Embed Size (px)
Citation preview

Case reports
Br. J. Surg. 1989, Vol. 76, December, 1257-1 258
Unusual cause of thoracic outlet sy nd ro me
R. M . R. McAllister, G. Watkin and M. Adiseshiah
Bloomsbury Vascular Unit, The Middlesex Hospital, London, UK Correspondence to: Dr R. M. R. McAllister, Department of Surgery, The Middlesex Hospital, Mortirner Street, London W I N 8AA, UK
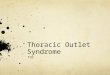
Figure 1 in the subclavian artery on abduction of the right arm
An intravenous digital subtraction angiogram showing a kink
a Case report A 22-year-old builder presented with a 4-year history of recurrent pain in the right wrist, a 3-month history of paraesthesia radiating from the right wrist to the elbow, and intermittent right-sided neck pain, all of which were exacerbated by sneezing. The symptoms began when he started a new job which involved heavy lifting.
On examination he was generally fit. The upper limb pulses were present but with a reduced volume in the right radial. The systolic blood pressure was lower by 20mmHg when measured in the right arm. A loud bruit was audible over the right subclavian artery. There was no muscle wasting in the arm but there was reduced power in the intrinsic muscles of the hand, together with reduced perception of pin-prick and light touch in the seventh and eighth cervical nerve root sensory distribution. Radiographs excluded a cervical rib. Electromyo- graphy identified a conduction abnormality in the ulnar nerve, not localized to the elbow. An intravenous digital subtraction angiogram showed a kink in the right subclavian artery at the first rib (Figure 1).
Right first rib resection was carried out via a standard axillary approach'. An abnormal swelling at the origin of the subclavian artery gave the impression of a haematoma around the artery. Median sternotomy was performed and the innominate artery was controlled. The first thoracic nerve root was defined within the thorax and the lesion previously thought to be a haematoma was found to arise within the nerve root. The mass was excised, a drain was inserted and the chest was closed. Histopathology of the specimen revealed a benign schwannoma with degenerative features (Figure 2). The patient recovered and was discharged home.
Discussion b
Pang and Wessel found no reports of brachial plexus tumours causing thoracic outlet obstruction in a review of 159 papers between 1846 and 19872. Lusk et al. reported 147 patients with primary tumours of the brachial plexus in the world literature since 18863. In a series of 600 brachial plexus lesions between 1969 and 1985,384 were operated upon and 57 were tumours3. Eight of these were benign schwannomas. Presentation was usually as a painless, palpable, mass with mild or no neuronal loss, which contrasts with the present case in which the tumour was out of reach and caused the pressure symptoms of thoracic outlet obstruction. Five of the eight schwannomas were located on the fifth or sixth nerve root, or on the upper trunk. The remainder were on the lower trunk or on the lateral and the medial cords. In another review of 480 benign schwannomas, Gyhra et al. found only 24 arising from the brachial plexus4. A case report was given of such a patient with intrathoracic extension of the tumour which had not been previously reported. The difficulties of diagnosing brachial plexus tumours before operation have been emphasized, especially when these tumours are inaccessible to palpation5s6.
l?igure 2 a ~~~i~~ cystic containing clotted blood. b Microscopic appearance of benign schwannoma with degenerative features. Nerve fibres were present in the capsule of the tumour
0007-1323/89/12125742$3.00 0 1989 Butterworth & Co (Publishers) Ltd 1257

Case reports
Thoracic outlet syndrome caused by brachial plexus is exceptionally rare. We of such a presentation in the literature.
References
a schwannoma of the have found no reports
3.
4.
Lusk MD, Kline DG, Garcia CA. Tumours of the brachial plexus. Neurosurgery 1987; 21: 439-53. Gyhra A, Israel J , Santander C, Acunz D. Schwannoma of the brachial plexus with intrathoracic extension. Thorax 1980; 35: 7 0 3 4 . Seddon HJ. Surgical Disorders of Peripheral Nerves. Edinburgh: Churchill Livinastone. 1972.
5. ”
1 .
2.
Roos DB. Transaxillary approach for first rib resection to relieve thoracic outlet syndrome. Ann Surg 1966; 163: 354-8. Pang D, Wessel HH. Thoracic outlet syndrome. Neurosurgery 1988; 22: 105-21.
