Embed Size (px)
Citation preview

University of Missouri Antimicrobial Stewardship Program : Patient Safety and NPSG CompliancePerformance Improvement Leadership Develop ProgramUniversity of Missouri – ColumbiaFebruary 19, 2010

Team Members
•Joe Cameron, Pharm.D., BCPS•Gordon Christensen, MD•Ed Ege, Pharm.D.•Stephanie Lumley-Hemme, RPh•Jennifer Meyer, Pharm.D., BCPS•Stevan Whitt, MD

Focus Area• With the arrival of the Centers for Medicare &
Medicaid's no-pay rules, The Joint Commission's National Patient Safety Goals, and the ever-growing emphasis on quality improvement of patient care, prevention has become the standard of care.
• Participation in multiple quality improvement, automated data surveillance, and antimicrobial stewardship programs have garnered successes for hospitals in terms of improving systems, and in turn care and cost.

AIM Statement• University of Missouri Hospital aims to implement
a process for monitoring and an intervention protocol intended to standardize the use of evidence based antibiotic regimens in the adult surgical intensive care unit.
• The process starts with a list of new antibiotic orders and a daily culture and sensitivity report from the lab.
• The process ends with conclusion of antibiotic therapy

AIM Statement
•Our goal is to standardize empiric antibiotic therapy
•Our secondary outcomes include: improving patient outcomes, decreasing duration of antibiotic therapy, containing antibiotic costs, and decreasing antibiotic resistance and related adverse reactions compared to current practice.

Institutional Strategic Goals• National Patient Safety Goal 7 : Reduce the risk
of health care associated infections• New standards for 2009
▫NPSG.07.03.01: Implement evidence-based practices to prevent health care associated infections due to multiple drug-resistant organisms in acute care hospitals.
▫NPSG.07.04.01: Implement best practices or evidence-based guidelines to prevent central line-associated bloodstream infections.
▫NPSG.07.05.01: Implement best practices for preventing surgical site infections.

Institutional Strategic Goals
•Diagnosis Driven Therapy
•Uniformity in Prescribing Practices
•Cost Avoidance
•Education

Project TimelineECOMS
Initial Approval
ID Acceptance
Data analysis and
modification
SICU Intial Acceptance
Presentation and
Implementation of Program August
2009
New Process
Development
Lab Report Order Sheet
Creation with ID
Current Process
Evaluation
ECOMS Approval to
move forward
IV to PO Conversion
Policy
Preliminary Data
Discussion with
PowerChart Documentatio
n
Process Modification and Initiation
Feb 2010
Jan 2010
Dec 2009
Nov 2009
Oct 2009
Sept 2009

Current Process
Continued on Next
Slide

Current Process

Fishbone Diagram

UpstreamStakeholder
s
Point of Change
Stakeholders
DownstreamStakeholder
s
• Patients
• Administration
• Pharmacy
• ICU Physicians• Attendings• Residents
• Infectious Disease
• Pathology
• IT Dept.
• Pharmacy
• Infection Control • Units throughout hospital
• Pharmacy
Stakeholders

Interventions ConsideredStrategy 1 Strategy 2 & 3
• Active Intervention and Feedback
• Location Based• Patient Based• Organism Based
• Prior-authorization▫ ID Physician or
Pharmacist with authority
• Restricted Formulary▫ Partially implemented, no
authority in Pharmacy
• Education▫ Driven by Attending
Physicians
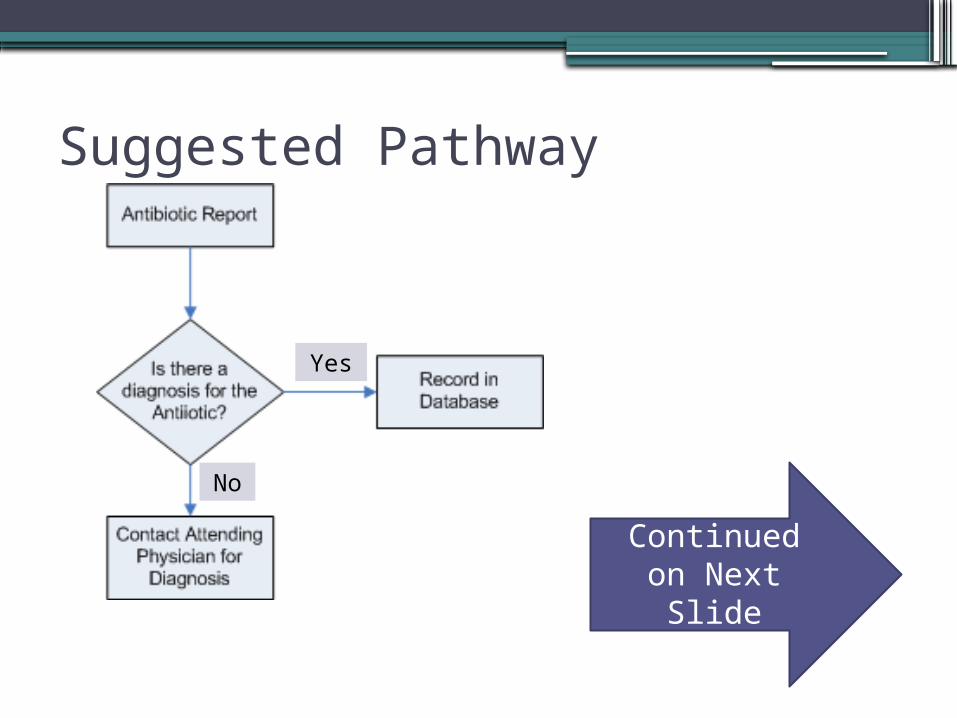
Suggested Pathway
Continued on Next
Slide
Yes
No

