7/31/2019 Unusual Cause of Bleeding in Liver Cirrhosis
Patient
1/3
Clinical picture
Unusual cause of bleeding in liver cirrhosis patient
A 42-year-old man presented to the emergencydepartment with 2
weeks history of fatigue anddark tarry stool. He had past medical
history signifi-cant for primary sclerosing cholangitis with
livercirrhosis, complicated with ascites and small non-bleeding
esophageal varices. He denied nausea,vomiting, abdominal pain,
weight loss or changein appetite. He also denied excessive use
ofnon-steroid anti-inflammatory drugs (NSAIDs). On
presentation he was on spironolactone, furosomide,omeprazole and
nadalol. On exam, he appearedpale with stable vitals signs. Skin
examinationrevealed spider angiomata and palmar erythema.Abdomen
was non-distended with no abdominaltenderness or organomegaly.
There was no asterixis.Initial blood work revealed hemoglobin of
5.8 g/dl(normal 13.517.5g/l) down from his baseline of13g/dl.
Platelet count was 87/ml (normal 150000400 000/ml). Prothrombin
time and INR were15.2 s (normal 9.913 s) and 1.8 (normal
0.91.2),respectively. His Childs Pugh Score was 7 (Class B),Model
of End-Stage Liver Disease (MELD) score was 8.
The patient received two units of packed red bloodcells and two
units of fresh frozen plasma.Continuous intravenous esomeprazole
and octreo-tide were started soon after admission. The
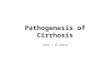
patientunderwent esophagogastroduodenoscopy (EGD).This revealed
duodenal bulbar varices without stig-mata of bleeding (Figure 1).
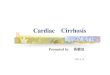
Endoscopic ultrasound(EUS) showed a submucosal anechoic lesion
corres-ponding to the endoscopic finding in the second
portion of the duodenum (Figure 2). Color Dopplerimaging
revealed a vascular lesion. Patienthemoglobin responded well to
blood transfusionand remained stable. Liver vascular
ultrasoundshowed patent hepatic vasculature. Echocardiogramshowed
normal right ventricular size and function.The patient underwent
transjugular intrahepaticportosystemic shunt (TIPS) procedure which
resultedin a decrease in the porto-systemic pressure gradientfrom
23 to 5 mmHg. He was discharged home fewdays later in a stable
condition.
Patients with liver cirrhosis have an increased riskof mortality
and morbidity due to their susceptibility
Figure 1. (A) EGD showing duodenal bulbar varices without
stigmata of bleeding (arrow). (B) Normal duodena mucosa.
! The Author 2012. Published by Oxford University Press on
behalf of the Association of Physicians.All rights reserved. For
Permissions, please email: [email protected] Page 1 of
3
Q J Meddoi:10.1093/qjmed/hcs151
QJM Advance Access published August 11, 2012
7/31/2019 Unusual Cause of Bleeding in Liver Cirrhosis
Patient
2/3
to a variety of complications.1 Variceal bleeding is
one of the most life-threatening complications in
cirrhotics, with mortality up to 30% for each bleed-
ing episode.2 The prevalence of duodenal varices in
cirrhotic patient has been reported at about 0.4%.3
Bleeding duodenal varices is known to be severeand often life
threatening.4 This prompts early diag-
nosis and treatment. Although esophageal varicesare easily
diagnosed with EGD alone, the sub-
mucosal location and the lack of red color signs of
duodenal varices pose a diagnostic challenge.5 Anycirrhotic
patient with GI bleed should undergo a
thorough endoscopic evaluation of the duodenum.
When the diagnosis is in doubt, EUS, is a valuabletool in
confirming the diagnosis. There are mul-
tiple therapeutic options in the management of
duodenal varices which include: (i) non-selective
beta blockers; (ii) TIPS procedure; (iii) endoscopic
management of varices with ligation and glue
injection; and (iv) balloon-occluded retrograde
transvenous obliteration.5,6 However, a case bycase management
decision has to be made taking
into consideration the experience of the physician
and available therapeutic options. In our patient, he
underwent TIPS with no further bleeding on
subsequent follow-ups.
Acknowledgements
All authors had access to the manuscript and a rolein writing
the manuscript.
Photographs and text from: Shadi Al Halabi,Digestive Disease
Institute, Cleveland Clinic,Cleveland, OH, USA; M. Chadi Alraies,
ClinicalAssistant Professor of Medicine, Cleveland ClinicLerner
College of Medicine of Case WesternReserve University, Department
of HospitalMedicine, Cleveland Clinic, Cleveland, OH, USA;Abdul
Hamid Alraiyes, Department of PulmonaryDiseases, Critical Care
& Environmental Medicine,Tulane University Health Sciences
Center, New
Orleans, LA, USA; Ibrahim Hanouneh, DigestiveDisease Institute,
Cleveland Clinic, Cleveland, OH,USA; William D. Carey, Professor of
Medicine,Cleveland Clinic Lerner College of Medicine ofCase,
Western Reserve University, Center forContinuing Education and
Digestive DiseaseInstitute, Cleveland Clinic, Cleveland, OH,
USA.email: [email protected]
Conflict of interest: None declared.
References1. Sorensen HT, Thulstrup AM, Mellemkjar L, Jepsen
P,
Christensen E, Olsen JH, et al. Long-term survival and
cause-specific mortality in patients with cirrhosis of the
liver: a nationwide cohort study in Denmark. J Clin
Epidemiol2003; 56:8893.
2. Graham DY, Smith JL. The course of patients after
variceal
hemorrhage. Gastroenterology1981; 80:8009.
3. Hashizume M, Tanoue K, Ohta M, Ueno K, Sugimachi K,
Kashiwagi M, et al. Vascular anatomy of duodenal varices:
angiographic and histopathological assessments. Am J
Gastroenterol1993; 88:19425.
Figure 2. EUS showing anechoic lesion corresponding to the
endoscopic finding of the duodenum consistent with vascularlesion
(arrow).
Page 2 of 3
Clinical picture
7/31/2019 Unusual Cause of Bleeding in Liver Cirrhosis
Patient
3/3
4. Amin R, Alexis R, Korzis J. Fatal ruptured duodenal varix:
a
case report and review of literature. Am J
Gastroenterol1985;
80:138.
5. Matsui S, Kudo M, Ichikawa T, Okada M, Miyabe Y.
The clinical characteristics, endoscopic treatment, and
prognosis for patients presenting with duodenal varices.
Hepatogastroenterology2008; 55:95962.
6. Haruta I, Isobe Y, Ueno E, Toda J, Mitsunaga A, Noguchi
S,
et al. Balloon-occluded retrograde transvenous obliteration
(BRTO), a promising nonsurgical therapy for ectopic
varices: a case report of successful treatment of
duodenal varices by BRTO. Am J Gastroenterol 1996;
91:25947.
Page 3 of 3
Clinical picture