 minutes at 37°C in a humidity chamber. Slides were
washed for 5 minutes in Wash Buffer SSC and for 1 minute in deionized water. Slides were dehydrated by
placing in a series of ethanol concentrations, 70%, 90%, and 100% for 1 minute each. Slides were allowed to
air dry. The remaining steps were performed in the dark to protect the probe. ZytoLight FISH probe (10µL) was
pipetted onto the slide, a coverslip was placed over the probe and sealed with rubber cement. The slide was
placed on a heat block at 72°C for 10 minutes. Finally, slides were incubated overnight in a humidity chamber
at 37°C. On day two, slides continued to be protected from light. Rubber cement was carefully removed and
the slides were placed in 1 X Wash Buffer at 37°C for 3 minutes to ensure coverslip removal. Slides were then
washed twice in 1 X Wash Buffer at 37°C for 5 minutes. Slides were incubated in a series of ethanol
concentrations, 70%, 90%, and 100% for 1 minute each. After being allowed to air dry, 1 drop (~30µL) of
VECTASHIELD Mounting Medium with DAPI (Vector Laboratories) was added to the slide. A coverslip was
placed over the mounting medium and sealed with nail polish. Slides were stored in the dark at 4°C until ready
to analyze. Slides were analyzed using a confocal microscope (Leica TCS SP-X, Leica Microsystems CMS
GmbH) with three filters, red, blue, and green. Images were analyzed using LAS AF Lite (Leica Microsystems
CMS GmbH) and Image J.

References
1. Ho CS, Lunney JK, Franzo-Romain MH, Lee JH, Smith DM.. Molecular characterization of swine leucocyte
antigen class I genes in outbred pig populations. Anim Genet. 2009;40:468-78.
2. Ho CS, Lunney JK, Lee JH, Franzo-Romain MH, Martens GW, Rowland RR, Smith DM.. Molecular
characterization of swine leucocyte antigen class II genes in outbred pig populations. Anim Genet.
2010;41:428-32.
3. Terrovitis JV, Smith RR, Marbán E. Assessment and optimization of cell engraftment after transplantation into
the heart. Circ Res. 2010;106:479-494.
4. Johnston PV, Sasano T, Mills K, Evers R, Lee ST, Smith RR, Lardo AC, Lai S, Steenbergen C, Gerstenblith G,
Lange R, Marbán E. Engraftment, differentiation, and functional benefits of autologous cardiosphere-derived
