Embed Size (px)
Citation preview

USE OF CONTRAST-ENHANCED ULTRASOUND FOR
CHARACTERIZATION OF FOCAL SPLENIC LESIONS
FEDERICA ROSSI, VITO FERDINANDO LEONE, MASSIMO VIGNOLI, ETSER LADDAGA, ROSSELLA TERRAGNI
Contrast-enhanced ultrasound was used to study focal and multifocal lesions of the spleen in 26 dogs and two
cats affected by 11 benign and 18 malignant splenic diseases. A second-generation microbubble contrast medium
(Sonovue) was injected into the cephalic vein and enhancement patterns were subjectively described and time
intensity curves calculated. Final diagnosis was obtained by histopathologic examination after splenectomy
(n¼ 19) or by needle aspiration and sonographic follow-up after 4 and 8 weeks (n¼ 9). Contrast-enhanced
ultrasound parameters, improving the characterization between benign and malignant lesions, were established.
The most useful criterion was the hypoechogenicity of the lesion in the wash-out phase combined with the
presence of tortuous feeding vessels, which was observed in association with malignancy. All malignant lesions
were hypoechoic to the surrounding spleen 30 s after starting the contrast medium injection. Lymphosarcoma
and hemangiosarcoma had characteristic perfusion patterns. Lymphosarcoma had rapid time to peak and early
wash-out phase with a honeycomb pattern during the wash-out. Hemangiosarcomas were large nonperfused
masses in all phases surrounded by hypervascular splenic parenchyma. Benign lesions except one hematoma and
a benign histiocytoma had the same perfusion pattern as the surrounding spleen. Ultrasonographic and contrast-
enhanced ultrasound findings of an accessory spleen are reported. Contrast-enhanced ultrasound can improve
the characterization of focal or multifocal lesions of the spleen. Veterinary Radiology & Ultrasound, Vol. 49,
No. 2, 2008, pp 154–164.
Key words: contrast-enhanced ultrasound, microbubble contrast medium, small animals, spleen, sulfur
hexafluoride.
Introduction
FOCAL SPLENIC LESIONS are frequently identified during
routine ultrasonographic examination, especially in
old animals. They are often incidental findings and repre-
sent a diagnostic challenge. Because the echo pattern and
large vascular architecture of benign and malignant con-
ditions of the spleen are similar,1–5 baseline gray-scale and
color Doppler ultrasound have limited accuracy in char-
acterizing splenic disorders. Therefore, cytology or histol-
ogy are required for the final diagnosis.
Contrast-enhanced ultrasound involves injecting a small
quantity of a microbubble contrast medium into a periph-
eral vein with subsequent sonographic enhancement of a
vessel or tissue. With second generation contrast media, the
nonlinear oscillation of the microbubbles can be detected in
real time, and the perfusion of parenchymal focal lesions
can be compared with the surrounding tissue.
In Europe, contrast-enhanced ultrasound is routinely
used in humans to characterize liver lesions and the diag-
nostic accuracy is similar to that of contrast-enhanced
computed tomography (CT) and magnetic resonance (MR)
imaging.6–8 Recently, abdominal extrahepatic application
has been proposed.9,10 Initial studies suggest that contrast-
enhanced ultrasound is of diagnostic value in patients with
splenic and perisplenic lesions,11–16 but little information is
available on the perfusion pattern of focal splenic nodules.
Benign neoplasia is uncommon in humans and malignancy
is extremely rare. Lymphoma and angiosarcoma are re-
ported only occasionally,17,18 nodular hyperplasia is a rare
condition with a postmortem incidence ranging from
0.024% to 0.13%.19
In small animals, contrast-enhanced ultrasound has
been used to study normal liver perfusion,20, 21 liver focal
lesions,22 portosystemic shunts,23 and lymphadenomegaly
caused by lymphoma.24 This method can be used in small
animals without adverse effects and it is useful in charac-
terizing liver nodules and in identifying the vascular archi-
tecture of malignant lymph nodes.
The aim of this prospective study was to evaluate
whether contrast-enhanced ultrasound can be used to more
accurately characterize the perfusion of splenic focal ab-
normalities in small animals. Moreover, we attempted to
establish criteria that can be used to distinguish benign
from malignant splenic lesions and different types of
malignancies.
Address correspondence and reprint requests to F. Rossi, at the aboveaddress. E-mail: [email protected]
Received April 20, 2007; accepted for publication October 4, 2007.doi: 10.1111/j.1740-8261.2008.00343.x
From the Veterinary Clinic dell’Orologio–Via Gramsci 1/4 - 40037Sasso Marconi, Bologna, Italy (Rossi, Leone, Vignoli, Terragni), DVL,Veterinary Laboratory, Via Gramsci 1/3–40037 Sasso Marconi, Bologna,Italy (Laddaga).
154

Materials and Methods
Dogs and cats were included in this study according
to the following criteria: (1) single focal or multifocal
sonographic splenic lesions identified during routine sono-
graphy, (2) it was possible to perform the contrast-
enhanced ultrasound study without sedation or anesthe-
sia, and (3) splenectomy with subsequent histopathologic
examination, or diagnostic cytology was performed.
After the initial gray-scale ultrasound study, a 20G
intravenous cannula was placed in the cephalic vein. Saline
was administered during the procedure. Animals were
maintained in right lateral recumbency without sedation or
anesthesia and, during the examination, heart, and breath-
ing rate, femoral pulse, and mucosal refilling time were
recorded.
