Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Use of pegfilgrastim primary prophylaxis and risk of infection,by chemotherapy cycle and regimen, among patients with breastcancer or non-Hodgkin’s lymphoma
Wendy J. Langeberg & Conchitina C. Siozon &
John H. Page & P. K. Morrow & Victoria M. Chia
Received: 24 December 2013 /Accepted: 2 March 2014# Springer-Verlag Berlin Heidelberg 2014
AbstractPurpose This study aims to examine granulocyte colony-stimulating factor (G-CSF) prophylaxis by cancer type, che-motherapy regimen, and cycle in a real-world setting to assessif practice conforms to clinical guidelines, which recommendG-CSF prophylaxis every cycle when a patient’s risk of febrileneutropenia (FN) is 20 % or greater, and to describe theincidence of FN among patients who discontinue pegfilgrastim(peg) prophylaxis.Methods The cohort was selected from administrative claimsdata and includes adults diagnosed with non-Hodgkin’s lym-phoma (NHL) or breast cancer (BC) who began chemothera-py 2005–2010.Results About 83.2 % of the 4,470 patients with BC treatedwith dose-dense doxorubicin, cyclophosphamide (ddAC),83.6 % of 2,197 patients with BC treated with docetaxel,doxorubicin, cyclophosphamide (TAC), and about 55.6 % ofthe 2,722 patients with NHL treated with cyclophosphamide,doxorubicin, vincristine, with or without prednisone for 3-week cycles (CHOP-R Q3W) received peg prophylaxis incycle 1. Among patients on these regimens who receivedpeg prophylaxis in cycle 1 and were still on the regimen incycle 4, about 90 % received peg prophylaxis in that cycle.Among patients with BC or NHL who discontinued G-CSF,the incidence proportion of infection or FN varied by regimenand cycle, with a range from 0 to 14 %.Conclusions Despite clinical guidelines recommending G-CSF prophylaxis with chemotherapy regimens with a highrisk of FN, many NHL and BC patients do not receive FNprophylaxis in cycle 1. However, among patients who receive
G-CSF in cycle 1 and remain on the regimen, the majorityappear to continue prophylaxis as indicated.
Keywords Granulocyte colony-stimulating factor .
Neutropenia . Myelosuppressive . Chemotherapy cycle .
Breast cancer . Non-Hodgkin’s lymphoma
Introduction
Myelosuppressive chemotherapy can induce febrile neutrope-nia (FN), which can lead to life-threatening infections,resulting in dose reductions, treatment delays, lengthy hospi-talizations, early morbidity, and early mortality [1–4]. Clinicaltrials have shown that prophylactic use of granulocyte colony-stimulating factors (G-CSFs) can reduce rates of FN, infec-tions, use of intravenous antibiotics, hospitalizations, and dosereductions and delays in patients with non-Hodgkin’s lym-phoma (NHL), breast cancer (BC), and other cancer types[5–10]. Clinical guidelines recommend the prophylactic useof G-CSF every chemotherapy cycle where a patient’s risk ofFN is 20 % or greater, a risk determined from the chemother-apy regimen, patient risk factors, and therapeutic intent (cura-tive vs. palliative) [1, 11–13].
Several studies have found that the risk for FN is highestduring the first two cycles of chemotherapy [6, 7, 14, 15].Based on this evidence, Aarts and colleagues performed anopen-label, randomized, phase III study in patients with BCtreated with myelosuppressive chemotherapy, comparing theincidence of FN among patients who received pegfilgrastim(peg) prophylaxis during the first two chemotherapy cyclesonly with those who received pegprophylaxis during all che-motherapy cycles [16]. They found more than a threefoldhigher incidence of FN among patients who received pegprophylaxis during the first two cycles only compared to those
W. J. Langeberg (*) :C. C. Siozon : J. H. Page : P. K. Morrow :V. M. ChiaAmgen, Inc., Thousand Oaks, CA, USAe-mail: [email protected]
Support Care CancerDOI 10.1007/s00520-014-2184-5

who continued peg prophylaxis through all six cycles and thusrecommend primary G-CSF prophylaxis throughout all che-motherapy cycles in patients with breast cancer at risk for FN.To our knowledge, there are no other studies of FN ratesamong patients who discontinue the use of pegfilgrastimprophylaxis in later chemotherapy cycles.
The aims of this descriptive study are to examine in a real-world setting the use of prophylactic G-CSF by chemotherapyregimen and cycle among patients with breast cancer or NHLand to describe the incidence of infection and FN amongpatients who discontinue G-CSF prophylaxis but stay on theregimen.
Methods
The study cohort was selected from the MarketScan ResearchDatabases maintained by Truven Health Analytics. TheMarketScan Commercial Claims and Encounters and Medi-care Supplemental and Coordination of Benefits databasesconsist of medical claims, outpatient pharmacy claims, andpatient enrollment data from employer-sponsored health in-surance plans in the USA, including fee-for-service, fully/partially capacitated systems, health maintenance organiza-tions, preferred provider organizations, point of service, andindemnity plans. The databases cover over 15 million personsannually, including employees and their spouses and depen-dents. All patient-identifying information are either encryptedor removed from the databases; therefore, they are fully com-pliant with the Health Insurance Portability and Accountabil-ity Act of 1996 [17] and the federal guidance on PublicWelfare and the Protection of Human Subjects [18]. Accord-ing to the Code of Federal Regulations, institutional reviewboard approval was not required for a study of this nature.
