Embed Size (px)
Citation preview
UNSCEAR 1988 REPORTAppendix to Annex G
“EARLY EFFECTS IN MAN OF HIGH RADIATION DOSES”
Acute radiation effects in victimsAcute radiation effects in victimsAcute radiation effects in victimsAcute radiation effects in victimsof the Chernobyl accidentof the Chernobyl accidentof the Chernobyl accidentof the Chernobyl accident
Prepared, under the supervision of A.K. Guskova, by:
A.K. GuskovaA.V. BarabanovaA.Y. BaranovG.P. GruszdevY.K. PyatkinN.M. NadezhinaN.A. MetlyaevaG.D. SelidovkinA.A. MoiseevI.A. GusefE.M. DorofeevaI.E. Zykova
CONTENTS
INTRODUCTION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2A. INITIAL DIAGNOSIS OF ACUTE RADIATION SICKNESS . . . . . . . . . . . . . . . . . . . . . . 4B. THE BONE MARROW SYNDROME AND ITS TREATMENT . . . . . . . . . . . . . . . . . . . . 4C. OTHER INJURIES AND THEIR TREATMENT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
1. Intestinal syndrome . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 122. Oropharyngeal reactions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 123. Lung reactions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 124. Causes of death . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 135. Eye damage . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 136. Treatment of radiation burns and other injuries . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
Tables . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21

UNSCEAR 1988 REPORT2
INTRODUCTION
3. This Appendix sets out the essential findings of theclinical observation of a group of patients suffering fromacute radiation sickness following the accident at theChernobyl nuclear power plant on 26 April 1986. Theobservations were conducted at the specialized treatmentcentre in Moscow over a period of two years.
4. An initial report on the accident was submitted by theSoviet representatives to the Post-Accident ReviewMeeting held at the International Atomic Energy Agency inAugust 1986 and was summarized in IAEA Safety SeriesTechnical Report No. 75 [I1] and in [G2]. The proposal topresent this information in its present form was endorsed atthe thirty-sixth session of UNSCEAR in March 1987.
5. The basic information on the radionuclide releases andthe types of exposures of the irradiated persons coincidedwith the expected pattern for an accident at a nuclear powerplant of similar type: as much as 100% of gaseous fraction ofthe noble gases and nuclides may have escaped from theplant; caesium, iodine and tellurium isotopes accounted forup to 10�20% of the nuclide inventory, and otherradionuclides for up to 30% [I1].
6. The plant personnel and auxiliary staff present at theindustrial site in the immediate vicinity of the accident zonewere subjected to the combined effect of radiation fromseveral sources: (a) short-term external gamma/beta radiationfrom the gas emission cloud (in the case of persons in theimmediate area of the accident zone at the time of theexplosion); (b) external gamma/beta radiation of decreasingintensity, from fragments of the damaged reactor corescattered over the industrial site; (c) inhalation of gases andaerosol dust particles containing a mixture of radionuclides;and (d) deposition of these particles on the skin and mucousmembranes at the time of the intensive generation of steam ordust and the wetting of clothing (as a result of them beingblown or washed off contaminated objects).
7. However, the most significant factor was the general,external and relatively uniform whole-body gamma-irradiation and the beta-irradiation of extensive bodysurfaces, coupled (except in two cases) with a very smallintake of nuclides through inhalation, predominantly ofradioiodine and caesium isotopes. Thus, the basic clinicalpicture was that of a distinctive acute radiation sicknesscaused by gamma-irradiation of the whole body and bybeta-irradiation of extensive areas of the skin surface.
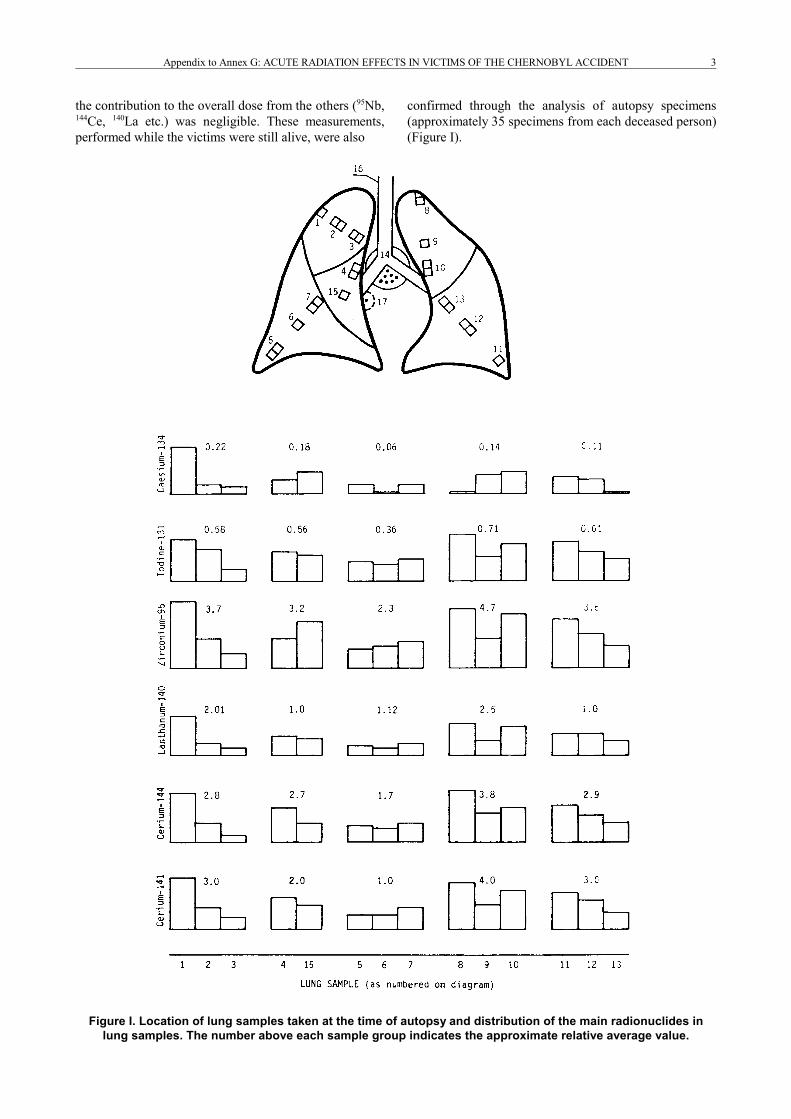
8. Direct and indirect dosimetry methods were used todetermine the nuclide content in the body. A great manytests were carried out, both while the victims were alive and(in 28 cases) after they had died, so that it was possible toestimate the nuclide content in the body and the resultantdose levels. An example of these types of analyses is shownin Figure I., giving the distribution of various radionuclidesin the lungs.
9. The iodine isotope content in the thyroid gland wasdetermined repeatedly (as many as four to six times) fromthe second day after the accident. These measurementsshowed that 131I accounted for 80 ± 20% of the total activityof all iodine isotopes, 133I for 15 ± 10%, and the remainingisotopes (123I, 124I, 126I and 130I) for not more than 2%.
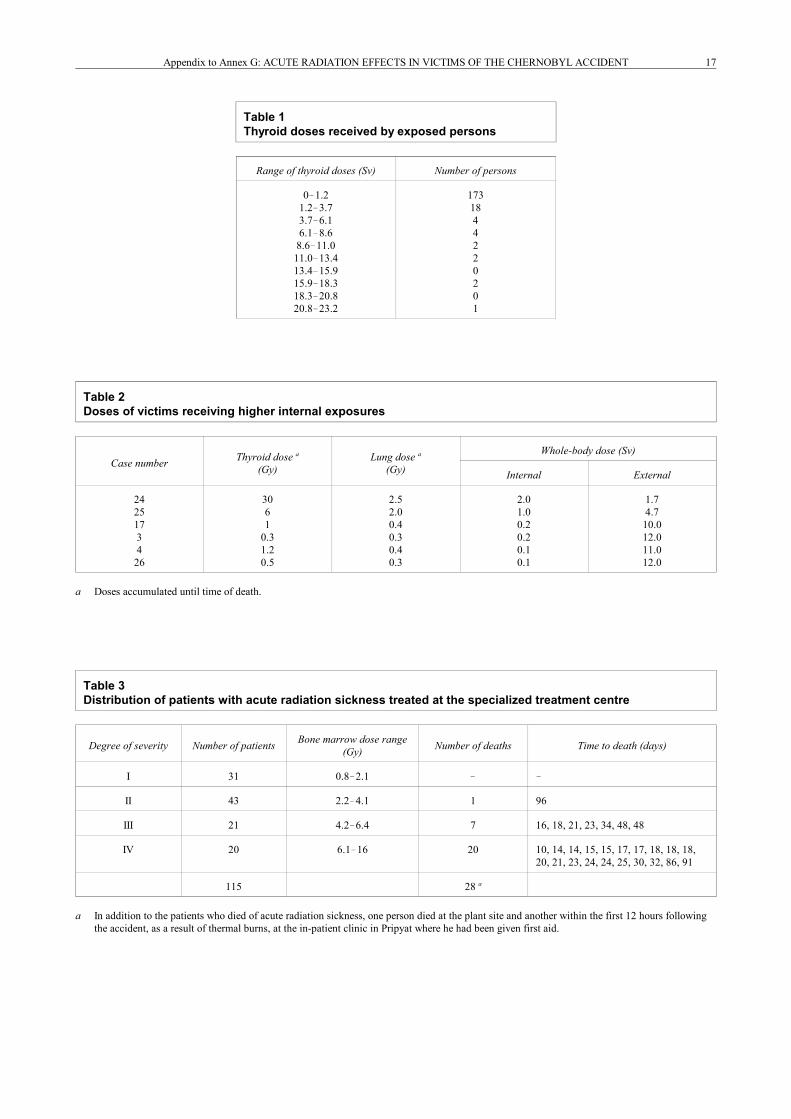
10. The calculations for estimating intake quantities fromthe thyroid measurements were performed according to therecommendations of the International Commission onRadiological Protection [I2]. On the basis of thedistribution of thyroid doses in exposed individuals (Table1), it may be stated that in the overwhelming majority ofcases the thyroid doses were below the levels likely tocause direct injury to that organ (<3.7 Sv) or ofsignificantly influencing the clinical picture during theonset of acute radiation sickness. Low radioiodine doselevels were also suggested by the post-mortem nuclidemeasurements of the 28 persons who subsequently died.
11. Internal dose values according to post-mortemmeasurements for 6 patients are shown in Table 2. Themaximum amount of 137Cs and 134Cs incorporated activitywas 7.4 MBq, except for two patients with extensive steamburns, which allowed intake of nuclides through the wound.The post-mortem dosimetry gave 40 and 80 MBq of 137Csplus 134Cs, and 450 and 1,100 MBq of 131I, for these twopatients, respectively. The whole-body internal doses inthese two individuals from these nuclides were estimated asapproximately 1 Sv and 2 Sv during the two to three weeksbefore they died, which are commensurable with theirexternal gamma doses. This fact was taken into accountduring the interpretation of clinical data. Internal doses forother patients did not exceed 1�3% of the externalirradiation doses.