The ultrasound equipment included two systems with
coded harmonic capabilities� with two probes, a curvilin-
ear transducer with a receive frequency of 3.2MHz and a
linear probe with a receive frequency of 5MHz. The first
system was used for the first 21 dogs. The last nine dogs
were examined with the other equipment, which became
available during the second part of the study. For the
contrast study, the two machines functioned with the same
detection mode (contrast-tuned imaging mode). The same
two probes were used during the entire study. To reduce
the acoustic impact of the ultrasound waves on the micro-
bubble contrast agent, and to increase the persistence of the
contrast medium in the blood, the mechanical index was
always lower than 0.1 (range 0.05–0.1), which corresponds
to an acoustic pressure lower than 45kPa. A single focal
zone was placed in the deepest part of the lesion. The
overall gain and time-gain compensation were set so that
no signal from the underlying parenchyma of the spleen
was present; only very low background signal from the
splenic capsule or perisplenic vessels were maintained to
have an anatomic reference in the image. Standard and
contrast-enhanced ultrasound examinations were per-
formed by the same operator (F.R.). Part of the normal
splenic parenchyma surrounding the lesion was included in
the image so that it was possible to compare flow in two
different areas. A bolus of a second-generation sulfur
hexafluoride contrast mediumw was injected intravenously
at a dosage of 0.03ml/kg of prepared solution (5mg/ml). A
5ml normal saline flush followed. The timer was activated
at the moment of starting the injection and the flow of the
contrast medium into the lesion was observed in real time.
Care was taken to keep the probe in exactly the same po-
sition for at least 2min. Each animal received two injec-
tions of contrast medium. During the first injection the
total gain, time-gain compensation and position of the fo-
cal zone were occasionally changed to optimize the image,
and this setting was then maintained unchanged for the
subsequent injection. The second injection was performed
at about 5min following the first. Between the two injec-
tions, the ultrasound system was reset to its fundamental
setting and the cranial abdomen was scanned so that re-
sidual microbubbles could be destroyed before the second
examination.
In patients where there was more than one splenic lesion
with a similar baseline sonographic appearance, the largest
and more clearly imaged lesion was evaluated first. The
entire procedure was digitally recorded for later review.
Recorded movies were subjectively reviewed and a group
consensus formulated to describe the perfusion of the le-
sions and surrounding spleen.
The lesions were analyzed as follows. Echogenicity dur-
ing the wash-in, peak, and wash-out phases was defined as
hyper-, iso-, or hypoechoic compared with normal sur-
rounding spleen. Contrast enhancement in the lesion was
classified as absent (no enhancement), rim-like (continuous
ring of uniform peripheral enhancement), peripherally
irregular (with a peripheral rim of enhancement of vari-
able thickness), honeycomb (small hypoechoic areas),
diffusely homogeneous, and diffusely heterogeneous
(Table 1). Afferent vessels were described as either peri-
pheral or central, and straight or tortuous.
A commercial softwarez application was used to mea-
sure the mean pixel value in a region of interest. Because
any change in the setting parameters modifies the results of
a quantitative analysis, only the videos acquired during the
second injection were used for this evaluation. A frame was
selected every 2 s for the first 2min of the videos. In each
sampled frame, two different regions of interest were
drawn, inside the lesion and in the normal splenic paren-
chyma, at approximately the same depth. Inside homoge-
neous lesions, one region of interest (as large as possible)
was depicted in the center, whereas inhomogeneous chang-
es were sampled by two or more regions of interest, rep-
resenting parts with different perfusion.
Time–intensity curves were constructed using commer-
cial software.y The peak intensity, time to peak, average
up- and down-slope of the lesions and surrounding splenic
parenchyma were calculated. Time to peak was measured
from T0 (time of injection). To calculate average up- and
down-slope, the part of the curve with values above 10% of
baseline and up to about 90% of the peak enhancement
was used.
Nineteen dogs underwent splenectomy and the final
diagnosis was obtained upon histologic analysis of the
surgical specimen. In the remaining nine patients (seven
dogs and two cats), needle aspiration of the lesion was
�CnTI Megas Esatune, Esaote Firenze, Italy CnTI Mylab 30, EsaoteFirenze, Italy.wSonovue
s
, Bracco, Milano, Italy.zNIH Image J (US National Institute of Health, Bethesda, MD).yMicrosoft Excel 2000, Microsoft Corporation, Richmond, WA.
155CONTRAST-ENHANCED ULTRASOUND OF SPLENIC LESIONSVol. 49, No. 2

performed, followed by cytology. Because a diagnosis
based on cytologic sampling can be incorrect,25 ultrasound
examinations were performed again after 4 and 8 weeks to
reassess the sonographic features. Number, size, and echo-
genicity of the splenic nodules were compared with the
findings observed at the time of the contrast study.
Results
Between October 2003 and December 2006, 26 dogs and
two cats were studied. There were 14 males (13 dogs and
one cat) and 14 females (13 dogs and one cat). Mean age
was 10.0� 2.7 years (standard deviation [SD]) with a range
from 2.6 to 15 years.
On gray-scale ultrasound examination, single (n¼ 19) or
multiple parenchymal lesions (n¼ 9) of variable size and
echogenicity were detected (Table 1). The final diagnosis
included 11 benign and 18 malignant splenic lesions. One
dog had two different conditions, nodular hyperplasia and
accessory spleen. The 11 benign lesions included nodular
hyperplasia (n¼ 6), extramedullary hematopoiesis (n¼ 2),
hematoma (n¼ 1), benign fibrous histiocytoma (n¼ 1), and
one accessory spleen (splanunculus) (n¼ 1). Malignancy
was represented by the following diseases: lymphosarcoma
(n¼ 7), hemangiosarcoma (n¼ 4), malignant fibrous hist-
iocytoma (n¼ 2), undifferentiated sarcoma (n¼ 1), hist-
iocytic sarcoma (n¼ 1), liposarcoma (n¼ 1), mast cell
tumor (n¼ 1) and metastasis (n¼ 1).
