Embed Size (px)
Citation preview

Jean-François Rahier , MD
CHU UCL Mont- Godinne, Belgium
Vaccinations in patients with immune mediated inflammatory diseases

“Safety means first aid to the uninjured”
unknown author


10472 situations !!
Immune mediated inflammatory diseases in GI
Ulcerative Colitis
Crohn’s disease

Immunomodulatory drugs commonly used in gastro
Corticosteroids
Methotrexate (MTX)
Azathioprine (AZA) and analogues
Anti Tumor Necrosis Factor α agents (infliximab (IFX),
adalimumab (ADA), certolizumab)
Cyclosporine

Potential triggers of autoimmunity
• Viral infection (Epstein Barr virus, Human Herpes virus-6,
HIV, Human Parvovirus B19…)
• Bacterial infection (Campylobacter jejuni, Yersinia
enterocolitica, Streptococcal group A, H Pylori …)
• Parasitic infection (malaria, schistosomiasis, leishmaniasis…)
• Vaccines
• Silicone implants
• Occupational and chemical exposures
Molina V et al., Autoimmunity 2005

Vaccination and auto immune diseases
Reality or fairy tales ?

IMID (Dermatology) following vaccination... Reality or fairy
tales ?
• Extremely rare cases of psoriasis following BCG vaccination
• No induction of psoriasis by other vaccines in large database !
• Köbner phenomenon !
R Koca et al., J Trop Ped 2004
K Takayama et al., Acta Derm Venereol 2008
BCG vaccination:

IMID (Gastroenterology) following vaccination... Reality or
fairy tales ?
- Controversial statement: Measles-vaccination may play a role in
the development of IBD
NP Thompson et al., Lancet 1995
No association Measles, mumps and rubella
(infection/vaccination) and onset of IBD
M Feeney et al., Lancet 1997
RL Davis et al., Arch Pediatr Adolesc Med 2001
C Bernstein et al., Inflamm Bowel Dis 2007
-
Measles vaccination:

IMID (Rheumatology) following vaccination... Reality or fairy
tales ?
• Arthritis and MMR: increased risk of joint symptoms in
immunized children BUT risk of frank arthritis less than after
wild rubella infection!
• RA : transient rise in rheumatoid factor or some form of
arthritis in patient immunized with variety of viruses (tetanus,
thyphoid, parathyphoid, mumps, diphtheria, polio, smallpox )
BUT
• Incidence of RA among vaccinated population not higher than
in non vaccinated population !
CM Benjamin et al., BMJ 1992; K Aho et al., Acta Path Microbiol Scand 1962;RN
Peeler et al,. Ann Intern Med 1956;LT Kurland et al., May Clin Proc 1984
MMR, tetanus, thyphoid, parathyphoid, mumps, diphtheria,
polio, smallpox, HBV

IMID following vaccination... Reality or fairy tales ?
• There are subjects who, subsequent to vaccination have developed
diseases that they may not have developed if not vaccinated
• We are not able to identify those subjects and not all who have the
genetic predisposition end up with post vaccine autoimmune
illness
• ?? Would those subjects who acquired autoimmune illnesses after
immunization, have acquired those illnesses had they been
exposed to the natural infection?
Y Shoenfeld et al., J Autoimmunity 2000

Which vaccines for adults ?
Increased severity of infection in
immunocompromised patients ?
Routine:
Tetanus No
Diphtheria No
Pertussis No
Polyomyelitis No
Measles Yes
Canada Communicable Disease Report (CCDR RMTC). Advisory Committee Statement (ACS) - Committee to Advise on Tropical Medicine and Travel (CATMAT) The Immunocompromised Traveler. 04/2007

Which vaccines for adults ?
Canada Communicable Disease Report (CCDR RMTC). Advisory Committee Statement (ACS) - Committee to Advise on Tropical Medicine and Travel (CATMAT) The Immunocompromised Traveler. 04/2007
In selected groups:
Invasive Pneumococcal Disease Yes
Influenza Yes
Others:
Human Papilloma virus Yes
Varicella /Zoster Yes
Hepatitis B Yes
Increased severity of infection
in IC patients ?

