Embed Size (px)
Citation preview

Update Pain Management in Children
วนัธณี วิรฬุหพ์านิช, Ph.D., RN
คณะพยาบาลศาสตร ์ มหาวิทยาลยัสงขลานครนิทร์

What Update?
* Definition of pain* Pain Assessment
>> Pain Scale>> Smart Phone Application
* Pharmacologic & Non-Pharmacologic* Nursing Education Intervention

Definition of Pain
whatever the person experiencing it says it is, existing whenever the person says it does. (McCaffery, 1999)
ระดบัความปวดท่ีแทจ้รงิตอ้งมาจากค าพดูเด็ก
ส าหรบัเด็กท่ีสามารถบอกความปวดไดด้ว้ยตนเอง
เมือ่ไหร่ก็ตามที่บคุคลประสบความปวดบอกว่าปวด
ความปวดยงัคงอยู่ตราบเทา่ที่บคุคลนัน้บอกวา่ปวด
ความปวดสามารถสงัเกตไดจ้ากการตอบสนองทาง
สรีรวิทยาและพฤตกิรรมการแสดงออกที่เด็กสื่อ
ออกมา (Anand & Craig, 1996)
ความปวดไมไ่ดม้าจากค าพดูเพียงอย่างเดียว

“ความรูส้ึกที่ไมส่ขุสบายร่วมกบัประสบการณท์าง
อารมณท์ี่เกิดจากการบาดเจ็บของเนือ้เย่ือจากการ
ผา่ตดั ที่บคุคลสื่อออกมาดว้ยลกัษณะทา่ทาง
และ/หรือ การเปลี่ยนแปลงทางสรีรวิทยา และ/
หรือ พฤตกิรรมการตอบสนองความปวดที่สื่อว่า
มกีารบาดเจ็บของเนือ้เย่ือ (วนัธณี, 2561)
เด็กกลุม่ที่ไดร้บัการผา่ตดัและถกูจ ากดัการสื่อสารดว้ย
ทอ่ชว่ยหายใจ

* 3 Approaches>> Self-report
# What the child says>> Behavioral
# How the child behaves>> Physiological indicators
# How the child’s body reacts
Pain Assessment: Pain Scales

* Self-report# Old enough to understand# Not overtly distressed# Not cognitively impaired# Child must assess himself/herself
* Behavioral # Preverbal: Infants, Toddlers# Non verbal: Cognitive impaired, Sedated
or Ventilated children# Nurses must assess & rank them.
* If overtly distress: Anxiety, stress# Lessening the child distress (Analgesics,
coping strategies, non-pharmaclogical pain management)

* New pain scales were developed>> Modified from the previous one >> Most pediatric pain scales were
originally developed to measureprocedural-related pain
* Special population>> On ventilator & Non-verbal communicate>> The child’s cognitive level and
communication abilities>> Cognitive impairment: Cerebral palsy,
Autism
Development of Pain scales

Self-Report Pain Scales
Self-Report Pain Scales
* Popular & well established reliability & validity >> Faces Pain Scale Revised (FPS-R)>> Numeric Rating Scale (NRS)>> Visual Analog Scale (VAS)>> Wong-Baker FACES Pain Scale>> Oucher

มาตรวดัเสน้ตรงแบบเรียงล าดบัเลข
(Numeric Rating Scale)
0 1 2 3 4 5 6 7 8 9 10
* เสน้ตรงยาว 10 cm & ตวัเลขระบคุวามรนุแรงของ
ความปวด 10 ระดบั
* นยิมวดัในเด็กวยัเรียน (Wong & Baker, 1988)
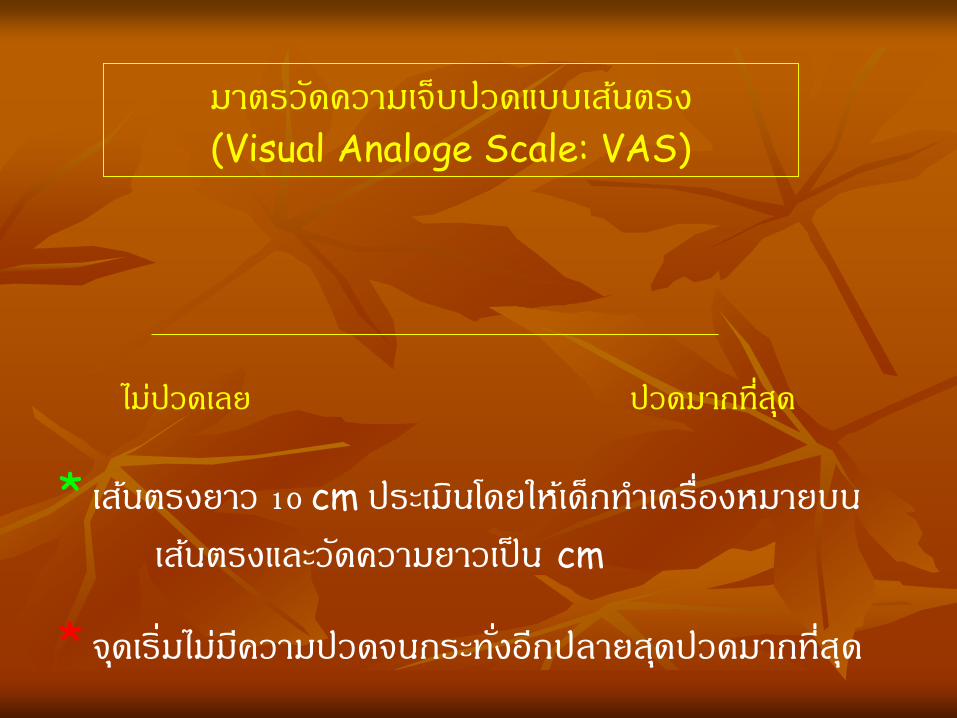
มาตรวดัความเจ็บปวดแบบเสน้ตรง
(Visual Analoge Scale: VAS)
ไมป่วดเลย ปวดมากที่สดุ
* เสน้ตรงยาว 10 cm ประเมนิโดยใหเ้ด็กท าเคร่ืองหมายบน
เสน้ตรงและวดัความยาวเป็น cm
* จดุเร่ิมไมม่คีวามปวดจนกระทัง่อีกปลายสดุปวดมากที่สดุ

