Embed Size (px)
Citation preview

Upper Airway Obstruction: Infectious Cases
By Michelle D. Stevenson, MD, and Javier A. Gonzalez del Rey, MD, FAAP
CINCINNATI, OHIO
O NE OF THE MOST CHALLENGING ASPECTS of pediatric emergency medicine is the evaluation of the child with stridor and partial airway obstruction. Although viral etiologies are most common, clinicians must know how to recognize respi-
ratory emergencies through history and physical examination, un- derstand when to request subspecialty consultation, and be able to choose appropriate diagnostic and therapeutic interventions. The following cases will review the current management of several com- mon pediatric upper airway respiratory emergencies.
Case l
A 2-year-old African American female known to have asthma was admitted in July 2001. Her chief complaint was trouble breathing. Her mother reported a 4-day history of dry cough, wheezing, and labored breathing. She had been seen in the emergency department (ED) 24 hours before this evaluation and was discharged with a diagnosis of an asthma exacerbation. Despite nebulized albuterol every 4 hours at home, the mother reported worsening work of breathing, the new onset of fever to 38.9~ a hoarse voice, and drooling. Past medical history was significant for 5 ED visits per year for asthma without hospitalization. Current medica- tions included albuterol, prednisolone, inhaled fluticasone, and diphenhydramine.
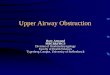
Physical examination on her re turn visit revealed a temper- ature of 37.7~ a heart rate of 138 beats/min, a respiratory rate of 44, and an oxygen saturation of 97% on room air. The child's positioning is shown in Figure 1. She remained in a tripod position in moderate respiratory distress, with a hoarse
INFECTIOUS CASES OF UAO / STEVENSON AND GONZALEZ DEL REY 163

1 6 4 INFECTIOUS CASES OF UAO / STEVENSON AND GONZALEZ DEL REY
Figure I. Case I--Patient's position.
voice and ill appearance. Her mucous membranes were moist. Her neck was supple with mild lymphad- enopathy. Lung examination revealed audible in- spiratory stridor at rest and deereased breath sounds bilaterally without audible wheezes. Nasal flaring and supraclavicular retractions were present. The remainder of her physical examination was normal.
Partial upper airway obstruetion was sus- pected. Beeause of the uneer ta inty regarding her diagnosis, it was unelear if the patient was suffer- ing from epiglottitis or severe eroup. Therefore, a trial of raeemie epinephrine was given, immedi- ate consultation with an otolaryngologist was un- dertaken, and upper airway films were obtained (Fig 2). Because of these results, she was taken to the operating room where the diagnosis of epi- glottitis was confirmed (Fig 3). A complete blood count obtained after intubation showed a white blood cell count of 15,000 with 66% neutrophils, 5% bands, and 17% lymphoeytes. Her blood cul- ture was negative. Both a throat eulture and a traeheal aspirate obtained immediately after in- tubation grew many J3-hemolytic group A strep- tococcus and oropharyngeal flora. Ampieillin- sulbactam was administered intravenously until discharge. She remained intubated for 3 days and was diseharged without significant complieations on the fifth hospital day. She completed a 10-day eourse of antibiotics with amoxicillin-elavulinic acid.
Discussion
Clinical P r e s e n t a t i o n and E p i d e m i o l o g y
Epiglottitis has been described in all age groups from neonates to adults. 1,2 Historieally, pediatric patients have presented most often between the ages of 2 and 6 years. In a recent series by Gonzalez et al, 3 children with epiglottitis were noted to have acute onset of a febrile illness characterized by respiratory distress (43%), fever and sore throat (68%), which rapidly progressed to stridor (68%), drooling (68%), and dysphagia (43%). Affected chil- dren may be irritable and often prefer to sit upright, with the chin thrust forward and mouth open for airway maintenance (tripod position).
Before the routine use of the conjugate Hae- mophilus influenzae type b (HIB) vaccine, this or- ganism aecounted for the vast majority of pediatric eases of epiglottitis. This life-threatening illness can progress to respiratory arrest and death and may be assoeiated with pneumonia, otitis media, meningi- tis, and soft tissue infeetions. 4
Since 1990, multiple studies worldwide have shown a marked decrease to near eradication of all
Figure 2. Case 2--Lateral airway radiograph showing markedly thickened epiglottis.