The entire ultrasound procedure was always performed
in o10min and there were no changes in the monitored
physiologic parameters.
Small and superficial lesions (n¼ 19) were examined with
the 5MHz linear probe only, whereas only the 3.2MHz
curvilinear probe was used for large and deep nodules or
masses (n¼ 10). When possible (n¼ 3), the same lesion was
studied with both transducers and the two contrast se-
quences were compared. In these three patients, no differ-
ence was found in the perfusion pattern. With the linear
probe, image spatial resolution was subjectively judged to
be higher for both the fundamental and the contrast study.
During the first injection, the parameters were some-
times adjusted slightly, so that they were set optimally for
the second injection. This was necessary primarily for small
and superficial nodules, where the time gain compensation
in the near field was initially too low according to the
technical suggestions delivered from the experience in
human imaging.
The flow of the contrast medium in the abnormal and
surrounding normal spleen was easily detected and com-
pared in all patients by subjective analysis. The quantita-
tive analysis and construction of the perfusion curves
helped to better describe the perfusion patterns primarily
in the first seconds of the examination, during the wash-in
phase, when the changes in echogenicity were sometimes
very fast. Moreover, additional information was obtained
in the hematoma, where the quantitative analysis enabled
identification of low perfusion, which was difficult to detect
with subjective analysis.
In the fundamental study, the benign lesions were of
various size and echogenicity (see Table 1). In nine of the
11 benign lesions (nodular hyperplasia, extramedullary he-
matopoiesis, and accessory spleen), the lesions had similar
wash-in and wash-out to the surrounding spleen, so that
after a few seconds the nodules were isoechoic and diffusely
homogeneous. In this group, only two small hyperplastic
nodules were briefly hyperechoic in the early arterial phase,
but at peak and in the wash-out phase they had the
same echogenicity as the surrounding normal spleen (Fig.
1A–D). No feeding vessels were evident. The accessory
spleen was a round hilar structure (about 2 cm in diame-
ter), homogeneous, and isoechoic to the spleen. With
contrast-enhanced ultrasound, the perfusion of the acces-
sory spleen was identical to that of the adjacent spleen
(Fig. 2A and B). In the nine benign lesions, mean time to
Table 1. Histological Type and Gray-Scale Appearance of Splenic Focal Lesions
LesionMean Size
(Range) (cm)Single (s)
or Multiple (m) Hypoechoic Hyperechoic Isoechoic Mixed Complex Target
Malignancy (n¼ 18)
LSA (n¼ 6) 2.1 (0.7–3) 5 sþ 1m 5 1HSA (n¼ 4) s 1 1 2Malignant fibrous histiocytoma (n¼ 2) 9 (8–10) s 1 1Undifferentiated sarcoma (n¼ 1) 6 s 1Histiocytic sarcoma (n¼ 1) 1.6 s 1Liposarcoma (n¼ 1) 4 s 1Mast cell tumour (n¼ 1) o1 m 6Metastasis (n¼ 1) o1 m 3Benignancy (n¼ 11)
Nodular hyperplasia (n¼ 6) 1.1 (0.3–2) 2 sþ 4m 3 4 2 1Extramedullary hematopoiesis (n¼ 2) o1 m 1 1Hematoma (n¼ 1) 0.8 s 1Benign fibrous histiocytoma (n¼ 1) 3.5 s 1Accessory spleen (n¼ 1) 1 s 1
156 ROSSI ET AL. 2008

peak was 34.4 s (SD 6.6) for lesions and 34.4 (SD 8.3) for
surrounding normal spleen. Mean lesion peak intensity was
93.7% of the surrounding normal spleen (SD 10.6%).
Mean up-slope was 3.5 mean pixel value/s (SD 0.6) for the
benign lesions and 3.1 mean pixel values/s (SD 1.0) for the
surrounding normal spleen. Mean down-slope was �0.89mean pixel value/s (SD 1.0) for the benign lesions and
�0.58 mean pixel values/s (SD 0.6) for the surrounding
normal spleen.
The hematoma (Fig. 3) appeared as a small (0.8 cm)
target lesion in gray-scale imaging. After contrast medium
injection, it was a round homogeneous hypoechoic area
with constant, low homogeneous perfusion. Lesion mean
pixel value intensity, measured from the initial rise of the
curve (12 s) to the end of the examination, was 22% of the
peak intensity measured in the surrounding spleen (range
15–27%). The benign histiocytoma, a 3.5 cm hypoechoic
nodule in baseline imaging, was the only clearly hyperper-
fused lesion. Compared with the surrounding parenchyma,
it had rapid, intense enhancement and was strongly hype-
rechoic in the wash-in phase. After the peak, the echo-
genicity decreased slowly and the lesion was isoechoic to
the surrounding normal spleen after 50 s. In the first few
seconds after contrast medium injection, multiple small
vessels were seen, homogeneously distributed in the central
part of the lesion. Time to peak intensity was 16 s, peak
intensity was more than 2.5 times the peak intensity of the
surrounding normal spleen (268%). Up- and down-slope
of the lesions were 12.8 and �1.5 mean pixel value/s, the
up- and down-slope of the surrounding spleen were 2.0 and
�0.6 mean pixel value/s.