Study population
The cohort included women diagnosed with breast cancer andmen or women diagnosed with NHL who had at least onechemotherapy claim in the database. The first date of chemo-therapy (the index date) had to occur between January 1, 2005and December 31, 2010, and the diagnosis for cancer had tooccur within the 180 days before the index date. A diagnosiswas defined as one or more inpatient or two or more outpatientclaims at least 30 days apart with International Classificationof Diseases, Clinical Modification (ICD-9-CM) codes 174.0–174.9 for breast cancer or 200.0–200.8, 202.0–202.2, or202.7–202.9 for NHL. The earliest of these dates was consid-ered as the date of diagnosis. In addition, patients had to meetthe following inclusion criteria: (1) 18 years or older at diag-nosis, (2) continuously enrolled in their insurance plan for atleast 12 months prior to the index date, (3) had at least12 months without a claim for any chemotherapy prior to
the index date, and (4) had at least one claim for pegfilgrastimon or before day 5 of the first chemotherapy cycle. Patientswere excluded if they had more than one cancer diagnosisduring the 180 days before or after the index date. A secondcancer diagnosis was defined as one or more inpatient or twoor more outpatient claims 30–365 days apart with the ICD-9-CM codes 140.x–195.x or 200.x–209.x, excluding the breastor NHL ICD-9-CM codes. Patients were also excluded if theyhad medical claims for a bone marrow or stem cell transplantfrom 1 year before the index date to the last day of thechemotherapy course or if they had medical claims for radio-therapy from the index date to 30 days after the last chemo-therapy date. Patients were considered to have metastaticdisease if they had ICD-9-CM codes for secondary malignantneoplasms (ICD-9-CM 196.x–198.x) within 180 days beforeor after the diagnosis date.
Chemotherapy course and cycles
A chemotherapy course started with the first claim for che-motherapy and ended after a 60-day gap in chemotherapy orafter the sixth cycle, whichever came first. Chemotherapycycles were defined from the first service date of a chemo-therapy claim through the first service date for chemotherapy14 or more days later. Thus, all cycle lengths were at least14 days in length. Exceptions were made for certain regimens,such as those that administer drugs weekly. Chemotherapyclaims were identified via ICD-9-CM, National Drug Codes(NDC), Healthcare Common Procedure Coding System(HCPCS), and Current Procedural Terminology (CPT) codes.
Chemotherapy regimens
Chemotherapy regimens were defined by the combinations ofdrug claims and dates of service observed in each cycle, asdefined by clinical practice guidelines [19–22] and informa-tion from clinical trials. Myelosuppressive regimens (regi-mens that have a high or intermediate risk of FN) and regi-mens with at least 100 patients who received peg prophylaxisin cycle 1 are presented. Because oral medications such asprednisone are not well-captured in administrative claim data,these agents were not required to define the regimens. Forbreast cancer, the regimens shown are: doxorubicin (A), doxo-rubicin, cyclophosphamide (AC), docetaxel, carboplatin, withor without trastuzumab (TCH), dose-dense doxorubicin, cy-clophosphamide (ddAC), epirubicin, cyclophosphamide(EC), fluorouracil, epirubicin, cyclophosphamide (FEC), do-cetaxel, doxorubicin, cyclophosphamide (TAC), and docetax-el, cyclophosphamide (TC). For NHL, the regimens shownare: CHOP-R (cyclophosphamide, doxorubicin, vincristine,with or without prednisone or rituxumab) for 2-week (Q2W)or 3-week (Q3W) cycles, and COP (cyclophosphamide, vin-cristine with or without prednisone or rituxumab). Because we
Support Care Cancer

are evaluating the first four or six cycles, we did not distin-guish regimens by the follow-on drugs; for example, patientswould be categorized into the AC regimen if they receivedcyclophosphomide and doxorubicin, whether or not they re-ceived docetaxel, paclitaxel, or trastuzumab after the cycles ofAC.
G-CSF use
Administration of G-CSF was identified using HCPCS andNDC codes for filgrastim (NEUPOGEN®) and pegfilgrastim(Neulasta®). Pegfilgrastim prophylaxis was defined as havinga claim for pegfilgratim on days 1 to 5 of the cycle. Filgrastimuse was defined as having a claim for filgrastimwithin the firstfive days of the cycle start date.
Infection or febrile neutropenia
The definition of infection or FNwas defined as any diagnosisof infection including sepsis, identified using any diagnosis ofneutropenia (ICD-9-CM 288.0x) within 7 days of a diagnosisof fever (ICD-9-CM 780.6x), use of IV antibiotics (identifiedthrough HCPCS codes), or an ICD-9-CM code for infection:001–139, 254.1, 320–326, 360.0, 372–372.39, 373.0–373.2,376.0, 380.14, 382–382.4, 383, 386.33, 386.35, 388.60, 390,391, 392.0, 392.9, 393, 415.12, 420.99, 421.0, 421.1, 422.0,422.91–422.93, 449, 457.2, 460–466, 472.0–474.02, 475–476.1, 478.21–478.24, 478.29, 480–490, 491.1, 491.21,494, 510–511.1, 513, 518.6, 519.01, 522.5, 522.7, 526.4,527.3, 528.3, 540–542, 562.01, 562.03, 562.11, 562.13,566–567.9, 569.5, 569.61, 572–572.1, 573.1–573.3, 575–575.12, 590–590.9, 595–595.4, 597.0–597.89, 598, 599.0,601, 604, 607.1–607.2, 608.0, 608.4, 611.0, 614–616.1,616.3–616.4, 616.8, 670, 675.1, 680–686.9, 706.0, 711–711.9, 728.86, 730.0–730.2, 730.3, 730.8–730.9, 785.52,790.7, 790.8, 958.3, 995.91, 995.92, 996.60–996.61,996.63–996.69, 997.62, 998.5, 999.3, or 996.62 (with ICD-9procedure codes 38.7 or 39 (except 39.27) within 6 months).