INFECTIOUS CASES OF UAO / STEVENSON AND GONZALEZ DEL REY | 6 S
Figure 3. Case I--Intraoperative photograph of epiglottis.
types of HIB disease, including epiglottitis. 3-s How- ever, other bacterial pathogens can cause epiglotti- tis including group A and B Streptococci, Staphylococcus aureus, Neisseria meningitides, KlebsieUa pneumoniae, and Pseudomonas aerogi- nosa. 1,2,9-11 Candida, viruses, and noninfectious causes such as corrosive ingestions, burns, and trauma have also been reported.3,12-14
In a report by Goreliek and Baker, 7 isolates of group A/3-hemolytic streptococcus were recovered from the surface of the epiglottis in 3 of 8 children with epiglottitis. Only 25 % of inpatient eases be- tween 1990 and 1992 were ultimately eaused by HIB. The average patient age also increased from 35 to 80 months in comparison to the prevaeeination group. 7 Other ease reports of group A streptococ- cus supraglottitis indicate a variable course of ill- ness, an older age at presentation, and negative blood cultures.9,15
Diagnosis and M a n a g e m e n t
Epiglottitis is also known as supraglottitis be- cause of the frequent involvement of supraglottie structures. This illness should be suspeeted in a ehild or adult of any age with the presenee of fever, stridor, drooling, dysphonia, dysphagia, and respi- ratory distress. Most patients appear toxic and may
position their airway in the sniffing position: neck flexed distally and extended proximally. Most pedi- atric institutions have developed a multidisci- plinary protocol approach to children with elinieal signs and symptoms of epiglottitis. These team members often include ED personnel, a respiratory therapist, an anesthesiologist, and either an oto- largyngologist or a general surgeon. Immediate ini- tiation of this protocol is advised in any child with a potential critical airway. This is especially impor- tant when the child maintains the positioning, drooling, or respiratory distress suggestive of epi- glottitis. Goals of the team approaeh include imme- diate availability of the physicians most skilled in maintaining a position of comfort for the child and minimization of testing before securing a safe air- way. 16 These goals should be implemented in any institution when epiglottitis or critical airway ob- struetion is suspected.
In the study by Gonzalez et al, 3 pharyngitis and croup were the most common initial diagnoses in misdiagnosed eases (20%) of epiglottitis. Clinieians should therefore maintain a high index of suspicion when ehildren present with atypical features of these illnesses. Although not entirely predictive, absence of cough and the presence of drooling and agitation are seen more often in epiglottitis than croup.17
Airway films are usually not needed unless the diagnosis is in doubt and unless there is no im- mediate airway compromise. When obtained, a thiekening of the epiglottis on lateral view, or the " thumbprint sign" (Fig 2) is commonly seen. A eommon abnormality in milder eases or in adults with epiglottitis is thickening of the aryepiglottic folds. The subglottic struetures typically appear normal, is The patient with epiglottitis should be allowed to remain in the position of maximal eomfort, with minimization of examination and testing in order to avoid airway compromise. Di- rect laryngoseopy in the operating room should be under taken as soon as possible. This test should be performed under the supervision of a physician with advanced skills in pediatrie airway management, including the ability to create an emergeney surgieal airway. Nasotraeheal intuba- tion is the preferred method of t rea tment in ehil- dren until edema of the epiglottis regresses, usually from 24 to 72 hours. 19 Antibiotics should include a broad spectrum eephalosporin such as eefotaxime or eeftriaxone. Blood and epiglottis surface eultures may be obtained intraopera- tively.

166 INFECTIOUS CASES OF UAO / STEVENSON AND GONZALEZ DEL REY
Case 2
An 8-year-old caucasian male presented to the ED in December with a 24-hour history of rhinor- rhea, sore throat, hoarseness, and cough. During the 12 hours before his arrival, his cough had be- come more severe, with reported occasional noisy breathing during inspiration, and a fever of 39.5~ His past medical history was positive only for croup at 2 years of age. His only current medication was aeetaminophen. Further history revealed some dif- ficulty swallowing liquids but no drooling. Both of his parents had been ill the previous week with fever, myalgias, and cough.
A physical examination of his vital signs revealed a temperature of 39.1~ a heart rate of 150, a respiratory rate of 26, a blood pressure of 105/55, and his oxygen saturation was 96% on room air. He appeared ill and had difficulty and pain with speak- ing. There was no stridor, drooling, or favored po- sitioning. He had an occasional bark-like cough and hoarse voice. His tympanic membranes were clear. His oropharynx was moist with symmetric tonsils without exudate or erythema. His neck was supple without lymphadenopathy. Despite mild tachy- pnea, his lungs were clear to auscultation with good air entry and no retractions. The remainder of his physical examination was normal.
