Embed Size (px)
Citation preview
Clinical and Experimental Ophthalmology
2005;
33
: 330–335
Letters to the Editor
_______________________________
Letter to the Editor
Clinical Case Notes
Presumed CMV associated necrotizing retinopathy in a non-HIV immunocompromised host
A
BSTRACT
Herpetic necrotizing retinitis is caused by the herpesvirus group ofviruses, including cytomegalovirus (CMV). Reports defining causativeviruses have shown CMV to be a rare cause of acute retinal necrosis.In fact, there is only one report in the literature of CMV associatedwith progressive outer retinal necrosis, which is most commonlyassociated with Varicella zoster virus. A case is presented of CMV-related necrotizing retinopathy concurrent with subtle signs ofherpetic retinitis in an immunocompromised patient, highlighting thespectrum of response of herpetic retinopathies.
Key words:
cytomegalovirus, herpetic necrotizing retinopathy,immunocompromised, progressive outer retinal necrosis.
I
NTRODUCTION
Herpetic necrotizing retinitis is caused by the herpesvirus group ofviruses: Herpes simplex virus
,
Varicella zoster virus, cytomegalo-virus (CMV) or Epstein–Barr virus. Reports defining causativeviruses have shown CMV to be a rare cause of acute retinalnecrosis; in fact, there is only one report in the literature of CMVassociated with progressive outer retinal necrosis (PORN).
1
Mostcommonly, PORN is associated with Varicella zoster virus, with60% of immunocompromised patients having a recent history ofHerpes zoster ophthalmia (HZO) infection.
2
We present a case of CMV-related necrotizing retinopathy inan immunocompromised patient concurrent with subtle signs ofherpetic retinitis, highlighting the spectrum of response of herpeticretinopathies, and confirmed by high vitreous polymerase chainreaction (PCR) copies of CMV.
C
ASE
REPORT
An otherwise well 58-year-old man presented to the haematologyservice with a peripheral blood lymphocytosis and cervical lymph-adenopathy consistent with Binet stage A chronic lymphocyticleukaemia (CLL). He was initially managed expectantly for18 months, but he presented with a falling haemoglobin and pro-gressive splenomegaly secondary to an autoimmune haemolyticanaemia. Despite treatment with chlorambucil and prednisolone,prior to a splenectomy, the anaemia persisted accompanied by alow reticulocyte count of 0.2% indicative of pure red cell aplasia.In view of this, a 6 month course of cyclosporin was commenced.
Progressive lymphocytosis over the subsequent 18 monthswarranted three further cycles of oral chlorambucil 10 mg daily.With no response to this, and six cycles of CAP (cyclophos-phamide, adriamycin, prednisolone) combination chemotherapy, abone marrow biopsy was performed, which demonstrated persist-ing disease. In an attempt to clear the bone marrow, and to allowstem cell harvesting, four cycles of oral fludarabine 90 mg daily for5 days were administered on a 4-weekly basis.
Around 10 weeks following completion of fludarabine, hedeveloped shingles affecting the right T5 distribution. This wasdiagnosed clinically without PCR or culture confirmation. Hereceived oral valacyclovir initially for a course of 7 days, withapparent crusting of the lesions. However, on cessation of the oralanti-viral therapy new crops of vesicles developed in the samedistribution, and he was admitted for 7 days of intravenous acy-clovir and subsequently another week of oral valacyclovir. Hemade a good recovery and was systemically well with stable CLLwhen he presented 1 month later with a 1 week history of progres-sive visual loss affecting both eyes.