มาตรวดัความปวดแบบเรยีงล าดบัใบหนา้
ใบหนา้ 0 = มคีวามสขุเนือ่งจากไมไ่ดร้บัความเจ็บปวด
ใบหนา้ 2 = ปวดเล็กนอ้ย
ใบหนา้ 4 = ปวดพอทน
ใบหนา้ 6 = ปวดมาก
ใบหนา้ 8 = ปวดมากที่สดุ
ใบหนา้ 10 = ปวดมากที่สดุเท่าที่คิดว่าจะจินตนาการได,้
ถึงจะไมร่อ้งไหก็้ร ูส้ึกไมด่กีบัความเจ็บปวดนัน้
หมายเหต.ุ จาก Wong’s essentials of pediatric nursing (p. 1301), by D. L. Wong, M.
Hockenberry-Eaton, D. Wilson, M. I. Winkelstein, P. Schwartz, 2001, St. Louis: Mosby. Copyright 2001 by Mosby.
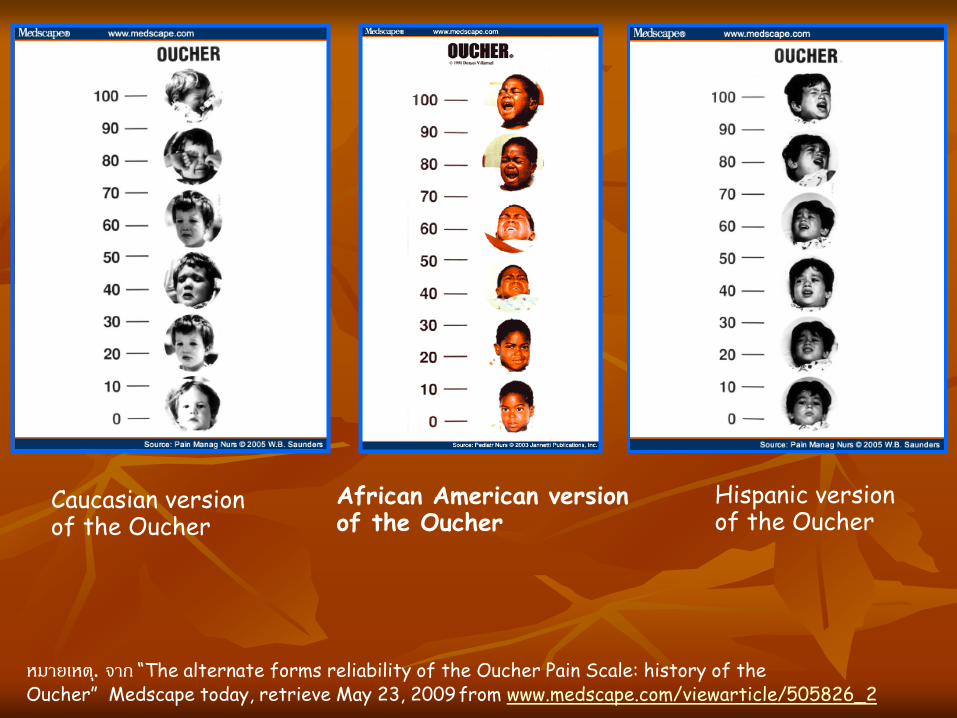
Caucasian version of the Oucher
African American version of the Oucher
Hispanic version of the Oucher
หมายเหต.ุ จาก “The alternate forms reliability of the Oucher Pain Scale: history of the Oucher” Medscape today, retrieve May 23, 2009 from www.medscape.com/viewarticle/505826_2
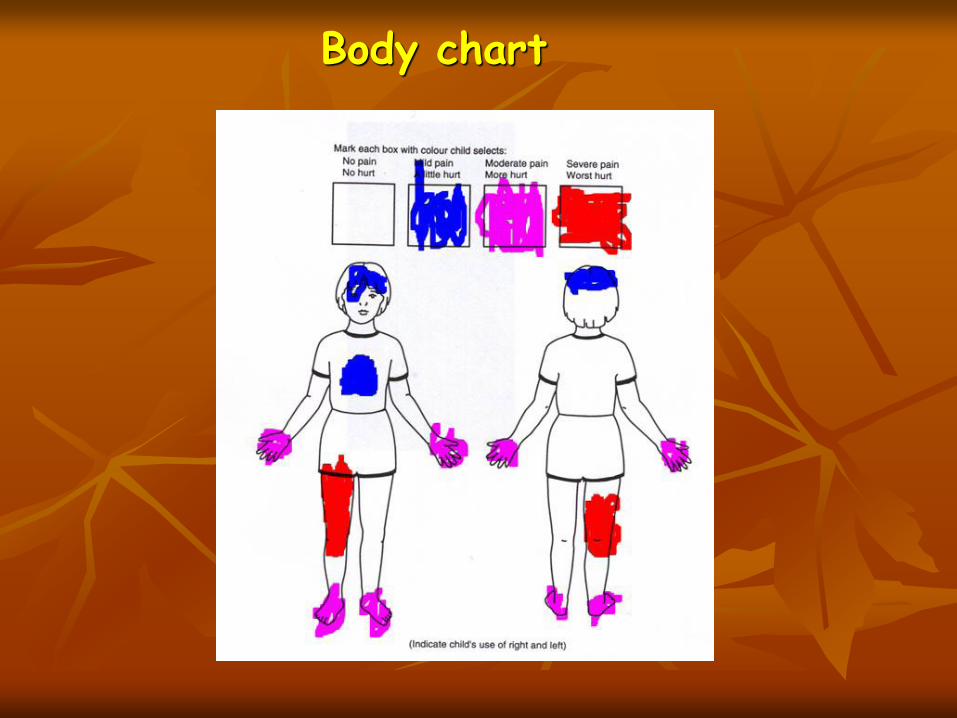
Body chart

Behavioral Pain Scales

Behavioral Pain Scales
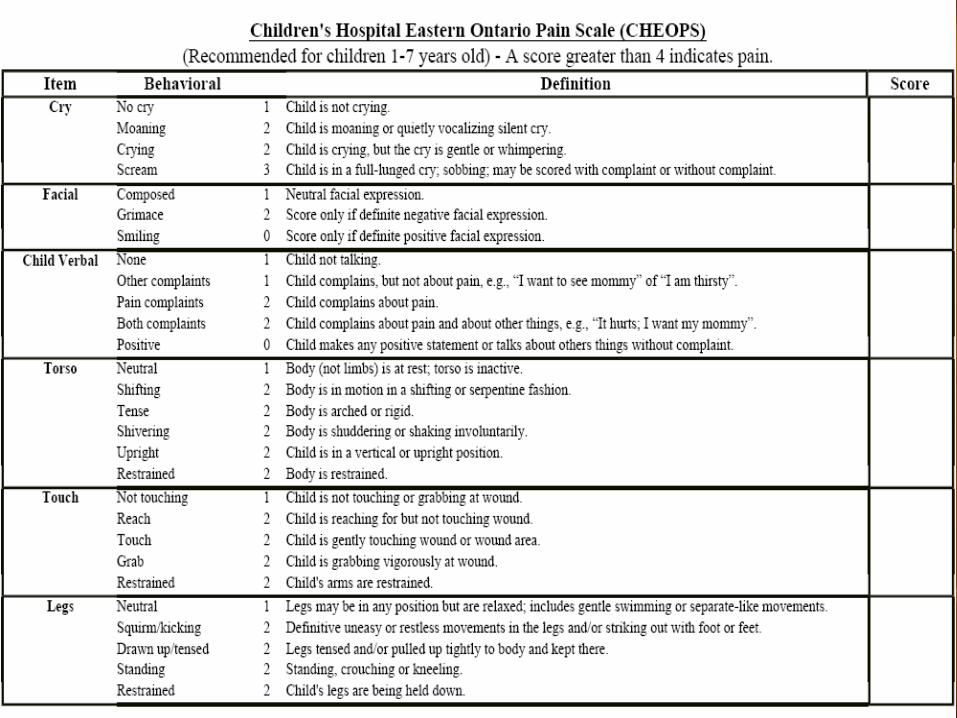
* Commonly used & well established reliability & validity >> Children’s Hospital of Eastern Ontario
Pain Scale (CHEOPS)>> Children’s and Infants’ Postoperative Pain
Scale (CHIPPS)>> COMFORT Behavior Scale>> Crying>> Distress Scale for Ventilated Newborn
Infants (DSVNI)>> Faces, Legs, Activity, Cry, and
Consolability Observational Tool (FLACC)

>> Neonatal Infant Pain Scale (NIPS)>> Neonatal Pain, Agitation, and Sedation Scale
(N-PASS)>> Noncommunicating Children’s Pain Checklist
(Acute Care NCCPC)>> Pediatric Pain Profile>> Premature Infant Pain Profile (PIPP)>> Toddler-Preschooler Postoperative Pain
Measure (TPPPM)
Manworren, R. C. B., & Stinson, J. (2016). Pediatric pain measurement, assessment, and evaluation. Seminars in Pediatric Neurology, 23, 189-200.doi.org/10.1016/j.spen.2016.10.001

Birth – 6 month 3-6 ปี 6 ปี - วนัร ุน่
Neonatal Infant Pain Scale (NIPS)
Neonatal Pain Assessment and Sedation Scale (N-PASS)
Neonatal Facial Coding System (NFCS)
CRIES
Wong Baker Faces
Oucher (3-12yrs
Children’s Hospital of Eastern Ontario Pain Scale (CHEOPS)
FLACC
self-report scale
Visual Analogue Scale (VAS)
Verbal Numeric Scale (VNS)/
Numeric Rating Scale (NRS

