Embed Size (px)
Citation preview
2018 Prescription Drug List
UnitedHealthcare & Affiliated Companies
1
Table of Contents
2018 Prescription Drug List . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-5
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Prescription Drug List Medication Overview . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Tier Designations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Over-the-Counter and Therapeutically Equivalent Medications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
Key to Symbols . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
Generic Medication Policy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
Specialty Medications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
Medications Requiring Prior Authorization and Other Pharmacy Programs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
How to Obtain Authorization . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
Chapters
Anti-Infectives . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Antineoplastic & Immunosuppressant Drugs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
Autonomic & CNS Drugs, Neurology & Psych . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Cardiovascular, Hypertension & Lipids . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
Dermatologicals/Topical Therapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
Ear, Nose & Throat Medications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
Endocrine/Diabetes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
Gastroenterology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
Immunology, Vaccines & Biotechnology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35
Musculoskeletal & Inflammatory . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36
Obstetrics & Gynecology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 38
Ophthalmology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42
Respiratory, Allergy, Cough & Cold . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44
Urologicals . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47
Vitamins, Hematinics & Electrolytes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 48
Diagnostics & Miscellaneous Agents . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 49
Index . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50
April 2018

3
IntroductionThe UnitedHealthcare Prescription Drug List (PDL)1 provides a list of medications in various therapeutic classes for use in meeting the prescription medication needs of your patients who are our members . This list is intended for use with UnitedHealthcare health plans and affiliated companies’ pharmacy benefit plan designs . The PDL applies only to prescription medications dispensed to outpatients and does not include inpatient medications or medications obtained or administered in a physician’s office . The PDL does not define benefit coverage . Benefit coverage is determined by the member’s pharmacy benefit plan .2 This means that there may be medications listed on the PDL that are not covered under a particular member’s pharmacy benefit plan .
You may also access PDL information by visiting our website at UHCprovider.com .
Prescription Drug List Medication OverviewTier decisions are made by our PDL Management Committee based on clinical, economic, and other factors . The PDL Management Committee is comprised of senior UnitedHealth Group physician and business leaders . The UnitedHealthcare Pharmacy & Therapeutics (P&T) Committee, comprised of physicians and pharmacists, reviews new and existing medications and provides clinical guidance to the PDL Management Committee . Guidance is based on similarities and differences compared with other medications that treat the same disease or condition .
The tier placement of a medication on the PDL may change . While medications change tiers infrequently, such changes generally occur two times per calendar year . Additionally, when a brand-name medication becomes available as a generic, the tier status of the brand-name medication and its corresponding generic will be evaluated . When a medication changes tiers, your patient may be required to pay more or less for that medication . These changes may occur without prior notice to you or your patient . However, you may visit our website at UHCprovider.com or use the PreCheck MyScript app for the most up-to-date information for a particular medication . Your patient can also find the most up-to-date tier status and cost* information for a particular medication by visiting our member website at myuhc.com® and/or calling the toll-free member phone number located on his or her health plan ID card .
Tier DesignationsPrescription medications are categorized within three tiers on the PDL .3 Each tier is assigned a cost,* which is determined by the member’s pharmacy benefit plan . You may refer to the PDL as a guide to select the most appropriate medication with the lowest member cost for your patients .
Tier 1 Tier 1 medications are your patient’s lowest-cost option . Members can maximize their cost savings when you prescribe Tier 1 medications, if you decide they are appropriate for your patient’s treatment .
Tier 2 Tier 2 medications are your patient’s midrange-cost option . Consider Tier 2 medications if no Tier 1 medication is appropriate to treat your patient’s condition .
Tier 3 Tier 3 medications are your patient’s highest-cost option . If your patient is currently taking a medication in Tier 3, you may want to determine if there is an appropriate alternative in Tier 1 or Tier 2 .
You and your patient make decisions about health care and medication treatments .
If the member has a “closed” pharmacy benefit (e .g . a two-tier pharmacy benefit plan that does not cover medications classified in Tier 3 of this PDL), medications in Tier 3 are generally not covered, except under certain processes consistent with applicable law .
Some members have a four-tier prescription plan, and these medications are noted as T4 throughout the document . Members with a four-tier prescription plan should refer to their enrollment materials, check the Medication Pricing / Coverage information on our member website or call the toll-free member phone number provided on their health plan ID card for more information about their benefit plan .
Not all medications are represented in this PDL . Only the most commonly prescribed medications are included .
2018 Prescription Drug List
* UnitedHealthcare operates a wide number of benefit programs and products, and some benefit programs may have alternative benefit designs . Physicians should always check the member’s specific benefit prior to prescribing medications .
Tier 1 Tier 2 Tier 3Your patient’s Your patient’s Your patient’slowest-cost midrange-cost highest-costmedications medications medications
4
Over-the-Counter and Therapeutically Equivalent MedicationsFor some conditions, you and your patient may decide that an over-the-counter (OTC) medication is the most appropriate treatment . According to UnitedHealthcare benefit design, OTC medications are defined as medications that do not require a prescription by federal or state law to be dispensed . In some instances, OTC medications are listed on the PDL for reference purposes only . OTC medications may cost less than the member’s out-of-pocket expense for prescription medications .
Therapeutically Equivalent means that medications can be expected to produce essentially the same efficacy or adverse event profile . Our benefit designs allow us to exclude a medication if determined to be Therapeutically Equivalent to another covered product or OTC option .
If the patient or physician requests a medication we have excluded based on determination of Therapeutic Equivalent, the patient may be required to pay the entire cost of the medication as it may not be covered under the member’s pharmacy benefit . Please refer to the member’s pharmacy benefit plan .
Keys To Symbols
Generic Medication Policy Many generic medications are included on the PDL in Tier 1; however generic medications can be placed into any tier of the PDL . When a generic medication does not offer significant financial savings, it may be placed in the same tier or a higher tier than the brand medication . Generic medications are noted in italic font .
Note that when a brand-name medication becomes available as a generic, that brand-name product may move to a higher tier or be excluded from coverage by the member’s plan . Members may be required to pay more for a prescription when a higher-tier brand-name product is dispensed . The member’s cost share is determined by the pharmacy benefit plan . When generic substitution conflicts with state regulations or restrictions, the pharmacist must obtain approval from the prescribing physician or other health care professional to substitute the generic equivalent .
Specialty MedicationsSome members may have coverage for self-administered injectable and oral specialty medications through their pharmacy benefit plan . You will find these medications included in the body of this document within the appropriate therapeutic categories . UnitedHealthcare has a specialty pharmacy program that requires most specialty medications to be obtained through a designated specialty pharmacy . These medications are noted by SP throughout the document . The specialty pharmacy program includes designated specialty pharmacies, each selected based on their clinical expertise for the targeted therapeutic classes, quality of services, and cost . Their pharmacists are trained to help educate patients for these specialty medications, which may help improve treatment adherence .
Participating members should be instructed to call the toll-free member number on their health plan ID card where a representative will answer questions about our program and then transfer them to a specialty pharmacy based on their particular specialty medication prescription .
Symbols
E May be excluded from coverageH May be part of health care reform preventive^H-PA May be part of health care reform preventive with prior authorization^ MC Multiple copayPA Prior authorization required**RS May be eligible for the Refill and Save ProgramSL Supply limitSP Specialty medicationST Step therapy+
T4 May be covered on Tier 4 in select benefits
^ Health Care Reform drug lists may vary by plan; your patient can find the most up-to-date Tier status and cost information for a particular medication by visiting myuhc .com and/or calling the toll-free member phone number on their health plan ID card .
** Depending on your patients’ benefit and/or medication, notification or medical necessity criteria will be applied to determine if covered under the pharmacy benefit .
+ For New Jersey fully insured members, this program is referred to as First Start .
* UnitedHealthcare operates a wide number of benefit programs and products, and some benefit programs may have alternative benefit designs . Physicians should always check the member’s specific benefit prior to prescribing medications .

5
Medications Requiring Prior Authorization and Other Pharmacy Programs Select medications may require prior authorization to be eligible for coverage under the member’s pharmacy benefit plan . Such medications are noted with a PA . Depending on your patients’ benefit and/or medication, a coverage review may apply to determine coverage under the pharmacy benefit . The pharmacy benefit may exclude coverage of medications for certain uses .
Clinical criteria for PA medications are available on our website at UHCprovider.com . The criteria reflect UnitedHealthcare’s P&T Committee decisions . For a member to receive benefit coverage for a medication requiring prior authorization, the physician or the physician’s designee must provide information to the prior authorization department .
Some benefit plans may include our Step Therapy+ program . Step Therapy offers a “stepwise” approach to therapy for certain high-cost medications and requires that a member first try a more cost-effective medication before another high-cost medication . Step Therapy medications are noted as ST .
Supply limits define the maximum supply of medication per copayment or period of time . Supply limits are based on several factors that may include FDA-approved dosing guidelines as defined in the product package insert, medical literature, guidelines, or supportive data . Supply limit medications are noted as SL .
The Refill and Save Program encourages members to adhere to their treatment regimens by rewarding them with a discounted copayment/coinsurance for refilling their prescription within the defined time period . Eligible medications are noted as RS .
How to Obtain AuthorizationUse the PreCheck MyScript app on Link . By using the PreCheck MyScript app, you can now run a pharmacy trial claim and get real-time prescription coverage detail for your patients who are UnitedHealthcare benefit plan members . This will allow you to check current prescription coverage and price, including out-of-pocket prescription costs for UnitedHealthcare members at their selected pharmacy, as well as:
• Get information on lower-cost prescription alternatives, if available, to help save members money .
• See which prescriptions currently require prior authorization, or are non-covered or non-preferred .
• Request prior authorization and receive status and results .
The app is now available to all Link users; to access, sign in to UHCprovider.com, then select the Link Marketplace from your Link dashboard and search for the PreCheck MyScript app . Add the app to your dashboard and start using it .
The below are also options to obtain authorization:
• Online: Use the Online Prior Authorization tool (available through UHCprovider.com) . The majority of online prior authorizations are approved in real-time, and an autopopulation feature provides 95 percent of a member’s information . Prior authorizations can also be submitted online by signing in to optumrx.com > Healthcare Professionals > Prior Authorizations .
• By Phone: Call the OptumRx Prior Authorization team at 800-711-4555 .
+For New Jersey fully insured members this program is referred to as First Start .
1 In certain documents the Prescription Drug List (PDL) was referred to as the “Preferred Drug List (PDL) .” This change in descriptive terms does not affect your patient’s benefit coverage .
2 Where differences are noted, the benefit plan documents will govern .
3 In certain documents Tier 1 was referred to as “generics;” Tier 2 was referred to as “preferred brands” or “brand-name” on the PDL; and Tier 3 was referred to as “non-preferred brands,” “not on the PDL,” or “brand-name not on the PDL .” These changes in descriptive terms do not affect your patient’s benefit coverage .

7
Please refer to page 4 for a definition of notations/symbols.
* Products listed in Tier 1 may be covered in Tier 3 in a non-standard Prescription Drug List *** Products listed in Tier 3 may be covered in Tier 1 in a non-standard Prescription Drug List ** Products listed in Tier 2 may be covered in Tier 1 in a non-standard Prescription Drug List ^̂ Products listed in Tier 2 may be covered in Tier 3 in a non-standard Prescription Drug List
© 2018 UnitedHealthCare Services, Inc. All rights reserved. 7/18
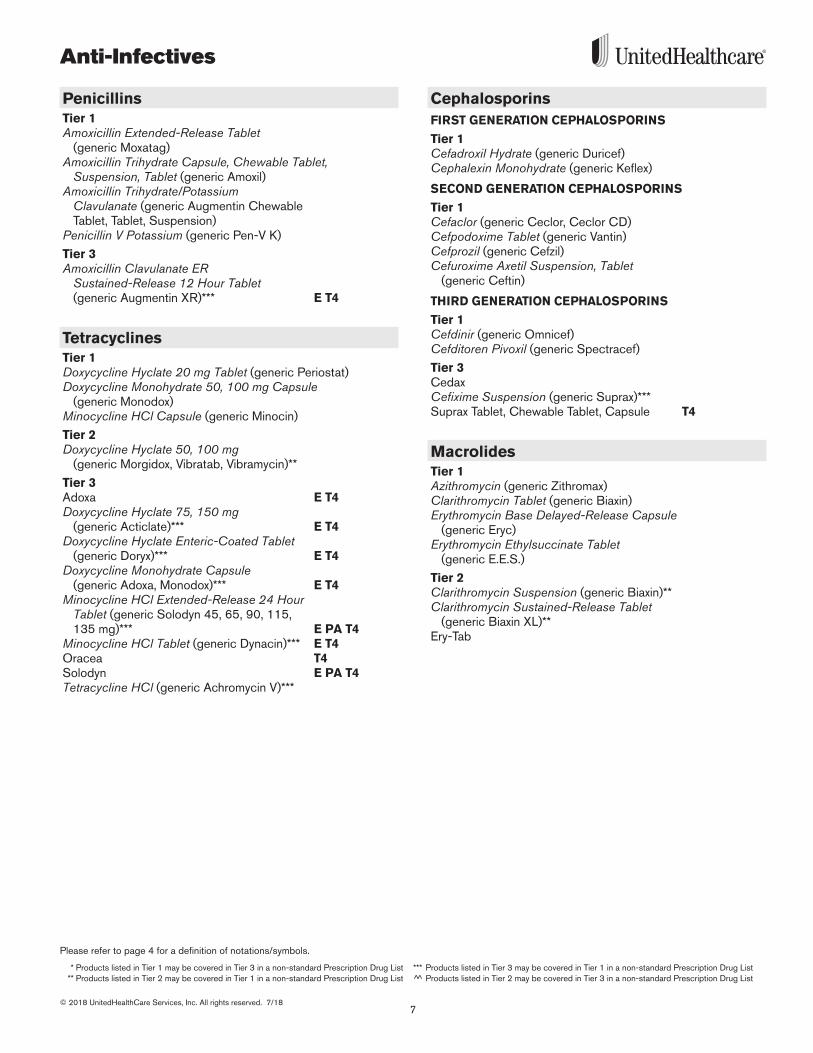
Anti-Infectives
PenicillinsTier 1Amoxicillin Extended-Release Tablet
(generic Moxatag) Amoxicillin Trihydrate Capsule, Chewable Tablet,
Suspension, Tablet (generic Amoxil)Amoxicillin Trihydrate/Potassium
Clavulanate (generic Augmentin Chewable Tablet, Tablet, Suspension)
Penicillin V Potassium (generic Pen-V K)
Tier 3Amoxicillin Clavulanate ER
Sustained-Release 12 Hour Tablet (generic Augmentin XR)*** E T4
TetracyclinesTier 1Doxycycline Hyclate 20 mg Tablet (generic Periostat) Doxycycline Monohydrate 50, 100 mg Capsule
(generic Monodox)Minocycline HCl Capsule (generic Minocin)
Tier 2Doxycycline Hyclate 50, 100 mg
(generic Morgidox, Vibratab, Vibramycin)**
Tier 3Adoxa E T4Doxycycline Hyclate 75, 150 mg
(generic Acticlate)*** E T4Doxycycline Hyclate Enteric-Coated Tablet
(generic Doryx)*** E T4Doxycycline Monohydrate Capsule
(generic Adoxa, Monodox)*** E T4Minocycline HCl Extended-Release 24 Hour
Tablet (generic Solodyn 45, 65, 90, 115, 135 mg)*** E PA T4
Minocycline HCl Tablet (generic Dynacin)*** E T4Oracea T4Solodyn E PA T4Tetracycline HCl (generic Achromycin V)***
CephalosporinsFIRST GENERATION CEPHALOSPORINS
Tier 1Cefadroxil Hydrate (generic Duricef)Cephalexin Monohydrate (generic Keflex)
SECOND GENERATION CEPHALOSPORINS
Tier 1Cefaclor (generic Ceclor, Ceclor CD)Cefpodoxime Tablet (generic Vantin)Cefprozil (generic Cefzil)Cefuroxime Axetil Suspension, Tablet
(generic Ceftin)
THIRD GENERATION CEPHALOSPORINS
Tier 1Cefdinir (generic Omnicef)Cefditoren Pivoxil (generic Spectracef)
Tier 3CedaxCefixime Suspension (generic Suprax)*** Suprax Tablet, Chewable Tablet, Capsule T4
MacrolidesTier 1Azithromycin (generic Zithromax)Clarithromycin Tablet (generic Biaxin)Erythromycin Base Delayed-Release Capsule
(generic Eryc)Erythromycin Ethylsuccinate Tablet
(generic E .E .S .)
Tier 2Clarithromycin Suspension (generic Biaxin)**Clarithromycin Sustained-Release Tablet
(generic Biaxin XL)**Ery-Tab
8
Anti-Infectives
© 2018 UnitedHealthCare Services, Inc. All rights reserved. 7/18
^ Health Care Reform drug lists may vary by plan, your patient can find the most up-to-date Tier status and cost information for a particular medication by visiting myuhc.com and/or calling the toll-free member phone number on their health care ID card.
**** Depending on your patients’ benefit and/or medication, notification or medical necessity criteria will be applied to determine if covered under the pharmacy benefit.
MC Multiple copayPA Prior authorization required****RS May be eligible for the refill and save programSL Supply limit
E May be excluded from coverageH May be part of health care reform preventive^H-PA May be part of health care reform preventive with
prior authorization^
SP Specialty medicationST Step therapyT4 May be covered on Tier 4 in selected benefits
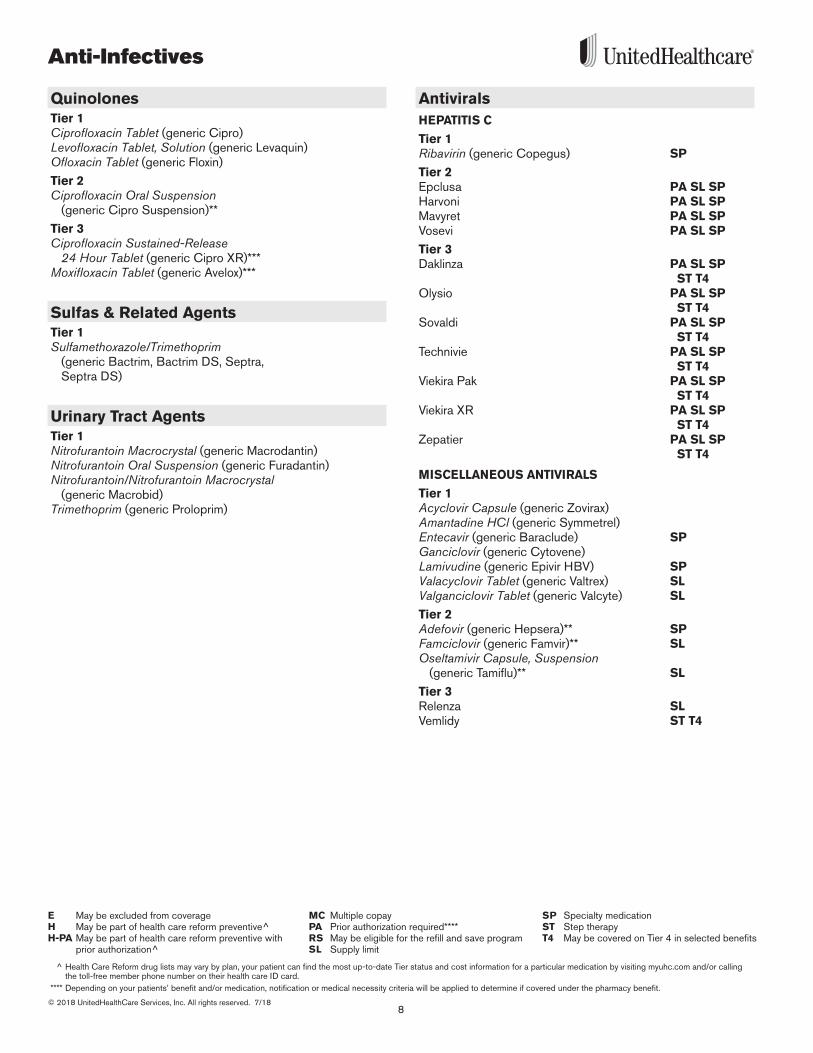
QuinolonesTier 1Ciprofloxacin Tablet (generic Cipro)Levofloxacin Tablet, Solution (generic Levaquin)Ofloxacin Tablet (generic Floxin)
Tier 2Ciprofloxacin Oral Suspension
(generic Cipro Suspension)**
Tier 3Ciprofloxacin Sustained-Release
24 Hour Tablet (generic Cipro XR)***Moxifloxacin Tablet (generic Avelox)***
Sulfas & Related AgentsTier 1Sulfamethoxazole/Trimethoprim
(generic Bactrim, Bactrim DS, Septra, Septra DS)
Urinary Tract AgentsTier 1Nitrofurantoin Macrocrystal (generic Macrodantin)Nitrofurantoin Oral Suspension (generic Furadantin)Nitrofurantoin/Nitrofurantoin Macrocrystal
(generic Macrobid)Trimethoprim (generic Proloprim)
AntiviralsHEPATITIS C
Tier 1Ribavirin (generic Copegus) SP
Tier 2Epclusa PA SL SPHarvoni PA SL SPMavyret PA SL SPVosevi PA SL SP
Tier 3Daklinza PA SL SP
ST T4Olysio PA SL SP
ST T4Sovaldi PA SL SP
ST T4Technivie PA SL SP
ST T4Viekira Pak PA SL SP
ST T4Viekira XR PA SL SP
ST T4Zepatier PA SL SP
ST T4
MISCELLANEOUS ANTIVIRALS
Tier 1Acyclovir Capsule (generic Zovirax)Amantadine HCl (generic Symmetrel)Entecavir (generic Baraclude) SPGanciclovir (generic Cytovene) Lamivudine (generic Epivir HBV) SPValacyclovir Tablet (generic Valtrex) SLValganciclovir Tablet (generic Valcyte) SL
Tier 2Adefovir (generic Hepsera)** SPFamciclovir (generic Famvir)** SLOseltamivir Capsule, Suspension
(generic Tamiflu)** SL
Tier 3Relenza SL Vemlidy ST T4

9
Please refer to page 4 for a definition of notations/symbols.
* Products listed in Tier 1 may be covered in Tier 3 in a non-standard Prescription Drug List *** Products listed in Tier 3 may be covered in Tier 1 in a non-standard Prescription Drug List ** Products listed in Tier 2 may be covered in Tier 1 in a non-standard Prescription Drug List ^̂ Products listed in Tier 2 may be covered in Tier 3 in a non-standard Prescription Drug List
© 2018 UnitedHealthCare Services, Inc. All rights reserved. 7/18
Anti-Infectives
HIV/AIDS THERAPY
Tier 1Abacavir (generic Ziagen) SPAbacavir/Lamivudine/Zidovudine
(generic Trizivir) SPDidanosine Enteric-Coated Capsule
(generic Videx EC) SPLamivudine Solution, Tablet (generic Epivir) SPNevirapine (generic Viramune) SPStavudine Capsule (generic Zerit) SPZidovudine (generic Retrovir) SPZidovudine/Lamivudine (generic Combivir) SP
Tier 2Abacavir/Lamivudine (generic Epzicom)** SPAptivus SPAtazanavir Capsule (generic Reyataz)** SP Atripla SPCrixivan SPEdurant SPEfavirenz (generic Sustiva)** SPEmtriva SPEvotaz SPFosamprenavir Tablet (generic Lexiva)** SPFuzeon SPIntelence SPInvirase SPIsentress SPJuluca SP Kaletra Tablet SPLopinavir/Ritonavir Solution
(generic Kaletra)** SP Norvir Capsule, Solution SPPrezcobix SPPrezista SPRitonavir Tablet (generic Norvir)** SPSelzentry PA SPTenofovir Tablet (generic Viread)** SPTriumeq SPTybost SPViracept SP
Tier 3Complera SP T4Descovy SP T4Genvoya SP ST T4Nevirapine Extended-Release
(generic Viramune XR)*** E SP T4Odefsey SP T4Stribild SP STTivicay SPTruvada SP T4
Antifungal AgentsTier 1Clotrimazole Troche (generic Mycelex)Fluconazole Tablet (generic Diflucan)Griseofulvin Microsize (generic Grifulvin V)Griseofulvin Ultramicrosize (generic Gris-Peg)Itraconazole Capsule
(generic Sporanox Capsule) SLKetoconazole Tablet (generic Nizoral)Nystatin Powder, Tablet (generic Mycostatin)Terbinafine Tablet (generic Lamisil) SLVoriconazole Tablet (generic Vfend) SL
Tier 2Noxafil Suspension, TabletSporanox Solution, Oral
Tier 3Cresemba Jublia PA SL ST T4Kerydin PA SL ST T4Lamisil Granules SL
VancomycinTier 1Vancomycin Capsule (generic Vancocin HCl) SL
Miscellaneous Anti-infectivesTier 1Clindamycin Capsule (generic Cleocin HCl)Neomycin Sulfate (generic Neomycin Sulfate)
Tier 2Bethkis** PA SP SLCayston PA SP SLDapsone**Linezolid Tablet (generic Zyvox)** SL
Tier 3Dificid SL Tobi Podhaler PA SL SPTobramycin Nebulized Solution E PA SL SP T4
(generic Tobi)***
10
Anti-Infectives
© 2018 UnitedHealthCare Services, Inc. All rights reserved. 7/18
^ Health Care Reform drug lists may vary by plan, your patient can find the most up-to-date Tier status and cost information for a particular medication by visiting myuhc.com and/or calling the toll-free member phone number on their health care ID card.
**** Depending on your patients’ benefit and/or medication, notification or medical necessity criteria will be applied to determine if covered under the pharmacy benefit.
MC Multiple copayPA Prior authorization required****RS May be eligible for the refill and save programSL Supply limit
E May be excluded from coverageH May be part of health care reform preventive^H-PA May be part of health care reform preventive with
prior authorization^
SP Specialty medicationST Step therapyT4 May be covered on Tier 4 in selected benefits
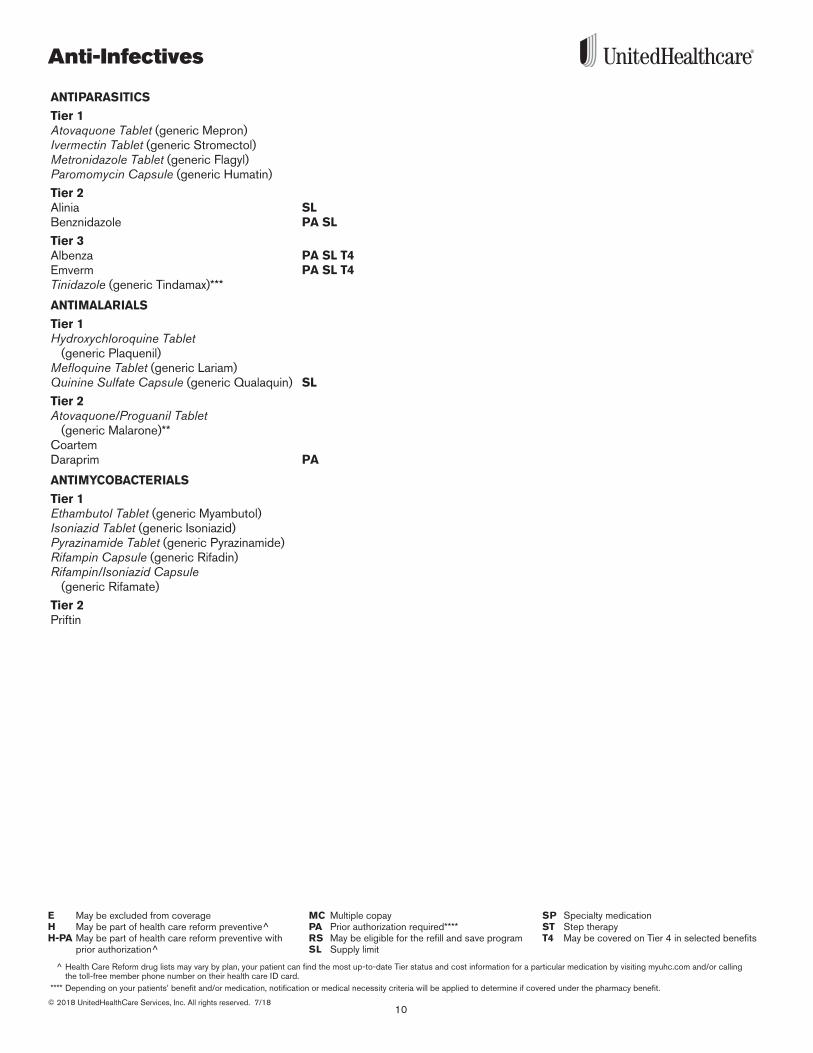
ANTIPARASITICS
Tier 1Atovaquone Tablet (generic Mepron)Ivermectin Tablet (generic Stromectol) Metronidazole Tablet (generic Flagyl)Paromomycin Capsule (generic Humatin)
Tier 2Alinia SLBenznidazole PA SL
Tier 3Albenza PA SL T4 Emverm PA SL T4 Tinidazole (generic Tindamax)***
ANTIMALARIALS
Tier 1Hydroxychloroquine Tablet
(generic Plaquenil)Mefloquine Tablet (generic Lariam)Quinine Sulfate Capsule (generic Qualaquin) SL
Tier 2Atovaquone/Proguanil Tablet
(generic Malarone)**CoartemDaraprim PA
ANTIMYCOBACTERIALS
Tier 1Ethambutol Tablet (generic Myambutol)Isoniazid Tablet (generic Isoniazid)Pyrazinamide Tablet (generic Pyrazinamide)Rifampin Capsule (generic Rifadin)Rifampin/Isoniazid Capsule
(generic Rifamate)
Tier 2Priftin
11
Please refer to page 4 for a definition of notations/symbols.
