Embed Size (px)
Citation preview
Urine Alkalinization
Passawat Na Nakorn, MD.
R3 Emergency Medicine
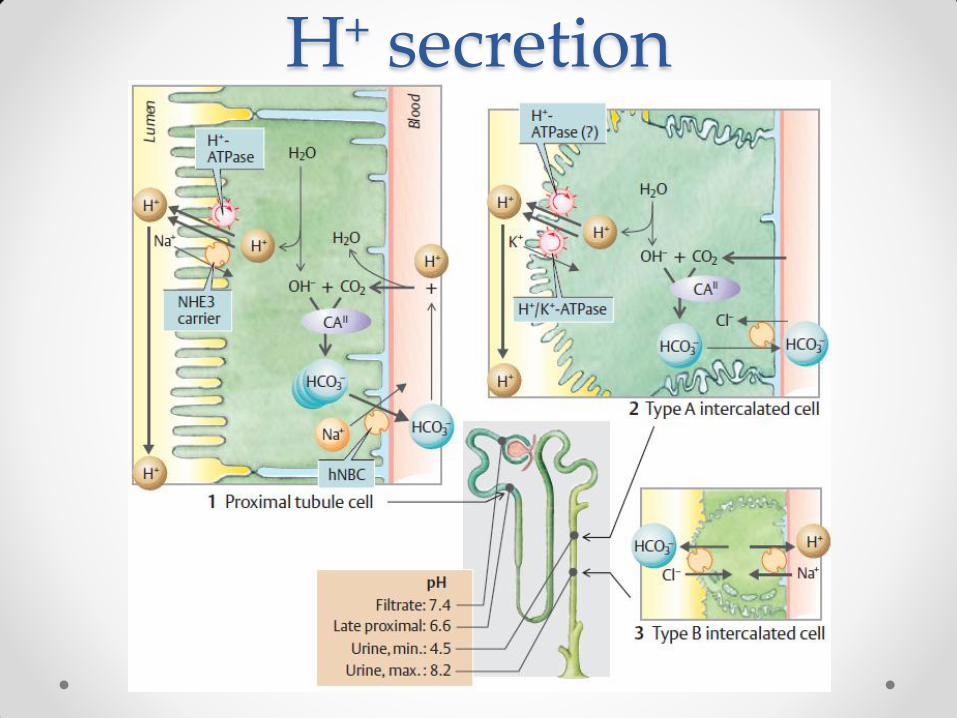
H+ secretion
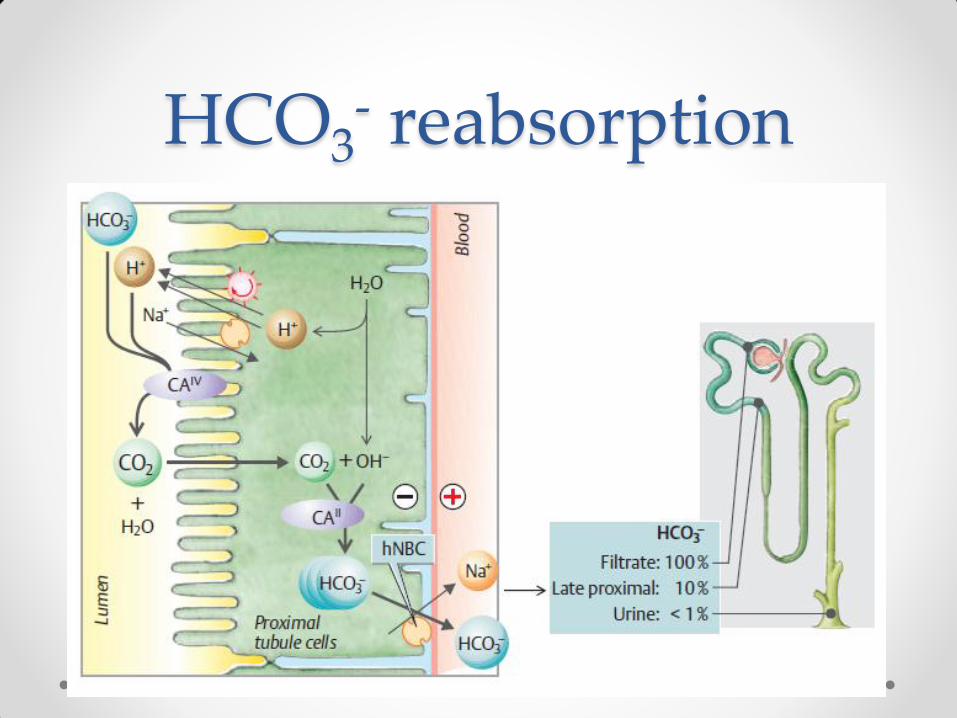
HCO3- reabsorption
Mechanism • Alkalinization of the urine increases urinary excretion
of weak acids different forms of the acid have different lipid solubility
• Alkalinisation - reducing the concentration of free
H+, more the ionised form to maintain an equilibrium less lipid soluble
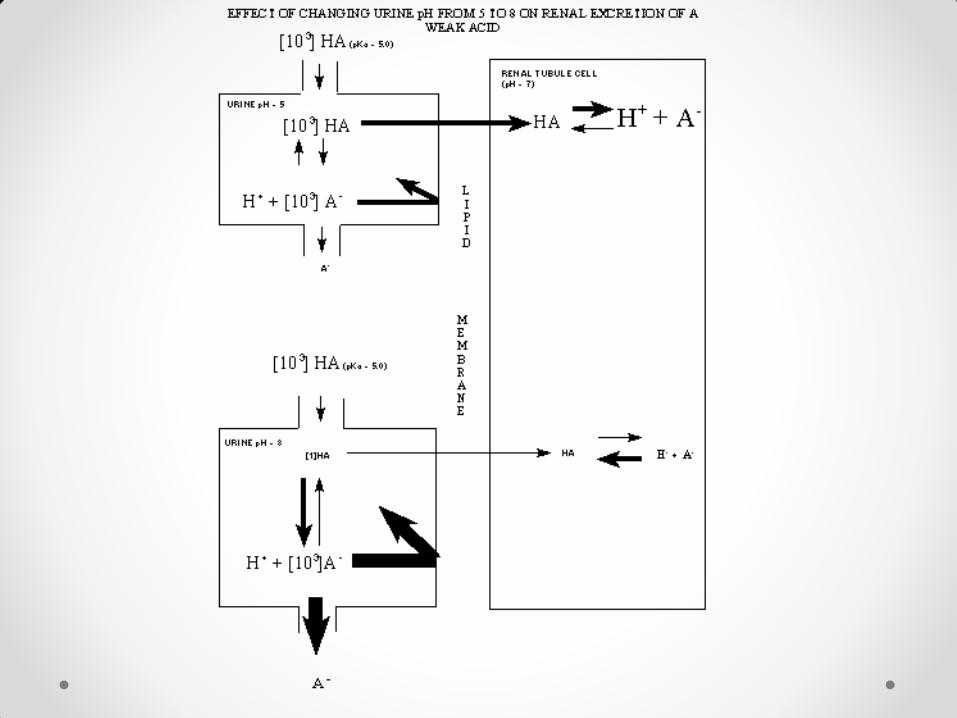
• Ionised form has low lipid and high water solubility 'trapped' in the renal tubules and is excreted in the urine
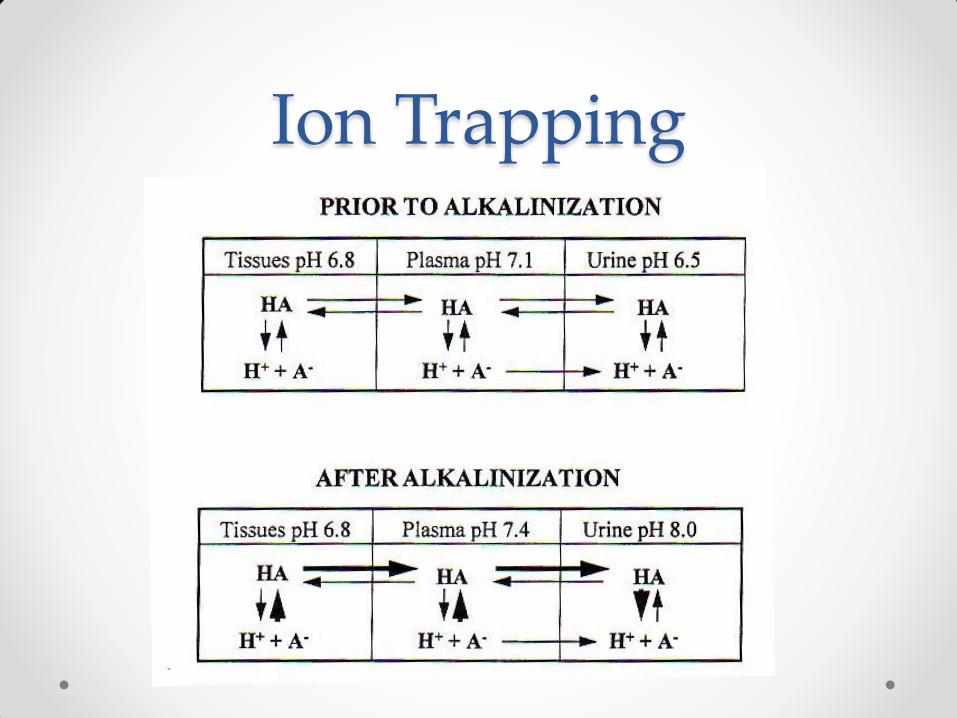
Ion Trapping
Applicable drugs
• Drugs must have the following characteristics for this
process to effectively increase total clearance 1. Weak acid (pKa 3.0 – 7.5)
2. Low protein binding & primarily extracellular fluid
3. Renal excretion is a substantial part of total excretion
4. Clinically significant toxicity
