Embed Size (px)
Citation preview

Dr Alex Aiken
London School of Hygiene and Tropical Medicine, UK
Usefulness
and challenges of SSI
surveillance in
settings with limited
resources: proposals for
feasible approaches
ICAN Conference, Harare, November 2013

Outline2
1. Why do surveillance for SSI ?
2. How to do SSI surveillance ?
3. How to do SSI surveillance with limited resources ?
4. Uses of SSI surveillance data ?
5. Challenges of SSI surveillance ?

What is a Surgical Site Infection (SSI)?
CDC/NHSN definition of SSI: “Infection occurring at the operation site within 30 days of the procedure.”
Less severe, but harder to
reliably diagnose
More severe, but
less common
ref: Horan TC, Am J Inf Cont 2008

SSI rates in high-income countries
USA: 2.6/100 surg. proc.
Europe: 3/100 surg. proc.
General surgery
3.1%
4.5%
4.7%
Abdominal surgery
23%
11%
Haridas et al, Surgery 2008
Misteli et al, Arch Surg 2009
Hawn et al, J Am Coll Surg ‘08
Greif et al, NEJM 2000
Duttaroy et al, Surg Infect 2009
Gaines RP et al, CID 2001
HELICS, SSI statistical report 2004

Allegranzi B et al.
Lancet 2011;377:228-41
Published on 5 May 2011
http://www.who.int/gpsc/en/
Bagheri Nejad S, et al. Bull OMS
2011;89:757-765
What about low and middle income countries ?

Africa Americas
Eastern
Med. Europe
South-East
Asia West Pacific Internat. Total
Type of
infection Adult Ped Adult Ped Adult Ped Adult Ped Adult Ped Adult Ped Adult Ped Adult Ped All
HAI
general 6 1 31 20 14 3 29 4 15 5 7 6 4 0 106 39 145
SSI 7 3 16 3 8 0 8 0 12 0 5 0 0 0 56 6 62
VAP 1 1 5 0 8 0 4 1 6 2 1 1 0 0 25 5 30
BSI 0 0 5 2 1 1 3 1 3 3 0 2 0 0 12 9 21
HAP 0 1 3 0 0 0 3 0 2 1 0 1 0 0 8 3 11
UTI 1 0 1 0 2 0 2 0 1 0 0 0 0 0 7 0 7
Total 15 6 61 25 33 4 49 6 39 11 13 10 4 0 214 62 276
Type of study by region (pre 2009)
All single centre studies, variable quality

Ethiopia: 21%
15%
Tanzania: 19%
24%
Uganda: 10%
Nigeria: 16-31%
Kenya: 19%
CAR: 18%
SSI incidence in Africa (studies from 1995-2009)
Bagheri Nejad S et al. WHO Bull 2011;89:757–765
Algeria: 12%

Ethiopia
12% & 18% (Obs)
SSI frequency in specific African countries
(studies from 2010-2013)
Nigeria
12% (Obs)
16% (Obs)
17% (Abd S)
20% & 24% (Ped)
Sudan
25% (GS)
Tanzania
26% (GS)
Kenya
7% (Ped)
Burkina
24% (GS)
Mali
12% (Ped)
Egypt
17% (GS)

Proportions of hospital-acquired infection, by type
29
24
19
1513
17
27
11
2421
20
36
11 11
22
0
5
10
15
20
25
30
35
40
L/M Income Europe USA
SSI
UTI
BSI
HAP/VAP
OTHERS
%

What is surveillance ? 10
“Epidemiological surveillance is the continued watchfulness over
the distribution and trends of incidence through the systematic
collection, consolidation and evaluation of morbidity and mortality
reports and other relevant data, and the regular dissemination of
data to all who need to know.”
Collection
Systematic Evaluation of disease data
Dissemination
NB: surveillance ≠ research

