Embed Size (px)
Citation preview

1202 Scientific Reports JAVMA, Vol 240, No. 10, May 15, 2012
SM
ALL
AN
IMA
LS
An 11-year-old 28.5-kg (62.7-lb) spayed female Collie was referred to the Veterinary Hospital of the Uni-
versity of Pennsylvania with a history of weight loss, re-gurgitation, productive cough, severe ptyalism, and ster-torous upper airway noise of approximately 12 weeks’ duration. The dog also had a chronic history of vesicular lupus erythematosus, signs of lumbosacral pain with weakness of the hind limbs, and hypothyroidism.
Results of esophagoscopy under general anesthesia 2 weeks prior to referral revealed an approximately 5-cm-diameter mass causing partial to complete obstruction of the esophageal lumen; a PEG tube had been placed by the referring veterinarian during the same anesthetic episode. Thoracic radiography was performed 1 day after PEG tube placement because the dog was febrile (body temperature, 39.8oC [103.6oF]). Results revealed osse-ous metaplasia of the lungs, dilation of the cranial aspect of the thoracic esophagus, and attenuation of the esoph-agus cranial to the heart base near a broad-based opac-ity consistent with an esophageal mass. No evidence of pneumonia was detected. A diagnosis of squamous cell
Use of a self-expanding metallic stent to palliate esophageal neoplastic obstruction in a dog
Katherine S. Hansen, dvm; Chick Weisse, vmd, dacvs; Allyson C. Berent, dvm, dacvim; Marilyn Dunn, dvm, dacvim; Ana V. Caceres, dvm, dacvr; Kim L. Todd; Jeremy S. Diroff, dvm, dacvim
Case Description—An 11-year-old spayed female Collie was evaluated because of regurgi-tation, dysphagia, severe ptyalism, coughing, and weight loss of approximately 12 weeks’ duration. Esophageal squamous cell carcinoma had been diagnosed prior to referral on the basis of results of radiographic and endoscopic examination and histologic evaluation of biopsy samples. A percutaneous endoscopically placed gastrostomy (PEG) tube had been inserted 2 weeks prior to referral, and the dog was being treated for infection at the gas-trostomy site.Clinical Findings—Physical examination findings included marked ptyalism, stertor, and inflammation and discharge at the gastrostomy site. Treatment and Outcome—Surgical options were declined by the owner, and palliative treat-ment was chosen to alleviate clinical signs and facilitate PEG tube removal. With fluoroscopic guidance, a self-expanding metallic stent was placed in the esophageal lumen at the site of obstruction. Botulinum toxin A was injected into the mandibular salivary glands under ultrasonographic guidance as treatment for severe ptyalism. Following discharge, clinical improvement was reported until euthanasia for unrelated disease 12 weeks after stent placement. Necropsy revealed that the stent had not migrated and had remained patent with some tumor ingrowth but no evidence of stricture or obstruction.Clinical Relevance—Esophageal stenting effectively treated obstruction and improved clinical signs and may be beneficial for palliative treatment in other animals with malignant esophageal tumors. Although the degree to which botulinum toxin A injection into salivary glands improved clinical signs could not be determined, it may potentially be useful as ad-junctive treatment to reduce severe ptyalism. (J Am Vet Med Assoc 2012;240:1202–1207)
carcinoma was made on the basis of histologic evaluation of endoscopic biopsy samples.
The dog was discharged from the referring veteri-nary hospital, and the owner administered its total ca-loric energy requirement via the PEG tube. The dieta was blended with 90 to 120 mL of water, and 275 mL of the slurry was administered every 12 hours. Six days after the PEG tube was placed, the dog was evaluated by the refer-ring veterinarian because of purulent discharge around the PEG tube site and hind limb weakness attributed to suspected lumbosacral osteoarthritis. Bacterial culture of samples obtained at the PEG tube insertion site revealed infection with multidrug-resistant Escherichia coli.