Statistical analysis
The percent of patients who received pegfilgrastim prophy-laxis, at least one claim for filgrastim, or no G-CSF wascalculated respectively among patients who remained on theregimen each cycle. Patients were assessed as having pegprophylaxis during each cycle and all previous cycles, as wellas during each cycle regardless of use in previous cycles. Thepercent of patients diagnosed with infection or FN was calcu-lated in each cycle among patients who did not receive G-CSFprophylaxis but remained on the regimen that cycle. In orderto capture incident infection or FN, patients diagnosed withinfection or FN in a previous cycle were removed in subse-quent cycles. We used SAS v 9.2 (SAS Institute Inc., Cary,
NC, USA) for programming and analysis and STATA/SEv.9.2 (College Station, TX, USA) for graphs.
Results
The study cohort included 14,385 patients with breast cancerand 2,195 with NHL (Table 1). Of the patients with breastcancer, 47.1 % were 55 years of age or older and 20.6 % had adiagnosis code for metastatic disease. Of the patients withNHL, 77.2 % were 55 years of age or older.
Table 2 and Fig. 1 show G-CSF use among patients withbreast cancer by cycle and chemotherapy regimen. Over 80 %of the 6,357 patients treated with ddAC and the 2,197 patientstreated with TAC received peg prophylaxis in cycle 1. Over60% of the 565 patients treated with FEC and 246 treated withEC received peg prophylaxis in cycle 1. About half of the5,088 patients treated with TC, 1,930 patients treated withTCH, and 234 patients treated with A received peg prophy-laxis in cycle 1. Finally, about 41 % of the 5,088 patientstreated with AC received peg prophylaxis in cycle 1.Filgrastim was used in cycle 1 for less than 3 % of thesepatients, with one exception: 6 % of patients treated with ECreceived filgrastim in cycle 1.
Among patients with breast cancer who received peg pro-phylaxis in cycle 1 and were still on the same regimen in cycle4, most received peg prophylaxis in that cycle: 89 % for AC,
Table 1 Patient characteristics
Breast, n (%) NHL, n (%)
Total 14,385 2,195
Female 14,385 (100.0) 1,007 (45.9)
Age group
18–34 367 (2.6) 54 (2.5)
35–44 2,260 (15.7) 125 (5.7)
45–54 4,980 (34.6) 322 (14.7)
55–64 5,223 (36.3) 680 (31.0)
≥65 1,555 (10.8) 1,014 (46.2)
Region
Northeast 1,300 (9.0) 203 (9.3)
Midwest 3,846 (26.7) 779 (35.5)
South 6,932 (48.2) 887 (40.4)
West 2,257 (15.7) 320 (14.6)
Insurance type
HMO 1,672 (11.6) 226 (10.3)
PPO 9,715 (67.6) 1,184 (53.9)
POS 1,393 (9.7) 150 (6.8)
Indemnity 1,300 (9.0) 566 (25.8)
Diagnosis code for metastatic disease 2,956 (20.6) 204 (9.3)
HMO health maintenance organization, PPO preferred provider organi-zation, POS point of service
Support Care Cancer

Table 2 G-CSF use among patients with breast cancer, by regimen and cycle
Regimencycle
Patients nolonger on thisregimen, n
Denominator: patientsremaining on theregimena, n
Pegfilgrastim prophylaxis incurrent cycle and all previouscycles, n (%)
Pegfilgrastimprophylaxis incurrent cycle, n (%)
Filgrastimprophylaxis use incurrent cycleb, n (%)
No G-CSFProphylaxis incurrent cycle, n (%)
AC
1 – 5,088 2,066 (40.6 %) 2,066 (40.6 %) 81 (1.6 %) –
2 287 1,779 1,617 (90.9 %) 1,617 (90.9 %) 60 (3.4 %) 152 (8.5 %)