Because of his pain while speaking, airway films were obtained in the ED (Fig 4). The films showed subglottic narrowing with intraluminal debris sug- gestive of a membrane. Supraglottic structures ap- peared normal. Because of his clinical appearance and airway films, an otolaryngology consultation was obtained in the ED. Flexible bronchoscopy re- vealed yellow exudate at the vocal cords. The pa- tient was taken to the operating room where rigid bronchoscopy was performed and the trachea was debrided. Partial involvement of the trachea was noted. The patient did not require intubation. In- travenous cefuroxime was administered. The tra- cheal secretions subsequently grew MoraxeUa catarrhalis. After 24 hours of observation in the pediatric intensive care unit and 3 further inpatient hospital days, he was discharged home to complete a 10-day course of oral cefprozil. Nasopharyngeal viral cultures were subsequently positive for influ- enza A.
Discussion
Clinical P resen ta t ion and Epidemio logy
Bacterial traeheitis, or membranous laryngotra- cheobronchitis (MLTB), i s characterized by a bac-
Figure 4. Case 2--Lateral airway radiograph.
terial infection within the tracheal lumen causing progressive upper airway obstruction. Although re- ported much earlier, two descriptive case series appeared in the late 1970s by Jones and Han, spark- ing debate about nomenclature and pathogene- sis. 20,21 Reports of MLTB throughout the last several decades have shown great variability in clinical pre- sentation and epidemiology32
MLTB has been reported in patients ranging from an age of 3 weeks to adults. 21,23 Many researchers have suggested that a relationship exists among a preceding viral infection, epithelial damage, and bacterial superinfection. Viral pathogens include parainfluenza, influenza, respiratory syncytial vi- rus, and measles34-27 It has therefore been argued that a viral prodrome may be seen in most cases. MLTB has also been reported after tonsillectomy and adenoidectomy and as a complication of endo- tracheal intubation. 2s,29
A review of all published cases before 1989 by Gallagher and Myer 22 found a mean age at presen- tation of 4 years with a 2:1 male to female ratio.

iNFECTIOUS CASES OF UAO t STEVENSON AND GONZALEZ DEL REY 1 6 7
Despite the wide variety in symptoms and course, the authors concluded that the diagnosis should be considered in any child who has a fever, cough, and stridor, particularly in the toxic child. 22 A previous historic review of infectious airway disorders by Nelson 3~ recommended that the diagnosis be con- sidered when "an infant or child with acute laryn- gitis is or becomes more seriously ill than is ordinarily expected. ''3o
Recently, a series of 46 children with MLTB from the pediatric intensive care unit at Children's Hos- pital Medical Center in Cincinnati described a mean age of 5.8 years and a mean duration of symptoms of 2.5 days. Most of these children came to the ED between August and December of 1995. Of the 25 viral cultures ordered on those children, 72% were positive for influenza A. 25 In addition, the incidence of toxicity was lower than previously re- ported, with 20% of the nonintubated group and 12% of the intubated group reported as toxic in general appearance. Other atypical factors prompt- ing investigation in this series included high tem- perature (17% ~ 40 ~ C), acute onset or change in symptoms (24%), dysphagia, neck pain, choking, or drooling (19%). 25
Studies of the bacteriology of MLTB have found S. aureus to be the most common pathogen.a1, 22 Numerous other organisms have been recovered from tracheal secretions, including Haemophilus influenzae, Streptococcus pneumoniae, other streptococci, and gram-negative organisms such as P s e u d o m o n a s aer~ginos~.20,21,31, 32 Interestingly, M. catarrhalis was the bacterial pathogen isolated most frequently in the series by Bernstein. 2s Brook 33 demonstrated the presence of anaerobes (21%), mixed anaerobic and aerobic organisms (36%), and polymicrobial flora as potential patho- gens in MLTB.
Diagnosis and M a n a g e m e n t
Although rare and variable in presentation, diag- nosis of MLTB requires a high index of suspicion. As discussed, atypical features of viral laryngotracheo- bronchitis should raise suspicion. In our patient, the child's age (older than typical), ill appearance, and difficulty speaking are unusual symptoms of croup. Signs or symptoms of severe respiratory distress, anxiety in older children, or copious mu- copurulent secretions should also prompt investi- gation. There is a lack of support in the literature for the efficacy of inhaled racemic epinephrine for MLTB, although Gallagher 22 notes that this may temporarily improve symptoms. Viral croup, epi-
glottitis, and foreign body aspiration are common differential diagnoses.