At the time of referral, the patient was receiving su-cralfateb (35 mg/kg [16 mg/lb], PO, q 12 h), cyclospo-rine (5.26 mg/kg [2.4 mg/lb], via PEG tube, q 24 h), de-racoxibc (1.75 mg/kg [0.80 mg/lb], via PEG tube, q 24 h), chloramphenicol (3.5 mg/kg [1.59 mg/lb], via PEG tube, q 12 h), tramadold (1.75 mg/kg, via PEG tube, q 12 h), metoclopramidee (0.35 mg/kg [0.16 mg/lb], via PEG tube, q 12 h), levothyroxine (0.007 mg/kg [0.003 mg/lb], via PEG tube, q 12 h), an omega-3 fatty acids supplementf (45.6 mg/kg [20.7 mg/lb], via PEG tube, q 12 h), tacrolimus ointmentg (applied topically to affected skin, q 12 h), and a nutritional supplement containing a
From the Department of Radiation Oncology, Medical Center, School of Medicine, Duke University, Durham, NC 27710 (Hansen); The Ani-mal Medical Center, 510 E 62nd St, New York, NY 10065 (Weisse, Berent); Veterinary Hospital, Faculty of Veterinary Medicine, Univer-sity of Montreal, Montreal, QC H3C 3J7, Canada (Dunn); Matthew J. Ryan Veterinary Hospital, School of Veterinary Medicine, University of Pennsylvania, Philadelphia, PA 19104 (Caceres, Todd); and Veteri-nary Specialty Center of Delaware, 290 Churchmans Rd, New Castle, DE 19720 (Diroff).
Address correspondence to Dr. Hansen ([email protected]).
Abbreviation
PEG Percutaneous endoscopically placed gastrostomy

JAVMA, Vol 240, No. 10, May 15, 2012 Scientific Reports 1203
SM
ALL A
NIM
ALS
microencapsulated form of Enterococcus faecium probiotich (one 30-g packet, via PEG tube, q 24 h in food slurry).
Physical examination findings included marked ptyalism, respiratory stertor suggestive of possible laryn-geal paralysis, and inflammation and discharge at the PEG tube site. Results of a CBC revealed leukocytosis (24,000 WBCs/mL; reference range, 4,500 to 15,000 WBCs/mL), neutrophilia with no band cells (20,880 neutrophils/mL; reference range, 2,060 to 10,600 neutrophils/mL), mono-cytosis (1,200 monocytes/mL; reference range, 0 to 840 monocytes/mL), thrombocytosis (454,000 platelets/mL; reference range, 170,000 to 400,000 platelets/mL), and PCV of 39.6% (reference range, 36% to 60%). Results of serum biochemical analysis revealed a high BUN concen-tration (47 mg/dL; reference range, 6 to 25 mg/dL), hyper-kalemia (5.8 mEq/L; reference range, 3.6 to 5.5 mEq/L), hyperchloremia (122 mEq/L; reference range, 102 to 120 mEq/L), high BUN-to-creatinine concentration ratio (47; reference range, 4 to 27), and a low-normal thyroxine concentration (1.3 mg/dL; reference range, 1.0 to 4.0 mg/dL). Remaining values were within anticipated limits (to-tal protein concentration, 6.0 g/dL [reference range, 5.0 to
7.4 g/dL]; creatinine concentration, 1.0 mg/dL [reference range, 0.5 to 1.6 mg/dL]).
Surgical excision of the mass with esophageal re-section and anastomosis was discussed with the owner but was declined. To help alleviate persistent clinical
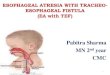
Figure 1—Lateral fluoroscopic views of the thorax of an 11-year-old Collie with squamous cell carcinoma causing esophageal ob-struction. A—A hydrophilic guidewire (arrows) is advanced past the obstructive tumor (asterisk) to facilitate placement of a pig-tail marker catheter and esophageal stent. B—A pigtail marker catheter (arrows) is positioned across the obstructed region. C—Contrast agent injected through the marker catheter reveals the extent of the obstructive lesion. Notice the borders of contrast agent within the air-filled esophagus (arrows).
