Embed Size (px)
Citation preview

Update in Nephrology
Delaying CKD progression
1/29/2016
Arasu Gopinath, MD Nephrology Associates of Utah
Clinical Learning Day

Declaration of Independence
I am not indebted to anyone except…. My parents My family My teachers My friends My colleagues My bank My credit union ………….
1/29/2016
• CKD staging • Our at risk population • KDIGO guidelines
– BP control – Proteinuria management – Lipids
• Monitoring • iCentra prompts • Summary • Questions
1/29/2016
Delaying CKD progression
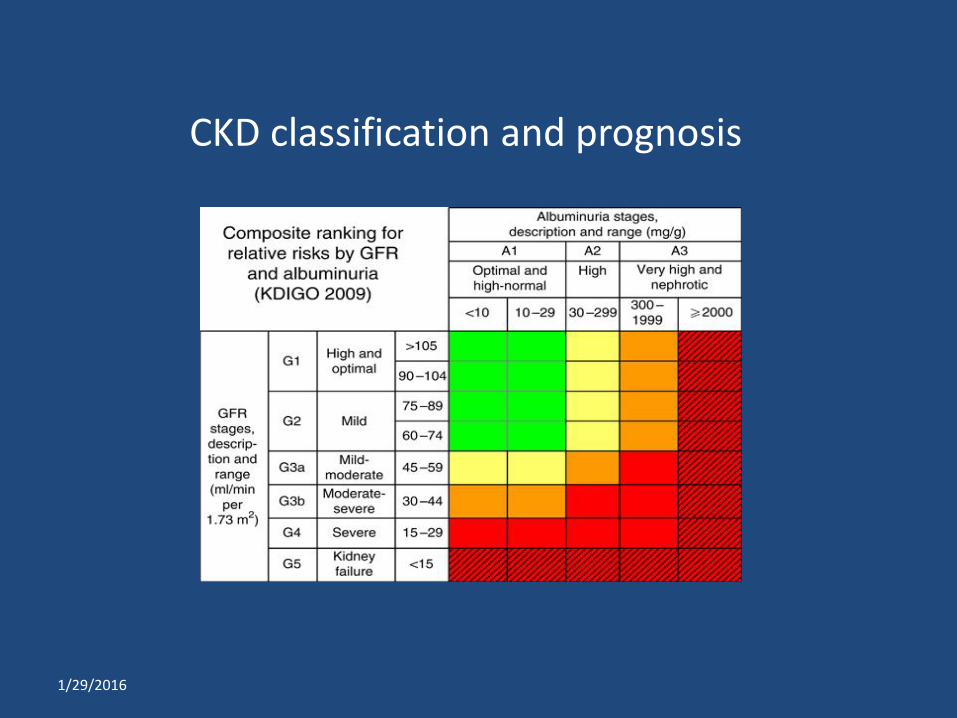
CKD classification and prognosis
1/29/2016

INTERMOUNTAIN DATA
68,723
11,563
25,398
16,829
32,470
-
10,000
20,000
30,000
40,000
50,000
60,000
70,000
80,000
Unique Patients PROBLEM_LIST DIAGNOSIS ACR30 GFR60
System Wide CKD Cohort Counts
The CKD population in Intermountain
1/29/2016
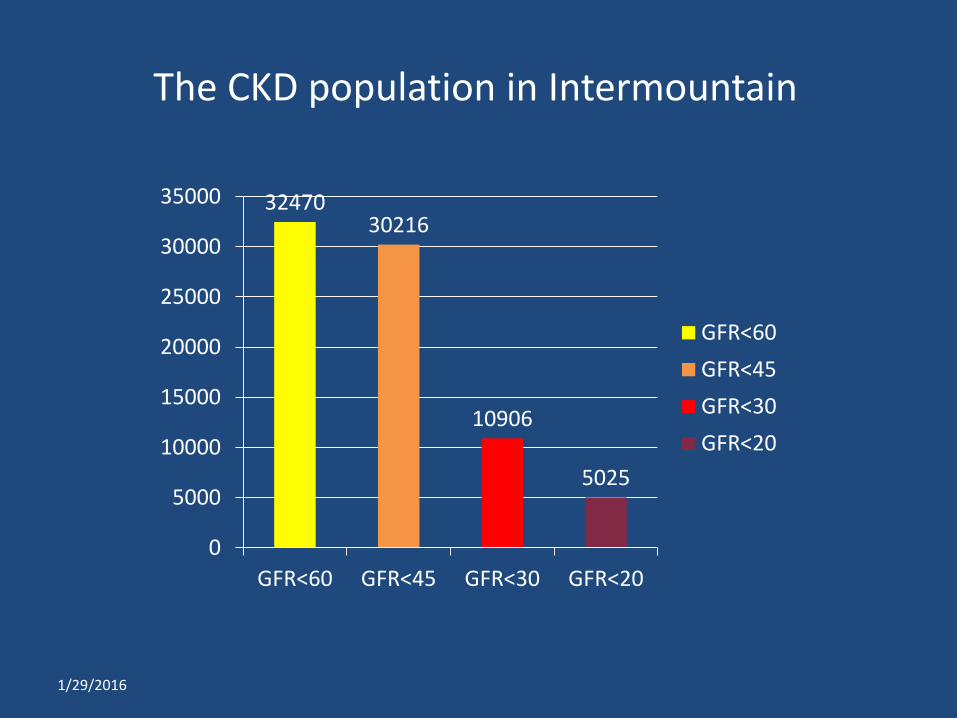