12. The transuranic elements (e.g., 239Pu) were studied inurine specimens from 266 persons (635 analyses),including, in some of the cases, analyses conducted beforeand after the administration of pentacine. The urine activityvalues and a negative finding after chelation treatmentconfirmed the absence of a significant plutoniumcontamination of all the patients observed. Post-mortemtests by alpha spectrometry for transuranic elementsshowed their presence (74�300 Bq per organ) only in thelungs; curium accounted for as much as 90% of thespecimen activity, and plutonium and americium for 10%.
13. Gamma-spectrometric analysis of the first specimenswithin 36�39 hours of the accident failed to reveal any signof 22,24Na activation, which confirmed that neutronirradiation of the victims was not significant.
14. For most of the victims, the energy peaks of morethan 20 radionuclides were detectable in the spectrum oftheir whole-body gamma measurements; however, apartfrom the iodine and caesium isotopes previously mentioned,
Appendix to Annex G: ACUTE RADIATION EFFECTS IN VICTIMS OF THE CHERNOBYL ACCIDENT 3
the contribution to the overall dose from the others (95Nb,144Ce, 140La etc.) was negligible. These measurements,performed while the victims were still alive, were also
confirmed through the analysis of autopsy specimens(approximately 35 specimens from each deceased person)(Figure I).
Figure I. Location of lung samples taken at the time of autopsy and distribution of the main radionuclides inlung samples. The number above each sample group indicates the approximate relative average value.

UNSCEAR 1988 REPORT4
15. The dose levels from external irradiation werereconstructed from the indication of several measurementson the basis of previous experience. Subsequently, in threecases with a lethal outcome, these findings were refinedusing methods earlier proposed by Kraytor for clothingfabrics [B1] and according to the electron spin resonancetechnique for dental enamel [T1]. These measurementsagreed within ± 20% with the dose estimates based onclinical and biological criteria.
16. The total number of affected individuals among thepersons present at the reactor site in the early hours of 26April 1986 was 203, as given in the report presented bySoviet representatives at the Post-Accident Review Meetingin August 1986 [I1]. Of these, 115 were treated, beginningon day 2, at the specialized treatment centre in Moscow; itwas this group that provided most of the scientificanalytical data discussed in this report. At other hospitals inKiev there were only 12 patients with a clearly definedclinical pattern of second-degree acute radiation sicknessand one person with fourth-degree acute radiation sickness,a fact that cannot in any substantial way alter the overallassessment of the data for the entire group of victims.
17. The increase in the total number of affectedindividuals from 203 to 237, announced in November 1986,was due solely to persons suffering from first-degree acuteradiation sickness. There were 31 persons suffering fromfirst-degree acute radiation sickness at the special treatmentcentre in Moscow and 109 persons in Kiev. The task ofestablishing a diagnosis distinguishing between first-degreeacute radiation sickness and ordinary somatic diseasesaccording to generally accepted criteria is a complex one,and one that continued throughout 1986. On the whole, acritical analysis of the data shows a decrease in the numberof persons suffering from first-degree acute radiationsickness in comparison with the number given originally.At the time of writing this report, up to three quarters ofthese persons are for all practical purposes healthy. Theirclinical signs of reaction to the accident during the firstthree months were neither individually significant nortypical of a reaction to irradiation. Table 3 shows thedistribution of patients with acute radiation sicknessaccording to its degree of severity [B1] in the groupselected for scientific analysis.
A. INITIAL DIAGNOSIS OF ACUTE RADIATION SICKNESS
18. The medical unit serving the plant was informed ofthe accident within 10�15 minutes of its occurrence. Firstaid to the affected individuals was provided b,, middle-levelmedical personnel and emergency teams over a time periodfrom 30�40 minutes to 3�6 hours after the accident. Firstaid consisted in the evacuation of the victims from theindustrial site, the simplest forms of medical attention, theadministration of antiemetic and symptomatic (sedative,cardiotonic) drugs, the distribution of potassium iodide andthe transportation of persons suffering from a pronounced
primary reaction to the medical unit. During the first 12�24hours after the accident, other persons who were insatisfactory condition were urged to go to the medical unitfor examination; a total of 132 persons were hospitalizedthere during the first 12 hours. One person with severethermal burns died during the first hour. Another, a reactoroperator, could not be found; his working station waslocated in the collapsed high-activity zone.
19. Within 12 hours, a specialized emergency teamarrived at the site and began work. Within 36 hours, thisteam, together with the on-site medical unit, examined morethan 350 persons and carried out approximately 1,000blood tests, each person undergoing two to three such tests.The treatment with potassium iodide was continued.
20. Within the first three days, 299 persons suspected ofsuffering from acute radiation sickness were sent to thespecialized treatment centre in Moscow and to hospitals inKiev, and over the subsequent days some 200 additionalpersons were admitted for examination.
21. The primary diagnostic criteria for assessing thepriority for hospitalization were the presence, time of onsetand intensity of nausea and vomiting and of primaryerythema of the skin and mucosae, and a decrease of thelymphocyte count in the peripheral blood to below IT/1during the first days following irradiation.
22. The diagnosis of acute radiation sickness wassubsequently confirmed in 99 of the 128 persons (firemen,Unit 4 operators, turbine-room duty officer and auxiliarypersonnel) admitted to the specialized treatment centre inMoscow during the first two days and in six of the 74victims hospitalized during the following three days. Thisis an indication of the high specificity of the screeningmethods used. An additional 10 cases of minor acuteradiation sickness were diagnosed among persons presentat the site at the time of the accident, who were lateradmitted to the hospital facility for a variety of reasons. Inthe reception area the patients were monitored again forcontamination and, if necessary, subjected to decontamina-tion measures (washing under a shower with ordinary soapand change of underwear). Blood and urine samples weretaken for a quick test of the presence of radionuclides; thepatients also underwent measurements (repeated a further4�6 times during the first 6�10 days) of the radioactiveiodine content in the thyroid. Measuring devices consistingof a scintillation detector or a semiconductor detection unitwere used for the whole-body counting of radionuclideactivity.
B. THE BONE MARROW SYNDROME AND ITS TREATMENT
23. Dosimetric data, together with an analysis of thecircumstances of the accident and the presence in aconsiderable number of the victims of obvious primaryreaction symptoms (nausea, vomiting, diarrhoea, hyper-

Appendix to Annex G: ACUTE RADIATION EFFECTS IN VICTIMS OF THE CHERNOBYL ACCIDENT 5
Figure II. Estimation of the total gamma dose according to the blood lymphocyte counts. Upper panel: Dose-effect relationships for lymphocyte counts at the days post irradiation shown on the curves;
analytical expression and coefficients of these relationships. Lower panels: Curves showing the dependence of average lymphocyte counts on days 4�7 and the minimum
lymphocyte count on days 1�8 as a function of the irradiation dose.

UNSCEAR 1988 REPORT6
D � (�a � a 2�4by) /2b
y � (a ± 2.24)D � (b ± 0.56)D 2
aemia of the mucosae and skin, lymphopenia), confirmedthat the principal modes of irradiation had been: (a) byexternal, relatively uniform gamma-radiation; and (b) bydeposition of beta/gamma-emitting nuclides on the skin.Radionuclide ingestion was below the level likely to causeacute radiation injury. As already noted, two patientssuffered from all three of these irradiation modalities, incombination with extensive steam burns.
24. The important diagnostic task during the first fewdays after the accident was the assessment of the degree ofseverity of the bone marrow syndrome resulting from theexternal gamma-irradiation dose. This was possible throughthe use of previously devised methods, which are based onthe number of lymphocytes and on chromosome aberrationsin peripheral-blood lymphocytes or on the incidence ofchromosome aberrations in bone marrow cells [B1, B2,G1]. These data were later transformed into a prognosis ofthe overall dynamics of the blood picture. A subsequentreassessment of dose levels involving a larger sample ofcells scored revealed not more than 5�10% changes in theestimated doses.
25. Dose-effect relationships for these indicators hadbeen derived earlier through the analysis of relativelyuniform accidental or therapeutic irradiations of humansubjects having normal initial haematological character-istics and exposed to well established doses [P1]. Figure IIshows the curves (and analytical expressions) for therelationships between the dose and the blood lymphocytecount for each of the first nine days and the averagelymphocyte count on days 4�7 and days 1�8 after irradia-tion. The radiation dose received by each person wasestimated according to the number of chromosomeaberrations (dicentrics) in a blood-lymphocyte culture,using a dose-effect curve for 100 first-mitosis cells that hadbeen obtained after whole-body gamma-irradiation to treatacute leukaemia patients during a period of full clinical andhaematological remission [P2].
26. The formula for calculating of the dose is as follows:
This assumes that the yield of dicentrics shows a linear-quadratic dependence on dose:
where D is the average gamma-irradiation dose in the body(Gy), y is the dicentric count per 100 cells; a = 8.36; b = 5.70.
27. Up to day 7 after the accident, the estimates of theaverage dose of total gamma-irradiation were refined,mostly on the basis of the peripheral-blood lymphocytecounts but also, in the more severe cases and to a lesser
degree, on the chromosome aberration count. Ibis made itpossible to divide the patients into various prognosticgroups [B1], according to the severity of the bone marrowsyndrome as follows (see Table 3):
(I) slight (1�2 Gy)(II) intermediate (2�4 Gy)(III) severe (4�6 Gy)(IV) extremely severe (6 Gy and above)
It was also possible to separate those persons who receiveddoses of less than 1 Gy.
28. Particular attention during the first days was directedat identifying persons with an extremely severe andirreversible degree of myelodepression, for whom an urgentdecision was required regarding a bone marrow transplant.Additional signs providing further evidence that a patientbelonged to this group were (a) vomiting during the firsthalf-hour and of diarrhoea during the first 1�2 hours fromthe start of irradiation; (b) a swelling of the parotid glandsduring the first 24�36 hours; and (c) the ascertainment ofan irreversible degree of myelodepression using adiagnostic table previously devised (Table 4).
29. The results of numerous biochemical, immunologicaland biophysical indicators are undergoing processing andanalysis at the time of writing this report. None of theseindicators is as informative as the signs described above.However, it may be noted, for example, that hyper-amylasemia has used as a supplementary prognostic test.