cells in porcine ischemic cardiomyopathy. Circulation. 2009;120:1075-1083.
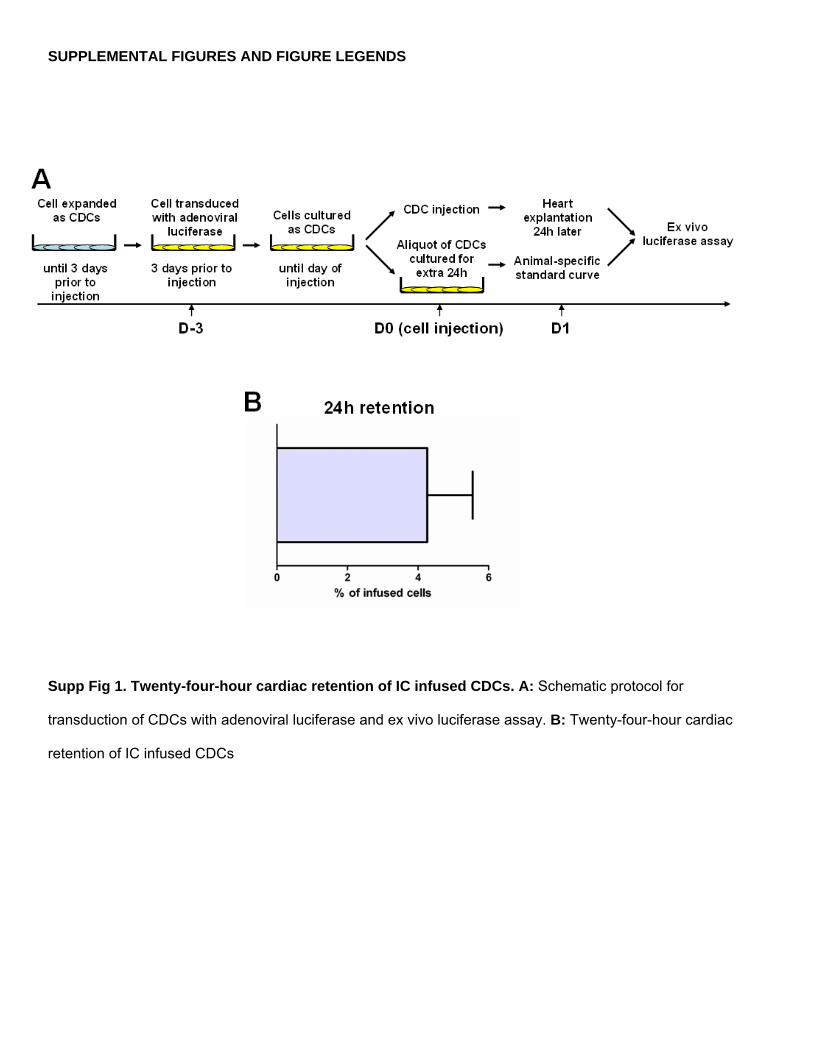
SUPPLEMENTAL FIGURES AND FIGURE LEGENDS
Supp Fig 1. Twenty-four-hour cardiac retention of IC infused CDCs. A: Schematic protocol for
transduction of CDCs with adenoviral luciferase and ex vivo luciferase assay. B: Twenty-four-hour cardiac
retention of IC infused CDCs

Supp Fig 2. Long-term engraftment of IC infused CDCs. A: Control preparation of male donor CDCs show
both red and green fluorescence signals in each nucleus, corresponding to one X and one Y chromosome,
respectively, in each cell. B: A male CDC (box) in the recipient myocardium at 2 weeks post-infusion.
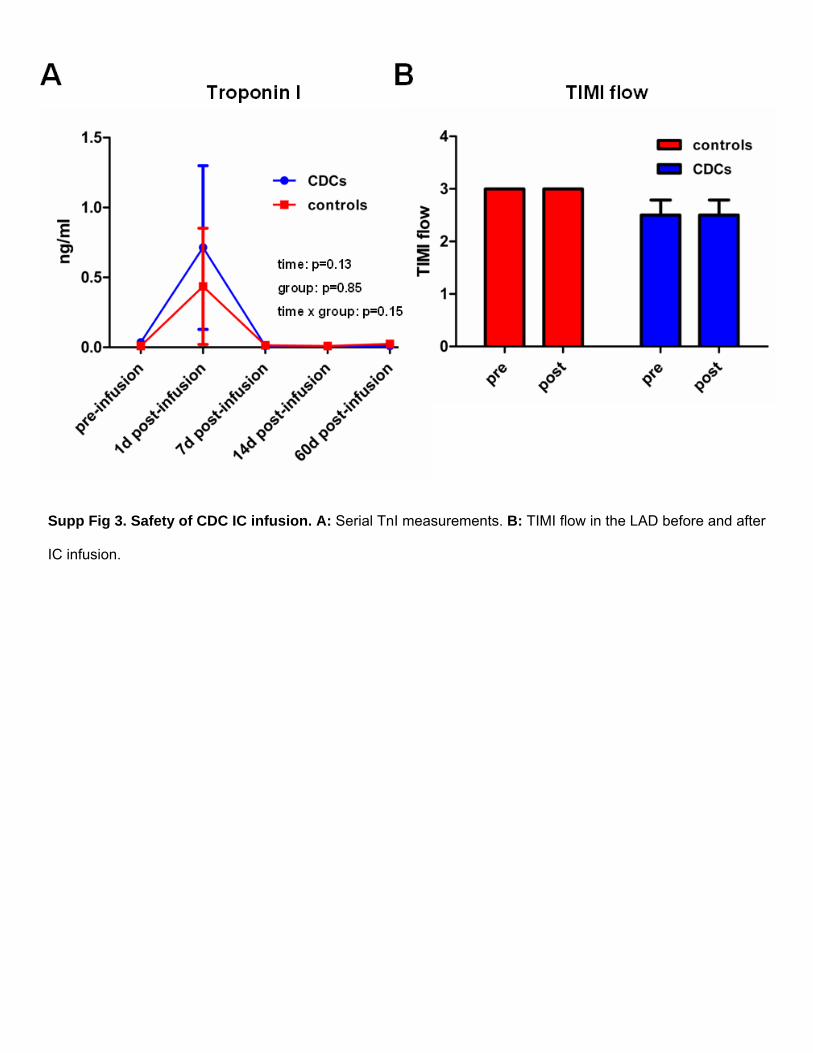
Supp Fig 3. Safety of CDC IC infusion. A: Serial TnI measurements. B: TIMI flow in the LAD before and after
IC infusion.
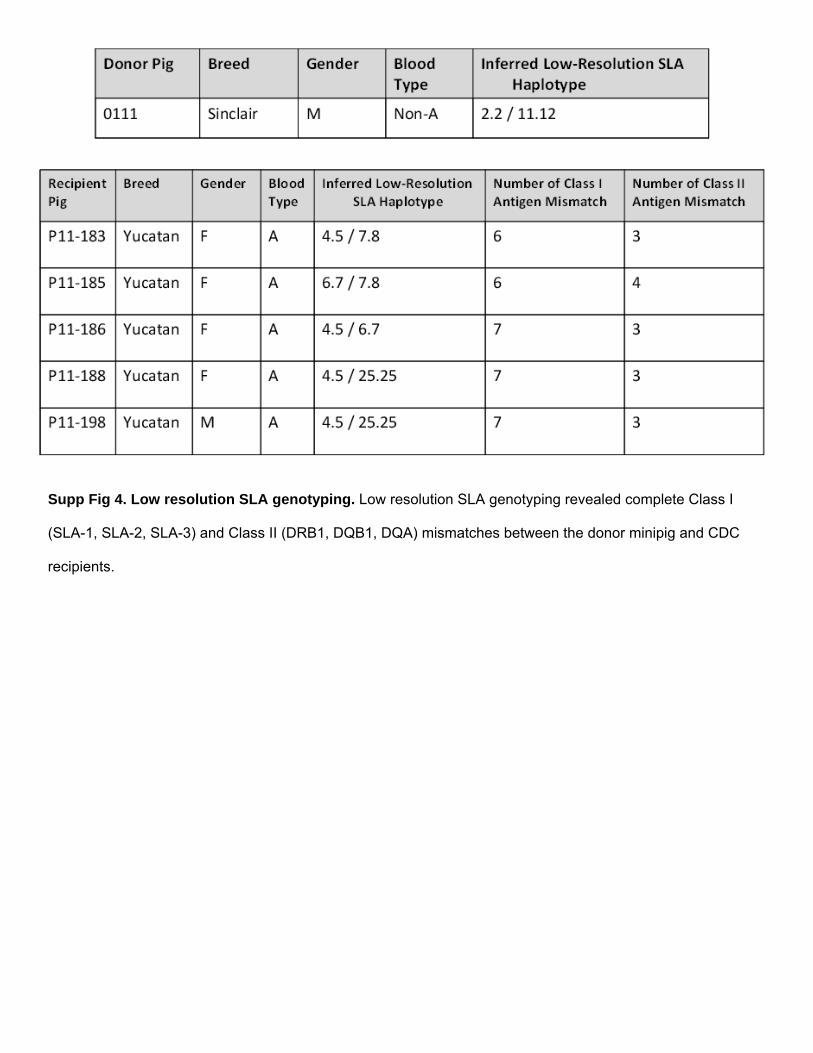
Supp Fig 4. Low resolution SLA genotyping. Low resolution SLA genotyping revealed complete Class I
(SLA-1, SLA-2, SLA-3) and Class II (DRB1, DQB1, DQA) mismatches between the donor minipig and CDC
recipients.

