Embed Size (px)
Citation preview

Using Data to Promote Continuity of Care and Increase Accountability

D E C E M B E R 1 7 , 2 0 1 3 W A S H I N G T O N , D C
KAREN WOLK FEINSTEIN, PHD PRESIDENT AND CHIEF EXECUTIVE OFFICER PITTSBURGH REGIONAL HEALTH INITIATIVE
USING DATA TO PROMOTE CONTINUITY OF CARE AND
INCREASE ACCOUNTABILITY

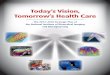
THE SYSTEMS VISION: TRANSFORMING THE CARE OF COMPLEX PATIENTS
Acr
oss
Car
e Se
tting
s
Essential Services System Requirements
Care Mgt
Clinical Pharmacy
Patient Engagement
Health IT
QI Training
Performance Incentives
Collaboration and
Integration
Medication Reconciliation
Informed, Activated, Discerning
Consumers, particularly at End-of-Life
Data to Treat,
Measure, Evaluate
Perfect Patient Care
Rewards for
Collaboration
Hospice/Palliative Long-Term Care
Rehab
Hospital
Emergency Services
Specialty Care
Primary Care
Screening and Tx
Behavioral Health

© Pittsburgh Regional Health Initiative 2013 4
What is essential to our vision for reducing
readmissions?
Care Management
Clinical Pharmacy
Patient Engagement
Behavioral Health
HIT QI Training
Isn’t reimbursed

JHF CURRENT PROGRAMS TESTING HOW TO KEEP PEOPLE OUT OF HOSPITALS
REACH Regional Extension
Center
PRIMARY CARE RESOURCE
CENTER
TOMORROW’S HEALTHCARETM
Salk Fellowship
PARTNERS IN INTEGRATED
CARE
Long-Term Care Champions
Health Careers Futures
Lean Engagements
PERFECTING PATIENT CARESM
UNIVERSITY
RAVEN Reduce Avoidable
Hospitalizations among Nursing Facility Residents
MAI Minority AIDS Initiative
Patient Safety
Fellowship
QI2T Center Where Quality
Improvement meets Information Technology
COMPASS Care Of Mental, Physical,
And Substance Use Syndromes
Safety Net Medical Home
Initiative
HIV QI in AIDS Service Organizations
The Fine Awards
Excellence in QI
Closure (End-of-Life and Palliative Care)
QI2T Health Innovators Fellowship


Connecting LTPAC to the
Healthcare System of the Future
LTQA’s 3rd Annual Conference December 17th, 2013

Physician Office
Living at Home
CBS Outpt. Rehab
Home Health
Adult Day Care
PACE
Acute Care
Hospital Psych Hospital
Hospice Facility
Home Hospice
Outpt. Behav. Health
Acuity of Illness
Inte
nsity
of C
are
Adapted from Derr and Wolf, 2012
Low
High
High
Outpatient Testing/Pharmacy/DME
8
The Spectrum of Care is Vast…

Physician Office
Living at Home
CBS Outpt. Rehab
Home Health
Adult Day Care
PACE
Acute Care
Hospital Psych Hospital
Hospice Facility
Home Hospice
Outpt. Behav. Health
Acuity of Illness
Inte
nsity
of C
are
Adapted from Derr and Wolf, 2012
Low
High
High
Outpatient Testing/Pharmacy/DME
9
…as are the Barriers to Care Coordination

IMPACT Grant
February 2011 – HHS/ONC awarded $1.7M HIE Challenge Grant to state of Massachusetts (MTC/MeHI):
Improving Massachusetts Post-Acute Care Transfers (IMPACT)
10

Datasets for Coordinated Care
• Traditionally – What the sender thinks is important to the receiver
• Future – Also take into account what the receiver says they need
• 1000+ Receiver surveys, along with national and international review
11

12
Consultation Note: • Office Visit to PHR • Consultant to PCP • ED to PCP, SNF, etc…
Referral Note: • PCP to Consultant • PCP, SNF, etc… to ED
Transfer Summary: • Hospital to SNF, PCP, HHA, etc… • SNF, PCP, etc… to HHA • PCP to new PCP
Home Health Plan of Care (with esMD Digital Signature)
Care Plan
NYeC, Healthix, CCITINY, ASPE, S&I LCC, HL7, and Lantana update C-CDA for MU3

LAND & SEE • Sites with EHR or electronic assessment tool
use these applications to enter data elements –LAND (“Local” Adaptor for Network
Distribution) acts as a data courier to gather, transform, and securely transfer data if no support for Direct SMTP/SMIME or IHE XDR (live since 10/2012)
• Non-EHR users complete all of the data fields and routing using a web browser to access their “Surrogate EHR Environment” (SEE) (go-live 1/7/2014)

Hassle-Free to ED
St. Vincent Hospital
Reliant Medical Group’s Epic EHR
Outside Record Icon in MedHost Bedboard
CCD with SVH MRN
ADT for Reliant
Patients
CCD with SVH MRN
30 seconds after ED registration, Reliant’s CCD Summary Document is automatically loaded into ED’s EHR using LAND