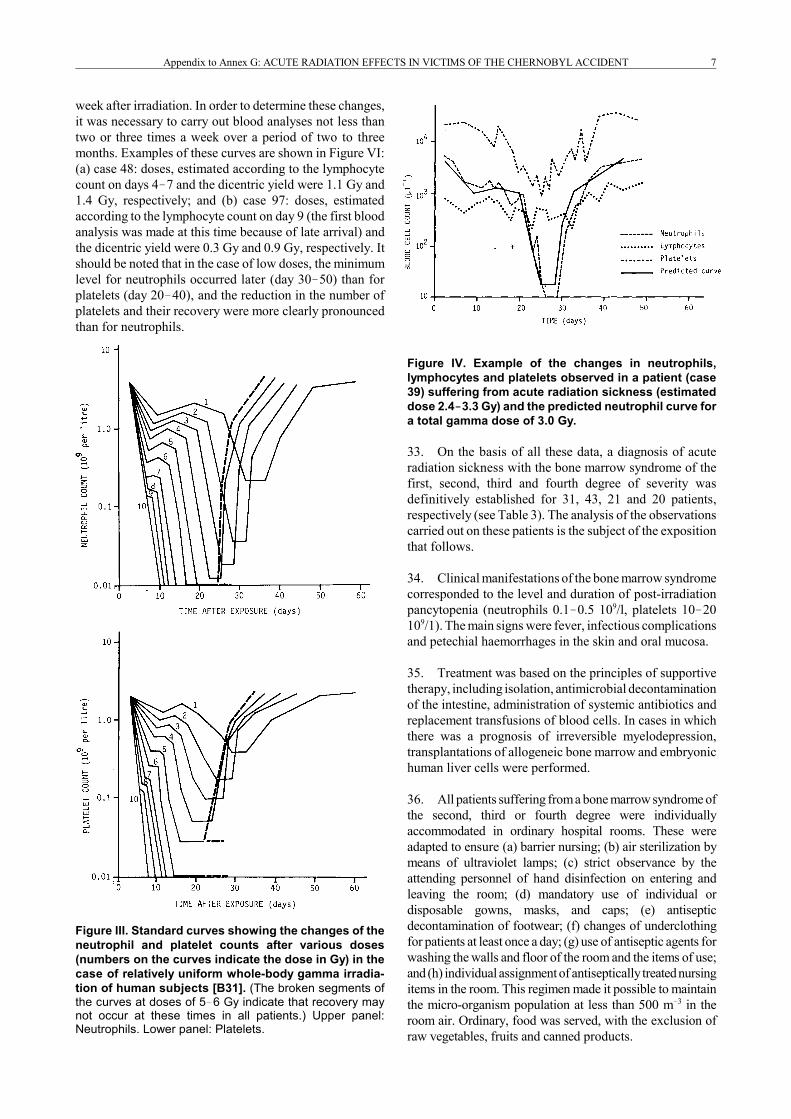
30. On the basis of the estimated dose, a prediction wasmade using standard curves [P1], of the overall trend withtime in the neutrophil and platelet counts (Figure III). By wayof example, Figure IV shows the real and predictedneutrophil curves for one patient (case 39). The total gamma-irradiation doses estimated according to the averagelymphocyte count from day 4 to day 7 and according to thedicentric yield totalled 2.4 and 3.3 Gy, respectively. Thepatient's measured neutrophil curve almost coincided with thepredicted neutrophil curve for 3.0 Gy of total gamma-irradiation.
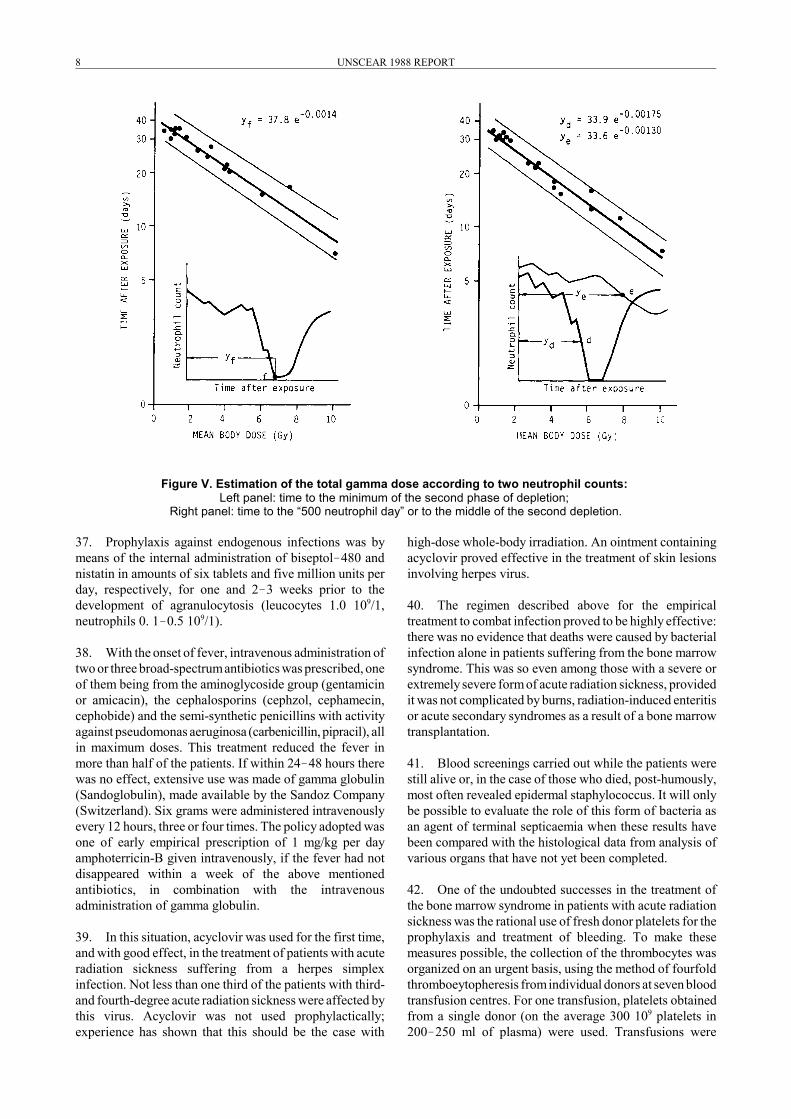
31. The calibration curves of neutrophil counts as afunction of dose were also used for a final assessment ofthe magnitude of the total gamma-irradiation dose. Thedose calibration curve was chosen that coincided with themeasured second depletion phase. Also. use was made ofthe dose dependency, of the second depletion phase, suchas the time required for the neutrophil count to decrease to0.5 109/1 or the time to reach the minimum of the seconddepletion phase (Figure V).
32. For relatively low doses (1.0�1.5 Gy), the diagnosiswas finally established over time periods of up to threemonths only in those cases that showed typical post-irradiation neutrophil and/or platelet time courses withdistinct second depletion and restoration phases. The lattergenerally developed beginning in the fourth to the fifth
Appendix to Annex G: ACUTE RADIATION EFFECTS IN VICTIMS OF THE CHERNOBYL ACCIDENT 7
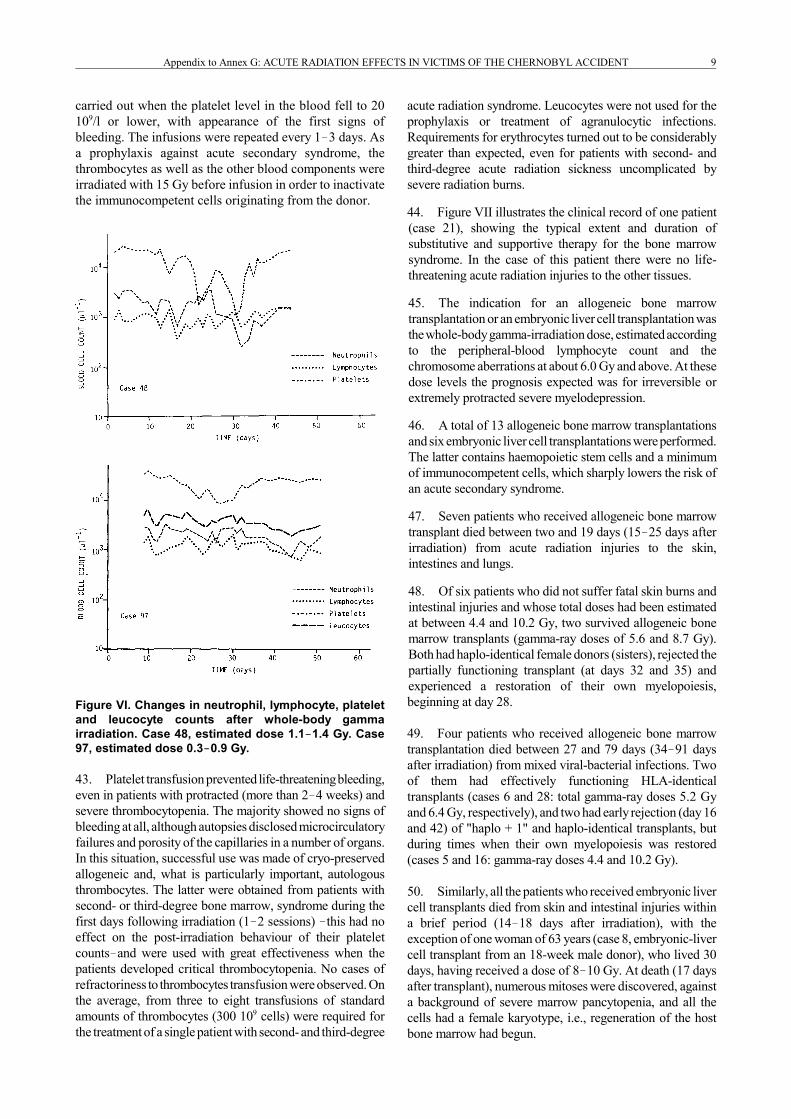
week after irradiation. In order to determine these changes,it was necessary to carry out blood analyses not less thantwo or three times a week over a period of two to threemonths. Examples of these curves are shown in Figure VI:(a) case 48: doses, estimated according to the lymphocytecount on days 4�7 and the dicentric yield were 1.1 Gy and1.4 Gy, respectively; and (b) case 97: doses, estimatedaccording to the lymphocyte count on day 9 (the first bloodanalysis was made at this time because of late arrival) andthe dicentric yield were 0.3 Gy and 0.9 Gy, respectively. Itshould be noted that in the case of low doses, the minimumlevel for neutrophils occurred later (day 30�50) than forplatelets (day 20�40), and the reduction in the number ofplatelets and their recovery were more clearly pronouncedthan for neutrophils.
Figure III. Standard curves showing the changes of theneutrophil and platelet counts after various doses(numbers on the curves indicate the dose in Gy) in thecase of relatively uniform whole-body gamma irradia-tion of human subjects [B31]. (The broken segments ofthe curves at doses of 5�6 Gy indicate that recovery maynot occur at these times in all patients.) Upper panel:Neutrophils. Lower panel: Platelets.
Figure IV. Example of the changes in neutrophils,lymphocytes and platelets observed in a patient (case39) suffering from acute radiation sickness (estimateddose 2.4����3.3 Gy) and the predicted neutrophil curve fora total gamma dose of 3.0 Gy.