Supp Fig 5. Immune reaction to allogeneic CDCs. A: Increased focal lymphoplasmacytic infiltration (Grade
1R), deemed to be unrelated to the natural inflammatory response to the ischemic insult, was detected in the
peri-infarct area of CDC-treated minipigs (16/22 slides) compared to placebo. B: Representative image of
H&E-stained heart section revealing infiltrating cells localized within the interstitial space. C, D: Recipient
minipig serum samples were screened for circulating anti-donor IgG antibodies by flow cytometry. No
alloreactive antibodies were detected in any recipients of allogeneic CDCs at any time point. In contrast, in
minipigs that were allosensitized by intradermal and subcutaneous PBMNC injections, high titers of circulating
alloreactive IgG antibodies were detected at two weeks post-injection.
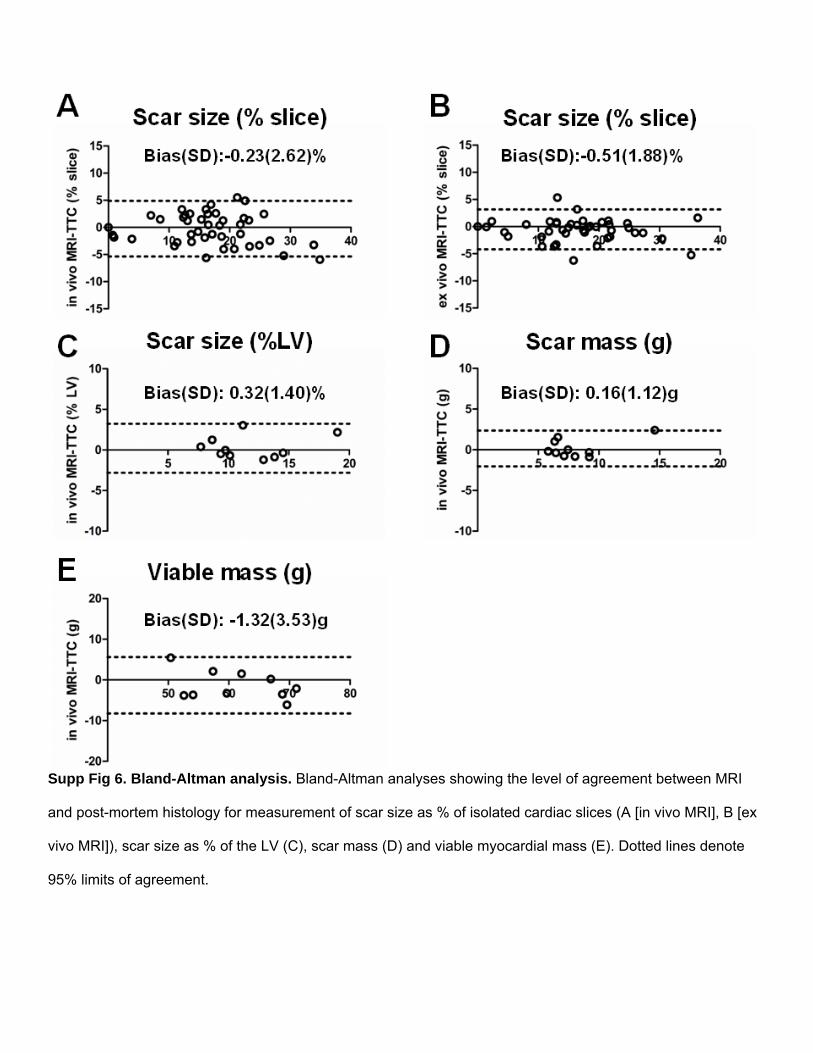
Supp Fig 6. Bland-Altman analysis. Bland-Altman analyses showing the level of agreement between MRI
and post-mortem histology for measurement of scar size as % of isolated cardiac slices (A [in vivo MRI], B [ex
vivo MRI]), scar size as % of the LV (C), scar mass (D) and viable myocardial mass (E). Dotted lines denote
95% limits of agreement.

