Embed Size (px)
Citation preview

Urinary diversion and UTI:
Adaptation of epithelial response
Rob Pickard
Professor of Urology
Newcastle [email protected]
My Talk
• Epithelial – Bacterial interactions
– Tolerance versus immune response
• Ileal conduit – a surgically-fashioned
epithelial paradox
• The clinical problem
• The laboratory investigation
• The clinical application
• Summary

Bacteria – Epithelium Interaction
Urinary Tract
Maintain sterility
•Surveillance
•Seek & destroy
•Immune response
•Innate
•Encourages virulence
GI – Tract
Symbiotic relationship
•Control
•Tolerance
•Arm’s length
•Discourage virulence
Ureter
Ileum
Escherichia coli (E. coli)

Bacterial adaption
The changing face of E. coli
• Planktonic– ‘Floaters’ Asymptomatic bacteriuria
(ABU)
• Motile– Flagellin
• Invasive – Uropathogenic E. coli(UPEC)– Adhesion molecules
• Adhesins
• Pili
– Membrane digestion
• Hyalurinidase
Changin
g g
enoty
pe

Urinary surveillance
• Fluid flow – 5 ml/min
• pH < 7
• Antimicrobials– Proteins
• Tamm Horsfall
• Lipocalin
• Lactoferrin
– Peptides• Cathelicidin (LL-37)
• Alpha defensins (HD5)
• Beta defensins (BD1)

Epithelial Response
• Cell surface receptors
– Pathogen Recognition Receptors
• TLRs 4- LPS; 5 - flagellin
• Signal Transduction
– NFκB
– NOD2
• Transcription
• Effectors
– Anti-microbial peptides (AMP)
– Anti-microbial proteins
– Cytokines
Toll - Like receptor 4
Adapter molecules
Intermediaries
NF B
Activation
Cell Nucleus
leading to AMP secretion
Inside
cell
Outside
cell
ABU
UPEC
+Transcription factors gene (DNA) mRNA functional peptide

Ileal conduit – epithelial paradoxJoining the
bacterially–tolerant
ileal mucosa to the
Immune-active ureteric
mucosa
Constant bacterial threat
•Ileum
•Skin
What does the conduit do:
•Seek and destroy?
•Or tolerate?

The Clinical Question
Why do some people with
a urostomy get lots of
urinary infections and
others don’t?

Defining a urinary infection (CDC)
Symptomatic UTI
• Collection of symptoms– ‘Flu-like’ feelings
– Fever
– Rigors
– Loin pain
• > 104/ml of 1 or 2 organisms in catheterised specimen of urine
Asymptomatic bacteriuria
• > 104/ml of 1 or 2 organisms in catheterised specimen of urine
• No symptoms
• May have changes in urine– Cloudy
– Smelly
– Mucus ↑
UTIs – some are worse than
others!
• Simple– Local symptoms
– Get better quickly
– May not need antibiotics
• Fever/shivers– Toxaemia
– Need antibiotics
• Bacteraemia– Need IV antibiotics in
hospital

Symptomatic UTIs – How common
are they in people with urostomy?
•c80% have bacteriuria
•Symptomatic recurrent UTIs are common 20 -30%
•The problem continues over many years

Are recurrent UTIs important?
Antibiotics don’t help much
& cause problems
Loss of functioning renal tissue
Costs: Personal and health care
Miserable

The Paradox
0
25
50
75
100
Bugs
in
urine
% People withurostomy
0
25
50
75
100
Infection
% People withurostomy
Is it the person or the bug?

What may keep bacteria at bay?
Anti-microbial peptides (AMPs)
• Small protein molecules (15 – 30 ααs)– Highly conserved
– Made by epithelia
• Constitutively
• Induced
– Bacteriocidal
• +ve charged segment – hydrophilic
• Non-charged segment – lipophilic
– defensins
– defensins
– Cathelicidin