33. On the basis of all these data, a diagnosis of acuteradiation sickness with the bone marrow syndrome of thefirst, second, third and fourth degree of severity wasdefinitively established for 31, 43, 21 and 20 patients,respectively (see Table 3). The analysis of the observationscarried out on these patients is the subject of the expositionthat follows.
34. Clinical manifestations of the bone marrow syndromecorresponded to the level and duration of post-irradiationpancytopenia (neutrophils 0.1�0.5 109/l, platelets 10�20109/1). The main signs were fever, infectious complicationsand petechial haemorrhages in the skin and oral mucosa.
35. Treatment was based on the principles of supportivetherapy, including isolation, antimicrobial decontaminationof the intestine, administration of systemic antibiotics andreplacement transfusions of blood cells. In cases in whichthere was a prognosis of irreversible myelodepression,transplantations of allogeneic bone marrow and embryonichuman liver cells were performed.
36. All patients suffering from a bone marrow syndrome ofthe second, third or fourth degree were individuallyaccommodated in ordinary hospital rooms. These wereadapted to ensure (a) barrier nursing; (b) air sterilization bymeans of ultraviolet lamps; (c) strict observance by theattending personnel of hand disinfection on entering andleaving the room; (d) mandatory use of individual ordisposable gowns, masks, and caps; (e) antisepticdecontamination of footwear; (f) changes of underclothingfor patients at least once a day; (g) use of antiseptic agents forwashing the walls and floor of the room and the items of use;and (h) individual assignment of antiseptically treated nursingitems in the room. This regimen made it possible to maintainthe micro-organism population at less than 500 m�3 in theroom air. Ordinary, food was served, with the exclusion ofraw vegetables, fruits and canned products.
UNSCEAR 1988 REPORT8
Figure V. Estimation of the total gamma dose according to two neutrophil counts: Left panel: time to the minimum of the second phase of depletion;
Right panel: time to the “500 neutrophil day” or to the middle of the second depletion.
37. Prophylaxis against endogenous infections was bymeans of the internal administration of biseptol�480 andnistatin in amounts of six tablets and five million units perday, respectively, for one and 2�3 weeks prior to thedevelopment of agranulocytosis (leucocytes 1.0 109/1,neutrophils 0. 1�0.5 109/1).
38. With the onset of fever, intravenous administration oftwo or three broad-spectrum antibiotics was prescribed, oneof them being from the aminoglycoside group (gentamicinor amicacin), the cephalosporins (cephzol, cephamecin,cephobide) and the semi-synthetic penicillins with activityagainst pseudomonas aeruginosa (carbenicillin, pipracil), allin maximum doses. This treatment reduced the fever inmore than half of the patients. If within 24�48 hours therewas no effect, extensive use was made of gamma globulin(Sandoglobulin), made available by the Sandoz Company(Switzerland). Six grams were administered intravenouslyevery 12 hours, three or four times. The policy adopted wasone of early empirical prescription of 1 mg/kg per dayamphoterricin-B given intravenously, if the fever had notdisappeared within a week of the above mentionedantibiotics, in combination with the intravenousadministration of gamma globulin.
39. In this situation, acyclovir was used for the first time,and with good effect, in the treatment of patients with acuteradiation sickness suffering from a herpes simplexinfection. Not less than one third of the patients with third-and fourth-degree acute radiation sickness were affected bythis virus. Acyclovir was not used prophylactically;experience has shown that this should be the case with
high-dose whole-body irradiation. An ointment containingacyclovir proved effective in the treatment of skin lesionsinvolving herpes virus.
40. The regimen described above for the empiricaltreatment to combat infection proved to be highly effective:there was no evidence that deaths were caused by bacterialinfection alone in patients suffering from the bone marrowsyndrome. This was so even among those with a severe orextremely severe form of acute radiation sickness, providedit was not complicated by burns, radiation-induced enteritisor acute secondary syndromes as a result of a bone marrowtransplantation.
41. Blood screenings carried out while the patients werestill alive or, in the case of those who died, post-humously,most often revealed epidermal staphylococcus. It will onlybe possible to evaluate the role of this form of bacteria asan agent of terminal septicaemia when these results havebeen compared with the histological data from analysis ofvarious organs that have not yet been completed.
42. One of the undoubted successes in the treatment ofthe bone marrow syndrome in patients with acute radiationsickness was the rational use of fresh donor platelets for theprophylaxis and treatment of bleeding. To make thesemeasures possible, the collection of the thrombocytes wasorganized on an urgent basis, using the method of fourfoldthromboeytopheresis from individual donors at seven bloodtransfusion centres. For one transfusion, platelets obtainedfrom a single donor (on the average 300 109 platelets in200�250 ml of plasma) were used. Transfusions were
Appendix to Annex G: ACUTE RADIATION EFFECTS IN VICTIMS OF THE CHERNOBYL ACCIDENT 9
carried out when the platelet level in the blood fell to 20109/l or lower, with appearance of the first signs ofbleeding. The infusions were repeated every 1�3 days. Asa prophylaxis against acute secondary syndrome, thethrombocytes as well as the other blood components wereirradiated with 15 Gy before infusion in order to inactivatethe immunocompetent cells originating from the donor.
Figure VI. Changes in neutrophil, lymphocyte, plateletand leucocyte counts after whole-body gammairradiation. Case 48, estimated dose 1.1����1.4 Gy. Case97, estimated dose 0.3����0.9 Gy.
43. Platelet transfusion prevented life-threatening bleeding,even in patients with protracted (more than 2�4 weeks) andsevere thrombocytopenia. The majority showed no signs ofbleeding at all, although autopsies disclosed microcirculatoryfailures and porosity of the capillaries in a number of organs.In this situation, successful use was made of cryo-preservedallogeneic and, what is particularly important, autologousthrombocytes. The latter were obtained from patients withsecond- or third-degree bone marrow, syndrome during thefirst days following irradiation (1�2 sessions) �this had noeffect on the post-irradiation behaviour of their plateletcounts�and were used with great effectiveness when thepatients developed critical thrombocytopenia. No cases ofrefractoriness to thrombocytes transfusion were observed. Onthe average, from three to eight transfusions of standardamounts of thrombocytes (300 109 cells) were required forthe treatment of a single patient with second- and third-degree
acute radiation syndrome. Leucocytes were not used for theprophylaxis or treatment of agranulocytic infections.Requirements for erythrocytes turned out to be considerablygreater than expected, even for patients with second- andthird-degree acute radiation sickness uncomplicated bysevere radiation burns.
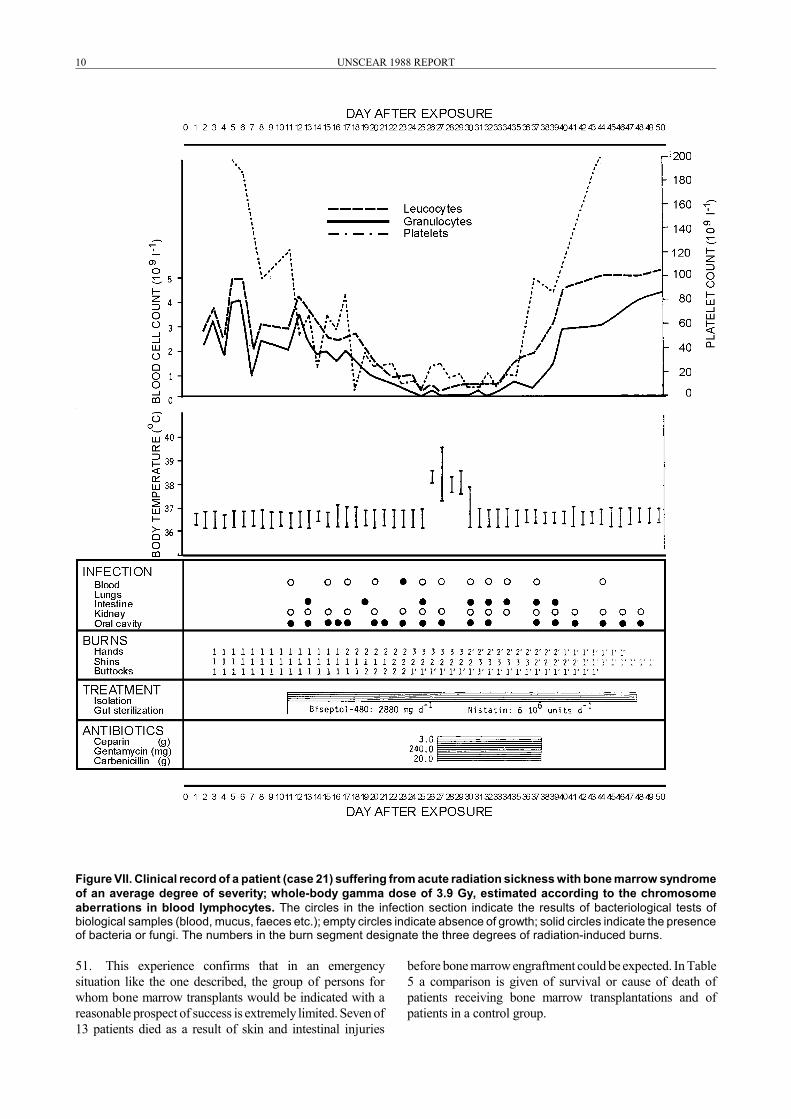
44. Figure VII illustrates the clinical record of one patient(case 21), showing the typical extent and duration ofsubstitutive and supportive therapy for the bone marrowsyndrome. In the case of this patient there were no life-threatening acute radiation injuries to the other tissues.
45. The indication for an allogeneic bone marrowtransplantation or an embryonic liver cell transplantation wasthe whole-body gamma-irradiation dose, estimated accordingto the peripheral-blood lymphocyte count and thechromosome aberrations at about 6.0 Gy and above. At thesedose levels the prognosis expected was for irreversible orextremely protracted severe myelodepression.
46. A total of 13 allogeneic bone marrow transplantationsand six embryonic liver cell transplantations were performed.The latter contains haemopoietic stem cells and a minimumof immunocompetent cells, which sharply lowers the risk ofan acute secondary syndrome.
47. Seven patients who received allogeneic bone marrowtransplant died between two and 19 days (15�25 days afterirradiation) from acute radiation injuries to the skin,intestines and lungs.
48. Of six patients who did not suffer fatal skin burns andintestinal injuries and whose total doses had been estimatedat between 4.4 and 10.2 Gy, two survived allogeneic bonemarrow transplants (gamma-ray doses of 5.6 and 8.7 Gy).Both had haplo-identical female donors (sisters), rejected thepartially functioning transplant (at days 32 and 35) andexperienced a restoration of their own myelopoiesis,beginning at day 28.