3 274 1,505 1,311 (87.1 %) 1,362 (90.5 %) 54 (3.6 %) 130 (8.6 %)
4 286 1,219 1,030 (84.5 %) 1,090 (89.4 %) 37 (3.0 %) 119 (9.8 %)
ddACc
1 – 6,357 5,252 (82.6 %) 5,252 (82.6 %) 143 (2.2 %) –
2 70 5,182 4,836 (93.3 %) 4,836 (93.3 %) 99 (1.9 %) 331 (6.4 %)
3 233 4,949 4,464 (90.2 %) 4,577 (92.5 %) 97 (2.0 %) 349 (7.1 %)
4 1,100 3,849 3,341 (86.8 %) 3,476 (90.3 %) 86 (2.2 %) 342 (8.9 %)
TC
1 – 5,088 2,613 (51.4 %) 2,613 (51.4 %) 72 (1.4 %) –
2 218 2,395 2,108 (88.0 %) 2,108 (88.0 %) 73 (3.0 %) 259 (10.8 %)
3 201 2,194 1,869 (85.2 %) 1,934 (88.1 %) 65 (3.0 %) 232 (10.6 %)
4 235 1,959 1,590 (81.2 %) 1,683 (85.9 %) 67 (3.4 %) 242 (12.4 %)
5 1,504 455 374 (82.2 %) 402 (88.4 %) 15 (3.3 %) 43 (9.5 %)
6 66 389 310 (79.7 %) 341 (87.7 %) 6 (1.5 %) 44 (11.3 %)
TACc
1 – 2,197 1,837 (83.6 %) 1,837 (83.6 %) 45 (2.0 %) –
2 170 1,667 1,558 (93.5 %) 1,558 (93.5 %) 46 (2.8 %) 95 (5.7 %)
3 102 1,565 1,428 (91.2 %) 1,467 (93.7 %) 37 (2.4 %) 88 (5.6 %)
4 127 1,438 1,284 (89.3 %) 1,341 (93.3 %) 29 (2.0 %) 89 (6.2 %)
5 140 1,298 1,143 (88.1 %) 1,219 (93.9 %) 23 (1.8 %) 72 (5.5 %)
6 135 1,163 1,005 (86.4 %) 1,081 (92.9 %) 16 (1.4 %) 76 (6.5 %)
TCH
1 – 1,930 1,026 (53.2 %) 1,026 (53.2 %) 23 (1.2 %) –
2 84 942 564 (59.9 %) 564 (59.9 %) 12 (1.3 %) 375 (39.8 %)
3 319 623 468 (75.1 %) 485 (77.8 %) 12 (1.9 %) 132 (21.2 %)
4 107 516 416 (80.6 %) 444 (86.0 %) 7 (1.4 %) 70 (13.6 %)
5 96 420 342 (81.4 %) 367 (87.4 %) 7 (1.7 %) 49 (11.7 %)
6 55 365 287 (78.6 %) 315 (86.3 %) 7 (1.9 %) 47 (12.9 %)
FEC
1 – 565 357 (63.2 %) 357 (63.2 %) 10 (1.8 %) –
2 40 317 296 (93.4 %) 296 (93.4 %) 15 (4.7 %) 12 (3.8 %)
3 40 277 252 (91.0 %) 261 (94.2 %) 11 (4.0 %) 10 (3.6 %)
4 169 108 99 (91.7 %) 104 (96.3 %) 3 (2.8 %) 2 (1.9 %)
5 79 29 26 (89.7 %) 26 (89.7 %) 3 (10.3 %) 2 (6.9 %)
6 26 3 3 (100.0 %) 3 (100.0 %) 0 (0.0 %) 0 (0.0 %)
EC
1 – 246 148 (60.2 %) 148 (60.2 %) 15 (6.1 %) –
2 23 125 119 (95.2 %) 119 (95.2 %) 10 (8.0 %) 6 (4.8 %)
3 22 103 93 (90.3 %) 95 (92.2 %) 8 (7.8 %) 7 (6.8 %)
4 18 85 73 (85.9 %) 77 (90.6 %) 10 (11.8 %) 6 (7.1 %)
A
1 – 234 124 (53.0 %) 124 (53.0 %) 6 (2.6 %) –
2 39 85 76 (89.4 %) 76 (89.4 %) 4 (4.7 %) 8 (9.4 %)
3 7 78 66 (84.6 %) 70 (89.7 %) 2 (2.6 %) 7 (9.0 %)
Support Care Cancer

91 % for ddAC, 86 % for TC, 93 % for TAC, 86 % for TCH,96 % for FEC, 91 % for EC, and 92 % for A. A slightly lowerpercentage received peg prophylaxis in cycle 4 and all previ-ous cycles: 85 % for AC, 87 % for ddAC, 81 % for TC, 89 %for TAC, 81 % for TCH, 92 % for FEC, 86 % for EC, and83 % for A.
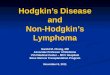
Table 3 and Fig. 2 show G-CSF use among patients withNHL by cycle and regimen. About 56 % of the 2,621 patientstreated with CHOP-R Q3W, 72 % of the 195 patients treatedwith CHOP-RQ2W, and 23% of the 847 patients treated withCOP received peg prophylaxis in cycle 1. Filgrastim was usedin cycle 1 for less than 3 % of these patients.
Among patients with NHL who received peg prophylaxisin cycle 1 who were still on the regimen in cycle 4, about 93%
of patients treated with CHOP-R Q3W, 95 % of patientstreated with CHOP-R Q2W, and 87 % of patients treated withCOP received peg prophylaxis in cycle 4. A slightly lowerpercentage received peg prophylaxis in cycle 4 and all previ-ous cycles: 86% for CHOP-RQ3W, 92% for CHOP-RQ2W,and 78 % for COP.