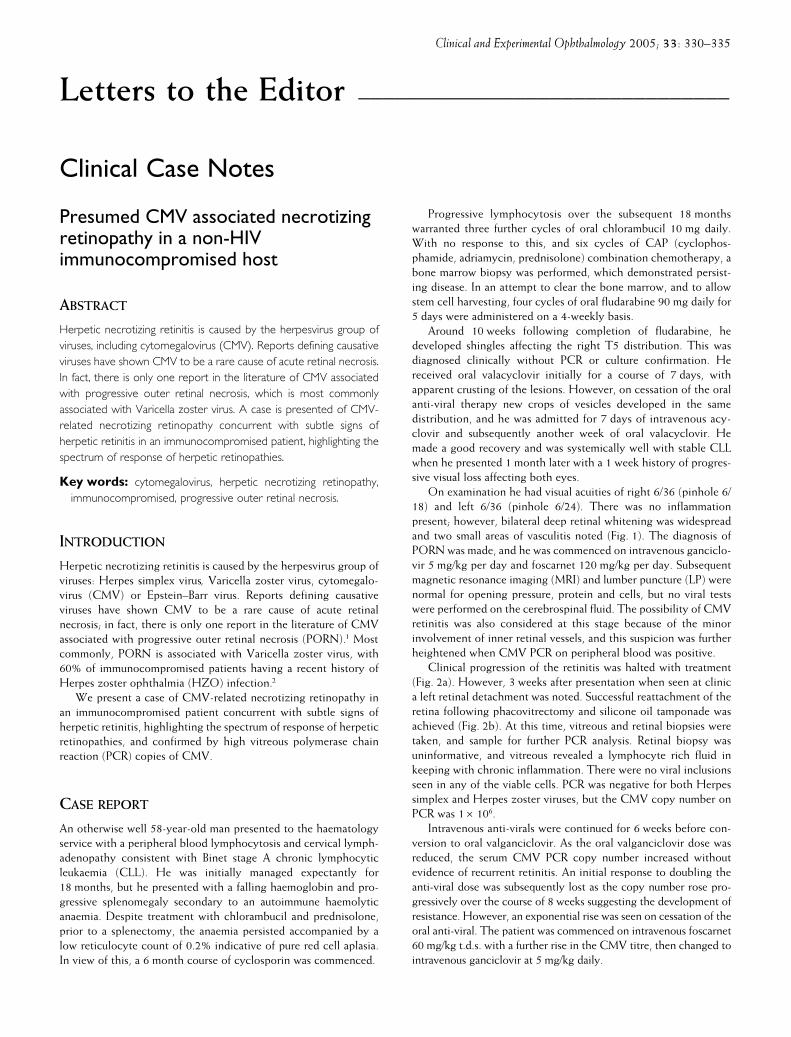
On examination he had visual acuities of right 6/36 (pinhole 6/18) and left 6/36 (pinhole 6/24). There was no inflammationpresent; however, bilateral deep retinal whitening was widespreadand two small areas of vasculitis noted (Fig. 1). The diagnosis ofPORN was made, and he was commenced on intravenous ganciclo-vir 5 mg/kg per day and foscarnet 120 mg/kg per day. Subsequentmagnetic resonance imaging (MRI) and lumber puncture (LP) werenormal for opening pressure, protein and cells, but no viral testswere performed on the cerebrospinal fluid. The possibility of CMVretinitis was also considered at this stage because of the minorinvolvement of inner retinal vessels, and this suspicion was furtherheightened when CMV PCR on peripheral blood was positive.
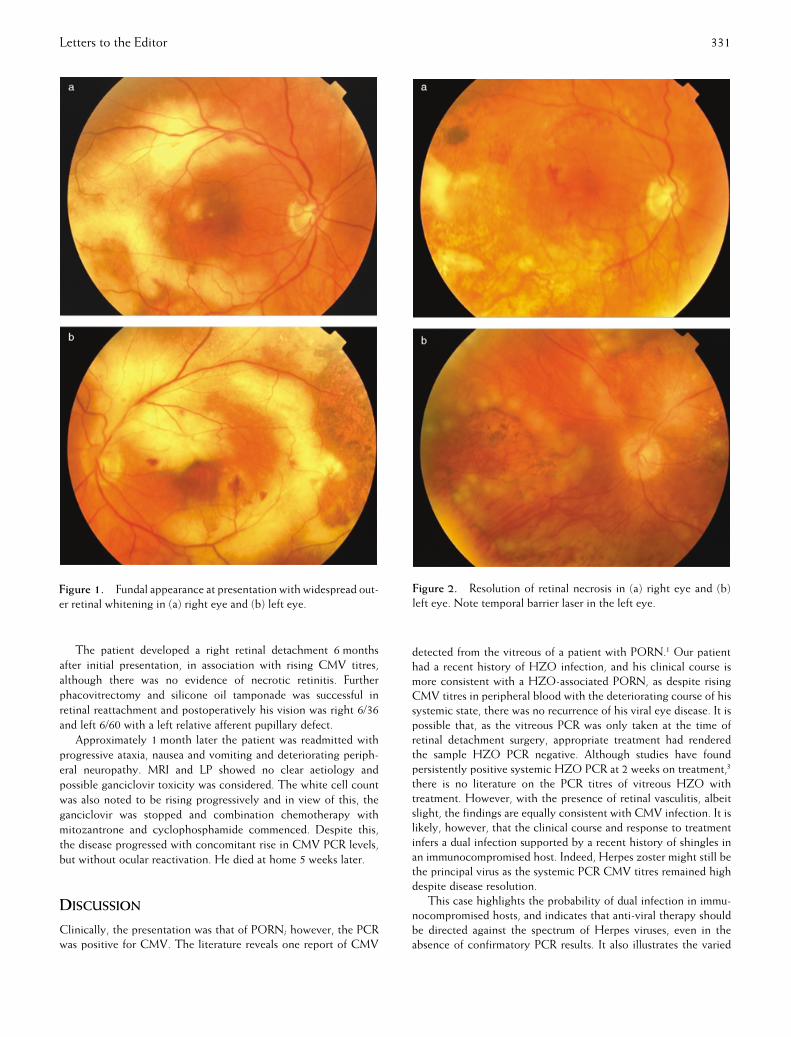
Clinical progression of the retinitis was halted with treatment(Fig. 2a). However, 3 weeks after presentation when seen at clinica left retinal detachment was noted. Successful reattachment of theretina following phacovitrectomy and silicone oil tamponade wasachieved (Fig. 2b). At this time, vitreous and retinal biopsies weretaken, and sample for further PCR analysis. Retinal biopsy wasuninformative, and vitreous revealed a lymphocyte rich fluid inkeeping with chronic inflammation. There were no viral inclusionsseen in any of the viable cells. PCR was negative for both Herpessimplex and Herpes zoster viruses, but the CMV copy number onPCR was 1
×
10
6
.Intravenous anti-virals were continued for 6 weeks before con-