49. Four patients who received allogeneic bone marrowtransplantation died between 27 and 79 days (34�91 daysafter irradiation) from mixed viral-bacterial infections. Twoof them had effectively functioning HLA-identicaltransplants (cases 6 and 28: total gamma-ray doses 5.2 Gyand 6.4 Gy, respectively), and two had early rejection (day 16and 42) of "haplo + 1" and haplo-identical transplants, butduring times when their own myelopoiesis was restored(cases 5 and 16: gamma-ray doses 4.4 and 10.2 Gy).
50. Similarly, all the patients who received embryonic livercell transplants died from skin and intestinal injuries withina brief period (14�18 days after irradiation), with theexception of one woman of 63 years (case 8, embryonic-livercell transplant from an 18-week male donor), who lived 30days, having received a dose of 8�10 Gy. At death (17 daysafter transplant), numerous mitoses were discovered, againsta background of severe marrow pancytopenia, and all thecells had a female karyotype, i.e., regeneration of the hostbone marrow had begun.
UNSCEAR 1988 REPORT10
Figure VII. Clinical record of a patient (case 21) suffering from acute radiation sickness with bone marrow syndromeof an average degree of severity; whole-body gamma dose of 3.9 Gy, estimated according to the chromosomeaberrations in blood lymphocytes. The circles in the infection section indicate the results of bacteriological tests ofbiological samples (blood, mucus, faeces etc.); empty circles indicate absence of growth; solid circles indicate the presenceof bacteria or fungi. The numbers in the burn segment designate the three degrees of radiation-induced burns.
51. This experience confirms that in an emergencysituation like the one described, the group of persons forwhom bone marrow transplants would be indicated with areasonable prospect of success is extremely limited. Seven of13 patients died as a result of skin and intestinal injuries
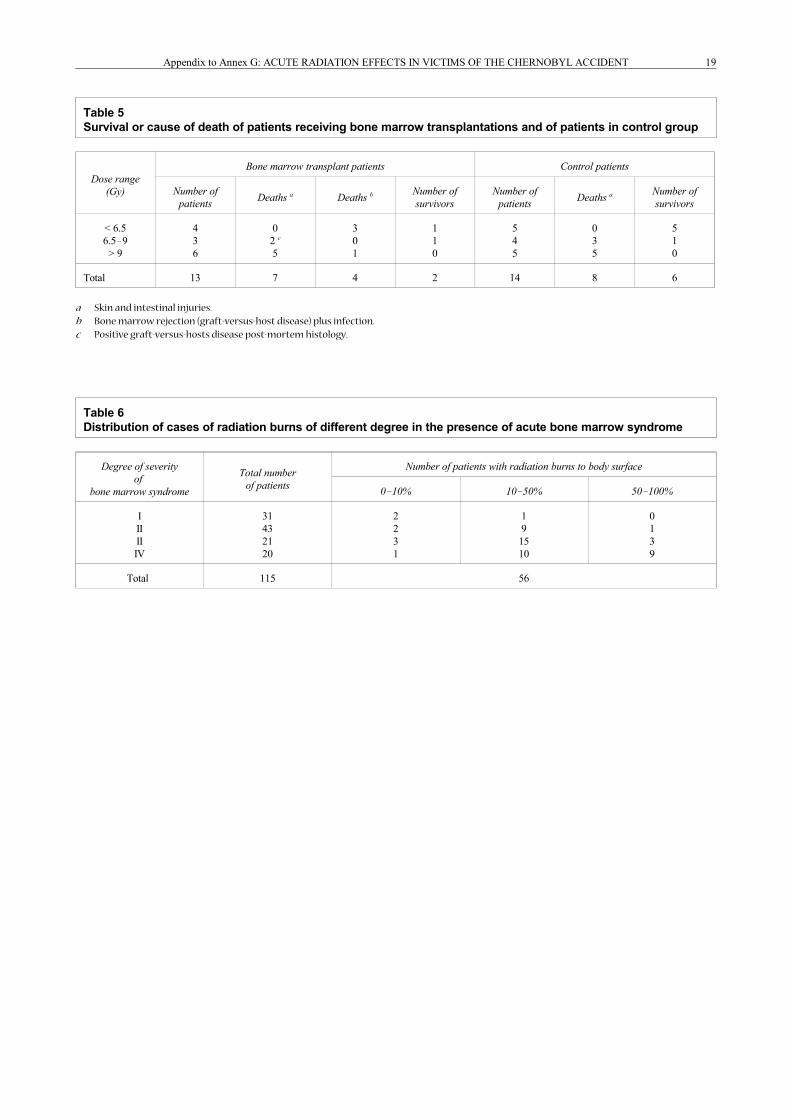
before bone marrow engraftment could be expected. In Table5 a comparison is given of survival or cause of death ofpatients receiving bone marrow transplantations and ofpatients in a control group.
Appendix to Annex G: ACUTE RADIATION EFFECTS IN VICTIMS OF THE CHERNOBYL ACCIDENT 11
C. OTHER INJURIES AND THEIRTREATMENT
52. The extensive skin lesions caused by beta-radiationrepresented a distinctive feature of the injuries suffered inthis emergency situation. Radiation-induced skin burns infiremen and personnel from the plant were observed only incombination with radiation injury, to haemopoiesis andwere therefore an integral part of the general acute radiationsickness.
53. This situation may be regarded as one in which thereis an extremely non-uniform distribution of dose as afunction of the depth of penetration within the body; theskin doses are estimated to be 10�20 times greater than thebone marrow doses. There was a definite correlation in theseverity of the injuries in both tissues.
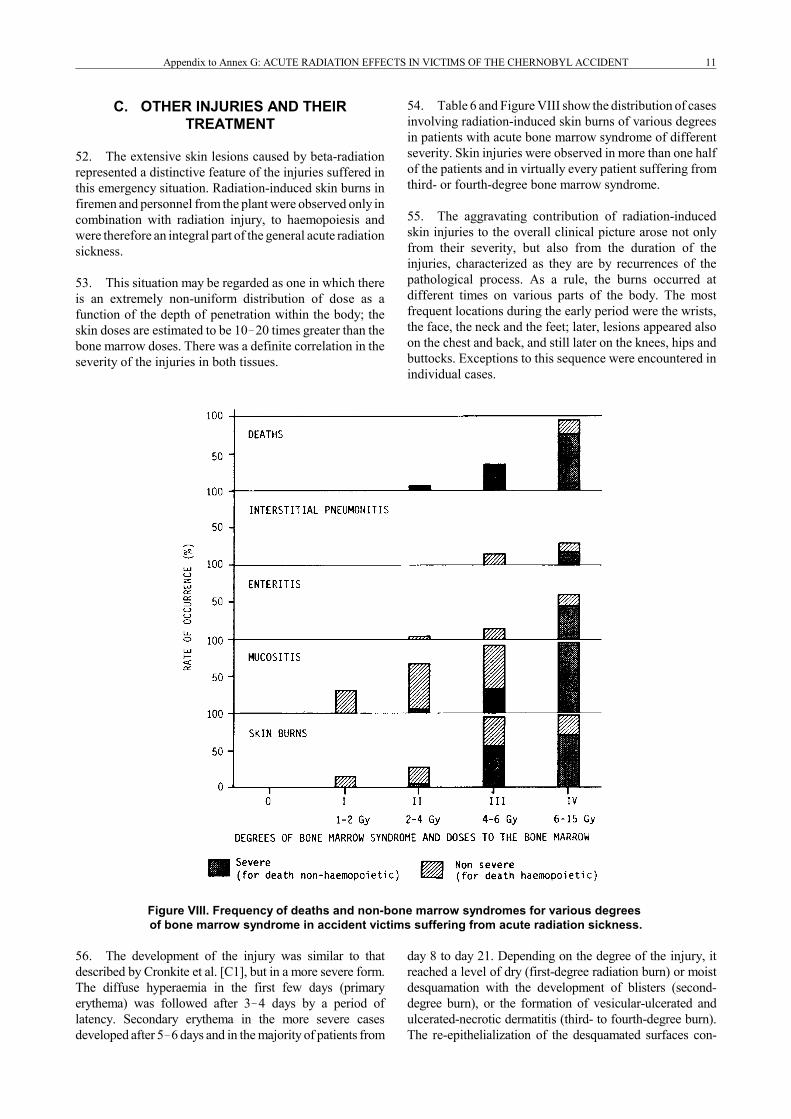
54. Table 6 and Figure VIII show the distribution of casesinvolving radiation-induced skin burns of various degreesin patients with acute bone marrow syndrome of differentseverity. Skin injuries were observed in more than one halfof the patients and in virtually every patient suffering fromthird- or fourth-degree bone marrow syndrome.
55. The aggravating contribution of radiation-inducedskin injuries to the overall clinical picture arose not onlyfrom their severity, but also from the duration of theinjuries, characterized as they are by recurrences of thepathological process. As a rule, the burns occurred atdifferent times on various parts of the body. The mostfrequent locations during the early period were the wrists,the face, the neck and the feet; later, lesions appeared alsoon the chest and back, and still later on the knees, hips andbuttocks. Exceptions to this sequence were encountered inindividual cases.
Figure VIII. Frequency of deaths and non-bone marrow syndromes for various degrees of bone marrow syndrome in accident victims suffering from acute radiation sickness.
56. The development of the injury was similar to thatdescribed by Cronkite et al. [C1], but in a more severe form.The diffuse hyperaemia in the first few days (primaryerythema) was followed after 3�4 days by a period oflatency. Secondary erythema in the more severe casesdeveloped after 5�6 days and in the majority of patients from
day 8 to day 21. Depending on the degree of the injury, itreached a level of dry (first-degree radiation burn) or moistdesquamation with the development of blisters (second-degree burn), or the formation of vesicular-ulcerated andulcerated-necrotic dermatitis (third- to fourth-degree burn).The re-epithelialization of the desquamated surfaces con-

UNSCEAR 1988 REPORT12
tinued for two or three weeks from the occurrence of thevisible injury to the skin. In six patients, the healing of theburns over skin areas involving deep necrosis did not beginuntil the end of the second month. A characteristic feature inthe time course of the burns, and one which could bemonitored throughout in this group of victims, was theappearance of recurrent waves of erythema, beginning by theend of the fourth week and continuing up to days 45�60.These changes were characterized by hyperaemia on thepreviously unaffected skin areas or by the increase in clinicalsigns of injury at the foci of the primary lesions then in theprocess of healing. For example, late secondary erythemaappeared in the area of the ankles and feet, or on the hips andbuttocks, of those patients who during the first three weeksdisplayed "flowering" burns on their knees. By the time ofappearance of this late erythema, the lesions that hadoccurred earlier in many instances had already been repaired.As a rule, late erythema was accompanied by oedema of thesubcutaneous tissues, which was particularly noticeable whenlocated on the knees: pain was experienced in walking;palpation of the skin and underlying tissues (muscles,tendons) caused discomfort. The most severe cases involvedfever and a general worsening of the patient's condition. Latesecondary erythema was successfully resolved within twoweeks by purely topical treatment, although in the moresevere cases it was necessary to resort to additionaltherapeutic means, such as the prescription ofglucocorticoids, a form of treatment that fairly rapidlyeliminated all manifestations of epidermatitis andsubcutaneous oedema, both general and local.