Suggested Pathway
Continued on Next
SlideNo
NoYes
Yes

Suggested Pathway
No
No
Yes
Yes

Key Driver Diagram

Order Sheets
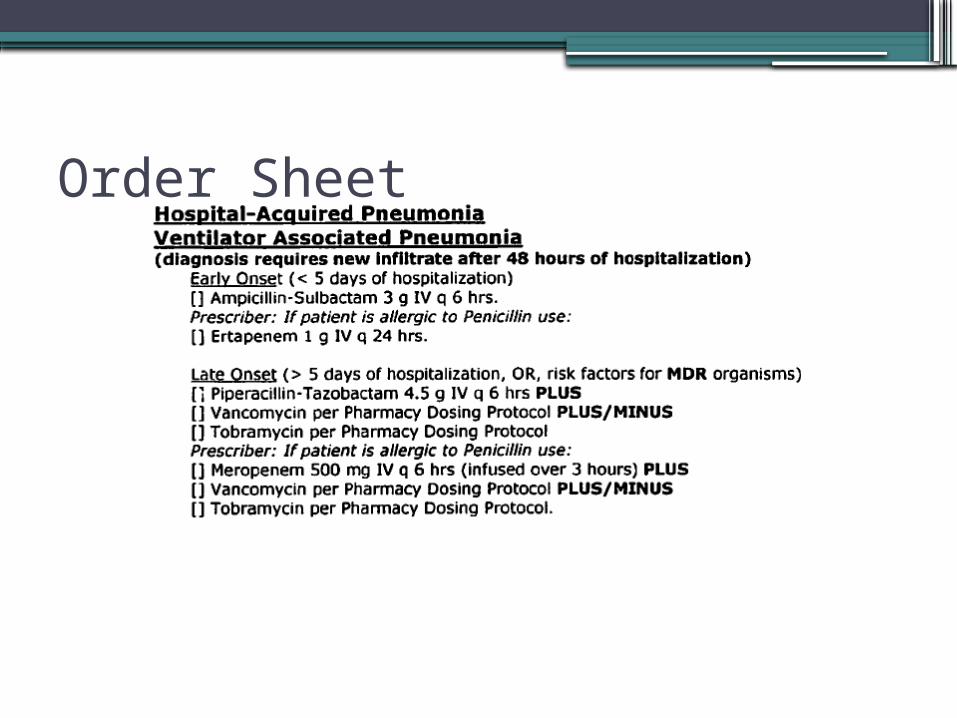
Order Sheet

Microbiology Reports

Microbiology Reports

Measurements
•Diagnosis Stated / Use of Preprinted Order Set
>75%
•De-escalation>75%
•IV to PO Conversion>75%

Baseline Data (2 Weeks)• Diagnosis Stated
▫ Zero (0%)
• Patients in SICU▫ 21 Patients
• Antibiotics Prescribed▫ 37 Antibiotics
• One Time Dose (Pre-op)▫ 4 Antibiotics
• De-escalation▫ 2 Accomplished (40%)▫ 3 Missed
• IV to PO Conversion▫ None (0%)
Process and Outcomes Indicators•Outcome Indicators
▫Increased knowledge of appropriate therapy for common infectious diagnoses throughout the institution. Bacteremia, Pneumonia, and Intra-abdominal
Infections▫Compliance with JCAHO NPSG 7
•Process Indicators▫De-escalation of therapy when appropriate▫IV to PO Conversion

Anticipated Return on Investment / Benefits Realized•Increased resident understanding of
appropriate empiric evidence based therapy and de-escalation
•Consistent management of patient specific disease states
•Decreased development of multi-drug resistant organisms
•Decreased medication expenditure

Lessons Learned
•Health care team acceptance
•Analysis of current practice
•Prediction of program implementation
•Process improvement application
Next Steps
•Encompass all intensive care units•Education of Pharmacists, Nurses, and
Physicians• Increase number of disease state protocols• Increase roll out to all of institution•Successful reduction in multi-drug
resistant organisms•Decreased length of antibiotic therapy and
potentially patient stay

Questions?Joe CameronEd EgeStephanie Lumley-HemmeJennifer Meyer

Thank You!








![[List University Name] Quality Assurance Program ... Assurance Foms/University... · [List University Name] Quality Assurance Program Description Document ... Quality Assurance Program](https://img.dokumen.tips/doc/110x75/5ab8c3d37f8b9aa6018d08ac/list-university-name-quality-assurance-program-assurance-fomsuniversitylist.jpg)




