The CKD population in Intermountain
32470 30216
10906
5025
0
5000
10000
15000
20000
25000
30000
35000
GFR<60 GFR<45 GFR<30 GFR<20
GFR<60GFR<45GFR<30GFR<20
1/29/2016
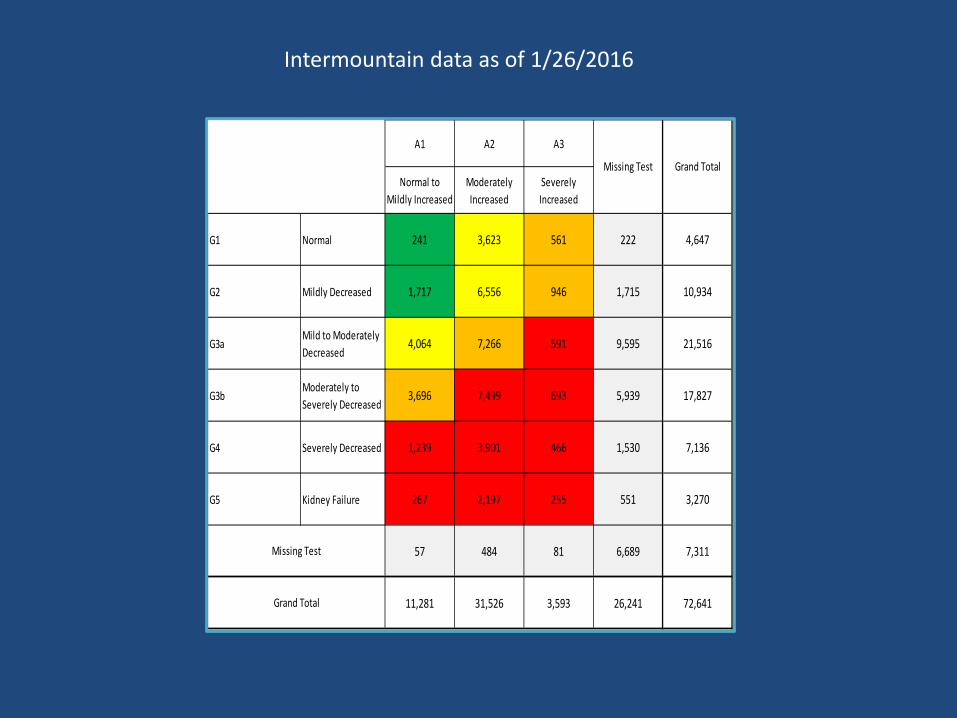
A1 A2 A3
Normal to Mildly Increased
Moderately Increased
Severely Increased
G1 Normal 241 3,623 561 222 4,647
G2 Mildly Decreased 1,717 6,556 946 1,715 10,934
G3aMild to Moderately Decreased
4,064 7,266 591 9,595 21,516
G3bModerately to Severely Decreased
3,696 7,499 693 5,939 17,827
G4 Severely Decreased 1,239 3,901 466 1,530 7,136
G5 Kidney Failure 267 2,197 255 551 3,270
57 484 81 6,689 7,311
11,281 31,526 3,593 26,241 72,641Grand Total
Grand TotalMissing Test
Missing Test
Intermountain data as of 1/26/2016
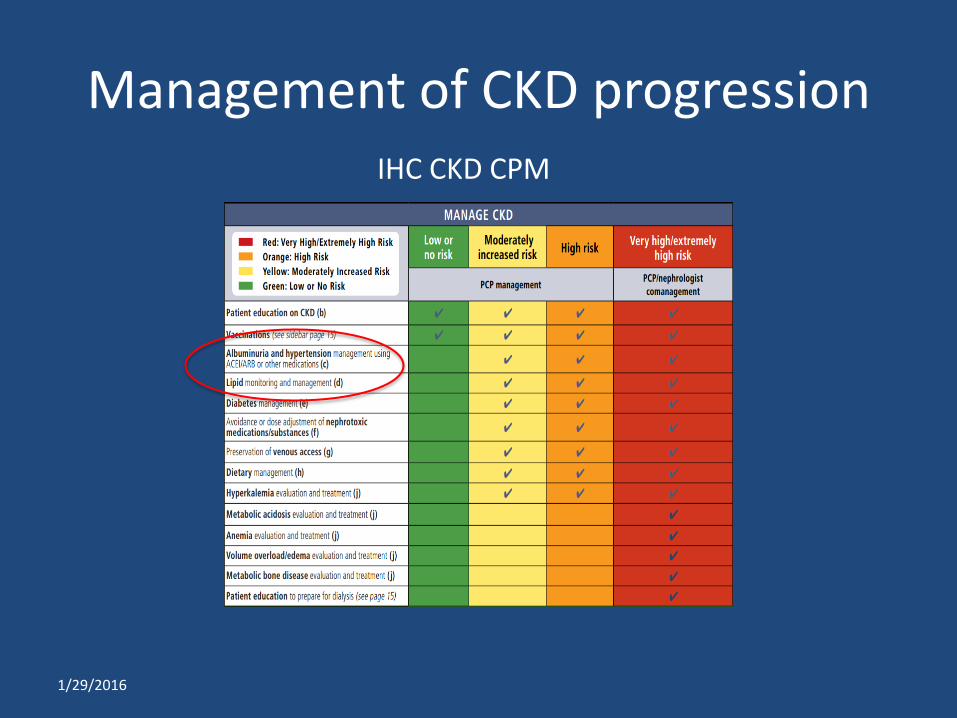
Management of CKD progression IHC CKD CPM
1/29/2016
• BP control
• Goal BP < 130/80, if patient has UACR more than 30 mg/g