version to oral valganciclovir. As the oral valganciclovir dose wasreduced, the serum CMV PCR copy number increased withoutevidence of recurrent retinitis. An initial response to doubling theanti-viral dose was subsequently lost as the copy number rose pro-gressively over the course of 8 weeks suggesting the development ofresistance. However, an exponential rise was seen on cessation of theoral anti-viral. The patient was commenced on intravenous foscarnet60 mg/kg t.d.s. with a further rise in the CMV titre, then changed tointravenous ganciclovir at 5 mg/kg daily.
Letters to the Editor 331
The patient developed a right retinal detachment 6 monthsafter initial presentation, in association with rising CMV titres,although there was no evidence of necrotic retinitis. Furtherphacovitrectomy and silicone oil tamponade was successful inretinal reattachment and postoperatively his vision was right 6/36and left 6/60 with a left relative afferent pupillary defect.
Approximately 1 month later the patient was readmitted withprogressive ataxia, nausea and vomiting and deteriorating periph-eral neuropathy. MRI and LP showed no clear aetiology andpossible ganciclovir toxicity was considered. The white cell countwas also noted to be rising progressively and in view of this, theganciclovir was stopped and combination chemotherapy withmitozantrone and cyclophosphamide commenced. Despite this,the disease progressed with concomitant rise in CMV PCR levels,but without ocular reactivation. He died at home 5 weeks later.
D
ISCUSSION
Clinically, the presentation was that of PORN; however, the PCRwas positive for CMV. The literature reveals one report of CMV
detected from the vitreous of a patient with PORN.
