Embed Size (px)
Citation preview
University College Hospital
Laparoscopic colorectal surgeryGastrointestinal Services Division

2
Colon

If you would like a large print, audio or translated version of this document contact us on 0845 155 5000 Ext 77059. We will do our best to meet your needs.
33
ContentsWhat is Laparoscopic colorectal surgery? 5How can Laparoscopic colorectal surgery help? 6What are the possible complications of the procedure? 6What alternatives are available? 6How should I prepare? 6Asking for your consent 7What happens during the procedure? 7What should I expect after the procedure? 7Laparoscopic Surgery explained 9Where can I get more information? 10Contact details 10How to fi nd us 11

4

5
What is Laparoscopic colorectal surgery?Traditional abdominal surgery involves a large cut in the abdomen. Laparoscopic colorectal surgery (or keyhole surgery) involves a number of smaller cuts in the abdominal wall. The idea is that the surgery will be less painful and that as a consequence you will recover quicker. In principle, the same operation is being performed in open or laparoscopic abdominal (keyhole) surgery. All operations are performed under general anaesthesia (pain relievers).
What bowel conditions can be performed as laparoscopic operations?• Bowel cancer
• Diverticular disease (little pockets or outpouchings in the lining of the bowel)
• Crohn’s disease and ulcerative colitis
• Removal of large colonic polyps
• Appendicitis
• Rectal prolapse (where the lower end of the bowel has fallen through the anus)
Can all bowel operations be performed laparoscopically?No. It will be the decision of your consultant surgeon as to whether your operation may be performed laparoscopically. It may not be technically possible due to a number of factors including scarring from previous surgery. On a few occasions, an operation may be started laparoscopically and subsequently converted to an open operation due to technical factors such as bleeding or inability to clearly see and recognise the area to be operated on.

6
How can Laparoscopic colorectal surgery help? • Shorter hospital stay than traditional surgery
• Faster recovery to normal activities or work
• Less pain and problems with incisions
What are the possible complications of the procedure? • Leakage of the bowel join which may require re-operation with the
formation of a stoma (bowel end brought out to skin and a bag applied to skin to collect bowel contents)
• Wound infection
• Abdominal abscess
Problems that are rare, but serious• Bleeding requiring transfusion or re-operation
What alternatives are available?The same operation may be performed as an open procedure i.e. large incision.
How should I prepare?This will depend on the individual Consultant Surgeon preference. Usually there is no need for bowel preparation for patients having the right side of their large bowel removed. Patients having the left side of the large bowel removed or the very lower part of the bowel (rectum) removed may have either enemas (liquid solution put into the lower bowel to cleanse it) on the evening and morning prior to surgery, or a full bowel preparation.

7
Asking for your consentIf you decide to go ahead with treatment, by law we must ask for your consent and will ask you to sign a consent form. This confi rms that you agree to have the procedure and understand what it involves. Staff will explain all the risks, benefi ts and alternatives before they ask you to sign a consent form. If you are unsure about any aspect of your proposed treatment, please don’t hesitate to speak with a senior member of staff again.
What happens during the procedure?A small cut is placed in the abdomen (10mm to 12mm) to allow carbon dioxide gas to distend (expand) the abdomen. This initial cut is usually placed at the umbilicus (belly-button) but it may be placed on the right hand side of the abdomen depending on the proposed operation. Next a fi ne-optic telescope (laparoscope) is placed through this incision. The image of the abdomen is displayed on video monitors in the operating room. A number of smaller incisions are then made in the abdominal wall and through these incisions the operation is performed with laparoscopic instruments. One of these incision sites may be extended in size to remove the specimen and join the ends of the bowel together if appropriate.
What should I expect after the procedure?It would be normal practice to place a catheter (tube) in the bladder at the time of surgery. An abdominal drain may be placed at the end of the operation. Depending on the exact operation, a stoma bag may be present. All wounds will usually be closed with an absorbable suture (stitch) which does not need to be removed and covered with a sterile dressing.
How long will I be in hospital?This will depend on the exact operation, which will be discussed with your consultant.
8
How will my pain be controlled?You will either have an epidural (which numbs the pain nerves at the level of the spine and gives a slow continuous infusion of pain relief) or a ‘patient controlled analgesia’ (PCA) pump. With the PCA, you press a control button to give you a small amount of morphine at times that you feel pain. There are a number of safety measures employed which will prevent you from overdosing on the pain medication.
When may I start eating food again?We have an active ‘enhanced recovery programme’ in this hospital, which looks at all aspects of your recovery in an effort to streamline and speed-up your recovery. We will make every effort to encourage you to eat and drink at an early stage subject to satisfactory clinical progress. The details of this programme are discussed with the patient prior to the operation.
After discharge from the hospital, what factors should cause me concern and require urgent medical attention/advice?• High fevers, sweating and chills
• Severe abdominal pain or increasing abdominal pain not relieved by painkillers
• Persistent nausea and vomiting
• Pain, redness, swelling or discharge from your abdominal wounds
Will I have a follow-up appointment?Your follow-up appointment will depend on the nature of your operation. A routine appointment is usually made six to eight weeks after your operation.

