Embed Size (px)
Citation preview

Updates in HIV/AIDS Treatment- The Good, The Bad and the Ugly
Global Health Mini-UniversityOctober 9, 2009
Dr. Thomas Minior
Dr. Robert Ferris
USAID HIV/AIDS Treatment Advisors

Objectives
Define Antiretroviral (ARV) Treatment and review the different classes therapy
Understand the HIV life cycle and how it lends itself to ARV development
Review some interesting new issues in the field of HIV treatment and understand their potential impact on global HIV programs
Identify challenges in resource poor settings

Outline
HIV Life Cycle Antiretroviral Therapy 3 Hot Topics in HIV Treatment:
Links between HIV and Chronic disease When to Start antiretroviral therapy Treatment as Prevention
3 Important Public Health Implementation Issues: Challenges in Resource-Limited Settings The Treatment Time-Bomb Pediatric Issues

HIV Pathophysiology
The Life cycle of HIVImpact on the Immune
System

Human Immunodeficiency VirusA retrovirus

HIV Virus As a virus, HIV is dependent
on host cell machinery for its replication Needs to package its own enzymes to utilize the host machinery
HIV composition: Glycoprotein Envelope with
key transmembrane proteins: gp41 & gp120.
Largely made from human cell membrane lipoproteins
Viral capsid (inner shell) with p24 protein
RNA Genome (2 copies) Enzymes:
Reverse Transcriptase (2 copies)
Integrase (2 copies) Protease (2 copies)
High resolution light microscopy of HIV



Life cycle

HIV Life Cycle Summary
HIV attaches to & enters the T-Cell HIV Copies itself from RNA to DNA HIV DNA integrates into our genes Our T-Cells mistakenly copy the
virus HIV assembles itself and buds out of
the T-Cells to infect other cells

How HIV causes AIDS HIV virus enters the bloodstream HIV attaches to Host cell
Mediated through gp41, gp120 Host cells are CD4+ lymphocyte cells (T-Cells)
Can also infect other cells (macrophages, dendritic cells, kidney cells, etc.)
T-Cells are part of our immune systems Help facilitate cell-mediated immunity (regulates the
immune response; augments humoral immunity; particularly active againts viruses, fungi & protozoa)
Over time, significant HIV replication leads to CD4+ Cell destruction
This destruction impairs the immune system’s response to other pathogens

Natural History of HIV Infection

OIs, Clinical Staging, and CD4
WHO 1
WHO 2
WHO 3
WHO 4

Opportunistic Infections

Antiretroviral Therapy
(The Good)

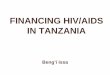
The Birth of HIV/AIDS Therapeutics
0
5
10
15
20
25
Num
ber o
f Ava
ilabl
e Age
nts
1987 1990 1993 1996 1999 2002 2005 2008
RaltegravirEtravirineMaravirocDarunavirTipranavirEnfuviritideFosamprenavirAtazanavirFTCTenofovirLopinivirAmprenavirAbacavirEfavirenzDelavridineNeviripineNelfinivirIndinivirRitonivirSaquinivirDDCD4T3TCDDIAZT

HIV Life Cycle Summary HIV attaches to & enters the T-Cell
Entry Inhibitors
HIV Copies itself from RNA to DNANucleoside Reverse Transcriptase Inhibitors (NRTIs)
Non-Nucleoside Reverse Transcriptase Inhibitors (NNRTIs)
HIV DNA integrates into our genesIntegrase Inhibitors
Our T-Cells mistakenly copy the virus
HIV assembles itself and buds out of the T-Cells to infect other cells
Protease InhibitorsViral Maturation Inhibitors

Efficacy in HIV Treatment: Decreased Mortality
What lead to the precipitous decline?

Multiple Drug Approach

Adult Resource Poor Settings
http://www.who.int/hiv/pub/guidelines/WHO%20Adult%20ART%20Guidelines.pdf

Pediatric Resource Poor Settings
http://www.who.int/hiv/pub/guidelines/WHOpaediatric.pdf

ART Works: HIV and life-expectancy
Over 40% of HIV positive individuals died of illnesses not attributable to HIV.
Survival was long – For 30 year old patients with CD4>500,
median survival ranges from 26.8-31.3 years For 50 year old patients with CD4>500,
median survival ranges from 21.1-22.3 years This may improve with improving therapies
Braithwaite, R, Justice, A, et al. “Estimating the proportion of patients with HIV who will die of comorbid diseases”. American Journal of Medicine (2005) 118, 890-898.