1. Why do SSI surveillance ? 11
SENIC: Study on the Efficacy of Nosocomial Infection
Control, conducted by CDC, USA 1974-80
This was conducted as there were:
Increasing numbers of “vulnerable” patients
Emerging bacterial resistance to antibiotics
Increasing rates of HAI observed in USA in 1960-70’s

SENIC study: methods12
Comparison 338 hospitals sampled from across the USA
Measured the rates of nosocomial infections in random samples of 500 patient-admissions from each hospital
Standardised definitions of HAI used.
Measured confounding factors: size and type of hospital, region, nurse-to-patient ratio and many others.
Assessed the quality of Hospital Infection Control Program in each hospital
Ref: Haley, RW. “Efficacy of infection surveillance and control programs in preventing nosocomial infections in US hospitals”, Am J Epi 1985

SENIC study: SSI13
Excellent
Good
Fair
Poor
Excellent
Good
Fair
PoorSurveillance
Activity
Infection
Control Activity
Results: lowest rates of
nosocomial infection with
the combination of
surveillance and IC activity

SENIC study: results14
Hospitals with an “effective” infection control program had 32% lower rates of HAI, even after controlling for other differences between hospitals.
Recommendations from SENIC:
An “effective” Infection Control Program requires
1. A system of surveillance for detecting HAI
2. An Infection Control Physician
3. 1 Infection Control Nurse / 250 beds
4. A system of reporting infection rates to practicing surgeons

2. How to do SSI surveillance ? 15
In USA – following CDC recommendations
Other high-income countries typically follow these.
Important principles
Lead by infection control staff
30-day follow-up time-period
Both IP and OP periods
Combine data from diverse sources
Risk stratification by NNIS criteria

3. How to do SSI surveillance with limited $
In many African hospitals …
Lack of IPC facilities, materials, staff, budget
Limited microbiology services
Excessive (+ irrational?) antibiotic usage
Hard to discriminate prophylaxis v treatment ?
SSI surveillance very rarely performed

17
Kenya
AIC Kijabe Hospital, Nairobi
Jack Barasa, Carol Mwangi,
Peter N’thumba…
Uganda
1. Kisiizi Hospital, Kisiizi
Gabriel Okumu, Robert
Mugrobe, Agnes Katwsigye…
2. Mulago Hospital, Kampala
Peter Ongom, Alex Elobu,
Dorah Nakamwa…
Zimbabwe
Parirenyatwa Hospital, Harare
Sheba Chuma, Matthew Wazara,
Salome Biri…
Zambia
Ndola Central Hospital, Ndola
Joseph Musowoya, Margaret
Kasepa, Mayaba Maimbo…
Benedetta Allegranzi
Alex Aiken
Zeynep Kubilay
Joyce Hightower
Sean Berenholtz
Kathryn Taylor
And many, many others
Project planning throughout 2013,
SSI surveillance since Jan 2014 – currently ongoing

SUSP study format – ideally 18
SSI Surveillance
SUSP intervention
1
Start of data collection
approx Jan 2014
End data collection
approx Dec 2014
SSI Surveillance
SUSP intervention
2
SSI Surveillance
SUSP intervention
3
SSI Surveillance
SUSP intervention
4
SSI Surveillance5SUSP intervention

SUSP study format – actually 19
SSI Surveillance
SUSP intervention
1
Start of data collection
approx Jan 2014
End data collection
approx March 2015
SSI Surveillance
SUSP intervention
2
SSI Surveillance
SUSP intervention
3
SSI Surveillance
SUSP intervention
4
SSI Surveillance
SUSP intervention
5
Now

3. How to do SSI surveillance with limited $
There is no “right” method for surveillance …
(but there are probably some “wrong” ones !)
Important questions
- What data to collect, over what time-period ?
- How to evaluate the data ?
- What will you do these data ?
- How can you do all this at low cost ?
This is what we have
been doing in …