Supp Fig 7. Cardiomyocyte cross-sectional area in the remote myocardium.

SUPPLEMENTAL TABLES
ID group
EF base (%)
EDV base (ml)
ESV base (ml)
scar mass base (g)
scar size base
(% LV)
viable mass base (g)
EF 2mos (%)
EDV 2mos (ml)
ESV 2mos (ml)
scar mass 2mos
(g)
scar size
2mos (%)
viable mass 2mos (m)
11P183 CDCs 47.76 63.49 33.17 5.94 8.84 61.25 46.56 83.76 44.76 5.72 7.92 66.5211P185 CDCs 49.79 76.44 33.38 8.27 12.88 55.93 44.83 99.24 54.75 7.61 9.79 70.0911P186 CDCs 43.23 70.29 39.90 7.61 11.69 57.48 45.96 93.12 50.32 6.86 9.28 67.0311P188 CDCs 46.08 69.08 37.25 10.39 16.28 53.45 48.40 92.50 47.73 6.75 9.14 67.0811P198 CDCs 49.91 74.21 37.18 7.87 14.36 46.93 48.37 73.27 37.59 6.26 9.74 58.0311P182 controls 49.65 81.05 40.81 6.35 11.50 48.88 37.68 88.89 55.39 7.39 12.73 50.6711P187 controls 46.62 67.16 35.85 8.34 13.69 52.59 38.03 89.85 55.68 8.76 14.35 52.2712P03 controls 42.92 71.54 40.84 13.99 18.93 59.92 32.70 132.97 89.50 15.81 20.10 62.8412P58 controls 49.79 71.26 35.78 7.23 13.16 47.69 40.11 97.61 58.46 7.45 12.30 53.1412P59 controls 48.08 75.19 39.04 8.51 13.40 54.96 39.15 109.15 66.42 9.03 13.38 58.46
Supp Table 1. A complete list of MRI-measured parameters for each experimental animal (EF: ejection fraction; EDV: End-diastolic volume; ESV: End-systolic volume; LV: left ventricle; base: baseline; mos: months).
ID group
scar size TTC
(% LV)
scar mass
TTC (g)
viable mass
TTC (g) 11P183 CDCs 7.52 5.91 72.6411P185 CDCs 10.47 8.44 72.211P186 CDCs 8.04 5.84 66.811P188 CDCs 9.61 7.51 70.611P198 CDCs 9.77 6.64 61.3211P182 controls 9.69 5.85 54.511P187 controls 14.71 9.65 55.9412P03 controls 17.93 13.4 61.3412P58 controls 13.51 7.45 47.6812P59 controls 14.25 9.36 56.33
Supp Table 2. A complete list of histological measurements of scar size, scar mass and viable mass for each experimental animal (TTC: 2,3,5-triphenyltetrazolium chloride).

LEGENDS FOR VIDEO FILES
Supplemental Video 1. Video of short-axis cine acquisition of a CDC-treated pig at baseline (before CDC
infusion).
Supplemental Video 2. Video of short-axis cine acquisition of a CDC-treated pig at 2 months post-CDC
infusion.
Supplemental Video 3. Video of short-axis cine acquisition of a control pig at baseline (before vehicle infusion).
Supplemental Video 4. Video of short-axis cine acquisition of a control pig at 2 months post-vehicle infusion.