HIV and life-expectancy (2)
Mean life expectancy for individuals living with HIV in the US has improved from 10.5 years in 1996 to 22.5 years in 2005.
While improvements were seen in all groups, disparities still exist by gender, race.
Life expectancy still short of HIV negative peers.
Dependent on many factors.
Harrison K, Song R, Zhang X. “Life Expectancy after HIV diagnosis based on National HIV Surveillance Data from 25 States, United States”. JAIDS. Pre-print 2009.

clinicaloptions.com/hiv
Stay Tuned: Evolving Concepts in Antiretroviral Therapy
Reduced Mortality After First 3 Mos of ART in Developing Countries ART-LINC dataset[1] (N =
2725 with active follow-up) Botswana National HIV
Treatment Program[2] (N = 53,423 with adequate follow-up data)
47.8% of patients who died received HAART for < 3 mos
If patients survived > 3 mos, 94.3% likelihood of survival for > 5 yrs0 50 100 150 200
Mos 3-4
Mos 7-12
Mortality/1000 Pt-Yrs
27
51
Mo 2 106
147Mo 1
51Mos 5-6
1. Braitstein P, et al. Lancet. 2006;367:817-824. 2. Puvimanasinghe JP, et al. IAC 2008. Abstract MOAB0204.

Hot Topics in HIV Treatment
HIV & Chronic DiseaseWhen to Start HIV treatment
Treatment as Prevention

HIV and Chronic Disease (1)
Early on the major causes of morbidity were Opportunistic Infections and HIV wasting
As ART became more effective, causes of death began to switch to chronic diseases: cardiovascular disease, liver disease, kidney disease
This was initially presumed due to metabolic toxicities of the antiretroviral therapy.
However, recent research suggests that uncontrolled viral replication has long term complications as well. HIV has reservoirs other than CD4+ lymphocytes:
Macrophages, CNS Glial Cells, and Kidney cells. Ongoing HIV replication leads to diffuse immune system
activation and inflammation – which can have harmful consequences.

clinicaloptions.com/hiv
Optimal Timing of Antiretroviral Therapy
Immunosuppression Increases Risk of HIV- and Non-HIV–Related Mortality Cohort study of > 23,000
patients in Europe, Australia, and US
– 76,577 patient-years of follow-up
1248 (5.3%) deaths from 2000-2004
Both HIV- and non-HIV–related mortality associated with CD4+ cell count depletion
1.0
Weber R, et al. CROI 2005. Abstract 595.
500
100
0.1
10
< 50 50-99 100-199
200-349
350-499
CD4+ Cell Count (cells/mm3)
RR
OverallHIVMalignancyHeartLiver

clinicaloptions.com/hiv
When to Start Antiretroviral Therapy
CASCADE: Nadir CD4+ Cell Count Predicts AIDS and Non-AIDS Events
Marin B, et al. IAS 2007. Abstract WEPEB019.
1.000.01 1.00 100.00
Nadir CD4+ cell countAIDS-Related Death
0.01 100.00
200-349 vs ≥ 35050-199 vs ≥ 350
< 50 vs ≥ 350
Non-AIDS–Related Death
1.000.01 100.00
Non-AIDS Cancer Death
1.000.01 100.00
Liver Disease Death
200-349 vs ≥ 35050-199 vs ≥ 350
< 50 vs ≥ 350
200-349 vs ≥ 35050-199 vs ≥ 350
< 50 vs ≥ 350
200-349 vs ≥ 35050-199 vs ≥ 350
< 50 vs ≥ 350
CASCADE Collaboration cohort: N = 9858
Several clinical markers of HIV progression correlated with death due to AIDS-related causes, non-AIDS–related severe infection, liver diseases, and non-AIDS–related malignancies including
– Latest and nadir CD4+ cell counts
– Time spent with CD4+ cell count < 350 cells/mm3