Risk factors for SSI
Operation factors
• Surgical Wound Class
•Procedure
•Contamination
• Surgeon’s skill
• Length of operation
• Use of prophylaxis
• Use of drains/prostheses
• Number of people in room
Patient-related factors
• Age
• ASA score
• Diabetes
• HIV status
• Nutritional status
• Smoking
Microbiological factors
• Skin/GI/nasal carriage of micro-organisms
• Bacterial virulence factors + drug resistance
• Length of pre-operative admission
Institutional factors
• Operating theatre construction: airflow, bacterial contamination, cleaning
• Staffing – nurse:patient ratio
• Crowding of patients

1. How long to follow-up ? How to contact patient ?
2. Relevant PROCESS data
3. Risk stratification data SWC, ASA, op duration
4. OUTCOME data SSI outcomes
What data to collect + when ?
Eg. Surgeon handwashing,
pt skin prep, door openings,
antibiotic prophylaxis use
How many
contacts with
patient in
30 days ?

Why we need 30 day follow-up23
Day 0 Day 3 Day 7 Day 10 Day 14 Day 28
Dete
ctio
n o
f SSI
Operation ? Discharge ?
Inpatient periodOut-patient period

Telephone calls after discharge
Clinician review
= GOLD STANDARD
No SSI SSI
Pho
ne c
all
sta
tus No SSI 66 7
SSI 0 16
On this basis
Sensitivity of phone call = 69.6% (95%CI 47.1-86.8%)
Specificity of phone call = 100% (95%CI 95-100%)
When phone calls and clinical reviews were within 48 hours of each other
Ref: Aiken et al, Evaluation of surveillance for SSI at Thika Hospital, Kenya; JHI, 2011

Risk stratification – NNIS system 25
Surgical Wound Class
0 if Clean or Clean-Contaminated
1 if Contaminated or Dirty/Infected
ASA score
0 if ASA score = 1 or 2
1 if ASA score = 3, 4 or 5
Length of operation
0 if < procedure-specific duration
1 if ≥ procedure-specific duration
Total score of 0 – 3 for each operation
Compares “like with like” within operation-type

Risk stratification with limited $ 26
Is NNIS system suitable ?
Measurable ?
Minimal additional cost / effort to collect data
Each component possible to record reliably
Easy to use system
Predictive of SSI risk ?
Different results in different studies
Surgical Wound Class most consistently predictive

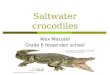
SSI risk in developing countries
according to wound classification
SSI pooled means:
11.5, 16.6, 21.3, 38.8
episodes per 100 SP
(from clean to dirty)
◊ NNIS reports
Adapted from Allegranzi B et al. Lancet 2011;377:228-41

A standard definition of an SSI ?
CDC/NHSN definition of SSI: “Infection occurring at the operation site within 30 days of the procedure.”
ref: Horan TC, Am J Inf Cont 2008

What not to include in SSI surveillance?29
Risk factors that are…
Extremely rare eg. morbid obesity ?
Hard to measure eg. S.aureus colonisation ?
Process data that are
Hard to alter eg. theatre air-flow data ?
Outcomes that are
Unrelated to SSI eg wound cosmesis ?

SUSP method for surveillance
Peri-operative form Post-operative form
Slide 30/20
Plus Epi-Info database, handbook, regular quality feedback, other training materials …

Page 31
Francis Mwangi Kirathi
Perforated appendix
123456789029yrs
Male Number comes from EpiInfo !
Appendisectomy ( APPY)
Appendisectomy + washout
20/12/2013
Jack Barasa
Consultant
5
20/12/2013
4 15
4
6
11
Use of the peri-operative form …

SUSP tools for SSI surveillance
Peri-operative form Post-operative form
Slide 32/20
Plus Epi-Info database, handbook, regular quality feedback, other training materials …

Page 33
Appendisectomy
Seen on ward round – some wound pain only
20/12/2013
AA
AA
24/12/2013
2/1/2014
Re-admitted with wound breakdown and pus +++
Use of the post operative form …
28/12/2013 discharged AA