Table 4 shows the percent of patients who developedinfection or FN in each cycle among patients who remainedon the regimen but discontinued G-CSF use in that cycle. Forregimens with more than 25 such patients with breast cancer,the percent of patients who developed infection or FN rangedfrom about 5–12 % in cycle 2, 4–7 % in cycle 3, 3–9 % incycle 4, 6–14 % in cycle 5, and 0–3 % in cycle 6. For patientswith NHL treated with the CHOP-R Q3W regimen, the
Table 2 (continued)
Regimencycle
Patients nolonger on thisregimen, n
Denominator: patientsremaining on theregimena, n
Pegfilgrastim prophylaxis incurrent cycle and all previouscycles, n (%)
Pegfilgrastimprophylaxis incurrent cycle, n (%)
Filgrastimprophylaxis use incurrent cycleb, n (%)
No G-CSFProphylaxis incurrent cycle, n (%)
4 19 59 49 (83.1 %) 54 (91.5 %) 3 (5.1 %) 4 (6.8 %)
A doxorubicin, AC doxorubicin, cyclophosphamide, TCH docetaxel, carboplatin, with or without trastuzumab, ddAC dose-dense doxorubicin,cyclophosphamide, EC epirubicin, cyclophosphamide, FEC fluorouracil, epirubicin, cyclosphosphamide, TAC docetaxel, doxorubicin, cyclophospha-mide, TC docetaxel, cyclophosphamidea The denominator for cycle 1 includes all patients who received that regimen, whether or not they received G-CSF prophylaxis in cycle 1b Filgrastim users are not mutually exclusive from pegfilgrastim usersc Regimens with a high risk for FN (NCCN 2013)
020
4060
8010
0
AC ddAC TC TAC TCH FEC EC A
2 3 4 2 3 4 2 3 4 5 6 2 3 4 5 6 2 3 4 5 6 2 3 4 5 6 2 3 4 2 3 4
Pegfilgrastim prophylaxis in current cycle
Pegfilgrastim prophylaxis in current cycle and all previous cycles
Fig. 1 Pegfilgrastim prophylaxisamong patients with breast cancerwho received pegfilgrastimprophylaxis in cycle 1 andremained on the regimen, byregimen and cycle. Adoxorubicin, AC doxorubicin,cyclophosphamide, TCHdocetaxel, carboplatin, with orwithout trastuzumab, ddACdose-dense doxorubicin,cyclophosphamide, ECepirubicin, cyclophosphamide,FEC fluorouracil, epirubicin,cyclosphosphamide, TACdocetaxel, doxorubicin,cyclophosphamide, TC docetaxel,cyclophosphamide
Support Care Cancer

Table 3 G-CSF use among patients with NHL, by regimen and cycle
Regimencycle
Patients nolonger on thisregimen, n
Denominator: patientsremaining on theregimena, n
Pegfilgrastim prophylaxis incurrent cycle and all previouscycles, n (%)
Pegfilgrastimprophylaxis incurrent cycle, n (%)
Filgrastimprophylaxis use incurrent cycleb, n (%)
No G-CSFprophylaxis incurrent cycle, n (%)
CHOP-R Q3W
1 – 2,621 1,464 (55.9 %) 1,464 (55.9 %) 57 (2.2 %) –
2 197 1,267 1,177 (92.9 %) 1,177 (92.9 %) 39 (3.1 %) 82 (6.5 %)
3 152 1,115 984 (88.3 %) 1,021 (91.6 %) 30 (2.7 %) 89 (8.0 %)
4 191 924 793 (85.8 %) 855 (92.5 %) 23 (2.5 %) 63 (6.8 %)
5 179 745 622 (83.5 %) 685 (91.9 %) 25 (3.4 %) 52 (7.0 %)
6 187 558 459 (82.3 %) 509 (91.2 %) 19 (3.4 %) 41 (7.3 %)
CHOP-R Q2W
1 – 195 141 (72.3 %) 141 (72.3 %) 5 (2.6 %) –
2 56 85 77 (90.6 %) 77 (90.6 %) 1 (1.2 %) 7 (8.2 %)
3 21 64 60 (93.8 %) 62 (96.9 %) 0 (0.0 %) 2 (3.1 %)
4 26 38 35 (92.1 %) 36 (94.7 %) 0 (0.0 %) 2 (5.3 %)
5 16 22 19 (86.4 %) 20 (90.9 %) 0 (0.0 %) 2 (9.1 %)
6 17 5 5 (100.0 %) 5 (100.0 %) 0 (0.0 %) 0 (0.0 %)
COP
1 – 847 196 (23.1 %) 196 (23.1 %) 11 (1.3 %) –
2 30 166 138 (83.1 %) 138 (83.1 %) 8 (4.8 %) 27 (16.3 %)
3 23 143 112 (78.3 %) 123 (86.0 %) 6 (4.2 %) 19 (13.3 %)
4 16 127 99 (78.0 %) 110 (86.6 %) 7 (5.5 %) 15 (11.8 %)
5 21 106 81 (76.4 %) 90 (84.9 %) 4 (3.8 %) 16 (15.1 %)
6 25 81 60 (74.1 %) 68 (84.0 %) 1 (1.2 %) 13 (16.0 %)
CHOP-R cyclophosphamide, doxorubicin, vincristine, with or without prednisone, rituxumab, COP cyclophosphamide, vincristine with orwithoutprednisone, rituxumab, Q2W 2 weeks, Q3W 3 weeksa The denominator for cycle 1 includes all patients who received that regimen whether or not they received G-CSF prophylaxis in cycle 1b Filgrastim users are not mutually exclusive from pegfilgrastim users
020
4060
8010
0
CHOPR Q3W CHOPR Q2W COP
2 3 4 5 6 2 3 4 5 6 2 3 4 5 6
Pegfilgrastim prophylaxis in current cycle
Pegfilgrastim prophylaxis in current cycle and all previous cycles
Fig. 2 Pegfilgrastim prophylaxisamong patients with NHL whoreceived pegfilgrastimprophylaxis in cycle 1 andremained on the regimen, byregimen and cycle. CHOP-Rcyclophosphamide, doxorubicin,vincristine, with orwithoutprednisone, rituxumab,COP cyclophosphamide,vincristine with or withoutprednisone, rituxumab, Q2W2 weeks, Q3W 3 weeks
Support Care Cancer

percent of patients who developed infection or FN rangedfrom about 4 % in cycles 3 and 6 to about 7 % in cycle 2.