57. As may be seen in Table 6, the burns suffered by thepatients with acute radiation sickness covered from 1% to100% of the body surface. It may be noted, in thisconnection, that if there were relatively early (from day5�6) second- or third-degree burns over an area of even30�40% of the body, followed by the spread ofhyperaemia, these burns were life-threatening. In 19 of the56 patients suffering from burns, the burns proved fatal(Figure VIII). It was found that patients with earlysecondary erythema over a body area of more than 40%first developed a febrile-toxemic syndrome, followed byrenal-hepatic insufficiency and encephalopathic coma withcerebral oedema, resulting in death at 14�48 days afterirradiation. A causal link connecting the fatal renal-hepaticinsufficiency and the encephalopathic coma to the skininjuries is confirmed by the fact that a similar developmentof such fatal syndromes was observed in several patientswho had neither severe bone marrow syndromes norintestinal syndromes. However, in the majority of cases,burns were combined with an extremely severe bonemarrow syndrome and severe acute enteritis, and in somecases the burns may have been the primary cause of death.
1. Intestinal syndrome
58. The intestinal syndrome was one of the morethreatening manifestations of acute radiation sickness. In 10patients, diarrhoea was observed from day 4 to day 8. Thissuggested that these persons had received total gamma
doses of about 10 Gy or above, all these patients diedduring the first three weeks following irradiation. Theoccurrence of diarrhoea after eight days in seven otherpersons was an indication that they had received lowerdoses. The presence of radiation-induced enteritis lastingfrom day 10 to days 18�25 in spite of intensive water-electrolyteprotein supportive treatment suggests that theintestinal syndrome was not the main cause of death.
2. Oropharyngeal reactions
59. Acute radiation-induced inflammation of the oral andpharyngeal mucosa was observed in 82 patients. Its morebenign manifestations (first and second degree of severity)were characterized by desquamation and oedema of themucosa in the area of the cheeks and tongue and bytenderness of the gums. These were observed in 42 persons(dose range 1.7�4.0 Gy) from days 8�9 to days 20�25. Thebasic signs of a more acute oropharyngeal reaction wereobserved in 40 patients with third and fourth degree acuteradiation sickness (dose range 4.5�16.0 Gy), and thesewere erosions and ulcers of the oral mucosa, sharp pain,and a large production of rubber-like mucus occasionallyblocking the throat and causing breathing problems. Thefirst signs appeared as early as days 3�4, attained theirmaximum intensity by day 10 and then subsided after days18�20, when there was also granulocytopenia. The processinvolved no selective localization, as is characteristic of theulcerated lesions in the area of the tonsils and gums whenthere are infectious complications. However, in a signifi-cant number of cases, the radiation-induced inflammationof the mucous membranes was complicated by secondarymicrobial and viral infection, which prolonged its course.
60. Another typical finding was the early (days 3�4)appearance of herpes-like rashes forming massive crusts onthe lips and facial skin; this was observed in nearly 30% ofthe patients with severe bone marrow syndrome. Withinthis group of patients, primarily those suffering fromfourth-degree acute radiation sickness, a pronouncedradiation-induced parotitis was observed, coupled with aninability to salivate and a high level of amylase in the bloodfrom days 1�4. The swelling of the parotid glandsdisappeared without special treatment, whereas recovery ofsalivary gland secretion was slower.
3. Lung reactions
61. Lung reactions were observed in seven patientssuffering from third- and fourth-degree acute radiationsickness. Its characteristic signs were a rapidly intensifyingdyspnoea together with respiratory insufficiencyprogressing over a period of two to three days culminatingin death. Autopsies revealed large, blue lungs withpronounced interstitial oedema, without destruction of themucous membranes of the trachea and bronchi. As a rule,interstitial pneumonitis developed several days beforedeath, generally in combination with extremely severelesions of the skin and the intestine. The times to deathwere 14�30 days after irradiation.

Appendix to Annex G: ACUTE RADIATION EFFECTS IN VICTIMS OF THE CHERNOBYL ACCIDENT 13
4. Causes of death
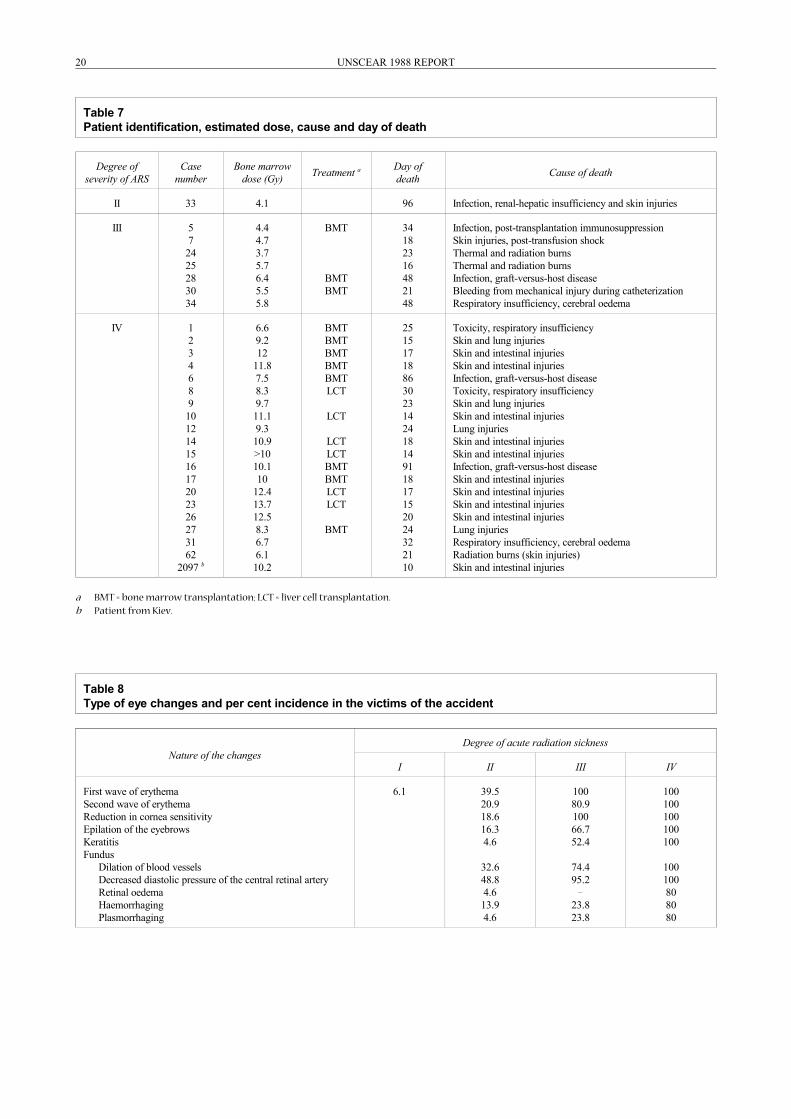
62. The frequency of non-haemopoietic injury increasedas a function of total dose (Figure VIII). Clinical observa-tions indicated the essential role of skin injuries in patho-logical processes prior to death. Among the patients thatdied, in two thirds of them there was extensive and severeradiation and thermal skin burns, which were consideredlife-threatening. In five cases skin injuries were the solecause of death, because there was neither radiation enteritisor irreversible myelodepression. Deaths were observedbetween 10 and 96 days after exposure. The clinical picturein all fatal cases was characterized as following a difficultcourse, because in every case two or three radiationsyndromes had occurred with complex toxicity, infectionand circulation disorders. A summary listing of patientidentification and causes of death is given in Table 7.
63. A detailed clinico-morphological analysis made itpossible to identify the predominance, within specified timeperiods, of particular lethal syndromes. Up to day 24, a totalof 19 patients (65%) died. In one half of these patients thecompeting causes of death were skin and intestinalreactions (cases 3, 4, 10, 14, 15, 17, 20, 23, 26, 2097; in allthe cases the gamma-radiation dose in the bone marrow wasestimated to be greater than 10 Gy). Four patients showedacute radiation injury in the lung (cases 2, 9, 12 and 27; thedoses were, respectively, 9.2, 9.7, 9.3 and 8.3 Gy), and, ofthese, two (cases 2 and 9) suffered also severe injuries tothe skin. Two patients died of combined thermo-radiationburns (cases 24 and 25; the gamma-radiation doses in thebone marrow were estimated to be 3.7 and 5.7 Gy,respectively, in combination with internal irradiation doses.Within this time-frame, one patient (case 62, dose about6 Gy) died almost exclusively from severe radiation bumsat a time when haemopoiesis had begun to be restored.Three cases (cases 17, 26, 62) had involvement ofmycobacterial sepsis. One patient (case 30, dose about5.5 Gy) died of bleeding caused by mechanical injury to thesubclavicular vein during catheterization, and another (case7, dose about 4.7 Gy), suffering from severe radiationinjury to the skin, died of post-transfusion shock.Characteristics of the deaths on days 11�24 were markedcirculatory problems during the terminal period. This wasshown by the relatively high frequency of signs indicatingcerebral oedema and focal haemorrhaging into the brain andspinal cord.
64. Six patients died during the period from days 25�48.All six cases were characterized by extremely severecomplications of a toxic or infectious nature. Two patients(cases 31 and 34) involved subtotal skin injuries (bonemarrow doses about 6.7 and 5.8 Gy, respectively, withdeath occurring on days 32 and 48, respectively), coupledwith practically restored haemopoiesis. The immediatecause of death in these cases was severe respiratoryinsufficiency and cerebral oedema. In one patient (case 28,dose about 6.4 Gy; death on day 48) the cause of death wassevere, graft-versus-host disease and fungal and viralinfections. One additional patient (case 5, dose about
4.4 Gy) died on day 34 of severe pulmonary and renalinsufficiency, caused, most likely, by the transplantation ofHLA-non-identical bone marrow and by post-transplantimmunosuppression using cyclosporin and methotrexate.Two patients (cases 1 and 8, doses about 6.6 and 8.3 Gy)died on days 25 and 30, respectively, with symptoms ofsevere toxicity and pulmonary insufficiency. In nearly allsix cases there were marked circulatory disorders in thelungs, intestines, brain and myocardium.
65. At a relatively late stage, days 86�96, three patientsdied. One patient (case 6, dose about 7.5 Gy) died on day86 of graft-versus-host disease complicated by cytomegalo-virus (CMV) infection. Cytomegalovirus infection was alsothe cause of death for another patient (case 16, dose about10.1 Gy) on day 91. A female patient (case 33, dose about4.1 Gy) died on day 96 displaying marked disruptions ofcerebral blood circulation against a background of renal-hepatic insufficiency and foci of mycococcal infection(pneumonia). This patient suffered also skin injuries frombeta-radiation which extended over one third of her skinsurface and underwent a severe recurrent wave of erythemawith oedema of the subcutaneous tissue.