The gold standard for diagnosis remains endos- copy with suctioning, aerobic and anaerobic cul- ture, and debridment. 33,34 The use of flexible bronchoscopy by an otolaryngologist when marked distress is not present has been well described and may reveal mucopurulent secretions coming from the trachea. 22,2s Subsequent rigid endoscopy con- firms debris, membranes, or erosions involving all or part of the trachea. Previously, more than 80% of children required intubation subsequent to endos- copy. 21 However, in the more recent Bernstein 25 series, 43% of children were managed without en- dotraeheal intubation. By comparison, the non-in- tubated children were older and had a shorter hospital stay.
Adjunctive studies such as white blood cell count are as variable as clinical presentation and of little diagnostic value in MLTB. 22,34 Blood cultures are rarely positive. Antibiotics should be tailored to intraoperative gram stain results. Initial choices may include a eephalosporin such as eefuroxime with additional anaerobic coverage as indicated by culture and sensitivity. 33
Although controversial, airway radiographs may be useful in evaluating the patient with clinically atypical stridor. Several studies have found a low correlation between radiographs and endoscopy findings. 2~ A more recent retrospective review by Walner et a135 analyzed radiographs in all causes of pediatric upper airway obstruction. While specific- ity for all airway diseases was lower overall, airway films were 100% sensitive and 97% predictive for the 32 eases of MLTB. Radiographs included both an- teroposterior and lateral views and showed linear airway filling defects, membranes, plaques or asym- metric subglottie narrowing. Of note, the Walner study was completed with a trained pediatric radi- ologist interpreting the films. The Bernstein 25 series showed that 82% of patients with MLTB had similar positive radiographic findings.
Significant complications reported with MLTB include associated pulmonary infiltrates, respira- tory arrest (11%), toxic shock syndrome, pulmo- nary edema, adult respiratory distress syndrome, subglottic stenosis, and death (3.7%). 22,26,31,37 No deaths occurred in the Bernstein series. 25
Case 3
An ll-month-old caucasian male infant was ad- mitted in July with a 3-day history of irritability, decreased feeding, a fever as high as 39.3~ and

168 INFECTIOUS CASES OF UAO / STEVENSON AND GONZALEZ DEL REY
noisy breathing. During the preceding 24 hours, his mothe r had noticed that the child was tilting his head to the left. She also repor ted an increase in noisy breathing during a nap that had occurred 3 hours before his arrival. He also exper ienced exces- sive drooling and refused to eat after waking. Past medical history was significant for one episode of otitis media, which was t reated with oral antibiotics 2 months previously. Acetaminophen was the only medicat ion he had taken. Review of systems was positive for purulent rh inorrhea for 1 month. There was no vomiting, diarrhea, cough, ear drainage, or ill contacts.
Physical examination revealed an irritable but con- solable infant in mild respiratory distress. Vital signs showed a temperature of 39.5~ (rectal), a heart rate of 124, a respiratory rate of 54, blood pressure of 88/60, and an oxygen saturation of 98% on room air. The child's physical exam was significant for purulent rhinorrhea, and bilateral erythema of the tympanic membranes with purulent fluid. The child was drool- ing profusely and the posterior pharynx was difficult to see. Stridor was exacerbated during attempts at examination of the oropharynx. The patient preferred to hold his head tilted to the left and cried with movement or examination of his neck. There were multiple anterior cervical lymph nodes 1 to 2 cm in size, more prominent and tender on the left. There was mild tachypnea with nasal flaring and subcostal retractions. Lungs were clear to auscultation. Cardio- vascular examination showed tachycardia without murmur. The remainder of the physical examination was normal.
Because of the presence of drooling and the re- fusal of any oral intake, the pat ient had airway films and a chest radiograph. The radiograph was without pu lmonary infiltrate. Airway films revealed a signif- icant widening of the prevertebral soft tissues (Fig 5). Complete blood count, blood cultures, and an otolaryngology consultat ion were obtained. The pe- ripheral white blood cell count was 25,400 with 13% bands, 64 % neutrophils , 19% lymphoeytes , 3% monoeytes , and 1% eosinophils. The remainder of the hemogram was normal. Based on the child's airway films, computed tomography of the neck was obtained. A 2 x 3 em mass was noted in the retro- pharyngeal space, originating from the left side of the poster ior pharynx (Fig 6).
Because of his age and respiratory status, he was taken to the operating room where 10 mL of puru- lent material was drained from his retropharyngeal space. Ampicillin-sulbactam was adminis tered in- travenously. Gram stain of the aspirate showed gram-positive cocci in pairs and subsequently grew a-hemolytic streptococcus. After 1 night of obser-
Figure 5. Case 3--Lateral airway radiograph.
vation in the intensive care unit, he cont inued hos- pitalization until the fifth hospital day when he was discharged to complete a 10-day course of amoxi- cillin-clavulinic acid.