* Products listed in Tier 1 may be covered in Tier 3 in a non-standard Prescription Drug List *** Products listed in Tier 3 may be covered in Tier 1 in a non-standard Prescription Drug List ** Products listed in Tier 2 may be covered in Tier 1 in a non-standard Prescription Drug List ^̂ Products listed in Tier 2 may be covered in Tier 3 in a non-standard Prescription Drug List
© 2018 UnitedHealthCare Services, Inc. All rights reserved. 7/18
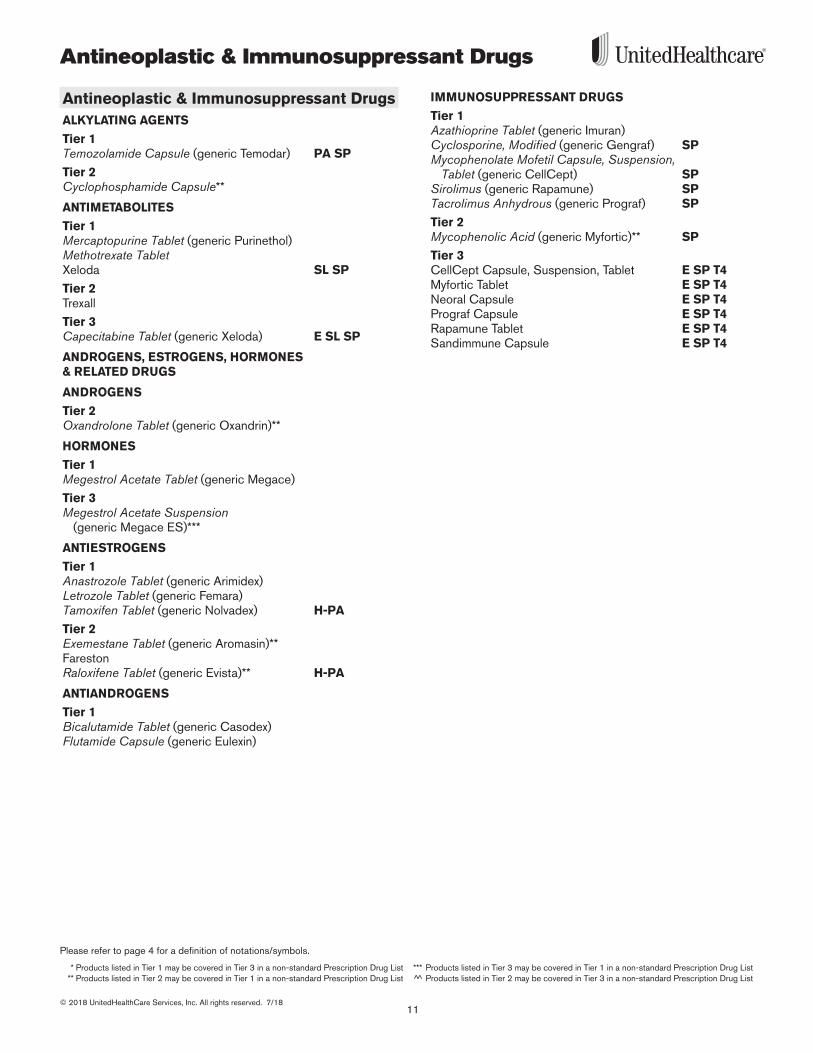
Antineoplastic & Immunosuppressant Drugs
Antineoplastic & Immunosuppressant DrugsALKYLATING AGENTS
Tier 1Temozolamide Capsule (generic Temodar) PA SP
Tier 2Cyclophosphamide Capsule**
ANTIMETABOLITES
Tier 1Mercaptopurine Tablet (generic Purinethol)Methotrexate TabletXeloda SL SP
Tier 2Trexall
Tier 3Capecitabine Tablet (generic Xeloda) E SL SP
ANDROGENS, ESTROGENS, HORMONES & RELATED DRUGS
ANDROGENS
Tier 2Oxandrolone Tablet (generic Oxandrin)**
HORMONES
Tier 1Megestrol Acetate Tablet (generic Megace)
Tier 3Megestrol Acetate Suspension
(generic Megace ES)***
ANTIESTROGENS
Tier 1Anastrozole Tablet (generic Arimidex)Letrozole Tablet (generic Femara)Tamoxifen Tablet (generic Nolvadex) H-PA
Tier 2Exemestane Tablet (generic Aromasin)**FarestonRaloxifene Tablet (generic Evista)** H-PA
ANTIANDROGENS
Tier 1Bicalutamide Tablet (generic Casodex)Flutamide Capsule (generic Eulexin)
IMMUNOSUPPRESSANT DRUGS
Tier 1Azathioprine Tablet (generic Imuran)Cyclosporine, Modified (generic Gengraf) SPMycophenolate Mofetil Capsule, Suspension,
Tablet (generic CellCept) SPSirolimus (generic Rapamune) SPTacrolimus Anhydrous (generic Prograf) SP
Tier 2Mycophenolic Acid (generic Myfortic)** SP
Tier 3CellCept Capsule, Suspension, Tablet E SP T4Myfortic Tablet E SP T4 Neoral Capsule E SP T4Prograf Capsule E SP T4Rapamune Tablet E SP T4Sandimmune Capsule E SP T4
Antineoplastic & Immunosuppressant Drugs
12© 2018 UnitedHealthCare Services, Inc . All rights reserved . 7/18
^ Health Care Reform drug lists may vary by plan, your patient can find the most up-to-date Tier status and cost information for a particular medication by visiting myuhc .com and/or calling the toll-free member phone number on their health care ID card .
**** Depending on your patients’ benefit and/or medication, notification or medical necessity criteria will be applied to determine if covered under the pharmacy benefit .
MC Multiple copayPA Prior authorization required****RS May be eligible for the refill and save programSL Supply limit
E May be excluded from coverageH May be part of health care reform preventive^H-PA May be part of health care reform preventive with
prior authorization^
SP Specialty medicationST Step therapyT4 May be covered on Tier 4 in selected benefits
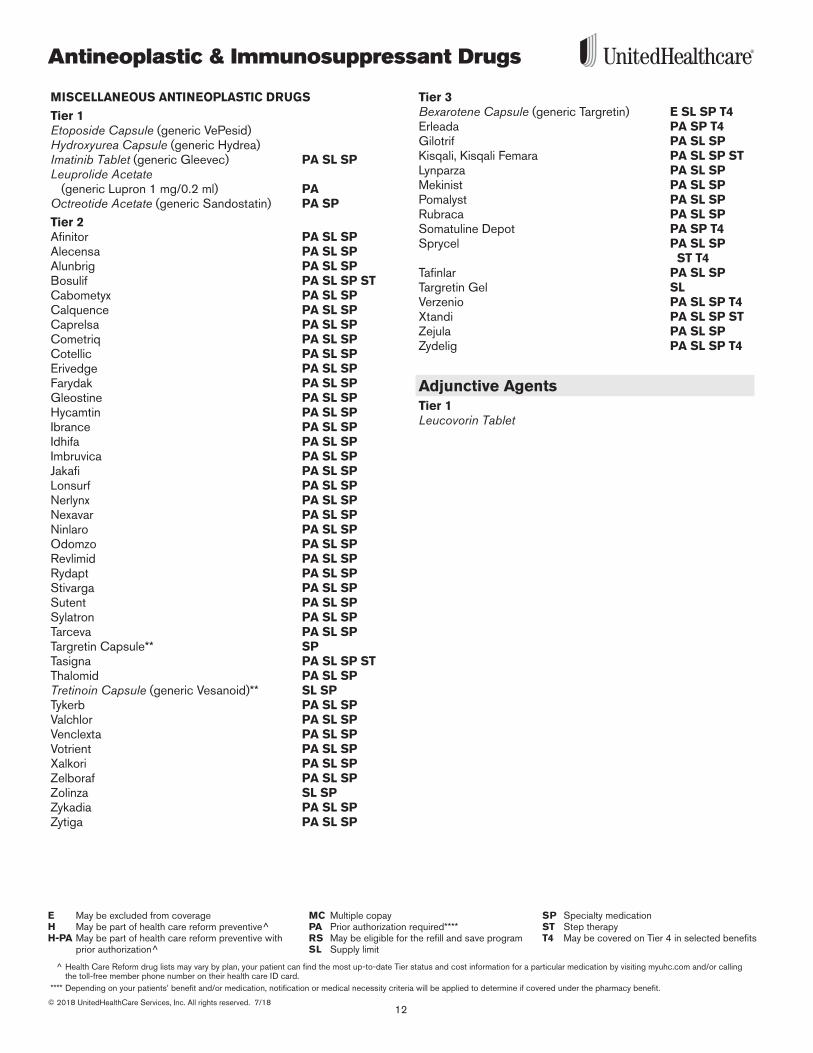
MISCELLANEOUS ANTINEOPLASTIC DRUGS
Tier 1Etoposide Capsule (generic VePesid)Hydroxyurea Capsule (generic Hydrea)Imatinib Tablet (generic Gleevec) PA SL SPLeuprolide Acetate
(generic Lupron 1 mg/0 .2 ml) PAOctreotide Acetate (generic Sandostatin) PA SP
Tier 2Afinitor PA SL SPAlecensa PA SL SPAlunbrig PA SL SP Bosulif PA SL SP STCabometyx PA SL SPCalquence PA SL SP Caprelsa PA SL SPCometriq PA SL SPCotellic PA SL SPErivedge PA SL SPFarydak PA SL SPGleostine PA SL SPHycamtin PA SL SPIbrance PA SL SPIdhifa PA SL SP Imbruvica PA SL SPJakafi PA SL SPLonsurf PA SL SPNerlynx PA SL SP Nexavar PA SL SPNinlaro PA SL SPOdomzo PA SL SPRevlimid PA SL SPRydapt PA SL SP Stivarga PA SL SPSutent PA SL SPSylatron PA SL SPTarceva PA SL SPTargretin Capsule** SP Tasigna PA SL SP STThalomid PA SL SPTretinoin Capsule (generic Vesanoid)** SL SPTykerb PA SL SPValchlor PA SL SPVenclexta PA SL SPVotrient PA SL SPXalkori PA SL SPZelboraf PA SL SPZolinza SL SPZykadia PA SL SP Zytiga PA SL SP
Tier 3Bexarotene Capsule (generic Targretin) E SL SP T4 Erleada PA SP T4 Gilotrif PA SL SPKisqali, Kisqali Femara PA SL SP STLynparza PA SL SP Mekinist PA SL SPPomalyst PA SL SPRubraca PA SL SPSomatuline Depot PA SP T4Sprycel PA SL SP
ST T4Tafinlar PA SL SPTargretin Gel SLVerzenio PA SL SP T4 Xtandi PA SL SP STZejula PA SL SP Zydelig PA SL SP T4
Adjunctive AgentsTier 1Leucovorin Tablet
13
Please refer to page 4 for a definition of notations/symbols.
* Products listed in Tier 1 may be covered in Tier 3 in a non-standard Prescription Drug List *** Products listed in Tier 3 may be covered in Tier 1 in a non-standard Prescription Drug List ** Products listed in Tier 2 may be covered in Tier 1 in a non-standard Prescription Drug List ^̂ Products listed in Tier 2 may be covered in Tier 3 in a non-standard Prescription Drug List
© 2018 UnitedHealthCare Services, Inc. All rights reserved. 7/18
Autonomic & CNS Drugs, Neurology & Psych
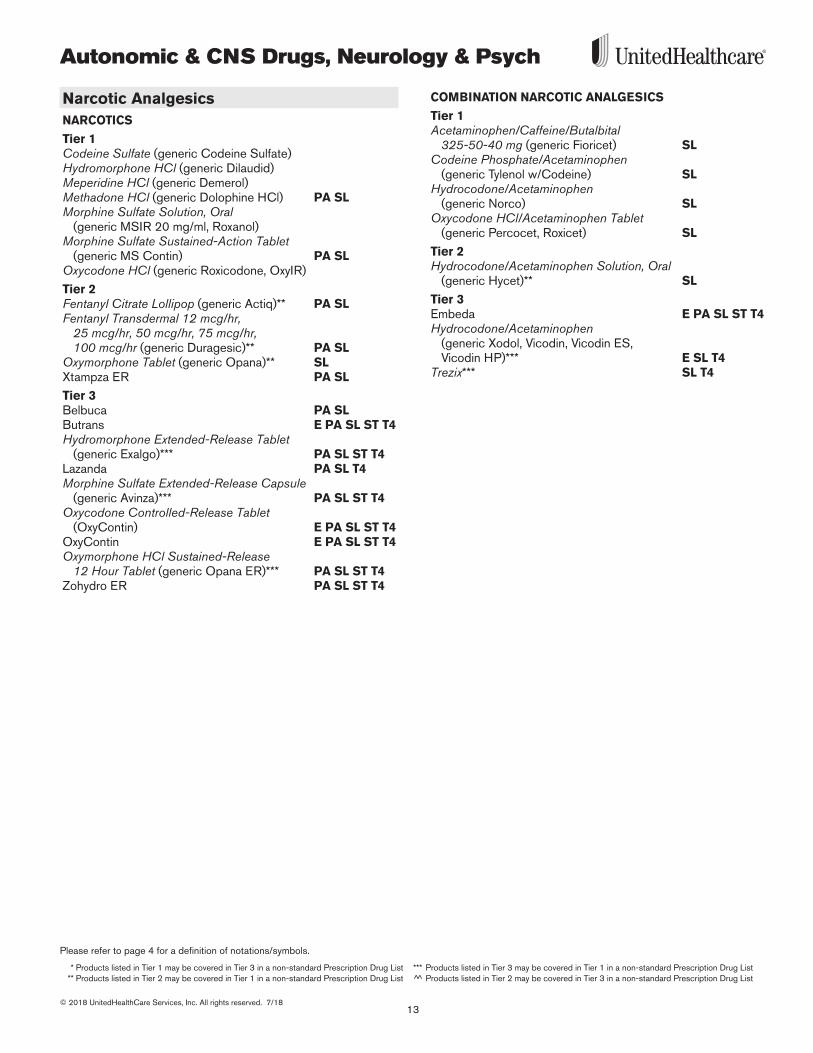
Narcotic AnalgesicsNARCOTICS
Tier 1Codeine Sulfate (generic Codeine Sulfate) Hydromorphone HCl (generic Dilaudid)Meperidine HCl (generic Demerol)Methadone HCl (generic Dolophine HCl) PA SLMorphine Sulfate Solution, Oral
(generic MSIR 20 mg/ml, Roxanol)Morphine Sulfate Sustained-Action Tablet
(generic MS Contin) PA SLOxycodone HCl (generic Roxicodone, OxyIR)
Tier 2Fentanyl Citrate Lollipop (generic Actiq)** PA SL Fentanyl Transdermal 12 mcg/hr,
25 mcg/hr, 50 mcg/hr, 75 mcg/hr, 100 mcg/hr (generic Duragesic)** PA SL
Oxymorphone Tablet (generic Opana)** SLXtampza ER PA SL
Tier 3Belbuca PA SLButrans E PA SL ST T4Hydromorphone Extended-Release Tablet
(generic Exalgo)*** PA SL ST T4Lazanda PA SL T4Morphine Sulfate Extended-Release Capsule
(generic Avinza)*** PA SL ST T4Oxycodone Controlled-Release Tablet
(OxyContin) E PA SL ST T4 OxyContin E PA SL ST T4Oxymorphone HCl Sustained-Release
12 Hour Tablet (generic Opana ER)*** PA SL ST T4Zohydro ER PA SL ST T4
COMBINATION NARCOTIC ANALGESICS
Tier 1Acetaminophen/Caffeine/Butalbital
325-50-40 mg (generic Fioricet) SLCodeine Phosphate/Acetaminophen
(generic Tylenol w/Codeine) SLHydrocodone/Acetaminophen
(generic Norco) SLOxycodone HCl/Acetaminophen Tablet
(generic Percocet, Roxicet) SL
Tier 2Hydrocodone/Acetaminophen Solution, Oral
(generic Hycet)** SL
Tier 3Embeda E PA SL ST T4Hydrocodone/Acetaminophen
(generic Xodol, Vicodin, Vicodin ES, Vicodin HP)*** E SL T4
Trezix*** SL T4

Autonomic & CNS Drugs, Neurology & Psych
14© 2018 UnitedHealthCare Services, Inc. All rights reserved. 7/18
^ Health Care Reform drug lists may vary by plan, your patient can find the most up-to-date Tier status and cost information for a particular medication by visiting myuhc.com and/or calling the toll-free member phone number on their health care ID card.
**** Depending on your patients’ benefit and/or medication, notification or medical necessity criteria will be applied to determine if covered under the pharmacy benefit.
MC Multiple copayPA Prior authorization required****RS May be eligible for the refill and save programSL Supply limit
E May be excluded from coverageH May be part of health care reform preventive^H-PA May be part of health care reform preventive with
prior authorization^
SP Specialty medicationST Step therapyT4 May be covered on Tier 4 in selected benefits
Non-Narcotic AnalgesicsMISCELLANEOUS ANALGESICS
Tier 1Tramadol HCl (generic Ultram) Tramadol HCl/Acetaminophen
(generic Ultracet) SL
Tier 2Butorphanol Tartrate Aerosol, Spray
(generic Stadol)** SLTramadol HCl Sustained-Release
24 Hour Tablet (generic Ultram ER)** SL
Tier 3Nucynta SL T4Nucynta ER PA SL
NARCOTIC ANTAGONISTS/OPIOID DEPENDENCE
Tier 1Buprenorphine HCl Tablet, Sublingual
(generic Subutex) SL Naloxone Injection (generic Narcan) SL Naltrexone HCl (generic ReVia)
Tier 2Narcan Nasal Spray SL Zubsolv** SL
Tier 3Bunavail E PA SL T4 Buprenorphine HCl/Naloxone HCl Tablet,
Sublingual (generic Suboxone)** E PA SL T4Evzio E PA SL T4 Suboxone Film E PA SL T4
Migraine & Cluster Headache TherapyTier 1Naratriptan HCl (generic Amerge) SLRizatriptan Benzoate Orally Disintegrating
Tablet, Tablet (generic Maxalt, Maxalt MLT) SLSumatriptan Succinate Injection
(generic Imitrex Injection) SLSumatriptan Succinate Tablet
(generic Imitrex Tablet) SL
Tier 2Eletriptan (generic Relpax)** SLSumatriptan Succinate Nasal Spray
(generic Imitrex Nasal Spray)** SL
Tier 3Almotriptan (generic Axert)*** SL Dihydroergotamine Nasal Spray
(generic Migranal)*** PA SL T4Frovatriptan (generic Frova)*** SL Onzetra Xsail E SL T4 Sumatriptan/Naproxen 85-500 mg
(generic Treximet) E SL T4Zembrace SymTouch E SL T4 Zolmitriptan Orally Disintegrating Tablet
(generic Zomig-ZMT)*** SLZolmitriptan Tablet (generic Zomig)*** SLZomig Nasal Spray SL
15
Please refer to page 4 for a definition of notations/symbols.
* Products listed in Tier 1 may be covered in Tier 3 in a non-standard Prescription Drug List *** Products listed in Tier 3 may be covered in Tier 1 in a non-standard Prescription Drug List ** Products listed in Tier 2 may be covered in Tier 1 in a non-standard Prescription Drug List ^̂ Products listed in Tier 2 may be covered in Tier 3 in a non-standard Prescription Drug List
© 2018 UnitedHealthCare Services, Inc. All rights reserved. 7/18
Autonomic & CNS Drugs, Neurology & Psych
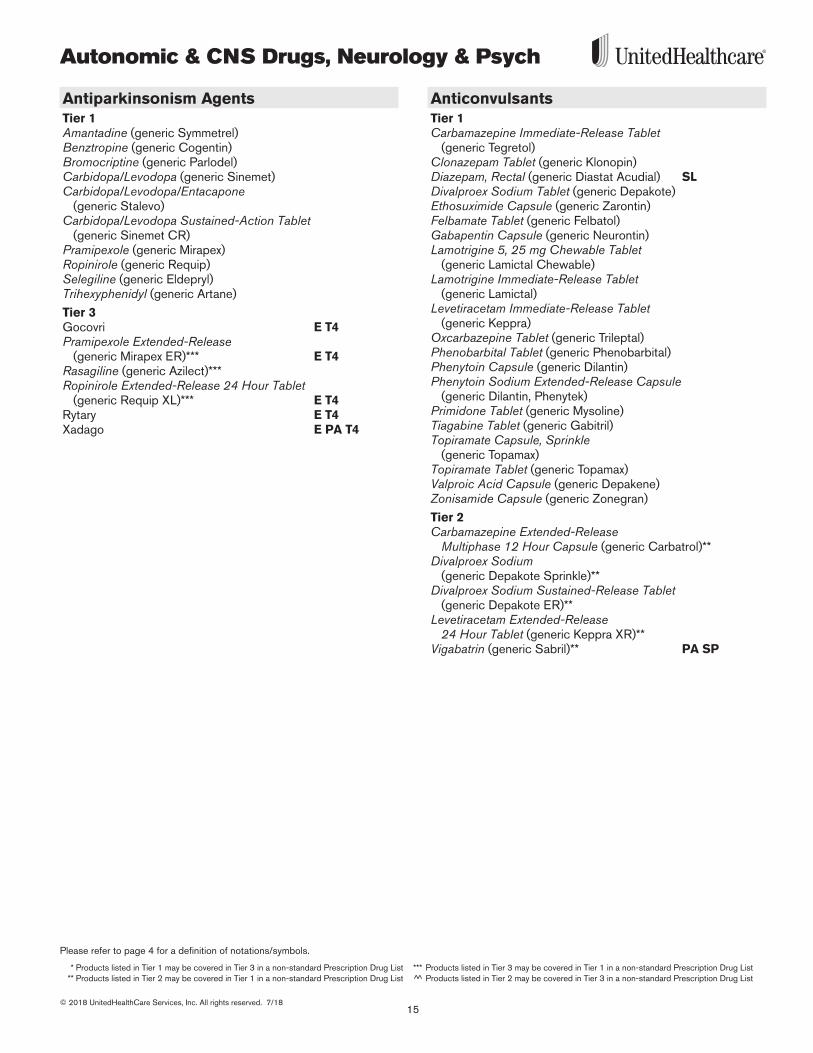
Antiparkinsonism AgentsTier 1Amantadine (generic Symmetrel)Benztropine (generic Cogentin)Bromocriptine (generic Parlodel)Carbidopa/Levodopa (generic Sinemet)Carbidopa/Levodopa/Entacapone
(generic Stalevo)Carbidopa/Levodopa Sustained-Action Tablet
(generic Sinemet CR)Pramipexole (generic Mirapex)Ropinirole (generic Requip)Selegiline (generic Eldepryl)Trihexyphenidyl (generic Artane)
Tier 3Gocovri E T4Pramipexole Extended-Release
(generic Mirapex ER)*** E T4Rasagiline (generic Azilect)*** Ropinirole Extended-Release 24 Hour Tablet
(generic Requip XL)*** E T4Rytary E T4Xadago E PA T4
AnticonvulsantsTier 1Carbamazepine Immediate-Release Tablet
(generic Tegretol)Clonazepam Tablet (generic Klonopin)Diazepam, Rectal (generic Diastat Acudial) SLDivalproex Sodium Tablet (generic Depakote)Ethosuximide Capsule (generic Zarontin)Felbamate Tablet (generic Felbatol)Gabapentin Capsule (generic Neurontin)Lamotrigine 5, 25 mg Chewable Tablet
(generic Lamictal Chewable)Lamotrigine Immediate-Release Tablet
(generic Lamictal)Levetiracetam Immediate-Release Tablet
(generic Keppra)Oxcarbazepine Tablet (generic Trileptal)Phenobarbital Tablet (generic Phenobarbital)Phenytoin Capsule (generic Dilantin)Phenytoin Sodium Extended-Release Capsule
(generic Dilantin, Phenytek)Primidone Tablet (generic Mysoline)Tiagabine Tablet (generic Gabitril) Topiramate Capsule, Sprinkle
(generic Topamax)Topiramate Tablet (generic Topamax)Valproic Acid Capsule (generic Depakene)Zonisamide Capsule (generic Zonegran)
Tier 2Carbamazepine Extended-Release
Multiphase 12 Hour Capsule (generic Carbatrol)** Divalproex Sodium
(generic Depakote Sprinkle)**Divalproex Sodium Sustained-Release Tablet
(generic Depakote ER)** Levetiracetam Extended-Release
24 Hour Tablet (generic Keppra XR)**Vigabatrin (generic Sabril)** PA SP
Autonomic & CNS Drugs, Neurology & Psych
16© 2018 UnitedHealthCare Services, Inc. All rights reserved. 7/18
^ Health Care Reform drug lists may vary by plan, your patient can find the most up-to-date Tier status and cost information for a particular medication by visiting myuhc.com and/or calling the toll-free member phone number on their health care ID card.
**** Depending on your patients’ benefit and/or medication, notification or medical necessity criteria will be applied to determine if covered under the pharmacy benefit.
MC Multiple copayPA Prior authorization required****RS May be eligible for the refill and save programSL Supply limit
E May be excluded from coverageH May be part of health care reform preventive^H-PA May be part of health care reform preventive with
prior authorization^
SP Specialty medicationST Step therapyT4 May be covered on Tier 4 in selected benefits
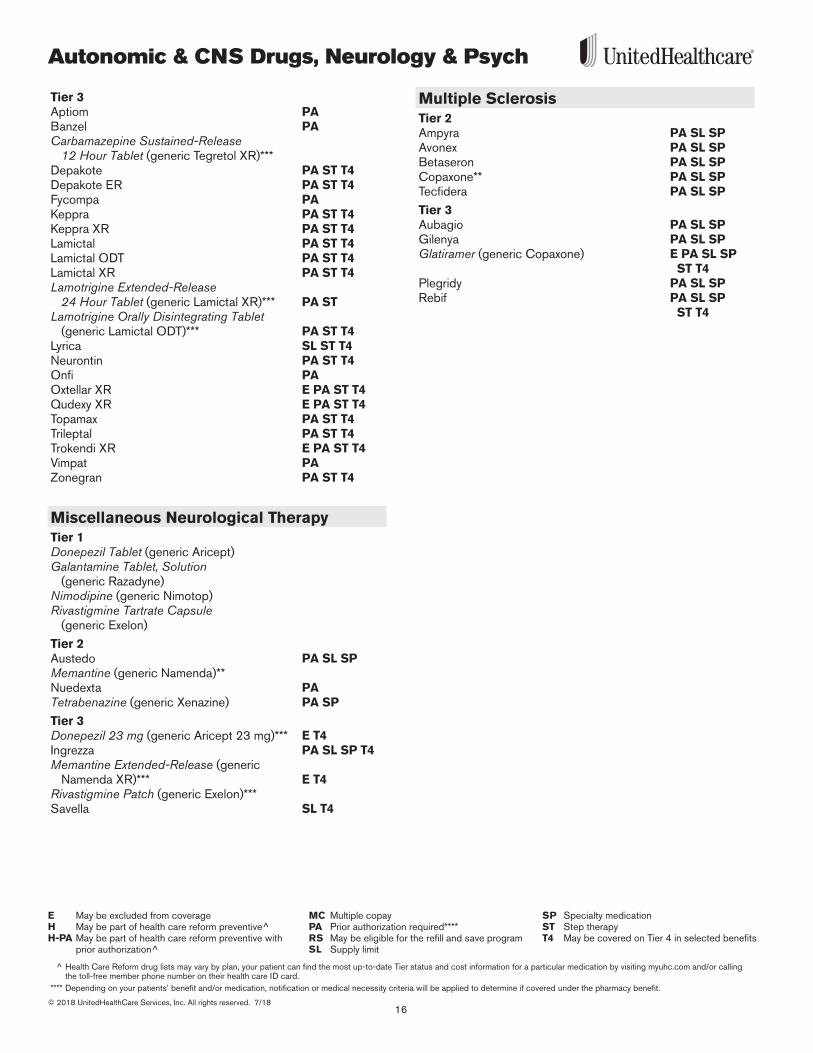
Tier 3Aptiom PABanzel PACarbamazepine Sustained-Release
12 Hour Tablet (generic Tegretol XR)*** Depakote PA ST T4Depakote ER PA ST T4Fycompa PAKeppra PA ST T4Keppra XR PA ST T4Lamictal PA ST T4Lamictal ODT PA ST T4Lamictal XR PA ST T4 Lamotrigine Extended-Release
24 Hour Tablet (generic Lamictal XR)*** PA STLamotrigine Orally Disintegrating Tablet
(generic Lamictal ODT)*** PA ST T4Lyrica SL ST T4 Neurontin PA ST T4Onfi PA Oxtellar XR E PA ST T4Qudexy XR E PA ST T4Topamax PA ST T4Trileptal PA ST T4Trokendi XR E PA ST T4Vimpat PAZonegran PA ST T4
Miscellaneous Neurological TherapyTier 1Donepezil Tablet (generic Aricept)Galantamine Tablet, Solution
(generic Razadyne)Nimodipine (generic Nimotop)Rivastigmine Tartrate Capsule
(generic Exelon)
Tier 2Austedo PA SL SPMemantine (generic Namenda)**Nuedexta PATetrabenazine (generic Xenazine) PA SP
Tier 3Donepezil 23 mg (generic Aricept 23 mg)*** E T4Ingrezza PA SL SP T4 Memantine Extended-Release (generic
Namenda XR)*** E T4Rivastigmine Patch (generic Exelon)*** Savella SL T4
Multiple SclerosisTier 2Ampyra PA SL SPAvonex PA SL SPBetaseron PA SL SPCopaxone** PA SL SP Tecfidera PA SL SP
Tier 3Aubagio PA SL SPGilenya PA SL SPGlatiramer (generic Copaxone) E PA SL SP
ST T4Plegridy PA SL SPRebif PA SL SP
ST T4
17
Please refer to page 4 for a definition of notations/symbols.
