Embed Size (px)
Citation preview
Update on Diabetic Eye Disease
Management
Dr Fred Chen
MBBS(Hons), PhD, FRANZCO
Consultant Ophthalmologist
Medical and Surgical Retina
Head, Ocular Tissue Engineering Laboratory, UWA
Director of Clinical Research, Lions Eye Institute
GP education event
2 September 2017

Summary
What’s new in diabetic eye diseases?
Clinical assessment
Treatment options
Treatment outcomes


Rank 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
1 Atorvastatin Atorvastatin Atorvastatin Atorvastatin Atorvastatin Atorvastatin Atorvastatin Rosuvastatin Adalimumab Ledipasvir + sofosbuvir
2 Simvastatin Esomeprazole Rosuvastatin Rosuvastatin Rosuvastatin Rosuvastatin Rosuvastatin Adalimumab Rosuvastatin Adalimumab
3 Esomeprazole Simvastatin Esomeprazol
e Ranibizumab Ranibizumab Ranibizumab Esomeprazole Esomeprazole Aflibercept Ranibizumab
4 Clopidogrel Clopidogrel Clopidogrel Adalimumab Salmeterol/Fl
uticasone Ranibizumab Sofosbuvir
5 Salmeterol/Fluti
casone Salmeterol/Flu
ticasone Salmeterol/Fl
uticasone Salmeterol/Fl
uticasone Atorvastatin
Salmeterol/Fluticasone
Aflibercept
6 Olanzapine Rosuvastatin Simvastatin Ranibizumab Aflibercept Esomeprazole Esomeprazole