In all malignant lesions, the perfusion was very different
in comparison to that in normal splenic parenchyma. After
contrast medium administration, lesion size and margins
were better defined because of higher contrast resolution of
the adjacent spleen. In three patients (two lymphosarcoma
and one hemangiosarcoma) additional smaller nodules
which had not been noted in the fundamental study were
detected. These nodules were small (mean size 0.4 cm) and
isoechoic to the surrounding normal spleen in gray-scale
imaging. With contrast-enhanced ultrasound, they were
easily detected due to different echogenicities. Malignant
lesions had variable echogenicity in the wash-in phase and
at peak. All malignant lesions became either completely or
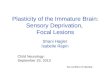
Fig. 1. Gray-scale (A) and contrast enhanced ultrasound (B–D) images of a hyperplastic splenic nodule. The lesion is a round hypoechoic nodule infundamental ultrasound (A). In the first seconds of the contrast-enhanced ultrasound examination (B), before the entrance of the contrast medium, the image isblack because of the suppression of the fundamental signal. After 13 s (C), the nodule is slightly hyperechoic to the surrounding spleen, but it becomescompletely homogeneous after a few more seconds (D).
157CONTRAST-ENHANCED ULTRASOUND OF SPLENIC LESIONSVol. 49, No. 2

extensively hypoperfused during the wash-out phase. In 12
patients (lymphosarcoma, malignant fibrous histiocytoma,
histiocytic sarcoma, mast cell tumor, metastasis), the wash-
out was fast and homogeneous. In the remaining six pa-
tients (hemangiosarcoma, undifferentiated sarcoma, and
liposarcoma), the wash-out was inhomogeneous with large
hypoperfused areas in the late phase. Table 2 summarizes
the observed perfusion patterns.
Excluding the hemangiosarcoma and the undifferentiat-
ed sarcoma, which had no peak, all other malignant lesions
had a mean time to peak of 23 s (SD 7.8). All malignant
lesions were hypoechoic to the surrounding spleen 30 s
after starting the injection.
Hemangiosarcoma (n¼ 4) and the undifferentiated
sarcoma (n¼ 1) were characterized in all phases by homo-
geneous anechoic (nonperfused) areas with highly
vascularized surrounding parenchyma (peripheral irregu-
lar perfusion pattern). Thin septae of hyperechoic tissue
entered the anechoic areas with a sharp demarcation be-
tween these two different parts. Tortuous vessels were vis-
ible on the periphery of the lesion (Fig. 4). Based on the
time–intensity curves, there was no enhancement in the
large anechoic lesions, and pixel intensity did not change
from the baseline.
Lymphosarcoma (n¼ 7) and histiocytic sarcoma (n¼ 1)
were isoechoic (n¼ 6) or hyperechoic (n¼ 2) in the wash-in
phase, with a diffuse homogeneous enhancement and a
rapid time to peak. At peak, they were hypoechoic (n¼ 6)
or hyperechoic (n¼ 2) to the surrounding spleen. The le-
sion wash-out phase started before the splenic peak (early
wash-out phase) and all nodules became hypoechoic dur-
ing this phase. The contrast medium washed out progres-
sively from the lesions, leaving a round hypoechoic lesion
characterized by small round anechoic areas (honeycomb
Fig. 3. Gray-scale (A) and contrast enhanced ultrasound (B) images of a hematoma, appearing as small (0.8 cm) target lesion in gray-scale imaging. Aftercontrast medium injection, it appeared as a round homogeneous hypoechoic area with constant, low homogeneous perfusion.
Fig. 2. Accessory spleen in a 9-year-old female Boxer. A round structure, homogeneous and isoechoic to the spleen, is visible at the splenic hilus (A). Withcontrast-enhanced ultrasound the perfusion of the accessory spleen is identical to the adjacent normal spleen (B). This enables differentiation between theaccessory spleen and a splenic lymph node.
158 ROSSI ET AL. 2008

Table2.Contrast
EnhancedUltrasoundDiagnostic
Findings/CriteriaforMalignancy
andBenignancy
Contrast
Enhan
cedUltrasoundDiagnostic
Findings/criteria
forMalignancy
andBenignancy
Lesion
Contrast
EnhancedUltrasoundFindings
Echogenicity(lesionvs.spleen)
EnhancementPattern
FeedingVessels
Wash-in
Peak
Wash-out
Malignancy
(n¼18)
LSA
(n¼7)
Hyper
(n¼2)–iso(n¼5)
Hyp
er(n¼2),
hypo(n¼5)
Hypo
Diffuse
homogeneous(w
ash-in,peak),
honeycomb(w
ash-out)
Finenet
ofthin
uniform
lydistributed
vesselin
thelesion
Hystiociticsarcoma(n¼1)
Iso
Hyp
oHypo
Diffuse
homogeneous(w
ash-in,peak),
honeycomb(w
ash-out)
Finenet
ofthin
uniform
lydistributed
vesselin
thelesion
HAS(n¼4)þ
Hyper
(periphery),
hypo(center)
Hyp
oHypo
Peripheralirregu
lar,absence
of
enhan
cementin
thehyp
oechoicareas
Tortuousvesselsattheperiphery
Undifferentiatedsarcoma(n¼1)
Hypo
Hyp
oHypo
Peripheralirregu
lar,absence
of
enhan
cementin
thehyp
oechoicareas
Tortuousvesselsattheperiphery
Malignantfibroushistiocytoma(n¼2)
Hypo
Hyp
oHypo
Diffuse
homogeneous
Tortuousvesselsattheperiphery
Metastasis(n¼1)
Hypo
Hyp
oHypo
Diffuse
heterogeneous(w
ash-in),
diffuse
homogeneous(peak,wash-
out)
Thin
tortuousvesselsaroundthenodules
Mast
celltumor(n¼1)
Hypo
Hyp
oHypo
Diffuse
heterogeneous(w
ash-in),
diffuse
homogeneous(peak,wash-
out)
Thin
tortuousvesselsin
theparenchym
a
Liposarcoma(n¼1)
Hyper
Iso
Hypo(centre),
iso(periphery)
Peripheralirregu
lar
Tortuousvesselsat
theperiphery
Benignancy
(n¼11)
Nodularhyperplasiaandextramedullary
hem
atopoiesis(n¼8)
Iso(n¼6)slightlyhyper-(n¼2)
Iso-
Iso
Diffuse
homogeneous
Sim
ilarto
thesurroundingspleen
Hem
atoma(n¼1)
Hypo
Hyp
oHypo
Diffuse
homogeneous,mild
enhan
cement
Novessels
Benignhistiocytoma(n¼1)
Clearlyhyper-
Hyp
er-
Hyper-
Diffuse
homogeneous(w
ash-in),
diffuse
heterogeneouswithring-
enhan
cement(w
ash-out)
Dense
vesselsdistributionin
thecentral
part
Accessory
spleen
(n¼1)
Iso
Iso
Iso
Diffuse
homogeneous
Sim
ilarto
thesurroundingspleen
159CONTRAST-ENHANCED ULTRASOUND OF SPLENIC LESIONSVol. 49, No. 2

pattern). Feeding vessels were represented by a fine net of
thin, uniformly distributed vessel (Fig. 5).