* Products listed in Tier 1 may be covered in Tier 3 in a non-standard Prescription Drug List *** Products listed in Tier 3 may be covered in Tier 1 in a non-standard Prescription Drug List ** Products listed in Tier 2 may be covered in Tier 1 in a non-standard Prescription Drug List ^̂ Products listed in Tier 2 may be covered in Tier 3 in a non-standard Prescription Drug List
© 2018 UnitedHealthCare Services, Inc. All rights reserved. 7/18
Autonomic & CNS Drugs, Neurology & Psych
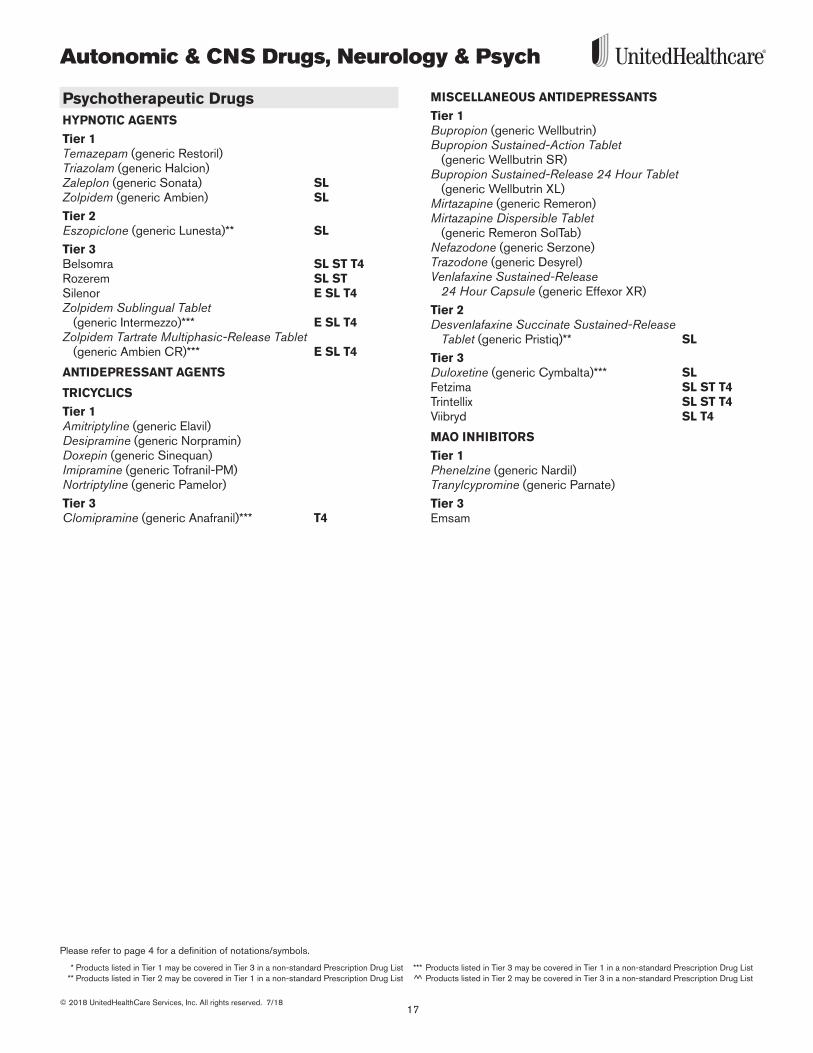
Psychotherapeutic DrugsHYPNOTIC AGENTS
Tier 1Temazepam (generic Restoril)Triazolam (generic Halcion)Zaleplon (generic Sonata) SLZolpidem (generic Ambien) SL
Tier 2Eszopiclone (generic Lunesta)** SL
Tier 3Belsomra SL ST T4Rozerem SL ST Silenor E SL T4Zolpidem Sublingual Tablet
(generic Intermezzo)*** E SL T4Zolpidem Tartrate Multiphasic-Release Tablet
(generic Ambien CR)*** E SL T4
ANTIDEPRESSANT AGENTS
TRICYCLICS
Tier 1Amitriptyline (generic Elavil)Desipramine (generic Norpramin)Doxepin (generic Sinequan)Imipramine (generic Tofranil-PM)Nortriptyline (generic Pamelor)
Tier 3Clomipramine (generic Anafranil)*** T4
MISCELLANEOUS ANTIDEPRESSANTS
Tier 1Bupropion (generic Wellbutrin)Bupropion Sustained-Action Tablet
(generic Wellbutrin SR)Bupropion Sustained-Release 24 Hour Tablet
(generic Wellbutrin XL)Mirtazapine (generic Remeron)Mirtazapine Dispersible Tablet
(generic Remeron SolTab)Nefazodone (generic Serzone)Trazodone (generic Desyrel)Venlafaxine Sustained-Release
24 Hour Capsule (generic Effexor XR)
Tier 2Desvenlafaxine Succinate Sustained-Release
Tablet (generic Pristiq)** SL
Tier 3Duloxetine (generic Cymbalta)*** SLFetzima SL ST T4Trintellix SL ST T4Viibryd SL T4
MAO INHIBITORS
Tier 1Phenelzine (generic Nardil)Tranylcypromine (generic Parnate)
Tier 3Emsam
Autonomic & CNS Drugs, Neurology & Psych
18© 2018 UnitedHealthCare Services, Inc. All rights reserved. 7/18
^ Health Care Reform drug lists may vary by plan, your patient can find the most up-to-date Tier status and cost information for a particular medication by visiting myuhc.com and/or calling the toll-free member phone number on their health care ID card.
**** Depending on your patients’ benefit and/or medication, notification or medical necessity criteria will be applied to determine if covered under the pharmacy benefit.
MC Multiple copayPA Prior authorization required****RS May be eligible for the refill and save programSL Supply limit
E May be excluded from coverageH May be part of health care reform preventive^H-PA May be part of health care reform preventive with
prior authorization^
SP Specialty medicationST Step therapyT4 May be covered on Tier 4 in selected benefits
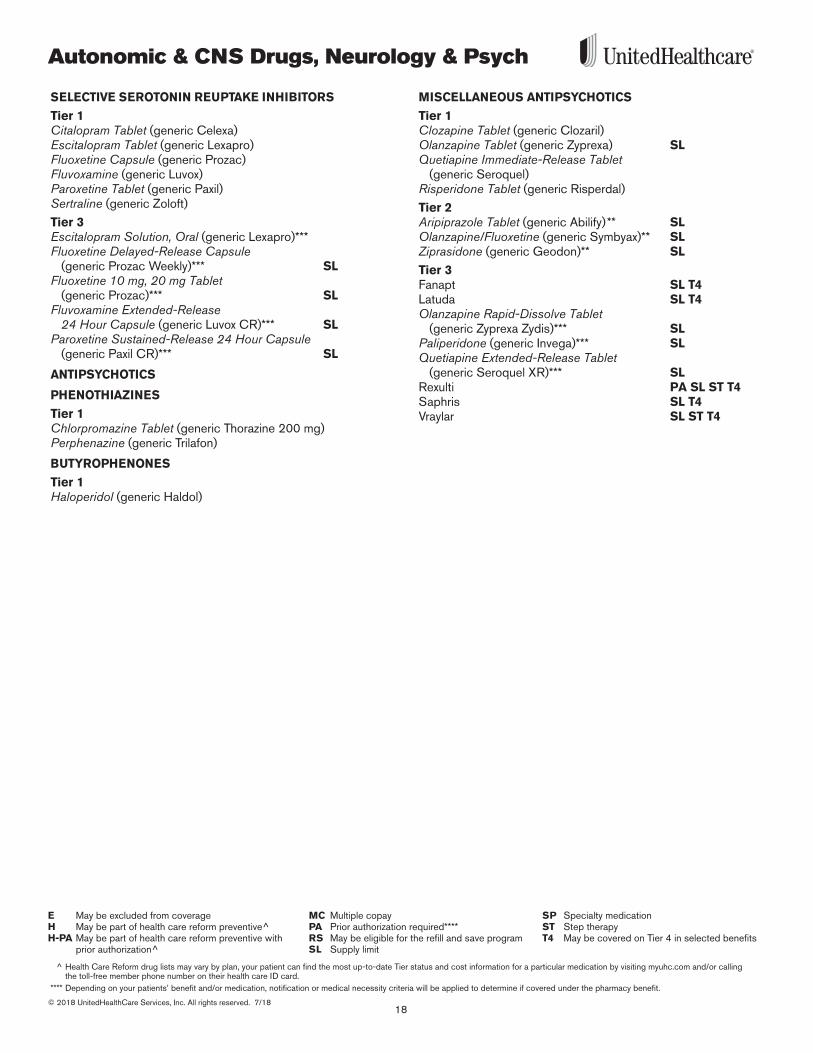
SELECTIVE SEROTONIN REUPTAKE INHIBITORS
Tier 1Citalopram Tablet (generic Celexa)Escitalopram Tablet (generic Lexapro)Fluoxetine Capsule (generic Prozac)Fluvoxamine (generic Luvox)Paroxetine Tablet (generic Paxil)Sertraline (generic Zoloft)
Tier 3Escitalopram Solution, Oral (generic Lexapro)***Fluoxetine Delayed-Release Capsule
(generic Prozac Weekly)*** SLFluoxetine 10 mg, 20 mg Tablet
(generic Prozac)*** SLFluvoxamine Extended-Release
24 Hour Capsule (generic Luvox CR)*** SLParoxetine Sustained-Release 24 Hour Capsule
(generic Paxil CR)*** SL
ANTIPSYCHOTICS
PHENOTHIAZINES
Tier 1Chlorpromazine Tablet (generic Thorazine 200 mg)Perphenazine (generic Trilafon)
BUTYROPHENONES
Tier 1Haloperidol (generic Haldol)
MISCELLANEOUS ANTIPSYCHOTICS
Tier 1Clozapine Tablet (generic Clozaril)Olanzapine Tablet (generic Zyprexa) SLQuetiapine Immediate-Release Tablet
(generic Seroquel) Risperidone Tablet (generic Risperdal)
Tier 2Aripiprazole Tablet (generic Abilify)** SLOlanzapine/Fluoxetine (generic Symbyax)** SLZiprasidone (generic Geodon)** SL
Tier 3Fanapt SL T4Latuda SL T4Olanzapine Rapid-Dissolve Tablet
(generic Zyprexa Zydis)*** SLPaliperidone (generic Invega)*** SL Quetiapine Extended-Release Tablet
(generic Seroquel XR)*** SLRexulti PA SL ST T4 Saphris SL T4Vraylar SL ST T4
19
Please refer to page 4 for a definition of notations/symbols.
* Products listed in Tier 1 may be covered in Tier 3 in a non-standard Prescription Drug List *** Products listed in Tier 3 may be covered in Tier 1 in a non-standard Prescription Drug List ** Products listed in Tier 2 may be covered in Tier 1 in a non-standard Prescription Drug List ^̂ Products listed in Tier 2 may be covered in Tier 3 in a non-standard Prescription Drug List
© 2018 UnitedHealthCare Services, Inc. All rights reserved. 7/18
Autonomic & CNS Drugs, Neurology & Psych
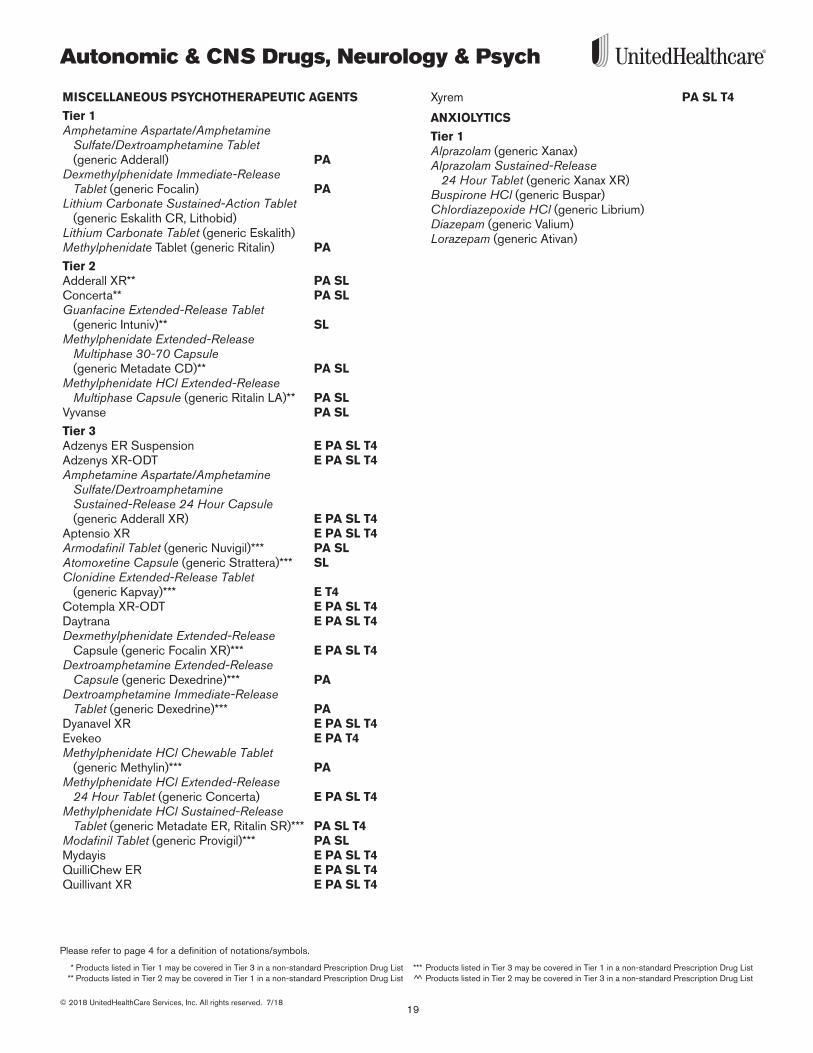
MISCELLANEOUS PSYCHOTHERAPEUTIC AGENTS
Tier 1Amphetamine Aspartate/Amphetamine
Sulfate/Dextroamphetamine Tablet (generic Adderall) PA
Dexmethylphenidate Immediate-Release Tablet (generic Focalin) PA
Lithium Carbonate Sustained-Action Tablet (generic Eskalith CR, Lithobid)
Lithium Carbonate Tablet (generic Eskalith)Methylphenidate Tablet (generic Ritalin) PA
Tier 2Adderall XR** PA SLConcerta** PA SLGuanfacine Extended-Release Tablet
(generic Intuniv)** SLMethylphenidate Extended-Release
Multiphase 30-70 Capsule (generic Metadate CD)** PA SL
Methylphenidate HCl Extended-Release Multiphase Capsule (generic Ritalin LA)** PA SL
Vyvanse PA SL
Tier 3Adzenys ER Suspension E PA SL T4 Adzenys XR-ODT E PA SL T4 Amphetamine Aspartate/Amphetamine
Sulfate/Dextroamphetamine Sustained-Release 24 Hour Capsule (generic Adderall XR) E PA SL T4
Aptensio XR E PA SL T4Armodafinil Tablet (generic Nuvigil)*** PA SLAtomoxetine Capsule (generic Strattera)*** SLClonidine Extended-Release Tablet
(generic Kapvay)*** E T4Cotempla XR-ODT E PA SL T4Daytrana E PA SL T4Dexmethylphenidate Extended-Release
Capsule (generic Focalin XR)*** E PA SL T4Dextroamphetamine Extended-Release
Capsule (generic Dexedrine)*** PADextroamphetamine Immediate-Release
Tablet (generic Dexedrine)*** PADyanavel XR E PA SL T4 Evekeo E PA T4 Methylphenidate HCl Chewable Tablet
(generic Methylin)*** PAMethylphenidate HCl Extended-Release
24 Hour Tablet (generic Concerta) E PA SL T4Methylphenidate HCl Sustained-Release
Tablet (generic Metadate ER, Ritalin SR)*** PA SL T4 Modafinil Tablet (generic Provigil)*** PA SLMydayis E PA SL T4 QuilliChew ER E PA SL T4 Quillivant XR E PA SL T4
Xyrem PA SL T4
ANXIOLYTICS
Tier 1Alprazolam (generic Xanax)Alprazolam Sustained-Release
24 Hour Tablet (generic Xanax XR)Buspirone HCl (generic Buspar)Chlordiazepoxide HCl (generic Librium)Diazepam (generic Valium)Lorazepam (generic Ativan)
Cardiovascular, Hypertension & Lipids
20© 2018 UnitedHealthCare Services, Inc. All rights reserved. 7/18
^ Health Care Reform drug lists may vary by plan, your patient can find the most up-to-date Tier status and cost information for a particular medication by visiting myuhc.com and/or calling the toll-free member phone number on their health care ID card.
**** Depending on your patients’ benefit and/or medication, notification or medical necessity criteria will be applied to determine if covered under the pharmacy benefit.
MC Multiple copayPA Prior authorization required****RS May be eligible for the refill and save programSL Supply limit
E May be excluded from coverageH May be part of health care reform preventive^H-PA May be part of health care reform preventive with
prior authorization^
SP Specialty medicationST Step therapyT4 May be covered on Tier 4 in selected benefits
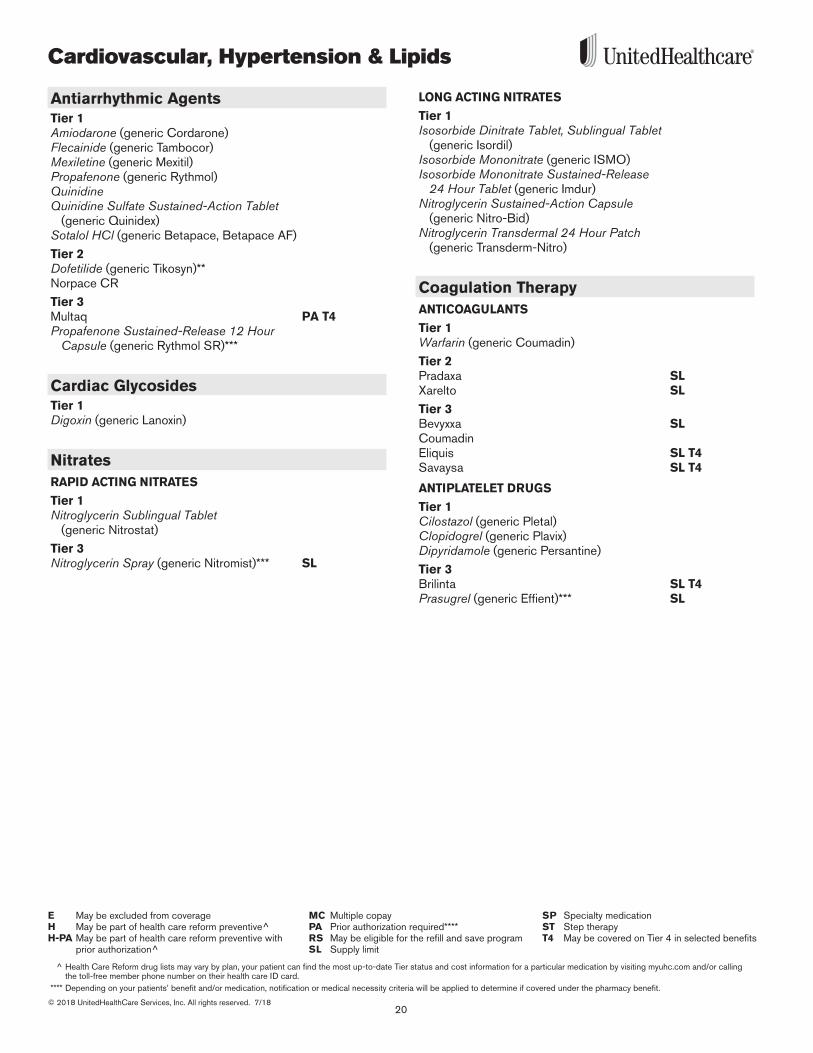
Antiarrhythmic AgentsTier 1Amiodarone (generic Cordarone)Flecainide (generic Tambocor)Mexiletine (generic Mexitil)Propafenone (generic Rythmol)QuinidineQuinidine Sulfate Sustained-Action Tablet
(generic Quinidex)Sotalol HCl (generic Betapace, Betapace AF)
Tier 2Dofetilide (generic Tikosyn)** Norpace CR
Tier 3Multaq PA T4Propafenone Sustained-Release 12 Hour
Capsule (generic Rythmol SR)***
Cardiac GlycosidesTier 1Digoxin (generic Lanoxin)
NitratesRAPID ACTING NITRATES
Tier 1Nitroglycerin Sublingual Tablet
(generic Nitrostat)
Tier 3Nitroglycerin Spray (generic Nitromist)*** SL
LONG ACTING NITRATES
Tier 1Isosorbide Dinitrate Tablet, Sublingual Tablet
(generic Isordil)Isosorbide Mononitrate (generic ISMO)Isosorbide Mononitrate Sustained-Release
24 Hour Tablet (generic Imdur)Nitroglycerin Sustained-Action Capsule
(generic Nitro-Bid)Nitroglycerin Transdermal 24 Hour Patch
(generic Transderm-Nitro)
Coagulation TherapyANTICOAGULANTS
Tier 1Warfarin (generic Coumadin)
Tier 2Pradaxa SLXarelto SL
Tier 3Bevyxxa SL CoumadinEliquis SL T4Savaysa SL T4
ANTIPLATELET DRUGS
Tier 1Cilostazol (generic Pletal)Clopidogrel (generic Plavix)Dipyridamole (generic Persantine)
Tier 3Brilinta SL T4Prasugrel (generic Effient)*** SL

21
Please refer to page 4 for a definition of notations/symbols.
* Products listed in Tier 1 may be covered in Tier 3 in a non-standard Prescription Drug List *** Products listed in Tier 3 may be covered in Tier 1 in a non-standard Prescription Drug List ** Products listed in Tier 2 may be covered in Tier 1 in a non-standard Prescription Drug List ^̂ Products listed in Tier 2 may be covered in Tier 3 in a non-standard Prescription Drug List
© 2018 UnitedHealthCare Services, Inc. All rights reserved. 7/18
Cardiovascular, Hypertension & Lipids
HEMOPHILIA AGENTS
Tier 2Alphanate vonWillebrand SPAlphanine SD SPBebulin SPBeneFix SPCoagadex SP Feiba SPHemlibra SP Hemofil-M SPHumate-P SPKoate-DVI SPKogenate FS SPKovaltry SPMonoclate-P SPMononine SPNovoeight SP Novoseven SPNuwiq SPProfilnine SD SPVonvendi SP
Tier 3Advate PA SP ST T4Adynovate E PA SP
ST T4Afstyla PA SP T4 Alprolix SP Eloctate PA SP T4Idelvion SPIxinity E PA SP
ST T4Recombinate PA SP ST T4Xyntha PA SP ST T4
HEPARIN
Tier 1Heparin (generic Heparin)
Tier 2Enoxaparin (generic Lovenox)** SLFondaparinux (generic Arixtra)** SL
VITAMIN K
Tier 2Mephyton SL
Antihypertensive TherapyTHIAZIDE & RELATED DIURETICS
Tier 1Amiloride (generic Midamor)Amiloride/Hydrochlorothiazide
(generic Moduretic)Bumetanide (generic Bumex)Chlorothiazide Tablet (generic Diuril)Furosemide (generic Lasix)Hydrochlorothiazide
(generic HydroDIURIL, Microzide)Metolazone (generic Zaroxolyn)Spironolactone (generic Aldactone)Spironolactone/Hydrochlorothiazide
(generic Aldactazide 25-25 mg)Triamterene/Hydrochlorothiazide
(generic Dyazide, Maxzide)
Tier 2Aldactazide 50-50 mgEplerenone (generic Inspra)**
BETA BLOCKERS
Tier 1Acebutolol (generic Sectral)Atenolol (generic Tenormin)Carvedilol Tablet (generic Coreg)Labetalol (generic Normodyne)Metoprolol Succinate Extended-Release
24 Hour Tablet (generic Toprol XL 25 mg)Metoprolol Tartrate 50, 100 mg (generic Lopressor)Nadolol (generic Corgard)Propranolol HCl Tablet (generic Inderal)
Tier 2BystolicMetoprolol Succinate Extended-Release
24 Hour Tablet (generic Toprol XL 50, 100, 200 mg)**
Propranolol HCl Sustained-Action Capsule (generic Inderal LA)**
Tier 3Carvedilol Phosphate Extended-Release
24 Hour Capsule (generic Coreg CR)*** E SL T4Metoprolol Tartrate 37 .5, 75 mg*** E T4
Cardiovascular, Hypertension & Lipids
22© 2018 UnitedHealthCare Services, Inc. All rights reserved. 7/18
^ Health Care Reform drug lists may vary by plan, your patient can find the most up-to-date Tier status and cost information for a particular medication by visiting myuhc.com and/or calling the toll-free member phone number on their health care ID card.
**** Depending on your patients’ benefit and/or medication, notification or medical necessity criteria will be applied to determine if covered under the pharmacy benefit.