1
Our patienthad a recent history of HZO infection, and his clinical course ismore consistent with a HZO-associated PORN, as despite risingCMV titres in peripheral blood with the deteriorating course of hissystemic state, there was no recurrence of his viral eye disease. It ispossible that, as the vitreous PCR was only taken at the time ofretinal detachment surgery, appropriate treatment had renderedthe sample HZO PCR negative. Although studies have foundpersistently positive systemic HZO PCR at 2 weeks on treatment,
3
there is no literature on the PCR titres of vitreous HZO withtreatment. However, with the presence of retinal vasculitis, albeitslight, the findings are equally consistent with CMV infection. It islikely, however, that the clinical course and response to treatmentinfers a dual infection supported by a recent history of shingles inan immunocompromised host. Indeed, Herpes zoster might still bethe principal virus as the systemic PCR CMV titres remained highdespite disease resolution.
This case highlights the probability of dual infection in immu-nocompromised hosts, and indicates that anti-viral therapy shouldbe directed against the spectrum of Herpes viruses, even in theabsence of confirmatory PCR results. It also illustrates the varied
Figure 1.
Fundal appearance at presentation with widespread out-er retinal whitening in (a) right eye and (b) left eye.
Figure 2.
Resolution of retinal necrosis in (a)
right eye and (b)left eye. Note temporal barrier laser in the left eye.

332 Letters to the Editor
presentations of herpetic necrotizing retinopathy, suggesting thismay be the preferred term to better describe both the clinical andpathological spectrum, as progressive
outer retinal
necrosis impliesthat the full thickness of the retina is not involved.
Helen M Long
FRANZCO
andAndrew Dick
MD FRCP FRCS
Bristol Eye Hospital, Lower Maudlin Street, Bristol, UK
R
EFERENCES
1. Biswas J, Choudry S, Priya K, Gopal L. Detection of cytomega-lovirus from vitreous humour in a patient with progressive outerretinal necrosis.
Indian J Ophthalmol
2002;
50
: 319–21.2. Nogueria ML, Siquira RC, Freitas N
et al.
Detection of herpes-virus DNA by the polymerase chain reaction in vitreoussamples from patients with necrotising retinitis.
J Clin Pathol
2001;
54
: 103–6.3. Tran THC, Rozenberg F, Cassoux N, Rao NA, LeHoang P,
Bodaghi B. Polymerase chain reaction analysis of aqueoushumour samples in necrotising retinitis.
Br J Ophthalmol
2003;
87
: 79–83.
Amblyopia due to inflamed chalazion in a 13-month-old infant
A
BSTRACT
Meibomian gland cysts (chalazia) are very common lesions in child-hood and are not thought of as visually threatening lesions. A caseis reported of dense amblyopia and secondary exotropia resultingfrom an upper eyelid chalazion.
Key words:
amblyopia, chalazion, exotropia, eyelid.
C
ASE
REPORT
A 13-month-old girl was referred for urgent ophthalmic reviewwith possible preseptal cellulitis. Examination revealed a grosslyswollen left upper lid due to an inflamed chalazion (Fig. 1). Shehad an unremarkable past medical and ocular history, and theremainder of the ocular examination was normal. She was afebrileand there were no signs of infection, so she was treated conserva-tively and observed closely.
The swelling resolved slowly but completely over the following2 weeks. There was complete ptosis for 9 days and partial ptosis fora further 4 days.
When the swelling finally resolved, she was noted to have acosmetically significant left divergent strabismus (Fig. 2a). It isunlikely that the deviation had been present prior to this, as nodeviation was noted until 2 weeks after presentation and multiplephotographs taken at various times before development of thechalazion demonstrated straight ocular alignment (Fig. 2b).
She was treated with intermittent patch occlusion of the righteye, and referred to one of us (GG) at age 21 months. On exami-nation she demonstrated a strong fixation preference for the righteye and left fixation was unmaintained. Cycloplegic refraction was–0.25 D bilaterally. A 30 PD left exotropia was present for distanceand near. There was bilateral +2 overaction of both inferioroblique muscles. She was treated with patching of the right eye for8 h daily.
On review at age 23 months, the fixation preference for theright eye persisted and the exotropia had increased to 40 PD fordistance and near. She underwent a left lateral rectus recession of8.0 mm and a left medial rectus resection of 6.0 mm, combinedwith bilateral 7.0 mm inferior oblique myectomies.