Mean time to peak was 21.7 s (SD 4.9) for the lesions
and 36 s (SD 9.6) for surrounding spleen. Mean peak in-
tensity was 92.7% (SD 25.6%) of the mean surrounding
spleen peak intensity. Mean up-slope was 10.1 mean pixel
values (SD 2.0) for the malignant lesions and 5.0 mean
pixel values (SD 2.5) for surrounding normal spleen. Mean
down-slope was �2.0 mean pixel values (SD 0.4) for the
lesions and �0.92 mean pixel values (0.3 SD) for the sur-
rounding normal spleen.
All nine lesions diagnosed with cytology (nodular hy-
perplasia, extramedullary hematopoiesis, and the accessory
spleen) were benign. Based on the sonographic follow-up
examination after 4 and 8 weeks there were no changes in
number, size, or echogenicity of the nodules.
Discussion
Sonovue is a second generation ultrasound contrast me-
dium containing a central gaseous nucleus (sulfur hexaflu-
oride) stabilized by an external elastic phospholipidic shell.
The low solubility of sulfur hexafluoride improves its
stability in the vascular compartment. These very small
microbubbles (mean diameter 2.5mm) are able to pass the
pulmonary capillary circulation and remain in the blood
pool for a longer time compared with first-generation
contrast media like Levovist. For this reason, sulfur hexa-
fluoride can be used both as a macrovascular and a
microvascular enhancer.
When exposed to an ultrasound wave, microbubbles
have significantly higher reflectivity than blood and soft
tissues,26 so they enhance the acoustic signal in the blood
circulation. When imaged with an ultrasound wave of low
acoustic power (mechanical index lower than 0.1 or
45kPa), the microbubbles are minimally destructed and
oscillate continuously, allowing real-time imaging of tissue
perfusion. When compared with the incident wave, the
reflected ultrasound is modified in two ways:27 First, it
contains nonlinear components, as a consequence of the
asymmetric oscillation of the microbubbles. Second, it in-
cludes harmonic frequencies. To improve the contrast-to-
tissue ratio and maximize the distinction between blood-
derived signal and tissue-derived signal, contrast-specific
Fig. 4. Contrast-enhanced ultrasound examination (A–C) and time–intensity curve (D) of a large complex mass in a dog with hemoperitoneum (finaldiagnosis: hemangiosarcoma). In the first few seconds, tortuous vessels are seen at the periphery of the lesion (A). The lesion has a peripheral irregular perfusionpattern, with a homogeneous anechoic (nonperfused) central area surrounded by highly vascularized parenchyma (B). Smaller anechoic nodules are visible (C).The enhanced parenchyma on the left of the images is the caudal left margin of the liver. (D) Time–intensity curve. Triangle line, region of interest in the centreof the lesion has no enhancement; dotted line, region of interest in the surrounding spleen.
160 ROSSI ET AL. 2008

imaging modalities were developed. Because the difference
in microbubble tissue backscatter is much higher for har-
monic frequencies, harmonic imaging can be used as a
contrast-specific method to clearly depict differences in the
perfusion of tissues. The flow of contrast medium can be
assessed by coded harmonic imaging, - that is, by sup-
pressing the contribution of the fundamental frequencies in
the image construction. Another way to distinguish the
contrast-specific signal from the tissue-derived signal is to
detect nonlinear components by pulse-cancellation tech-
niques. With this modality, multi-pulse sequences with
precise changes in transmitted inter-pulse amplitude and
phases are used to reject the linear fundamental tissue sig-
nal and retain the nonlinear signal from the microbubbles.
If precise, this modulation produces very good contrast-to-
tissue ratio and has high sensibility in the detection of the
contrast medium signal.28
In this study, coded harmonic imaging was used to
evaluate the perfusion of focal splenic lesions in a popu-
lation of 26 dogs and two cats of various ages. The flow of
contrast medium could be visualized easily in the vascular
part of the lesion and in the surrounding normal splenic
parenchyma in the real-time examination. The linear
5MHz probe was adequate for small and superficial le-
sions, whereas the 3.2MHz convex probe was necessary for
examining large and deeper masses and for screening the
liver. In patients where both probes were used, no differ-
ence was found regarding the analysis of perfusion; how-
ever, the study quality was subjectively judged to be
superior with the linear probe because of its higher spatial
resolution.