* วดัการแสดงออกทางพฤตกิรรม 6 ดา้น:
>> การแสดงออกทางใบหนา้, การรอ้งไห,้
แบบแผนการหายใจ, การเคลื่อนไหวของแขน,
การเคลื่อนไหวของขา, ระดบัการหลบัตืน่
แบบวดัความปวดในทารกแรกเกิด
(Neonatal Infant Pain Scale: NIPS)
* Lawrence et al., 1993
* วดัพฤตกิรรมความปวด:
>> Acute procedure pain
>> Preterm & Full term
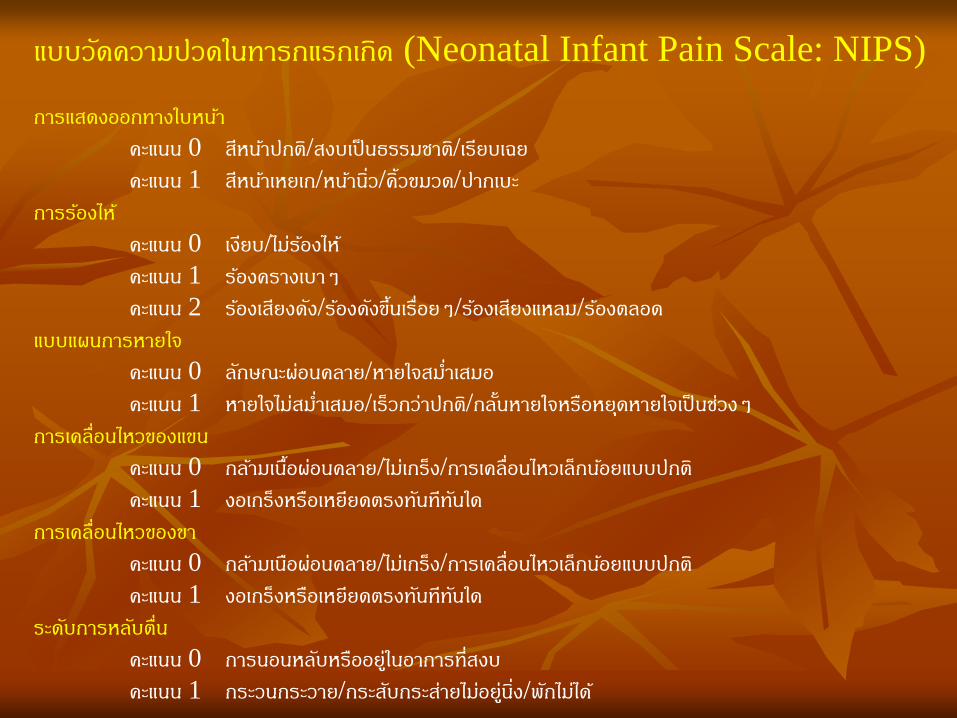
แบบวดัความปวดในทารกแรกเกิด (Neonatal Infant Pain Scale: NIPS)
การแสดงออกทางใบหนา้
คะแนน 0 สีหนา้ปกติ/สงบเป็นธรรมชาต/ิเรียบเฉย
คะแนน 1 สีหนา้เหยเก/หนา้นิว่/ค้ิวขมวด/ปากเบะ
การรอ้งไห้
คะแนน 0 เงยีบ/ไมร่อ้งไห้
คะแนน 1 รอ้งครางเบาๆ
คะแนน 2 รอ้งเสียงดงั/รอ้งดงัขึน้เร่ือยๆ/รอ้งเสียงแหลม/รอ้งตลอด
แบบแผนการหายใจ
คะแนน 0 ลกัษณะผอ่นคลาย/หายใจสม า่เสมอ
คะแนน 1 หายใจไมส่ม า่เสมอ/เร็วกว่าปกต/ิกลัน้หายใจหรือหยดุหายใจเป็นชว่งๆ
การเคลื่อนไหวของแขน
คะแนน 0 กลา้มเนือ้ผอ่นคลาย/ไมเ่กร็ง/การเคลื่อนไหวเล็กนอ้ยแบบปกติ
คะแนน 1 งอเกร็งหรือเหยียดตรงทนัทีทนัใด
การเคลื่อนไหวของขา
คะแนน 0 กลา้มเนอืผอ่นคลาย/ไมเ่กร็ง/การเคลื่อนไหวเล็กนอ้ยแบบปกติ
คะแนน 1 งอเกร็งหรือเหยียดตรงทนัทีทนัใด
ระดบัการหลบัตื่น
คะแนน 0 การนอนหลบัหรืออยู่ในอาการที่สงบ
คะแนน 1 กระวนกระวาย/กระสบักระสา่ยไมอ่ยู่นิง่/พกัไมไ่ด้
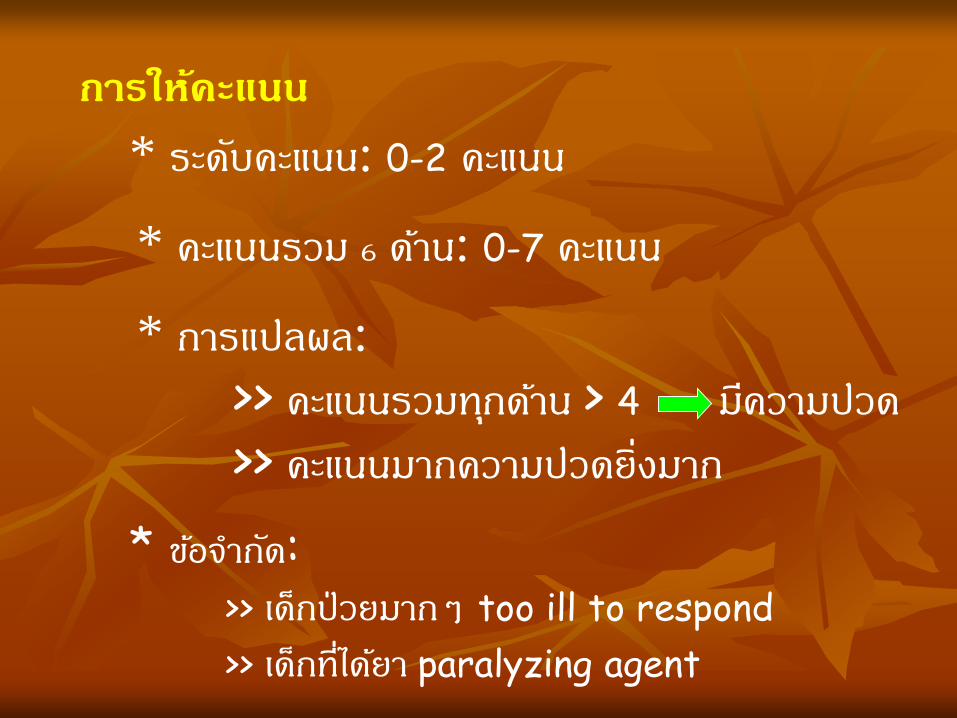
การใหค้ะแนน
* ระดบัคะแนน: 0-2 คะแนน
* คะแนนรวม 6 ดา้น: 0-7 คะแนน
* การแปลผล:
>> คะแนนรวมทกุดา้น > 4 มคีวามปวด
>> คะแนนมากความปวดย่ิงมาก
* ขอ้จ ากดั: >> เด็กป่วยมากๆ too ill to respond
>> เด็กที่ไดย้า paralyzing agent

แบบวดัพฤติกรรมความปวดในทารกคลอดกอ่นก าหนด
PIPP (Premature Infant Pain Scale)
* University of Toronto & McGill, Canada
* Indicator: ไมม่พีฤตกิรรมการรอ้ง
>> Gestational age>> Behavioral state before painful stimuli >> Change in heart rate during painful stimuli >> Change in O2 Sat during painful stimuli >> Brow bulge during painful stimuli >> Eyes squeeze during painful stimuli >> Nasolabial furrow during painful stimuli
* Premature: Acute pain & prolong pain
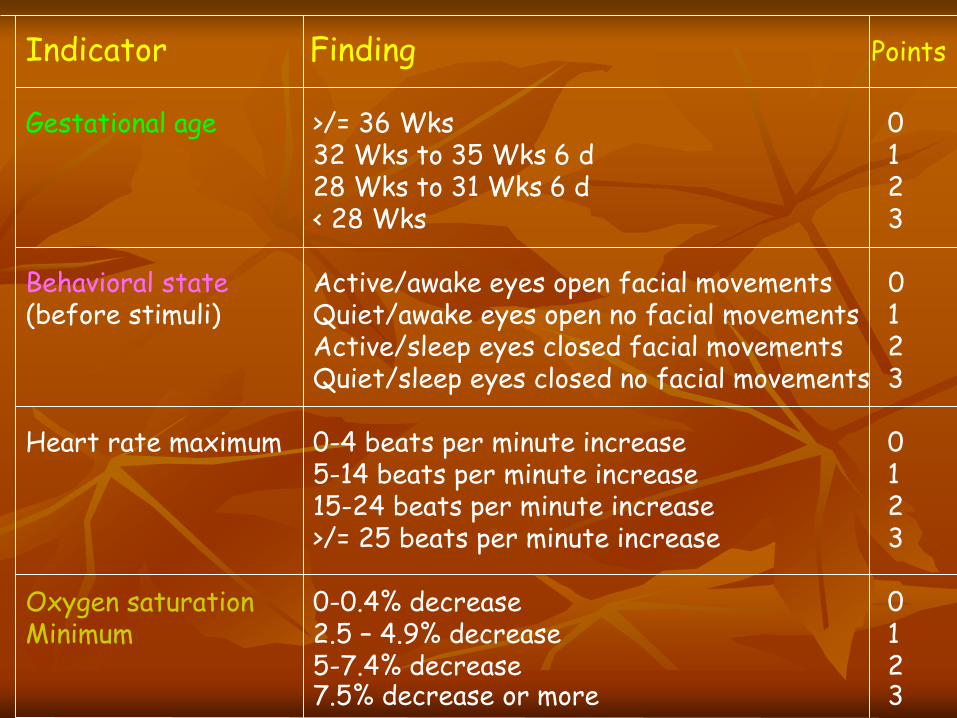
Indicator Finding Points
Gestational age >/= 36 Wks 032 Wks to 35 Wks 6 d 128 Wks to 31 Wks 6 d 2< 28 Wks 3
Behavioral state Active/awake eyes open facial movements 0(before stimuli) Quiet/awake eyes open no facial movements 1
Active/sleep eyes closed facial movements 2Quiet/sleep eyes closed no facial movements 3
Heart rate maximum 0-4 beats per minute increase 05-14 beats per minute increase 115-24 beats per minute increase 2>/= 25 beats per minute increase 3
Oxygen saturation 0-0.4% decrease 0Minimum 2.5 – 4.9% decrease 1
5-7.4% decrease 27.5% decrease or more 3

