Embed Size (px)
Citation preview

Eduard Gratacós
www.fetalmedicinebarcelona.org/
UPDATE ON DIAGNOSIS AND MANAGEMENT OF
FETAL GROWTH RESTRICTION
BCNatal – Barcelona Center of Maternal-Fetal and Neonatal Medicine!Hospital Clínic and Hospital Sant Joan de Déu, Universitat de Barcelona!
www.fetalmedicinebarcelona.org/

www.fetalmedicinebarcelona.org/
Placental insufficiency = high risk of IUFD and fetal/neonatal acidosis!Fetal Smallness = higher risk of placental insufficiency
Risk of placental insufficiency
10
50
Feta
l wei
ght
cent
ile
“Small fetuses”
Placental “respiratory” !smallness = risk distress + IUFD
Non-“respiratory” smallness != no distress/IUFD risk

www.fetalmedicinebarcelona.org/
1. Identify small fetus!
2. Identify placental insufficiency (FGR vs. SGA)!
3. Determine timing of delivery

www.fetalmedicinebarcelona.org/
Neonatal and Fetal GA-adjusted “normal” weight in the same population

Mula 2013, Lobmaier 2013www.fetalmedicinebarcelona.org/
IMPROVING DETECTION: THE DEFINITION OF “RESTRICTION”!Birthweight inverse relation with perinatal outcome AND brain-cardiac remodelling
RESE
ARCH

www.fetalmedicinebarcelona.org/
1. Identify small fetus!
2. Identify placental insufficiency (FGR vs. SGA)!
3. Determine timing of delivery

www.fetalmedicinebarcelona.org/
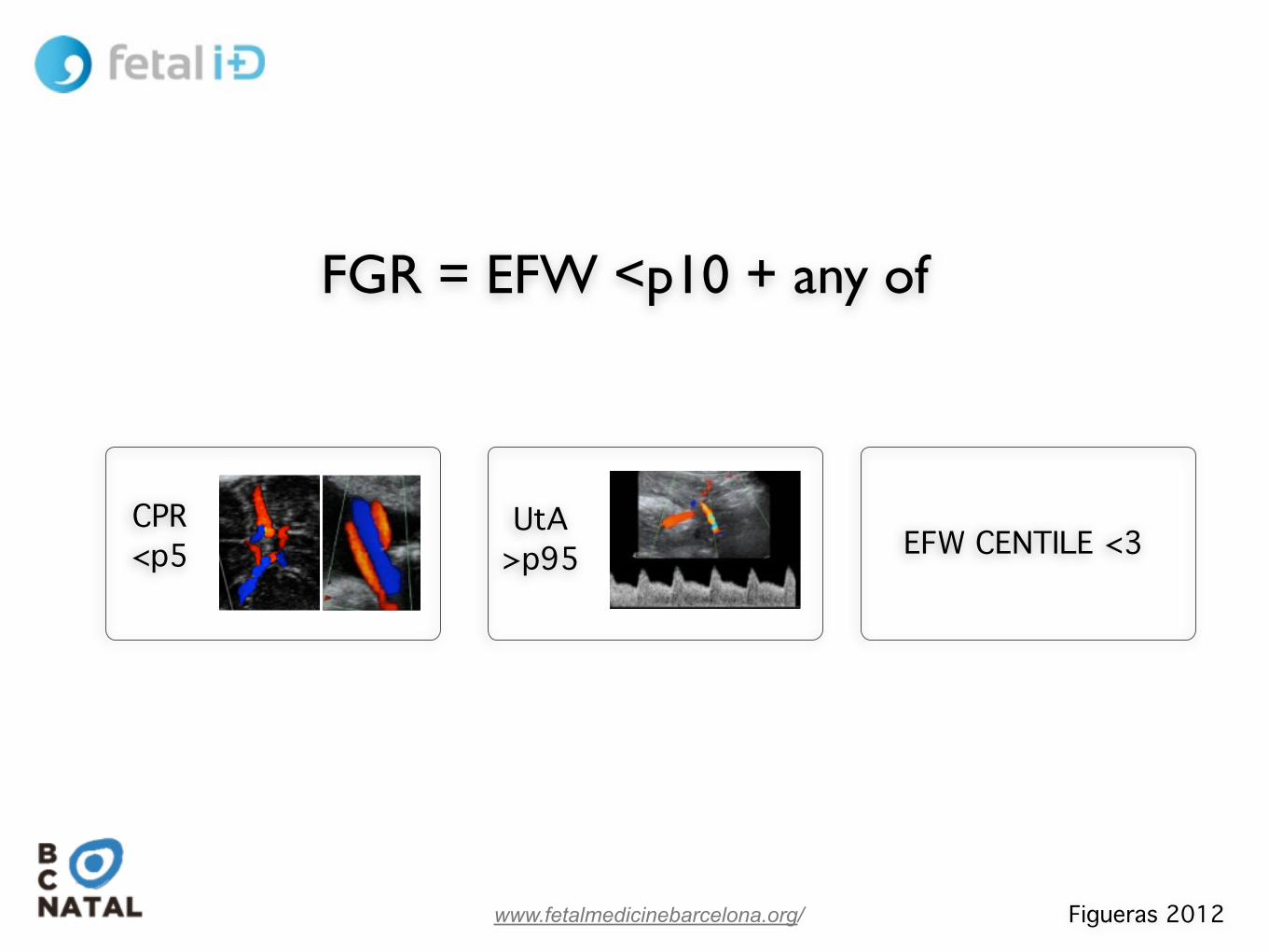
SGA Unknown (constitutional + others)
IUGR Placental insufficiency
ISOLATED FETAL SMALLNESS = POORER PROGNOSIS!Perinatal and Long-term Outcomes
Exclude extrinsic cause
Exclude primary fetal defect
Poor perinatal outcome + IUFD!(Doppler) Signs of adaptation
Perinatal outcome normal - No IUFD!NO signs of adaptation
FGR vs. SGA: DIFFERENT MANAGEMENT

www.fetalmedicinebarcelona.org/
Constitutionally small Placental insufficiency Extrinsic cause
Primary fetal defect
SGA FGR
The discovery of UA and hemodynamics of IUGR
FGR = abnormal UA Doppler
20 30 4025 35
0
N cases
N cases
UA Doppler +!(EARLY-ONSET)
UA Doppler N!(LATE-ONSET)
Savchev 2013

www.fetalmedicinebarcelona.org/
FGR = abnormal UA Doppler?
20 30 4025 35
0
N cases
N cases
UA Doppler +!(EARLY-ONSET)
UA Doppler N!(LATE-ONSET)
Savchev 2013
not a
nymore