7 Omeprazole Olanzapine Ranibizumab Aflibercept Ranibizumab Etanercept Etanercept
8 Venlafaxine Venlafaxine Fluticasone +
salmeterol
9 Pantoprazole Pantoprazole Fingolimod
10 Tioptropium Br Ranibizumab Insulin
Glargine
PBS Drugs sorted by highest government cost 2007-2016
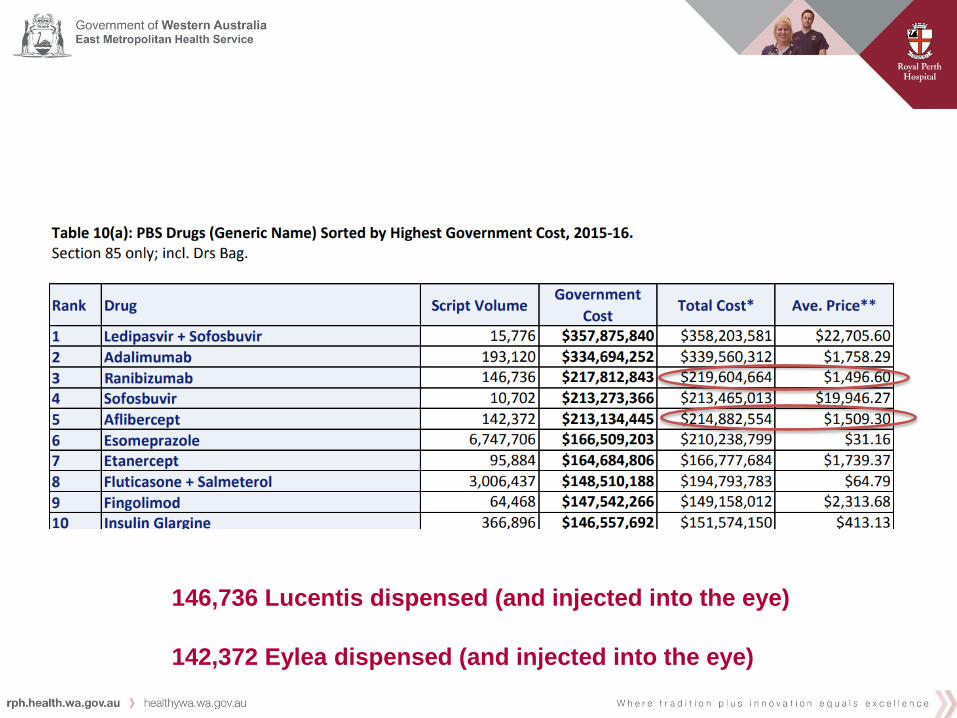
146,736 Lucentis dispensed (and injected into the eye)
142,372 Eylea dispensed (and injected into the eye)
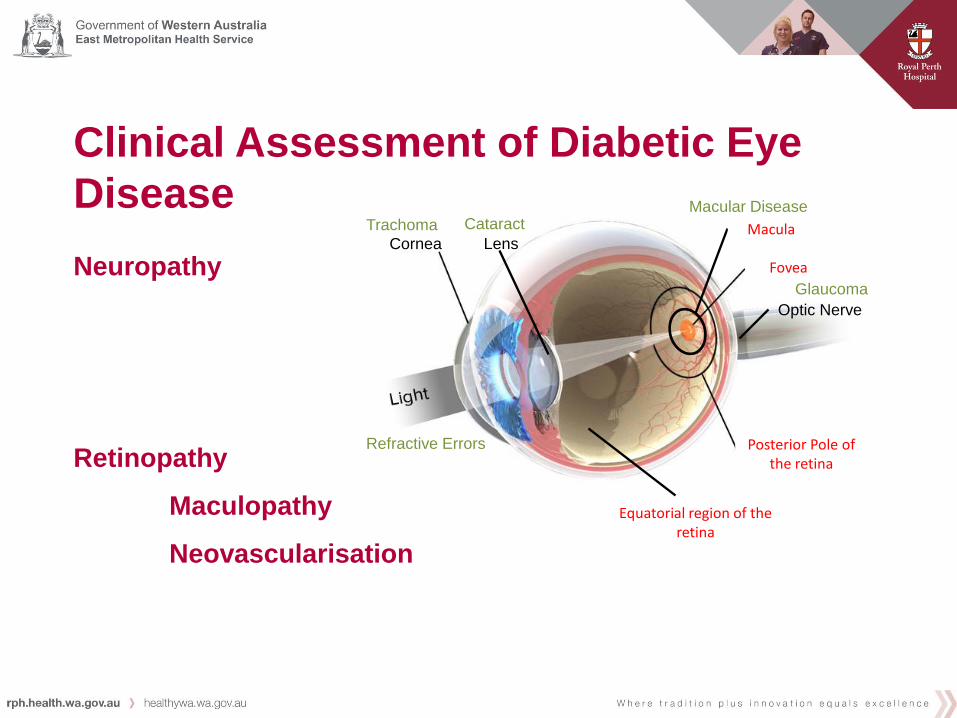
Clinical Assessment of Diabetic Eye
Disease
Neuropathy
Motor: cranial nerve III, IV, VI
Sensory: cranial nerve V (trigeminal) – cornea
Retinopathy
Maculopathy
Neovascularisation
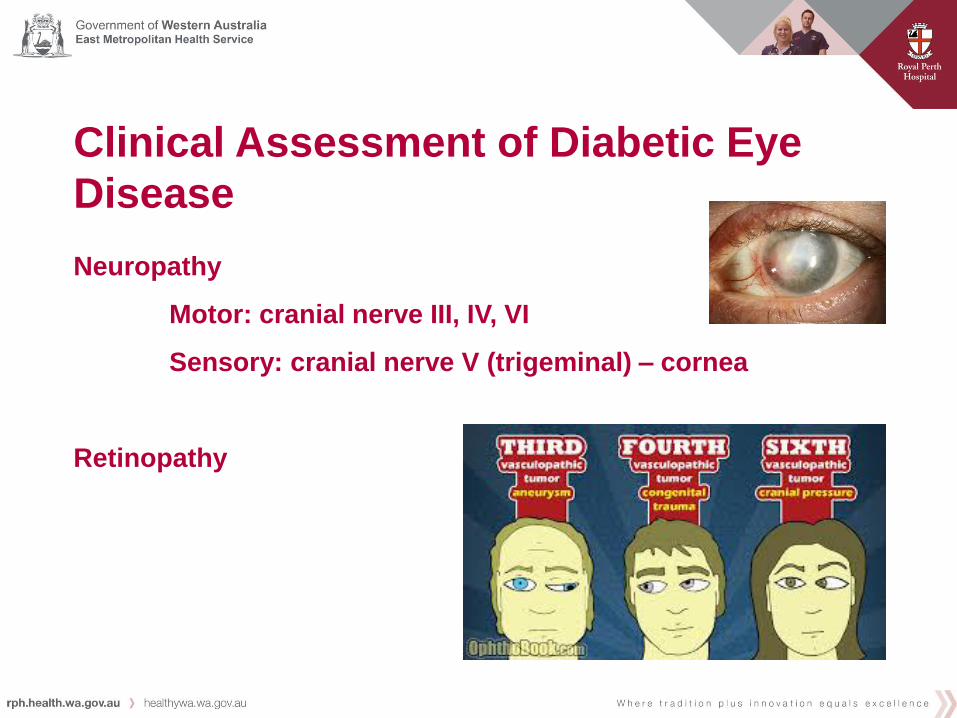
Clinical Assessment of Diabetic Eye
Disease
Neuropathy
Motor: cranial nerve III, IV, VI
Sensory: cranial nerve V (trigeminal) – cornea
Retinopathy
Clinical Assessment of Diabetic Eye
Disease
Neuropathy
Motor: cranial nerve III, IV, VI
Sensory: cranial nerve V (trigeminal) – cornea
Retinopathy
Maculopathy
Neovascularisation
Optic Nerve
Lens Cornea
Fovea
Posterior Pole of the retina
Equatorial region of the retina
Macula Cataract Macular Disease
Refractive Errors
Glaucoma
Trachoma