Indicator Finding Points
Brow bulge None (</= 9% of time) 0Minimum (10-39% of time) 1Moderate (40-69% of time) 2Maximum (>/= 70% of time) 3
Eyes squeeze None (</= 9% of time) 0Minimum (10-39% of time) 1Moderate (40-69% of time) 2Maximum (>/= 70% of time) 3
Nasolabial furrow None (</= 9% of time) 0Minimum (10-39% of time) 1Moderate (40-69% of time) 2Maximum (>/= 70% of time) 3
*** ตอ้งค านวน ไมเ่ป็นที่นยิม***

The COMFORTneo Scale
* Developer: Monique van Dijk & Colleague>> The COMFORT Behavior Scale in 1999
# Age 0-3 year ventilated intubated with sedative and anlgesic
>> พฒันา The COMFORTneo Scale in the Year 2004-2005
# Preterm neonate with ventilator or without ventilator
# Prolong pain (Ventilator/Disease such as NEC)
# Cut-off point เทา่กนัในเด็กกลุม่ Low birth weight, small for gestational age
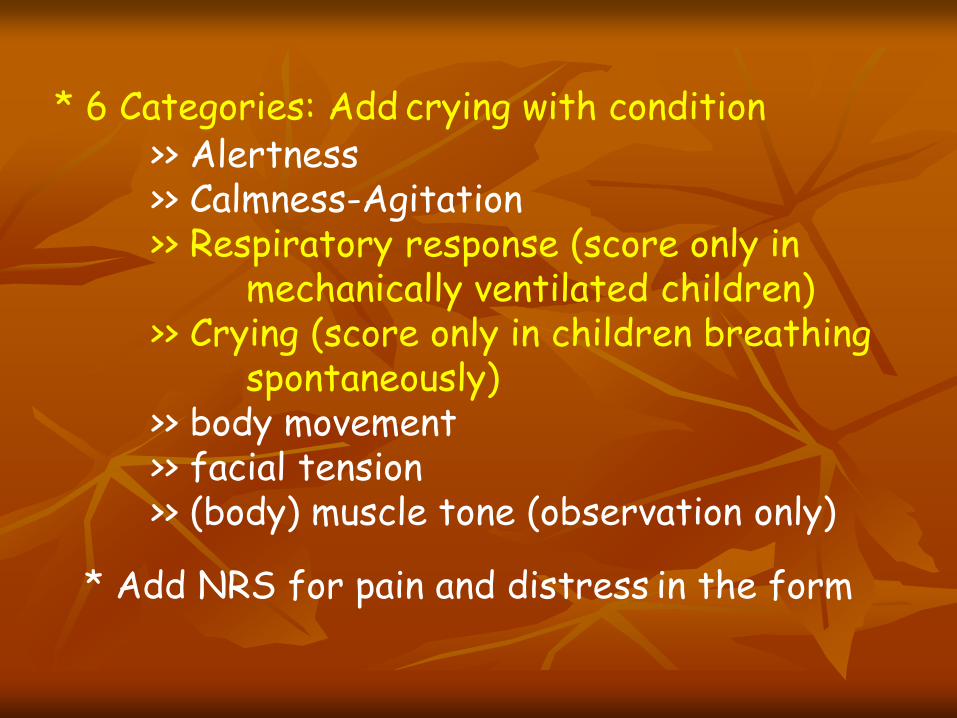
* 6 Categories: Add crying with condition>> Alertness>> Calmness-Agitation>> Respiratory response (score only in
mechanically ventilated children)>> Crying (score only in children breathing
spontaneously)>> body movement>> facial tension>> (body) muscle tone (observation only)
* Add NRS for pain and distress in the form

Please tick the appropriate responsealertness1 quiet sleep (eyes closed, no facial movement)2 active sleep (eyes closed, facial movement)3 quietly awake (eyes open, no facial movement)4 actively awake (eyes open, facial movement)5 awake and hyperalertcalmness/agitation1 calm (appears lucid and serene)2 slightly anxious (shows slight anxiety3 anxious (appears agitated but remains in control)4 very anxious (apperars very agitated, just able to control)5 panicky (severe distress with loss of control)respiratory response (only in mechanically ventilated children)1 no spontaneous respiration2 spontaneous respiration on ventilator3 unret or resistance to ventilator4 actively breathes against ventilator or coughs regularly5 fights ventilatorcrying (only in spontaneously breathing children)1 no crying2 faint crying3 soft crying or moaning4 hard crying5 intense crying or screamingbody movement1 no or minimal movement2 up to three slight arm and / or leg movements3 more than three slight arm and / or leg movements4 up to three vigorous arm and/ or leg movements5 more than three vigorous arm and / or leg movements, or whole bodyficial tension1 facial muscles fully relaxed, relaxed open mouth2 normal facial tension3 intermittent eye squeeze and brow furrow4 continuous eye queeze and brow furrow5 facial muscles contorted and grimacing (eye squeeze, brow furrow, open mouth, nasal.-labial lines)(body) muscle tone (observation only)1 muscles fully relaxed (open hands, dribbling, open mouth)2 reduced muscle tone; less resistance than normal3 normal muscle tone4 increased muscle tone (clenched hands and/or clenched, bent toes)5 extreme muscle tone (rigidity and flexion of fingers and/ or toes)total Details medication / treatment……………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………Details child;s condition…….……………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………Type of assessment………….…………………………………………………………………………………………………………………………………………………………………
Estimate of pain (0 = no pain to 10 = worst possible pain)
Estimate of distress (0 = no distress tot 10 = worst possible distress)
COMFORTneoScale
Date :Time :Observer :
Patient sticker
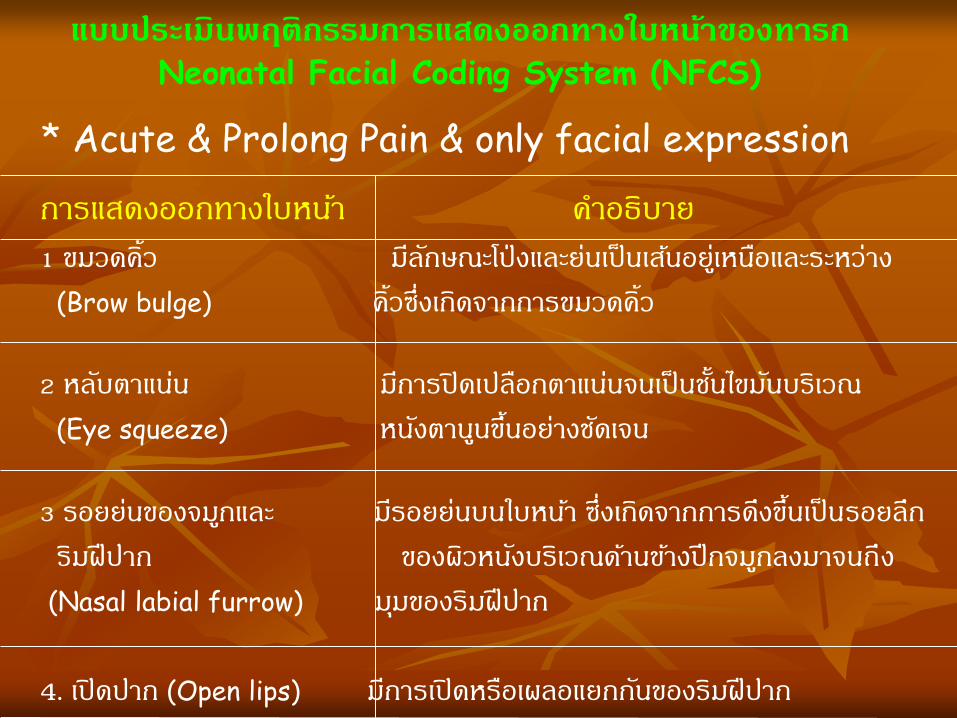
แบบประเมินพฤติกรรมการแสดงออกทางใบหนา้ของทารก
Neonatal Facial Coding System (NFCS)
การแสดงออกทางใบหนา้ ค าอธิบาย
1 ขมวดค้ิว มลีกัษณะโป่งและยน่เป็นเสน้อยูเ่หนอืและระหว่าง
(Brow bulge) ค้ิวซ่ึงเกิดจากการขมวดค้ิว
2 หลบัตาแนน่ มกีารปิดเปลือกตาแนน่จนเป็นชัน้ไขมนับริเวณ
(Eye squeeze) หนงัตานนูขึน้อยา่งชดัเจน
3 รอยยน่ของจมกูและ มรีอยยน่บนใบหนา้ ซ่ึงเกิดจากการดงึขึน้เป็นรอยลึก
ริมฝีปาก ของผวิหนงับริเวณดา้นขา้งปีกจมกูลงมาจนถึง
(Nasal labial furrow) มมุของริมฝีปาก
4. เปิดปาก (Open lips) มกีารเปิดหรือเผลอแยกกนัของริมฝีปาก
* Acute & Prolong Pain & only facial expression