MC Multiple copayPA Prior authorization required****RS May be eligible for the refill and save programSL Supply limit
E May be excluded from coverageH May be part of health care reform preventive^H-PA May be part of health care reform preventive with
prior authorization^
SP Specialty medicationST Step therapyT4 May be covered on Tier 4 in selected benefits
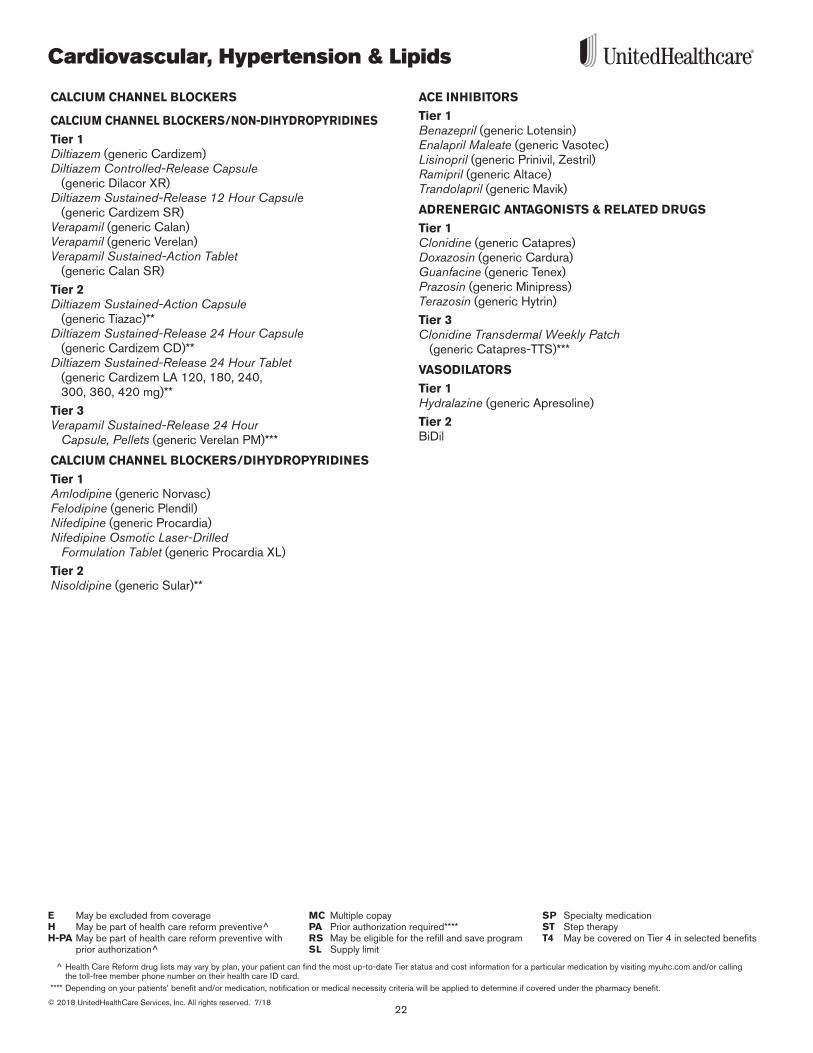
CALCIUM CHANNEL BLOCKERS
CALCIUM CHANNEL BLOCKERS/NON-DIHYDROPYRIDINES
Tier 1Diltiazem (generic Cardizem)Diltiazem Controlled-Release Capsule
(generic Dilacor XR)Diltiazem Sustained-Release 12 Hour Capsule
(generic Cardizem SR)Verapamil (generic Calan)Verapamil (generic Verelan)Verapamil Sustained-Action Tablet
(generic Calan SR)
Tier 2Diltiazem Sustained-Action Capsule
(generic Tiazac)**Diltiazem Sustained-Release 24 Hour Capsule
(generic Cardizem CD)**Diltiazem Sustained-Release 24 Hour Tablet
(generic Cardizem LA 120, 180, 240, 300, 360, 420 mg)**
Tier 3Verapamil Sustained-Release 24 Hour
Capsule, Pellets (generic Verelan PM)***
CALCIUM CHANNEL BLOCKERS/DIHYDROPYRIDINES
Tier 1Amlodipine (generic Norvasc)Felodipine (generic Plendil)Nifedipine (generic Procardia)Nifedipine Osmotic Laser-Drilled
Formulation Tablet (generic Procardia XL)
Tier 2Nisoldipine (generic Sular)**
ACE INHIBITORS
Tier 1Benazepril (generic Lotensin)Enalapril Maleate (generic Vasotec)Lisinopril (generic Prinivil, Zestril)Ramipril (generic Altace)Trandolapril (generic Mavik)
ADRENERGIC ANTAGONISTS & RELATED DRUGS
Tier 1Clonidine (generic Catapres)Doxazosin (generic Cardura)Guanfacine (generic Tenex)Prazosin (generic Minipress)Terazosin (generic Hytrin)
Tier 3Clonidine Transdermal Weekly Patch
(generic Catapres-TTS)***
VASODILATORS
Tier 1Hydralazine (generic Apresoline)
Tier 2BiDil
23
Please refer to page 4 for a definition of notations/symbols.
* Products listed in Tier 1 may be covered in Tier 3 in a non-standard Prescription Drug List *** Products listed in Tier 3 may be covered in Tier 1 in a non-standard Prescription Drug List ** Products listed in Tier 2 may be covered in Tier 1 in a non-standard Prescription Drug List ^̂ Products listed in Tier 2 may be covered in Tier 3 in a non-standard Prescription Drug List
© 2018 UnitedHealthCare Services, Inc. All rights reserved. 7/18
Cardiovascular, Hypertension & Lipids
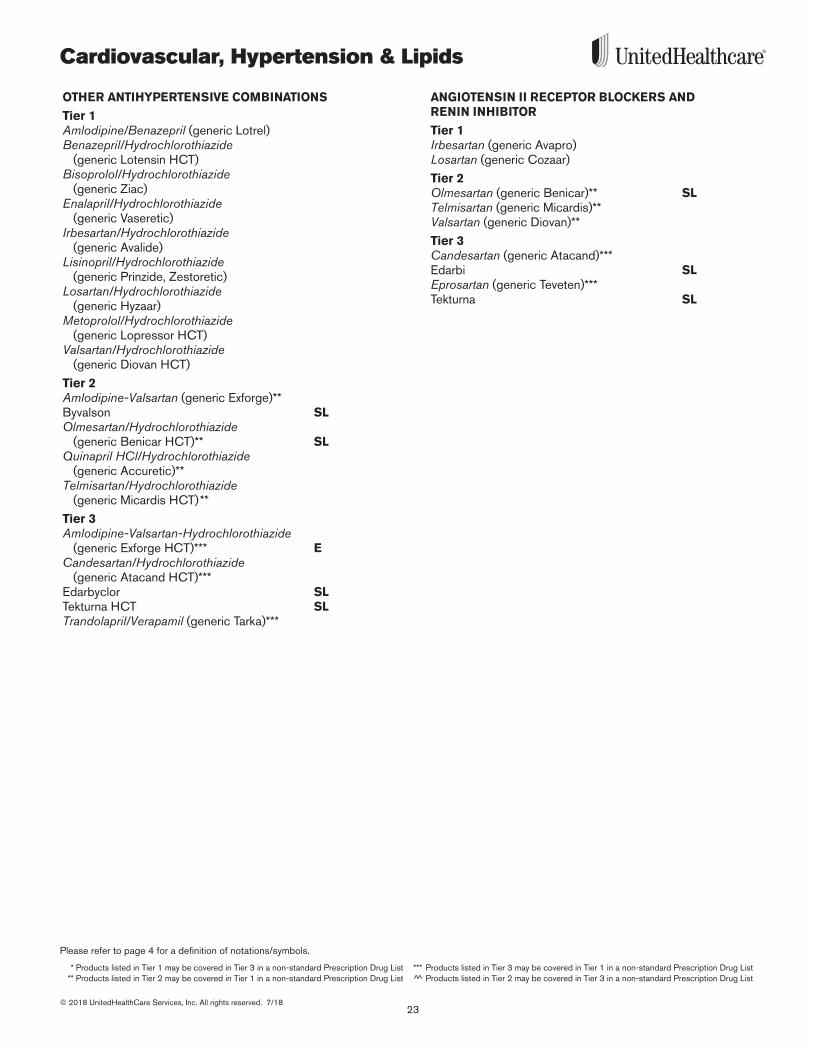
OTHER ANTIHYPERTENSIVE COMBINATIONS
Tier 1Amlodipine/Benazepril (generic Lotrel)Benazepril/Hydrochlorothiazide
(generic Lotensin HCT)Bisoprolol/Hydrochlorothiazide
(generic Ziac)Enalapril/Hydrochlorothiazide
(generic Vaseretic)Irbesartan/Hydrochlorothiazide
(generic Avalide)Lisinopril/Hydrochlorothiazide
(generic Prinzide, Zestoretic)Losartan/Hydrochlorothiazide
(generic Hyzaar)Metoprolol/Hydrochlorothiazide
(generic Lopressor HCT)Valsartan/Hydrochlorothiazide
(generic Diovan HCT)
Tier 2Amlodipine-Valsartan (generic Exforge)** Byvalson SLOlmesartan/Hydrochlorothiazide
(generic Benicar HCT)** SL Quinapril HCl/Hydrochlorothiazide
(generic Accuretic)**Telmisartan/Hydrochlorothiazide
(generic Micardis HCT)** Tier 3Amlodipine-Valsartan-Hydrochlorothiazide
(generic Exforge HCT)*** ECandesartan/Hydrochlorothiazide
(generic Atacand HCT)***Edarbyclor SLTekturna HCT SLTrandolapril/Verapamil (generic Tarka)***
ANGIOTENSIN II RECEPTOR BLOCKERS AND RENIN INHIBITOR
Tier 1Irbesartan (generic Avapro)Losartan (generic Cozaar)
Tier 2Olmesartan (generic Benicar)** SL Telmisartan (generic Micardis)**Valsartan (generic Diovan)**
Tier 3Candesartan (generic Atacand)*** Edarbi SLEprosartan (generic Teveten)***Tekturna SL
Cardiovascular, Hypertension & Lipids
24© 2018 UnitedHealthCare Services, Inc. All rights reserved. 7/18
^ Health Care Reform drug lists may vary by plan, your patient can find the most up-to-date Tier status and cost information for a particular medication by visiting myuhc.com and/or calling the toll-free member phone number on their health care ID card.
**** Depending on your patients’ benefit and/or medication, notification or medical necessity criteria will be applied to determine if covered under the pharmacy benefit.
MC Multiple copayPA Prior authorization required****RS May be eligible for the refill and save programSL Supply limit
E May be excluded from coverageH May be part of health care reform preventive^H-PA May be part of health care reform preventive with
prior authorization^
SP Specialty medicationST Step therapyT4 May be covered on Tier 4 in selected benefits
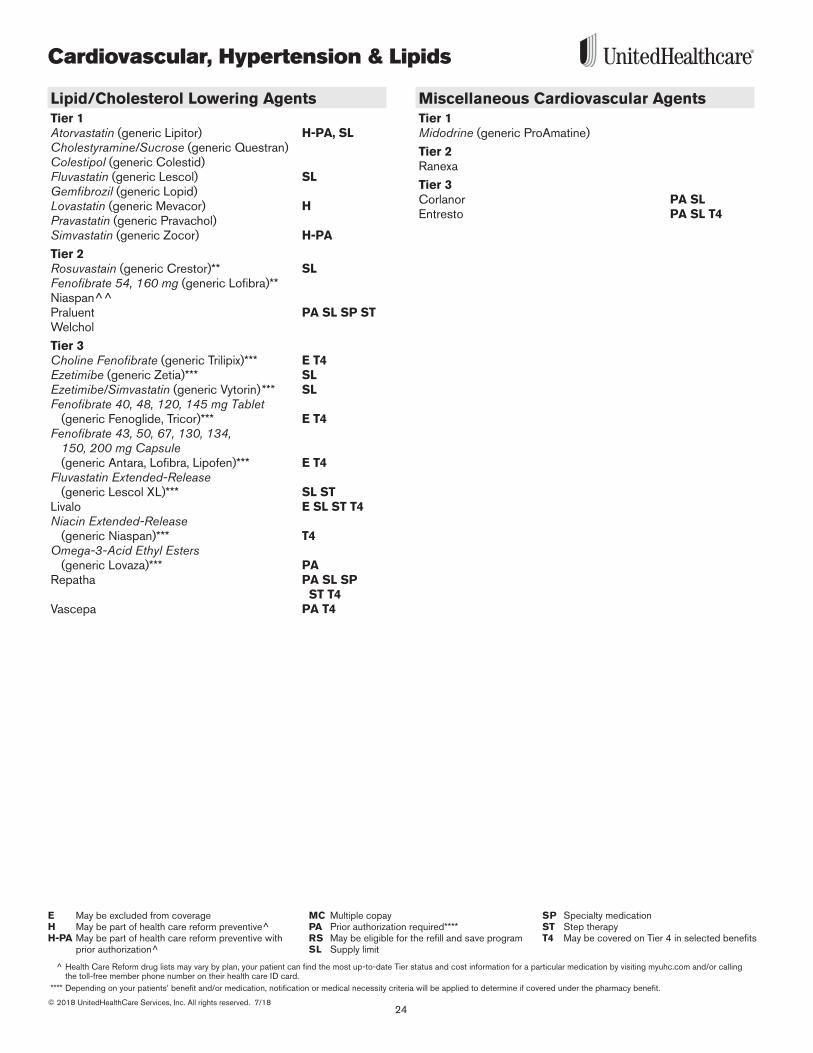
Lipid/Cholesterol Lowering AgentsTier 1Atorvastatin (generic Lipitor) H-PA, SLCholestyramine/Sucrose (generic Questran)Colestipol (generic Colestid)Fluvastatin (generic Lescol) SLGemfibrozil (generic Lopid)Lovastatin (generic Mevacor) HPravastatin (generic Pravachol) Simvastatin (generic Zocor) H-PA
Tier 2Rosuvastain (generic Crestor)** SLFenofibrate 54, 160 mg (generic Lofibra)**Niaspan^^Praluent PA SL SP ST Welchol
Tier 3Choline Fenofibrate (generic Trilipix)*** E T4 Ezetimibe (generic Zetia)*** SL Ezetimibe/Simvastatin (generic Vytorin)*** SL Fenofibrate 40, 48, 120, 145 mg Tablet
(generic Fenoglide, Tricor)*** E T4Fenofibrate 43, 50, 67, 130, 134,
150, 200 mg Capsule (generic Antara, Lofibra, Lipofen)*** E T4
Fluvastatin Extended-Release (generic Lescol XL)*** SL ST
Livalo E SL ST T4Niacin Extended-Release
(generic Niaspan)*** T4Omega-3-Acid Ethyl Esters
(generic Lovaza)*** PA Repatha PA SL SP
ST T4 Vascepa PA T4
Miscellaneous Cardiovascular AgentsTier 1Midodrine (generic ProAmatine)
Tier 2Ranexa
Tier 3Corlanor PA SL Entresto PA SL T4
25
Please refer to page 4 for a definition of notations/symbols.
* Products listed in Tier 1 may be covered in Tier 3 in a non-standard Prescription Drug List *** Products listed in Tier 3 may be covered in Tier 1 in a non-standard Prescription Drug List ** Products listed in Tier 2 may be covered in Tier 1 in a non-standard Prescription Drug List ^̂ Products listed in Tier 2 may be covered in Tier 3 in a non-standard Prescription Drug List
© 2018 UnitedHealthCare Services, Inc. All rights reserved. 7/18
Dermatologicals/Topical Therapy
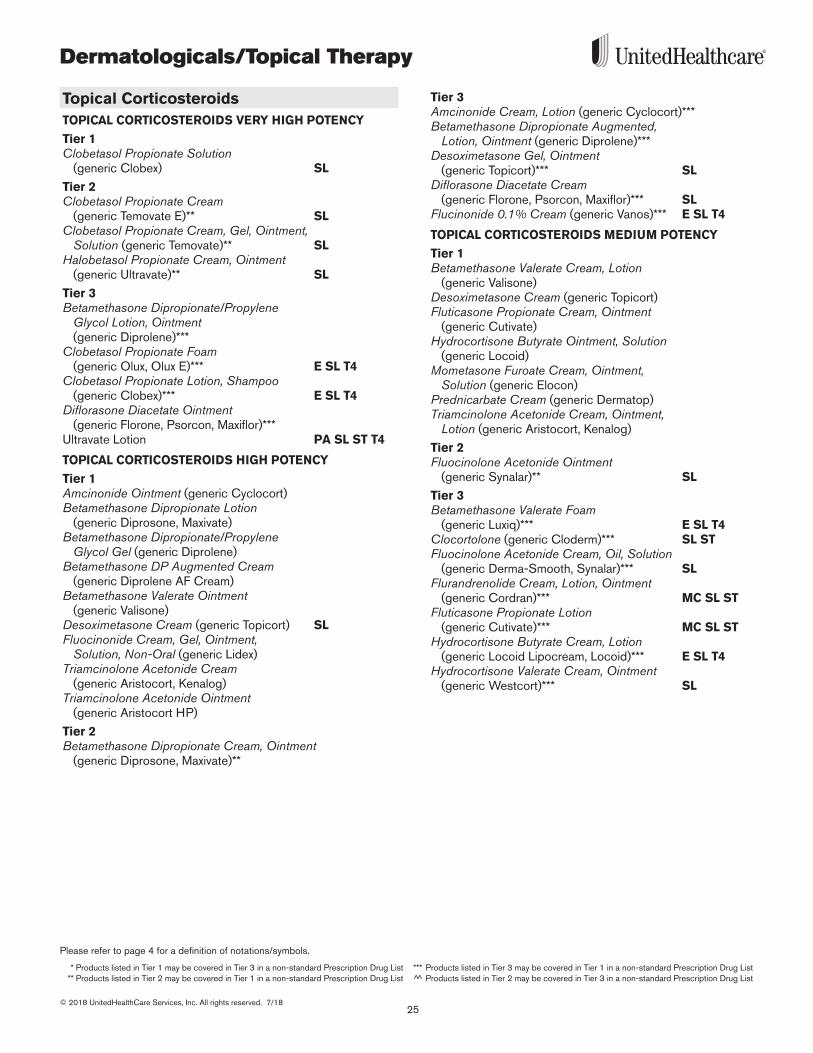
Topical CorticosteroidsTOPICAL CORTICOSTEROIDS VERY HIGH POTENCY
Tier 1Clobetasol Propionate Solution
(generic Clobex) SL
Tier 2Clobetasol Propionate Cream
(generic Temovate E)** SLClobetasol Propionate Cream, Gel, Ointment,
Solution (generic Temovate)** SLHalobetasol Propionate Cream, Ointment
(generic Ultravate)** SL
Tier 3Betamethasone Dipropionate/Propylene
Glycol Lotion, Ointment (generic Diprolene)***
Clobetasol Propionate Foam (generic Olux, Olux E)*** E SL T4
Clobetasol Propionate Lotion, Shampoo (generic Clobex)*** E SL T4
Diflorasone Diacetate Ointment (generic Florone, Psorcon, Maxiflor)***
Ultravate Lotion PA SL ST T4
TOPICAL CORTICOSTEROIDS HIGH POTENCY
Tier 1Amcinonide Ointment (generic Cyclocort) Betamethasone Dipropionate Lotion
(generic Diprosone, Maxivate)Betamethasone Dipropionate/Propylene
Glycol Gel (generic Diprolene)Betamethasone DP Augmented Cream
(generic Diprolene AF Cream)Betamethasone Valerate Ointment
(generic Valisone)Desoximetasone Cream (generic Topicort) SLFluocinonide Cream, Gel, Ointment,
Solution, Non-Oral (generic Lidex)Triamcinolone Acetonide Cream
(generic Aristocort, Kenalog)Triamcinolone Acetonide Ointment
(generic Aristocort HP)
Tier 2Betamethasone Dipropionate Cream, Ointment
(generic Diprosone, Maxivate)**
Tier 3Amcinonide Cream, Lotion (generic Cyclocort)***Betamethasone Dipropionate Augmented,
Lotion, Ointment (generic Diprolene)***Desoximetasone Gel, Ointment
(generic Topicort)*** SLDiflorasone Diacetate Cream
(generic Florone, Psorcon, Maxiflor)*** SLFlucinonide 0.1% Cream (generic Vanos)*** E SL T4
TOPICAL CORTICOSTEROIDS MEDIUM POTENCY
Tier 1Betamethasone Valerate Cream, Lotion
(generic Valisone)Desoximetasone Cream (generic Topicort)Fluticasone Propionate Cream, Ointment
(generic Cutivate)Hydrocortisone Butyrate Ointment, Solution
(generic Locoid)Mometasone Furoate Cream, Ointment,
Solution (generic Elocon)Prednicarbate Cream (generic Dermatop)Triamcinolone Acetonide Cream, Ointment,
Lotion (generic Aristocort, Kenalog)
Tier 2Fluocinolone Acetonide Ointment
(generic Synalar)** SL
Tier 3Betamethasone Valerate Foam
(generic Luxiq)*** E SL T4Clocortolone (generic Cloderm)*** SL STFluocinolone Acetonide Cream, Oil, Solution
(generic Derma-Smooth, Synalar)*** SLFlurandrenolide Cream, Lotion, Ointment
(generic Cordran)*** MC SL ST Fluticasone Propionate Lotion
(generic Cutivate)*** MC SL STHydrocortisone Butyrate Cream, Lotion
(generic Locoid Lipocream, Locoid)*** E SL T4Hydrocortisone Valerate Cream, Ointment
(generic Westcort)*** SL
Dermatologicals/Topical Therapy
26© 2018 UnitedHealthCare Services, Inc. All rights reserved. 7/18
^ Health Care Reform drug lists may vary by plan, your patient can find the most up-to-date Tier status and cost information for a particular medication by visiting myuhc.com and/or calling the toll-free member phone number on their health care ID card.
**** Depending on your patients’ benefit and/or medication, notification or medical necessity criteria will be applied to determine if covered under the pharmacy benefit.
MC Multiple copayPA Prior authorization required****RS May be eligible for the refill and save programSL Supply limit
E May be excluded from coverageH May be part of health care reform preventive^H-PA May be part of health care reform preventive with
prior authorization^
SP Specialty medicationST Step therapyT4 May be covered on Tier 4 in selected benefits
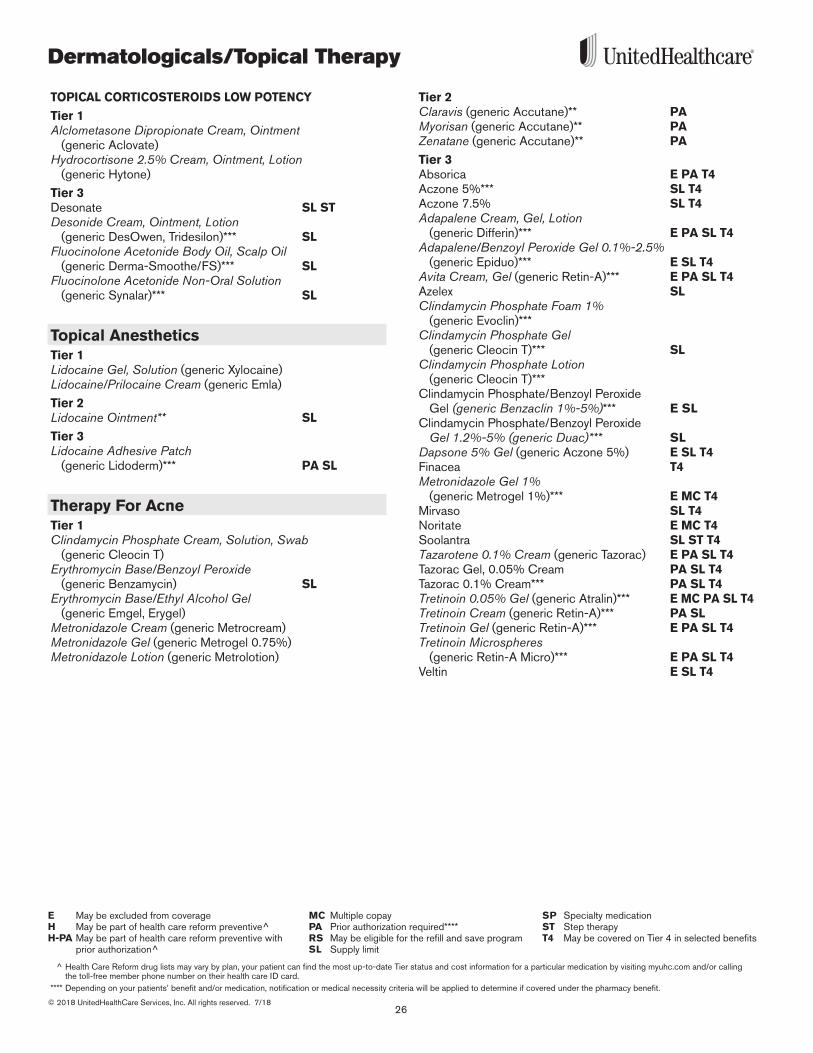
TOPICAL CORTICOSTEROIDS LOW POTENCY
Tier 1Alclometasone Dipropionate Cream, Ointment
(generic Aclovate)Hydrocortisone 2.5% Cream, Ointment, Lotion
(generic Hytone)
Tier 3Desonate SL STDesonide Cream, Ointment, Lotion
(generic DesOwen, Tridesilon)*** SLFluocinolone Acetonide Body Oil, Scalp Oil
(generic Derma-Smoothe/FS)*** SLFluocinolone Acetonide Non-Oral Solution
(generic Synalar)*** SL
Topical AnestheticsTier 1Lidocaine Gel, Solution (generic Xylocaine)Lidocaine/Prilocaine Cream (generic Emla)
Tier 2Lidocaine Ointment** SL
Tier 3Lidocaine Adhesive Patch
(generic Lidoderm)*** PA SL
Therapy For AcneTier 1Clindamycin Phosphate Cream, Solution, Swab
(generic Cleocin T)Erythromycin Base/Benzoyl Peroxide
(generic Benzamycin) SLErythromycin Base/Ethyl Alcohol Gel
(generic Emgel, Erygel)Metronidazole Cream (generic Metrocream)Metronidazole Gel (generic Metrogel 0 .75%)Metronidazole Lotion (generic Metrolotion)
Tier 2Claravis (generic Accutane)** PAMyorisan (generic Accutane)** PAZenatane (generic Accutane)** PA
Tier 3Absorica E PA T4Aczone 5%*** SL T4Aczone 7 .5% SL T4Adapalene Cream, Gel, Lotion
(generic Differin)*** E PA SL T4Adapalene/Benzoyl Peroxide Gel 0.1%-2.5%
(generic Epiduo)*** E SL T4 Avita Cream, Gel (generic Retin-A)*** E PA SL T4 Azelex SLClindamycin Phosphate Foam 1%
(generic Evoclin)***Clindamycin Phosphate Gel
(generic Cleocin T)*** SLClindamycin Phosphate Lotion
(generic Cleocin T)***Clindamycin Phosphate/Benzoyl Peroxide
Gel (generic Benzaclin 1%-5%)*** E SLClindamycin Phosphate/Benzoyl Peroxide
Gel 1.2%-5% (generic Duac)*** SLDapsone 5% Gel (generic Aczone 5%) E SL T4 Finacea T4Metronidazole Gel 1%
(generic Metrogel 1%)*** E MC T4Mirvaso SL T4Noritate E MC T4Soolantra SL ST T4 Tazarotene 0.1% Cream (generic Tazorac) E PA SL T4Tazorac Gel, 0 .05% Cream PA SL T4Tazorac 0 .1% Cream*** PA SL T4Tretinoin 0.05% Gel (generic Atralin)*** E MC PA SL T4Tretinoin Cream (generic Retin-A)*** PA SL Tretinoin Gel (generic Retin-A)*** E PA SL T4 Tretinoin Microspheres
(generic Retin-A Micro)*** E PA SL T4Veltin E SL T4
27
Please refer to page 4 for a definition of notations/symbols.
* Products listed in Tier 1 may be covered in Tier 3 in a non-standard Prescription Drug List *** Products listed in Tier 3 may be covered in Tier 1 in a non-standard Prescription Drug List ** Products listed in Tier 2 may be covered in Tier 1 in a non-standard Prescription Drug List ^̂ Products listed in Tier 2 may be covered in Tier 3 in a non-standard Prescription Drug List
© 2018 UnitedHealthCare Services, Inc. All rights reserved. 7/18
Dermatologicals/Topical Therapy
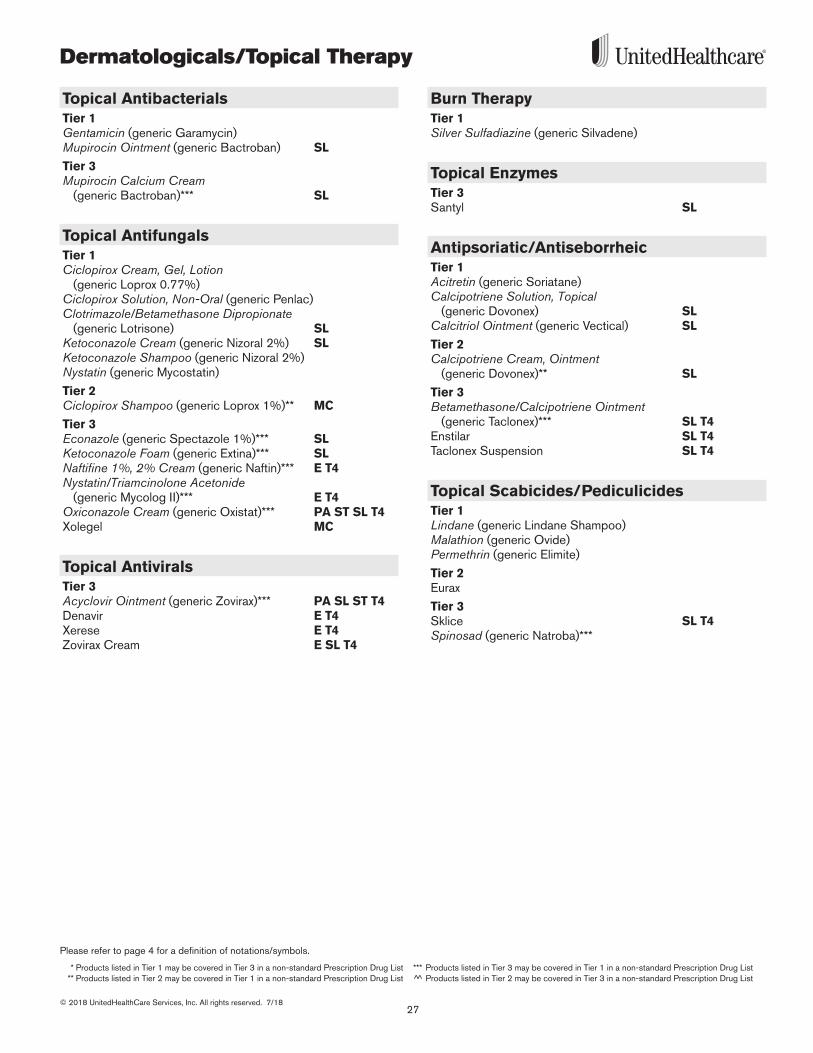
Topical AntibacterialsTier 1Gentamicin (generic Garamycin)Mupirocin Ointment (generic Bactroban) SL
Tier 3Mupirocin Calcium Cream
(generic Bactroban)*** SL
Topical AntifungalsTier 1Ciclopirox Cream, Gel, Lotion
(generic Loprox 0 .77%) Ciclopirox Solution, Non-Oral (generic Penlac)Clotrimazole/Betamethasone Dipropionate
(generic Lotrisone) SLKetoconazole Cream (generic Nizoral 2%) SLKetoconazole Shampoo (generic Nizoral 2%) Nystatin (generic Mycostatin)
Tier 2Ciclopirox Shampoo (generic Loprox 1%)** MC
Tier 3Econazole (generic Spectazole 1%)*** SL Ketoconazole Foam (generic Extina)*** SLNaftifine 1%, 2% Cream (generic Naftin)*** E T4 Nystatin/Triamcinolone Acetonide
(generic Mycolog II)*** E T4Oxiconazole Cream (generic Oxistat)*** PA ST SL T4Xolegel MC
Topical AntiviralsTier 3Acyclovir Ointment (generic Zovirax)*** PA SL ST T4Denavir E T4Xerese E T4Zovirax Cream E SL T4
Burn TherapyTier 1Silver Sulfadiazine (generic Silvadene)
Topical EnzymesTier 3Santyl SL
Antipsoriatic/AntiseborrheicTier 1Acitretin (generic Soriatane) Calcipotriene Solution, Topical
(generic Dovonex) SLCalcitriol Ointment (generic Vectical) SL
Tier 2Calcipotriene Cream, Ointment
(generic Dovonex)** SL
Tier 3Betamethasone/Calcipotriene Ointment
(generic Taclonex)*** SL T4Enstilar SL T4Taclonex Suspension SL T4
Topical Scabicides/PediculicidesTier 1Lindane (generic Lindane Shampoo)Malathion (generic Ovide)Permethrin (generic Elimite)
Tier 2Eurax
Tier 3Sklice SL T4 Spinosad (generic Natroba)***

Dermatologicals/Topical Therapy
28© 2018 UnitedHealthCare Services, Inc. All rights reserved. 7/18
^ Health Care Reform drug lists may vary by plan, your patient can find the most up-to-date Tier status and cost information for a particular medication by visiting myuhc.com and/or calling the toll-free member phone number on their health care ID card.