Clinical Assessment of Diabetic Eye
Disease
Neuropathy
Motor: cranial nerve III, IV, VI
Sensory: cranial nerve V (trigeminal) – cornea
Retinopathy
Maculopathy
Neovascularisation
At 6 m At 4 m
6/60 = 35
6/24 = 55
6/12 = 70
6/6 = 85

Clinical Assessment of Diabetic Eye
Disease
Neuropathy
Motor: cranial nerve III, IV, VI
Sensory: cranial nerve V (trigeminal) – cornea
Retinopathy
Maculopathy
Neovascularisation

Clinical Assessment of Diabetic Eye
Disease
Neuropathy
Motor: cranial nerve III, IV, VI
Sensory: cranial nerve V (trigeminal) – cornea
Retinopathy
Maculopathy
Neovascularisation

Clinical Assessment of Diabetic Eye
Disease
Neuropathy
Motor: cranial nerve III, IV, VI
Sensory: cranial nerve V (trigeminal) – cornea
Retinopathy
Maculopathy
Neovascularisation

Clinical Assessment of Diabetic Eye
Disease
Neuropathy
Motor: cranial nerve III, IV, VI
Sensory: cranial nerve V (trigeminal) – cornea
Retinopathy
Maculopathy
Neovascularisation
Clinical Assessment of Diabetic Eye
Disease
Neuropathy
Motor: cranial nerve III, IV, VI
Sensory: cranial nerve V (trigeminal) – cornea
Retinopathy
Maculopathy
Neovascularisation
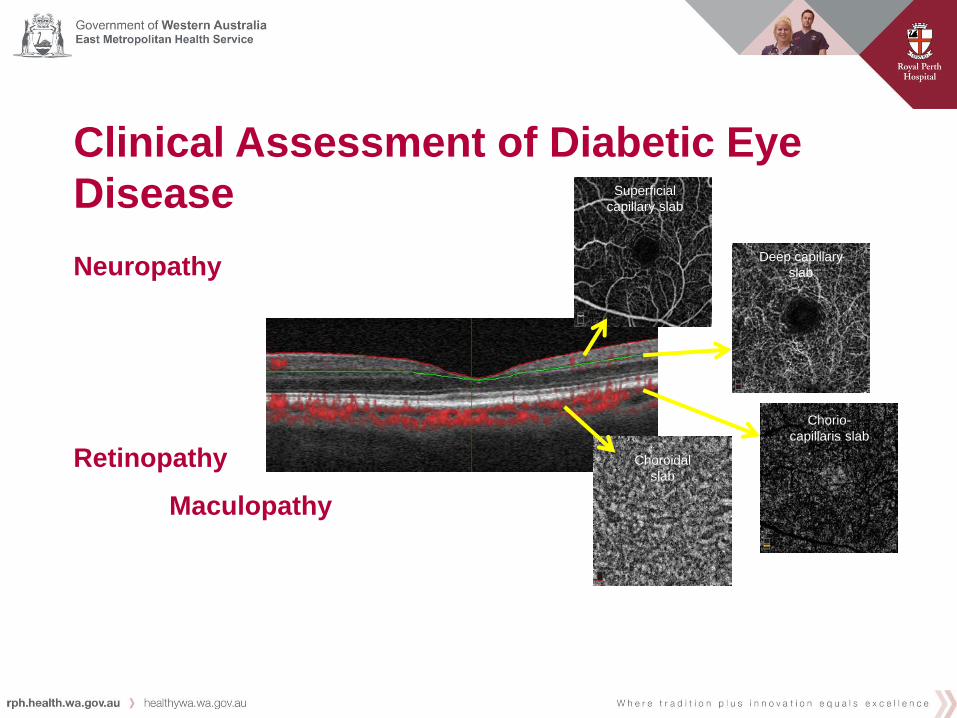
Superficial
capillary slab
Deep capillary
slab
Chorio-
capillaris slab
Choroidal
slab

Clinical Assessment of Diabetic Eye
Disease
Neuropathy
Motor: cranial nerve III, IV, VI
Sensory: cranial nerve V (trigeminal) – cornea
Retinopathy
Neovascularisation