5 อา้ปากแนวดิง่ มกีารยืดเกร็งของกึ่งกลางริมฝีปากบนแนะลา่งใน
(Vertical mouth stretch) แนวขึน้และลงโดยแยกจากกนัตามแนวดิง่
6 ริมฝีปากเหยียดตรง มกีารยืดของมมุปากทัง้ขวาและซา้ยออกจากกนั
(Horizontal mouth stretch) ทางดา้นขา้งตามแนวราบ
7 ห่อปาก (Lop purse) ริมฝีปากจะห่อเหมอืกบัเวลาท่ีเปลง่เสียงไอ
8 เร็งลิ้น (Taut tongue) มกีารยกและห่อลิ้นจนเห็นการเกร็งของขอบลิ้นอยา่ง
ชดัเจน การเกิดขึน้ครัง้แรกของการเกร็งลิ้นจะเห็น
ไดง้า่ยจากการอม้ปากกวา้งหลงัจากนัน้แลว้
ปากจะปิดลง การเกร็งลิ้นจะมกีารใหค้ะแนนถา้ยงั
สามารมมองเห็นขอบของลิ้น
9 คางสัน่ มกีารเคลื่อนไหวขึน้และลงอย่างถ่ีๆของขากรรไกรลา่ง
(Chin quiver) อยา่งชดัเจน
10 แลบลิ้น มองเห็นลิ้นและลิ้นย่ืนออกมานอกริมฝีปาก
(Tongue protrusion)

ตวัชว้ดั คะแนน
0 1 2
ใบหนา้ ไมม่ีการแสดงออกทางหนา้
หรือ ย้ิม
หนา้นิว่/ ค้ิวขมวด เป็นครัง้คราว
เฉยเมยหรือไมส่นใจสิ่งแวดลอ้ม
คางสัน่สม า่เสมอบ่อยๆ ถึงสัน่
ตลอดเวลา ขบขากรรไกร
ขา อยู่ในทา่ปกต ิหรือผอ่นคลาย ขาเคลื่อนไหวไมอ่ยู่กบัที่ เกร็งๆ เตะ หรือ ยกขาขึน้
กจิกรรม/การ
เคลื่อนไหว
นอนสงบนิง่ วางทา่ปกติ
เคลื่อนไหวตามสบาย
ดิน้ บิดตวัไปมา เกร็ง ล าตวัโกง่ แข็งเกร็งหรือสะบัดตวั
รอ้งไห ้ ไมร่อ้งไห้ รอ้งครางหรือ คร า่ครวญ
บ่น/รอ้งเป็นครัง้คราว
รอ้งไหต้ลอดเวลา กรีดรอ้งหรือ
สะอ้ืน บ่น/รอ้งบ่อยๆตลอด
การปลอบโยน รูสึ้กพอใจ
ผอ่นคลาย
สงบเป็นครัง้คราวเมื่อไดร้บัการ
ปลอบโยนดว้ยการสมัผสั กอด
หรือ พดูคยุ การเบ่ียงเบนความ
สนใจ
ยากตอ่การปลอบโยน
หรือท าใหส้งบ
FLACC Scale
แบบสงัเกตพฤตกิรรมความปวดแบบประยกุต์
Modified Behavioral Pain Scale (MBPS)
* Taddio et al., 1995
* ประเมนิทารก 2-6 เดอืน ชนดิเฉียบพลนั
* วดัการแสดงออกทางพฤตกิรรมความปวด
3 ดา้น: >> การแสดงออกทางสีหนา้ >> การรอ้งไห ้
>> การเคลื่อนไหวของร่างกาย

การแสดงออกทางสีหนา้
คะแนน 0 แสดงสีหนา้ไปทางบวกอย่างชดัเจน เชน่ ย้ิม
คะแนน 1 แสดงสีหนา้ปกตธิรรมชาติ
คะแนน 2 แสดงสีหนา้คอ่นขา้งไปทางลบ เชน่ คิ้วขมวด ย่นหนา้ผาก ปากแบะ
คะแนน 3 แสดงสีหนา้ค่อนขา้งไปทางลบชดัเจน เชน่ คิ้วขมวด ย่นหนา้ผาก หลบัตาแนน่
อา้ปากคา้ง หนา้แดงหรือไมแ่ดง
ดา้นการรอ้งไห้
คะแนน 0 หัวเราะ
คะแนน 1 ไมร่อ้งไห้
คะแนน 2 รอ้งครางเบาๆ/รอ้งครางเป็นระยะ
คะแนน 3 รอ้งเสียงดงั/รอ้งไหส้ะอึกสะอื้น
คะแนน 4 รอ้งแผดเสียงดงัมากกว่าการรอ้งไหป้กติ
ดา้นการเคลื่อนไหวของร่างกาย
คะแนน 0 เคลื่อนไหวปกต/ิสงบ หรือผอ่นคลาย
คะแนน 1 เคลื่อนไหวร่างกายบางสว่นหรือพยายามหลีกเลี่ยงการถกูฉีดยาโดยชกัขา
ขา้งที่ถกูฉีดยาหนี
คะแนน 2 ดิน้รน โดยเคลื่อนไหวร่างกายทกุสว่น ทัง้ศรีษะ ล าตวั แขนขา/เกร็งทัง้ตวั
Modified Behavioral Pain Scale (MBPS)
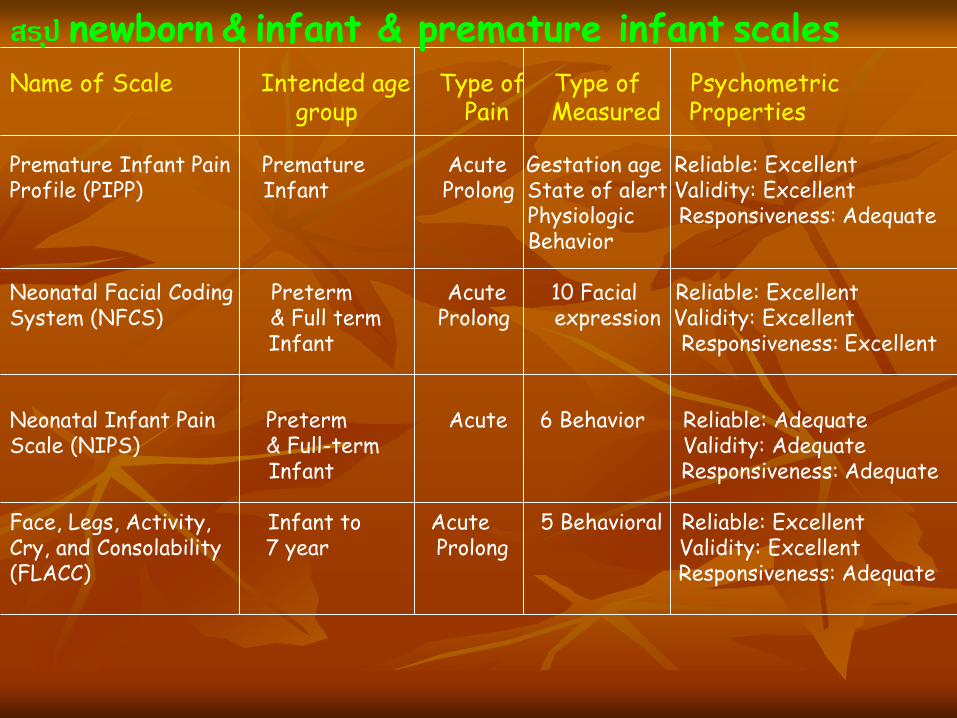
Name of Scale Intended age Type of Type of Psychometricgroup Pain Measured Properties
Premature Infant Pain Premature Acute Gestation age Reliable: ExcellentProfile (PIPP) Infant Prolong State of alert Validity: Excellent
Physiologic Responsiveness: AdequateBehavior
Neonatal Facial Coding Preterm Acute 10 Facial Reliable: ExcellentSystem (NFCS) & Full term Prolong expression Validity: Excellent
Infant Responsiveness: Excellent
Neonatal Infant Pain Preterm Acute 6 Behavior Reliable: Adequate Scale (NIPS) & Full-term Validity: Adequate
Infant Responsiveness: Adequate
Face, Legs, Activity, Infant to Acute 5 Behavioral Reliable: ExcellentCry, and Consolability 7 year Prolong Validity: Excellent(FLACC) Responsiveness: Adequate
สรปุ newborn & infant & premature infant scales

How?