**** Depending on your patients’ benefit and/or medication, notification or medical necessity criteria will be applied to determine if covered under the pharmacy benefit.
MC Multiple copayPA Prior authorization required****RS May be eligible for the refill and save programSL Supply limit
E May be excluded from coverageH May be part of health care reform preventive^H-PA May be part of health care reform preventive with
prior authorization^
SP Specialty medicationST Step therapyT4 May be covered on Tier 4 in selected benefits
Miscellaneous DermatologicalsTier 1Fluorouracil 5% Cream (generic Efudex)Imiquimod (generic Aldara) SLPodofilox Liquid (generic Condylox Liquid)Urea 40% Emulsion (generic Umecta)
Tier 2Carac Oxsoralen-UltraRegranex PA SLTacrolimus (generic Protopic)** SL ST
Tier 3Condylox Gel Diclofenac 3% Gel (generic Solaraze)*** PA SLDupixent PA SL SP
ST T4Elidel SL STEucrisa SL ST Fluoroplex T4 Fluorouracil 0 .5% Cream (generic Carac) T4 Picato SLRhofade PA SL T4
29
Please refer to page 4 for a definition of notations/symbols.
* Products listed in Tier 1 may be covered in Tier 3 in a non-standard Prescription Drug List *** Products listed in Tier 3 may be covered in Tier 1 in a non-standard Prescription Drug List ** Products listed in Tier 2 may be covered in Tier 1 in a non-standard Prescription Drug List ^̂ Products listed in Tier 2 may be covered in Tier 3 in a non-standard Prescription Drug List
© 2018 UnitedHealthCare Services, Inc. All rights reserved. 7/18
Ear, Nose & Throat Medications
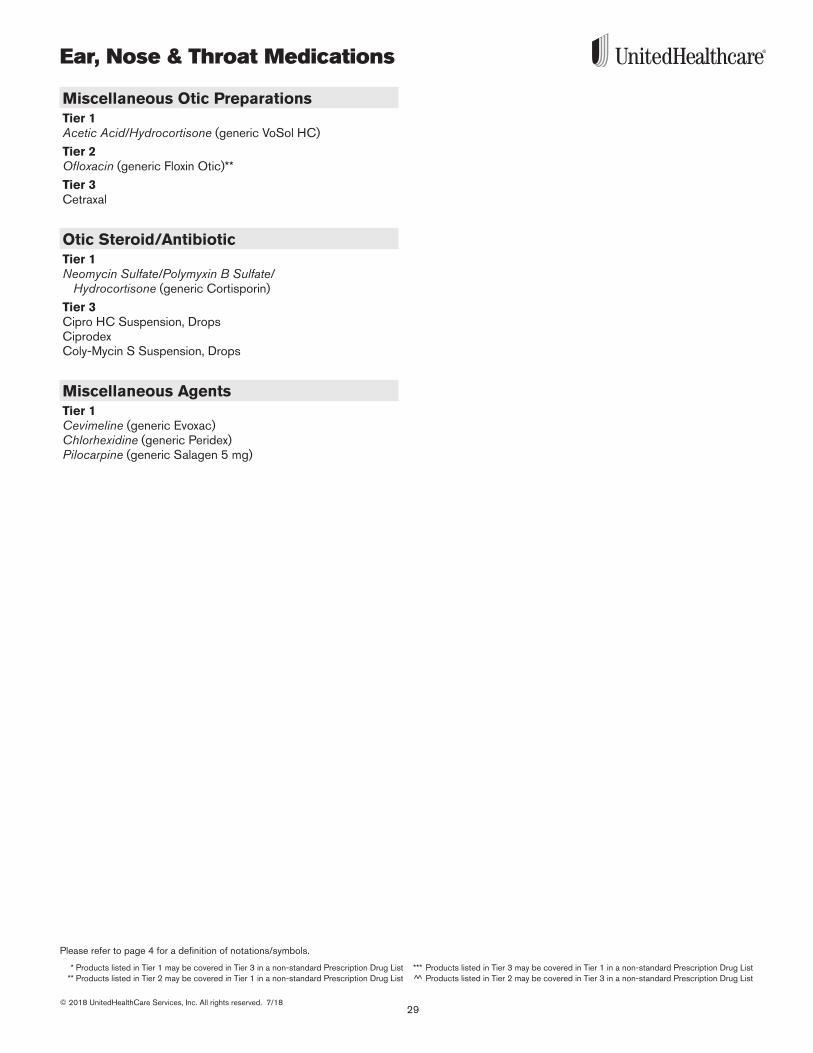
Miscellaneous Otic PreparationsTier 1Acetic Acid/Hydrocortisone (generic VoSol HC)
Tier 2Ofloxacin (generic Floxin Otic)**
Tier 3Cetraxal
Otic Steroid/AntibioticTier 1Neomycin Sulfate/Polymyxin B Sulfate/
Hydrocortisone (generic Cortisporin)
Tier 3Cipro HC Suspension, DropsCiprodex Coly-Mycin S Suspension, Drops
Miscellaneous AgentsTier 1Cevimeline (generic Evoxac)Chlorhexidine (generic Peridex)Pilocarpine (generic Salagen 5 mg)
Endocrine/Diabetes
30© 2018 UnitedHealthCare Services, Inc. All rights reserved. 7/18
^ Health Care Reform drug lists may vary by plan, your patient can find the most up-to-date Tier status and cost information for a particular medication by visiting myuhc.com and/or calling the toll-free member phone number on their health care ID card.
**** Depending on your patients’ benefit and/or medication, notification or medical necessity criteria will be applied to determine if covered under the pharmacy benefit.
MC Multiple copayPA Prior authorization required****RS May be eligible for the refill and save programSL Supply limit
E May be excluded from coverageH May be part of health care reform preventive^H-PA May be part of health care reform preventive with
prior authorization^
SP Specialty medicationST Step therapyT4 May be covered on Tier 4 in selected benefits
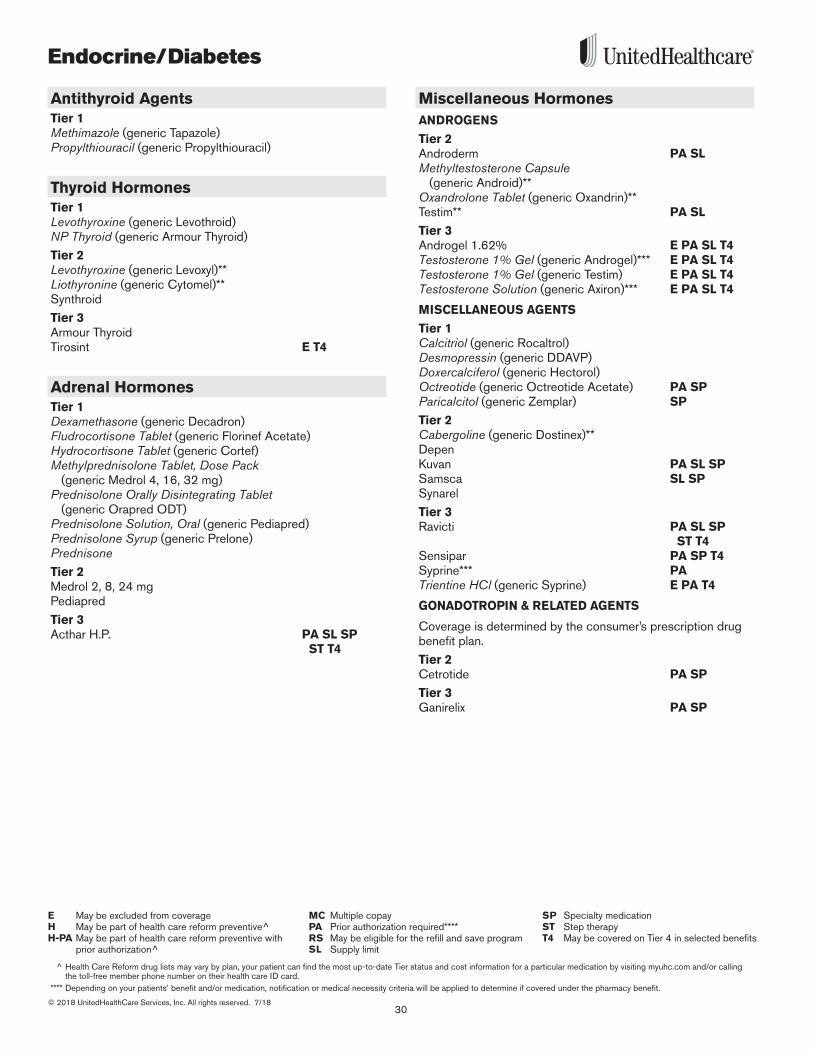
Antithyroid AgentsTier 1Methimazole (generic Tapazole)Propylthiouracil (generic Propylthiouracil)
Thyroid HormonesTier 1Levothyroxine (generic Levothroid)NP Thyroid (generic Armour Thyroid)
Tier 2Levothyroxine (generic Levoxyl)**Liothyronine (generic Cytomel)**Synthroid
Tier 3Armour Thyroid Tirosint E T4
Adrenal HormonesTier 1Dexamethasone (generic Decadron)Fludrocortisone Tablet (generic Florinef Acetate)Hydrocortisone Tablet (generic Cortef)Methylprednisolone Tablet, Dose Pack
(generic Medrol 4, 16, 32 mg)Prednisolone Orally Disintegrating Tablet
(generic Orapred ODT)Prednisolone Solution, Oral (generic Pediapred)Prednisolone Syrup (generic Prelone)PrednisoneTier 2Medrol 2, 8, 24 mgPediapred
Tier 3Acthar H .P . PA SL SP
ST T4
Miscellaneous HormonesANDROGENS
Tier 2Androderm PA SLMethyltestosterone Capsule
(generic Android)**Oxandrolone Tablet (generic Oxandrin)**Testim** PA SL
Tier 3Androgel 1 .62% E PA SL T4Testosterone 1% Gel (generic Androgel)*** E PA SL T4 Testosterone 1% Gel (generic Testim) E PA SL T4Testosterone Solution (generic Axiron)*** E PA SL T4
MISCELLANEOUS AGENTS
Tier 1Calcitriol (generic Rocaltrol)Desmopressin (generic DDAVP)Doxercalciferol (generic Hectorol)Octreotide (generic Octreotide Acetate) PA SPParicalcitol (generic Zemplar) SP
Tier 2Cabergoline (generic Dostinex)**DepenKuvan PA SL SPSamsca SL SP Synarel
Tier 3Ravicti PA SL SP
ST T4Sensipar PA SP T4Syprine*** PATrientine HCl (generic Syprine) E PA T4
GONADOTROPIN & RELATED AGENTS
Coverage is determined by the consumer’s prescription drug benefit plan .
Tier 2Cetrotide PA SP
Tier 3Ganirelix PA SP
31
Please refer to page 4 for a definition of notations/symbols.
* Products listed in Tier 1 may be covered in Tier 3 in a non-standard Prescription Drug List *** Products listed in Tier 3 may be covered in Tier 1 in a non-standard Prescription Drug List ** Products listed in Tier 2 may be covered in Tier 1 in a non-standard Prescription Drug List ^̂ Products listed in Tier 2 may be covered in Tier 3 in a non-standard Prescription Drug List
© 2018 UnitedHealthCare Services, Inc. All rights reserved. 7/18
Endocrine/Diabetes
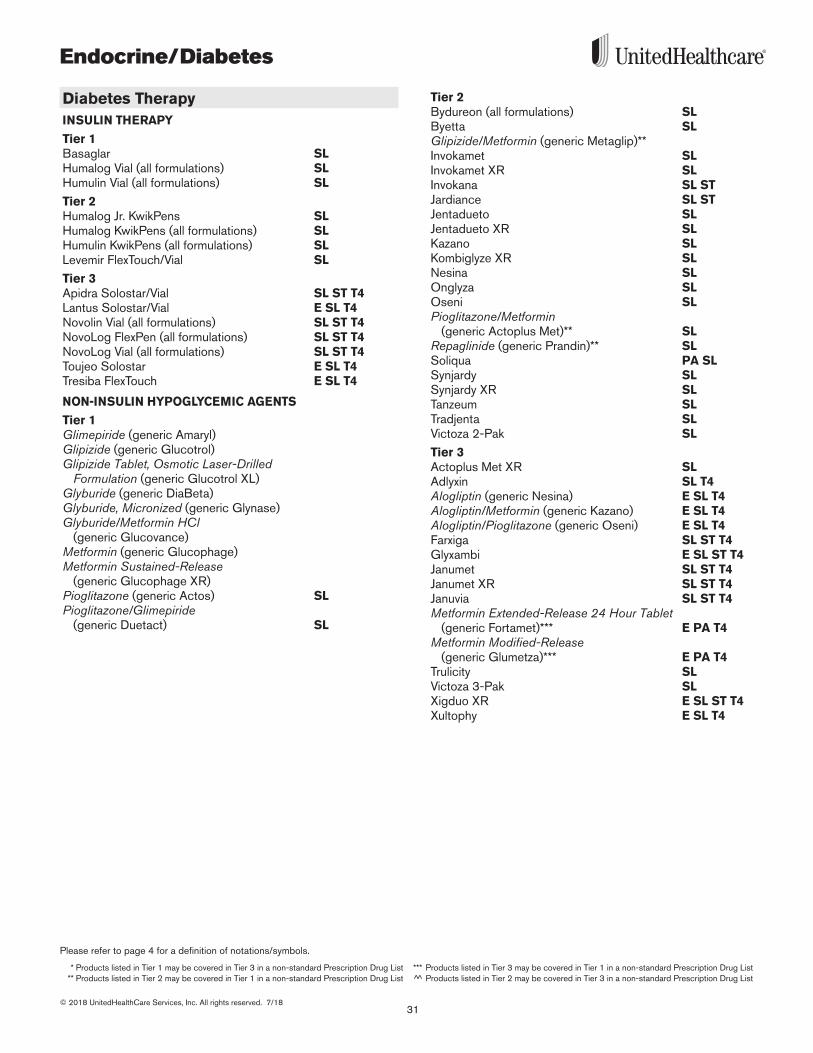
Diabetes TherapyINSULIN THERAPY
Tier 1Basaglar SLHumalog Vial (all formulations) SLHumulin Vial (all formulations) SL
Tier 2Humalog Jr . KwikPens SL Humalog KwikPens (all formulations) SLHumulin KwikPens (all formulations) SLLevemir FlexTouch/Vial SL
Tier 3Apidra Solostar/Vial SL ST T4Lantus Solostar/Vial E SL T4Novolin Vial (all formulations) SL ST T4NovoLog FlexPen (all formulations) SL ST T4NovoLog Vial (all formulations) SL ST T4Toujeo Solostar E SL T4Tresiba FlexTouch E SL T4
NON-INSULIN HYPOGLYCEMIC AGENTS
Tier 1Glimepiride (generic Amaryl)Glipizide (generic Glucotrol)Glipizide Tablet, Osmotic Laser-Drilled
Formulation (generic Glucotrol XL)Glyburide (generic DiaBeta)Glyburide, Micronized (generic Glynase)Glyburide/Metformin HCl
(generic Glucovance)Metformin (generic Glucophage)Metformin Sustained-Release
(generic Glucophage XR)Pioglitazone (generic Actos) SLPioglitazone/Glimepiride
(generic Duetact) SL
Tier 2Bydureon (all formulations) SLByetta SLGlipizide/Metformin (generic Metaglip)**Invokamet SLInvokamet XR SL Invokana SL STJardiance SL STJentadueto SLJentadueto XR SLKazano SLKombiglyze XR SLNesina SLOnglyza SLOseni SLPioglitazone/Metformin
(generic Actoplus Met)** SLRepaglinide (generic Prandin)** SLSoliqua PA SLSynjardy SL Synjardy XR SL Tanzeum SLTradjenta SLVictoza 2-Pak SL
Tier 3Actoplus Met XR SLAdlyxin SL T4Alogliptin (generic Nesina) E SL T4Alogliptin/Metformin (generic Kazano) E SL T4Alogliptin/Pioglitazone (generic Oseni) E SL T4 Farxiga SL ST T4Glyxambi E SL ST T4 Janumet SL ST T4Janumet XR SL ST T4Januvia SL ST T4Metformin Extended-Release 24 Hour Tablet
(generic Fortamet)*** E PA T4Metformin Modified-Release
(generic Glumetza)*** E PA T4Trulicity SLVictoza 3-Pak SLXigduo XR E SL ST T4Xultophy E SL T4
Endocrine/Diabetes
32© 2018 UnitedHealthCare Services, Inc. All rights reserved. 7/18
^ Health Care Reform drug lists may vary by plan, your patient can find the most up-to-date Tier status and cost information for a particular medication by visiting myuhc.com and/or calling the toll-free member phone number on their health care ID card.
**** Depending on your patients’ benefit and/or medication, notification or medical necessity criteria will be applied to determine if covered under the pharmacy benefit.
MC Multiple copayPA Prior authorization required****RS May be eligible for the refill and save programSL Supply limit
E May be excluded from coverageH May be part of health care reform preventive^H-PA May be part of health care reform preventive with
prior authorization^
SP Specialty medicationST Step therapyT4 May be covered on Tier 4 in selected benefits
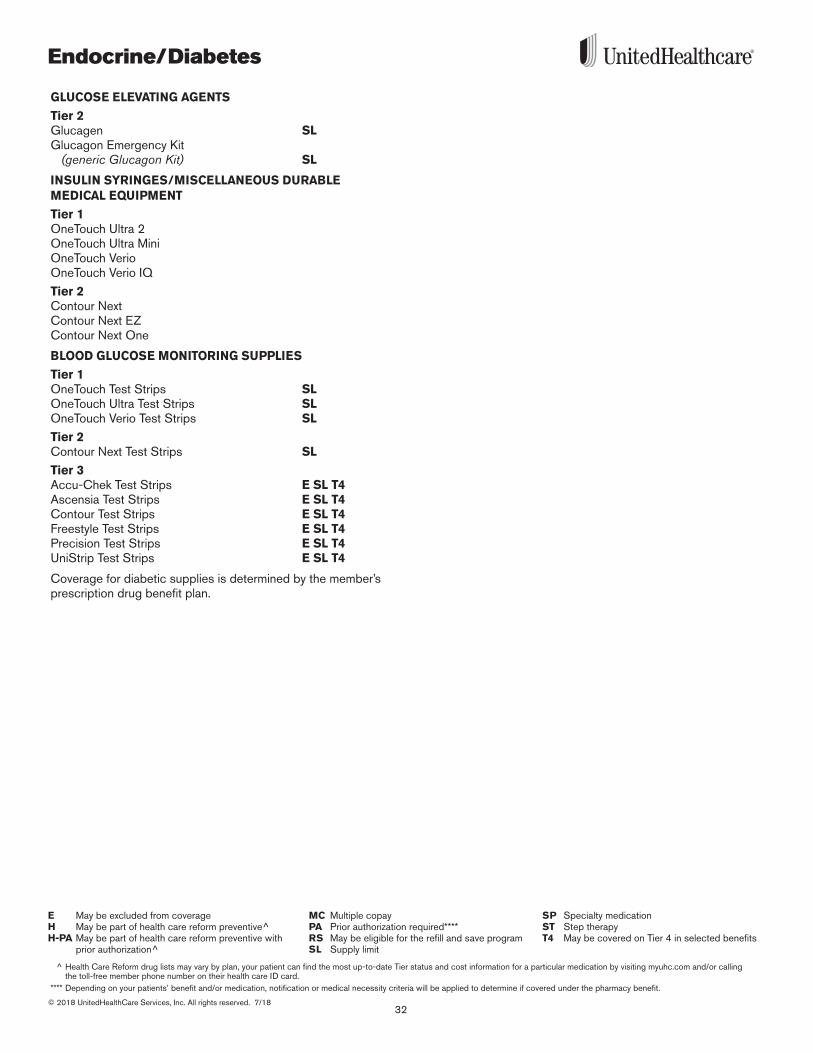
GLUCOSE ELEVATING AGENTS
Tier 2Glucagen SLGlucagon Emergency Kit
(generic Glucagon Kit) SL
INSULIN SYRINGES/MISCELLANEOUS DURABLE MEDICAL EQUIPMENT
Tier 1OneTouch Ultra 2OneTouch Ultra MiniOneTouch Verio OneTouch Verio IQ
Tier 2Contour NextContour Next EZContour Next One
BLOOD GLUCOSE MONITORING SUPPLIES
Tier 1OneTouch Test Strips SLOneTouch Ultra Test Strips SLOneTouch Verio Test Strips SL
Tier 2Contour Next Test Strips SL
Tier 3Accu-Chek Test Strips E SL T4Ascensia Test Strips E SL T4Contour Test Strips E SL T4Freestyle Test Strips E SL T4Precision Test Strips E SL T4UniStrip Test Strips E SL T4
Coverage for diabetic supplies is determined by the member’s prescription drug benefit plan .
33
Please refer to page 4 for a definition of notations/symbols.
* Products listed in Tier 1 may be covered in Tier 3 in a non-standard Prescription Drug List *** Products listed in Tier 3 may be covered in Tier 1 in a non-standard Prescription Drug List ** Products listed in Tier 2 may be covered in Tier 1 in a non-standard Prescription Drug List ^̂ Products listed in Tier 2 may be covered in Tier 3 in a non-standard Prescription Drug List
© 2018 UnitedHealthCare Services, Inc. All rights reserved. 7/18
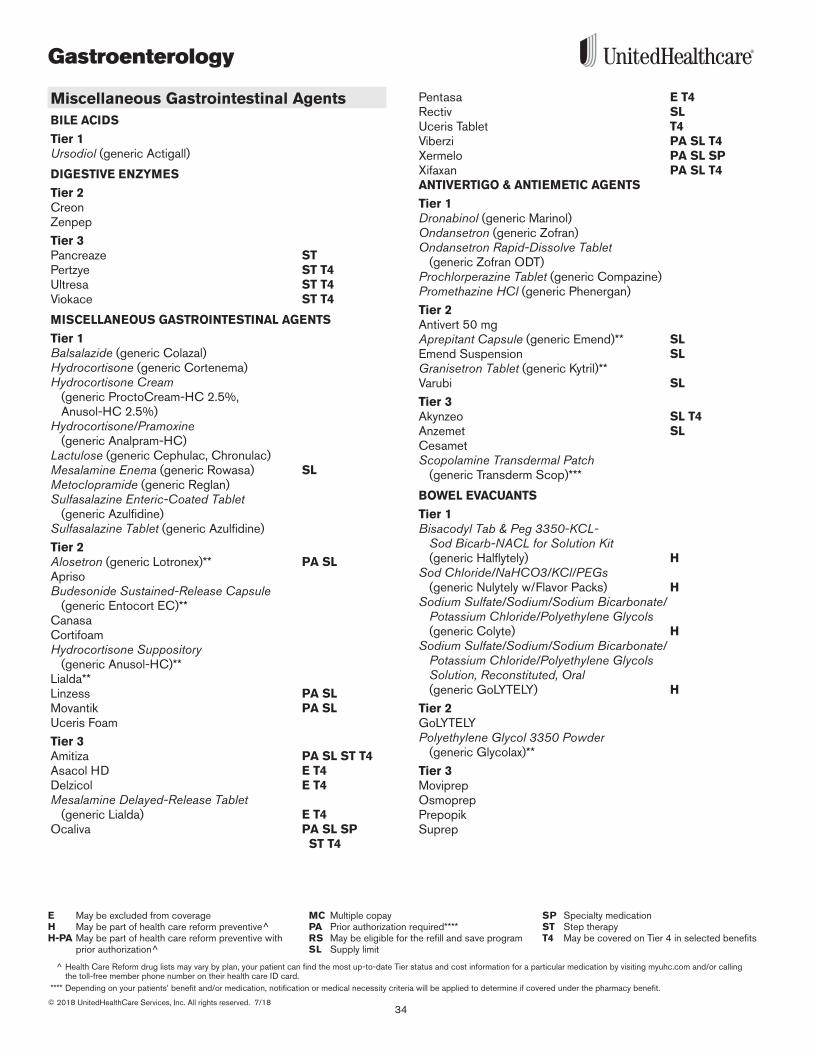
Gastroenterology
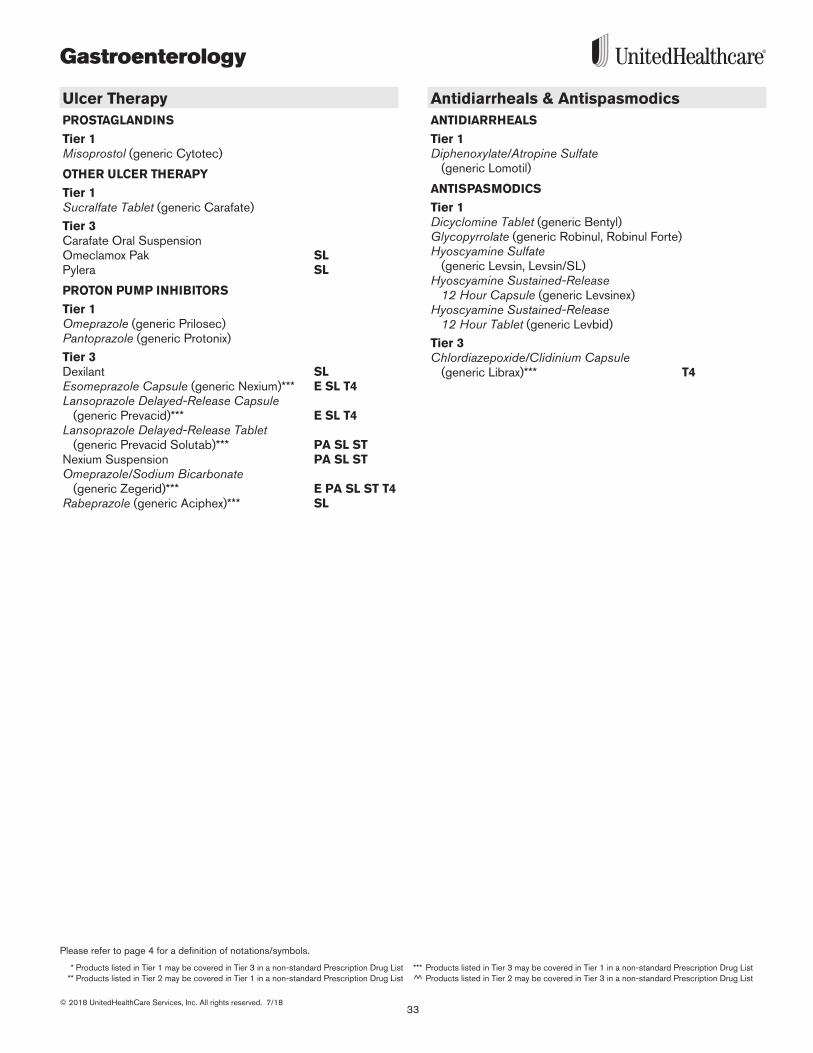
Ulcer TherapyPROSTAGLANDINS
Tier 1Misoprostol (generic Cytotec)
OTHER ULCER THERAPY
Tier 1Sucralfate Tablet (generic Carafate)
Tier 3Carafate Oral SuspensionOmeclamox Pak SLPylera SL
PROTON PUMP INHIBITORS
Tier 1Omeprazole (generic Prilosec)Pantoprazole (generic Protonix)
Tier 3Dexilant SLEsomeprazole Capsule (generic Nexium)*** E SL T4Lansoprazole Delayed-Release Capsule
(generic Prevacid)*** E SL T4Lansoprazole Delayed-Release Tablet
(generic Prevacid Solutab)*** PA SL ST Nexium Suspension PA SL STOmeprazole/Sodium Bicarbonate
(generic Zegerid)*** E PA SL ST T4Rabeprazole (generic Aciphex)*** SL
Antidiarrheals & AntispasmodicsANTIDIARRHEALS
Tier 1Diphenoxylate/Atropine Sulfate
(generic Lomotil)
ANTISPASMODICS
Tier 1Dicyclomine Tablet (generic Bentyl)Glycopyrrolate (generic Robinul, Robinul Forte)Hyoscyamine Sulfate
(generic Levsin, Levsin/SL)Hyoscyamine Sustained-Release
12 Hour Capsule (generic Levsinex)Hyoscyamine Sustained-Release
12 Hour Tablet (generic Levbid)
Tier 3Chlordiazepoxide/Clidinium Capsule
(generic Librax)*** T4
Gastroenterology
34© 2018 UnitedHealthCare Services, Inc. All rights reserved. 7/18
^ Health Care Reform drug lists may vary by plan, your patient can find the most up-to-date Tier status and cost information for a particular medication by visiting myuhc.com and/or calling the toll-free member phone number on their health care ID card.