Clinical Assessment of Diabetic Eye
Disease
Neuropathy
Retinopathy
Neovascularisation

Clinical Assessment of Diabetic Eye
Disease
Neuropathy
Retinopathy
Neovascularisation
Clinical Assessment of Diabetic Eye
Disease
Neuropathy
Motor: cranial nerve III, IV, VI
Sensory: cranial nerve V (trigeminal) – cornea
Retinopathy
Maculopathy
Neovascularisation
Don’t forget Cataract and Refractive Error Change

Treatment Options in Diabetic Eye
Disease
Retinopathy
Maculopathy
Anti-VEGF / Steroid injections
Laser
Surgery
Neovascularisation
Laser
Anti-VEGF injections
Surgery
Vascular endothelial growth factor
• Identified in 1983
• Structure in 1996
• Hypoxia stimulate release
• Restore oxygen supply
• Vasculogenesis, angiogenesis, lymphangiogenesis
• Naturally higher in asthma, diabetes
• Pathologically higher in solid cancers, retinopathy
• Family of 5 GF: VEGF-A, B, C, D, Placental GF
• Binds to a tyrosine kinase receptor and neuropilin co-
receptor

• Monoclonal antibody – Bevacizumab (Avastin)
• Variation 1:
– Antibody fragment (Use the Fab portion) – Ranibizumab (Lucentis)
• Variation 2:
– Fc-Fusion protein (Use the Fc portion) – Aflibercept (Eylea)
Anti-vascular endothelial growth factor Drugs



• Abicipar pegol – Design ankyrin repeat protein (DARPin)
– Allergan
• Bolucizumab – ESBA-1008 / RTH-258
– Alcon
• Conbercept – Fusion of IgG and key domains of VEGFR
– Chengdu Kanghong Pharmaceuticals