5. Eye damage
66. Eye injuries were characterized by the early andsubsequent involvement of all eye tissues in thepathological process (Table 8). In this group of patients,damage to the skin and eyelid conjunctiva was caused, to aconsiderable degree, by beta-radiation.
67. At doses not exceeding 1 Gy there were no visiblealterations in the structure of the eyes. In the case ofpatients suffering from first-degree acute radiation sickness,changes were noted only in the front segment of the eye:there was in individual cases a slight erythema in eyelidskin during the first two to four days and an intensificationof the vascular pattern in the lid and conjunctiva of theeyeball. In 40% and 100% of the patients suffering fromsecond- and third-degree acute radiation sickness,respectively, the eyelid skin showed a first wave oferythema within 6�12 hours of irradiation, and within 2�3weeks there was a second wave. These cutaneousalterations disappeared without trace, leavinghyperpigmentation and scaling. In all patients sufferingfrom fourth-degree acute radiation sickness, the times to theappearance of the first and second wave of erythema were1�2 hours and 8�10 days, respectively.
68. Microscopy of the bulbar conjunctiva revealed anumber of alterations in the microcirculation: there was adilation of the venules and capillaries (more rarely thearterioles), and an increase in the number of functioningvessels coupled with a reduced blood flow.
69. Two patients suffering from combined radiation andthermal second-degree lesions on the lid skin andconjunctiva experienced ulcerations on the skin around theeye that did not re-epithelialize for a long time. Epilation of

UNSCEAR 1988 REPORT14
the eyebrows was noted at days 15�17 in 16% of thepersons with second-degree acute radiation sickness, and in67% and 100% of those with third-and fourth-degree acuteradiation sickness, respectively. The epilation was partialand transient. Hair growth on the head was fully restored.All patients retained their eyelashes.
70. Corneal damage was manifested in an early reductionin corneal sensitivity coinciding with the first wave oferythema, although first-degree patients did not show suchan effect. At later times (days 35�55), superficial radiation-induced keratitis was observed in patients suffering fromsecond-, third- and fourth-degree radiation sickness in 5%,52%, and 100% of the cases, respectively. Also noted werefocal defects on the superficial epithelium of the cornea;these defects, which often merged, stained with fluorescein.The radiation keratitis regressed over a period of 1�1.5months, leaving no opacification of the cornea.
71. Signs of disturbances in the haemodynamics of theretina were related to the dose and the degree of severity ofradiation sickness. From a few days after irradiation, areduction was observed in the level of diastolic pressure inthe central retinal artery, followed later by signs ofhypotonic angiopathy of the retina. Coinciding in time withthe peak of the sickness, other injuries appeared, e.g.,retinal oedema along the vessels and increased permeabilityof the retinal vessels (plasma discharge andhaemorrhaging). The low diastolic pressure in the centralretinal artery persisted over the entire acute phase.
72. In one severely ill patient (case 29, dose about8.7 Gy) with fourth-degree acute radiation sickness, whosurvived the acute phase, the symptoms of angioretinopathywith haemorrhaging and plasma discharge recurred within4.5 months, accompanied by a persistently low diastolicpressure in the central retinal artery (up to 5�10 mm Hg).
73. In the acute period, the treatment consisted in thetopical application of ointments to the scaling surface of theeyelid skin and the instillation of 20% albucid, sophradex andvitamin solutions as eye drops into the conjunctival cavity.
74. Within observation periods of up to one year. noobvious radiation-induced alterations of the lens were noted.
6. Treatment of radiation burns and other injuries
75. The treatment of radiation burns and other non-bone-marrow syndromes and their complications posed complexand multifaceted problems [J1]. From day 2 through day 8,15 haemosorption sessions (purification using activatedcharcoal) were conducted for 13 patients suffering from themost severe skin lesions. Three patients who had beenexposed to a total dose range of 2.0�4.6 Gy survived; theyunderwent haemosorption on a single occasion at days 5�8,i.e., considerably later than the time at which this mighthave affected the treatment of the bone marrow syndrome.This method of treatment did not change the outcome of theillness by modifying the haemocytopenia.
76. During the haemosorption process, and particularlytowards the end of the session, many patients experienceda short-term improvement (lasting from a few hours to asingle day), a reduction or disappearance of the pain in theextremities, and also a decrease of the oedema in theirtissues. In this connection, contributory effects from themedication accompanying the procedure cannot be totallyexcluded.
77. A more widely used technique to combat thedevelopment of renal-hepatic insufficiency and fatalencephalopathic coma was plasmapheresis. Lesionsinduced by beta-irradiation over 30�40% and more of thebody surface served as an indication for the application ofthis procedure. Plasmapheresis sessions were conducted for17 patients from days 18�37. For a number of patients,daily sessions were conducted, up to six times.
78. The positive effect of repeated plasmapheresis wasshown by a reduction of bilirubinemia and transaminasemiaand a lowering of the nitrate level in patients suffering fromrenal-hepatic insufficiency caused by skin burns. Onoccasion, the plasmapheresis sessions were accompanied byreactions of minor severity such as chills and fever; therewere no fatal complications. Another method used to treattoxicosis due to skin injuries was the injection of 1,000 ml offreshly-frozen plasma, accompanied by round-the-clockadministration of heparin (1,000 active units/hour) with aliquid load (2�6 litres/day) and forced diuresis adequate tothe intake volume. A precondition for this treatment was thepresumption of disseminated intravascular clotting (DIC)syndrome (no typical anomalies in respect of coagulationwere present) as a possible cause of encephalopathy andrenal-hepatic syndrome. In its most strictly applied form, theheparin treatment method was used with two patients over aperiod of 7�15 days. The impression was that these patientssurvived longer than did patients whose condition wassimilar in terms of severity and extent of their burns. Theirrenal-hepatic insufficiency was less pronounced; however, adeath due to encephalopathic coma was not averted.
79. The topical treatment of the burns required theinvolvement of a group of surgeons and nurses. A broadrange of preparations and agents having an anti-inflammatory, bacteriostatic and regeneration-stimulatingeffect was used. Good results were achieved with lioxanolaerosol, an anti-burn ointment based on hydrocortisonewith locally acting antibiotics, as well as BALIZ-2 solutionand collagenous coatings. In each individual case thetreatment varied in accordance with the stage of the lesions.Experience gained in the use of bactericidal fabric, both asa dressing material and for supplementary bedding, forpatients with extensive burns deserves a particularlyfavourable comment in this connection [Z1].
80. Treatment of pain, as is typical of radiation injuries,was rather ineffective. At present, there are clearly nosuitably effective local anaesthetics.

Appendix to Annex G: ACUTE RADIATION EFFECTS IN VICTIMS OF THE CHERNOBYL ACCIDENT 15
81. Inpatients suffering from severe radiation-inducedinflammation of the oral mucosa, and enteritis, totalparenteral nutrition had a positive effect; this was based onalvesin hydrolysate or an aminoacid mixture, aminone anda 40% glucose solution as the energy material. Thetreatment was carried out according to the principles andrules described by Dudrick et al. [D1]. This method wastested over a number of years with good results in patientsreceiving whole-body therapeutic gamma-irradiation at adose level of 10 Gy for allogeneic bone marrowtransplantation. The danger, which has possibly not beenfully evaluated, is the probability that certain severelyinjured, comatose patients may enter a state ofhyperosmolarity. Data on plasma osmolarity that wouldappear to be necessary in a programme of total parenteralnutrition were not provided for all patients.
82. For the majority of patients suffering from first-andsecond-degree bone marrow syndrome, the period ofclinical convalescence was completed by the third or fourthmonth. A longer period of treatment was required bypersons suffering from severe radiation burns and thesequelae of third- and fourth-degree bone marrowsyndrome. At the present time, the bulk of the patients haveresumed work with the exclusion of any contact withradiation sources.
83. Over the period from the fourth month to one year afterthe accident, the specialized treatment centre wasperiodically visited by patients with skin lesions (dystrophicand ulcerated areas and also oedema of the subcutaneoustissues, mainly on the knees and feet). These patients arebeing treated with agents designed to improve local bloodcirculation and tissue trophism. Five patients with deep andextensive ulcers on their arms and other areas of the bodyunderwent repeated plastic surgery, and a number of themwill require more extended treatment.
84. Immunological examination data, acquired 0.5�1.5years after the accident, have shown that in the peripheralblood of the patient groups with a history of acute radiationsickness of the second, third and fourth degrees a decline was
observed in the number of T-lymphocytes with helperactivity along with an increase in the number ofT-lymphocytes with suppressor activity. This led to aconsiderable reduction in the normal ratio between theseimmunoregulatory lymphocyte sub-populations. At the sametime, there was no reduction in the general lymphocyte levelor in their T- and B-sub-populations. As an average for thegroups, the level of class A, M and G immunoglobulins in thepatients' blood serum corresponded to the physiologicalnorm. Similar changes were not observed in the case ofpatients with a history of acute radiation sickness of the firstdegree. During this time they experienced no severe or life-threatening infections. In a number of cases an effort wasmade at immuno-corrective therapy using T- and B-activin.
85. Within these same patient groups, an estimate of thenumber of respiratory illnesses over the same period of timewas conducted retrospectively. It was found that theincidence of illness in the group of 19 patients with a historyof first-degree acute radiation sickness did not differ from theincidence of illness for the group of persons for whom noacute radiation sickness diagnosis had been established, andthat it averaged 0.3 cases per person per year. During thesame period, this indicator approached 1 for 22 patients whohad experienced second-degree acute radiation sickness, and3 for 8 persons with a history of third- to fourth-degree acuteradiation sickness.
86. This comparison underlines the importance of theimmune system in maintaining anti-infection resistance inradiation convalescents and raises the question as to theusefulness of conducting supportive immunomodulatingtherapy courses, long after the incident, for persons who haveundergone severe forms of radiation sickness.
87. The experience of the specialized treatment centres inMoscow and Kiev in the organization of medical care ofpersons exposed in this nuclear reactor accident has beendescribed [N1]. For the survivors, a plan of scheduled follow-up observation is in effect, and decisions as how best toarrange their living and working conditions are being taken.
CONCLUSIONS
88. The analytical data presented in this Appendix andderived from clinical observations of the victims of theaccident at the Chernobyl nuclear power plant are inagreement with the data in Annex G.
89. However, the fact that such a large group of 115patients, who had all received uniform whole-body irradia-tion, was treated simultaneously for acute radiation sicknessof varying degrees of severity, represents a unique event thatmakes it possible to clarify numerous aspects of early effectsin man. A complicating factor was the presence of severe andextensive beta-radiation skin injuries in 58 patients which
aggravated the course of the sickness in 19 of the 28 whodied. Two more patients died during the first days as a resultof severe combined injuries (trauma plus thermal burns plusirradiation).