Risk of CS for distress and/or neonatal acidosis!
N=509 SGA + 509 controls
www.fetalmedicinebarcelona.org/
UtA >p95
CPR <p5
EFW CENTILE <3
%
Prognostic criteria for poor outcome among small fetuses with normal UA Doppler
Figueras 2012
www.fetalmedicinebarcelona.org/
UtA >p95
CPR <p5 EFW CENTILE <3
Figueras 2012
FGR = EFW <p10 + any of

www.fetalmedicinebarcelona.org/
Distribution of cases when IUGR = abnormal UA Doppler
Savchev 2013

www.fetalmedicinebarcelona.org/
Distribution of cases when IUGR = abnormal CPR or UtA or EFW<p3
Savchev 2013
www.fetalmedicinebarcelona.org/
SGA Unknown (constitutional + others)
IUGR Placental insufficiency
ISOLATED FETAL SMALLNESS = POORER PROGNOSIS!Perinatal and Long-term Outcomes
Exclude extrinsic cause
Exclude primary fetal defect
Poor perinatal outcome + IUFD!(Doppler) Signs of adaptation
Perinatal outcome normal - No IUFD!NO signs of adaptation
FGR vs. SGA: DIFFERENT MANAGEMENT

www.fetalmedicinebarcelona.org/
1. Identify small fetus!
2. Identify placental insufficiency (FGR vs. SGA)!
3. Determine timing of delivery
www.fetalmedicinebarcelona.org/
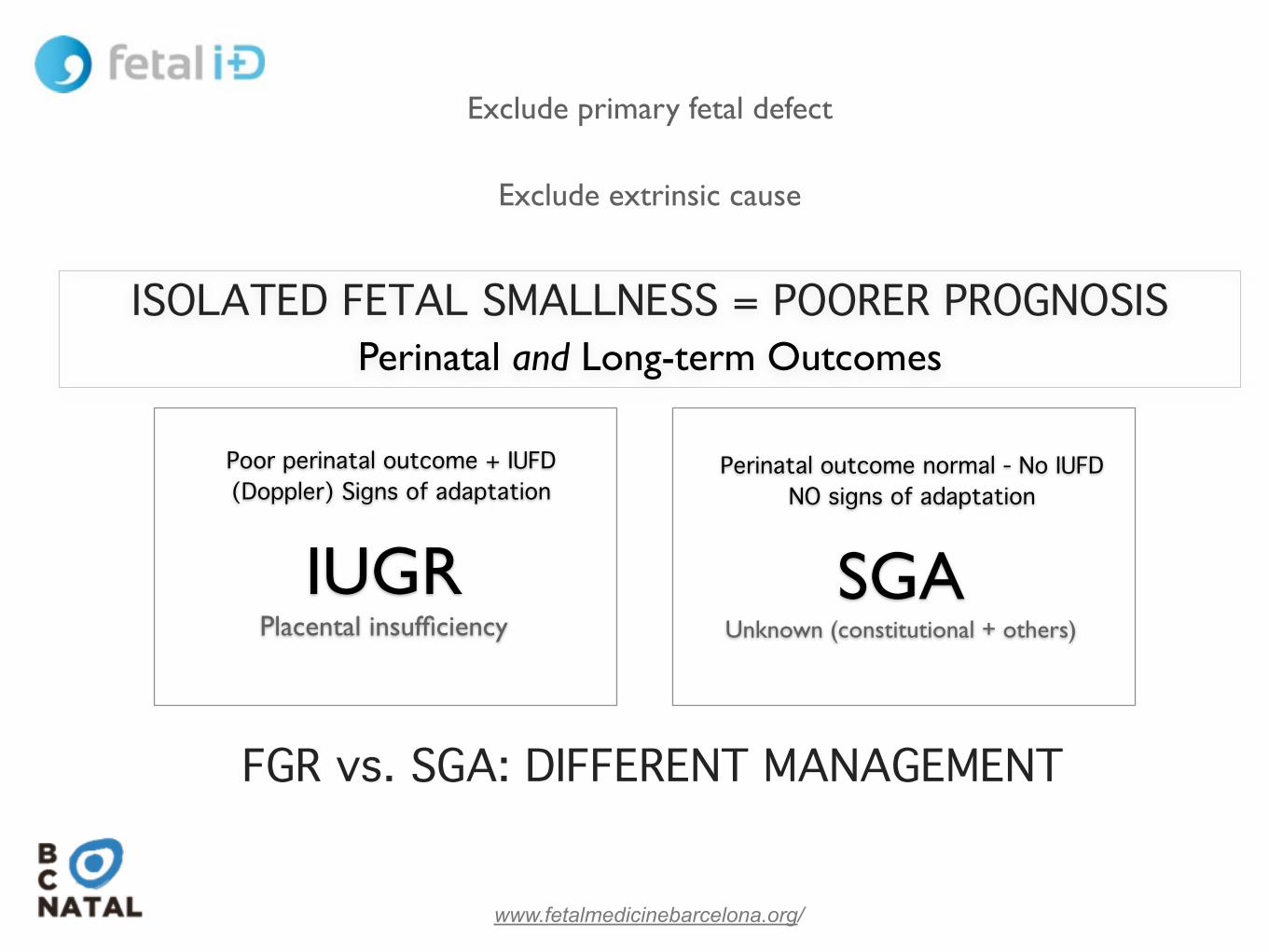
IUGR = abnormal CPR or UtA or EFW<p3
Savchev 2013