Our Research 8/07 – 12/09
Aims
1. Are the AMPs present
and active in ileal
conduits?
2. Do people with
urostomies who get
recurrent symptomatic
UTIs have reduced
amounts or activity of
AMPs?
1. 10 People undergoing
ileal conduit surgery
2. 20 people with a conduit
and no infections
3. 20 people with a conduit
and > 2 UTIs per year
Stoma clinic Freeman Hospital FMS Newcastle University
Participants
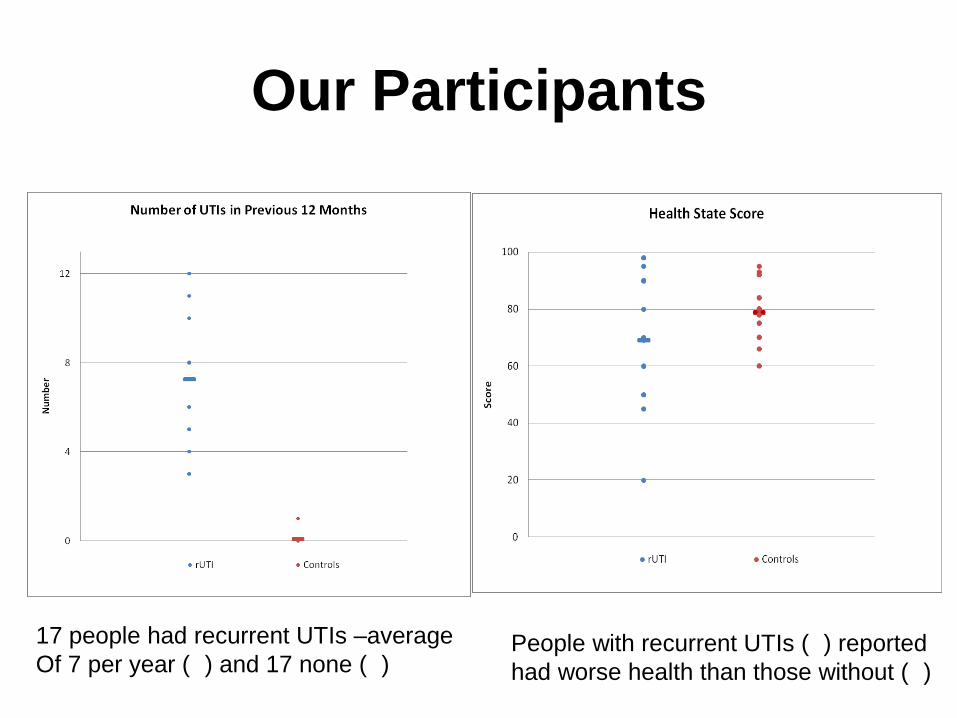
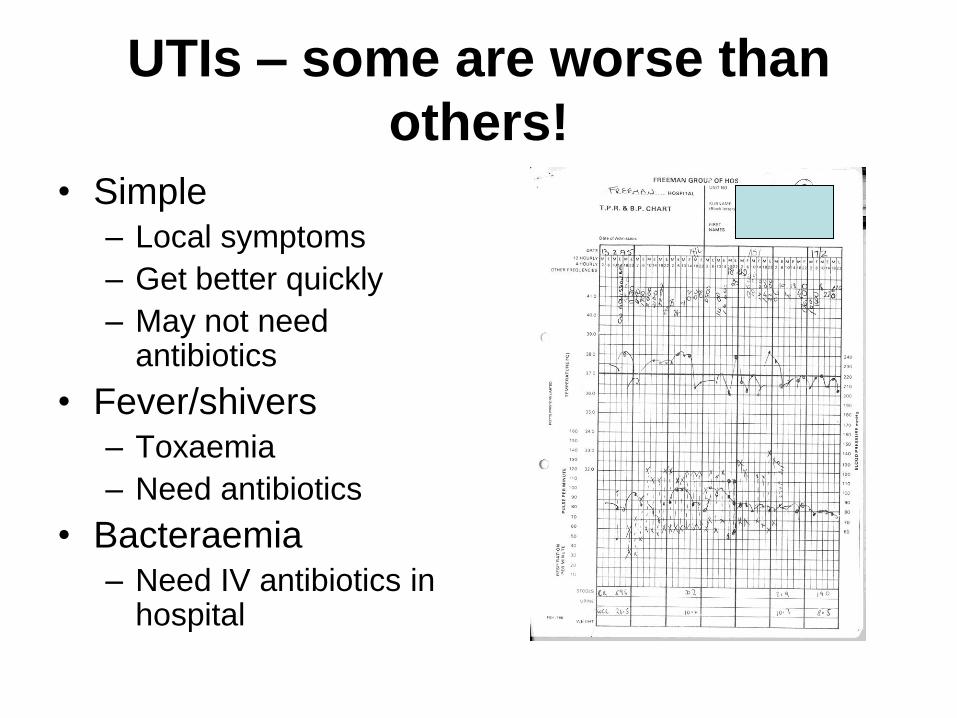
Our Participants
17 people had recurrent UTIs –average
Of 7 per year ( ) and 17 none ( )People with recurrent UTIs ( ) reported
had worse health than those without ( )