On day one postoperatively, the fixation preference for theright eye persisted, and there was 35 PD of esotropia, with –3underaction of the left lateral rectus. She was managed with con-tinued patching of the right eye. The amblyopia remained resistantto patching, and the esotropia persisted. Six months postopera-tively, the ocular deviation was six PD for distance and 18 PD fornear. A 5.0 mm recession of the left medial rectus was performed.This was successful in regaining orthotropia; however, a definitivefixation preference for the right eye remains, and patching therapycontinues.
Figure 1.
Left upper lid oedema due to inflamed chalazion in a13-month-old girl.
Figure 2.
(a)
Exodeviation noted after resolution of oedema.(b)
Orthotropia prior to development of chalazion.
*Present address: Royal Victorian Eye & Ear Hospital, Melbourne, Victoria, Australia.

Letters to the Editor 333
D
ISCUSSION
Conservative management is often recommended for chalazia.Advantages of conservative management include a high successrate,
1
and the lack of risks associated with surgical treatment.Chalazia have been reported to cause astigmatism due to pres-
sure on the cornea.
2
However, Bogan
et al.
found little correlationbetween the presence of a chalazion and astigmatism.
3
They pos-tulated that due to their size, consistency and location, theselesions may be less likely to deform the globe than haemangiomas.Santa Cruz
et al.
reported three cases of decreased vision in adultsdue to acquired hyperopia caused by chalazia of the upper lid.
4
However, to our knowledge, there have been no reports ofchalazion-induced refractive error or lid closure resulting in ambly-opia or secondary exotropia in children.
The ability of capillary haemangiomas to cause anisometropicor deprivation amblyopia in infants is well known. It would appearthat the mechanism of the deprivation amblyopia in our patientwas the same as that which occurs in patients with capillaryhaemangiomas large enough to occlude the visual axis. In this casethe oedema associated with the chalazion occluded the visual axislong enough to induce amblyopia.
This case demonstrates that amblyopia can occur due to lidoedema induced by an inflamed chalazion. The potential foramblyopia must always be considered when the optic axis isoccluded during childhood. Surgical drainage of chalazia should beconsidered if the visual axis is likely to be occluded beyond thecritical period for the development of amblyopia in the particularchild’s age group.
Mark J Donaldson
MB BS(Hons)
1
* andGlen A Gole
FRANZCO
1,2
1
Department of Ophthalmology, Royal Children’s Hospital, and
2
Department of Paediatrics & Child Health, the University ofQueensland, Brisbane, Queensland, Australia
R
EFERENCES
1. Perry HD, Serniuk RA. Conservative treatment of chalazia.
Ophthalmology
1990;
87
: 218–21.2. Ormond AW. Notes on three cases of acquired astigmatism
associated with meibomian cysts.
Br J Ophthalmol
1921;
5
: 117–18.3. Bogan S, Simon JW, Krohel GB, Nelson LB. Astigmatism
associated with adnexal masses in infancy.
Arch Ophthalmol
1987;
105
: 1368–70.4. Santa Cruz C, Culotta T, Cohen EJ, Rapuano CJ. Chalazion-
induced hyperopia as a cause of decreased vision.
OphthalmicSurg Lasers
1997;
28
: 683–4.
Unusual cause for non-detection of retained metallic foreign body on ocular ultrasonography
A
BSTRACT
Ultrasound biomicroscopy has become a valuable adjunct in theevaluation of occult ocular foreign bodies. An unusual cause for
non-detection of a metallic retained intraocular foreign body isdescribed. In this case, the usual ‘shadowing’ was not discernibleas the foreign body was lying just over the optic disc.
Key words:
occult foreign body, radiograph, retained intraocularforeign body, ultrasonography.
I
NTRODUCTION
In recent years, ocular ultrasound has become an indispensablediagnostic tool that has increased our ability to detect and differ-entiate many intraocular and orbital disorders, especially in caseswith opaque ocular media. Ultrasound biomicroscopy has becomea valuable adjunct in the evaluation of occult ocular foreign bodiesthat are suspected to be located anteriorly.
1
We describe anunusual cause for non-detection of a metallic retained intraocularforeign body (RIOFB) using routine ocular ultrasonography (USG),which was evident on a plain orbital radiograph.
On B-scan, a typical metallic foreign body produces a verybright signal that persists at low sensitivity settings.