All examinations were performed without sedation or
anesthesia, and the animals were easily restrained in right
lateral recumbency for the time required for the study,
which was always o10min. The injection of contrast me-
dium did not produce any physiologic changes, supporting
that the procedure is safe and well tolerated. Noncooper-
ative animals, mainly cats, may need to be sedated or
anesthetized, and possible secondary changes in splenic
blood flow must be considered. It is known that anesthetic
drugs such as acepromazine, thiopental and medetomi-
dine–diazepam–ketamine can increase splenic volume in
Fig. 5. Contrast enhanced ultrasound examination (A–C) and time–intensity curve (D) of a dog with a splenic lymphosarcoma. During the wash-in phase(A), the nodule is slightly hyperechoic with a diffuse homogeneous enhancement. In the wash-out phase (B), the lesion becomes hypoechoic with small anechoicround areas (honeycomb pattern). A second smaller nodule is visible on the left. This was not detected in the fundamental examination. (D) Time–intensityCurve. Pink line, region of interest in the center of the lesion; blue line, region of interest in the surrounding normal spleen.
161CONTRAST-ENHANCED ULTRASOUND OF SPLENIC LESIONSVol. 49, No. 2

dogs.29,30 Smooth muscle relaxation has been hypothetized
to produce passive congestion during anesthesia and in this
situation the presence of microbubbles in the red pulp si-
nusoids would probably increase. It has been reported that
propofol does not modify splenic size, whereas it shortens
the time to peak enhancement of the liver in normal dogs
after Sonovue administration.21 No studies have yet been
performed to quantify the perfusion rate of the spleen in
anesthetized animals. It would be necessary to compare the
same animals before and after sedation or anesthesia to
establish whether these drugs modify the normal splenic
enhancement and the appearance of focal lesions during
the contrast study.
In this study, 29 focal or multi-focal splenic lesions in 26
dogs and two cats were examined with contrast-enhanced
ultrasound. Subjective and quantitative analysis of the vid-
eo enabled the perfusion of the lesions to be described
during the wash-in, peak and wash-out phases, comparing
the focal changes with the surrounding normal spleen.
Sonographic findings were compared and grouped accord-
ing to the final diagnosis, with the aim of establishing cri-
teria that could be associated with benign and malignant
splenic lesions (Table 1). In this series, most benign lesions
(10/12) had a perfusion pattern similar to the adjacent
parenchyma, so that the lesions were isoechoic to the
surrounding normal spleen after the first few seconds. All
these lesions were homogeneously isoechoic in the wash-
out phase. This can be explained by the similar architecture
of the vascular network associated with benign hyperplas-
tic conditions and normal spleen.
The hematoma was the only benign-hypoperfused lesion
and it had very mild enhancement, which could represent
revascularization after hemorrhage. Unfortunately, this
was a single lesion and nothing can be assessed about the
perfusion pattern in hematomas of different ages. Absence
of associated hyperperfused areas and tortuous feeding
vessels were recognized as criteria for differentiating this
hematoma from the hypovascular areas observed in all
hemangiosarcomas. In this comparison, the quantitative
analysis added another differential criterion of a low but
constant perfusion in the hematoma vs. a complete absence
of any enhancement in the large hypoechoic areas associ-
ated with the hemangiosarcomas. This single observation
agrees with a recent CT study, in which splenic hematomas
were characterized by higher attenuation in comparison
with hemangiosarcomas after contrast medium adminis-
tration.31 When comparing these results, it must be con-
sidered that the enhancement mechanism is different in CT
vs. contrast-enhanced ultrasound, because the iodinated
contrast medium diffuses in the extracellular space whereas
the microbubble contrast medium is a pure blood-pool
agent. Despite this difference, sonographic and CT features
of splenic lesions overlap in humans.11,32 Spontaneous
splenic hemorrhage is an uncommon condition in dogs;
however, hematomas inside nodular hyperplasia lesions oc-
cur frequently and are believed to represent a continuum.33
Therefore, areas of low uptake associated with benign hy-
perplasia may be expected with contrast-enhanced ultra-
sound. Even though the examination of this hematoma
suggests that contrast-enhanced ultrasound could be helpful
in differentiating this type of lesion from hemangiosarcoma,
no conclusion can be made from a single patient.
In this study, we also identified a hilar accessory spleen
in a dog. Accessory spleens are frequently reported as in-
cidental sonographic findings in humans. These single or
multiple islands of normal splenic parenchyma occur fre-
quently at the splenic hilum, and they may also be found in
the gastrosplenic and splenorenal ligaments or in the tail of
the pancreas, but rarely elsewhere in the abdomen.34 Mi-
crobubble contrast medium helps distinguish them from an
enlarged hilar lymph node or a pancreatic mass.11,15 The
accessory spleen has enhancement identical to that of the
parent spleen and retains contrast medium in the paren-
chymal phase.32,33 Hilar lymph nodes have transient
enhancement in the arterial phase.12 In 14 human patients
with perisplenic lesions, six neoplastic conditions were
differentiated from eight accessory spleens because of the
contrast-enhanced ultrasound pattern.15
The perfusion pattern of malignant lesions was different
than observed in the surrounding normal parenchyma. Af-
ter variable wash-in and peak phases, all malignant lesions
became completely or extensively hypoperfused during the
wash-out phase. Thirty seconds after injection, these hypo-
echoic lesions were easily detected, as they were surrounded
by hyperechoic splenic parenchyma. Associated tortuous
vessels were observed in all malignant lesions. These results
confirm the observations reported for splenic malignancy in
humans9–11 and are analogous to the contrast-enhanced
sonographic features of liver neoplasia in small animals,22
suggesting that hepatic and splenic tumors behave similarly
with contrast-enhanced ultrasound, even though the nor-
mal vascular anatomy of these organs is different.