Discussion
Despite clinical guidelines recommending G-CSF prophylax-is with chemotherapy regimens with a high (>20 %) risk ofFN, we found only about 83 % of patients with BC whoreceived ddAC or TAC, and about 72 % of patients withNHL who received CHOP-R Q2W received peg prophylaxisin cycle 1. However, among patients with BC or NHL whoreceived peg prophylaxis in cycle 1 and remained on the samechemotherapy regimen through four cycles, 80–96 % contin-ued to receive FN prophylaxis in subsequent cycles. Theincidence proportion of infection or FN in patients whoremained on the regimen but discontinued G-CSF use variedby regimen and cycle, with a range from 4 to 7 % amongpatients with NHL and a range from 0 to 14 % among patientswith breast cancer.
Several studies have evaluated the patterns of G-CSF use inreal-world populations of patients with breast cancer or NHL[23–25]; however, we are not aware of any observationalstudies that have described G-CSF use by cycle, through latercycles and within well-defined chemotherapy regimens (as
Table 4 Infection or FN among patients who received pegfilgrastimcycle 1 and discontinued G-CSF use in subsequent cycles but remainedon the chemotherapy regimen, by cancer type, regimen, and cycle
Cycle No G-CSF incurrent cycle, n
Developed infectionor FN, n (%)
Breast cancer
AC
2 136 13 (9.6 %)
3 101 7 (6.9 %)
4 99 3 (3.0 %)
ddAC
2 314 18 (5.7 %)
3 311 22 (7.1 %)
4 294 18 (6.1 %)
TC
2 230 13 (5.7 %)
3 199 10 (5.0 %)
4 193 5 (2.6 %)
5 30 4 (13.3 %)
6 34 1 (2.9 %)
TAC
2 85 10 (11.8 %)
3 74 3 (4.1 %)
4 69 6 (8.7 %)
5 51 7 (13.7 %)
6 49 0 (0 %)
TCH
2 354 18 (5.1 %)
3 118 7 (5.9 %)
4 56 3 (5.4 %)
5 33 2 (6.1 %)
6 31 0 (0 %)
FEC
2 11 0 (0 %)
3 9 0 (0 %)
4 1 0 (0 %)
5 2 0 (0 %)
6 0 0 (0 %)
EC
2 6 0 (0 %)
3 6 0 (0 %)
4 4 0 (0 %)
A
2 8 0 (0 %)
3 6 0 (0 %)
4 4 0 (0 %)
NHL
CHOP-R Q3W
2 69 5 (7.2 %)
3 70 3 (4.3 %)
4 53 3 (5.7 %)
Table 4 (continued)
Cycle No G-CSF incurrent cycle, n
Developed infectionor FN, n (%)
5 33 2 (6.1 %)
6 23 1 (4.3 %)
CHOP-R Q2W
2 6 0 (0 %)
3 2 0 (0 %)
4 2 0 (0 %)
5 2 0 (0 %)
6 0 0 (0 %)
COP
2 24 2 (8.3 %)
3 16 1 (6.3 %)
4 12 0 (0 %)
5 13 1 (7.7 %)
6 12 0 (0 %)
A doxorubicin, AC doxorubicin, cyclophosphamide, TCH docetaxel,carboplatin, with or without trastuzumab, ddAC dose-dense doxorubicin,cyclophosphamide, EC epirubicin, cyclophosphamide, FEC luorouracil,epirubicin, cyclosphosphamide, TAC docetaxel, doxorubicin, cyclophos-phamide, TC docetaxel, cyclophosphamide, CHOP-R cyclophospha-mide, doxorubicin, vincristine, with or without prednisone, rituxumab,COP cyclophosphamide, vincristine with or without prednisone,rituxumab
Support Care Cancer

opposed to individual myelosuppressive agents). Likewise,several observational studies have examined the risk of FNamong patients with breast cancer or NHL who received G-CSF prophylaxis [4, 5, 26–33]; however, we are not aware ofobservational studies that describe the risk of FN or infectionby cycle among patients who discontinue G-CSF prophylaxis.
The dataset we used for this analysis has limitations andstrengths when used for research purposes. Administrativeclaims do not include patient and clinical characteristics suchas tumor stage or grade, performance status, body tempera-ture, and absolute neutrophil count. This meant we could notprecisely measure FN [34], so we instead used a diagnosis ofinfection, use of antibiotics, or diagnosis codes for fever andneutropenia as the outcome of interest. The lack of clinicalinformation also meant we could not determine several factorsthat predict FN risk, such as therapeutic intent, and thus couldnot examine reasons why a patient did not receive ordiscontinued use of G-CSF nor factors that would influencerisk of infection or FN. The lack of sufficient information onmany covariates also prevented making causal inferences onthe difference in infection incidence for patients who discon-tinue peg versus those who continued until the chemotherapyregimen was complete. In addition, dose is not well-describedin claims data and the service date recorded may or may notrepresent the actual date on which the therapeutic agent isadministered. Finally, the Medicare population is largely un-represented in this database, so the results may not be gener-alizable to an older cancer population nor to cancer popula-tions outside the USA or the uninsured cancer populationwithin the USA. The strengths of administrative claims arethe large size of the database, which allowed us to identify asubstantial number of patients. In addition, the database iswell distributed across the USA so that we can reasonablyassume that the study population represents real-world oncol-ogy practice in the USA for patients aged <65.
