Embed Size (px)
Citation preview

Update on Colorectal Cancer
Screening Tests
Source: Levin Bernard et al. Screening and Surveillance for the Early Detection of Colorectal Cancer and Adenomatous Polyps, 2008: A Joint Guideline from the American Cancer Society, the US Multi-Society Task Force on Colorectal Cancer, and the American College of Radiology. CA A Cancer Journal for Clinicians 58(3):130-160, May/June 2008.

Colorectal Cancer
America’s# 2
CancerKiller
America’s# 2
CancerKiller

Expert Panel Opinion Colorectal cancer prevention (not CRC
mortality reduction) should be primary goal of CRC screening.
Tests designed to detect both early cancer and adenomatous polyps should be encouraged if resources available and patients willing to undergo test.

Testing Options for Early Detection of Colorectal Cancer and Adenomatous Polyps for Average-risk
Women and Men Aged 50 Years and Older Partial or full structural exams (invasive tests that detect
adenomatous polyps and cancer)– Flexible sigmoidoscopy every 5 years– Colonoscopy every 10 years– Double-contrast barium enema every 5 years– Computed tomographic colonography every 5 years
Fecal tests with high test sensitivity* (noninvasive tests that primarily detect cancer)– Annual guaiac-based fecal occult test (gFOBT) – Annual fecal immunochemical test (FIT)– Stool DNA test
*Note: Expert panel does NOT recommend gFOBT testing in doctor’s office as a single-panel test following digital rectal exam.

Limitations and Requirements of Fecal Tests
Less likely to prevent cancer compared with invasive tests
Must be repeated at regular intervals to be effective
If abnormal, an invasive test (colonoscopy) will be needed

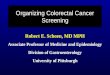
Stool DNA TestNew Recommended Test

Colorectal cancerA series of genetic defects
NormalNormal CarcinomaCarcinoma
5q(APC)alterations
K-RASmutation
17p (p53)alterations
Colonic epithelium
Benignneoplasia
LargerTumor
Malignantneoplasia
18q alterations
Adenoma AdvancedAdenoma

Stool DNA Test Prototype assay of this test (version 1.0)
– 23 DNA markers assayed» 21 point mutations in K-ras, APC, and p53» 1 microsatellite instability marker: BAT-26» DNA Integrity Assay (DIA)
– Minimum 30 grams of stool required– Specific for human DNA - diet not needed
Currently available assay (version 1.1)– Same DNA marker panel– Incorporates technical advances in processing and
specimen preservation to increase test sensitivity

Stool DNA Screening Process
PhysicianSends
Requisitionto Lab
Lab ProvidesCollection and
Shipping Materialsto Patient
Patient CollectsStool at Home
Patient ReturnsSpecimen to Lab
Physician
:
PhysicianCommunicates
Results to Patient
Stool DNA AnalysisIs Performed in Lab
and Reported to
DNA AlterationIdentified
Perform colonoscopy
No DNA AlterationIdentified
Continue screening
Ice Pack

Stool DNA TestPros: Noninvasive, private No dietary restriction or
cathartics One specimen & no need to
handle stool Acceptable sensitivity High acceptance by patient and
provider Detects other cancers
Cons: Sensitivity less than colonoscopy Cost high relative to FIT or gFOBT Performance intervals unknown Cost-effectiveness needs further
study Panel of markers identifies majority,
but not all, of CRC Significance of positive test result in
patient with negative follow-up evaluation unknown

Stool DNA TestKey Issues for Informed Patient Decisions
Adequate stool sample must be obtained and packaged with appropriate preservative agents in shipping to laboratory
Unit cost of currently available test significantly higher than other forms of stool testing (e.g., $575 – DNAdirect Genetic Testing Online)
If test positive, colonoscopy recommended If test negative, appropriate interval for repeat test
uncertain (manufacturer recommending 5-year interval)

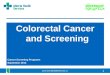
Virtual Colonoscopy or CTC (Computed Tomographic Colonography)
New Recommended Test
Minimally invasive CT imaging examination of the entire colon and rectum
Adequate bowel prep and gaseous distention of colorectum essential to quality exam
Uses advanced 2-dimensional and 3-dimensional image display techniques for interpretation
Since introduction in mid-1990s, rapid advancements in CTC technology have occurred

CT-scanner for Virtual Colonography
ColonoscopyView
VirtualColonography
View

Virtual Colonoscopy or CTCPros: Time-efficient procedure Good accuracy Minimal invasiveness No sedation or recovery
time Patient can return to
work same day Potential for same day
colonoscopy Detection of non-GI
abnormalities
Cons: Reimbursement for
screening CTC currently limited
Professional capacity to deliver limited
Requires bowel prep Quality of interpretation
highly operator dependent Controversy over radiation
dose effects Relatively expensive ($400 -
$800)

Virtual Colonoscopy or CTCKey Issues for Informed Patient Decisions
Complete bowel prep required If patient has one or more polyps >= 6 mm,
colonoscopy recommended; if same day colonoscopy not available, second complete bowel prep required
Risks are low; rare cases of perforation reported Extracolonic abnormalities may be identified

Summary
Colorectal Cancer Screening Report
from Expert Panel Promote colorectal cancer prevention as
primary goal Endorses two new screening tests – Stool
DNA and CTC Recommends fecal tests with high test
sensitivity