HIV & Chronic Disease (2)
HIV+ individuals have higher rates of heart disease, cancer, renal disease even when accounting for known factors. General rule: unchecked HIV infection
makes any unrelated chronic disease worse... (there are exceptions, of course)
Hypothesized why overall life expectancy (even for those on treatment) doesn’t reach HIV- peers

When to Initiate Therapy Initiation of antiretroviral therapy is a balancing
act When treatment is initiated it is presumed to be
lifelong We must balance the benefits with long-term
toxicities, cost, pill burden, and resistance Until recently, clinicians have tried to wait until
the immune system is weaker to start ARV treatment:
Resource-Limited Settings typically wait until CD4+ falls to <200-250
Resource-Rich Settings typically wait until CD4+ falls to <350
This saves money and prevents toxicities from medicines.
But is this approach still the most effective? ART is easier to take and less toxic now We’ve already seen that unchecked HIV can worsen chronic
disease…

clinicaloptions.com/hiv
HIV/AIDS Annual Update 2006
CD4+ Count Response Based on Baseline CD4+ Count
Magnitude of CD4+ increase greatest if therapy started at low CD4+ counts, but greater likelihood of CD4+ count normalization with earlier therapy
Keruly J, et al. CROI 2006. Abstract 529. Gras L, et al. CROI 2006. Abstract 530.
Johns Hopkins HIV Clinical Cohort
Mea
n C
D4+
Co
un
t (c
ells
/mm
3 )
1000
800
600
400
200
00 48 96 144 192 240 288 336
ATHENA National Cohort
0 1 2 3 4 5
200
400
600
800
0
1000
Years on HAART Weeks From Starting HAART

clinicaloptions.com/hiv
Answering the Questions: Initiating Antiretroviral Therapy
HAART and Survival Based on Initial CD4+ Cell Count Modeled data from ART Cohort
Collaborative 10,855 patients included 934 progressed to AIDS or died IDUs excluded from model
Sterne J, et al. CROI 2006. Abstract 525.
CD4+ < 200 vs 201-350
CD4+ < 350 vs 351-500
Hazard ratio for AIDS (95% CI)
3.68 (3.01-4.51)
1.52 (1.10-2.10)
Hazard ratio for AIDS or death (95% CI)
2.93 (2.41-3.57)
1.26 (0.94-1.68)
Cumulative Probability of AIDS/Death According to CD4+ Count at Initiation
of HAART
Years Since Initiation of HAART
0 1 2 3 4 5
0.00
0.02
0.04
0.06
0.08
0.10
0.12
Pro
bab
ility
of
AID
S o
r D
eath
101-200 cells/mm3
201-350 cells/mm3
351-500 cells/mm3

HIV Treatment as Prevention
Transmission only occurs from people infected with HIV
HIV viral load (amount of HIV measurable in the blood) is the biggest predictor of transmission
ART lowers viral load Proof of concept: HIV
treatment prevents mother to child transmission
Advantages: Easily measurable Few other prevention
trials have been successful
CDC HIV Testing Recs
PACTG 076 & USPHS ZDV Recs

HIV Treatment Reduces Heterosexual Transmission
174 discordant, monogamous couples in Raiki, Uganda, retrospectively analyzed for factors associated with transmission[1]
1. Gray RH, et al. Lancet. 2001;40:1149-1153.2. Castilla J, et al. J Acquir Immune Defic Syndr. 2005;40:96-101.
30
1.0< 1700 1700-
12,49912,500-38,499
> 38,500
HIV-1 RNA (copies/mL)
Ad
just
ed R
ate
Rat
io o
f Tr
ansm
issi
on
/Co
ital
Act
10
20
0.1
393 steady heterosexual couples[2]
HIV prevalence among partners declined from 10.3% during pre-HAART period to 1.9% during late HAART period (P = .0061)
Enrollment Period
OR (95% CI) P Value
Pre-HAART (1991-1995)
1
Early HAART (1996-1998)
0.55 (0.19-1.61)
.2763
Late HAART (1999-2003)
0.14 (0.03-0.66)
.0127

Universal Testing & Treatment?
Mathematical modeling suggests that identification of ~90% of HIV+ patients through VCT coupled with immediate lifelong treatment in Southern Africa could reduce HIV incidence to < 1/1000 in 10 years. Would even realize
cost-savings by 2030. How realistic is this?