**** Depending on your patients’ benefit and/or medication, notification or medical necessity criteria will be applied to determine if covered under the pharmacy benefit.
MC Multiple copayPA Prior authorization required****RS May be eligible for the refill and save programSL Supply limit
E May be excluded from coverageH May be part of health care reform preventive^H-PA May be part of health care reform preventive with
prior authorization^
SP Specialty medicationST Step therapyT4 May be covered on Tier 4 in selected benefits
Miscellaneous Gastrointestinal AgentsBILE ACIDS
Tier 1Ursodiol (generic Actigall)
DIGESTIVE ENZYMES
Tier 2CreonZenpep
Tier 3Pancreaze STPertzye ST T4Ultresa ST T4Viokace ST T4
MISCELLANEOUS GASTROINTESTINAL AGENTS
Tier 1Balsalazide (generic Colazal)Hydrocortisone (generic Cortenema)Hydrocortisone Cream
(generic ProctoCream-HC 2 .5%, Anusol-HC 2 .5%)
Hydrocortisone/Pramoxine (generic Analpram-HC)
Lactulose (generic Cephulac, Chronulac)Mesalamine Enema (generic Rowasa) SLMetoclopramide (generic Reglan)Sulfasalazine Enteric-Coated Tablet
(generic Azulfidine)Sulfasalazine Tablet (generic Azulfidine)
Tier 2Alosetron (generic Lotronex)** PA SLAprisoBudesonide Sustained-Release Capsule
(generic Entocort EC)**CanasaCortifoamHydrocortisone Suppository
(generic Anusol-HC)** Lialda**Linzess PA SLMovantik PA SLUceris Foam
Tier 3Amitiza PA SL ST T4Asacol HD E T4Delzicol E T4Mesalamine Delayed-Release Tablet
(generic Lialda) E T4Ocaliva PA SL SP
ST T4
Pentasa E T4Rectiv SLUceris Tablet T4Viberzi PA SL T4Xermelo PA SL SPXifaxan PA SL T4ANTIVERTIGO & ANTIEMETIC AGENTS
Tier 1Dronabinol (generic Marinol)Ondansetron (generic Zofran)Ondansetron Rapid-Dissolve Tablet
(generic Zofran ODT)Prochlorperazine Tablet (generic Compazine)Promethazine HCl (generic Phenergan)
Tier 2Antivert 50 mgAprepitant Capsule (generic Emend)** SL Emend Suspension SLGranisetron Tablet (generic Kytril)**Varubi SL
Tier 3Akynzeo SL T4 Anzemet SLCesamet Scopolamine Transdermal Patch
(generic Transderm Scop)***
BOWEL EVACUANTS
Tier 1Bisacodyl Tab & Peg 3350-KCL-
Sod Bicarb-NACL for Solution Kit (generic Halflytely) H
Sod Chloride/NaHCO3/KCl/PEGs (generic Nulytely w/Flavor Packs) H
Sodium Sulfate/Sodium/Sodium Bicarbonate/ Potassium Chloride/Polyethylene Glycols (generic Colyte) H
Sodium Sulfate/Sodium/Sodium Bicarbonate/ Potassium Chloride/Polyethylene Glycols Solution, Reconstituted, Oral (generic GoLYTELY) H
Tier 2GoLYTELYPolyethylene Glycol 3350 Powder
(generic Glycolax)**
Tier 3MoviprepOsmoprep PrepopikSuprep
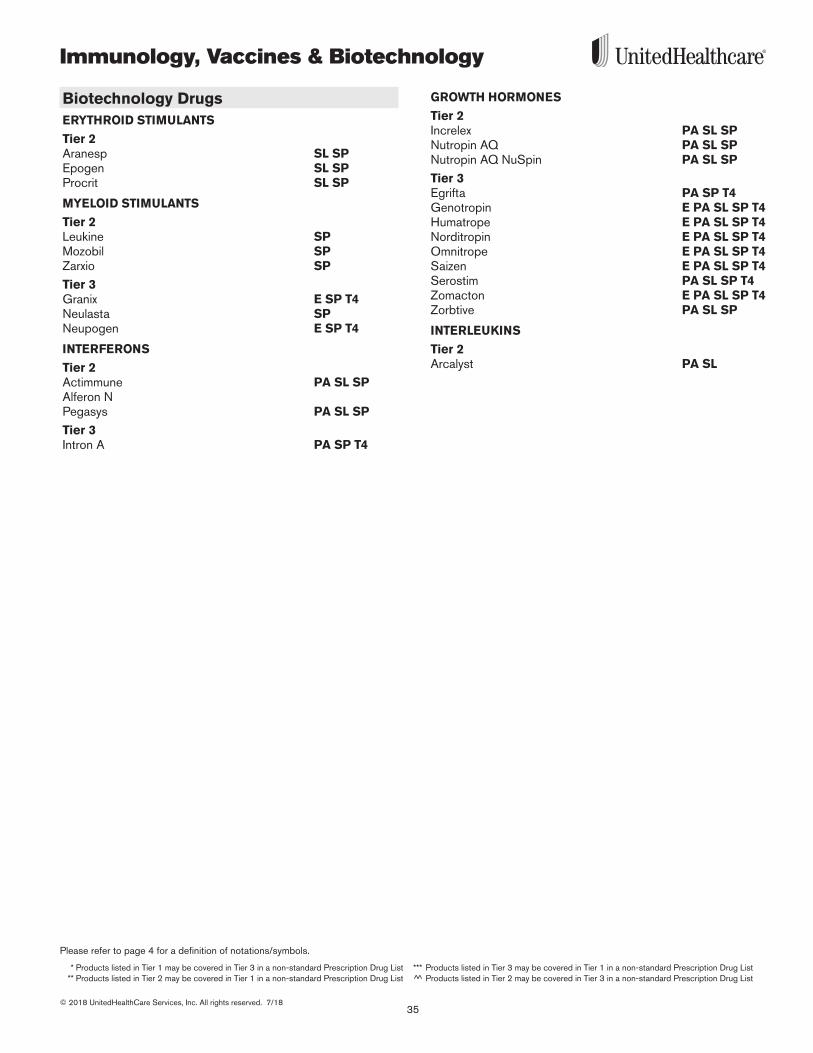
35
Please refer to page 4 for a definition of notations/symbols.
* Products listed in Tier 1 may be covered in Tier 3 in a non-standard Prescription Drug List *** Products listed in Tier 3 may be covered in Tier 1 in a non-standard Prescription Drug List ** Products listed in Tier 2 may be covered in Tier 1 in a non-standard Prescription Drug List ^̂ Products listed in Tier 2 may be covered in Tier 3 in a non-standard Prescription Drug List
© 2018 UnitedHealthCare Services, Inc. All rights reserved. 7/18
Immunology, Vaccines & Biotechnology
Biotechnology DrugsERYTHROID STIMULANTS
Tier 2Aranesp SL SPEpogen SL SPProcrit SL SP
MYELOID STIMULANTS
Tier 2Leukine SPMozobil SPZarxio SP
Tier 3Granix E SP T4Neulasta SPNeupogen E SP T4
INTERFERONS
Tier 2Actimmune PA SL SPAlferon NPegasys PA SL SP
Tier 3Intron A PA SP T4
GROWTH HORMONES
Tier 2Increlex PA SL SPNutropin AQ PA SL SPNutropin AQ NuSpin PA SL SP
Tier 3Egrifta PA SP T4Genotropin E PA SL SP T4Humatrope E PA SL SP T4Norditropin E PA SL SP T4Omnitrope E PA SL SP T4Saizen E PA SL SP T4Serostim PA SL SP T4Zomacton E PA SL SP T4Zorbtive PA SL SP
INTERLEUKINS
Tier 2Arcalyst PA SL
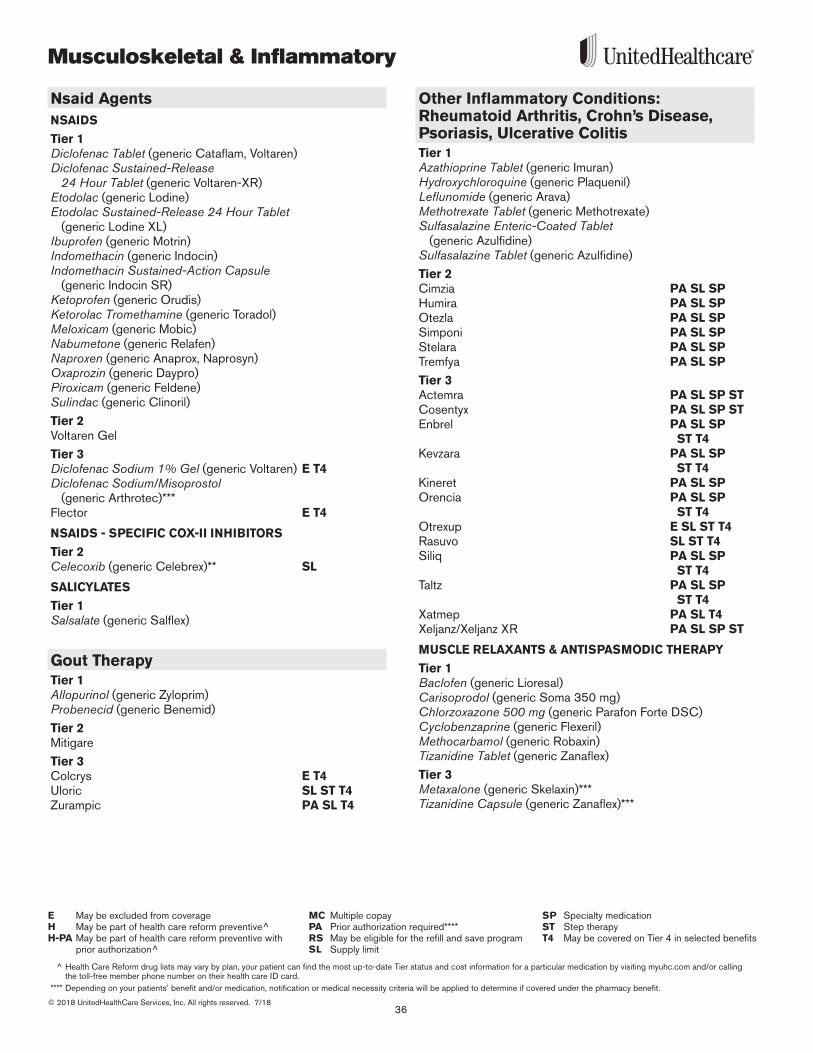
Musculoskeletal & Inflammatory
36© 2018 UnitedHealthCare Services, Inc. All rights reserved. 7/18
^ Health Care Reform drug lists may vary by plan, your patient can find the most up-to-date Tier status and cost information for a particular medication by visiting myuhc.com and/or calling the toll-free member phone number on their health care ID card.
**** Depending on your patients’ benefit and/or medication, notification or medical necessity criteria will be applied to determine if covered under the pharmacy benefit.
MC Multiple copayPA Prior authorization required****RS May be eligible for the refill and save programSL Supply limit
E May be excluded from coverageH May be part of health care reform preventive^H-PA May be part of health care reform preventive with
prior authorization^
SP Specialty medicationST Step therapyT4 May be covered on Tier 4 in selected benefits
Nsaid AgentsNSAIDS
Tier 1Diclofenac Tablet (generic Cataflam, Voltaren)Diclofenac Sustained-Release
24 Hour Tablet (generic Voltaren-XR)Etodolac (generic Lodine)Etodolac Sustained-Release 24 Hour Tablet
(generic Lodine XL)Ibuprofen (generic Motrin)Indomethacin (generic Indocin)Indomethacin Sustained-Action Capsule
(generic Indocin SR)Ketoprofen (generic Orudis)Ketorolac Tromethamine (generic Toradol)Meloxicam (generic Mobic)Nabumetone (generic Relafen)Naproxen (generic Anaprox, Naprosyn) Oxaprozin (generic Daypro)Piroxicam (generic Feldene)Sulindac (generic Clinoril)
Tier 2Voltaren Gel
Tier 3Diclofenac Sodium 1% Gel (generic Voltaren) E T4 Diclofenac Sodium/Misoprostol
(generic Arthrotec)***Flector E T4
NSAIDS - SPECIFIC COX-II INHIBITORS
Tier 2Celecoxib (generic Celebrex)** SL
SALICYLATES
Tier 1Salsalate (generic Salflex)
Gout TherapyTier 1Allopurinol (generic Zyloprim)Probenecid (generic Benemid)
Tier 2Mitigare
Tier 3Colcrys E T4Uloric SL ST T4Zurampic PA SL T4
Other Inflammatory Conditions: Rheumatoid Arthritis, Crohn’s Disease, Psoriasis, Ulcerative ColitisTier 1Azathioprine Tablet (generic Imuran)Hydroxychloroquine (generic Plaquenil)Leflunomide (generic Arava)Methotrexate Tablet (generic Methotrexate)Sulfasalazine Enteric-Coated Tablet
(generic Azulfidine)Sulfasalazine Tablet (generic Azulfidine)
Tier 2Cimzia PA SL SPHumira PA SL SPOtezla PA SL SPSimponi PA SL SPStelara PA SL SPTremfya PA SL SP
Tier 3Actemra PA SL SP STCosentyx PA SL SP STEnbrel PA SL SP
ST T4Kevzara PA SL SP
ST T4 Kineret PA SL SPOrencia PA SL SP
ST T4Otrexup E SL ST T4Rasuvo SL ST T4Siliq PA SL SP
ST T4 Taltz PA SL SP
ST T4 Xatmep PA SL T4 Xeljanz/Xeljanz XR PA SL SP ST
MUSCLE RELAXANTS & ANTISPASMODIC THERAPY
Tier 1Baclofen (generic Lioresal)Carisoprodol (generic Soma 350 mg)Chlorzoxazone 500 mg (generic Parafon Forte DSC)Cyclobenzaprine (generic Flexeril)Methocarbamol (generic Robaxin)Tizanidine Tablet (generic Zanaflex)
Tier 3Metaxalone (generic Skelaxin)***Tizanidine Capsule (generic Zanaflex)***
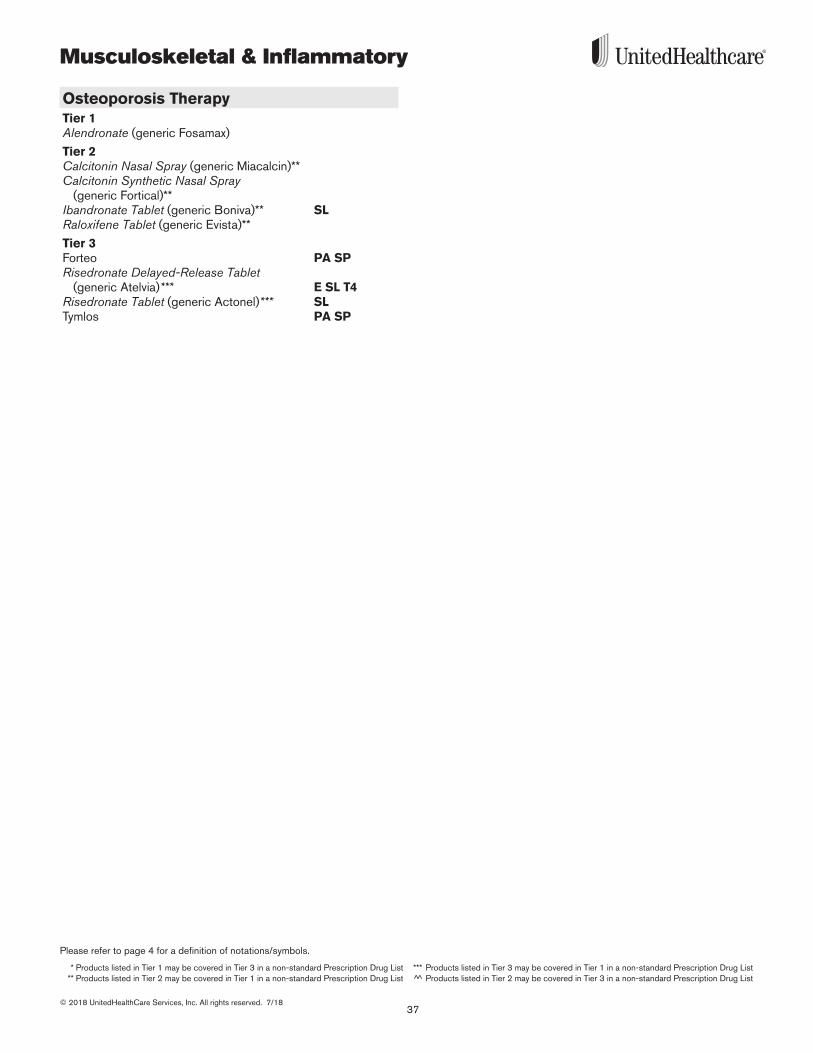
37
Please refer to page 4 for a definition of notations/symbols.
* Products listed in Tier 1 may be covered in Tier 3 in a non-standard Prescription Drug List *** Products listed in Tier 3 may be covered in Tier 1 in a non-standard Prescription Drug List ** Products listed in Tier 2 may be covered in Tier 1 in a non-standard Prescription Drug List ^̂ Products listed in Tier 2 may be covered in Tier 3 in a non-standard Prescription Drug List
© 2018 UnitedHealthCare Services, Inc. All rights reserved. 7/18
Musculoskeletal & Inflammatory
Osteoporosis TherapyTier 1Alendronate (generic Fosamax)
Tier 2Calcitonin Nasal Spray (generic Miacalcin)**Calcitonin Synthetic Nasal Spray
(generic Fortical)**Ibandronate Tablet (generic Boniva)** SLRaloxifene Tablet (generic Evista)**
Tier 3Forteo PA SPRisedronate Delayed-Release Tablet
(generic Atelvia)*** E SL T4 Risedronate Tablet (generic Actonel)*** SLTymlos PA SP
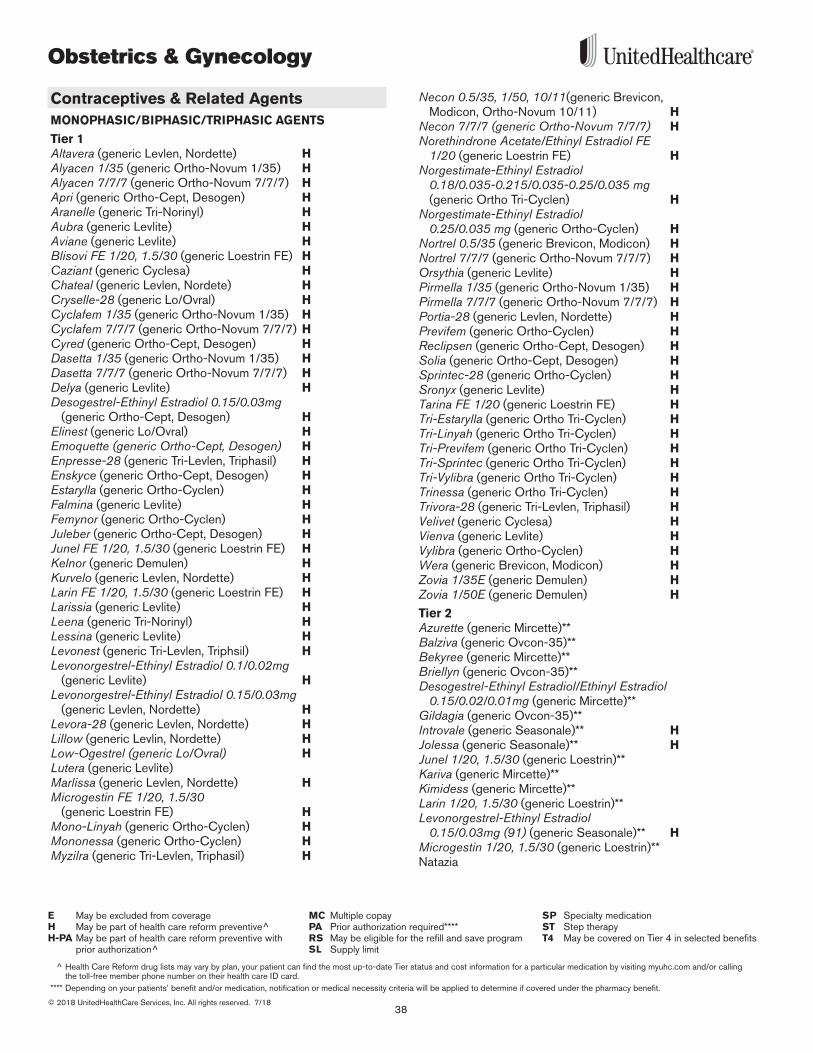
Obstetrics & Gynecology
38© 2018 UnitedHealthCare Services, Inc. All rights reserved. 7/18
^ Health Care Reform drug lists may vary by plan, your patient can find the most up-to-date Tier status and cost information for a particular medication by visiting myuhc.com and/or calling the toll-free member phone number on their health care ID card.
**** Depending on your patients’ benefit and/or medication, notification or medical necessity criteria will be applied to determine if covered under the pharmacy benefit.
MC Multiple copayPA Prior authorization required****RS May be eligible for the refill and save programSL Supply limit
E May be excluded from coverageH May be part of health care reform preventive^H-PA May be part of health care reform preventive with
prior authorization^
SP Specialty medicationST Step therapyT4 May be covered on Tier 4 in selected benefits
Contraceptives & Related AgentsMONOPHASIC/BIPHASIC/TRIPHASIC AGENTS
Tier 1Altavera (generic Levlen, Nordette) HAlyacen 1/35 (generic Ortho-Novum 1/35) HAlyacen 7/7/7 (generic Ortho-Novum 7/7/7) H Apri (generic Ortho-Cept, Desogen) HAranelle (generic Tri-Norinyl) HAubra (generic Levlite) HAviane (generic Levlite) HBlisovi FE 1/20, 1.5/30 (generic Loestrin FE) H Caziant (generic Cyclesa) HChateal (generic Levlen, Nordete) HCryselle-28 (generic Lo/Ovral) HCyclafem 1/35 (generic Ortho-Novum 1/35) HCyclafem 7/7/7 (generic Ortho-Novum 7/7/7) HCyred (generic Ortho-Cept, Desogen) H Dasetta 1/35 (generic Ortho-Novum 1/35) H Dasetta 7/7/7 (generic Ortho-Novum 7/7/7) H Delya (generic Levlite) HDesogestrel-Ethinyl Estradiol 0.15/0.03mg
(generic Ortho-Cept, Desogen) HElinest (generic Lo/Ovral) HEmoquette (generic Ortho-Cept, Desogen) HEnpresse-28 (generic Tri-Levlen, Triphasil) HEnskyce (generic Ortho-Cept, Desogen) HEstarylla (generic Ortho-Cyclen) HFalmina (generic Levlite) HFemynor (generic Ortho-Cyclen) HJuleber (generic Ortho-Cept, Desogen) H Junel FE 1/20, 1.5/30 (generic Loestrin FE) HKelnor (generic Demulen) HKurvelo (generic Levlen, Nordette) H Larin FE 1/20, 1.5/30 (generic Loestrin FE) HLarissia (generic Levlite) H Leena (generic Tri-Norinyl) HLessina (generic Levlite) HLevonest (generic Tri-Levlen, Triphsil) HLevonorgestrel-Ethinyl Estradiol 0.1/0.02mg
(generic Levlite) HLevonorgestrel-Ethinyl Estradiol 0.15/0.03mg
(generic Levlen, Nordette) HLevora-28 (generic Levlen, Nordette) HLillow (generic Levlin, Nordette) H Low-Ogestrel (generic Lo/Ovral) HLutera (generic Levlite)Marlissa (generic Levlen, Nordette) HMicrogestin FE 1/20, 1.5/30
(generic Loestrin FE) HMono-Linyah (generic Ortho-Cyclen) HMononessa (generic Ortho-Cyclen) H Myzilra (generic Tri-Levlen, Triphasil) H
Necon 0.5/35, 1/50, 10/11(generic Brevicon, Modicon, Ortho-Novum 10/11) H
Necon 7/7/7 (generic Ortho-Novum 7/7/7) H Norethindrone Acetate/Ethinyl Estradiol FE
1/20 (generic Loestrin FE) H Norgestimate-Ethinyl Estradiol
0.18/0.035-0.215/0.035-0.25/0.035 mg (generic Ortho Tri-Cyclen) H
Norgestimate-Ethinyl Estradiol 0.25/0.035 mg (generic Ortho-Cyclen) H
Nortrel 0.5/35 (generic Brevicon, Modicon) HNortrel 7/7/7 (generic Ortho-Novum 7/7/7) H Orsythia (generic Levlite) HPirmella 1/35 (generic Ortho-Novum 1/35) HPirmella 7/7/7 (generic Ortho-Novum 7/7/7) H Portia-28 (generic Levlen, Nordette) HPrevifem (generic Ortho-Cyclen) HReclipsen (generic Ortho-Cept, Desogen) HSolia (generic Ortho-Cept, Desogen) HSprintec-28 (generic Ortho-Cyclen) H Sronyx (generic Levlite) HTarina FE 1/20 (generic Loestrin FE) HTri-Estarylla (generic Ortho Tri-Cyclen) HTri-Linyah (generic Ortho Tri-Cyclen) HTri-Previfem (generic Ortho Tri-Cyclen) HTri-Sprintec (generic Ortho Tri-Cyclen) HTri-Vylibra (generic Ortho Tri-Cyclen) H Trinessa (generic Ortho Tri-Cyclen) H Trivora-28 (generic Tri-Levlen, Triphasil) HVelivet (generic Cyclesa) HVienva (generic Levlite) H Vylibra (generic Ortho-Cyclen) H Wera (generic Brevicon, Modicon) HZovia 1/35E (generic Demulen) HZovia 1/50E (generic Demulen) H
Tier 2Azurette (generic Mircette)** Balziva (generic Ovcon-35)** Bekyree (generic Mircette)** Briellyn (generic Ovcon-35)** Desogestrel-Ethinyl Estradiol/Ethinyl Estradiol
0.15/0.02/0.01mg (generic Mircette)** Gildagia (generic Ovcon-35)** Introvale (generic Seasonale)** HJolessa (generic Seasonale)** HJunel 1/20, 1.5/30 (generic Loestrin)** Kariva (generic Mircette)** Kimidess (generic Mircette)** Larin 1/20, 1.5/30 (generic Loestrin)** Levonorgestrel-Ethinyl Estradiol
0.15/0.03mg (91) (generic Seasonale)** HMicrogestin 1/20, 1.5/30 (generic Loestrin)** Natazia
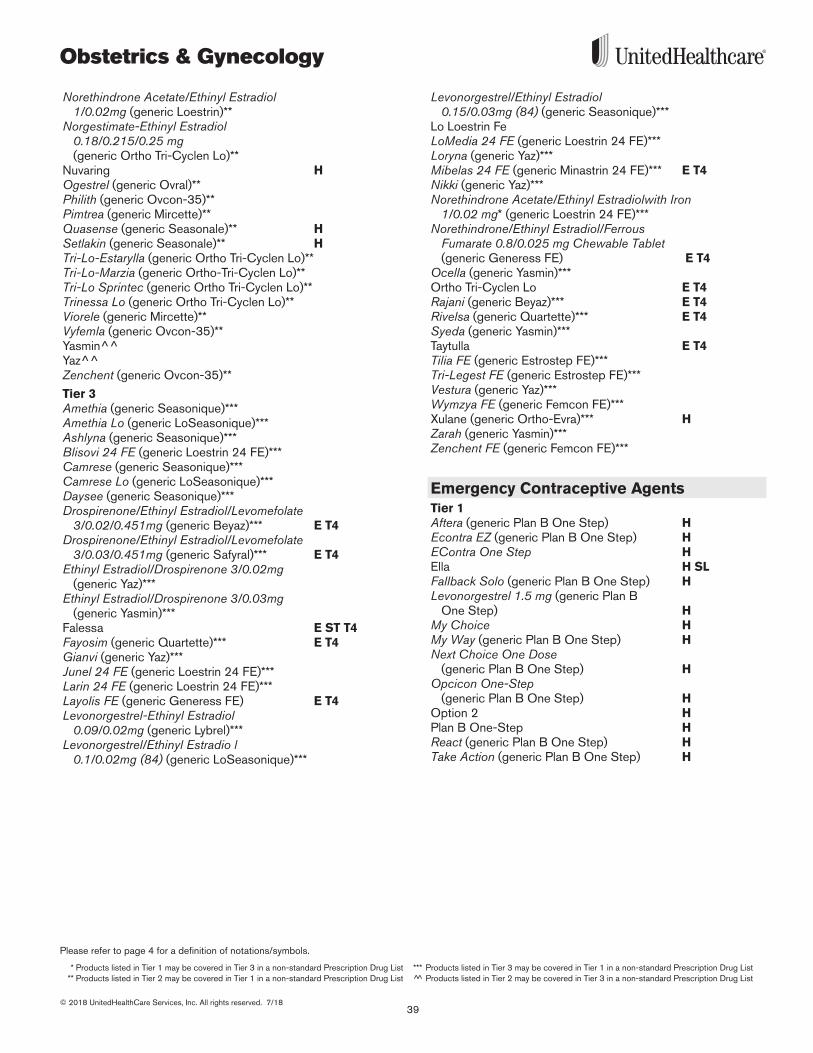
39
Please refer to page 4 for a definition of notations/symbols.