Discussion
Cl in ica l P r e s e n t a t i o n a n d E p i d e m i o l o g y
Retropharyngeal abscess (RPA), although un- common, is an impor tant diagnosis to consider in the differential diagnosis of an infant with respira- tory distress and stridor. 38 Like epiglottitis, retro- pharyngeal cellulitis/abscess may also present from the neonatal period into adulthood. Up to 71% of neonates and younger infants may present with respiratory distress or stridor. 39 In the 3 rare neo- natal cases repor ted by Coulthard and Isaacs, 4~ all were afebrile and had significant respiratory dis- tress. Traumatic intubation and congenital neck

INFECTIOUS CASES OF UAO ! STEVENSON AND GONZALEZ DEL REY 16g
Figure 6. Case 3--Cornputed tomography of the neck.
abnormalities, such as third branchial cleft anom- alies, are proposed eauses of neonatal e a s e s . 4~
As children age, symptoms become more local- izable and are often deteeted sooner. Despite this, the mean duration of illness to diagnosis is 5 to 6 d a y s . 39,42 Thompson et a142 reported that 50% of cases occur under the age of 3, and 71% occurred in children under 6 years of age. A recent review by Lee et a143 dubbed it the "epiglottitis of the new millennium" because of the associated symptoms including fever (77%), sore throat (46%), dysphagia and/or decreased oral intake (35-69%), and neck pain or stiffness (35-42%). The median age reported in the 26 patient series was 3.5 years. Other signs included tortieollis (35%), drooling (35%), asymme- try in the oropharynx (46%), and neck mass (58%).
These symptoms are caused by the anatomic position of the retropharyngeal space from the skull base to the posterior mediastinum. It is encom- passed by the buecopharyngeal fascia and prever- tebral fascia. Draining the paranasal sinuses, entire pharynx, and middle ear, retropharyngeal lymph
nodes reside within in the retropharyngeal space and are a potential source for infection and abscess formation, especially in young children. 44 An infec- tious etiology with presumed lymphatic extension (eg, otitis media, sinusitis, or pharyngitis), was identified in 71% of eases in a series by Goldenberg et al. 45 However, only 37% of subjects in the Thompson 42 series had a "significant" illness before the onset of RPA. Croup and pharyngitis were the most common. 42 Though it is rare, children may be afebrile on presentation. 42,43,46
Traumatic RPA occurs in children and should be considered in the differential of a febrile child with sore throat and recent penetrating injury of the oropharynx. 39,47,4s Although traumatic RPA caused by foreign bodies or dental procedures is also seen in adults, the cause was idiopathic in 56% of adults in the Goldenberg series. 4s
The bacteriology of RPA has been well studied. A high percentage of patients (41%- 86%) in many series receive oral antibiotics for several days before presen- tation. 42,43,49,5~ Many abscesses are polymierobial. The most common bacteria isolated are alpha-hemo- lytic streptococci, S. aureus, Neisseria sp., and group A streptococcus.42,49,5~ Many anaerobic organisms are also reported, usually in combination with aerobes. 5~ Other gram negatives, S. pneumoniae, and mycobac- teria have also been reported. 43,49-51
Diagnosis a n d M a n a g e m e n t
Febrile ehildren with signs and symptoms of RPA such as torticollis, asymmetry of the posterior oro- pharynx, or neck mass, should undergo evaluation of the retropharyngeal space. Occasionally, a child with RPA will have meningismus as a significant finding along with drooling. When the child's respi- ratory status is not in question and the diagnosis is not clear, airway films may be initially useful. Wholey et a152 and later Barratt et a144 defined the upper limit of normal for the retropharyngeal space to be 7 mm, and found limits of 14 mm in children and 22 mm in adults for the retrotraeheal space. It is necessary to obtain lateral airway films in expi- ration without swallowing and with the neck in extension. If this is not possible and the child is stable, fluoroscopy or eornputed tomography may be a reasonable alternative if RPA is clinically in doubt before proceeding with endoscopy. 53
Because of the process of abscess formation from cellulitis to phelgmon to frank abscess, it is often not possible to distinguish the stage of illness based on airway films or fluoroscopy alone. The presence of abnormal air or an air fluid level on plain films is more suggestive of abscess. 44 The stage of inflam-

170 INFECTIOUS CASES OF UAO / SIEVENSOH AND 60NZALEZ DEL REY
mation may influence the decision of surgical drainage versus medical management. Contrast-en- hanced computed tomography is more helpful in precisely localizing and defining RPA, although the correlation with surgical findings of an abscess re- portedly ranges from 73.5% to 92%. 54,55 Of clinical importance, Stone et a154 reported 5 patients who underwent surgical drainage of significant abscess because of a deteriorating clinical condition, de- spite suggestion of only phlegmon or cellulitis on computed tomography. 54 The diagnosis should therefore be made on the basis of a combination of clinical and radiographic findings.