• Goal BP < 140/90, if patient has UACR less than 30 mg/g
1/29/2016
Delaying CKD progression
1/29/2016
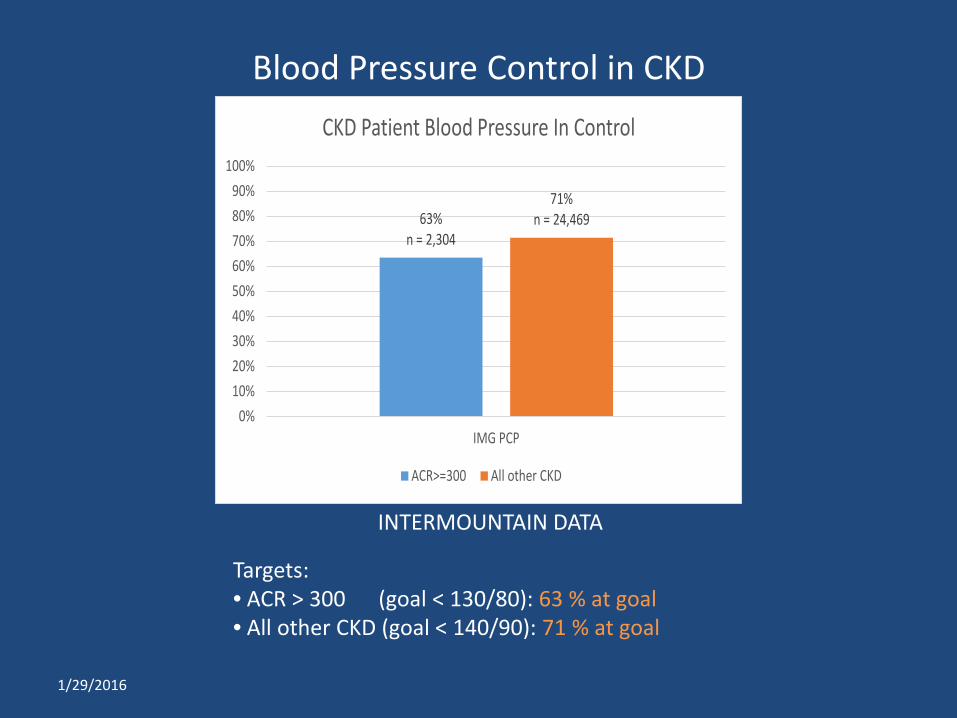
63%n = 2,304
71%n = 24,469
0%10%20%30%40%50%60%70%80%90%
100%
IMG PCP
CKD Patient Blood Pressure In Control
ACR>=300 All other CKD
INTERMOUNTAIN DATA
Blood Pressure Control in CKD
Targets: • ACR > 300 (goal < 130/80): 63 % at goal • All other CKD (goal < 140/90): 71 % at goal
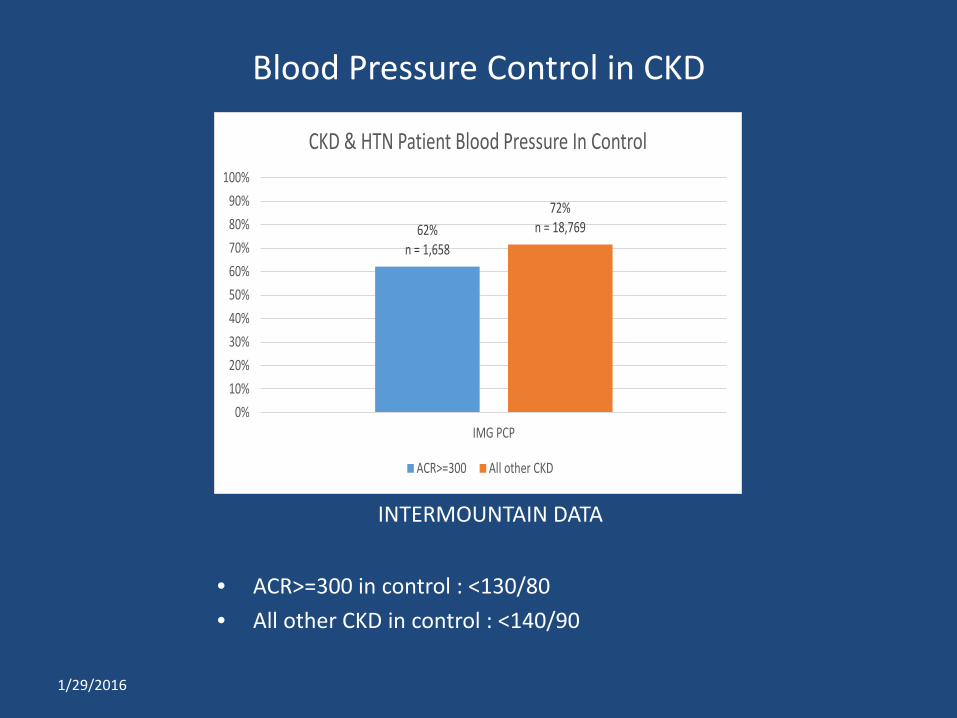
• ACR>=300 in control : <130/80 • All other CKD in control : <140/90
1/29/2016
62%n = 1,658
72%n = 18,769
0%10%20%30%40%50%60%70%80%90%
100%
IMG PCP
CKD & HTN Patient Blood Pressure In Control
ACR>=300 All other CKD
INTERMOUNTAIN DATA
Blood Pressure Control in CKD
• Albuminuria reduction
• ACEI or ARB in all adults with UACR > 300 mg/g
• ACEI or ARB in diabetics with UACR > 30 mg/g
1/29/2016
Delaying CKD progression