1. Results – id of AMPs
RNA level
Protein level
HD5 - ileum BD1 - ureter HD5 - ureter
Ileum
Ureter*
*
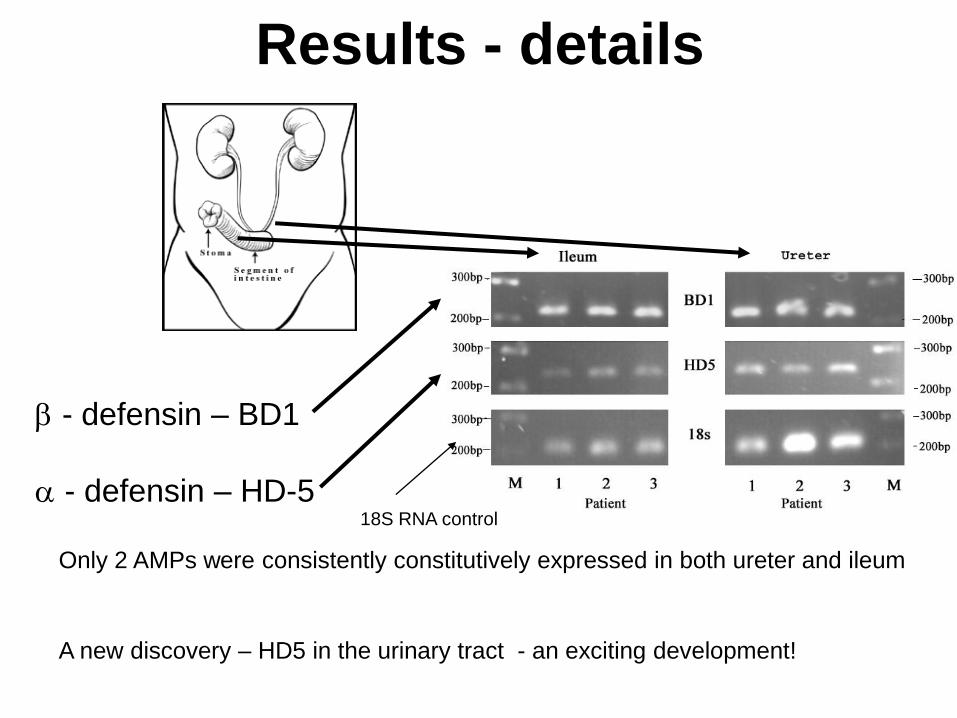
Results - details
- defensin – BD1
- defensin – HD-5
A new discovery – HD5 in the urinary tract - an exciting development!
Only 2 AMPs were consistently constitutively expressed in both ureter and ileum
18S RNA control
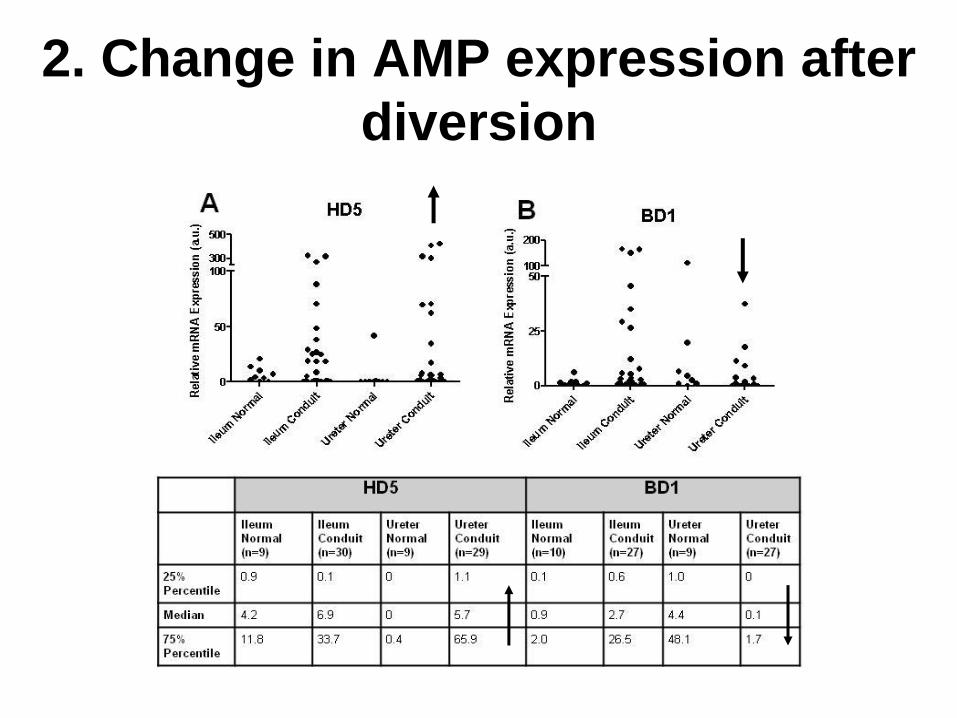
2. Change in AMP expression after
diversion