An increasing number of children have been managed medically despite the presence of a frank abscess. 45,55,56 Broughton 56 reported that 8 of 14 children with RPA but without respiratory distress between 1981 and 1990 were successfully managed with broad-spectrum antibiotics alone. 56 Mean time to clinical improvement was 1.6 days in these pa- tients.
To address some of these controversies, Lalekea and Messner 57 surveyed the membership of the American Society of Pediatric Otolaryngology re- garding diagnosis and management of RPA in chil- dren. The results indicated that 62% of those surveyed routinely obtained airway films. Com- puted tomography was the method of choice for radiographic evaluation for 72% of physicians ver- sus 22% for lateral neck radiographs and 3% for ultrasound. Yet, only 58% of respondents routinely used computed tomography for diagnosis, suggest- ing again that the diagnosis is confirmed on a case- by-case basis. With regards to management, 31% favored a routine trial of antibiotics, and another 31% occasionally instituted a trial of antibiotics. The antibiotic choices of these subspecialists most commonly included clindamycin (32%), ampicillin- sulbactam (17%), a second-generation cephalospo- rin (12%), or a combination of clindamycin plus a second-generation cephalosporin (12%). These an- tibiotic regimens are widely supported in the liter- ature.49,5o,56
When surgieal drainage is deemed necessary, ei- ther intraoral or lateral neck approach may be used. The Lalakea and Messner 57 survey revealed an 83% preference among respondents for the in- traoral approach, with most physicians indicating that external drainage is required in less than 5% of cases. When respiratory compromise is present, endotraeheal intubation is recommended until de- finitive surgical exploration is undertaken. 43 Re- cently, continuous positive airway pressure has been used to support patients with respiratory eom- promise from RPA until drainage. 5s
Other complications include airway obstruction, rupture of the abscess into the pharynx, persistence of the abscess despite drainage, pneumonia, sepsis, mediastinitis, spinal canal abscess and rarely, at- lantoaxial subluxation or vascular complications of the internal jugular vein or carotid ar- tery. 42,43,45,59,60 Early diagnosis and the use of anti- biotics have helped reduce the incidence of these life-threatening complications.
Summary
These eases illustrate the continued need for vigilance for life-threatening upper airway infec- tions in the era of antibiotics and immunizations. Despite the experience with the overwhelming ma- jority of children who present with non life-threat- ening viral respiratory illnesses, bacterial illness that may cause airway or respiratory compromise still exist. Clinicians should proceed with diagnos- tic evaluation of any child with suspected upper airway obstruction, especially in the presence of drooling, abnormal positioning of the airway or head, toxicity, neck mass, or failure of traditional therapy.
Acknowledgment v
We thank Dr. Gary Geis for his identification of case 1 for presentation and discussion.
References
1. Rosenfeld RM, Fletcher MA, Marban SL: Acute epiglottitis in a newborn infant. Pediatr Infect Dis J 11: 594-595, 1992.
2. Young N, Finn A, Powell C: Group B streptococcal epiglottitis. Pediatr Infect Dis J 15:95-96, 1996.
3. Gonzalez Valdepena H, Wald ER, Rose E, et al: Epiglottitis and Haemophilus influenzae immunization: the Pittsburgh experience- A five year review. Pediatrics 96:424-427, 1995.
4. Senior BA, Radkowski D, MacArthur C, et al: Changing patterns in pediatric supraglottitis: A multi- institutional review, 1980 to 1992. Largyngoscope 104: 1314-1322, 1993.
5. Broadhurst LE, Erickson RL, Kelley PW: De- creases in invasive Haemophilus influenzae diseases in US Army children, 1984 through 1991. JAMA 269:227- 231, 1993.
6. Garepenholt O: Epiglottitis in Sweden before and after introduction of vaccination against Haemophilus influenzae type B. Pediatr Infect Dis J 18:490-493, 1999.
7. Gorelick MH, Baker MD: Epiglottitis in chil- dren,1979 through 1992. Effects of Haemophilus influ-

INFECTIOUS CASES OF UAO / STEVENSON AND GONZALEZ DEL REY 171
enzae type B immunization. Arch Pediatr Adolesc Med 148:47-50, 1993.
8. Liptak GS, McConnochie KM, Roghmann K J, et al: Decline of pediatric admissions with Haemophilus influ- enzae type B in New York through 1993: Relation to immunizations. J Pediatr 130:923-930, 1997.