Early-severe High risk IUFD preterm
www.fetalmedicinebarcelona.org/
IUGR = abnormal CPR or UtA or EFW<p3
Management = when should we deliver?
Savchev 2013
Late-mild Low risk IUFD (high at term)

deliver when risks are:
www.fetalmedicinebarcelona.org/
RATIONALE FOR AN INTEGRATED STAGE-BASED APPROACH TO THE MANAGEMENT OF FGR
PLACENTAL DISEASE HYPOXIA ACIDOSIS SERIOUS INJURY DEATH
cardiac ischemiaDiastolic failure
Systolic cardiac failure
Centralization
Increment placental impedance
cCTG: reduced STV
Diagnostic/chronic markers!DIFFERENCE !FGR VS SGA
Prognostic/Acute markers!INDICATION ABOUT THE SHORT-TERM RISK!
OF IUFD/BRAIN INJURY
IVIIIIIIStage fetal deterioration
HIGHMILDMINIMALRisks of prematurity

www.fetalmedicinebarcelona.org/
Protocol IUGRFirst step: UtA + CPR + EFW = SGA or IUGR
CPR!<p5
Ut A !>p95
MCA!<p5
DV !(a rev)
CGT decelerations of reduced short-term
variability
REDV DV >p95
!I low EFW (<p3) or mild placental
resistance / redistribution!!!
II Severe placental resistance / redistribution!
!!
III Severe hemodynamic adaptation - Low suspicion acidosis!
!!
IV High suspicion of acidosis - !High risk of death
AEDV AoI >p95

VERY HIGH HIGH MODERATE
Mort. >90% 50% <10% Morb. >90% 50%
www.fetalmedicinebarcelona.org/
<26w 26-28 28-30 30-34 34-37
IUGR!Management protocol according to severity stages
Deliver at Any 7me
Risk of IUFD/brain injury
DV(a-‐), cCTG, CTG dec
Stage IV
Mode CS
Follow-‐up Hours/Daily
30
DV>p95, REDV
III
CS
1-‐2 d
34
AEDV, AoI>95
II
CS or LI
2/w
37
EFW<p3, CPR <p5, UtA>95
I
LI
1/w
LOW

www.fetalmedicinebarcelona.org/
First goal:!Identify of small fetus (EFW<p10) and classify as FGR
vs SGA according to CPR, UtA and EFW<3.!!
Second goal: !Decide timing of delivery and followup scheme: use a
stage-based integrated protocol.

www.fetalmedicinebarcelona.org/
Early vs. Late onset IUGR
Return

20 30 4025 35
www.fetalmedicinebarcelona.org/
EARLY-ONSET LATE-ONSET
PREECLAMPSIA
IUGR
PREECLAMPSIA + IUGR
1 %
1 %
4-8 %
4-8 %

www.fetalmedicinebarcelona.org/
IUGR
SGA?
20 30 4025 35
0
3
6 %
IUGR= low CPR or high UtA or EFW<p3 or low PlGF
EARLY IUGR (1-2%) LATE IUGR (5-6%)
PROBLEM: MANAGEMENT PROBLEM: DIAGNOSIS
Placental disease: high (UA+, PE high) Placental disease: low (UA-, PE low)
Hypoxia ++: systemic CV adaptation Hypoxia +/-: central CV adaptation
Tolerance to hypoxia. Natural history Low tolerance: no natural history
High mortality and morbidity Low mortality but poor long outcome.
32w @diagnosis

www.fetalmedicinebarcelona.org/
FETAL DETERIORATION IN PLACENTAL INSUFFICIENCY
PLACENTAL DISEASE COMPENSATED HYPOXIA DECOMPENSATED HYPOXIA SERIOUS INJURY!DEATH
cardiac ischemia!Diastolic failure
Systolic cardiac failure
Centralization
Increment placental impedance
growth
MIDDLE CEREBRAL A. <p5
CPR <p5
DUCTUS VENOSUS >p95 and a-
CTG ABNORMAL
UTERINE A. >p95
cCTG: reduced short-term variability
Ao ISTHMUS >p95
UMBILICAL A. >p95

www.fetalmedicinebarcelona.org/
FETAL DETERIORATION IN PLACENTAL INSUFFICIENCY !EARLY VS LATE IUGR (>34s)
PLACENTAL DISEASE COMPENSATED HYPOXIA DECOMPENSATED HYPOXIA SERIOUS INJURY!DEATH
cardiac ischemia!Diastolic failure
Systolic cardiac failure
growth
UMBILICAL A. >p95
DUCTUS VENOSUS >p95 and a-
CTG / BPP ABNORMAL
Placental injury <30%
mild hypoxia no cardiovascular adaptation
minimal tolerance to hypoxia
MIDDLE CEREBRAL A. <p5
CPR <p5
UTERINE A. >p95
Ao ISTHMUS >p95
Centralization
Increment placental impedance

www.fetalmedicinebarcelona.org/
IUGR
SGA?
20 30 4025 35
0
3
6 %
IUGR= low CPR or high UtA or EFW<p3 or low PlGF
EARLY IUGR (1-2%) LATE IUGR (5-6%)
PROBLEM: MANAGEMENT PROBLEM: DIAGNOSIS
Placental disease: high (UA+, PE high) Placental disease: low (UA-, PE low)
Hypoxia ++: systemic CV adaptation Hypoxia +/-: central CV adaptation
Tolerance to hypoxia. Natural history Low tolerance: no natural history
High mortality and morbidity Low mortality but poor long outcome.
32w @diagnosis

www.fetalmedicinebarcelona.org/
Parameters for fetal follow up in IUGR
Return

www.fetalmedicinebarcelona.org/
umbilical artery normal and anormal hemodynamics
DS
Cardiac pump normal function
Cardiac pump abnormal function
Placental status
<30%
placenta + cardiac ischemia

middle cerebral artery normal and abnormal hemodynamics
[marked vasodilation]
[normal waveform]
[mild vasodilation]
Normal oxygenation
hypoxia

www.fetalmedicinebarcelona.org/
IPUA=p80
Cerebroplacental ratio is more sensitive than UA or MCA alone
CPR <p5
IPMCA=p20
=+