Figure 2—Lateral fluoroscopic views of the thorax of the same dog in Figure 1 undergoing placement of a self-expanding me-tallic stent. A—The stent delivery system (black arrows) is posi-tioned across the malignant esophageal obstruction. B—Partial deployment of the stent (white arrows) at the aboral aspect of the obstruction is shown; part of the stent remains within the delivery system (black arrows). C—With the stent fully deployed (white arrows), an hourglass shape is evident, with narrowing in the region of the obstruction. D—Contrast agent injected via a pigtail marker catheter immediately following stent deployment reveals restored esophageal patency.

1204 Scientific Reports JAVMA, Vol 240, No. 10, May 15, 2012
SM
ALL
AN
IMA
LS
signs (inability to swallow food and wa-ter, respiratory signs attributed to re-current aspiration of saliva, and severe ptyalism) as well as to facilitate removal of the PEG tube associated with local infection, placement of an esophageal stent was offered. Adjunctive injection of botulinum toxin A into the mandibular salivary glands was also offered to help reduce ptyalism.
The dog was premedicated with methadonei (0.3 mg/kg [0.14 mg/lb], IV) and midazolamj (0.06 mg/kg [0.03 mg/lb], IV). A complete laryngeal examina-tion revealed substantially reduced bilat-eral arytenoid cartilage abduction during inspiration, confirming the suspected la-ryngeal paralysis. The dog was intubated, and general anesthesia was maintained with isoflurane in oxygen. Propofolk (5 mg/kg [2.27 mg/lb]) was given via IV bolus administration 3 times during im-aging procedures. The dog was placed in left lateral recumbency for the stenting procedure, which was performed with fluoroscopic guidance. A combination 5F pigtail marker catheterl and 0.035-inch angled hydrophilic guidewirem were ad-vanced across the malignant obstruction, the wire was removed, and approximately 10 mL of a 1:1 mixture of iohexol and saline (0.9% NaCl) solution was injected through the catheter to define the borders of the esophageal tumor (Figure 1). The esophagus was insufflated with air to help determine diameter of the stent to be used. The marker catheter was removed over a wire and replaced with a 22 X 70-mm, stainless steel mesh, self-expanding metallic stent delivery system.n The stent was advanced until it extended past the ma-lignant obstruction in oral and aboral directions and was deployed (Figure 2). Positive-contrast esophagography was repeated to document patency. Esophagoscopy was also performed to confirm stent position and patency. Botulinum toxin Ao was then injected once into each mandibular salivary gland under ultrasonographic guid-ance at a dose of 30 U/gland. The dog recovered well from anesthesia; total procedural time was approximate-ly 2 hours and 15 minutes. Immediately following anes-thetic recovery, ptyalism was subjectively determined to be substantially reduced, according to annotations in the patient’s medical record indicating a marked reduction in the frequency of mouth wiping necessary.
The dog was discharged from the hospital the day af-ter the procedure. The previously described medications were continued, and ranitidinep (1.3 mg/kg [0.59 mg/lb], via PEG tube, q 12 h) was additionally prescribed.
At follow-up examination 7 weeks after stent place-ment, the PEG tube was still in place. Fluoroscopy re-vealed that the stent was still in place and the esophageal lumen was patent through the stented region (Figure 3).
According to the owner, a veterinarian, the dog had substantial improvement of clinical signs attribut-able to the esophageal tumor, including regurgitation, dysphagia, and ptyalism, for 12 weeks following stent
placement and was able to consume its total caloric en-ergy requirement for target normal weight as a blended, liquid diet fed in an elevated bowl. Medications were continued via the PEG tube. To continue the feedings, the owner reported it was necessary to further dilute the canned diet slurry during the second month after stent placement. The dog’s body weight increased by 6.3 kg (13.9 lb) during the 12 weeks following stent placement.