9. Glenn GM, Schofield T, Krober M: Group A strep- tococcal supraglottitis. Clin Pediatr 29:674-676, 1990.
10. Nelson K, Watanakunakorn C, Watkins, DA: Acute epiglottitis due to serogroup Y Neisseria meningitidis in an adult. Clin Infect Dis 23:1192-1193, 1996.
11. Lacroix J, Ahronheim G, Girouard G: Pseudomo- nas aeruginosa supraglottitis in a six-month-old child with severe combined immunodeficiency. Pediatr Infect Dis J 7:739-741, 1988.
12. Parsons DS, Smith RB, Mair EA, et al: Unique case presentations of acute epiglottic swelling and a protocol for acute airway compromise. Laryngoscope 106:1287- 1291, 1996.
13. Lai SH, Wong KS, Liao SL, et al: Non infectious epiglottitis in children: Two case reports. Int J Pediatr Otorhinolaryngol 55:57-60, 2000.
14. Narasimhan N: Acute supraglottitis caused by varicella. Pediatr Infect Dis J 12:619-620, 1993.
15. Wegner JK: Supraglottitis and group A streptococ- cus. Pediatr Infect Dis J 16:1005-1007, 1997.
16. Stroud RH, Friedman NR: An update on inflam- matory disorders of the pediatric airway: Epiglottitis, croup and tracheitis. Am J Otolaryngo122:268-275, 2001.
17. Mauro RD, Poole SR, Lockhart Ctt: Differentiation of epiglottitis from layrngotracheitis in the child with stridor. Am J Dis Child 142:679-682, 1988.
18. Swisehuk LE: Upper airway, nasal passages, si- nuses, and mastoid, in Emergency Radiology of the Acutely Ill or Injured Child (ed 2). Baltimore, MD, Wil- liams and Wilkins, 1986, pp 130-133.
19. Zulliger J J, Schuller DE, Beach TP, et al: Assess- ment of intubation in croup and epiglottitis. Ann Otol Rhinol Laryngol 91:403-406, 1982.
20. Han BK, Dunbar JS, Striker TW: Membranous la- ryngotracheobronchitis (membranous croup). AJR 133: 53-58, 1979.
21. Jones R, Santos JI, Overall JC, Jr: Bacterial tra- eheitis. JAMA 242:721-726, 1979.
22. Gallagher PG, Myer CM III: An approach to the diagnosis and treatment of membranous laryngotraeheo- bronchitis in infants and children. Pediatr Emerg Care 7:337-342, 1991.
23. Johnson IT, Liston SL: Bacterial traeheitis in adults. Arch Otolaryngol 113:204-205, 1987.
24. Alligood GA, Kenny IF: Tracheitis and supraglot- titis associated with Branhamella catarrhalis and respira- tory syncytial virus. Pediatr Infect Dis J 8:190-191, 1989.
25. Bernstein T, Brilli R, Jaeobs B: Is bacterial trache- itis changing? A 14-month experience in a pediatric in- tensive care unit. Clin Infect Dis 27:458-462, 1998.
26. Conley SF, Beste D J, Hoffmann RG: Measles-asso- ciated bacterial tracheitis. Pediatr Infect Dis J 12:414- 415, 1993.
27. Edwards KM, Dundon MC, Altemeier WA: Bacte-
rial tracheitis as a complication of viral croup. Pediatr Infect Dis 2:390-391, 1983.
28. Eid NS, Jones VF: Bacterial tracheitis as a com- plication of tonsillectomy and adenoidectomy. J Pediatr 125:401-402, 1994.
29. Farber HI, Berg RA: Baeterial traeheitis as a com- plication of endotraeheal intubation. Pediatr Pulmonol 11:87-89, 1991.
30. Nelson WE: Bacterial croup: A historical perspec- tive. J Pediatr 105:52-55, 1984.
31. Burns JA, Brown J, Ogle JW: Group A streptococ- cal tracheitis associated with toxic shock syndrome. Pe- diatr Infect Dis J 17:933-935, 1998.
32. Weinstoek A, Amir J, Starussberg R, et al: Bacte- rial traeheitis caused by Pscudomonas aeruginosa. Pe- diatr Infect Dis J 12:965-966, 1993.
33. Brook I: Aerobie and anaerobic microbiology of bacterial tracheitis in children. Pediatr Emerg Care 13: 16-18, 1997.
34. Eckel HE, Widemann B, Damm M, et al: Airway endoseopy in the diagnosis and treatment of bacterial tracheitis in children Int J Pediatr Otorhinolaryngol 27: 147-157, 1993.