* Products listed in Tier 1 may be covered in Tier 3 in a non-standard Prescription Drug List *** Products listed in Tier 3 may be covered in Tier 1 in a non-standard Prescription Drug List ** Products listed in Tier 2 may be covered in Tier 1 in a non-standard Prescription Drug List ^̂ Products listed in Tier 2 may be covered in Tier 3 in a non-standard Prescription Drug List
© 2018 UnitedHealthCare Services, Inc. All rights reserved. 7/18
Obstetrics & Gynecology
Norethindrone Acetate/Ethinyl Estradiol 1/0.02mg (generic Loestrin)**
Norgestimate-Ethinyl Estradiol 0.18/0.215/0.25 mg (generic Ortho Tri-Cyclen Lo)**
Nuvaring HOgestrel (generic Ovral)** Philith (generic Ovcon-35)** Pimtrea (generic Mircette)** Quasense (generic Seasonale)** HSetlakin (generic Seasonale)** H Tri-Lo-Estarylla (generic Ortho Tri-Cyclen Lo)**Tri-Lo-Marzia (generic Ortho-Tri-Cyclen Lo)**Tri-Lo Sprintec (generic Ortho Tri-Cyclen Lo)**Trinessa Lo (generic Ortho Tri-Cyclen Lo)**Viorele (generic Mircette)** Vyfemla (generic Ovcon-35)** Yasmin^^ Yaz^^ Zenchent (generic Ovcon-35)**
Tier 3Amethia (generic Seasonique)***Amethia Lo (generic LoSeasonique)***Ashlyna (generic Seasonique)*** Blisovi 24 FE (generic Loestrin 24 FE)*** Camrese (generic Seasonique)***Camrese Lo (generic LoSeasonique)***Daysee (generic Seasonique)***Drospirenone/Ethinyl Estradiol/Levomefolate
3/0.02/0.451mg (generic Beyaz)*** E T4 Drospirenone/Ethinyl Estradiol/Levomefolate
3/0.03/0.451mg (generic Safyral)*** E T4Ethinyl Estradiol/Drospirenone 3/0.02mg
(generic Yaz)*** Ethinyl Estradiol/Drospirenone 3/0.03mg
(generic Yasmin)*** Falessa E ST T4Fayosim (generic Quartette)*** E T4Gianvi (generic Yaz)*** Junel 24 FE (generic Loestrin 24 FE)***Larin 24 FE (generic Loestrin 24 FE)*** Layolis FE (generic Generess FE) E T4Levonorgestrel-Ethinyl Estradiol
0.09/0.02mg (generic Lybrel)***Levonorgestrel/Ethinyl Estradio l
0.1/0.02mg (84) (generic LoSeasonique)***
Levonorgestrel/Ethinyl Estradiol 0.15/0.03mg (84) (generic Seasonique)***
Lo Loestrin FeLoMedia 24 FE (generic Loestrin 24 FE)*** Loryna (generic Yaz)*** Mibelas 24 FE (generic Minastrin 24 FE)*** E T4Nikki (generic Yaz)*** Norethindrone Acetate/Ethinyl Estradiolwith Iron
1/0.02 mg* (generic Loestrin 24 FE)*** Norethindrone/Ethinyl Estradiol/Ferrous
Fumarate 0.8/0.025 mg Chewable Tablet (generic Generess FE) E T4
Ocella (generic Yasmin)*** Ortho Tri-Cyclen Lo E T4Rajani (generic Beyaz)*** E T4 Rivelsa (generic Quartette)*** E T4 Syeda (generic Yasmin)***Taytulla E T4 Tilia FE (generic Estrostep FE)*** Tri-Legest FE (generic Estrostep FE)*** Vestura (generic Yaz)*** Wymzya FE (generic Femcon FE)*** Xulane (generic Ortho-Evra)*** HZarah (generic Yasmin)*** Zenchent FE (generic Femcon FE)***
Emergency Contraceptive AgentsTier 1Aftera (generic Plan B One Step) HEcontra EZ (generic Plan B One Step) HEContra One Step HElla H SLFallback Solo (generic Plan B One Step) HLevonorgestrel 1.5 mg (generic Plan B
One Step) HMy Choice H My Way (generic Plan B One Step) HNext Choice One Dose
(generic Plan B One Step) HOpcicon One-Step
(generic Plan B One Step) H Option 2 H Plan B One-Step HReact (generic Plan B One Step) H Take Action (generic Plan B One Step) H
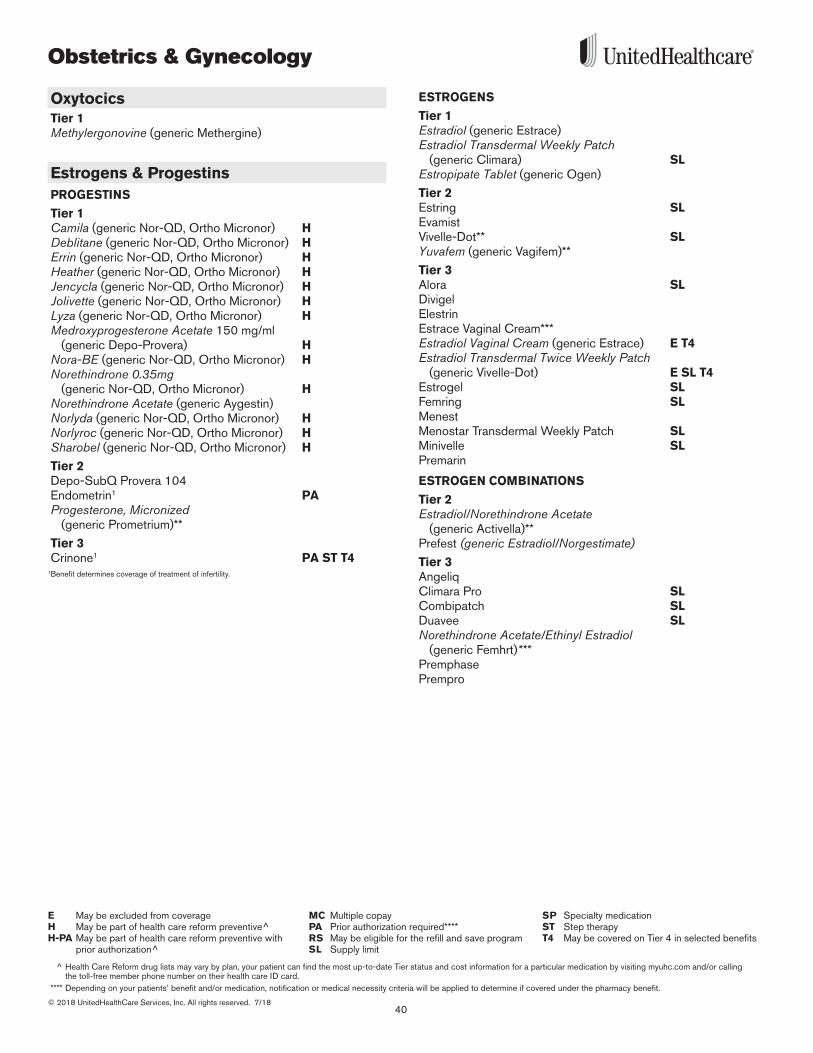
Obstetrics & Gynecology
40© 2018 UnitedHealthCare Services, Inc. All rights reserved. 7/18
^ Health Care Reform drug lists may vary by plan, your patient can find the most up-to-date Tier status and cost information for a particular medication by visiting myuhc.com and/or calling the toll-free member phone number on their health care ID card.
**** Depending on your patients’ benefit and/or medication, notification or medical necessity criteria will be applied to determine if covered under the pharmacy benefit.
MC Multiple copayPA Prior authorization required****RS May be eligible for the refill and save programSL Supply limit
E May be excluded from coverageH May be part of health care reform preventive^H-PA May be part of health care reform preventive with
prior authorization^
SP Specialty medicationST Step therapyT4 May be covered on Tier 4 in selected benefits
OxytocicsTier 1Methylergonovine (generic Methergine)
Estrogens & ProgestinsPROGESTINS
Tier 1Camila (generic Nor-QD, Ortho Micronor) H Deblitane (generic Nor-QD, Ortho Micronor) HErrin (generic Nor-QD, Ortho Micronor) HHeather (generic Nor-QD, Ortho Micronor) HJencycla (generic Nor-QD, Ortho Micronor) HJolivette (generic Nor-QD, Ortho Micronor) HLyza (generic Nor-QD, Ortho Micronor) HMedroxyprogesterone Acetate 150 mg/ml
(generic Depo-Provera) HNora-BE (generic Nor-QD, Ortho Micronor) H Norethindrone 0.35mg
(generic Nor-QD, Ortho Micronor) HNorethindrone Acetate (generic Aygestin)Norlyda (generic Nor-QD, Ortho Micronor) HNorlyroc (generic Nor-QD, Ortho Micronor) HSharobel (generic Nor-QD, Ortho Micronor) H
Tier 2Depo-SubQ Provera 104Endometrin1 PA Progesterone, Micronized
(generic Prometrium)**
Tier 3Crinone1 PA ST T4
1Benefit determines coverage of treatment of infertility .
ESTROGENS
Tier 1Estradiol (generic Estrace)Estradiol Transdermal Weekly Patch
(generic Climara) SLEstropipate Tablet (generic Ogen)
Tier 2Estring SLEvamistVivelle-Dot** SLYuvafem (generic Vagifem)**
Tier 3Alora SLDivigelElestrinEstrace Vaginal Cream***Estradiol Vaginal Cream (generic Estrace) E T4 Estradiol Transdermal Twice Weekly Patch
(generic Vivelle-Dot) E SL T4Estrogel SLFemring SLMenest Menostar Transdermal Weekly Patch SLMinivelle SLPremarin
ESTROGEN COMBINATIONS
Tier 2Estradiol/Norethindrone Acetate
(generic Activella)**Prefest (generic Estradiol/Norgestimate)Tier 3AngeliqClimara Pro SLCombipatch SLDuavee SLNorethindrone Acetate/Ethinyl Estradiol
(generic Femhrt)***PremphasePrempro
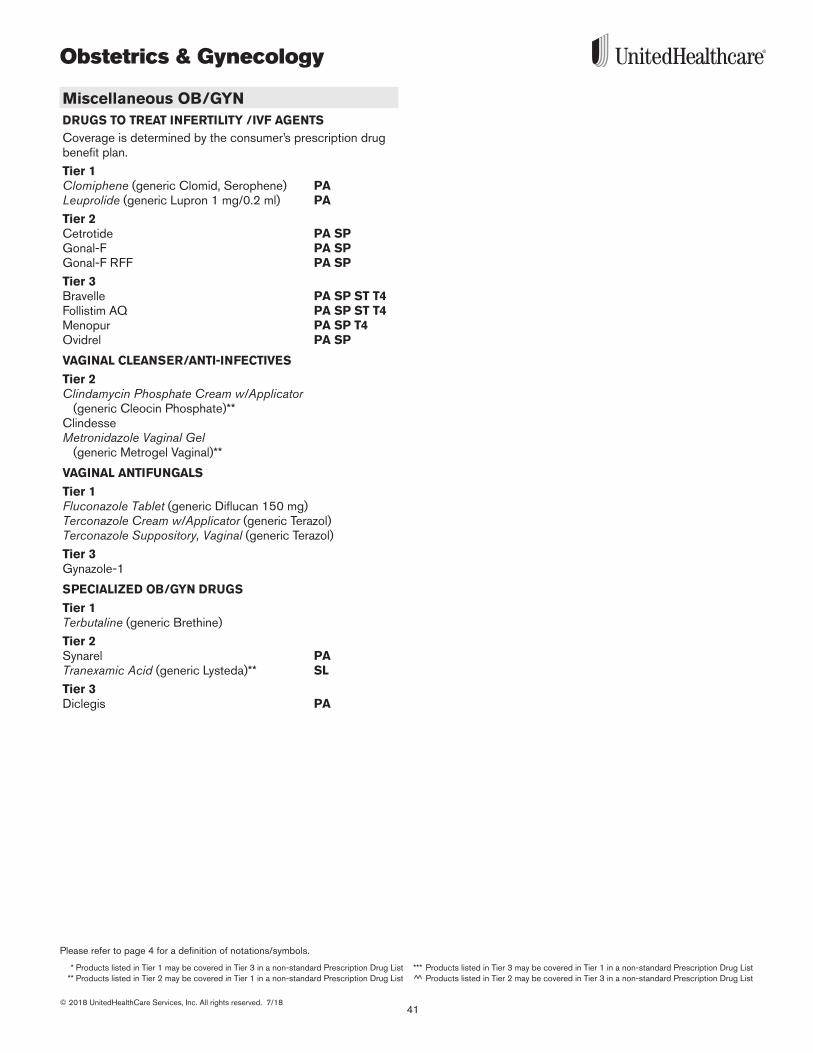
41
Please refer to page 4 for a definition of notations/symbols.
* Products listed in Tier 1 may be covered in Tier 3 in a non-standard Prescription Drug List *** Products listed in Tier 3 may be covered in Tier 1 in a non-standard Prescription Drug List ** Products listed in Tier 2 may be covered in Tier 1 in a non-standard Prescription Drug List ^̂ Products listed in Tier 2 may be covered in Tier 3 in a non-standard Prescription Drug List
© 2018 UnitedHealthCare Services, Inc. All rights reserved. 7/18
Obstetrics & Gynecology
Miscellaneous OB/GYNDRUGS TO TREAT INFERTILITY /IVF AGENTSCoverage is determined by the consumer’s prescription drug benefit plan .
Tier 1Clomiphene (generic Clomid, Serophene) PALeuprolide (generic Lupron 1 mg/0 .2 ml) PA
Tier 2Cetrotide PA SPGonal-F PA SPGonal-F RFF PA SP
Tier 3Bravelle PA SP ST T4Follistim AQ PA SP ST T4Menopur PA SP T4Ovidrel PA SP
VAGINAL CLEANSER/ANTI-INFECTIVES
Tier 2Clindamycin Phosphate Cream w/Applicator
(generic Cleocin Phosphate)**ClindesseMetronidazole Vaginal Gel
(generic Metrogel Vaginal)**
VAGINAL ANTIFUNGALS
Tier 1Fluconazole Tablet (generic Diflucan 150 mg)Terconazole Cream w/Applicator (generic Terazol)Terconazole Suppository, Vaginal (generic Terazol)
Tier 3Gynazole-1
SPECIALIZED OB/GYN DRUGS
Tier 1Terbutaline (generic Brethine)
Tier 2Synarel PATranexamic Acid (generic Lysteda)** SL
Tier 3Diclegis PA
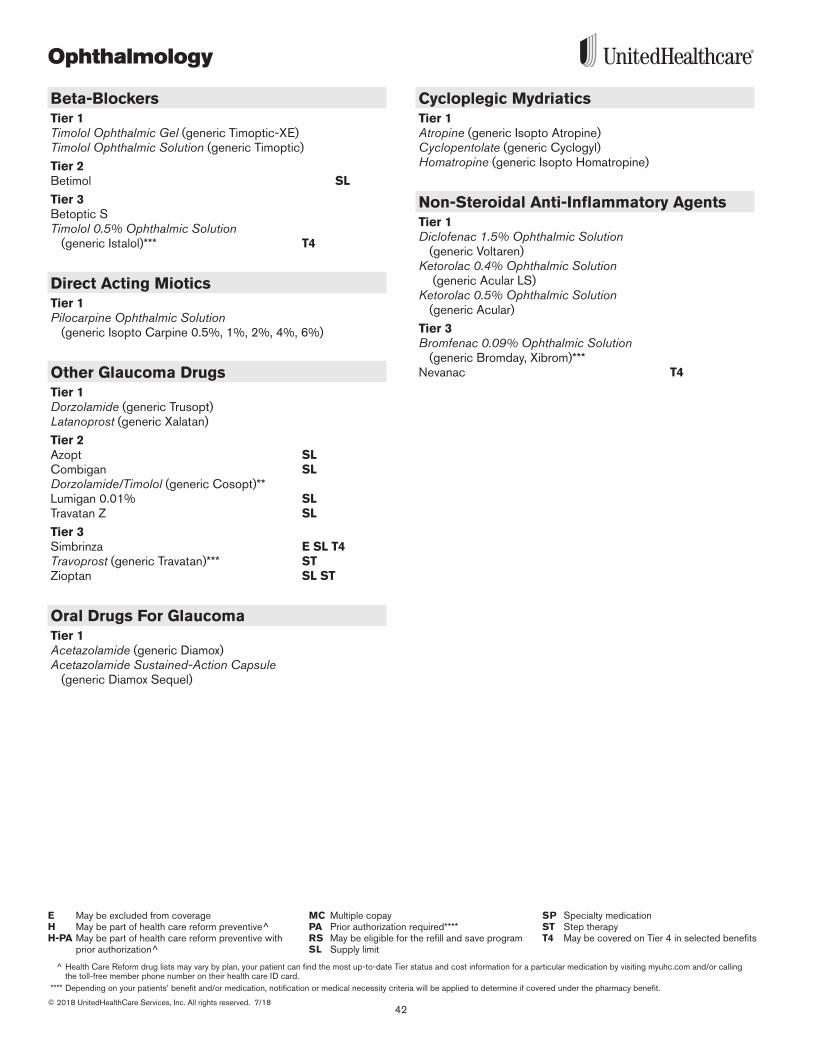
Ophthalmology
42© 2018 UnitedHealthCare Services, Inc. All rights reserved. 7/18
^ Health Care Reform drug lists may vary by plan, your patient can find the most up-to-date Tier status and cost information for a particular medication by visiting myuhc.com and/or calling the toll-free member phone number on their health care ID card.
**** Depending on your patients’ benefit and/or medication, notification or medical necessity criteria will be applied to determine if covered under the pharmacy benefit.
MC Multiple copayPA Prior authorization required****RS May be eligible for the refill and save programSL Supply limit
E May be excluded from coverageH May be part of health care reform preventive^H-PA May be part of health care reform preventive with
prior authorization^
SP Specialty medicationST Step therapyT4 May be covered on Tier 4 in selected benefits
Beta-BlockersTier 1Timolol Ophthalmic Gel (generic Timoptic-XE)Timolol Ophthalmic Solution (generic Timoptic)
Tier 2Betimol SL
Tier 3Betoptic STimolol 0.5% Ophthalmic Solution
(generic Istalol)*** T4
Direct Acting MioticsTier 1Pilocarpine Ophthalmic Solution
(generic Isopto Carpine 0 .5%, 1%, 2%, 4%, 6%)
Other Glaucoma DrugsTier 1Dorzolamide (generic Trusopt)Latanoprost (generic Xalatan)
Tier 2Azopt SLCombigan SLDorzolamide/Timolol (generic Cosopt)**Lumigan 0 .01% SLTravatan Z SL
Tier 3Simbrinza E SL T4 Travoprost (generic Travatan)*** STZioptan SL ST
Oral Drugs For GlaucomaTier 1Acetazolamide (generic Diamox)Acetazolamide Sustained-Action Capsule
(generic Diamox Sequel)
Cycloplegic MydriaticsTier 1Atropine (generic Isopto Atropine)Cyclopentolate (generic Cyclogyl)Homatropine (generic Isopto Homatropine)
Non-Steroidal Anti-Inflammatory AgentsTier 1Diclofenac 1.5% Ophthalmic Solution
(generic Voltaren)Ketorolac 0.4% Ophthalmic Solution
(generic Acular LS)Ketorolac 0.5% Ophthalmic Solution
(generic Acular)
Tier 3Bromfenac 0.09% Ophthalmic Solution
(generic Bromday, Xibrom)*** Nevanac T4

43
Please refer to page 4 for a definition of notations/symbols.
* Products listed in Tier 1 may be covered in Tier 3 in a non-standard Prescription Drug List *** Products listed in Tier 3 may be covered in Tier 1 in a non-standard Prescription Drug List ** Products listed in Tier 2 may be covered in Tier 1 in a non-standard Prescription Drug List ^̂ Products listed in Tier 2 may be covered in Tier 3 in a non-standard Prescription Drug List
© 2018 UnitedHealthCare Services, Inc. All rights reserved. 7/18
Ophthalmology
AntibioticsTier 1Bacitracin/Polymyxin B Sulfate (generic Polysporin)Ciprofloxacin Solution (generic Ciloxan)Erythromycin Base (generic Ilotycin)Gentamicin Sulfate (generic Garamycin)Levofloxacin (generic Quixin)Neomycin Sulfate/Bacitracin/Polymyxin B
Ointment (generic Neosporin)Neomycin Sulfate/Gramicidin D/Polymyxin B
Drops (generic Neosporin)Ofloxacin (generic Ocuflox)Polymyxin B Sulfate/Trimethoprim
(generic Polytrim)Tobramycin Sulfate Drops (generic Tobrex)
Tier 3AzasiteCiloxan Ointment Gatifloxacin (generic Zymaxid)*** Moxeza T4Moxifloxacin (generic Vigamox)***Tobrex Ointment
SulfonamidesTier 1Sulfacetamide Sodium (generic Bleph-10, Sodium Sulamyd)
SteroidsTier 1Fluorometholone (generic FML)Prednisolone Acetate (generic Pred Forte)Prednisolone Sodium Phosphate
(generic Inflamase Forte)
Tier 2FML ForteMaxidex
Tier 3Alrex SL T4Durezol T4Lotemax Gel E T4Lotemax Ointment, Suspension SL T4
Steroid-Antibiotic CombinationsTier 1Neomycin Sulfate/Bacitracin Zinc/Polymyxin B/
Hydrocortisone Ointment (generic Cortisporin)Neomycin Sulfate/Polymyxin B Sulfate/
Hydrocortisone Suspension, Drops (generic Cortisporin)
Neomycin/Polymyxin B Sulfate/Dexamethasone (generic Maxitrol)
Tier 2Tobramycin/Dexamethasone Suspension
(generic Tobradex)**
Tier 3Zylet
Steroid-Sulfonamide CombinationsTier 1Sulfacetamide Sodium/Prednisolone Sodium
Phosphate (generic Vasocidin)
Tier 3Blephamide Suspension, Drops
SympathomimeticsTier 2Alphagan P SLBrimonidine Tartrate 0.15%
(generic Alphagan P)** SL
Miscellaneous OphthalmologicsTier 1Azelastine Solution (generic Optivar)
Tier 3Lastacaft SLOlopatadine 0.1% (generic Patanol)*** SLOlopatadine 0.2% (generic Pataday)*** E SL T4 Restasis Multidose E PA SL T4Restasis Single Dose Vials PA SL T4Xiidra PA SL T4
AntiviralsTier 1Trifluridine (generic Viroptic)
Tier 3Zirgan
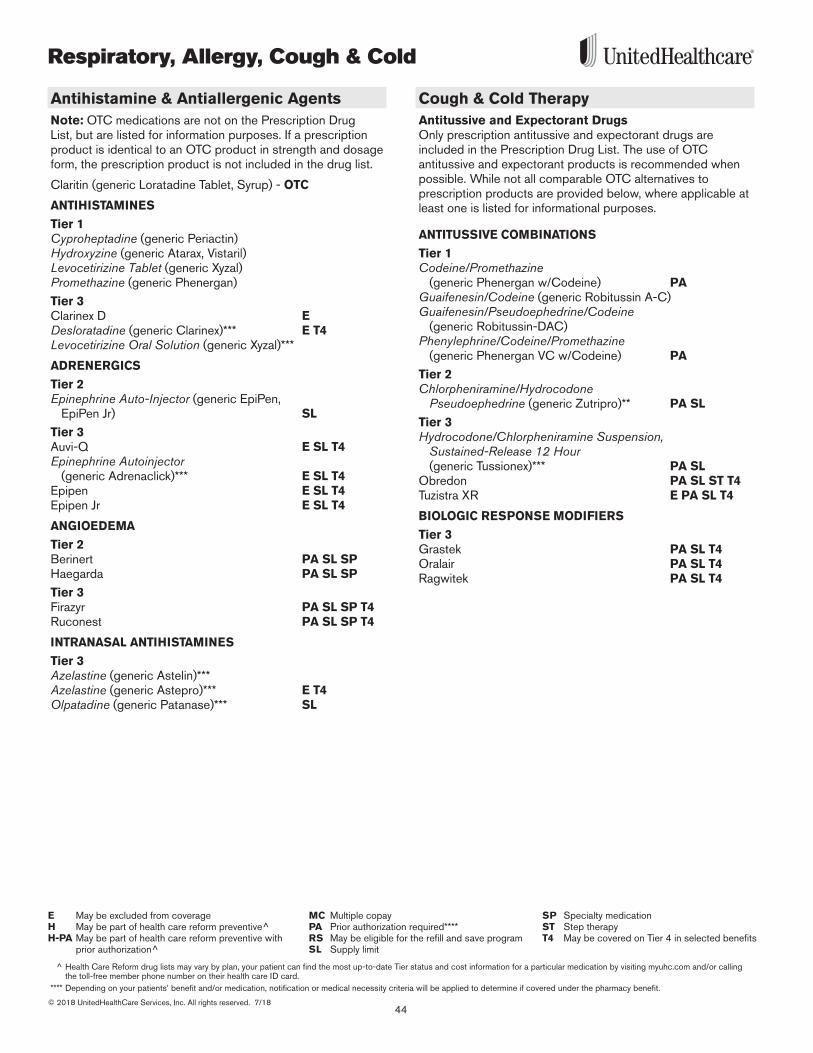
Respiratory, Allergy, Cough & Cold
44© 2018 UnitedHealthCare Services, Inc. All rights reserved. 7/18
^ Health Care Reform drug lists may vary by plan, your patient can find the most up-to-date Tier status and cost information for a particular medication by visiting myuhc.com and/or calling the toll-free member phone number on their health care ID card.
**** Depending on your patients’ benefit and/or medication, notification or medical necessity criteria will be applied to determine if covered under the pharmacy benefit.
MC Multiple copayPA Prior authorization required****RS May be eligible for the refill and save programSL Supply limit
E May be excluded from coverageH May be part of health care reform preventive^H-PA May be part of health care reform preventive with
prior authorization^
SP Specialty medicationST Step therapyT4 May be covered on Tier 4 in selected benefits
Antihistamine & Antiallergenic AgentsNote: OTC medications are not on the Prescription Drug List, but are listed for information purposes . If a prescription product is identical to an OTC product in strength and dosage form, the prescription product is not included in the drug list .