The patient was euthanized 12 weeks after stent placement because of unacceptable clinical signs of ve-sicular lupus erythematosus and lumbosacral disease. The patient removed the PEG tube several days prior to euthanasia and the tube was not replaced. Injectable medications were given from that point until euthanasia. At necropsy, the stent was in place with no evidence of migration. Mild tumor ingrowth was detectable within the mesh of the stent, but no overgrowth, obstruction, or stricture was noted at the orad or aborad ends of the stent. A small amount of liquid diet was found within the stent during dissection of the esophagus; however, this was considered a likely postmortem phenomenon. No clinically relevant gross or histopathologic lesions were detected in the mandibular salivary glands.
Discussion
Esophageal cancers comprise < 0.5% of cancers in companion animals. Although uncommon, esophageal sarcomas occurring secondary to Spirocerca lupi infec-tion have been reported in small animals in Africa, Is-rael, and the United States.1 The most common types of esophageal neoplasia include squamous cell carci-noma, leiomyosarcoma, fibrosarcoma, and osteosarco-
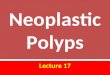
Figure 3—Lateral thoracic radiographic views of the same dog in Figure 1. A—Immediate-ly after stent deployment, some narrowing (arrow) of the stent and the esophageal lumen is evident at the tumor site. B—Seven weeks after stent placement, radial widening of the stented esophageal lumen at the tumor site is apparent (arrow). C—Orally administered contrast agent reveals esophageal patency (white arrow); notice contrast agent within the stomach (St) and persistent esophageal dilation (Eso) cranial to the stent.

JAVMA, Vol 240, No. 10, May 15, 2012 Scientific Reports 1205
SM
ALL A
NIM
ALS
ma; benign tumors can also occur, and paraesophageal tumors can invade the esophagus from the thymus or heart base.1 Tumors are most frequently identified in the middle third of the esophagus, complicating treat-ment options.2
Common clinical signs in affected animals can in-clude dysphagia, regurgitation, and weight loss. Aspira-tion pneumonia can also develop when an obstructive mass affects the ability to swallow food, water, and saliva. Examination of standard radiographic views can reveal gas in the esophagus or esophageal dilatation orad of the mass. Endoscopic examination of the esophagus can be used to identify the mass and to facilitate biopsy proce-dures, and strictures may be detected by use of contrast-enhanced radiography, fluoroscopy, or esophagoscopy.1,2
Prognosis for cure of esophageal cancer in small animals is generally poor, and options for palliation are limited. Esophageal cancers are typically diagnosed at an advanced stage, and ability to perform a complete surgical resection can be limited by poor visibility dur-ing surgery and a need to preserve important adjacent anatomic structures. Other potential complications in-clude tension at the anastomosis site after excision of a mass with extensive esophageal involvement and pos-sible reduced healing potential of the esophagus, com-pared with that of other tissues.1
In a recent study3 of esophageal sarcomas associ-ated with Spirocerca lupi infection, 6 of 17 dogs were treated by means of partial esophagectomy and adjuvant chemotherapy with doxorubicin, resulting in a 267-day median survival time. However, complete resection and anastomosis in 2 dogs resulted in a survival time of < 4 days after admission to the hospital for surgery, and dogs that did not undergo surgery survived between 1 and 60 days after the hospital admission date.3 Chemo-therapy has not been attempted routinely, and traditional radiation treatment is difficult because of the sensitiv-ity of surrounding lung parenchyma and heart, if these are within the radiation field.1 In addition, radiation- induced tumor reduction may take weeks, which can be problematic in patients with complete or nearly com-plete esophageal obstructions. A PEG tube can be used to provide nutritional support, but complications such as peristomal inflammation, infection, and premature tube removal can occur.4