Page 34
02/01/2014
02/01/2014 swab E. coli
Ampicllin R Gent R Cipro S
Ceftria x S Erythro R Clinda S
06/01/14Alex Aiken
Recording an SSI should look like this…

Quality Improvement measures
Process eg “correct” use of antibiotics,
appropriate pre-op skin preparation
Outcome eg. occurrence of SSI
Balancing effects eg. costs, staff time
Continuous v step-wise improvements ?
4. Uses of SSI surveillance data ?
Following slides courtesy of
Robert Mugrobe (Kisiizi Hospital)
from SUSP webinar October 2014

36
Kenya
AIC Kijabe Hospital, Nairobi
Jack Barasa, Carol Mwangi,
Peter N’thumba…
Uganda
1. Kisiizi Hospital, Kisiizi
Gabriel Okumu, Robert
Mugrobe, Agnes Katwsigye…
2. Mulago Hospital, Kampala
Peter Ongom, Alex Elobu,
Dorah Nakamwa…
Zimbabwe
Parirenyatwa Hospital, Harare
Sheba Chuma, Matthew Wazara,
Salome Biri…
Zambia
Ndola Central Hospital, Ndola
Joseph Musowoya, Margaret
Kasepa, Mayaba Maimbo…
Monthly webinars for
- Progress reports
- (Re-)training
- Sharing experiences …

- SSI surveillance since Jan - Feb 2014
- Developed local multi-modal SUSP
intervention plan
- Started intervention phase of SUSP
in July 2014
Rural area of SW Uganda
- Independent mission hospital
- Also participates in WHO African
Partnerships for Patient Safety (APPS)

INTERVENTION MEASURES
15
2123
26
44
30
47
59
52
8
16
26
29
23
18
15
21
8
0
10
20
30
40
50
60
70
1 2 3 4 5 6 7 8 9
Num
ber
of
op
era
tions
Month of 2014
Pre op patient bath
yes
no
Start of intervention

0
20
40
60
80
100
120
1 2 3 4 5 6 7 8 9
% p
art
icip
ants
Hair removal
clipper
not done
razor
1 2 3 4 5 6 7 8 9
Yes 13 41 8.2 0 4.5 47.9 100 94.9 100
No 87 59 91.8 100 95.5 52.1 0 5.1 0
0
20
40
60
80
100
120
% a
llow
ed to
dry
Patient skin prep allowed to dry

0
10
20
30
40
50
60
70
80
1 2 3 4 5 6 7 8 9
Num
ber
of
opera
tion
s
Pre-operative antibiotic prophylaxis administration
yes
no

5. Challenges of SSI surveillance?
our SUSP experience41
Data quality
Missing or inconsistent data ?
Incomplete follow-up ?
Data management
Epi-Info analysis issues …
Data sharing + back-up via
Staff issues
$ for extra staff = 1 new nurse / site
Intensive+repetitive work
Limiting to approx 50 surveillance ops / month
Hasn’t been a problem in
SUSP – but had intensive
training + support

42
Kenya
AIC Kijabe Hospital, Nairobi
Jack Barasa, Carol Mwangi,
Peter N’thumba…
Uganda
1. Kisiizi Hospital, Kisiizi
Gabriel Okumu, Robert
Mugrobe, Agnes Katwsigye…
2. Mulago Hospital, Kampala
Peter Ongom, Alex Elobu,
Dorah Nakamwa…
Zimbabwe
Parirenyatwa Hospital, Harare
Sheba Chuma, Matthew Wazara,
Salome Biri…
Zambia
Ndola Central Hospital, Ndola
Joseph Musowoya, Margaret
Kasepa, Mayaba Maimbo…
Benedetta Allegranzi
Zeynep Kubilay
Joyce Hightower
Sean Berenholtz
Kathryn Taylor
And many, many others
Many thanks to all my colleagues in SUSP
Questions?