Intravitreal injection procedure
• Topical anaesthetic (sub conj)
• Povidone iodine / Chlorhex wash
• 3-4 mm behind cornea
• 30G needle
• 0.05 mL of solution squirted in
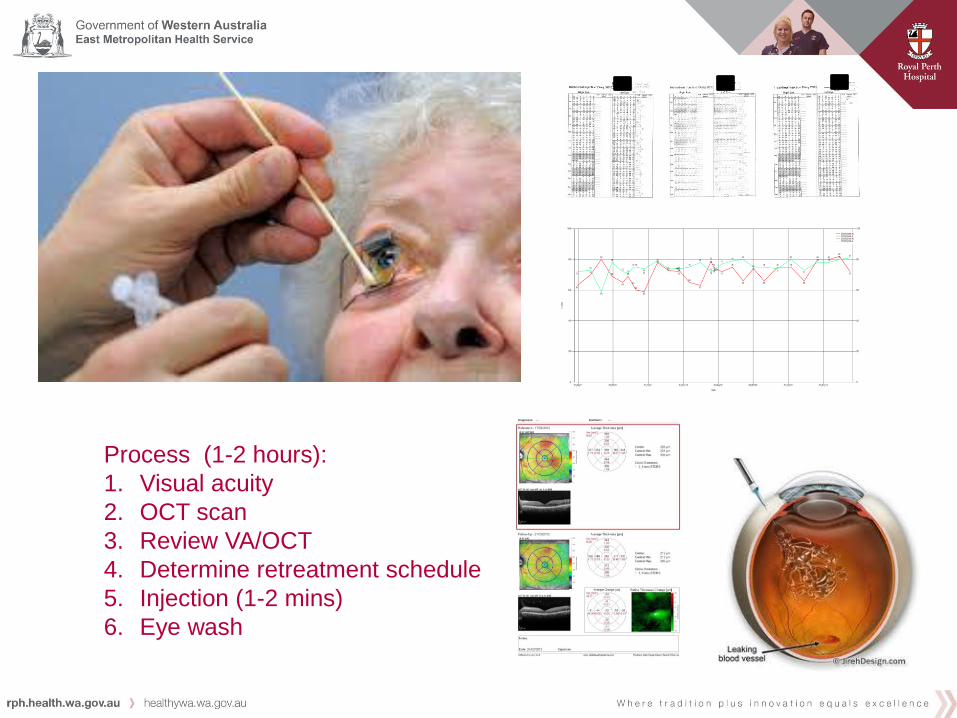
Process (1-2 hours):
1. Visual acuity
2. OCT scan
3. Review VA/OCT
4. Determine retreatment schedule
5. Injection (1-2 mins)
6. Eye wash