The low likelihood of achieving complete and du-rable remission in small animal patients with esopha-geal cancer has encouraged investigation into palliative treatments. Similar difficulties in treating advanced esophageal cancer in humans that are not considered candidates for surgery have led to evaluation of pallia-tive esophageal stent placement to provide an improved quality of life.5 Dysphagia has a substantial impact on quality of life in patients with esophageal malignancies and, as such, plays a major role in calculating quality-of-life grades in human cancer patients.6
Numerous studies7–12 have clearly demonstrated the safety and efficacy of palliative esophageal stenting for dysphagia caused by intrinsic or extrinsic esopha-geal obstruction in humans. There are several types of stents available for use in the esophagus; however, self-expanding metallic stents have largely replaced the pre-viously used plastic stents, and nitinol products may be
preferred to those made of stainless steel.11 Most com-monly, a mesh self-expanding metallic stent is used.8 Advantages of this type of stent include ease of deploy-ment and flexibility; they can be reconstrained and re-positioned (or removed) prior to complete deployment. These stents are also available in covered (and remov-able) versions designed to reduce tumor ingrowth and seal fistulas, although, not surprisingly, covered stents have been reported to have higher migration rates, compared with noncovered stents.7,12–15 Mesh self- expanding metallic stents can shorten over time as they achieve their ultimate diameter.16 This shortening must be anticipated when choosing an appropriately sized stent. Shortening does not occur with nonmesh laser-cut stents; however, these are more expensive and currently are not routinely available in the lengths and diameters needed for the esophageal applications regardless of pa-tient size.17 Stent length should be sufficient to allow the device to extend 2 cm beyond the oral and aboral tumor margins.16 For midesophageal lesions, eccentric stent placement with greater length beyond the oral aspect of the tumor has been recommended to decrease the risk of migration.7 Standard relative contraindications to esophageal stent placement include inability to place a stent across the full length of the tumor, clinically rel-evant coagulopathy, or tumor location within 2 to 3 cm of the cricopharyngeus muscle (because of difficulty in placing the stent so that it extends beyond the oral as-pect of the tumor).14
Stent placement can be performed with fluoroscop-ic guidance alone, but endoscopy may be considered in more proximal or distal lesions to help avoid stenting of the upper and lower esophageal sphincters, respec-tively. In 1 report,16 procedure times were shorter for fluoroscopically guided stent placement than for endo-scopically guided stent placement. It is unclear whether balloon dilation is necessary after a stent is deployed; the type of stent used in the dog of the present report has been reported to expand slowly over 2 to 14 days following placement11; for this reason, balloon dilation was not performed in this dog.
Generally, antimicrobials are not routinely admin-istered following placement of an esophageal stent, although antacids might be helpful, particularly if the stent crosses the lower esophageal sphincter and reflux is anticipated. Postoperative feeding instructions vary among published reports, but it has been recommended that only liquids are ingested for 24 hours and then the normal diet is resumed.16 Dogs may be encouraged to eat a blended, canned food diet, and warm water can be offered after feedings to help minimize food trap-ping within the stent. Cola beverages have been recom-mended in humans with esophageal stents to help clear food from the stent.13,14
Although reported mortality rates associated with esophageal stent placement in humans are low, com-plication rates of 26% to 52% have been described.18,19 Complications can include tumor ingrowth into the stent mesh, overgrowth or granulation tissue at the stent margins, stent migration (especially with covered stents), bleeding, food bolus impaction, and esophageal injury during stent placement.10,20 Similar complica-tions were not seen in the dog of the present report.

1206 Scientific Reports JAVMA, Vol 240, No. 10, May 15, 2012
SM
ALL
AN
IMA
LS
Although difficult to interpret in dogs, chest pain has also been reported in humans following esophageal stent placement.18 Potential complications should be discussed with owners, and future studies may help to evaluate the relative risks of stent-related complications in dogs.