1/29/2016
57%n = 2,304
67%n = 7,133
0%10%20%30%40%50%60%70%80%90%
100%
IMG PCP
Patients on an ACE/ARB
CKD with ACR>=300 CKD and Diabetes with ACR>=30
Proteinuric CKD on RAAS blockade
INTERMOUNTAIN DATA
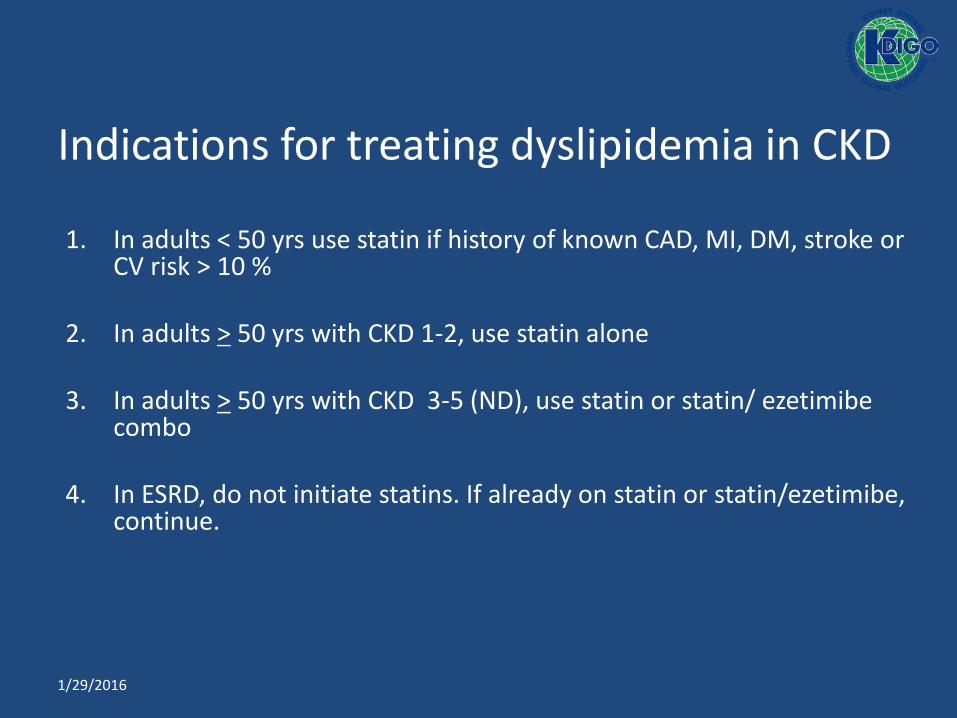
Indications for treating dyslipidemia in CKD
1. In adults < 50 yrs use statin if history of known CAD, MI, DM, stroke or CV risk > 10 %
2. In adults > 50 yrs with CKD 1-2, use statin alone
3. In adults > 50 yrs with CKD 3-5 (ND), use statin or statin/ ezetimibe combo