Treatment Outcomes in Diabetic Eye
Disease
Retinopathy
Maculopathy
Anti-VEGF / Steroid injections
Neovascularisation
Laser +/- anti-VEGF
Vitrectomy
Anti-VEGF vs Steroid
Anti-VEGF (intravitreal)
Avastin: solution
Lucentis: soluion
Eylea: solution
Steroid (intravitreal)
Triamcinolone (Kenacort A40): suspension
Dexamethasone (Ozurdex implant): sustained release
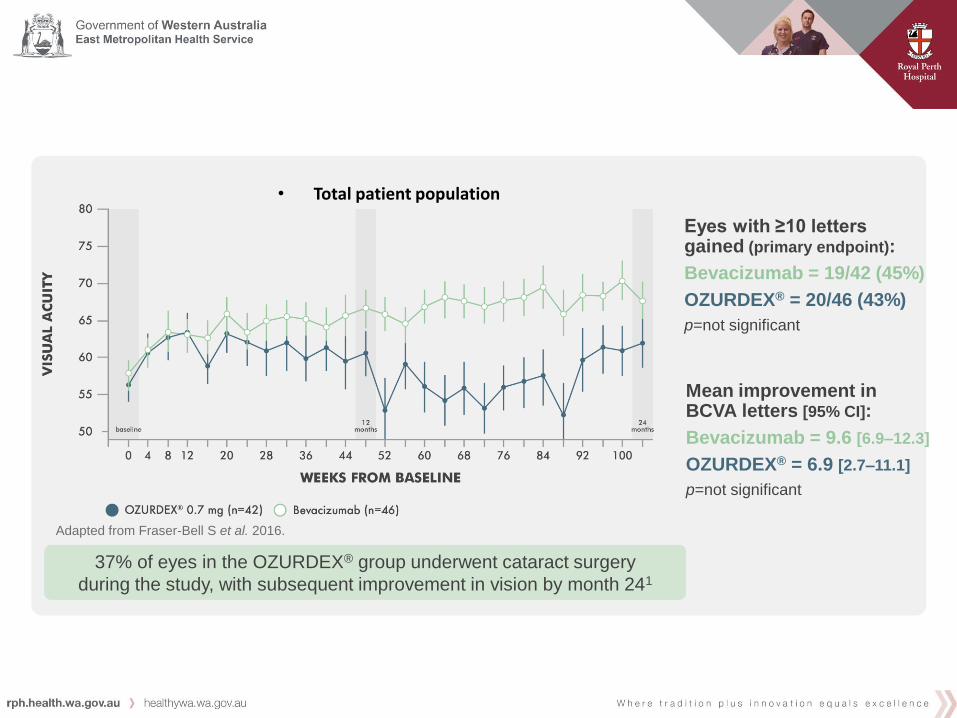
Avastin DEX 0.70
Mean change BCVA 9.6 6.9
P = 0.30
Trend may be driven by phakic eyes developing cataract. 37% of eyes in the OZURDEX® group underwent cataract surgery
during the study, with subsequent improvement in vision by month 241
Adapted from Fraser-Bell S et al. 2016.
• Total patient population
Eyes with ≥10 letters gained (primary endpoint):
Bevacizumab = 19/42 (45%)
OZURDEX® = 20/46 (43%)
p=not significant
Mean improvement in BCVA letters [95% CI]:
Bevacizumab = 9.6 [6.9–12.3]
OZURDEX® = 6.9 [2.7–11.1]
p=not significant

Avastin DEX 0.70
Predicted ? ?
CMT change -122 -198
P = 0.015
CMT peaked at 4 and 8 month visits due to drug wearing off Adapted from Fraser-Bell S et al. 2016.

Avastin DEX 0.70
Number of injection 8.6 2.7
P = not reported
Trend may be driven by phakic eyes developing cataract.

Steroid induced high intraocular pressure

0
1
2
3
4
5
6
7
8
9
10
11
0 4 8 12 16 20 24 28 32 36 40 44 48 52 56 60 64 68 72 76 80 84 88 92 96100104
Sham+pr
ompt
laser
Ranibizu
mab+pro
mpt
laser
Primary outcome time point
DRCR.net study (lucentis, steroid, laser)

DA VINCI Study (Eylea)
Take Home Messages
Diabetic eye disease is not just retinopathy. It included sensory and
motor neuropathy as well as cataract and refractive error
Adequate clinical assessment requires sophisticated instrumentation
and clinical expertise in image interpretation from a Medical Retina
Fellowship to differentiate diabetic retinopathy from other rarer
vascular diseases
Treatment posology is evolving. Currently, anti-VEGF / steroid implant
for centre-involving macular oedema and pan-retinal laser for
proliferative disease with or without anti-VEGF are preferred 1st line.
Early surgical intervention by vitreoretinal surgeons may prevent
permanent blindness from fibrotic complications and failed anti-VEGF
therapy.
Funding support
NHMRC Fellowship, Project Grant
Medical Research Foundation of RPH
The University of Western Australia
Lions Eye Institute
Ophthalmic Research Institute of Australia
Retina Australia





