Successful palliative stenting procedures for malig-nant obstructions involving the respiratory, gastroin-testinal, urogenital, and cardiovascular systems in dogs and cats have been described.21–24 Esophageal stenting for treatment of benign strictures has also been prelimi-narily investigated in dogs; however, stent migration was a commonly reported occurrence. Because stan-dard treatments were declined by the owner of the dog of this report, and considering the reportedly success-ful use of palliative stents in human esophageal can-cer patients with few serious complications,8 palliative esophageal stenting was offered as a potential means of improving quality of life.
It remains unclear whether the severe ptyalism ob-served in the dog of the present report resolved because of stent placement, injections of botulinum toxin Ao into the mandibular salivary glands, or a combination of the 2 treatments. A botulinum toxin A product was experimentally shown to reduce saliva production from the mandibular salivary glands in healthy dogs by up to 40% when injected into the glands at a 30 U/gland dose; the duration of effect was reportedly < 9 months, and few complications were reported.25 Saliva production by untreated salivary glands prevents xerostoma.25 Botuli-num toxin A application to the nasal cavity has also been reported to reduce nasal secretions in dogs with experi-mentally induced rhinorrhea.26 Injections of botulinum toxin A into the salivary glands have been successfully used to treat human patients with ptyalism and chronic aspiration,27–29 and 1 recent report29 described a > 50% reduction in the total number of hospitalizations and presumptive aspiration pneumonias in these patients following treatment with botulinum toxin A injections.29
Potency units are specific for each botulinum toxin A product preparation and should be noted. In the dog of this report, botulinum toxin A injections were adminis-tered under ultrasonographic guidance because this meth-od is typically used in human patients. Potential compli-cations are rare but can include chewing difficulties, dry mouth, dysphagia, facial nerve paralysis, and masseter muscle injections leading to weakened jaw closure.27
Placement of an esophageal stent in the dog of this report resulted in substantial improvement of clinical signs associated with esophageal squamous cell carci-noma. The degree to which intraglandular injections of botulinum toxin A contributed to alleviation of ptyalism could not be determined; however, ptyalism subjectively appeared to be substantially reduced im-mediately following anesthetic recovery, and no adverse effects were reported. Stents may be potentially useful as a palliative treatment for animals with obstructive esophageal malignancies when standard treatment op-tions cannot be pursued.
a. Maximum Calorie, Iams Co, Cincinnati, Ohio.b. Carafate, Aventis, Bridgewater, NJ.c. Deramaxx, Novartis, Basel, Switzerland.d. Tramadol, Ortho-McNeil, Raritan, NJ.
e. Reglan, Wyeth-Ayerst, Madison, NJ.f. Welactin, Nutramax Laboratories, Edgewood, Md.g. Protopic, Astellas, Tokyo, Japan.h. Fortiflora, Nestle-Purina, St Louis, Mo.i. Dolophine, Roxane, Columbus, Ohio.j. Versed, Hoffman-La Roche Ltd, Mississauga, ON, Canada.k. Propofol, Abbott Laboratories, Chicago, Ill.l. Marker catheter, Infiniti Medical LLC, Menlo Park, Calif.m. 180-cm 0.035-inch angled Weasel Wire, Infiniti Medical LLC,
Menlo Park, Calif.n. Wallstent, Boston Scientific Corp, Natick, Mass.o. Botox (Botulinum Toxin A), Allergan, Irvine, Calif.p. Zantac, GlaxoSmithKline, Research Triangle Park, NC.
References1. Withrow SJ. Tumors of the gastrointestinal tract. In: Withrow SJ,
Vail DM, eds. Small animal clinical oncology. 4th ed. Edinburgh: Saunders, 2007;477–479.
2. Head KW, Else RW, Dubielzig RR. Tumors of the esophagus and esophageal region of the stomach. In: Meuten, DJ, ed. Tumors in domestic animals. 4th ed. Ames, Iowa: Blackwell Publishing, 2002;439–441.
3. Ranen E, Lavy E, Aizenberg I, et al. Spirocercosis-associated esophageal sarcomas in dogs. A retrospective study of 17 cases (1997–2003). Vet Parasitol 2004;199:209–221.