4. In ESRD, do not initiate statins. If already on statin or statin/ezetimibe, continue.
1/29/2016

Dyslipidemia in CKD patients age ≥50
1/29/2016
55%n = 14,425
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
IMG PCP
CKD Patients on a Statin
INTERMOUNTAIN DATA
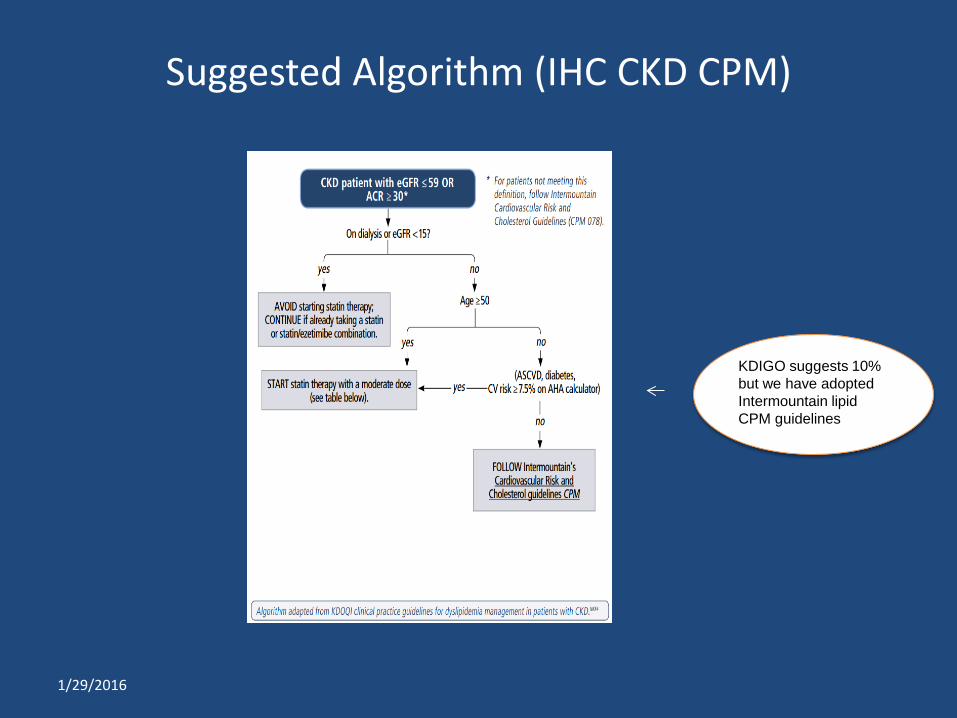
Suggested Algorithm (IHC CKD CPM)
KDIGO suggests 10% but we have adopted Intermountain lipid CPM guidelines
1/29/2016
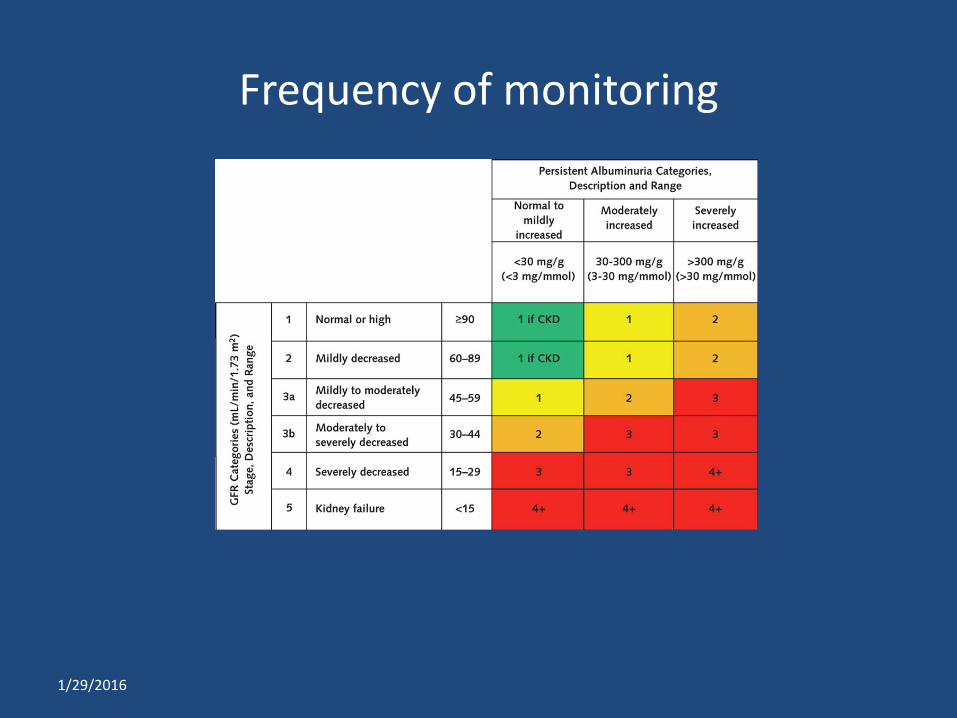
Frequency of monitoring
1/29/2016