2
Moreover,there is normally a marked ‘shadowing’ of the ocular and orbitalstructures just posterior to the RIOFB. Very small foreign bodies,however, may be highly reflective on A-scan and produce brightsignals on B-scan but may not produce obvious shadowing. Theseare usually <0.5 mm in diameter or are very thin.
3
With an overalldetection rate of 93%, USG is considered a more sensitive investi-gative tool than plain roentgenograms (40%) for the imaging ofRIOFB.
4
C
ASE
REPORT
A 24-year-old man presented with a history of injury in his righteye while working with a hammer and chisel 2 days previously. Hisvision was hand movements with accurate projection of rays in theaffected eye. Anterior segment of the right eye was normal and didnot reveal any sign of a penetrating wound. Vitreous haemorrhagein the involved eye obscured further posterior segment visualiza-tion. The left eye was normal.
A routine USG (A-B scan) revealed an inferior retinal detach-ment with vitreous echoes suggestive of vitreous haemorrhage.A routine radiograph of the orbit (all trauma cases undergo suchradiography in our institute) revealed a radio dense area in theregion of the right eyeball suggestive of an RIOFB. For preciselocalization of the RIOFB, USG was performed. Repeated exam-inations by this modality failed to reveal any intraocular ororbital foreign body. The dilemma of the presence (on radio-graph) or absence (on USG) of the RIOFB could have beencleared up with a computed tomography scan, but financialreasons prevented it.
The patient was booked for vitreoretinal surgery in view of theassociated retinal detachment. Perioperatively, as the initial vitrec-tomy was being performed, a 2 mm
×
1 mm-sized iron piece wasseen to lie just over the optic disc. The RIOFB was taken outthrough the parsplana route using an intraocular magnet. Theretina was reattached by internal subretinal fluid drainage followedby silicone oil injection. Had there not been a retinal detachment(picked up on USG only, as vitreous haemorrhage had obscuredproper visualization and intraocular pressure was normal) associ-ated with this case, we would not have operated immediately as theforeign body would have been intraorbital, rather than intraocular,

334 Letters to the Editor
and would have waited for the haemorrhage to clear up on its ownfor up to 2 months. The ‘missed’ RIOFB could have further deteri-orated the ocular condition.
D
ISCUSSION
There are several methods of ultrasonographic examination of apatient: supine, reclining or sitting. Most examinations are per-formed with the patient in a supine position. In B-scans, a typicalmetallic foreign body produces a very bright signal that persists atlow sensitivity settings
2
and there is a marked ‘shadowing’ justposterior to the structures. Tracing this ‘shadowing’ forwardsusually helps in locating the RIOFB. In our case, the ‘shadowing’was not discernible as the RIOFB was lying just over the optic discand the ‘shadowing’ might have coincided with the normal opticnerve echoes in B-scans. Initial as well as repeat USG were per-formed in the supine position. To reduce the occurrence of such anapparent contradiction, we recommend that in cases with a strongsuspicion of RIOFB (clinically or radiographically), a repeat ultra-sonography be performed in a sitting position as this may shift theRIOFB from its old dependent site (over the disc, while reclining)to a new one, as vitreous liquefaction tends to occur in traumatizedeyes.
Gunjan Prakash
MD
, Pradeep Venkatesh
MD
andSatpal Garg
MD
Dr Rajendra Prasad Centre for Ophthalmic Sciences,All India Institute of Medical Sciences,
Ansari Nagar, New Delhi,India
R
EFERENCES
1. Deramo VA, Shah GK, Baumal CR
et al.
Ultrasound biomicro-scopy as a tool for detecting and localizing occult foreignbodies after ocular trauma.
Ophthalmology
1999;
106
: 301–5.2. Green RL, Byrne SF. Diagnostic ophthalmic ultrasound. In:
Ryan SJ, ed.
Retina
, Vol. 1. St Louis: CV Mosby, 2001; 266.3. Byrne SF, Green RL.
Ultrasound of the Eye and Orbit
. St Louis: CVMosby, 1992; 108.
4. Bryden FM, Pyott AA, Bailey M, McGhee CN. Real timeultrasound in the assessment of intraocular foreign bodies.
Eye
1990;
4
: 727–31.
