8/2/2019 UNUSUALLY AGGRESSIVE MYOFIBROMATOSIS IN A NEONATE
1/2
Journal of Neonatal Surgery 2012;1(2):35
EL-MED-Pub Publishers.
http://www.elmedpub.com
C L I N I C A L I M A G E
UNUSUALLY AGGRESSIVE MYOFIBROMATOSIS IN A NEONATE
Jitendra Hazarey*, Shilpa Hazare1, Girish Moghe2
Department of Pediatric surgery*, Pediatrics1, and Pathology2,
Getwell Hospital and Research Institute, 20/1,
Dhantoli, Nagpur, India. 440012
* Corresponding Author
Available athttp://www.jneonatalsurg.com
This work is licensed under a Creative Commons Attribution 3.0
Unported LicenseHow to cite:Hazarey J, Hazare S, Moghe G. Unusually
aggressive myofibromatosis in a neonate. J Neonat Surg 2012; 1:
35
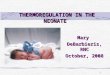
Figure 1:Exophytic masses arising from the knee and ankle. Scar
of two excised masses at the hip joint area.
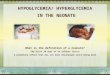
Figure 2: Photomicrograph showing abundant fibroblasts with
skeletal muscles. No evidence of malignancy at this time.
http://www.jneonatalsurg.com/http://www.jneonatalsurg.com/http://www.jneonatalsurg.com/http://www.jneonatalsurg.com/
8/2/2019 UNUSUALLY AGGRESSIVE MYOFIBROMATOSIS IN A NEONATE
2/2
UNUSUALLY AGGRESSIVE MYOFIBROMATOSIS IN A NEONATE
Journal of Neonatal Surgery Vol. 1(2); 2012
A 15 days old male newborn presented with four exophytic
swellings arising from the skin of right lower limb;not restricting
its mobility (Fig.1). The lesions were sequentially excised and
pathological examination revealedinfantile myofibromatosis in these
growths. No evidence of malignancy was found (Fig.2). The swelling
in thethigh recurred after 6 months and suspecting sarcomatous
change, a biopsy was done which confirmed thesarcomatous change.
Amputation and chemotherapy was offered, and the poor response to
chemo-
radiotherapy was explained. Parents refused further treatment
and child succumbed to the disease afterdeveloping inguinal nodes
and visceral metastasis.
Infantile myofibromatosis is a rare tumor of infancy. It is
mesenchymal in origin and involves superficial structures or
may be visceral. The lesions have been found in nearly all
kinds of tissues, including the orbit, bone, lip, oral
cavity,
central nervous system, gastrointestinal tract, lungs,
myocardium, liver, and biliary tree. It may present at birth
or appears during the first year of life. The exact etiology
is
unknown and most cases have been reported as sporadic.
Both, autosomal dominant and recessive inheritance modes
of transmission have been suggested. The prognosis is
excellent in solitary or multicentric lesions without
visceral
involvement, with possibility of spontaneous regression of
lesions confined to the skin, soft tissue and bone, and a
very
low recurrence rate after surgical excision. The prognosis
is
poor with visceral involvement [1-3]. In our patient the
lesion
recurred with a sarcomatous change which is an unusual
behavior for a lesion known to be benign with a capacity for
spontaneous regression.
REFERENCES
1. Chung EB, Enzinger FM. Infantile myofibromatosis.
Cancer1981;48:1807-18.
2. Inwards CY, Unni KK, Beabout JW, Shives TC.
Solitarycongenital fibromatosis (infantile myofibromatosis) of
bone. Am
J Surg Pathol 1991;15:935-41.
3. Wiswell TE, Davis J, Cunningham BE, Solenberger R, ThomasPJ.
Infantile myofibromatosis: the most common fibrous tumorof infancy.
J Pediatr Surg 1988;23:315-18.
Address for correspondenceDr. Jitendra Hazarey
Department of Pediatric surgery, Getwell Hospital and Research
Institute, 20/1, Dhantoli, Nagpur, India. 440012.
E mail: [email protected]
Hazarey et al, 2012
Submitted on: 11-01-2012
Accepted on: 21-01-2012
Published on: 01-04-2012Conflict of interest: None
Source of Support: Nil