The vascular network of the spleen is complex and or-
ganized differently in the two interconnected compart-
ments, the white and red pulp. The white pulp contains
small pulpar arteries, branches of the trabecular arteries,
which originate in the splenic hilus and follow the subdi-
vision of the splenic trabeculae. The lymphatic follicles are
organized around these small arterioles. The red pulp is the
real blood reservoir. Most of the erythrocytes are con-
tained in large, thin-walled splenic sinusoids. The sinusoids
are supplied by the penicillar arterioles of the adjacent
splenic cords and continue into the pulpar and trabecular
veins. The presence of such a large vascular space with slow
blood flow is the most probable explanation for splenic
enhancement after injection of Sonovue. Even the site of
Sonovue accumulation has not been established, and
although true splenic tropism has been suggested,37 passive
162 ROSSI ET AL. 2008

pooling of microbubbles in the sinusoids seems to be the
most reliable hypothesis.12 We conclude that contrast-en-
hanced ultrasound allows detection of abnormal perfusion
patterns associated with splenic malignancies. We did not
identify why malignant lesions have a different type of per-
fusion compared with the normal parenchyma, the reasons
are probably very complex and different for the various
types of lesions. The large nonperfused areas seen with
hemangiosarcoma may correspond to the necrotic and
hemorrhagic areas associated with these tumours. Lympho-
sarcoma had early wash-in and wash-out phases, and this
possibly reflects the lack of normal sinusoidal vessels of the
red pulp combined with neoplastic angiogenesis.
Limitations of this study are the heterogeneity of the
lesions and the lack of other common types of neoplastic
and nonneoplastic splenic conditions. Many types of sar-
comas (mixo-, leiomio-, fibro-, osteosarcoma) were not
observed in this study, therefore, it is not known if they
meet our criteria for malignancy. Other neoplastic condi-
tions (liposarcoma, mast cell tumor, metastatic disease)
were seen only in isolated patients, so it is not possible to
verify whether they have specific perfusion patterns. Benign
conditions, like abscess, hemorrhage, or infarction, can
appear as focal solid lesions on gray-scale ultrasound and
are expected to be hypoperfused areas with contrast-en-
hanced ultrasound, similar to the hematoma. Limitations
of contrast-enhanced ultrasound in the differentiation be-
tween benign from malignant conditions of the spleen
could be related to the complexity of the splenic lesion. The
borderline between benign and malignant splenic condi-
tions can be difficult to define, even with histopathology,
because some lesions have transitional features.38
We suggest there is a potential role for contrast-en-
hanced ultrasound in the differentiation of focal splenic
lesions. A larger number of patients, including all types of
conditions, are needed to confirm our findings and to in-
crease knowledge in this complex field. Traumatic splenic
injuries and vascular disease are indications to perform a
contrast-enhanced ultrasound study of the spleen in hu-
mans,11–15 and these are also possible applications in vet-
erinary medicine. In animals with thromboembolism,
infarction due to partial splenic torsion or posttraumatic
splenic rupture, contrast enhanced ultrasound could be
useful in confirming the diagnosis.
In humans, contrast-enhanced CT and MR imaging are
gold standard diagnostic imaging methods for diagnosing
and characterizing focal lesions of the spleen, and specific
perfusion patterns are known.11,39,40 Compared with CT
and MR imaging, contrast-enhanced ultrasound has sim-
ilar diagnostic performance with some advantages, being
less expensive, portable, and rapidly performed, without
ionizing radiation exposure.10 Therefore, contrast-en-
hanced ultrasound is considered to be a valid alternative
to contrast CT and MR imaging.
REFERENCES
1. Cuccovillo A, Lamb CR. Cellular features of sonographic targetlesions of the liver and spleen in 21 dogs and a cat. Vet Radiol Ultrasound2002;43:275–278.
2. Ramirez S, Douglass JP, Robertson ID. Ultrasonographic featuresof canine abdominal malignant histiocytosis. Vet Radiol Ultrasound2002;43:167–170.
3. Sato AF, Solano M. Ultrasonographic findings in abdominal mastcell disease: a retrospective study of 19 patients. Vet Radiol Ultrasound2004;45:51–57.
4. Hanson JA, Papageorges M, Girard E, Menard M, Hebert P.Ultrasonographic appearance of splenic disease in 101 cats. Vet RadiolUltrasound 2001;42:441–445.
5. Nyland TG, Mattoon JS, Herrgesell ER, Wisner ER. Spleen. In:Nyland TG, Mattoon JS (eds): Small Animal Diagnostic Ultrasound, 2nded. Philadelphia: Saunders, 2002.
6. Teefey SA, Hildeboldt CC, Dehdashti F, et al. Detection of primaryhepatic malignancy in liver transplant candidates: prospective comparison ofCT, MR imaging, US and PET. Radiology 2003;226:533–542.
7. Hohmann J, Albrecht T, Hoffmann CW, Wolf KJ. Ultrasono-graphic detection of focal liver lesions: increased sensitivity and specificitywith microbubble contrast agent. Eur J Radiol 2003;46:147–159.
8. Quaia E, Calliada F, Bertolotto M, et al. Characterization of focalliver lesions with contrast-specific US modes and a sulfur hexafluoridecontrast agent: diagnostic performance and confidence. Radiology2004;232:420–430.
9. Thorelius L. Contrast-enhanced ultrasound: beyond the liver. EurRadiol 2003;13(Suppl 3):N91–N108.
10. Thorelius L. Contrast-enhenced ultrasound for extrahepatic lesions:preliminary experience. Eur J Radiol 2004;51S:S31–S38.
11. Peddu P, Shah M, Sidhu PS. Splenic abnormalities: a comparativereview of ultrasound, microbubble-enhanced ultrasound and computedtomography. Clinical Radiol 2004;59:777–792.