3. rUTIs versus asymptomatic A. No difference in urinary activity against
standard organism.
B. Organisms isolated from
rUTI more virulent
C. High urinary activity against infecting
organism in rUTI group
D. High urinary activity in rUTI group
against highly virulent UPEC strain

Our Conclusions• Asymptomatic patients
– Adaptation of ureteral urothelium to a bacteria-tolerant phenotype
– Tolerance of bacterial colonization
– No evolutionary pressure towards virulent bacterial phenotype
• Patients with recurrent symptomatic UTIs– Maintenance of aggressive antimicrobial response typical of the normal
urinary tract
– In response evolution of pathogens toward virulent phenotype
– Temporary clearance of pathogen at expense of infective symptoms
• Key role for HD-5?– Expression increased significantly in ureter after diversion
– Trend toward greater ileal and ureteral HD-5 expression in rUTI group
• Next steps– Comparative longitudinal analysis of HD-5 urinary content
– Related to phase of infection – clearance – re-infection
– Define therapeutic potential
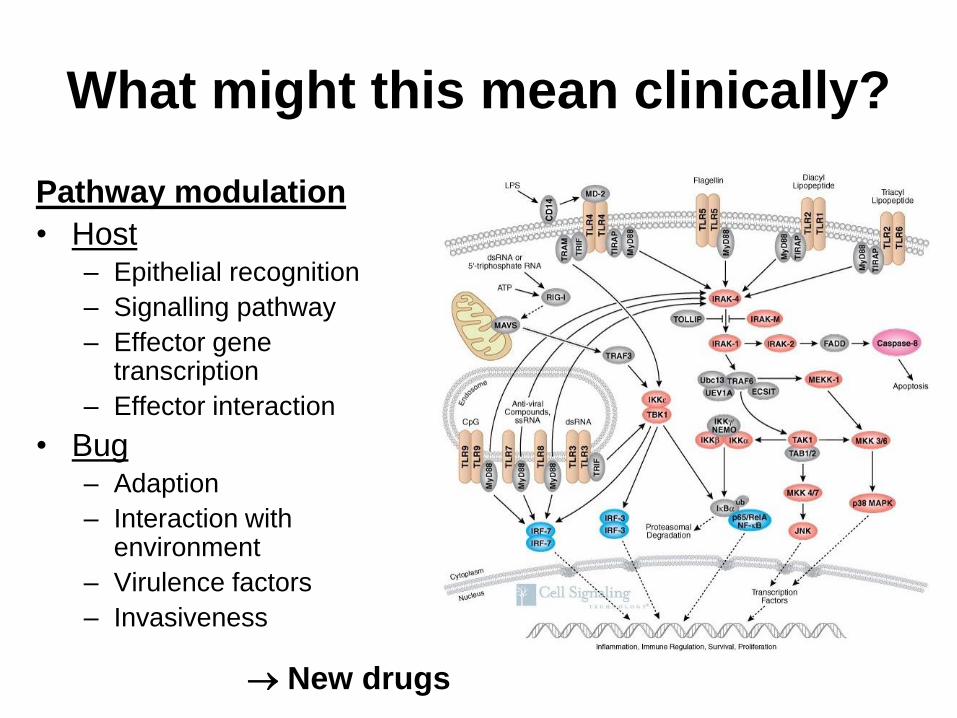
What might this mean clinically?
Pathway modulation
• Host– Epithelial recognition
– Signalling pathway
– Effector gene transcription
– Effector interaction
• Bug– Adaption
– Interaction with environment
– Virulence factors
– Invasiveness
New drugs