Suprachoroidal haemorrhage following Nd:YAG laser posterior capsulotomy
A
BSTRACT
Nd:YAG laser posterior capsulotomy is the commonest proce-dure for posterior capsule thickening following cataract surgery.Complications following this laser surgery are relatively few, andthis is ordinarily a safe and effective procedure. Herein a case isdescribed of suprachoroidal haemorrhage following Nd:YAGlaser posterior capsulotomy. To the best of the authors’ knowl-edge, this is the first report of this complication. Patients under-
going this procedure should be warned of this rare but potentiallydevastating complication.
Key words:
Nd:YAG capsulotomy, retinal detachment, supra-choroidal haemorrhage.
I
NTRODUCTION
Nd:YAG laser posterior capsulotomy is the most common proce-dure for posterior capsule thickening following cataract surgery.Complications following this laser surgery are relatively few; how-ever, raised intraocular pressure, anterior uveitis, cystoid macularoedema, macular hole, retinal tear and detachment, choroidaleffusion, damage to intraocular lens and intraocular lens dislocationhave been documented.
Herein, we describe a case of suprachoroidal haemorrhage(SCH) following Nd:YAG laser posterior capsulotomy, which webelieve has not been reported previously.
C
ASE
REPORT
A 66-year-old woman presented with a l-week history of painfulloss of vision in the left eye following Nd:YAG laser posteriorcapsulotomy. She gave a history of blurring of vision in her lefteye, which started several hours after the Nd:YAG laser capsulot-omy. She had uncomplicated extracapsular cataract surgery withinsertion of a +8.0 D posterior chamber intraocular lens, resultingin vision of 6/7.5 postoperatively. She was myopic and had an axiallength of 27.87 mm in this eye. Six years following surgery, thepatient presented with visual deterioration to 6/18 because ofposterior capsule thickening, and routine Nd:YAG laser capsulot-omy (total energy 50.4 mJ) was carried out without event. A statdose of Gt Iopidine 1.15% (Alcon Laboratories, Hemel Hemp-stead, Herts, UK) was given to this eye and the patient wasdischarged on Gt Predsol 0.5% (Celltech Pharmaceuticals, Slough,Berks, UK) q.i.d. for 4 days to the operated eye.
One week later, she presented with pain in the left eye withvision of counting fingers. On examination, the eye was slightlyinjected. However, the cornea was clear and the anterior chamberdeep. The intraocular lens was centred within the bag. There wasextensive herniation of vitreous in the anterior chamber andintraocular pressure (IOP) was 4 mmHg. Fundal examinationdemonstrated 270
°
of choroidal detachment, which was solidin appearance and consistent with SCH. This was confirmed byB-scan ultrasound (Fig. 1). Detailed retinal examination excludedrhegmatogenous retinal detachment and no retinal tear was identi-fied. The patient was normotensive and not on anticoagulanttherapy. Routine blood tests, including a clotting screen, werenormal. The patient was treated with Gt Maxidex (Alcon Labora-tories) six times a day and oral Flurbiprofen SR (Abbott Laborato-ries, Maidenhead, Berks, UK) 100 mg b.d.
Review at 1 week confirmed that the pain was less; however,vision had deteriorated to hand movements. The anterior chambersigns remained unchanged and the IOP remained at 4 mmHg.Fundal examination showed persistence of the SCH, but now therewas an associated rhegmatogenous retinal detachment and detachedmacula covering the inferior 6 clock hours with a tear at the6 o’clock position. Retinal detachment surgery by pars plana vitrec-tomy, retinal cryopexy (which was possible as the tear was on flatretina after external drainage of SCH following sclerotomies and

Letters to the Editor 335
internal drainage of subretinal fluid) and 16% C
3
F
8
endotemponadewas performed. Postoperatively, the patient was instructed toposition in the face-down posture for 1 week.
At 6 months post surgery, the retina was attached and the best-corrected visual acuity was 6/24, the reduced vision was attributedto photoreceptor and retinal pigment epithelium damage sub-sequent to the macular detachment.