12. Cosgrove D. Future prospects for SonoVue and CPS. Eur RadiolSuppl 2004;14:116–124.
13. Catalano O, Cusati B, Nunziata A, Siani A. Real time, contrastspecific sonography imaging of acute splenic disorders: a pictorial review.Emergency Radiol 2004;11:15–21.
14. Glen P, MacQuerrie J, Imrie CW, Leen E. A novel application ofultrasound contrast: demonstration of splenic arterial bleeding. Br J Radiol2004;77:333–334.
15. Gorg G, Bert T. Second generation sonographic contrast agentfor differential diagnosis of perisplenic lesions. Amer J Radiol 2006;186:621–626.
16. Tafuto S, Catalano O, Barba G, et al. Real-time contrast-enhancedspecific ultrasound in staging and follow-up of splenic lymphomas. FrontBiosci 2006;11:2224–2229s.
17. Iwasaki M, Hiyama Y, Myojo S, et al. Primary malignantlymphoma of the spleen: report of a case. Rinsho Hoshasen 1988;33:405–408.
18. Smith VC, Eisenberg BL, McDonald EC. Primary splenicangiosarcoma: case report and literature review. Cancer 1985;55:1625–1627.
19. Lam KY, Yip KH, Peh WC. Splenic vascular lesions: unusualfeatures and a review of the literature. Aust N Z J Surg 1999;69:422–425.
20. Ziegler LE, O’Brien RT, Waller KR, Zagzebsky JA. Quantitativecontrast harmonic ultrasound imaging of normal canine liver. Vet RadUltrasound 2003;44:451–454.
21. Nyman HT, Kristensen AT, Kjelgaard-Hansen M, McEvoy FJ.Contrast-enhanced ultrasonography in normal canine liver. Evaluation ofimaging and safety parameters. Vet Rad Ultrasound 2005;46:243–250.
22. O’Brien RT, Iani M, Matheson J, Delaney F, Young K. Constrastharmonic ultrasound of spontaneous liver nodules in 32 dogs. Vet RadUltrasound 2004;45:547–553.
163CONTRAST-ENHANCED ULTRASOUND OF SPLENIC LESIONSVol. 49, No. 2

23. Salwei RM, O’Brien RT, Matheson JS. Use of contrast harmonicultrasound for the diagnosis of congenital portosystemic shunts in threedogs. Vet Rad Ultrasound 2003;44:301–305.
24. Salwei RM, O’Brien RT, Matheson JS. Characterization oflymphomatous lymph nodes in dogs using contrast harmonic and powerDoppler ultrasound. Vet Rad Ultrasound 2005;46:411–416.
25. Ballegeer EA, Forrest LJ, Dickinson RM, et al. Correlation ofultrasonographic appearance of lesions and cytologic and histologicdiagnoses in splenic aspirates from dogs and cats: 32 cases (2002–2005). JAm Vet Med Assoc 2007;230:690–696.
26. Schneider M, Arditi M, Barrau M, et al. BR1: a new ultrasono-graphic contrast agent based on sulfur hexafluoride-filled microbubbles.Invest Radiol 1995;30:451–457.
27. Greis C. Technology overview: Sonovue (Bracco, Milan). EurRadiol Suppl 2004;11–15.
28. Philips P, Gardner E. Contrast-agent detection and quantification.Eur Radiol Suppl 2004;4–10.
29. O’Brian RT, Kenneth RW, Osgood TL. Sonographic features ofdrug-induced splenic congestion. Vet Rad Ultrasound 2004;45:225–227.
30. Wilson DV, Evans AT, Carpenter RE, Mullineaux DR. The effect offour anhestetic protocols on splenic size in dogs. Vet Anaest Analgesia2004;31:102–103.
31. Fife WD, Samii VF, Drost WT, Mattoon JS, Hoshaw-Woodard S.Comparison between malignant and nonmalignant splenic masses in dogsusing contrast-enhanced computed tomography. Vet Radiol Ultrasound2004;45:289–297.
32. Robert M, Abbott MD, Angela D, et al. Primary vascularneoplasms of the spleen: radiologic-pathologic correlation. Radiographics2004;24:1137–1163.
33. Spangler WL, Culbertson MR. Prevalence, type, and importance ofsplenic diseases in dogs: 1480 cases (1985–1989). J Am Vet Med Ass1992;15:829–883.
34. Wadham BM, Adams PB, Johnson MA. Incidence and locations ofaccessory spleens. N Engl J Med 1981;304:1111.
35. Ota T, Ono S. Intrapancreatic accessory spleen: diagnosis usingcontrast enhanced ultrasound. Br J Radiol 2005;77:148–149.
36. Valli VEO. The hematopoietic system. In: Hubb KVF, Kennedy PC,Palmer N (eds): Pathology of Domestic Animals, 3rd ed. San Diego, CA:Academic Press, 1985;194–216.
37. Lim AK, Patel N, Eckerslay RJ, Taylor-Robinson SD, CosgroveDO, Blomley MJK. Evidence for spleen-specific uptake of a microbubblecontrast agent: a quantitative study in healthy volunteers. Radiology2004;231:785–788.
38. Spangler WL, Kass PH. Pathologic and prognostic characteristics ofsplenomegaly in dogs due to fibrohistiocytic nodules: 98 cases. Vet Pathol1998;35:583–593.
39. Rabushka LS, Kawashima A, Fishman EK. Imaging of the spleen:CT with supplemental MR examination. Radiographics 1994;14:307–332.
40. Robertson F, Leander P, Ekberg O. Radiology of the spleen. EurRadiol 2001;11:80–95.
164 ROSSI ET AL. 2008