6. Sell PJ , Semple JC. Primary nerve tumours of the brachial plexus. Br J Surg 1987; 74: 7 3 4 .
Paper accepted 27 July 1989
Br. J. Surg. 1989, Vol. 76, December, 1258
Combined internal and external biliary fistulae treated by percutaneous cholecystlithotomy
M. G. Davies, E. Tadros, S. Gaine, G. P. McEntee, T. F. Gorey and T. P. J. Hennessy
Department of Clinical Surgery, Trinity College and Department of Surgery, St. James’s Hospital, Dublin, Ireland Correspondence to: Mr M. G . Davies, Department of Surgery, St. James’s Hospital, James’ Street, Dublin 8, Ireland
Spontaneous biliary fistulae are rare, occurring in approximately 3 per cent of all patients undergoing biliary surgery, and they usually communicate with the duodenum’,’.
Case report An 84-year-old man was referred with a 3-month history of a discharging sinus in the right-hypochrondrium. The patient had been admitted 1 year previously with an episode of acute cholecystitis; gallstones were confirmed on ultrasound scan and he settled on conservative treatment. The patient also had obstructive airways disease, congestive cardiac failure and chronic renal failure. A sinogram revealed cholecystcutaneous fistulae, multiple large gallstones and cholecystduodenal fistulae; the remainder of the biliary system appeared normal (Figure 1 ) . The tract was too small and tortuous to allow cannulization.
In view of the patient’s poor medical condition, direct exploration of the external cholecystcutaneous fistulae was undertaken under local anaesthesia. A small 3-cm incision was made after the tract was dilated, and six large gallstones were removed using a Desjardin’s forceps. A 12 Fr Fogarty catheter was inserted, the catheter was brought out through a separate skin incision. and a corrugated drain was placed in the fistula tract. Postoperative recovery was uneventful, and a catheter cholangiogram at 9 days showed a patent biliary system with contrast draining freely into the duodenum. At review, 3 months later, the patient was well, the fistula tract had closed and an oral cholecystogram was normal.
Discussion In 1670. Thilesus described the first external biliary fistula and, in the 19th century, when the condition was common, Courvoisier reported 169 cases of spontaneous external fistula f ~ r m a t i o n ~ , ~ . However, only 45 further cases have been reported to date with only nine cases reported from 1944 to 19855. The dramatic fall in incidence is attributable to the advent of modern biliary tract surgery.
Spontaneous biliary fistulae are usually the result of acute suppurative cholecystitis, and they drain into the duodenum in
Figure 1 Contrast fistulogram showing multiple gallstones in the gallbladder and fistulae to the skin and duodenum
75 per cent of all cases. Fistula formation into the colon, bronchial tree, stomach and urinary tract have also been reported but these fistulae are extremely rare6 ’; only one case of combined internal and external biliary fistulae has been reported to date5. In that case, the patient who was otherwise healthy was treated successfully by cholecystectomy and excision of the fistulous tracts. However, in high risk patients, percutaneous removal of the stones should be considered, and with an existing tract to the gallbladder endoscopic access may be feasible if the tract can be dilated. The presence of a patent cystic duct and distal biliary tree following the procedure should ensure that the cholecystcutaneous fistula closes spontaneously when the drain is removed.
References 1.
2.
3.
4.
5 .
6 .
7.
8.
Maingot R. Internal duodenal and biliary fistulae. Abdominal Operations. 6th ed. New York: Appleton-Century-Crofts, 1974:
Marshall SF, Folk RC. Spontaneous biliary fistula. Surg Clin North Am 1958; 6: 679-91. Horhammer C. Ueber estraperitoneale perforatio der Gallen- blase. Munchen med Wochenschr 1915; 63: 1451-2. Courvoisier L. Pathologie und Chirurgie der Gallerwege. Leipzig: F. C . W. Vogel, 1890. Reed MWR, Tweedle JH. Spontaneous simultaneous internal and external biliary fistulae. Br J Surg 1985; 72: 538. Glenn F, Reed C, Grafe WR. Biliary enteric fistula. Surg Gynecol Obstet 1981; 153: 327-31. Borman CN, Rigler LG. Spontaneous internal biliary fistula and gallstone obstruction. Surgery 1937; 1 : 349-78. Henry CL, Orr TG. Spontaneous external biliary fistulas. Surgery
160-8.
1949; 26: 641-6.
Paper accepted 19 April 1989
1258 0007-1323/89jl21258-01$3.00 1989 Butterworth & Co (Publishers) Ltd