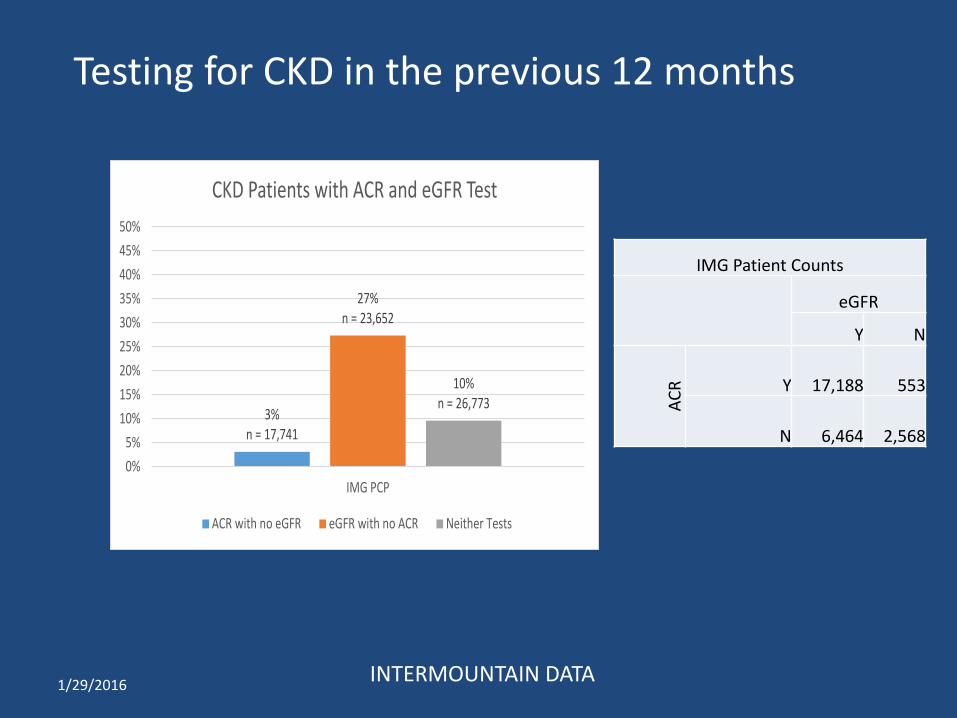
3%n = 17,741
27%n = 23,652
10%n = 26,773
0%5%
10%15%20%25%30%35%40%45%50%
IMG PCP
CKD Patients with ACR and eGFR Test
ACR with no eGFR eGFR with no ACR Neither Tests
IMG Patient Counts
eGFR
Y N
ACR Y 17,188 553
N 6,464 2,568
1/29/2016 INTERMOUNTAIN DATA
Testing for CKD in the previous 12 months
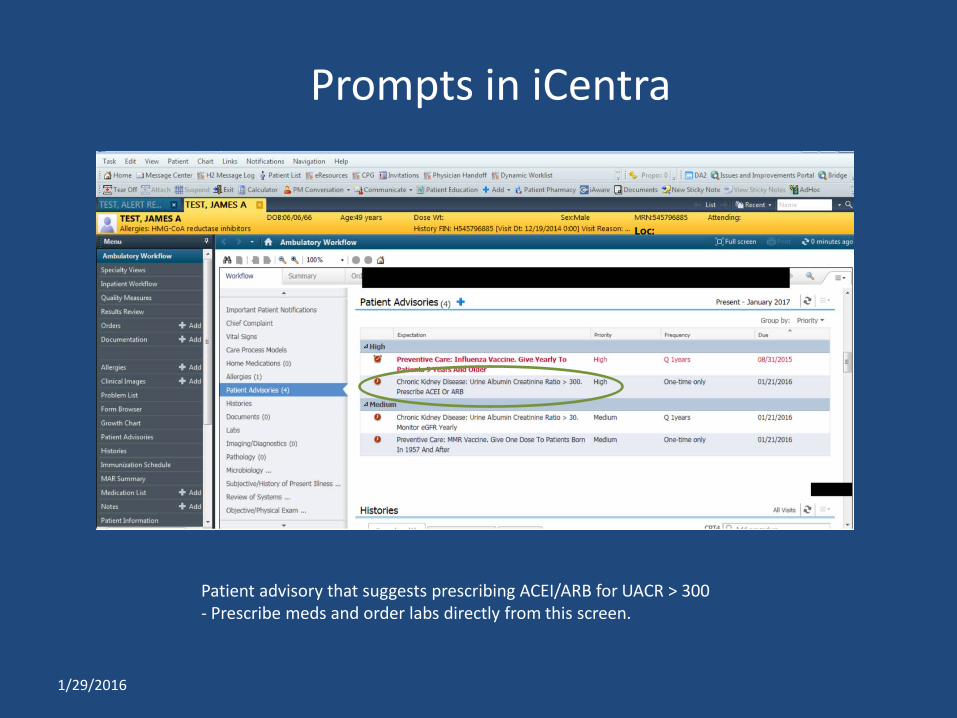
Prompts in iCentra
1/29/2016
Patient advisory that suggests prescribing ACEI/ARB for UACR > 300 - Prescribe meds and order labs directly from this screen.