Which vaccines for adults ?
Canada Communicable Disease Report (CCDR RMTC). Advisory Committee Statement (ACS) - Committee to Advise on Tropical Medicine and Travel (CATMAT) The Immunocompromised Traveler. 04/2007
Travel related
vaccine:
Hepatitis A No
Typhoid fever ?
Yellow fever ?
Japanese encephalitis No
Meningococcal meningitis ?
Tick born encephalitis ?
Rage No
(TBC/BCG) Yes
Cholera ?
Increased severity of infection
in IC patients ?

Live and inactivated vaccines

Do we need vaccines in IMID patients ? - HBV
- Prevalence of HBV in IBD population = general population
BUT consequences are different !
- Numerous reports of HBV infections in IBD patients
- Risk of reactivation and hepatic failure in chronic HBV
carriers
- Treatment for HBV – unfriendly for IBD
Esteve M et al, Gut 2004; Loras C et al, Am J Gastroenterol 2009; Chevaux JB et al,
Inflamm Bowel Dis 2009

Do we need vaccines in IBD? - VZV
- Immunosuppression increases the risk of dissemination and
complications such as pneumonia, hepatitis, encephalitis, or
haemorrhagic disorders
- Fatal cases of primary varicella infection in young IBD
patients
Arvin AM, Clin Microbiol Rev 1996; Hambleton S, Clin Microbiol Rev 2005; Deutsch DE, J Pediatr Gastroenterol Nutr 1995; Leung VS, Am J Gastroenterol 2004; Vergara M,Gastroenterol Hepatol 2001

Do we need vaccines in IBD? - HPV
- Higher incidence of abnormal Pap smears in women with IBD
- Increased risk in patients treated with immunomodulators
Kane S et al, Am J Gastroenterol 2008; Bhatia J et al, World J Gastroenterol 2006; Zabana Y
et al, Inflamm Bowel Dis 2009; Lees CW et al, Inflamm Bowel Dis 2009

Recommended vaccine in IMID patients ?
Rahier JF et al, J Crohn Colitis 2009

Recommended vaccine in IMID patients ?
Van Assen S et al, Ann Rheum Dis 2011

Recommended vaccine in IMID patients ?
Basic vaccines:
Tetanus (every 10 yrs)
Diphtheria (every 10 yrs)
Pertussis (1x)
Polio (1x)
HP Brezinschek et al., Curr Opin Rheumatol 2008 ; B Sands et al., Inflamm Bowel Dis
2004; JF Rahier et al., JCC 2009 ; M Lebwohl et al., J Am Acad Dermatol 2008; British
Society for Rheumatology 2002, Van Assen Ann Rheum Dis 2011
http://rheumatology.org.uk/guidelines/guidelines_other/vaccinations/view
Superior Health Council www.health.fgov.be/CSS_HGR
CDC http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5515a1.htm

Recommended vaccine in IMID patients ?
IMID Patients
Vaccine Impact
disease
in IC
patients ?
Belgian
Superior
Health
Council
CDC RA
Association
European
Crohn &
Colitis
Org.
Am.
Psoriasis
Found.
Influenza Increased
mortality
YES YES YES YES YES
Pneumo Increased
mortality
subgroups YES YES YES
HP Brezinschek et al., Curr Opin Rheumatol 2008 ; B Sands et al., Inflamm Bowel Dis
2004; JF Rahier et al., JCC 2009 ; M Lebwohl et al., J Am Acad Dermatol 2008; British
Society for Rheumatology 2002, Van Assen Ann Rheum Dis 2011
http://rheumatology.org.uk/guidelines/guidelines_other/vaccinations/view
Superior Health Council www.health.fgov.be/CSS_HGR
CDC http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5515a1.htm

4. Recommended vaccine in IMID patients ?
HP Brezinschek et al., Curr Opin Rheumatol 2008 ; B Sands et al., Inflamm Bowel Dis
2004; JF Rahier et al., JCC 2009 ; M Lebwohl et al., J Am Acad Dermatol 2008; British
Society for Rheumatology 2002, Van Assen Ann Rheum Dis 2011
http://rheumatology.org.uk/guidelines/guidelines_other/vaccinations/view
Superior Health Council www.health.fgov.be/CSS_HGR
CDC http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5515a1.htm
IMID Patients
Vaccine Impact
disease
in IC
patients ?
Belgian
Superior
Health
Council
CDC RA
Association
European
Crohn &
Colitis
Org.
Am.
Psoriasis
Found.
HPV Increased
morbidity
(yes )
Selected
YES
Varicella
/Zoster
Increased
mortality
YES YES YES
HBV Increased
morbidity
subgroups Sub
groups
(yes)
At risk
YES