Global Health Implications:
Taking the Public Health Approach
Challenges in Resource Limited Settings
The Treatment Time-BombPediatric Issues

Public Health Approach
All these recent controversies highlight the importance to get people on treatment: Earlier treatment
improves outcomes ART leads to few
chronic and opportunistic diseases
ART can prevent new infections
Is this feasible??

Challenges: Human Resources

Infrastructure

Supplies

Transport

Challenges: Cost
The “Treatment Timebomb”(The UGLY)

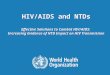
HIV/AIDS Funding
2003 2004 2005 2006 2007 20080
2,000
4,000
6,000
8,000
10,000
12,000
14,000
16,000
18,000
20,000
$4,200
$13,765
Philan-thropicMultilateralBilateral
US
$ M
illi
on
+ 62% Multilateral
+ 112%Bilateral
+ 616%Domestic
+ 244% Philanthrop.
Slide Adapted from Implementers Meeting Presentation by Stefano Bertozzi, 2009
UNAIDS estimates
$8.1 billion funding gap
for 2007

Sample Costing Exercises:
Resource Availability and Needs
Slide adapted courtesy of John Stover & Rachel Sanders, HPI/Futures Group

0
50
100
150
200
Hea
lth B
enefi
t
Global AIDS Expenditures
Health benefit from investing in HIV prevention, care and treatment
ARV becomes available in developing countries
M O N E Y
VA
LU
E

0
50
100
150
200
Hea
lth B
enefi
t
Global AIDS Expenditures
ECONOMIC CRISIS
??
ARV becomes available in developing countries
Two obvious responses:1. Strategies to
maintain/increase funding levels
2. Improve efficiency
Health benefit from investing in HIV prevention, care and treatment

0
50
100
150
200
Hea
lth B
enefi
t
Global AIDS Expenditures
Health benefit from investing in HIV prevention, care and treatment
Two obvious responses:1. Strategies to
maintain/increase funding levels
2. Improve efficiency

Special Pediatric Challenges

HIV Progression in Children is BiModal
20-25% rapidly develop profound immunosuppression and opportunistic infections.– Without treatment
few of these children survive 2 years
– Many die within the first 6 months of life
75-80% may have a slower progression – Mean time to AIDS is
6-9years – Still more rapid
progression than adults (8-11yrs)

Early Diagnosis is Essential!
< 18 months Persistence of maternal
antibody No EIA, Western Blot Tests for viral components:
HIV DNA or RNA PCR, Immune Complex Dissociated
(ICD) p24 antigen Dried Blood Spots (DBS)
> 18 months Can use EIA, Western Blot

Clinical Identification of HIV+ Children is Difficult
Signs often non-specific Respiratory distress Poor weight gain weight or
abnormal growth Missed milestones in
development crawling, walking and speaking
Poor school performance, seizures, and other symptoms of HIV encephalopathy

Why are children more vulnerable to the symptoms
of HIV? It is during the first few years of life that
the immune system is developing. Untreated HIV infection will stunt the overall
maturation of the immune system Adults have already developed immunologic
memory and are therefore less prone to infections
Children are frequently unable to express health needs, or comprehend the need for medications Also have frequently changing dosing
requirements Children are dependent on adults for food
choices and good nutrition, which impacts growth, development, and efficacy of medications

More Pediatric Challenges
Pediatric expertise and experience
Misperceptions that all infected children will die early in childhood
Caretaker dependence ART Issues for children:
Drug availability Taste Appropriate formulations (FDCs,
liquids, etc.) Dosing Affordable prices http://www.who.int/3by5/en/finalreport.pdf

“The Pearls” 1. HIV Treatment Works! 2. Evidence supports earlier
initiation of treatment! Lower mortality Fewer Ois and less chronic disease
3. Without adequate prevention, we face serious challenges in being able to meet the need for treatment!


Discussion
• www.usaid.gov• www.pepfar.gov • www.globalhealthlearning.org• http://depts.washington.edu/hivaids/index.html• www.who.int/hiv/pub/guidelines/en/