Needed because of ↑ antibiotic resistance
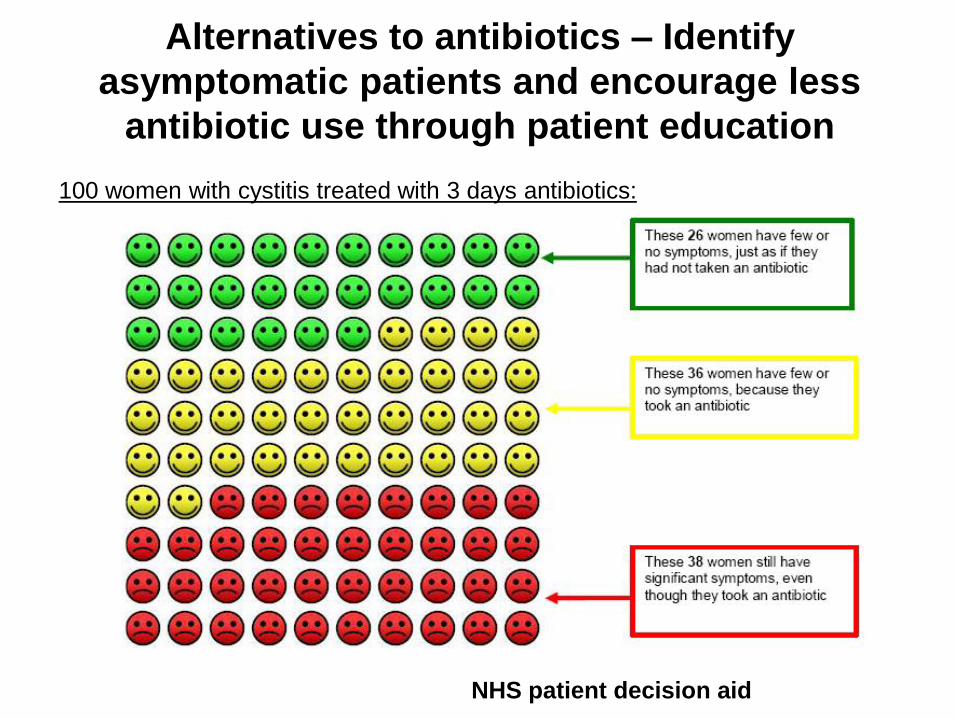
Alternatives to antibiotics – Identify
asymptomatic patients and encourage less
antibiotic use through patient education
100 women with cystitis treated with 3 days antibiotics:
NHS patient decision aid

Current alternatives
• High fluid intake
• Analgesia
• Urinary alkalinising agents x/
• Cranberry preparations x/
• Methenamine x/
• Pro-biotics x/
http://www.cks.nhs.uk/
Need more - urgently
Summary
• We know more about the bugs– Changing
phenotype/adaptatability
• We know more about the host– Defences
– Tolerance vs Response
• Need to put it together– New treatments strategies
– Stratify risk
• Induce tolerance
• Induce/enhance response

Acknowledgements
The workers
• Dr Judith Hall
• Dr Claire Townes
• Ased Ali
• Marcelo Lanz
+
• Wendy Robson
• Marian Haskin/Liz Davis/Helen Lake
• Kieran O’Toole
• Natasha Rigas
• Craig Robson
+
• The participants and urine collectors
Funding

Any Questions?
Read more!?
• Ali et al J Urol 2009: 182; 21-28
• Townes et al Urology 2010: In press
• http://www.uroweb.org/fileadmin/EAUN/guidelines/EAUN_IU_Guidelines_EN_2009_LR.pdf
• Sivick KE and Mobley HLT. Waging War against Uropathogenic Escherichia coli: Winning Back the Urinary Tract. INFECTION AND IMMUNITY 2010; 78:568–585
• Weichhart et al. Current concepts of molecular defence mechanisms operative during urinary tract infection. Eur J Clin Invest 2008; 38 (S2): 29–38