In summary, we found that most patients who start takingpegfilgrastim for primary prophylaxis of febrile neutropeniausually continue for as long as the chemotherapy regimenremains the same.
Given the results of the randomized trial of Aarts andcolleagues, this is reassuring. Future studies should examinepatterns of G-CSF prophylaxis continuation in Medicare pa-tients and in children.
Acknowledgments We thank Dr. Xiaoyan Li and Dr. Hairong Xu(Amgen Inc., Thousand Oaks, CA, USA) and Dr. Derek Weycker andDr. Alex Kartashov (Policy Analysis Inc., Brookline, MA, USA), whoassisted with diagnosis and drug codes and other aspects of data pro-gramming, and Jan Lethen, Lori Cyprien, Vincent Jones, and Jason Yuan(Amgen Inc., Thousand Oaks, CA, USA) who provided independentreview of the computer programming.
Conflict of interest All authors are employed by Amgen Inc., Thou-sandOaks, CA, USA, which sponsored this research. The authors had fullcontrol of the dataset.
References
1. National Comprehensive Cancer Network (2013) NCCN clinicalpractice guidelines in oncology. Myeloid growth factors. V.2.2013(www.nccn.org/professionals/physician_gls/PDF/myeloid_growth.pdf)
2. LymanGH,Michels SL, ReynoldsMWet al (2010) Risk of mortalityin patients with cancer who experience febrile neutropenia. Cancer116:5555–5563
3. Crawford J, Dale DC, Kuderer NM et al (2008) Risk and timing ofneutropenia events in adult cancer patients receiving chemotherapy:the results of a prospective nationwide study of oncology practice. JNatl Compr Cancer Netw 6:109–118
4. Kuderer NM, Dale DC, Crawford J et al (2006) Mortality, morbidity,and cost associated with febrile neutropenia in adult cancer patients.Cancer 106:2258–2266
5. Kuderer NM, Dale DC, Crawford J, Lyman GH (2007) Impact ofprimary prophylaxis with granulocyte colony-stimulating factor onfebrile neutropenia and mortality in adult cancer patients receivingchemotherapy: a systematic review. J Clin Oncol 25:3158
6. Timmer-Bonte JN, deBoo TM, Smit HJ et al (2005) Prevention ofchemotherapy-induced febrile neutropenia by prophylactic antibi-otics plus or minus granulocyte colony-stimulating factor in small-cell lung cancer: a Dutch randomized phase III study. J Clin Oncol23:7974
7. Vogel CL, Wojtukiewicz MZ, Carroll RR et al (2005) First andsubsequent cycle use of pegfilgrastim prevents febrile neutropeniain patients with breast cancer: a multicenter, double-blind, placebo-controlled phase III study. J Clin Oncol 23:1178–1184
8. Holmes FA, O’Shaughnessy JA, Vukelja S et al (2002) Blinded,randomized, multicenter study to evaluate single administrationpegfilgrastim once per cycle versus daily filgrastim as an adjunct tochemotherapy in patients with high-risk stage II or stage III/IV breastcancer. J Clin Oncol 20:727–731
9. Gerhartz HH, Engelhard M, Meusers P et al (1993) Randomized,double-blind, placebo-controlled, phase III study of recombinanthuman granulocyte-macrophage colony-stimulating factor as adjunctto induction treatment of high-grade malignant non-Hodgkin’s lym-phomas. Blood 82:2329
10. Crawford J, Ozer H, Stoller R et al (1991) Reduction by granulocytecolony-stimulating factor of fever and neutropenia induced by che-motherapy in patients with small-cell lung cancer. N Engl J Med 325:164–170
11. Crawford J, Caserta C, Roila F, ESMO Guidelines Working Group(2010) Hematopoietic growth factors: ESMO clinical practice guide-lines for the applications. Ann Oncol Suppl 5:v248–v251
12. Aapro MS, Bohlius J, Cameron DA, European Organisation forResearch and Treatment of Cancer et al (2011) 2010 update ofEORTC guidelines for the use of granulocyte-colony stimulatingfactor to reduce the incidence of chemotherapy-induced febrile neu-tropenia in adult patients with lymphoproliferative disorders andsolid tumours. Eur J Cancer 47:8–32
13. Smith TJ, Khatcheressian J, Lyman GH et al (2006) 2006 update ofrecommendations for the use of white blood cell growth factors: anevidence-based clinical practice guideline. J Clin Oncol 24:3187–3205
14. von Minckwitz G, Kümmel S, du Bois A, German Breast Group et al(2008) Pegfilgrastim +/− ciprofloxacin for primary prophylaxis withTAC (docetaxel/doxorubicin/cyclophosphamide) chemotherapy forbreast cancer. Results from the GEPARTRIO study. Ann Oncol 19:292–298
15. Martín M, Lluch A, Seguí MA et al (2006) Toxicity and health-related quality of life in breast cancer patients receiving adjuvantdocetaxel, doxorubicin, cyclophosphamide (TAC) or 5-fluorouracil,doxorubicin and cyclophosphamide (FAC): impact of adding primary