www.fetalmedicinebarcelona.org/
30 % venous return
REFLECTS DIASTOLIC PRESSURE IN RIGHT (AND LEFT) HEART
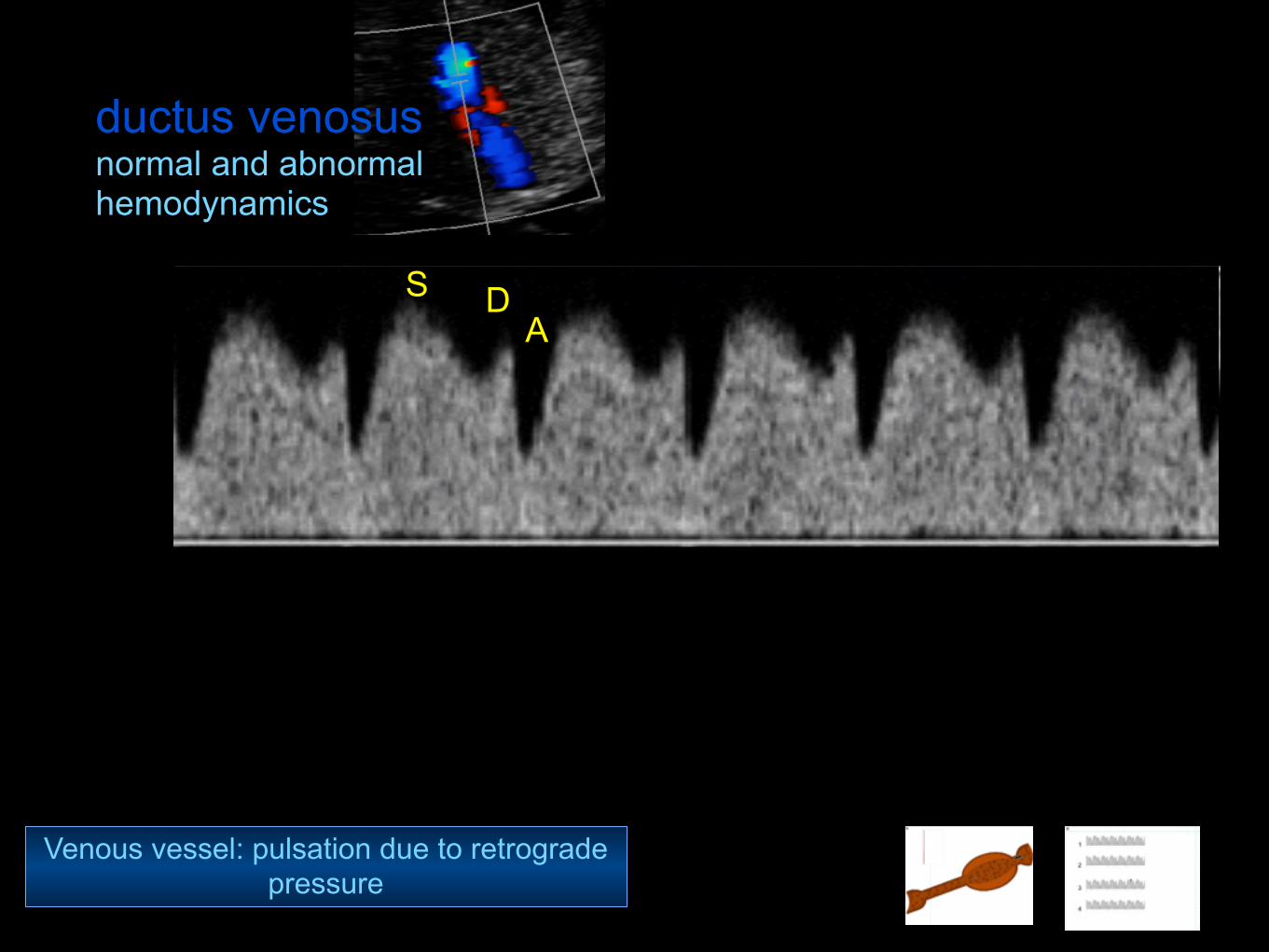
ductus venosus normal and abnormal hemodynamics
Venous vessel: pulsation due to retrograde pressure
S DA