กระบวนการประเมนิความปวดในเด็ก
Q = question the child
U = Use pain rating tools
E = Evaluate behavior
S = Sensitize parents (ask them to report the child pain)
T = Take action(Hain, 1997

Child’s Self-reported Nurses’ evaluation Parents’ evaluation
ประเมนิมากกว่า 1 sources

Special Population
Ventilated, unconscious, and/or sedated children

* ประเมินโดยใหเ้ด็กรายงานดว้ยตนเอง (Self-report)
* คน้หาสาเหตขุองความปวด (Search for potential causes of pain)
* สงัเกตพฤติกรรมของผ ูป่้วย (Observation of patient behavior)
* ใชเ้ครือ่งมือประเมินพฤติกรรมความปวด (Use of behavioral pain assessment tools)
* สมัภาษณค์วามปวดจากคนใกลชิ้ด (Proxy reporting of pain)
* พิจารณาใหย้าระงบัปวด (Analgesic trial)
วิธีการประเมินความปวดในเด็กถกูจ ากดัการสื่อสารดว้ยท่อช่วยหายใจ

** การบีบแขนพยาบาล (grabbing arm)
** การสง่สญัญาณดว้ยสายตา/ การขยิบตา (signaling
with heir eyes) (Pasero & McCaffery, 2011)
** การยกขาขึน้ลง (moving legs up) (Puntillo, 1990)
** การกางนิว้หวัแมม่อืและนิว้ชีเ้พื่อใหเ้ด็กประมาณระดบั
ความปวด (The finger span scale) (Merkel, 2002)
** การชจู านวนนิว้แสดงระดบัความปวด
วิธีการประเมินความปวดดว้ยตนเองในเด็กท่ีใส่
เครื่องช่วยหายใจ
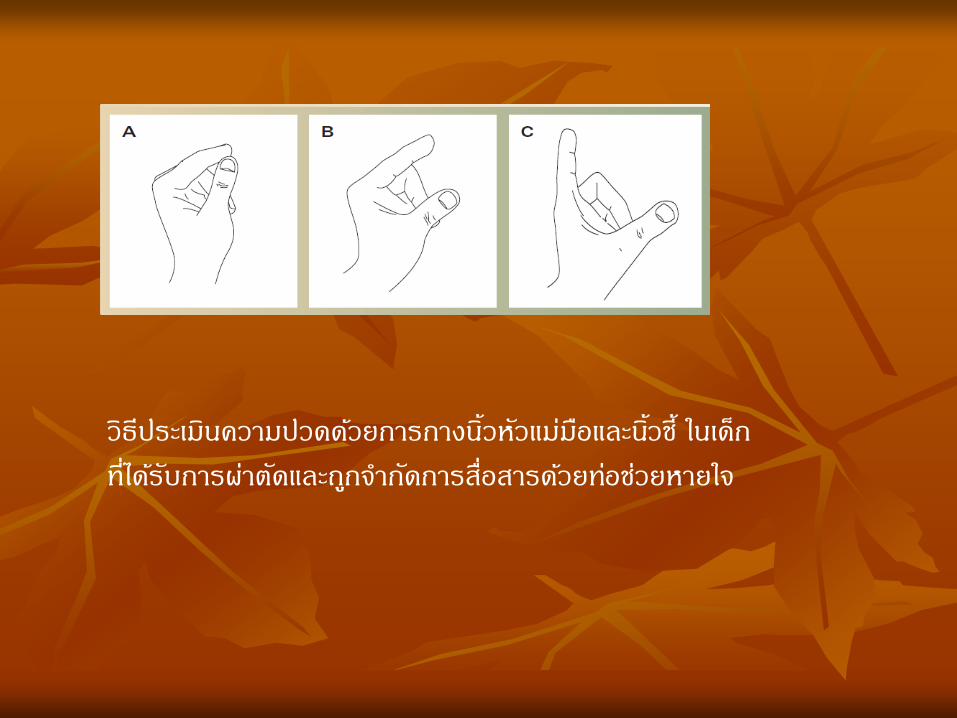
วิธีประเมนิความปวดดว้ยการกางนิว้หัวแมม่อืและนิว้ชี ้ในเด็ก
ท่ีไดร้บัการผา่ตดัและถกูจ ากดัการสื่อสารดว้ยทอ่ชว่ยหายใจ


เด็กที่ไดร้บัการผา่ตดัและถกูจ ากดัการสื่อสาร
ดว้ยทอ่ชว่ยหายใจ
*The modified FLACC Scale* COMFORT-B Scale * The Cardiac Analgesic Assessment Scale
(CAAS)>> Heart surgery
* The multidimensional Assessment of Pain Scale –Revised (MAPS-Revised)
* Hartwig Score

ตวัช้ีวดั คะแนน
0 1 2
ใบหนา้ ไมม่ีการแสดงออกทางหนา้
หรือ ย้ิม
หนา้นิว่/ค้ิวขมวด เป็นครัง้
คราว
เฉยเมยหรือไมส่นใจสิ่งแวดลอ้ม
คางสัน่สม า่เสมอบ่อยๆถึงสัน่
ตลอดเวลา ขบขากรรไกร
ขา อยู่ในทา่ปกติ หรือผอ่น
คลาย
ขาเคลื่อนไหวไมอ่ยู่กบัที่ เกร็งๆ เตะ หรือ ยกขาขึน้
กิจกรรม/การเคล่ือนไหว นอนสงบนิง่ วางทา่ปกติ
เคลื่อนไหวตามสบาย
ดิ้น บิดตวัไปมา เกร็ง ล าตวัโกง่ แขง็ หรือ
สะบัดตวั
การแสดงออกทางสีหนา้
ของการรอ้งไห ้(ให้
คะแนนในกรณีท่ีเด็กใช้
เครือ่งช่วยหายใจ)
สีหนา้เรียบเฉย
ไมแ่สดงออกทางใบหนา้ว่า
รอ้งไห้
สีหนา้บ่งบอกว่า รอ้งคราง
หรือ คร า่ครวญ บ่น/รอ้งเป็น
ครัง้คราว
สีหนา้ บ่งบอกว่า รอ้งไห้
ตลอดเวลา กรีดรอ้งหรือสะอ้ืน
บ่น/รอ้งบ่อยๆตลอด
รอ้งไห ้(ใหค้ะแนนใน
กรณีท่ีเด็กไมใ่ช้
เครือ่งช่วยหายใจ)
ไมร่อ้งไห้ รอ้งครางหรือ คร า่ครวญ
บ่น/รอ้งเป็นครัง้คราว
รอ้งไหต้ลอดเวลา กรีดรอ้งหรือ
สะอ้ืน บ่น/รอ้งบ่อยๆตลอด
การปลอบโยน รูส้ึกพอใจ ผอ่นคลาย สงบเป็นครัง้คราวเมือ่ไดร้ับ
การปลอบโยนดว้ยการสมัผสั
กอด หรือ พดูคยุ การเบ่ียงเบน
ความสนใจ
ยากตอ่การปลอบโยน
หรือท าใหส้งบ
The modified FLACC Scale (Johanson, & Kokinsky, 2009)
The COMFORT Behavior Scale
* Developer: Monique van Dijk & Colleague>> Modify the COMFORT Scale in
the Year 1999# The COMFORT Behavior Scale
>> A psychologist, nurse, senior researcher on pain, sedation in neonates & infants
>> Sophia Children’s Hospital, Netherland>> Infant-3 years