1/29/2016
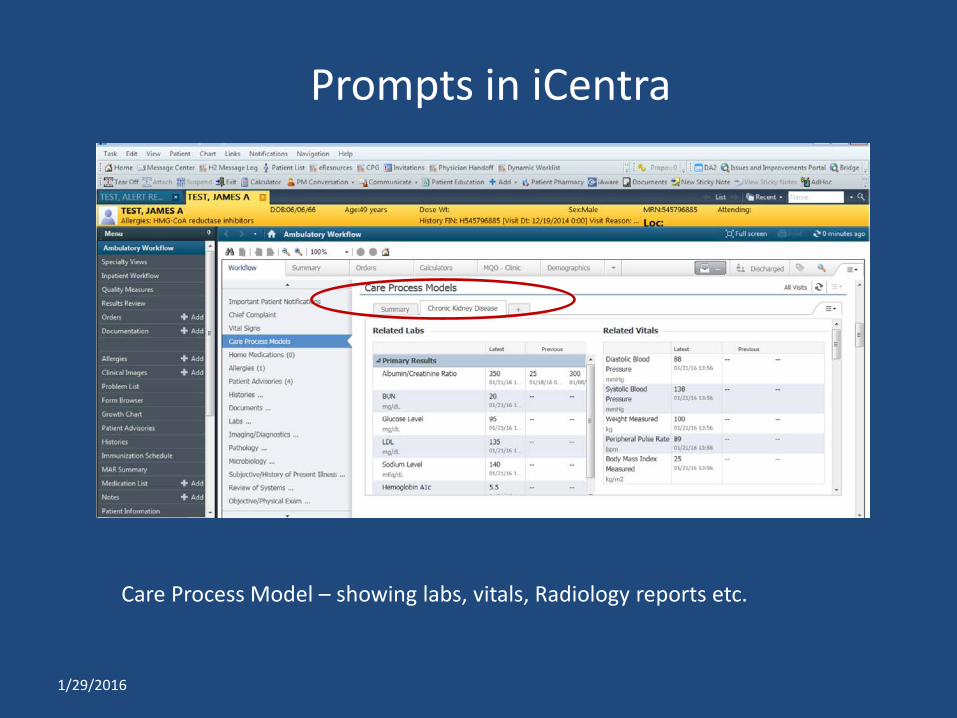
Care Process Model – showing labs, vitals, Radiology reports etc.