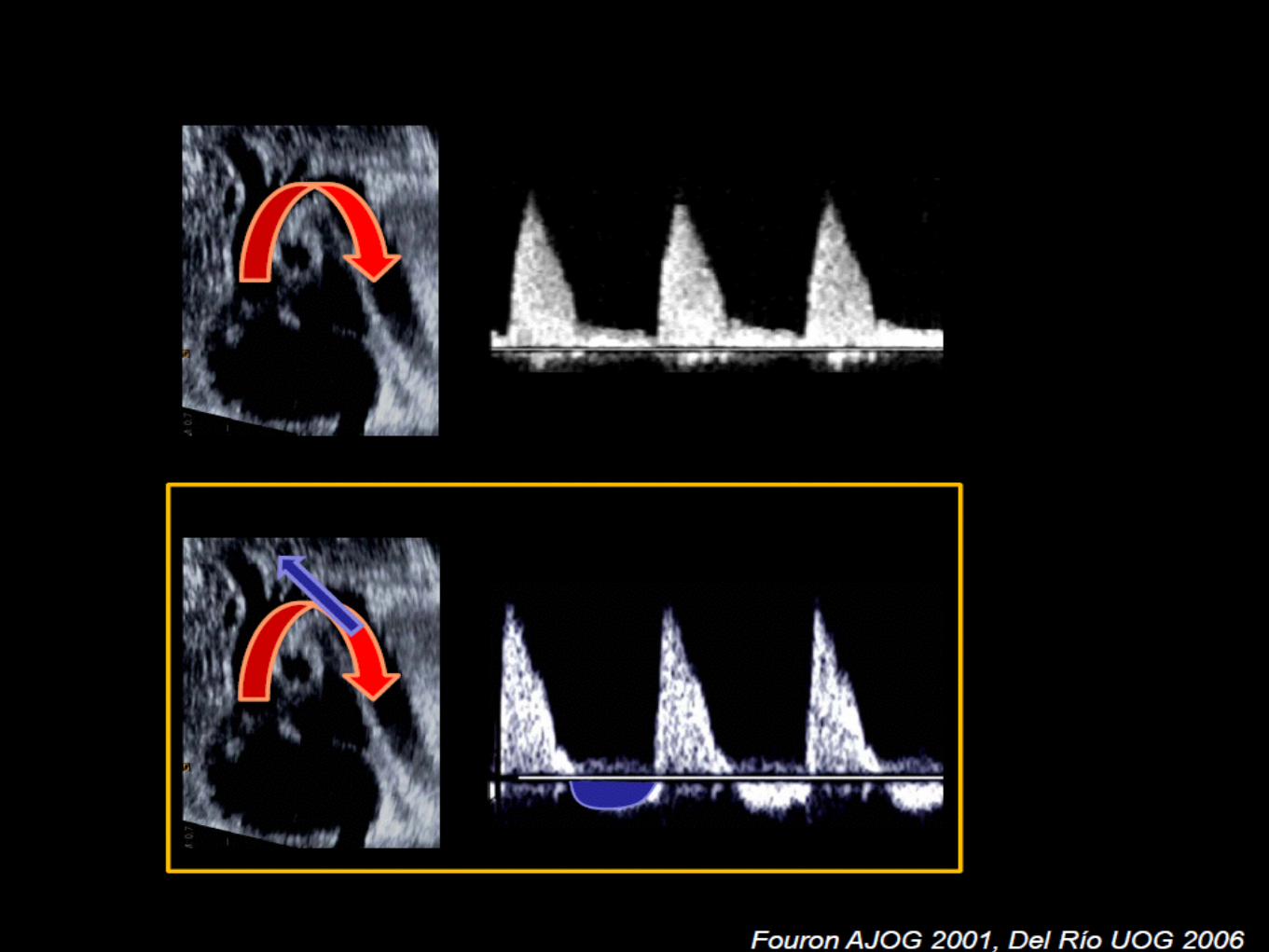
ductus venosus normal and abnormal hemodynamics
compliance right chambers: effect sobre
on venous return
DS A
P
P
P
P
Myocardial ischemia
compliance
no



www.fetalmedicinebarcelona.org/
When and how to deliver
Return

Early-severe High risk IUFD preterm
www.fetalmedicinebarcelona.org/
IUGR = abnormal CPR or UtA or EFW<p3
Management = when should we deliver?
Savchev 2013
Late-mild Low risk IUFD (high at term)
Stage II to IV PROTOCOL
Stage I >37w

Perinatal >90% 30-‐40% <10% Mortality
www.fetalmedicinebarcelona.org/
<26 26-28 29-30
Baschat 2003 Hecher 2003 Grivell 2009 Cruz-‐Lemini 2012
Early-onset IUGR!PROBLEM #1: MORTALITY
DVa (rev)
Yes No
60%
19%
cCTG-‐STV<3 ms
Pathological CGT
BPP!IUFD 23% in BPP=6 and 11% in BPP=8!
Poor correlation with DVa(rev)!Cochrane: poor contribution to prediction
Baschat 2007, Kafur 2008, Lalor 2010,
31-34
Stage IIStage IIIStage IV

Neurological >90% 30-‐40% <10% Morbidity
www.fetalmedicinebarcelona.org/
<29 29-32 >32.0
Fouron 2004 Del Rio 2008 Cruz-‐Mar7nez 2012
Early-onset IUGR!PROBLEM #2: (NEUROLOGICAL) MORBIDITY
(%)
0
15
30
45
60
Controls IUGR ant AoI IUGR REV AoI
Neonatal brain US anomalies in 30-34w IUGR

37-38 w (+/- check lung maturity)!
Do not use prostaglandins (Foley/Balloon)!
Select high risk cases (MCA Doppler)
www.fetalmedicinebarcelona.org/
Late-onset IUGR !PROBLEM #1: WHEN AND HOW TO DELIVER