Using HIT to Promote Continuity of Care and Increase
Accountability
LTQA December 2013 Kelly Cronin

HIT Efforts Supporting Care Integration
12/19/2013
EHR Incentives and HIT Certification Programs Stage 2 – Transitions of Care Measures; include sharing
summary records with LTPAC Stage 3 – TBD but care plans and advanced directives
are being considered by advisory committees HIT certification for LTPAC under consideration with
the goal of enabling interoperability across the care continuum
ACO spread, priorities and their HIT/HIE infrastructure can support continuity of care across acute, post-acute and long-term care settings Recent ACO survey showed reducing SNF utilization
and increasing community/home based care to be a priority

HIT Resources for LTPAC
12/19/2013
Enabling Health Information Exchange – Challenge grants and Beacon Communities KeyHIE http://transform.keyhie.org/
LAND and SEE http://mehi.masstech.org/what-we-do/hie/impact/land-and-see
LTPAC HIT website; existing Community of Practice; and Issue Brief http://www.healthit.gov/policy-researchers-
implementers/long-term-post-acute-care http://www.healthit.gov/sites/default/files/pdf/HIT_LTPAC
_IssueBrief031513.pdf

Current and Future HHS Programs and Policies advancing HIT in LTPAC
12/19/2013
State Innovation Models – many testing states are prioritizing LTPAC and LTSS to be part of multi-payer accountable care communities and primary care integration models
Value based Purchasing for SNFs and HH has the potential to drive adoption of interoperable HIT and exchange
HHS HIE Acceleration Strategy http://www.healthit.gov/sites/default/files/acceleratinghieprinciples_strategy.pdf HHS will seek to ensure that all new regulations and guidance
on existing programs enable a patient’s health information to follow them wherever they access care to support patient-centered care delivery.
Steps to accelerate HIE will stem from Affordable Care Act delivery reform programs and Medicare and Medicaid payment


Answers for life. Restricted © Siemens AG 2013 All rights reserved.
LTPAC and Care-Process Optimization Jim Walker 2013.12.03

Restricted © Siemens AG 2013 All rights reserved. Page 22
Outline
• Need
• What a solution would look like
• Early Information Services
• A Developing Solution

Restricted © Siemens AG 2013 All rights reserved. Page 23
Need
• Strategic Need
• High-reliability, high-efficiency provision to every patient of every relevant grade-A recommendation

Restricted © Siemens AG 2013 All rights reserved. Page 24
Need
• Strategic Need
• High-reliability, high-efficiency provision to every patient of every relevant grade-A recommendation
• Current State
• 2003: 55% received evidence-based interventions. McGlynn (2003) "The Quality of Health Care Delivered to Adults in the United States." NEJM 348: 2635-45.
• 2011:

Restricted © Siemens AG 2013 All rights reserved. Page 25
Need
• Strategic Need • High-reliability, high-efficiency provision to every patient of
every relevant grade-A recommendation
• Current State
• 2003: 55% received evidence-based interventions.
• 2011: 44% got evidence-based medication before PCI.
Borden (2011) Patterns and intensity of medical therapy in patients undergoing PCI. JAMA 305(18): 1882-89.

Restricted © Siemens AG 2013 All rights reserved. Page 26
Need
• Strategic Need
• High-reliability, high-efficiency provision to every patient of every relevant grade-A recommendation
• Salient Need
• High-reliability, high-efficiency care processes for the BCPI 48 (aka 90-day bundles)

Restricted © Siemens AG 2013 All rights reserved. Page 27
What a Solution Would Look Like
• Shared Care Processes
• Hospital
• LTPAC
• Patient
• Home Health
• Lay Caregiver
• Clinic

Restricted © Siemens AG 2013 All rights reserved. Page 28
Early Information Services
• ADT-based Alerts
• Auto-extracts of MDS and OASIS
• Regional, networked PHR (portal)
• Process-Management Reports

Restricted © Siemens AG 2013 All rights reserved. Page 29
Care-Process Optimization System
Process monitoring prompts re-contextualization and reporting.
Evidence-based, Engineered Model Process
Contextualization to Patient Needs and Preferences
Contextualization to specific Care Setting
Instantiated Process for BPM


Using HIT to Promote Continuity of Care and Increase Accountability
Karen Collishaw LTQA
December 2013 www.chapinc.org

To define and advance the highest quality of community-based care by:
• Objectively validating the excellence of community health care practice through consistent measurement of the delivery of quality service
• Motivating providers to achieve continuous improvement by adhering to standards of excellence
• Assisting the public in the selection of community health services and providers with demonstrated excellence
• Leading by example through organizational excellence and quality performance
32
CHAP’s Purpose

Integrated electronic applications and forms Automated workflow reminders and email
messaging Innovative reporting functionality to track long-
term performance Improved accreditation process Workflow driven Alerts and journal functionality to improve
communications