Prompts in iCentra
1/29/2016
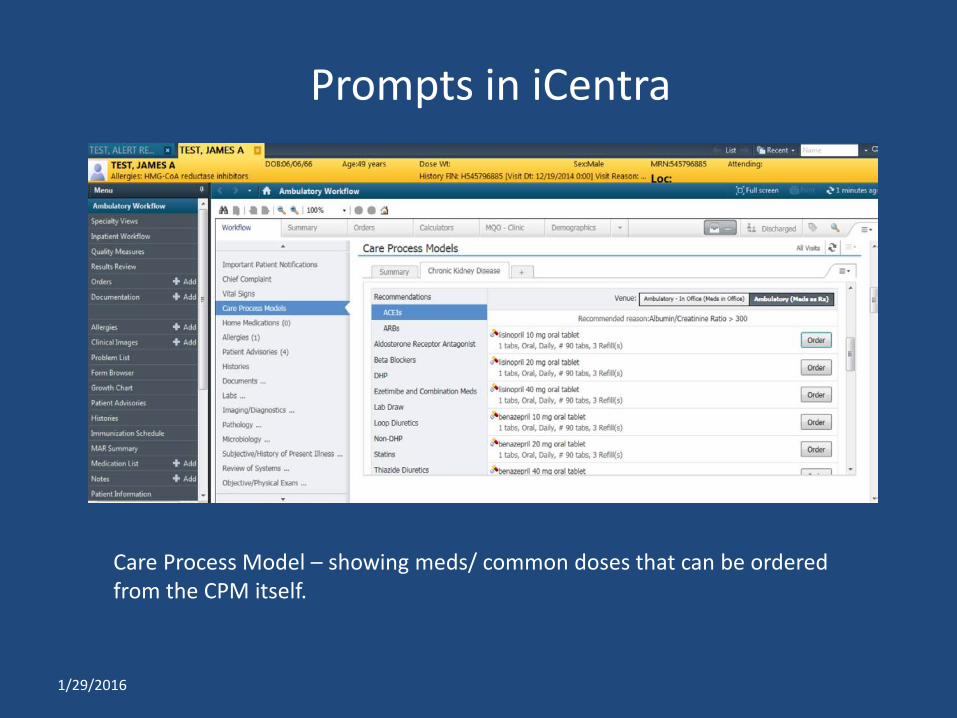
Care Process Model – showing meds/ common doses that can be ordered from the CPM itself.
Prompts in iCentra

NSAIDs in CKD
1. Impair glomerular autoregulation/ ATN 2. Resistant hypertension and make anti hypertensives less effective 3. Acute interstitial nephritis 4. Nephrotic syndrome (Minimal Change Disease and Membranous
Nephropathy) 5. Acute papillary necrosis and hematuria 6. Edema/ heart failure 7. Distal RTA and nephrolithiasis 8. Hyperkalemia 9. Chronic use associated with CKD and its progression
1/29/2016

dos and don’ts in CKD
1. Medications (+ RAAS blockade / - NSAIDs ) 1. Vein preservation
- Preserve veins in non dominant arm - Avoid PICC and Mid lines
2. Contrast (minimize contrast in Stage 3-5) - Avoid Gadolinum for MRI in stage G4-5
3. Anemia - Minimize blood draws (coordinate with others where possible)
4. Malnutrition - Do not limit protein intake if malnourished
1/29/2016
Delaying CKD progression
• Avoiding AKI • Avoid NSAIDs • Stop nephrotoxic agents prior to contrast • In GFR < 60 ml/min, avoid high osmolar
contrast, use lowest dose possible, hydrate with saline and repeat labs in 48-96 hours.
• Avoid phosphate containing bowel preparations
1/29/2016
Delaying CKD progression
• Limiting protein intake 0.8 g/kg/day in CKD G5 categories
• Salt intake
< 2.0 gram of Sodium or < 5 g of salt per day
• Lifestyle changes ~ exercise 30 minutes 5 x week, goal BMI 20-25, quit smoking
1/29/2016
Summary
1/29/2016
•Test regularly (monitor progression, complications and treatment) • Control BP
• < 140/90, if ACR < 30 • < 130/80 if ACR> 300 and perhaps 30-300 as well
• Prescribe ACEI/ ARB for ACR > 30 in Diabetics or ACR > 300 in others • Nutrition (MNT) consult • Avoid nephrotoxins • advise smoking cessation • advise regular exercise • statins if age > 50 and eGFR < 60 • Nephrology consult
Questions
1. Efforts to retard progression of CKD include all of the following except
1. Control of BP 2. Limit proteinuria 3. Treat dyslipidemia 4. Control hyperuricemia
1/29/2016
Questions
2. Which of the following statements is correct? 1. In a diabetic with ACR 500 mg/g, target BP <
130/80 2. In a diabetic with ACR 200 mg/g, target BP <
140/90 3. In a diabetic with ACR 10 mg/g, target BP <
130/80 4. In a non diabetic with ACR 200 mg/g, target BP <
130/80
1/29/2016
Questions
3. 58 yr old M, with eGFR 37 ml/min, ACR 500 mg/g and the following levels (TC 190, HDL 45, LDL 97, Trigly 240). What is the best lipid strategy in this CKD patient?
1. Start Statin 2. Start Fenofibrate 3. Start Ezetimibe 4. Start Fish Oil
1/29/2016
Questions
4. All of the following are recommended strategies in managing the CKD patient except:
1. Avoid NSAIDs 2. Consult dietitian 3. Minimize blood draws 4. Preserve veins in the dominant arm
1/29/2016
Answer keys
1. 4 2. 1 3. 1 4. 4
1/29/2016

CKD Clinical Learning Day
• Thank You for listening – Arasu Gopinath, MD
1/29/2016





