Safety of a vaccine
in terms of
• Adverse events
• Risk for flare up of the IMID
• Risk for infection by the vaccine itself (live vaccines)
Safety of a vaccine – adverse events
When evaluating the safety of a vaccine ,
consider “safety” of the disease !
Idiopathic thrombocytopenia following MMR vaccination: 1/
30000 vaccinated children. Risk of thrombocytopenia after
natural rubella or measles infection is 1/3000 and 1/6000
respectively!
DC Wraith et al,. Lancet 2003;362:1659-66

When evaluating the safety of a vaccine , consider “safety” of the disease !
Rahier JF et al, APT 2010
1918 – Spanish flu A/H1N1
40 millions deaths
WHO 2010:17000 H1N1 related deaths
88%

When evaluating the safety of a vaccine , consider “safety” of the disease !
Rahier JF et al, APT 2010
Rahier JF et al, APT 2010

When evaluating the safety of a vaccine , consider “safety” of the disease !
Rahier JF et al, APT 2010
Prepare and prevent, don't repair and repent.

Effect of vaccination (non-live vaccines) on IMID disease activity
Rahier JF, Rheumatology 2010; Brezinschek HP, Curr Opin Rheumatol 2008; Melmed
GY, Am J Gastroenterol 2010; Mamula P, CGH 2007; Lu Y, Am J Gastroenterol
2009, Chaparro M , P172 ECCO 2010 ; Rahier JF , Gut 2011
Safety of a vaccine – adverse events
Vaccination in patients with AIIRD should ideally be administered during stable disease (EL 5 RG D)

Efficacy of a vaccine
1/ demonstration of field efficacy
preferably trough well-conducted and well-controlled vaccine
efficacy trials; different possible end points (infection, disease,
hospitalization, death); in different settings and populations
not always possible or feasible…
SA Plotkin, CID 2008
Efficacy of a vaccine
2/ immunological markers (adaptive immune system)
used as “correlate” and/or “surrogate” of protection (against infection and/or disease)
MOST OFTEN :
demonstration of B cell–generated antibodies
- seroconversion & geometric mean titers / peak titers
- quality (e.g. avidity; bactericidal / opsonic / neutralizing antibodies; etc)
- rapidity of decline of titers or long term persistence
ALSO : effector T cells / memory B & T cells
SA Plotkin, CID 2008
Efficacy of a vaccine
- No vaccine is completely effective
- Heterogeneous studies( disease and combination of therapies)
Brezinschek HP, Curr Opin Rheumatol 2008
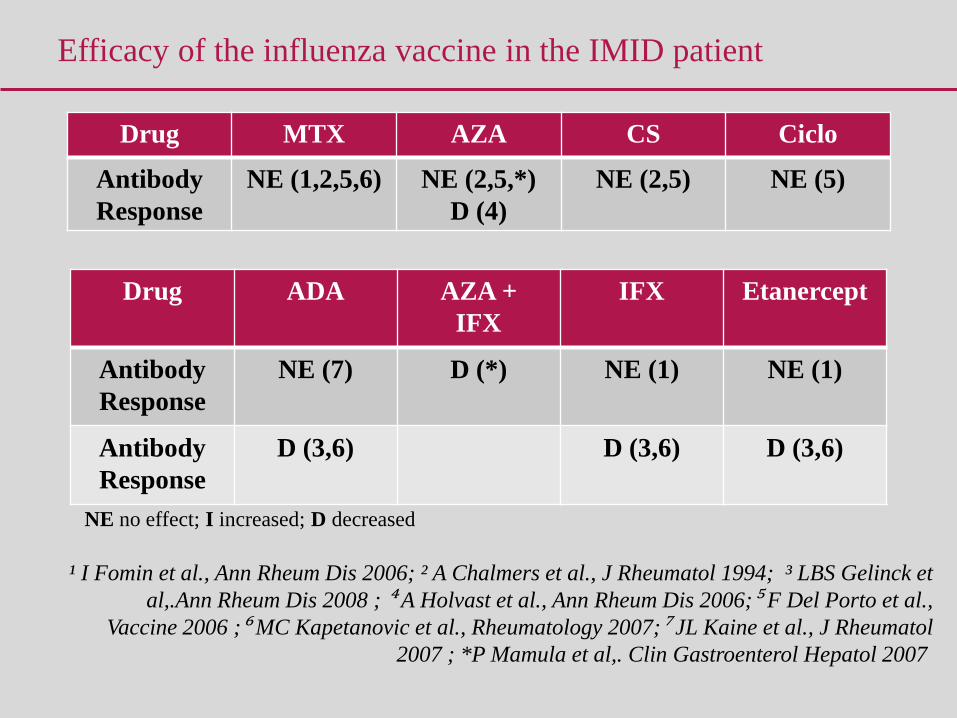
Efficacy of the influenza vaccine in the IMID patient
¹ I Fomin et al., Ann Rheum Dis 2006; ² A Chalmers et al., J Rheumatol 1994; ³ LBS Gelinck et
al,.Ann Rheum Dis 2008 ; ⁴ A Holvast et al., Ann Rheum Dis 2006;⁵ F Del Porto et al.,
Vaccine 2006 ;⁶ MC Kapetanovic et al., Rheumatology 2007;⁷ JL Kaine et al., J Rheumatol
2007 ; *P Mamula et al,. Clin Gastroenterol Hepatol 2007
Drug MTX AZA CS Ciclo
Antibody
Response
NE (1,2,5,6) NE (2,5,*)
D (4)
NE (2,5) NE (5)
Drug ADA AZA +
IFX
IFX Etanercept
Antibody
Response
NE (7) D (*) NE (1) NE (1)
Antibody
Response
D (3,6) D (3,6) D (3,6)
NE no effect; I increased; D decreased