4. Salinardi BJ, Harkin KR, Bulmer BJ, et al. Comparison of complica-tions of percutaneous endoscopic versus surgically placed gastrostomy tubes in 42 dogs and 52 cats. J Am Anim Hosp Assoc 2006;42:51–56.
5. Schrump D, Altorki N, Forastiere A, et al. Cancer of the esopha-gus. In: Devita VT, Hellman S, Rosenberg SA, eds. Cancer: prin-ciples and practice of oncology. 6th ed. Philadelphia: Lippincott-Williams & Wilkins, 2001;1319–1342.
6. Stahl M, Oliviera J. Esophageal cancer: ESMO clinical recom-mendations for diagnosis, treatment and follow-up. Ann Oncol 2008;19(suppl 2):ii21–ii22.
7. Conio M, Repici A, Battaglia G, et al. A randomized prospective comparison of self-expandable plastic stents and partially cov-ered self-expandable metal stents in the palliation of malignant esophageal dysphagia. Am J Gastroenterol 2007;102:2667–2677.
8. Yakoub D, Fahmy R, Athanasiou T, et al. Evidence-based choice of esophageal stent for the palliative management of malignant dysphagia. World J Surg 2008;32:1996–2009.
9. Xinopoulos D, Dimitroulopoulos D, Moschandrea I, et al. Natu-ral course of inoperable esophageal cancer treated with metallic expandable stents: quality of life and cost-effectiveness analysis. J Gastroenterol Hepatol 2004;19:1397–1402.
10. Selinger C, Ellul P, Smith P, et al. Oesophageal stent insertion for palliation of dysphagia in a district general hospital: experience from a case series of 137 patients. Q J Med 2008;101:545–548.
11. Rainer W, Niederle B, Wildling R, et al. Palliative treatment of obstructing esophageal cancer with nitinol stents: value, safety, and long-term results. AJR Am J Roentgenol 1996;66:79–84.
12. Keller R, Flieger D, Fischbach W, et al. Self-expanding metal stents for malignant esophagogastric obstruction: experience with a new design covered nitinol stent. J Gastrointestin Liver Dis 2007;16:239–243.
13. Clark TW, Berry RF, Islam MU, et al. Gastrointestinal obstruction. In: Ray CE, Hicks ME, Patel NH, eds. Interventions in oncology. Fairfax, Va: The Society of Interventional Radiology, 2003;281–286.
14. Cowling MG, Adam A. Gastrointestinal stenting: indications and techniques. In: Brandon JC, Teplick SK, eds. Nonsurgical therapies for the gut and abdominal cavity. New York: Thieme, 2001;35–45.
15. Kim E, Jeon S, Park S, et al. Comparison of double-layered and covered Niti-S stents for palliation of malignant dysphagia. J Gastroenterol Hepatol 2009;24:114–119.
16. Winkelbauer FW, Schofl R, Nierderle B, et al. Palliative treatment of obstructing esophageal cancer with nitinol stents: value, safety, and long-term results. AJR Am J Roentgenol 1996;166:79–84.
17. Costamagna G, Familiari P, Tringali A. Biliary and pancreatic stenting. In: Classen, M, Tytgat G, Lightdale C, eds. Gastroen-terological endoscopy. New York: Thieme, 2010;404–406.
18. Freeman, HJ. Endoscopic stenting—where are we now and where can we go? World J Gastroent 2008;14:3798–3803.

JAVMA, Vol 240, No. 10, May 15, 2012 Scientific Reports 1207
SM
ALL A
NIM
ALS
19. Kim JH, Song HY, Shin JH, et al. Palliative treatment of unresect-able esophagogastric junction tumors: balloon dilation com-bined with chemotherapy and/or radiation therapy and metallic stent placement. J Vasc Interv Radiol 2008;19:912–917.
20. Homs M, Steyerberg E, Kuipers E, et al. Causes and treatment of recurrent dysphagia after self-expanding metal stent placement for palliation of esophageal carcinoma. Endoscopy 2004;36:880–886.