35. Walner DL, Ouanounou S, Donnelly LF, et al: Utility of radiographs in the evaluation of pediatric upper airway obstruction. Ann Otol Rhinol Laryngol 108:378- 383, 1999.
36. Britto J, Habibi P, Waiters S, et al: Systemic com- plications assoeiated with bacterial tracheitis. Arch Dis Child 74:249-250, 1996.
37. Horowitz IN: Staphylococcal tracheitis, pneumo- nia and adult respiratory distress syndrome. Pediatr Emerg Care 12:288-290, 1996.
38. Tobaek S, Herr S: Retropharyngeal abscess in a toxic-appearing infant. Pediatr Emerg Care 17:255-257, 2001.
39. Coulthard M, Isaacs D: Retropharyngeal abscess in children. Arch Dis Child 66:1227-1230, 1991.
40. Coulthard M, Isaacs D: Neonatal retropharyngeal abseess. Pediatr Infect Dis J 10:547-549, 1991.
41. Huang RY, Damrose E J, Alavi S, et al: Third branchial eleft anomaly presenting as a retropharyngeal abscess. Int J Pediatr Otorhinolaryngol 54:167-172, 2000.
42. Thompson JW, Cohen SR, Reddix P: Retropharyn- geal abscess in children: A retrospective and historical analysis. Laryngoscope 98:589-592, 1988.
43. Lee SS, Schwartz RH, Bahadori RS: Retropharyn- geal abseess: Epiglottitis of the new millennium. J Pediatr 138:435-437, 2001.
44. Barratt GE, Koopmmann CF, Jr, Coulthard SW: Retropharyngeal abseess--a ten-year experience. Laryn- goscope 94:455-463, 1984.
45. Goldenberg D, Golz A, Joachims HZ: Retropha- ryngeal abscess: A elinical review. J Laryngol Otol 111: 546-550, 1997.
46. De Lorenzo RA, Singer JI, Matre WM: Retropha- ryngeal abscess in an afebrile child. Am J Emerg Med 11:151-154, 1993.
47. Morrison JE, Jr, Pashley NR: Retropharyngeal ab-

172 INFECTIOUS CASES OF UAO / STEVENSON AND GONZALEZ DEL REY
seesses in children: A 10-year review. Pediatr Emerg Care 4:9-11, 1988.
48. Siou G, Yates P: Retropharyngeal abscess as a complication of oropharyngeal trauma in an 18-month- old child. J Laryngol Otol 114:227-228, 2000.
49. Asmar BI: Bacteriology of retropharyngeal ab- scesses in children. Pediatr Infect Dis J 9:595-596, 1990.
50. Brook, I: Microbiology of retropharyngeal ab- scesses in children. Am J Dis Child 141:202-204, 1987.
51. Medina M, Goldfarb J, Traquina D, et al: Cervical adenitis and deep neck infection caused by Streptococ- cus pneumoniae. Pediatr Infect Dis J 16:823-824, 1997.
52. Wholey MH, Bruwer A J, Baker HL: The lateral roentgenogram of the neck. Radiology 71:350-356, 1958.
53. Breehtelsbauer PB, Garetz SL, Gebarski SS, et al: Retropharyngeal abscess: Pitfalls of plain films and com- puted tomography. Am J Otolaryngol 18:258-262, 1997.
54. Stone ME, Walner DL, Koch BL, et al: Correlation between computed tomography and surgical findings in retropharyngeal inflammatory processes in children. Int J Pediatr Otorhinolaryngol 29:121-125, 1999.
55. Wetmore RF, Mahboubi S, Soyupak SK: Com- puted tomography in th.e evaluation of pediatric neck infections. Otolaryngol Head Neck Surg 199:624-627, 1998.
56. Broughton RA: Nonsurgical management of deep neck infections in children. Pediatr Infect Dis J 11:14-18, 1992.
57. Lalakea MI, Messner AH: Retropharyngeal abscess management in children: Current practices. Otolaryngol Head Neck Surg 121:398-405, 1999.
58. Soong W J, Jeng M J, ttwang B: Respiratory support of children with a retropharyngeal abscess with nasal CPAP. Clin Pediatr 40:55-56, 2001.
59. Brookes A, Moriarty A: Pharyngeal abscess pre- senting with upper airway obstruction in atlanto-axial subluxation in a small infant. Anaesthesia 55:469-471, 2000.
60. Conway JH, Nyquist AC, Goldson E: Posterior mediastinal abscess caused by invasive group A Strep- tococcus infection. Pediatr Infect Dis J 15:547-549, 1996.