The Cardiac Analgesic Assessment Scale (CAAS)(Suominen, Caffin, Linton, McKinley, Ragg, Davie, & Eyres, 2004)
ตวัช้ีวดั คะแนน
0 1 2
ขนาดรมูา่นตา ≤ 2 มม.
(ขนาดหัวเข็มหมดุ)
3-4 มม.
(ขนาดกลาง)> 4 มม.
(ขยาย)
อตัราการหายใจ อยู่ในชว่งของคา่ปกติ เพิ่มขึน้ 5-15%
จากคา่ปกติ
เพิ่มขึน้ > 15%
จากคา่ปกติ
ความดนัโลหิต อยูใ้นชว่งของคา่ปกติ เพิ่มขึน้ 5-15%
จากคา่ปกติ
เพิ่มขึน้ > 15%
จากคา่ปกติ
การตอบสนองการ
หายใจและการ
เคลื่อนไหว
ไมต่อบสนอง ไอและเคลื่อนไหว
เล็กนอ้ย และกลบัสูภ่าวะ
ปกตหิลงัจากหยดุการ
กระตุน้
ไอและ/หรือเคลื่อนไหว
รนุแรงเป็นเวลา > 1
นาที หลงัจากหยดุการ
กระตุน้

MAPS-Revised (Ramelet, Rees, Bulsara, & Abu-Saae, 2007)
ตวัชีว้ดั 0 1 2 คะแนน
อตัราการเตน้
หัวใจและ/หรือ
ความดนัโลหิต
อยู่ในชว่งของค่าปกติ เพ่ิมขึน้มากกว่า
10%
เพ่ิมขึน้มากกว่า 20%
แบบแผนการ
หายใจ
ไมม่ีการเปลี่ยนแปลง เร่ิมหายใจล าบาก
เพิ่มขึน้
หายใจล าบากรนุแรงขึน้ พรอ้มๆกบั
การรอ้งไหเ้งยีบๆ หรือรอ้งไหเ้บาๆ
การแสดงออก
ทางใบหนา้
สงบผอ่นคลาย หนา้นิว่/ค้ิวขมวด หนา้นิว่/ค้ิวขมวดบ่อยครัง้ พรอ้มๆกบั
รอ้งเงยีบๆหรือรอ้งเบาๆ
การเคลื่อนไหว ไมม่ีการเคลื่อนไหว
หรือเคลื่อนไหวมี
เป้าหมาย
เคลื่อนไหว
ตลอดเวลา
แขง็ทื่อ และ/หรือการเคลื่อนไหวของ
ร่างกายถกูจ ากดั (เชน่ ไมส่ามารถงอ/
ดดัตวัได)้
ภาวะการปลกุตืน่ สงบเงยีบ หรือหลบั
(ปลกุตื่นงา่ย)
มีปฎิกริยาตอบสนอง
มากเกินไป
ไมต่อบสนอง
Special Population
* Cognitive Impairment: >> Cerebral palsy, Autism, Syndrome
with CI>> The revised FLACC Scale (Provide
information)
* Drown syndrome (0-3 y):>> COMFORT-B Scale

Smart Phone Application for Assessing Pain in Children
* Smartphone app: New standard of pain measurement>> Diary pain record:
# Self- report pain intensity, # Duration, # location, # medication, # pain management
>> Improved # Maximize adherence with reporting# Real time record # Validity of report compared with
paper


Which scales?

* วยั & พฒันาการ:
>> ความแตกตา่งของการแสดงออกถึงความปวด
# Premature baby: “Shut down” # Full term # Infant
# Intubated & Level of concious
>> Assessment cues: # PPIP: Physiological change &
gestational age & Behaviors # NFCS: การแสดงออกทางใบหนา้ 10 ตวัชีว้ดั

* งา่ย & สะดวก & รวดเร็วใชเ้วลานอ้ยในการประเมนิ
* Practical:
>> ใชไ้ดจ้ริงในทางปฏิบตัิ
* Validity & Reliability: >> Consistent & reliable score
>> มรีายงาน & การบนัทึกที่แนน่อน
* วดัมากกว่า 1 dimension
ผ ูป้ระเมินเขา้ใจความหมายในองคป์ระกอบยอ่ยของแต่
ละรายการในเครือ่งมือประเมินความปวดจรงิไม่ ???
ใชเ้ครือ่งมือประเมินความปวด// ใชค้วามร ูส้ึก???

Update Intervention
Pharmacologic & Non-PharmacologicPain Management

หลกัการพ้ืนฐาน
*Minimize intensity and duration of pain
*Maximize coping and recovery
*Break the pain-anxiety cycle

Update on Pharmacological Pain Management in Children
* Old drugs used in new ways>> Epidural>> Intrathecal:
# Morphine (Cardiac surgery, Children 5-55Kg)
>> Intranasal
* Pharmaceutical companies working feverishly to find new non‐opioid treatment alternatives

* By the clock* With the child* By the appropriate route* WHO Ladder of Pain Management
World Health Organization (WHO)
Principles of Pediatric Acute Pain Management

By the Clock
* Regular scheduling ensures a steadyblood level
* Reduces the peaks and troughs of PRNdosing
* PRN = as little as possible???

With the Child
* Analgesic treatment should be individualized according to:
>> The child’s pain>> Response to treatment>> Frequent reassessment>> Modification of plan as required
Correct Route
* Oral* Nebulized* Buccal* Transdermal* Sublingual* Intranasal* IM ไมน่ยิมใหใ้นเด็ก* IV / SC* Rectal

World Health Organization (WHO)

Intranasal Medications
* Use concentrated solution>> Ketamine 50 mg/ml
# Limited data # Use with caution until further studied
>> Fentanyl 50 mcg/ml*>> Midazolam 5mg/ml
* Use an atomizer>> If > 1ml divide between nares>> Aim spray toward turbinates/pinna>> Rapid CSF levels

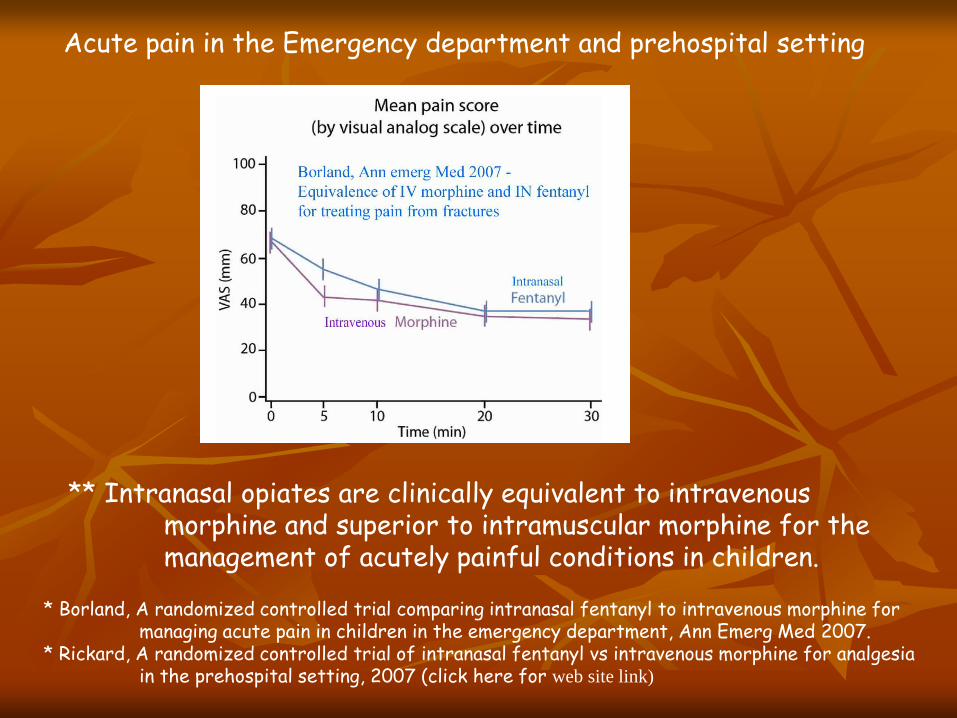
Acute pain in the Emergency department and prehospital setting
** Intranasal opiates are clinically equivalent to intravenous morphine and superior to intramuscular morphine for the management of acutely painful conditions in children.
* Borland, A randomized controlled trial comparing intranasal fentanyl to intravenous morphine for managing acute pain in children in the emergency department, Ann Emerg Med 2007.
* Rickard, A randomized controlled trial of intranasal fentanyl vs intravenous morphine for analgesia in the prehospital setting, 2007 (click here for web site link)