Influenza vaccine
- Decreased response in patients with IM+biologicals compared
to IM alone or IBD without IM: similar to controls ( healthy )
- The proportion of seroprotected patients and geometric mean
titers at post-vaccination were similar between NIS and IS
groups for all three strains
Mamula P CGH 2007; Lu Y Am J Gastro 2009; Debruyn JC , IBD 2011;
Efficacy of a vaccine in IBD
No vaccine is completely effective

Cullen G, Gut 2011
Efficacy of a vaccine in IBD

Melmed GY Am J Gastro 2010 ; Fiorino G, IBD 2011
Pneumococcal polysaccharide
Patients IBD IM+biologicals IBD no
IM
Healthy
controls
Vaccine response 40% 80% 85%
AZA: 79%
Biologics: 58%
Combination: 63%
88%
Efficacy of a vaccine in IBD

Efficacy of a vaccine in IBD
HBV vaccine
- various regimens (0, 1 and 2 months- 0,1 6)
- various cut-off point for adequate immunity (>10 mUI/ml or 100 mUI/ml)
- 211 IBD
- Response rate lower for patients on anti-TNF
- Overall , response rate in 60% patients
Chaparro M , P172 ECCO 2010 Prague
HPV vaccine (Gardasil ®; HPV6-11-16-18)
17/34 (50%) on immunomodulator therapy and 17/34 on anti-TNF therapy; majority of subjects had inactive disease throughout the study No serious adverse events Immune response to each serotype in the vaccine was strong and comparable to healthy controls
Lu, DDW 2011
Efficacy of a vaccine in IBD

Efficacy of vaccines in IMID patients
Rahier JF, Rheumatology 2010;

Efficacy of a vaccine IMID - summary
Heterogeneous results:
- Disease itself and treatment may impair response to vaccine
- Some anti TNF agents may impair the immune response for influenza vaccine and probably HBV vaccine
- MTX seems to impair responsiveness for pneumococcal vaccine
Brezinschek HP, Curr Opin Rheumatol 2008; Rahier JF JCC 2009; Van Assen S Ann
Rheum Dis 2011
Immunization is an unimpeachable measure to defend
against major causes for increased morbidity and mortality
Safety of the YF & other live vaccines
• Corticostéroïdes
• Méthotrexate
• Léflunomide
• Azathioprine & 6-mercaptopurine
• Cyclosporine A
• Cyclophosphamide
• Tacrolimus, Everolimus, Sirolimus, Temsirolimus
• Mycophenolat mofetil
• Anti Tumor Necrosis Factor α agents, Adalimumab (Humira®), certolizumab (Cimzia®),etanercept (Enbrel®), golimumab (Simponi®) en infliximab (Remicade®)
• Autres anticorps monoclonaux et biologiques: Rituximab (Mabthera®), Abatacept (Orencia®), Tocilizumab (Roactemra®), Basiliximab (Simulect®), Natalizumab (Tysabri®) et autres en cours de développement: Muromonab-CD3, …
• Antitumoraux: agents alkylants, antimétabolites, antibiotiques antitumoraux, inhibiteurs de la topo-isomérase, inhibiteurs des microtubules et antitumoraux divers