9
Laparoscopic surgery explainedLaparoscopic Right HemicolectomyThis involves removing the right side of the large bowel and a small part of the distal (lower) small bowel and subsequently joining the small bowel onto the transverse colon.
Laparoscopic Left HemicolectomyThis involves removing the left side of the colon (descending colon and sigmoid colon) and joining the transverse colon onto the rectum
Laparoscopic Sigmoid ColectomyThis involves removing the sigmoid colon and joining the descending colon onto the rectum
Laparoscopic Anterior ResectionThis involves removal of most of the rectum and joining of the descending colon onto the lower rectum or anus. This operation may necessitate the formation of a defunctioning ileostomy (stoma bag) upstream from the surgery.
Laparoscopic Hartmann’s procedureThis involves removal of the sigmoid and some of the rectum and the formation of a colostomy (stoma bag), usually on the left side of the lower abdominal wall. The distal part of the bowel is closed off as a rectal stump.
Laparoscopic Defunctioning Sigmoid ColostomyThis involves bringing the sigmoid colon up to the skin, usually on the left side of the lower abdominal wall, and opening the bowel to make a stoma. The bowel contents will then mainly collect in the stoma bag and not pass down into the lower rectum and anus.
Laparoscopic Defunctioning IleostomyThis involves bringing a loop of distal small bowel out to the skin on the right side of the lower abdomen to make a stoma. The small bowel contents will then collect in the bag and not pass into the colon.

10
Laparoscopic RectopexyThis involves mobilising the rectum from its surrounding structures and pulling it up and stitching it to the tissues overlying the sacrum (bone of the lower spine).
Laparoscopic AppendectomyThis involves removing the appendix by detaching it from the caecum.
Where can I get more information?Website: www.cancer.gov
Contact detailsPA to Mr Cohen / Mr Windsor: Telephone: 0845 155 5000 Ext: 77059
Fax: 020 3447 9217
PA to Mr ObichereTelephone: 020 3447 7059Fax: 020 3447 9217
Website: www.uclh.nhs.uk
Colorectal PA: Maleika Pitterson/Charlotte O’ConnellTelephone: 0203 447 7059
Surgical Admissions Enquires: Gareth DaviesTelephone: 0203 447 5490Switchboard: 0845 155 5000
In an emergency please contact A&E or your GP
11
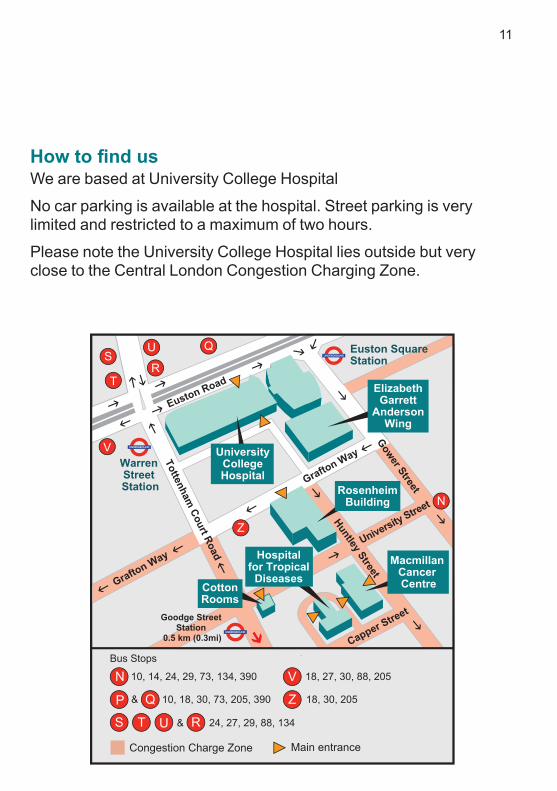
How to fi nd us We are based at University College Hospital
No car parking is available at the hospital. Street parking is very limited and restricted to a maximum of two hours.
Please note the University College Hospital lies outside but very close to the Central London Congestion Charging Zone.

Author: Mr James Crosbie, Consultant Colorectal Surgeon
First published: May 2010Last review date: March 2014Next review date: March 2016Leafl et code: UCLH/S&C/GI/LAPCOLORECTAL/1© University College London Hospitals NHS Foundation TrustCreated by Medical Illustration RNTNEH 020 3456 5103 Unique Code: 29331












![LAPAROSCOPIC SURGERY FOR COLONIC CANCERincluding surgery for colorectal malignancies, has been demonstrated [1-7]. Currently, indications for laparoscopic surgery are continuing to](https://img.dokumen.tips/doc/110x75/5f088a2f7e708231d4228374/laparoscopic-surgery-for-colonic-cancer-including-surgery-for-colorectal-malignancies.jpg)


![New approaches in laparoscopic surgery for colorectal ... · and totally laparoscopic low anterior resection[19]. ... specimen extraction for sigmoid diverticulitis, whereas all peritoneal](https://img.dokumen.tips/doc/110x75/5abf1cd37f8b9a5d718ddb4a/new-approaches-in-laparoscopic-surgery-for-colorectal-totally-laparoscopic-low.jpg)