D
ISCUSSION
Nd:YAG laser posterior capsulotomy is ordinarily a safe andeffective procedure for posterior capsular thickening followingextracapsular cataract surgery. To the best of our knowledge, SCHfollowing Nd:YAG laser posterior capsulotomy has not beenreported before. SCH generally occurs following shearing ordamage to the anterior ciliary vessels and their tributaries as theypass through the suprachoroidal space, and may result in perma-nent visual loss. Risk factors include long axial length, intraocularsurgery, high preoperative IOP, aphakia, vitreous loss, hyper-tension, use of anticoagulants and intraoperative tachycardia.
1
Itcan also happen spontaneously. In this patient, the only known riskfactor prior to Nd:YAG laser posterior capsulotomy was myopiaand axial length greater than 25 mm is a significant factor.
1
Visualoutcome is often poor in this condition.
2,3
It is possible that the SCH happened spontaneously but webelieve that the SCH in this patient was related to the Nd:YAGlaser posterior capsulotomy because of the temporal associationof the two events. Fluctuation in IOP following Nd:YAG laserposterior capsulotomy is well documented.
4–6
IOP rise usuallyreaches maximum within the first few hours after Nd:YAG laserposterior capsulotomy and returns to normal within 24 h.
7,8
Theprecise mechanism precipitating the SCH in our patient is not
known; however, we would speculate that the fluctuation in theIOP following Nd:YAG laser posterior capsulotomy may haveresulted in the rupture of ciliary and choroidal vessels as choroidalvascular fragility is known to be present in eyes with long axiallength, resulting in SCH and subsequent anterior prolapse of thevitreous. The acute rise in IOP following SCH could account forthe pain at presentation. It was likely that the vitreous tractionassociated with the anterior prolapse of the vitreous had caused aretinal tear and subsequent retinal detachment. Although a singlecase report may not carry much weight, we would like to stress thata relationship may well exist between Nd:YAG posterior capsulot-omy and SCH.
We believe that patients undergoing Nd:YAG laser posteriorcapsulotomy should be warned of this rare but potentiallydevastating ocular complication and to contact the treating oph-thalmologist so that prompt and appropriate treatment can beinstituted.
Wing C Chan
FRCOphth
, Stuart J McGimpsey
MRCOphth
,Martin F Murphy
FRCOphth
andRichard M Best
MD FRCOphth
Department of Ophthalmology, Eye and Ear Clinic, Royal VictoriaHospital, Belfast, Northern Ireland, UK
R
EFERENCES
1. Speaker MG, Guerriero PN, Met JA, Coad CT, Berger A,Marmor M. A case-control study of risk factors for intra-operative suprachoroidal expulsive haemorrhage.
Ophthalmol-ogy
1991;
98
: 202–10.2. Scott IU, Flynn HW, Schiffman J, Smiddy WE, Ehlies F.
Visual acuity outcomes among patients with appositional supra-choroidal haemorrhage.
Ophthalmology
1997; 104: 2039–46.3. Wirostko WJ, Han DP, Mieler WF, Pulido JS, Connor TB,
Kuhn E. Suprachoroidal haemorrhage: outcome of surgicalmanagement according to haemorrhage severity. Ophthalmol-ogy 1998; 105: 2271–5.
4. Channell MM, Beckman H. Intraocular pressure changes afterNd:YAG laser posterior capsulotomy. Arch Ophthalmol 1984;102: 1024–6.
5. Stark WJ, Worthen D, Halliday JT, Murray G. Nd:YAG laser:an FDA report. Ophthalmology 1985; 92: 209–12.
6. Kraff MC, Sanders DR, Lieberman HL. Intraocular pressureand the corneal endothelium after Nd:YAG laser posteriorcapsulotomy: relative effects of aphakia and pseudophakia.Arch Ophthalmol 1985; 103: 511–14.
7. Richter CU, Arzeno G, Pappas HR, Steinert RF, Puliafito C,Epstein DL. Intraocular pressure elevation following Nd:YAGlaser posterior capsulotomy. Ophthalmology 1985; 92: 636–40.
8. Slomovic AR, Parrish RK. Acute elevations of intraocularpressure following Nd:YAG laser posterior capsulotomy. Oph-thalmology 1985; 92: 973–6.
Figure 1. B-scan ultrasound illustrating suprachoroidal haemor-rhage on presentation.