90. The analysis provides a basis for describing theprincipal clinical syndrome, the bone marrow, syndrome,with various degrees of severity in all 115 patients. In thecase of some of them the bone marrow syndrome wascombined with intestinal and oropharyngeal injuries andradiation damage to the skin, the foreward segment of the eye(keratitis), and the lungs.

UNSCEAR 1988 REPORT16
91. The treatment provided was in accordance withinternational practice and proved highly effective for thepatient group exposed to doses of 2�4 Gy and for two thirdsof the patients who received doses of 4�6 Gy. In the group ofpatients receiving 6�16 Gy, two patients who received dosesof 8�9 Gy survived past 60 days.
92. The average bone marrow dose and the prognosisregarding the further course of the illness were determined onthe basis of biological criteria. During the early period, mostinformation was obtained from the karyological analyses, thelymphocyte counts and the primary reaction periods; later,
from the granulocyte counts. The remaining indications wereof an auxiliary nature. In three cases, the dose valuecoincided with the electron spin resonance study of dentalenamel after death.
93. There is a need for further analysis of the time courseof the early effects for a more accurate understanding of thenature of lung and neurological injuries, and for moredetailed data on the relevance of biological dose indicatorsand the reasons for disparities between them. It is hoped thatthese data will be of use in the preparedness to respond in theevent of an accident of a similar type in the provision ofmedical treatment.
Appendix to Annex G: ACUTE RADIATION EFFECTS IN VICTIMS OF THE CHERNOBYL ACCIDENT 17
a Doses accumulated until time of death.
a In addition to the patients who died of acute radiation sickness, one person died at the plant site and another within the first 12 hours followingthe accident, as a result of thermal burns, at the in-patient clinic in Pripyat where he had been given first aid.
Table 1Thyroid doses received by exposed persons
Range of thyroid doses (Sv) Number of persons
0�1.21.2�3.73.7�6.16.1�8.6
8.6�11.011.0�13.413.4�15.915.9�18.318.3�20.820.8�23.2
1731844220201
Table 2Doses of victims receiving higher internal exposures
Case number Thyroid dose a
(Gy)Lung dose a
(Gy)
Whole-body dose (Sv)
Internal External
24251734
26
3061
0.31.20.5
2.52.00.40.30.40.3
2.01.00.20.20.10.1
1.74.7
10.012.011.012.0
Table 3Distribution of patients with acute radiation sickness treated at the specialized treatment centre
Degree of severity Number of patients Bone marrow dose range(Gy) Number of deaths Time to death (days)
I 31 0.8�2.1 � �
II 43 2.2�4.1 1 96
III 21 4.2�6.4 7 16, 18, 21, 23, 34, 48, 48
IV 20 6.1�16 20 10, 14, 14, 15, 15, 17, 17, 18, 18, 18,20, 21, 23, 24, 24, 25, 30, 32, 86, 91
115 28 a

UNSCEAR 1988 REPORT18
a The diagnostic signs are used to determine the diagnostic scores, which are then added together. A sum of +10 is the basis for a prognosis ofirreversible myelodepression; a sum of �10 for a prognosis of no irreversible myelodepression. If after the diagnostic coefficients of all theavailable signs have been added no positive value has been reached, the answer is indeterminate (the available information is insufficient for adifferential diagnosis, with an error probability of not more than ±10%).
Table 4Assessment of irreversible myelodepression according to diagnostic scores in cases of acute radiation sickness
Sign Units Amount Diagnostic score a
Time to the onset of vomiting hours 0�0.40.41�0.80.81�1.21.21�1.61.61�2.0
>2.01
+ 8+ 4+ 2�2�6�10
Lymphocyte count on the second day 109 l-1 0�0.20.21�0.40.41�0.60.61�0.8
>0.81
+ 6+ 2�2�8�15
Lymphocyte count on the third day 109 l-1 0�0.10.11�0.20.21�0.30.31�0.4
>0.41
+ 8+ 2�2�9�10
Lymphocyte count on the fourth day 109 l-1 0�0.10.11�0.20.21�0.30.31�0.70.71�0.80.81�0.9
+ 4+ 20�2�3�8
Lymphocyte count from day 4 to day 7 109 l-1 0�0.10.11�0.20.21�0.30.31�0.40.41�0.5
>0.51
+ 5+ 2�1�5�13�15
Average reticulocyte count from day 3 to day 5 109 l-1 0�8.00.1�10.0
10.1�14.014.1�18.018.1�20.0
+ 20�4�6�10
Minimum neutrophil count from day 6 to day 7 109 l-1 0�0.30.31�0.60.61�0.90.91�1.21.21�2.42.41�3.0
+ 12+ 50�3�6�8
Appendix to Annex G: ACUTE RADIATION EFFECTS IN VICTIMS OF THE CHERNOBYL ACCIDENT 19
a Skin and intestinal injuries.b Bone marrow rejection (graft-versus-host disease) plus infection.c Positive graft-versus-hosts disease post-mortem histology.
Table 5Survival or cause of death of patients receiving bone marrow transplantations and of patients in control group
Dose range(Gy)
Bone marrow transplant patients Control patients
Number ofpatients Deaths a Deaths b Number of
survivorsNumber of
patients Deaths a Number ofsurvivors
< 6.56.5�9
> 9
436
02 c
5
301
110
545
035
510
Total 13 7 4 2 14 8 6
Table 6Distribution of cases of radiation burns of different degree in the presence of acute bone marrow syndrome
Degree of severityof
bone marrow syndrome
Total numberof patients
Number of patients with radiation burns to body surface
0�10% 10�50% 50�100%
IIIIIIV
31432120
2231
19
1510
0139
Total 115 56
UNSCEAR 1988 REPORT20
a BMT = bone marrow transplantation; LCT = liver cell transplantation.b Patient from Kiev.
Table 7Patient identification, estimated dose, cause and day of death
Degree ofseverity of ARS
Casenumber
Bone marrowdose (Gy) Treatment a Day of
death Cause of death
II 33 4.1 96 Infection, renal-hepatic insufficiency and skin injuries
III 57
2425283034
4.44.73.75.76.45.55.8
BMT
BMTBMT
34182316482148
Infection, post-transplantation immunosuppressionSkin injuries, post-transfusion shockThermal and radiation burnsThermal and radiation burnsInfection, graft-versus-host diseaseBleeding from mechanical injury during catheterizationRespiratory insufficiency, cerebral oedema
IV 1234689
101214151617202326273162
2097 b
6.69.212
11.87.58.39.711.19.310.9>1010.110
12.413.712.58.36.76.110.2
BMTBMTBMTBMTBMTLCT
LCT
LCTLCTBMTBMTLCTLCT
BMT
2515171886302314241814911817152024322110
Toxicity, respiratory insufficiencySkin and lung injuriesSkin and intestinal injuriesSkin and intestinal injuriesInfection, graft-versus-host diseaseToxicity, respiratory insufficiencySkin and lung injuriesSkin and intestinal injuriesLung injuriesSkin and intestinal injuriesSkin and intestinal injuriesInfection, graft-versus-host diseaseSkin and intestinal injuriesSkin and intestinal injuriesSkin and intestinal injuriesSkin and intestinal injuriesLung injuriesRespiratory insufficiency, cerebral oedemaRadiation burns (skin injuries)Skin and intestinal injuries
Table 8Type of eye changes and per cent incidence in the victims of the accident
Nature of the changesDegree of acute radiation sickness
I II III IV
First wave of erythemaSecond wave of erythemaReduction in cornea sensitivityEpilation of the eyebrowsKeratitisFundus
Dilation of blood vesselsDecreased diastolic pressure of the central retinal arteryRetinal oedemaHaemorrhagingPlasmorrhaging
6.1 39.520.918.616.34.6
32.648.84.613.94.6
10080.910066.752.4
74.495.2�
23.823.8
100100100100100
100100808080

Appendix to Annex G: ACUTE RADIATION EFFECTS IN VICTIMS OF THE CHERNOBYL ACCIDENT 21
References
B1 Barabanova, A.V., A.Y. Baranov, A.K. Guskova et al. Acuteradiation effects in man. USSR State Committee on theUtilisation of Atomic Energy. USSR Ministry of Health,National Commission on Radiation Protection. Moscow-TSNII Atominform (1986).
B2 Baranov, A.Y. Dose estimates and the prediction of thedynamics of the peripheral-blood neutrophil count accordingto haematological indicators in human gamma-irradiation.Med. Radiologiya 26: 11-16 (1981).
C1 Cronkite, E.P., V.P. Bond and C.L. Dunham. Some effectsof ionising radiation on human beings: A report on theMarshallese and Americans exposed to radiation from falloutand a discussion of radiation injury in the human being.AEC-TID 5385 (1956).
D1 Dudrick, S.J. and R.L. Ruberg. Principles and practice ofparenteral nutrition. Gastroenterology 61: 901-910 (1971).
G1 Guskova, A.K. Current problems of radiation sicknessprophylaxis and treatment. Med. Radiologiya 9: 3-8 (1986).
G2 Guskova, A.K., N.M. Nadezhina, A.V. Barabanova et al.Acute radiation effects after Chernobyl nuclear power plantaccident: immediate outcomes of sickness and the results oftreatment. The Medical Aspects of the Chernobyl Accident.Kiev, 1988. (In press).
I1 International Atomic Energy Agency. Summary Report onthe Post-Accident Review Meeting on the ChernobylAccident. Safety Series No. 75-INSAG-1. Vienna, 1986.
I2 International Commission on Radiological Protection. Limitsfor intakes of radionuclides by workers. ICRP Publication30. Pergamon Press, Oxford, 1979.
J1 Jammet, H. et al. (eds.). Radiation damage to skin.Fundamental and practical aspects. Proceedings of aWorkshop held in Saclay, France, 1985. Br. J. Radiol. 19(Suppl.): (1986).
N1 Nadezhina, N.M. Experience of a specialized centre in theorganization of medical care of persons exposed during anuclear reactor accident. Br. J. Radiol. 60: 1169-1170(1987).
P1 Pyatkin, E.K. and A.E. Baranov. Biological dose indicationby means of the analysis of chromosome aberrations and cellcount in peripheral blood. Itogi nauki i tekhniki VINITI ANSSSR. Ser. “Radiatsionnaya biologiya” 3: 103-179 (1980).
P2 Pyatkin, E.K. and V.Y. Nugis. Dose-dependence ofchromosome aberration outcome in in vitro and in vivoirradiation of humans. Med. Radiologiya 9: 30-35 (1986).
T1 Tatsumi-Miyajima, I. and S. Okajima. ESR dosimetry usinghuman tooth enamel. p. 397-405 in: ESR Dating andDosimetry (IONICS). (M. Ikeya and J. Miki, eds.). Tokyo,1985.
Z1 Zubarev, R.P., E.M. Sergeyuk, V.N. Zagvozkin et al. Pre-operation prophylaxis of surgical infection. Khirurgiya 5:131 (1985).





