www.fetalmedicinebarcelona.org/
Cesarean section for fetal distress after labor induction in term SGA according to MCA Doppler
(N=202)
Cruz et al, 2010
(OVERALL RISK OF CS AFTER INDUCTION 80 %)
0"
10"
20"
30"
40"
50"
60"
70"
Cesarean"sec1on"for"distress"
Neonatal"acidosis"
AGA"
SGA"normal"MCA"
SGA"abnormal"MCA"
JAMA Pediatrics 2013
www.fetalmedicinebarcelona.org/
≥
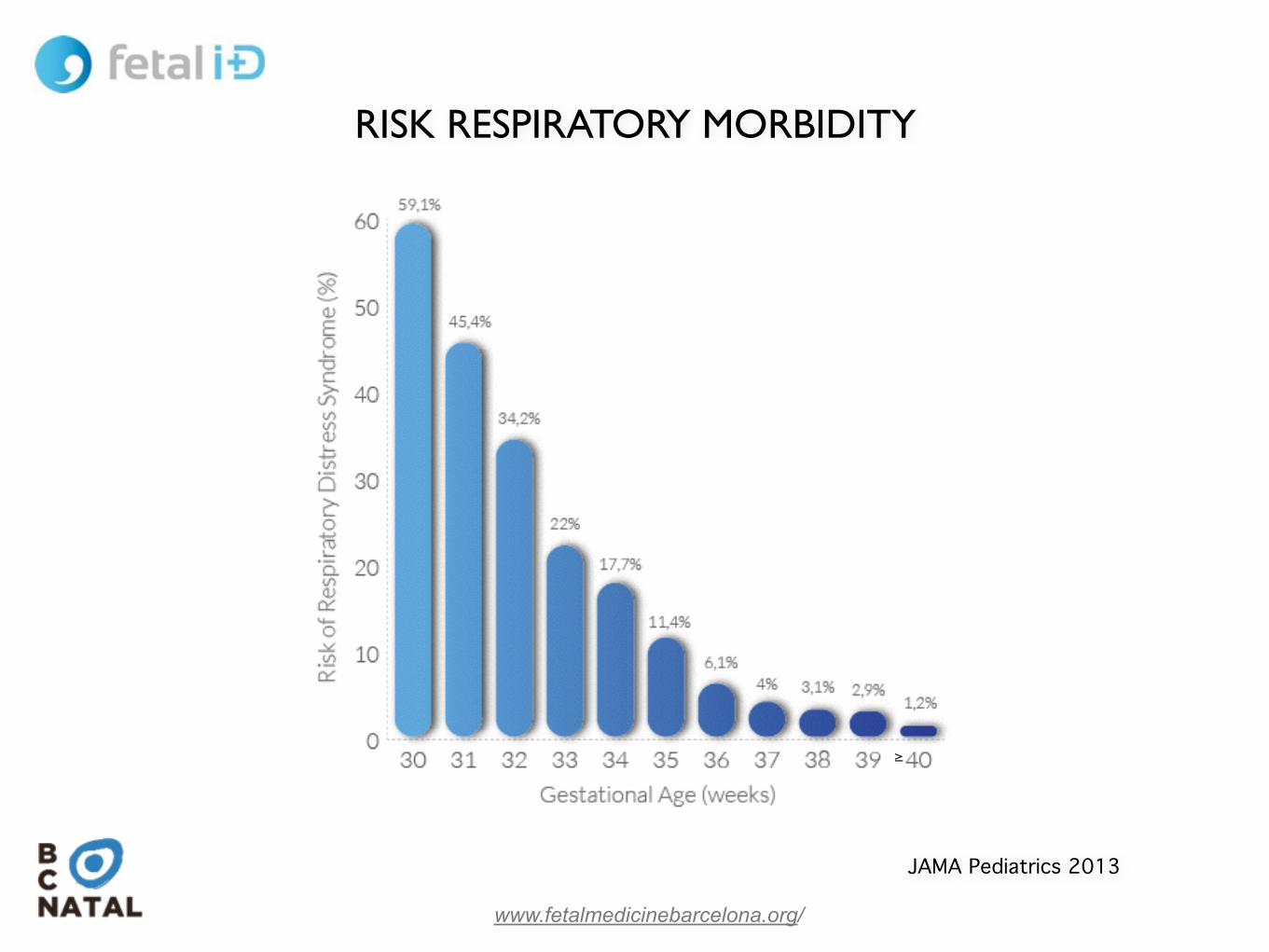
RISK RESPIRATORY MORBIDITY

Bonet, UOG 2014
www.fetalmedicinebarcelona.org/
• N=144!• Singleton
pregnancies !• 29.0 - 38.6 w !• Axial thoracic
sectionNeonatal Respiratory Morbidity (*):!• Respiratory Distress
Syndrome!• Transient tachypnea of
newborn
(*) RDS: Respiratory symptoms (eg, g r u n7ng , fl a r i n g , t a c hypnea , retrac7ons), O2 requirement + chest Rx + NICU admission TT: chest Rx impression + clinical diagnosis by clinician in charge. JAMA 2010
Patient�&�Provider�Informationwww.quantusFLM.com
Sabino�Arana�38�1Ͳ108028�Barcelona,�SpainCIF:�BͲ65084675
PATIENT NAME: CLINIC NAME:
PATIENT ID: REFERRING/ORDERING CLINICIAN:
QUANTUSFLM�ID: REPORT�DATE:�(dd/mm/yyyy)
Name�Surname
NHC12345678
btechͲ123
Complete�Center�Name
Clinician�Name�Surname
01/01/2000
Sample�Information
GESTATIONAL�AGE:
US�ACQUISITION�DATE:(dd/mm/yyyy)
REQUEST�DATE:(dd/mm/yyyy hh:mm)
##�weeks #�days
01/01/2000
01/01/2000�00:00
Test�Result���NEONATAL�RESPIRATORY�MORBIDITY
QUANTUSFLM�ID:
RESULT:
Theoretical risk for ##�weeks of�gestation:
quantusFLM risk:
RECOMMENDATION:(dd/mm/yyyy)
AUTHORIZED�SIGNER/S:
Technical�Responsible:Elisenda Bonet�i�Carné,�MSc
Imatge Firma
CLINICAL�DATA�Ͳ SPECIFICATIONSAccuracy 87%�(95%�CI:82Ͳ90%)
Sensitivity 91%�(95%�CI:77Ͳ98%)
Specificity 86%�(95%�CI:82Ͳ90%)
Positive Predictive Value 47%�(95%�CI:35Ͳ59%)
Negative Predictive Value 98%�(95%�CI:96Ͳ99%)
TEST DESCRIPTIONquantusFLM™ offers an automatic assessment of neonatal respiratory morbidity risk using an ultrasoundimage of the lateral axial transverse section of the fetal thorax at the level of the 4Ͳchamber section of thefetal heart. quantusFLM™ is based on quantitative ultrasound texture analysis to extract information fromultrasound images and a classifier which uses the extracted information to assess the risk. Test resultdepends on the delineation of the fetal lung and incorporated the gestational age. Neonatal respiratorymorbidity is defined as respiratory distress syndrome or transient tachypnea of the newborn.Test has been validated in singleton pregnancies from 28.0 to 39.0 weeks of gestation. Test are neitherintended nor validated for use in pregnancies with fetal structural abnormalities, chromosomalabnormalities, multiple pregnancies or maternal BMI>35. This result should not be considered as a finalindication but as additional information to be considered in evaluation of the patient.
quantusFLM Test�is�intended�for�clinical�use�and�should�not�be�regarded�as�investigational�or�for�research.�Present�result�has�been�obtained�using�quantusFLM X.X.�Under�the�previous�of�Law�15/1999�normative,�we�inform�you�that�your�data�will�be�included�in�a�data�base�owned�by�TransmuralBiotech,�S.L.�for�its�clinical�treatment.�You�may�exercise�the�rights�of�access,�rectification,�cancellation�and�opposition�contacting�us�at�[email protected].
REFERENCE:�Quantitative ultrasound texture analysis of�fetal�lung to�predict neonatal�respiratory morbidity.�UOG�(2014)
NonͲInvasive Assessment of�therisk of�Neonatal�Respiratory morbidity
Graphic�Test�Result NEONATAL�RESPIRATORY�MORBIDITY�RISK
HIGH LOWRISK RISK
100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0%
Theoretical Risk*
quantusFLM Risk
100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0%
LOW�RISK
##.#�%
##.#�%
Review results with patient
btechͲ123

www.fetalmedicinebarcelona.org/
Performance of Quantus FLM and comparison with currently used lab
8quantusFLM® ha sido validado mediante 144 muestras ciegas.