Safety of the YF & other live vaccines
• Severely immunosuppressed travelers strongly discouraged from
travel to destinations with true risk of yellow fever. If travel is
unavoidable and the vaccine is not given, travelers should be
instructed in methods to avoid mosquito bites and should be provided
a vaccination waiver letter.
• Patients with limited immune deficits (chronic hepatic disease
(cirrhosis and alcoholism), diabetes, and nutritional deficiencies,
interferon for hepatitis C infection) or asymptomatic HIV should be
offered the choice of vaccination and monitored closely for possible
adverse effects
CDC Travelers' Health - Yellow Book
http://wwwn.cdc.gov/travel/yellowBookCh9-Immunocompromised.aspx

Safety of Zoster vaccine
Therapy with low-doses immunomodulatory drugs for treatment of
rheumatoid arthritis, psoriasis, polymyositis, sarcoidosis, inflammatory
bowel disease, and other conditions including :
• methotrexate (<0.4 mg/Kg/week),
• azathioprine (<3.0 mg/Kg/day), or
• 6mercaptopurine (<1.5 mg/Kg/day)
are not considered sufficiently immunosuppressive to create vaccine
safety concerns and are not contraindications for administration of
zoster vaccine. … with antiviral therapy should complications ensue.
Prevention of Herpes Zoster ; Recommendations of the Advisory Committee on Immunization
Practices (ACIP); Recommendations and Reports June 6, 2008 / Vol. 57 / RR-5 Morbidity
and Mortality Weekly Report www.cdc.gov/mmwr

9. Vaccination of House hold Contacts of Persons with Altered
Immunocompetence
• Household and other close contacts of persons with altered immunocompetence : all age-appropriate vaccines, with the exception of live OPV and smallpox vaccine.
• MMR, varicella, and rotavirus vaccines should be administered when indicated. MMR vaccine viruses are not transmitted to contacts, and transmission of varicella vaccine is rare.
• To minimize potential rotavirus transmission, hand hygiene measures after contact with feces of a rotavirus-vaccinated infant for at least 1 week.
• Annual influenza vaccination.
General Recommendations on Immunization. Recommendations of the Advisory Committee
on Immunization Practices (ACIP)Morbidity and Mortality Weekly Report
Recommendations and Reports December 1, 2006 / Vol. 55 / No. RR-15
Centers for Disease Control and Prevention www.cdc.gov/mmwr

10. Timing of vaccination
Best before the start of immunomodulator therapy :
• Better immunogenicity (i.e MTX)
• No contraindication in case of live vaccines
• Patient today = traveler tomorrow
For live vaccine, if possible to interrupt temporarily the IMs
• How long to wait before vaccine administration : 3 months (except for
corticosteroids : 1 month)
• How long to wait to restart drug after the vaccination : 3-4 weeks
HP Brezinschek et al., Curr Opin Rheumatol 2008;20:295-299
Van assen S et al, Ann Rheum Dis 2011; JF Rahier et al., JCC 2009
British Society for Rheumatology 2002,
http://rheumatology.org.uk/guidelines/guidelines_other/vaccinations/view
M Lebwohl et al., J Am Acad Dermatol 2008;58 (1):94-105

Vaccination in practice in IMID
• Best before introduction of immunomodulator therapy.
• Immunization status of patients with IMID patients should be
checked and vaccination considered for routinely administrated
vaccines: tetanus, diphteria, poliomyelitis, pertussis.
• Immunization for specific vaccines must be considered in every
patient following national or international guidelines
• Vaccines for patients on immunomodulators traveling in
developing countries or frequently traveling around the world
should be discussed with an appropriate specialist.