21. Sura PA, Krahwinkel DJ. Self-expanding nitinol stents for the treatment of tracheal collapse in dogs: 12 cases (2001–2004). J Am Vet Med Assoc 2008;232:228–236.
22. Weisse C, Berent A, Todd K, et al. Evaluation of palliative stent-ing for management of malignant urethral obstructions in dogs. J Am Vet Med Assoc 2006;229:226–234.
23. Schlicksup MD, Weisse CW, Berent AC, et al. Use of endovas-cular stents in three dogs with Budd-Chiari syndrome. J Am Vet Med Assoc 2009;235:544–550.
24. Newman RG, Mehler SJ, Kitchell BE, et al. Use of a balloon-
expandable metallic stent to relieve malignant urethral obstruc-tion in a cat. J Am Vet Med Assoc 2009;234:236–239.
25. Shaari CM, Wu BL, Biller HF, et al. Botulinum toxin decreases salivation from canine submandibular glands. Otolaryngol Head Neck Surg 1998;118:452–457.
26. Shaari C, Sanders I, Wu D, et al. Rhinorrhea is decreased in dogs after nasal application of botulinum toxin. Otolaryngol Head Neck Surg 1995;12:566–571.
27. Pena AH, Cahill AM, Gonzalez L, et al. Botulinum toxin A in-jection of salivary glands in children with drooling and chronic aspiration. J Vasc Interv Radiol 2009;20:368–373.
28. Jongerius P, Rotteveel J, Van den Hoogen F, et al. Botulinum toxin A: a new option for treatment of drooling in children with cerebral palsy. Presentation of a case series. Eur J Pediatr 2001;160:509–512.
29. Kalf J, Smit A, Bloem B, et al. Botulinum toxin A for drooling in Parkinson’s disease: a pilot study to compare submandibular to pa-rotid gland injections. Parkinsonism Relat Disord 2007;13:532–534.
From this month’s AJVR
Evaluation of intraocular pressure measurements obtained by use of a rebound tonometer and applanation tonometer in dogs before and after elective phacoemulsificationAmy L. Thompson-Hom and Paul A. Gerding Jr
Objective—To determine whether an applanation tonometer and rebound tonometer can be used to detect similar intraocular pressure (IOP) measurements in eyes of dogs undergoing phacoemulsification.Animals—24 dogs (40 eyes) undergoing elective phacoemulsification.Procedures—IOP measurements were obtained from each eye by use of both the rebound tonom-eter and applanation tonometer. Central corneal thickness was measured by use of an ultrasonic pachymeter 3 hours before surgery and 2 and 24 hours after surgery. Statistical analysis was per-formed by use of paired t tests. Results—Mean ± SD IOP 3 hours before surgery, 2 hours after surgery, and 24 hours after surgery was 11.9 ± 4.7 mm Hg, 15.5 ± 11.7 mm Hg, and 10.9 ± 6.7 mm Hg, respectively, as measured with the rebound tonometer and 12.2 ± 5.3 mm Hg, 15.7 ± 12.5 mm Hg, and 12.4 ± 5.4 mm Hg, respectively, as measured with the applanation tonometer. Measured IOP did not differ significantly between the 2 tonometers 3 hours before surgery and 2 hours after surgery, but measured IOP dif-fered significantly between the tonometers 24 hours after surgery.Conclusions and Clinical Relevance—Use of a rebound tonometer underestimated IOP, relative to results for use of an applanation tonometer, by 1.65 mm Hg in eyes 24 hours after phacoemulsifi-cation. Caution should be used when IOP measurements obtained with a rebound tonometer are in the high part of the reference range, and verification of these values with an applanation tonometer would be advised. (Am J Vet Res 2012;73:709–713)
See the midmonth issues of JAVMA
for the expanded table of contents
for the AJVR or log on to
avmajournals.avma.org for access
to all the abstracts.
May 2012