www.fetalmedicinebarcelona.org/
Late IUGR with MCA<p5 Planned delivery at 37.0 weeks
LOW RISK =1.5%
Deliver
HIGH RISK =25%
Wait and follow-up until 37.6-38.0
PERSONALIZED: FETAL LUNG MATURITY
RISK RESPIRATORY MORBIDITY
BASELINE GA-ADJUSTED = 4%

www.fetalmedicinebarcelona.org/
Early and late-onset determines different severity, fetal response and natural history!
!
Doppler is the main tool for follow-up and timing of delivery in stage II to IV!
!
Stage I: challenge is to determine best timing and mode of delivery!
Return

Perinatal >90% 30-‐40% <10% Mortality
www.fetalmedicinebarcelona.org/
<26 26-28 >28
Baschat 2003 Hecher 2003 Grivell 2009 Cruz-‐Lemini 2012
BEING SMALL EARLY IN PREGNANCY IS A PROBLEM!PROBLEM #1: MORTALITY
DVa (rev)
Yes No
60%
19%
cCTG-‐STV<3 ms
Pathological CGT

Neurological >90% 30-‐40% <10% Morbidity
www.fetalmedicinebarcelona.org/
<29 29-32 >32.0
Fouron 2004 Del Rio 2008 Cruz-‐Mar7nez 2012
Early-onset IUGR!PROBLEM #2: (NEUROLOGICAL) MORBIDITY
(%)
0
15
30
45
60
Controls IUGR ant AoI IUGR REV AoI
Neonatal brain US anomalies in 30-34w IUGR