• salicylate, chlorpropamide, phenobarbital, fluoride
chlorphenoxy herbicides, diflunisal, methotrexate
Applicable drugs
• Dimercaprol therapy o Dimercaprol-metal complex dissociates faster in acidic urine
o The released metal can damage the kidney
• Rhabdomyolysis o Alkalinization of the urine has been postulated to minimize the breakdown
of myoglobin into its nephrotoxic metabolites & to reduce crystallization of
uric acid
o Some authorities believe that aggressive hydration sufficiently causes a
solute diuresis that alkalizes the urine
o Evidence for urine alkalinization mostly from animal studies and
retrospective adult studies
Forced Diuresis • Urine volumes of 200 – 300 mL/hour inhibited solute
tubular reabsorption o dilute urine prevented a favorable concentration gradient for passive
reabsorption in the distal tubule
• Increased urine volume through forced diuresis did not significantly enhance drug elimination when combined with urinary alkalinization
• Complication of force diuresis: volume overload, pulmonary edema, cerebral edema, electrolyte disorders

Method (Olson) • 50 – 100 mEq in 1 L of 5% dextrose in 0.25% NSS
or
• 100 – 150 mEq in 1 L of 5% dextrose at 2 – 3 mL/kg/h
(adults: 150 – 200 mL/h)
• Check urine pH and adjust flow rate hourly to
maintain urine pH level at 7 – 8.5 o Keep blood pH < 7.55 and prevent hypernatremia
• Add 20 – 40 mEq of K to each 1 L unless renal failure
Method (Brenner & Rectors)
• 50 mEq IV bolus of sodium bicarbonate
follow by
• 100 – 150 mEq in 1 L of 5% dextrose at 250 mL/h o Rate of infusion based on volume status
o Goal of urine output: 2 – 3 mL/kg/h
• Monitored electrolyte and urine pH q2-3h o Target urine pH: 7.5 – 8.5
• Carbonic anhydrase inhibitors not recommended o Systemic metabolic acidosis, hypokalemia
Contraindications
• Significant metabolic or respiratory alkalemia or
hypernatremia
• Severe pulmonary edema associated with volume
overload
• Intolerance to sodium load (renal failure, CHF)
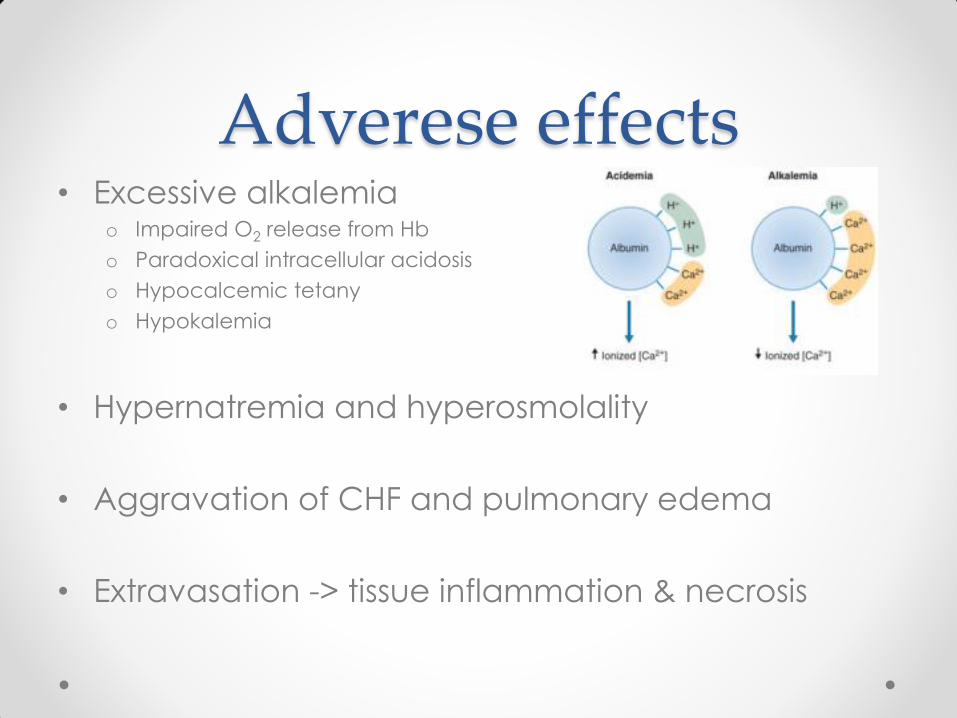
Adverese effects • Excessive alkalemia
o Impaired O2 release from Hb
o Paradoxical intracellular acidosis
o Hypocalcemic tetany
o Hypokalemia
• Hypernatremia and hyperosmolality
• Aggravation of CHF and pulmonary edema
• Extravasation -> tissue inflammation & necrosis
Salicylates
• keeps salicylates away from brain tissue and in the
blood with enhancing urinary excretion
• Raising the urinary pH level from 6.1 to 8.1 results in a
more than 18-fold increase in renal clearance by
preventing non-ionic tubular back-diffusion o decreases the half-life of salicylates from 20-24 hours to less than 8 hours
• Severe cases not meeting criteria for hemodialysis
Phenobarbital
• supportive Rx only is preferred for phenobarbital o shorter half life achieved with alkalinization increases the risk of withdrawal
symptoms
• Multiple dose activated charcoal may be more
effective
Others
• Methotrexate o Consider hemoperfusion instead
• Chlorpropamide o Dextrose infusion alone usually adequate
• 2,4-Dichlorophenoxyacetic o Goal urine pH > 8
o Urine output > 600 mL/h