Update Non-pharmacological Pain Management
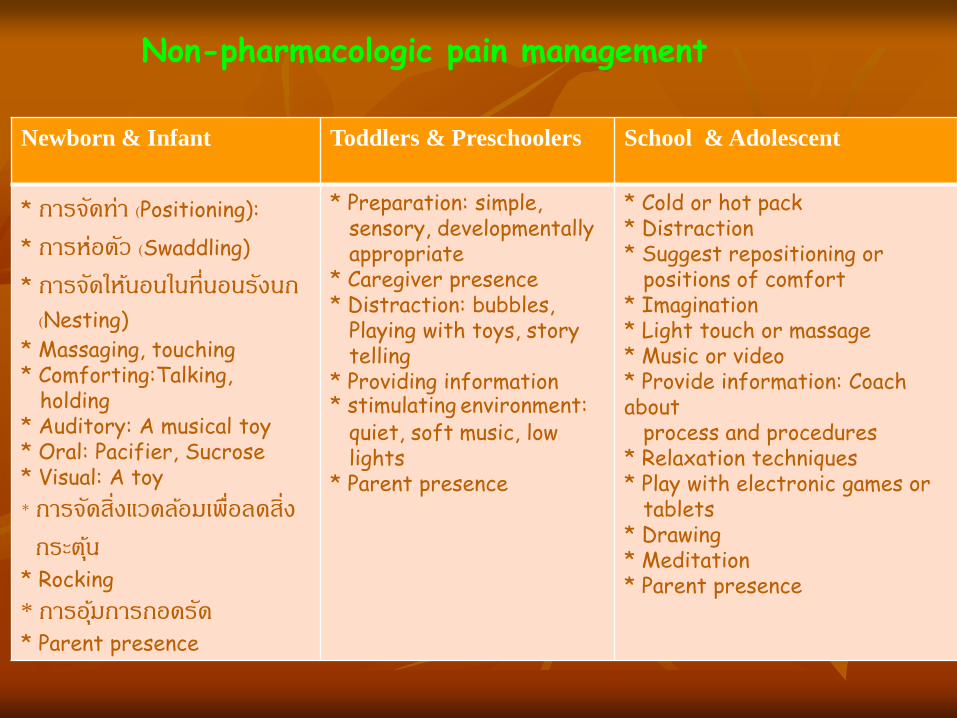
Newborn & Infant Toddlers & Preschoolers School & Adolescent
* การจดัทา่ (Positioning):
* การห่อตวั (Swaddling)
* การจดัใหน้อนในท่ีนอนรงันก
(Nesting)
* Massaging, touching* Comforting:Talking,
holding * Auditory: A musical toy * Oral: Pacifier, Sucrose * Visual: A toy
* การจดัสิ่งแวดลอ้มเพื่อลดสิ่ง
กระตุน้
* Rocking
* การอุม้การกอดรดั
* Parent presence
* Preparation: simple, sensory, developmentally appropriate
* Caregiver presence* Distraction: bubbles,
Playing with toys, story telling
* Providing information* stimulating environment:
quiet, soft music, low lights
* Parent presence
* Cold or hot pack* Distraction* Suggest repositioning or
positions of comfort* Imagination* Light touch or massage* Music or video* Provide information: Coach about
process and procedures* Relaxation techniques* Play with electronic games or
tablets* Drawing* Meditation* Parent presence
Non-pharmacologic pain management


Transmission point Non-Pharmacologicintervention of pain
Pharmacologicintervention
* Block by activation large fibers and preventing nocicdeptive
transmission* Block by binding
opioid receptors in spinal core
*Skin stimulation massage
* Acupuncture* Amplication of heat
and cold* Touch
* Epidural analgesia* Intrathecal
analgesia * Opioids
Pain intervention that alter spinal cord transmission of pain

Transmission point Non-Pharmacologicintervention of pain
Pharmacologicintervention
* Increase stimuli to the brain
* Increase blood flow to targeted areas, decrease pain chemicals
* Increase endorphines
*Distraction*Imagery*Relaxation* Biofeedback
* Systemic Opioids
Pain intervention that alter receptor site transmission of pain

สิ่งแวดลอ้ม
เด็ก พยาบาล
ผูด้แูล
การพยาบาลอยา่งมีสว่นร่วม
ความปวด บรรเทาปวด
------------------------------------------
2
3 4
1
รปูแบบการพยาบาลเพื่อบ าบดัความปวดในผูป่้วยเด็ก
(1= การพยาบาลอย่างมสีว่นร่วม 2,3,4=การสื่อสาร & การมสีว่นร่วม)

การมีสว่นรว่ม( partnership) ในการดแูลเพื่อชว่ยบ าบดัความปวดใน
เด็ก หมายถึง การเขา้มามสีว่นร่วมของเด็ก ผูด้แูล กบัพยาบาล
(รวมถึงเจา้หนา้ท่ีทางการแพทยท์ี่เกี่ยวขอ้งกบัการจดัการความปวด)
เพ่ือชว่ยกนับ าบดัความปวดใหเ้ด็กที่ไดร้บัการผา่ตดัและถกูจ ากดัการ
สื่อสารดว้ยท่อชว่ยหายใจ
เคารพในความเป็นบคุคล (dignity and respect) และตอ้งค านงึถึงความ
แตกตา่งของสมาชกิแตล่ะคนในครอบครวัและความแตกตา่งของแตล่ะ
ครอบครวั วฒันธรรม ความเชือ่ ค่านยิมของครอบครวัและสงัคม
การเขา้มามีสว่นรว่ม
* การแลกเปลี่ยนขอ้มลูที่เกี่ยวขอ้งกบัความปวดและการจดัการความปวด
ของเด็ก
* การประเมนิความปวดและแปลผลพฤตกิรรมการแสดงออกที่บ่งบอกว่า
เด็กปวด
* การวางแผนเพ่ือจดัการความปวด การเขา้มาร่วมตดัสินใจในการเลือก
วิธีจดัการความปวดใหแ้กเ่ด็ก
* การร่วมจดัการความปวดและการตดิตามประเมนิผลตัง้แตเ่ด็กเขา้รับ
การรกัษาในโรงพยาบาลจนกระทัง่เด็กมสีขุภาพดแีละกลบับา้น
* การเขา้มามสีว่นร่วมในการควบคมุปัจจยัสิ่งแวดลอ้มรอบๆ
***การสื่อสาร***
องคป์ระกอบ
* เด็ก
* ผูด้แูล/ผูป้กครอง
* พยาบาล/เจา้หนา้ที่ทางการแพทย์
* สิ่งแวดลอ้มรอบตวัเด็ก

เด็ก
* สื่อความปวดได้>> สื่อดว้ยค าพดู
>> แสดงออกทางพฤตกิรรม
* มกีลยทุธใ์นการลดปวดดว้ยตนเอง
พยาบาล
* มคีวามรูค้วามเขา้ใจในองคค์วามรูเ้ร่ืองความปวดในเด็ก
* มคีวามสามารถประเมนิพฤตกิรรมความปวดในทารก
แรกเกิดถึงขวบปีแรกได้
* มคีวามรูค้วามเขา้ใจ & สามารถใหก้ารบ าบดัความ
ปวดโดยการใชย้าและไมใ่ชย้าได ้
* ใหเ้วลา & ใหค้วามส าคญั
* ใหค้ าแนะน าและสอนวิธีการลดความปวด
ผ ูด้แูล/ผ ูป้กครอง
* มคีวามร ูใ้นเร่ืองความปวด:
>> ความปวดหลงัผา่ตดัจะลดลงเมือ่เวลาผา่นไป
* ประเมนิความปวดของเด็กไดถ้กูตอ้ง
* รูวิ้ธีจดัการความปวดโดยการไมใ่ชย้า
และชว่ยบรรเทาความปวด
* ม ีattitude ที่ดตีอ่การรกัษาดว้ยยา: การตดิยา

สิ่งแวดลอ้ม
* สิ่งแวดลอ้มที่ไมม่ชีวิีต: แสง สี เสียง กลิ่น
* สิ่งแวดลอ้มที่มชีวิีต: ยงุ มด ผูม้าเย่ียมไข ้
* ขจดัสิ่งแวดลอ้ม & จดัสิ่งแวดลอ้มที่คุน้เคย:
>> โทรทศัน ์ต ูป้ลา
>> น าสิ่งที่เด็กรกัมาอยู่ใกล้ๆ
Nursing Education Intervention
* Education and training
>> Pain assessment & management with improvement of paramedic confidence and performance (self-efficacy)
>> Inter-ratter reliability
* Mean experience: 4.04 (5.9) years. * 37% could assess pain without pain scales. * 49.4% had not previously heard of pain scales, * 47.1% used a pain scale in their routine practice.
An Educational Intervention to Improve Nurses’
Understanding of Pain in Children in Western India
(Dongara, Nimbalkar, Phatak, Patel, & Nimbalkar, 2017)

ทศันคติ ความร ู ้และความเช่ือของท่านเกี่ยวกบั
ความปวดในเด็กปรบัเปลี่ยนแลว้ยงั????
ท่านมีความร ู ้มีเวลา ใชก้ารจดัการความปวดโดย
การไม่ใชย้าช่วยบรรเทาปวดใหแ้กเ่ด็ก???

หายปวดแลว้ยงัค่ะ?