www.fetalmedicinebarcelona.org/
Significant increase in the risk of adverse perinatal outcome!
Hershkovitz et al. Ultrasound Obstet Gynecol 2000!Severi et al. Ultrasound Obstet Gynecol 2002!Figueras et al . Eur J Obstet Gynecol Reprod Biol 2008
e<p95
SGA
SGA = constitutionally small?
Significant increase in the risk of adverse neurodevelopment!
Eixarch et al. Ultrasound Obstet Gynecol 2008!Severi et al. Ultrasound Obstet Gynecol 2002!Figueras et al . Eur J Obstet Gynecol Reprod Biol 2008
BEING SMALL LATE IS ALSO A PROBLEM
www.fetalmedicinebarcelona.org/
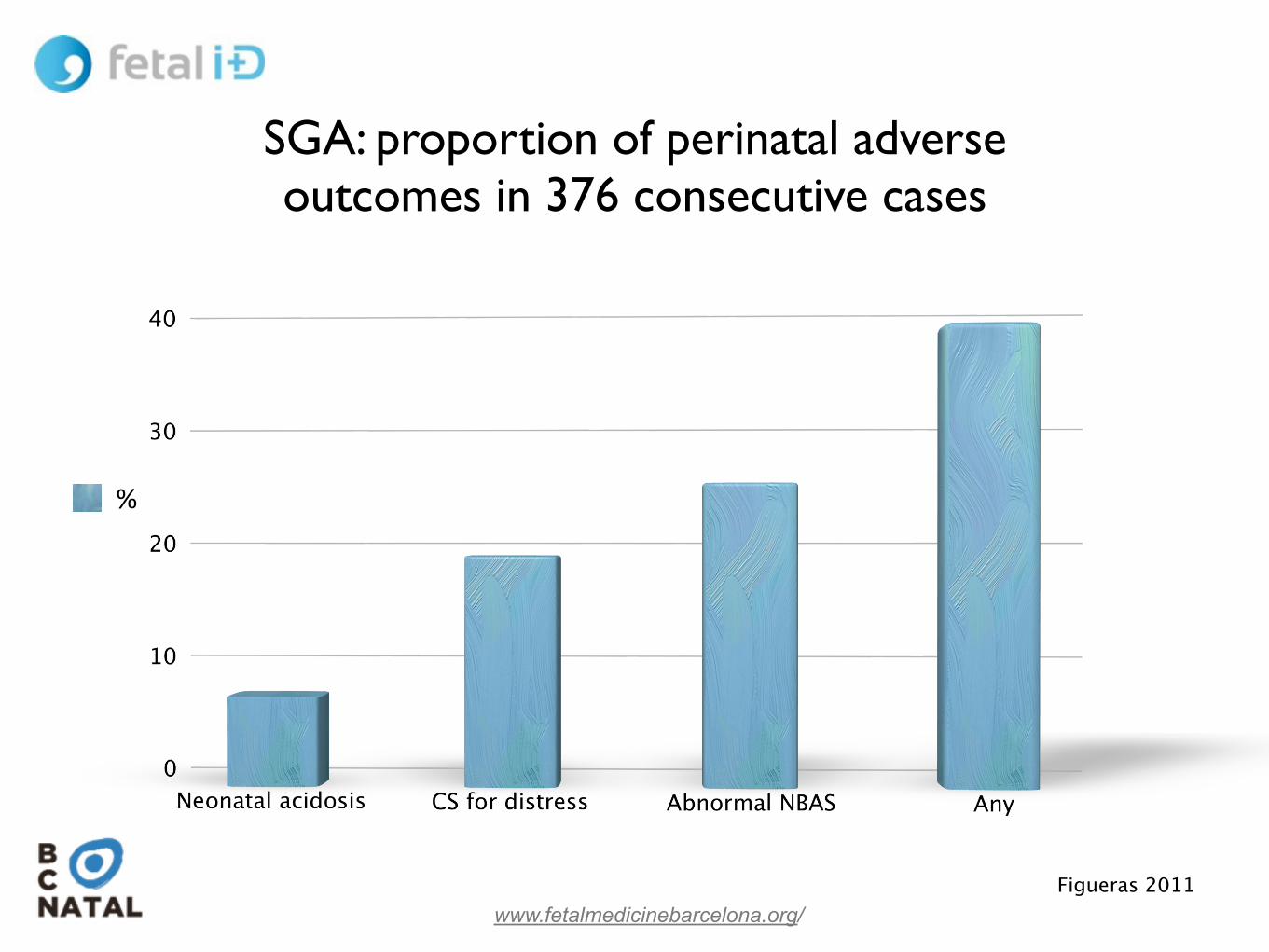
%
Figueras 2011
SGA: proportion of perinatal adverse outcomes in 376 consecutive cases
www.fetalmedicinebarcelona.org/
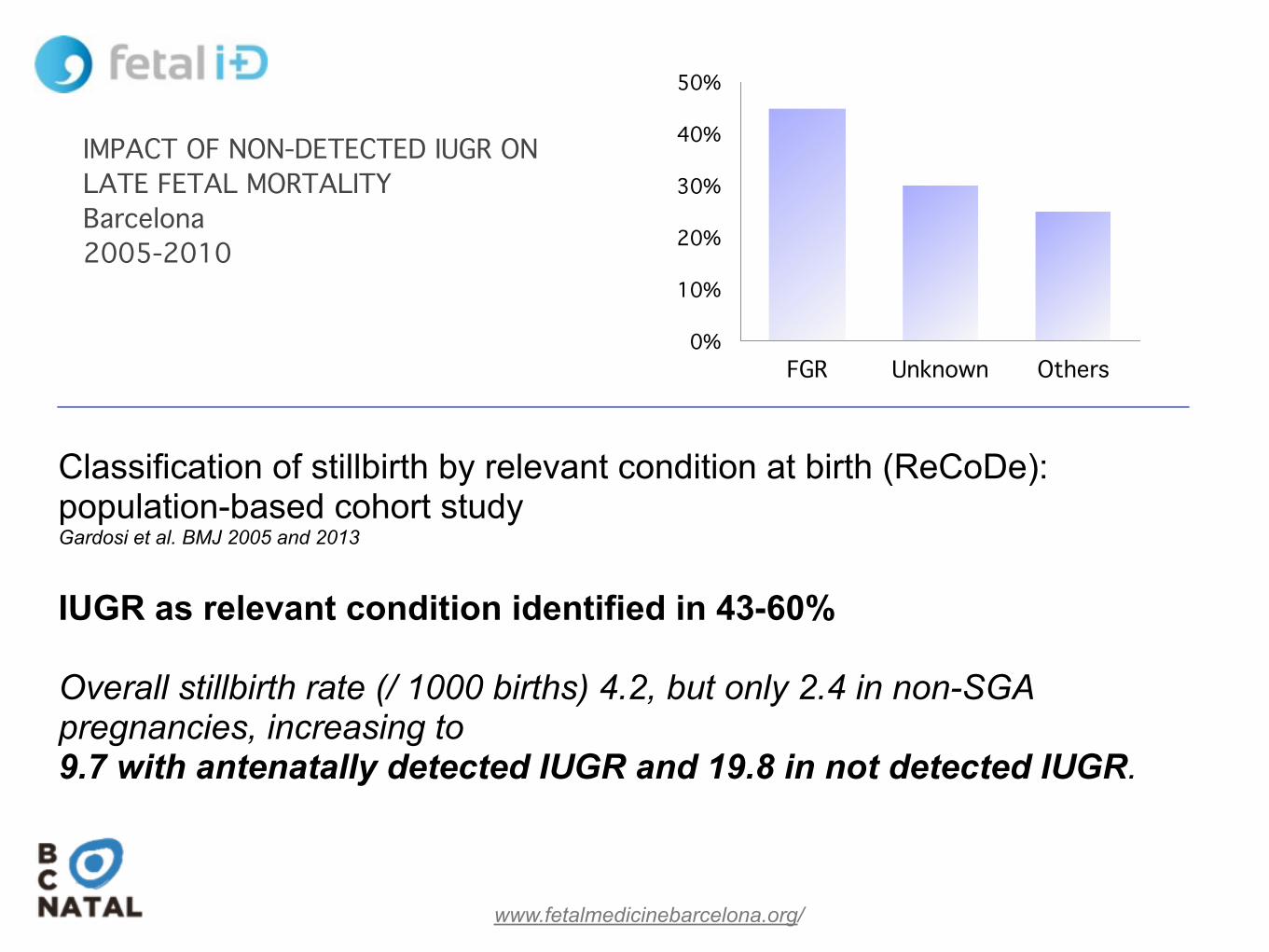
IMPACT OF NON-DETECTED IUGR ON LATE FETAL MORTALITY!Barcelona!2005-2010
0%
10%
20%
30%
40%
50%
FGR Unknown Others
25%30%
45%
Classification of stillbirth by relevant condition at birth (ReCoDe): population-based cohort study Gardosi et al. BMJ 2005 and 2013 !IUGR as relevant condition identified in 43-60% !Overall stillbirth rate (/ 1000 births) 4.2, but only 2.4 in non-SGA pregnancies, increasing to 9.7 with antenatally detected IUGR and 19.8 in not detected IUGR.

www.fetalmedicinebarcelona.org/
Neurobehavioral performance of term SGA newborns
* **
**
* p <0.05!Adjusted for GA, maternal age, socioeconomic status and smoking
Satchev, 2012!Geva 2008!
Figueras 2008!Eixarch 2010
N=120 SGA vs !
100 AGA
* * *
Bay
ley
Sco
re
20
40
60
80
100
120
cognitive language motor socio-emotional adaptivebehavior
* * *

www.fetalmedicinebarcelona.org/
control IUGR
Crispi 2012
Crispi 2010
Cardiovascular programming in !SGA / late-IUGRFetuses EFW<p10 evaluated at 5 years!!Classified by CPR, p3 and UtA Doppler:!
•All normal: SGA!•Any abnormal: late-IUGR