Support Care Cancer

prophylactic granulocyte colony stimulating factor to the TAC regi-men. Ann Oncol 17:1205–1212
16. Aarts MJ, Peters FP, Mandigers CM et al (2013) Primary granulocytecolony-stimulating factor prophylaxis during the first two cycles onlyor throughout all chemotherapy cycles in patients with breast cancerat risk for febrile neutropenia. J Clin Oncol 31:4290–4296
17. Health Insurance Portability and Accountability Act (HIPAA) of1996, 42 USC §1320-d2
18. US Dept of Health & Human Services (USDHH). Public welfare—protection of human subjects, 45 CFR 46. Effective July 14, 2009.(http://www.hhs.gov/ohrp/humansubjects/guidance/45cfr46.html)
19. National Comprehensive Cancer Network (2012) NCCN clinicalpractice guidelines in oncology. Breast cancer. V.3.2012 (http://www.nccn.org/professionals/physician_gls/pdf/breast.pdf)
20. National Comprehensive Cancer Network (2012) NCCN Clinicalpractice guidelines in oncology. Non-Hodgkin’s lymphomas.V.3.2012 (http://www.nccn.org/professionals/physician_gls/pdf/nhl.pdf)
21. Tilly H, Vitolo U, Walewski J, da Silva MG, Shpilberg O, André M,Pfreundschuh M, Dreyling M, ESMO Guidelines Working Group(2012) Diffuse large B-cell lymphoma (DLBCL): ESMO clinicalpractice guidelines for diagnosis, treatment and follow-up. AnnOncol 23(Suppl 7):vii78–vii82
22. Aebi S, Davidson T, Gruber G, Cardoso F, ESMO GuidelinesWorking Group (2011) Primary breast cancer: ESMO clinical prac-tice guidelines for diagnosis, treatment and follow-up. Ann Oncol22(Suppl 6):vi12–vi24
23. Baker J, McCune JS, Harvey RD 3rd, Bonsignore C, Lindley CM(2000) Granulocyte colony-stimulating factor use in cancer patients.Ann Pharmacother 34:851–857
24. Swanson G, Bergstrom K, Stump E, Miyahara T, Herfindal ET(2000) Growth factor usage patterns and outcomes in the communitysetting: collection through a practice-based computerized clinicalinformation system. J Clin Oncol 18:1764–1770
25. Du XL, Lairson DR, Begley CE, Fang S (2005) Temporal andgeographic variation in the use of hematopoietic growth fac-tors in older women receiving breast cancer chemotherapy:findings from a large population-based cohort. J Clin Oncol23:8620–8628
26. NaeimA, HenkHJ, Becker L, Chia V, Badre S, Li X, Deeter R (2013)Pegfilgrastim prophylaxis is associated with a lower risk of hospital-ization of cancer patients than filgrastim prophylaxis: a retrospectiveUnited States claims analysis of granulocyte colony-stimulating fac-tors (G-CSF). BMC Cancer 13:11
27. Weycker D, Malin J, Barron R, Edelsberg J, Kartashov A, Oster G(2012) Comparative effectiveness of filgrastim, pegfilgrastim, andsargramostim as prophylaxis against hospitalization for neutropeniccomplications in patients with cancer receiving chemotherapy. Am JClin Oncol 35:267–274
28. Rajan SS, Stearns SC, Lyman GH, Carpenter WR (2011) Effect ofprimary prophylactic G-CSF use on systemic therapy administrationfor elderly breast cancer patients. Breast Cancer Res Treat 130:255–266
29. Tan H, Tomic K, Hurley D et al (2011) Comparative effectiveness ofcolony-stimulating factors for febrile neutropenia: a retrospectivestudy. Curr Med Res Opin 27:79–86
30. HeaneyML, Toy EL, Vekeman F, Laliberte F, Dority BL, Perlman D,Barghout V, Duh MS (2009) Comparison of hospitalization risk andassociated costs among patients receiving sargramostim, filgrastim,and pegfilgrastim for chemotherapy-induced neutropenia. Cancer115:4839–4848
31. Morrison VA, Wong M, Hershman D, Campos LT, Ding B, Malin J(2007) Observational study of the prevalence of febrile neutropenia inpatients who received filgrastim or pegfilgrastim associated with 3–4 week chemotherapy regimens in community oncology practices. JManag Care Pharm 13:337–348
32. Chen-Hardee S, Chrischilles EA, Voelker MD, Brooks JM, Scott S,Link BK, Delgado D (2006) Population-based assessment of hospi-talizations for neutropenia from chemotherapy in older adults withnon-Hodgkin’s lymphoma (United States). Cancer Causes Control17:647–654
33. Caggiano V, Weiss RV, Rickert TS, Linde-Zwirble WT (2005)Incidence, cost, and mortality of neutropenia hospitalization associ-ated with chemotherapy. Cancer 103:1916–1924
34. Weycker D, Sofrygin O, Seefeld K, Deeter RG, Legg J, Edelsberg J(2013) Technical evaluation of methods for identifyingchemotherapy-induced febrile neutropenia in healthcare claims data-bases. BMC Health Serv Res 13:60
Support Care Cancer