Claritin (generic Loratadine Tablet, Syrup) - OTC
ANTIHISTAMINES
Tier 1Cyproheptadine (generic Periactin)Hydroxyzine (generic Atarax, Vistaril)Levocetirizine Tablet (generic Xyzal) Promethazine (generic Phenergan)
Tier 3Clarinex D E Desloratadine (generic Clarinex)*** E T4Levocetirizine Oral Solution (generic Xyzal)***
ADRENERGICS
Tier 2Epinephrine Auto-Injector (generic EpiPen,
EpiPen Jr) SL
Tier 3Auvi-Q E SL T4Epinephrine Autoinjector
(generic Adrenaclick)*** E SL T4Epipen E SL T4Epipen Jr E SL T4
ANGIOEDEMA
Tier 2Berinert PA SL SPHaegarda PA SL SP
Tier 3Firazyr PA SL SP T4Ruconest PA SL SP T4
INTRANASAL ANTIHISTAMINES
Tier 3Azelastine (generic Astelin)*** Azelastine (generic Astepro)*** E T4Olpatadine (generic Patanase)*** SL
Cough & Cold TherapyAntitussive and Expectorant Drugs Only prescription antitussive and expectorant drugs are included in the Prescription Drug List . The use of OTC antitussive and expectorant products is recommended when possible . While not all comparable OTC alternatives to prescription products are provided below, where applicable at least one is listed for informational purposes .
ANTITUSSIVE COMBINATIONS
Tier 1Codeine/Promethazine
(generic Phenergan w/Codeine) PAGuaifenesin/Codeine (generic Robitussin A-C)Guaifenesin/Pseudoephedrine/Codeine
(generic Robitussin-DAC)Phenylephrine/Codeine/Promethazine
(generic Phenergan VC w/Codeine) PA
Tier 2Chlorpheniramine/Hydrocodone
Pseudoephedrine (generic Zutripro)** PA SL Tier 3Hydrocodone/Chlorpheniramine Suspension,
Sustained-Release 12 Hour (generic Tussionex)*** PA SL
Obredon PA SL ST T4 Tuzistra XR E PA SL T4
BIOLOGIC RESPONSE MODIFIERS
Tier 3Grastek PA SL T4Oralair PA SL T4Ragwitek PA SL T4
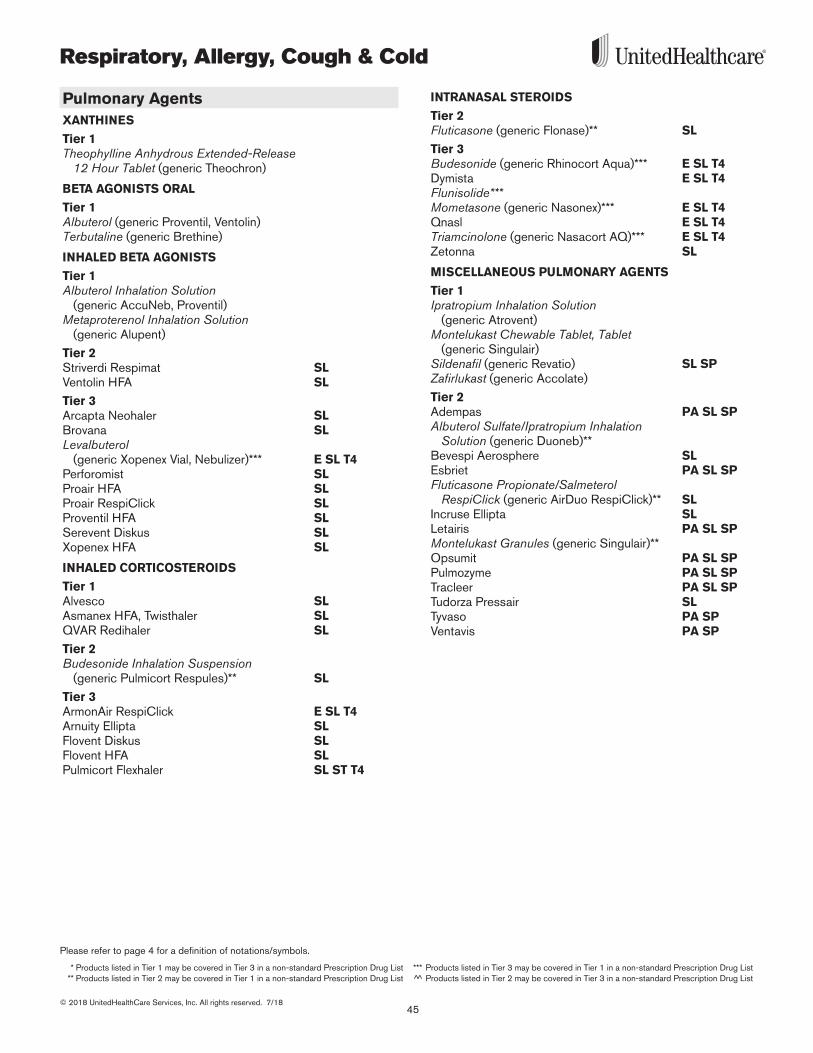
45
Please refer to page 4 for a definition of notations/symbols.
* Products listed in Tier 1 may be covered in Tier 3 in a non-standard Prescription Drug List *** Products listed in Tier 3 may be covered in Tier 1 in a non-standard Prescription Drug List ** Products listed in Tier 2 may be covered in Tier 1 in a non-standard Prescription Drug List ^̂ Products listed in Tier 2 may be covered in Tier 3 in a non-standard Prescription Drug List
© 2018 UnitedHealthCare Services, Inc. All rights reserved. 7/18
Respiratory, Allergy, Cough & Cold
Pulmonary AgentsXANTHINES
Tier 1Theophylline Anhydrous Extended-Release
12 Hour Tablet (generic Theochron)
BETA AGONISTS ORAL
Tier 1Albuterol (generic Proventil, Ventolin)Terbutaline (generic Brethine)
INHALED BETA AGONISTS
Tier 1Albuterol Inhalation Solution
(generic AccuNeb, Proventil)Metaproterenol Inhalation Solution
(generic Alupent)
Tier 2Striverdi Respimat SL Ventolin HFA SL
Tier 3Arcapta Neohaler SL Brovana SLLevalbuterol
(generic Xopenex Vial, Nebulizer)*** E SL T4Perforomist SLProair HFA SLProair RespiClick SL Proventil HFA SLSerevent Diskus SLXopenex HFA SL
INHALED CORTICOSTEROIDS
Tier 1Alvesco SLAsmanex HFA, Twisthaler SLQVAR Redihaler SL
Tier 2Budesonide Inhalation Suspension
(generic Pulmicort Respules)** SL
Tier 3ArmonAir RespiClick E SL T4 Arnuity Ellipta SLFlovent Diskus SLFlovent HFA SLPulmicort Flexhaler SL ST T4
INTRANASAL STEROIDS
Tier 2Fluticasone (generic Flonase)** SL
Tier 3Budesonide (generic Rhinocort Aqua)*** E SL T4Dymista E SL T4Flunisolide*** Mometasone (generic Nasonex)*** E SL T4Qnasl E SL T4Triamcinolone (generic Nasacort AQ)*** E SL T4Zetonna SL
MISCELLANEOUS PULMONARY AGENTS
Tier 1Ipratropium Inhalation Solution
(generic Atrovent)Montelukast Chewable Tablet, Tablet
(generic Singulair)Sildenafil (generic Revatio) SL SPZafirlukast (generic Accolate)
Tier 2Adempas PA SL SPAlbuterol Sulfate/Ipratropium Inhalation
Solution (generic Duoneb)**Bevespi Aerosphere SL Esbriet PA SL SP Fluticasone Propionate/Salmeterol
RespiClick (generic AirDuo RespiClick)** SLIncruse Ellipta SLLetairis PA SL SPMontelukast Granules (generic Singulair)** Opsumit PA SL SPPulmozyme PA SL SPTracleer PA SL SPTudorza Pressair SLTyvaso PA SPVentavis PA SP
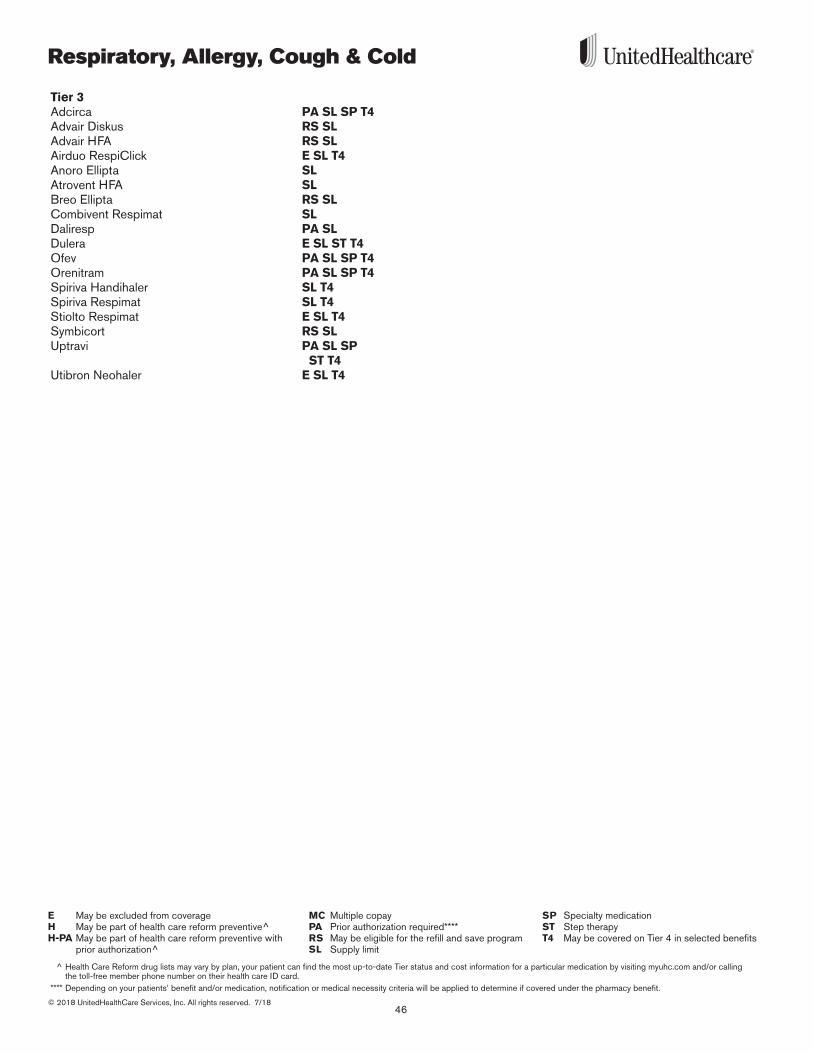
Respiratory, Allergy, Cough & Cold
46© 2018 UnitedHealthCare Services, Inc. All rights reserved. 7/18
^ Health Care Reform drug lists may vary by plan, your patient can find the most up-to-date Tier status and cost information for a particular medication by visiting myuhc.com and/or calling the toll-free member phone number on their health care ID card.
**** Depending on your patients’ benefit and/or medication, notification or medical necessity criteria will be applied to determine if covered under the pharmacy benefit.
MC Multiple copayPA Prior authorization required****RS May be eligible for the refill and save programSL Supply limit
E May be excluded from coverageH May be part of health care reform preventive^H-PA May be part of health care reform preventive with
prior authorization^
SP Specialty medicationST Step therapyT4 May be covered on Tier 4 in selected benefits
Tier 3Adcirca PA SL SP T4Advair Diskus RS SLAdvair HFA RS SLAirduo RespiClick E SL T4 Anoro Ellipta SL Atrovent HFA SLBreo Ellipta RS SL Combivent Respimat SLDaliresp PA SLDulera E SL ST T4Ofev PA SL SP T4 Orenitram PA SL SP T4 Spiriva Handihaler SL T4Spiriva Respimat SL T4Stiolto Respimat E SL T4Symbicort RS SLUptravi PA SL SP
ST T4 Utibron Neohaler E SL T4
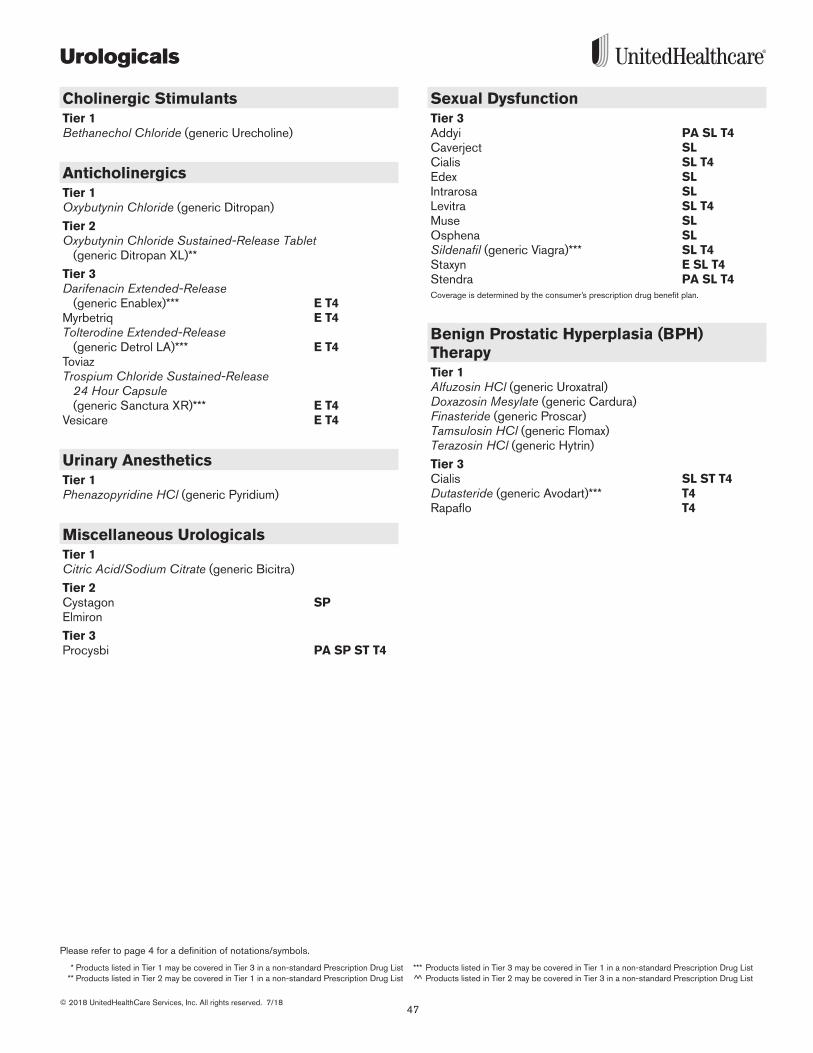
47
Please refer to page 4 for a definition of notations/symbols.
* Products listed in Tier 1 may be covered in Tier 3 in a non-standard Prescription Drug List *** Products listed in Tier 3 may be covered in Tier 1 in a non-standard Prescription Drug List ** Products listed in Tier 2 may be covered in Tier 1 in a non-standard Prescription Drug List ^̂ Products listed in Tier 2 may be covered in Tier 3 in a non-standard Prescription Drug List
© 2018 UnitedHealthCare Services, Inc. All rights reserved. 7/18
Urologicals
Cholinergic StimulantsTier 1Bethanechol Chloride (generic Urecholine)
Anticholinergics Tier 1Oxybutynin Chloride (generic Ditropan)
Tier 2Oxybutynin Chloride Sustained-Release Tablet
(generic Ditropan XL)**
Tier 3Darifenacin Extended-Release
(generic Enablex)*** E T4 Myrbetriq E T4Tolterodine Extended-Release
(generic Detrol LA)*** E T4ToviazTrospium Chloride Sustained-Release
24 Hour Capsule (generic Sanctura XR)*** E T4
Vesicare E T4
Urinary AnestheticsTier 1Phenazopyridine HCl (generic Pyridium)
Miscellaneous UrologicalsTier 1Citric Acid/Sodium Citrate (generic Bicitra)
Tier 2Cystagon SP Elmiron
Tier 3Procysbi PA SP ST T4
Sexual DysfunctionTier 3Addyi PA SL T4Caverject SLCialis SL T4Edex SLIntrarosa SL Levitra SL T4Muse SLOsphena SL Sildenafil (generic Viagra)*** SL T4 Staxyn E SL T4Stendra PA SL T4Coverage is determined by the consumer’s prescription drug benefit plan .
Benign Prostatic Hyperplasia (BPH) TherapyTier 1Alfuzosin HCl (generic Uroxatral)Doxazosin Mesylate (generic Cardura)Finasteride (generic Proscar)Tamsulosin HCl (generic Flomax)Terazosin HCl (generic Hytrin)
Tier 3Cialis SL ST T4Dutasteride (generic Avodart)*** T4 Rapaflo T4
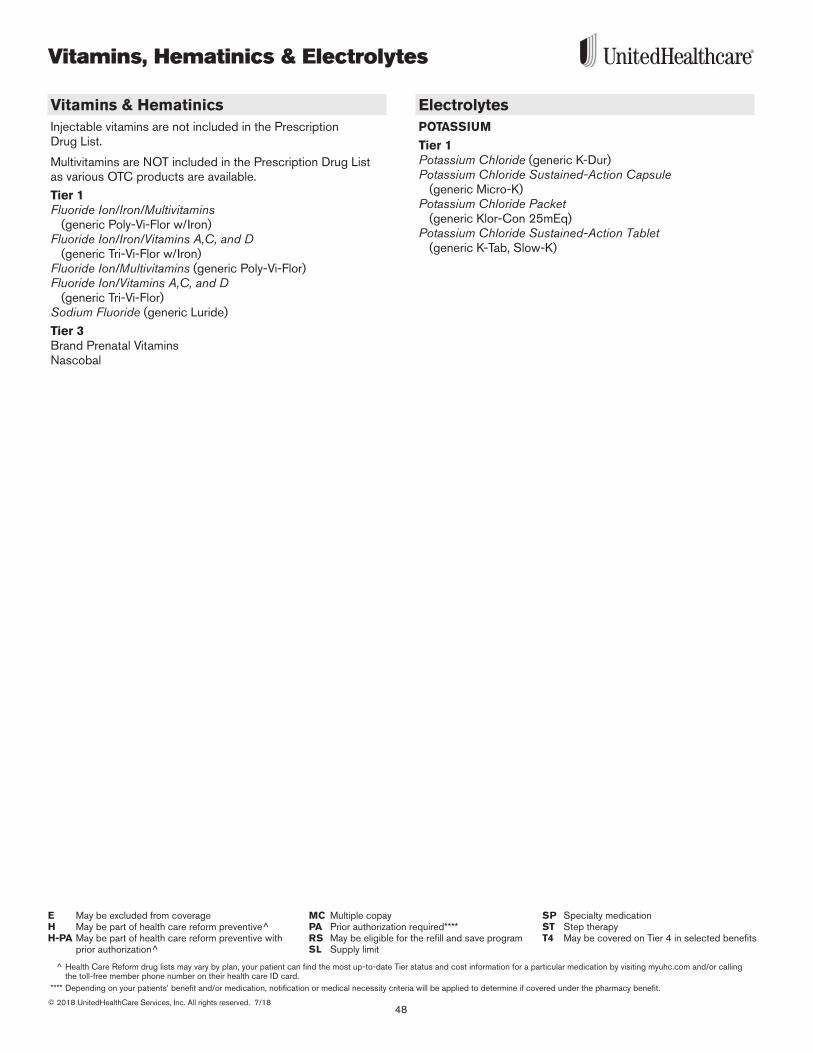
Vitamins, Hematinics & Electrolytes
48© 2018 UnitedHealthCare Services, Inc. All rights reserved. 7/18
^ Health Care Reform drug lists may vary by plan, your patient can find the most up-to-date Tier status and cost information for a particular medication by visiting myuhc.com and/or calling the toll-free member phone number on their health care ID card.
**** Depending on your patients’ benefit and/or medication, notification or medical necessity criteria will be applied to determine if covered under the pharmacy benefit.
MC Multiple copayPA Prior authorization required****RS May be eligible for the refill and save programSL Supply limit
E May be excluded from coverageH May be part of health care reform preventive^H-PA May be part of health care reform preventive with
prior authorization^
SP Specialty medicationST Step therapyT4 May be covered on Tier 4 in selected benefits
Vitamins & HematinicsInjectable vitamins are not included in the Prescription Drug List .
Multivitamins are NOT included in the Prescription Drug List as various OTC products are available .
Tier 1Fluoride Ion/Iron/Multivitamins
(generic Poly-Vi-Flor w/Iron)Fluoride Ion/Iron/Vitamins A,C, and D
(generic Tri-Vi-Flor w/Iron)Fluoride Ion/Multivitamins (generic Poly-Vi-Flor)Fluoride Ion/Vitamins A,C, and D
(generic Tri-Vi-Flor)Sodium Fluoride (generic Luride)
Tier 3Brand Prenatal VitaminsNascobal
ElectrolytesPOTASSIUM
Tier 1Potassium Chloride (generic K-Dur)Potassium Chloride Sustained-Action Capsule
(generic Micro-K)Potassium Chloride Packet
(generic Klor-Con 25mEq)Potassium Chloride Sustained-Action Tablet
(generic K-Tab, Slow-K)
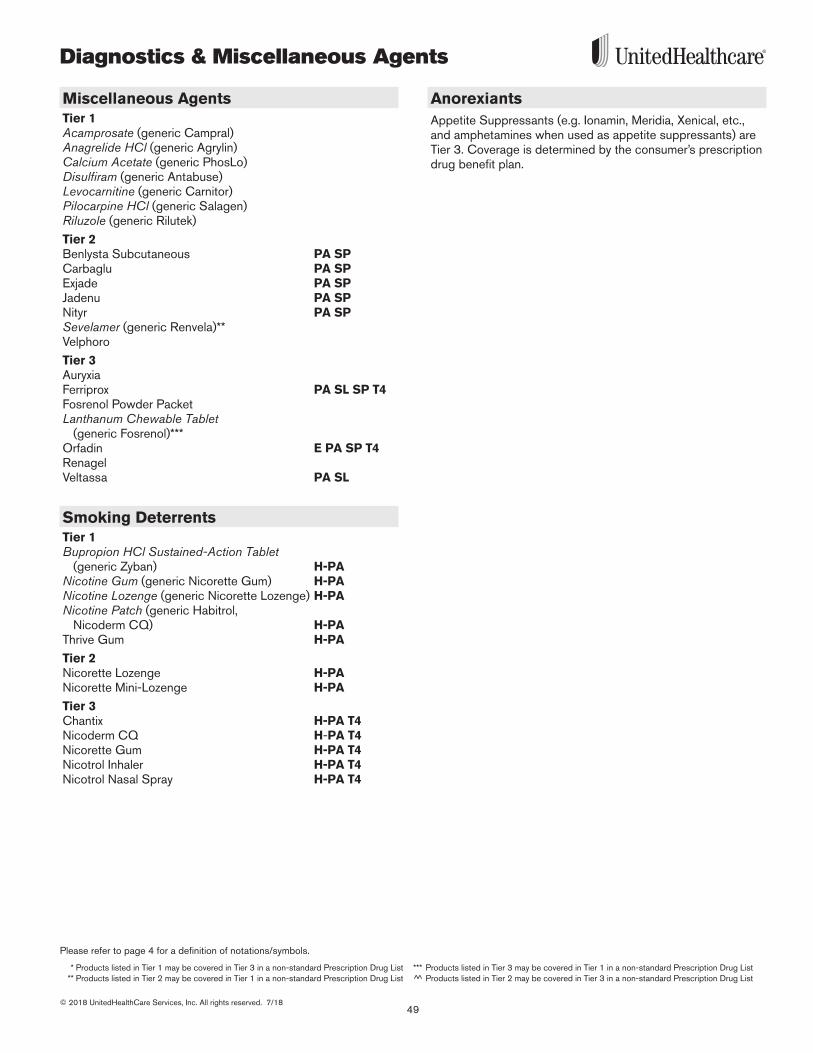
49
Please refer to page 4 for a definition of notations/symbols.
* Products listed in Tier 1 may be covered in Tier 3 in a non-standard Prescription Drug List *** Products listed in Tier 3 may be covered in Tier 1 in a non-standard Prescription Drug List ** Products listed in Tier 2 may be covered in Tier 1 in a non-standard Prescription Drug List ^̂ Products listed in Tier 2 may be covered in Tier 3 in a non-standard Prescription Drug List
© 2018 UnitedHealthCare Services, Inc. All rights reserved. 7/18
Diagnostics & Miscellaneous Agents
Miscellaneous AgentsTier 1Acamprosate (generic Campral) Anagrelide HCl (generic Agrylin)Calcium Acetate (generic PhosLo) Disulfiram (generic Antabuse)Levocarnitine (generic Carnitor)Pilocarpine HCl (generic Salagen)Riluzole (generic Rilutek)
Tier 2Benlysta Subcutaneous PA SP Carbaglu PA SPExjade PA SPJadenu PA SP Nityr PA SP Sevelamer (generic Renvela)** Velphoro
Tier 3Auryxia Ferriprox PA SL SP T4Fosrenol Powder Packet Lanthanum Chewable Tablet
(generic Fosrenol)***Orfadin E PA SP T4 RenagelVeltassa PA SL
Smoking DeterrentsTier 1Bupropion HCl Sustained-Action Tablet
(generic Zyban) H-PANicotine Gum (generic Nicorette Gum) H-PANicotine Lozenge (generic Nicorette Lozenge) H-PANicotine Patch (generic Habitrol,
Nicoderm CQ) H-PAThrive Gum H-PA
Tier 2Nicorette Lozenge H-PANicorette Mini-Lozenge H-PA
Tier 3Chantix H-PA T4Nicoderm CQ H-PA T4Nicorette Gum H-PA T4Nicotrol Inhaler H-PA T4Nicotrol Nasal Spray H-PA T4
AnorexiantsAppetite Suppressants (e .g . Ionamin, Meridia, Xenical, etc ., and amphetamines when used as appetite suppressants) are Tier 3 . Coverage is determined by the consumer’s prescription drug benefit plan .
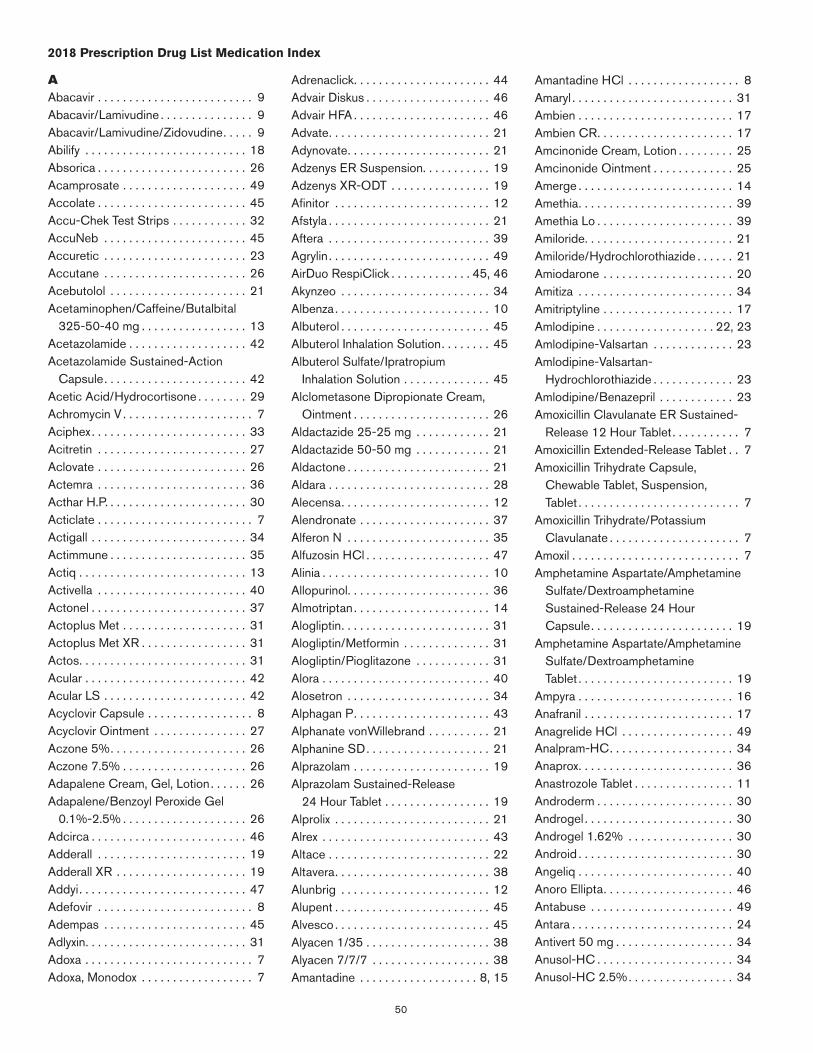
50
2018 Prescription Drug List Medication Index
AAbacavir . . . . . . . . . . . . . . . . . . . . . . . . . 9Abacavir/Lamivudine . . . . . . . . . . . . . . . 9Abacavir/Lamivudine/Zidovudine . . . . . 9Abilify . . . . . . . . . . . . . . . . . . . . . . . . . . 18Absorica . . . . . . . . . . . . . . . . . . . . . . . . 26Acamprosate . . . . . . . . . . . . . . . . . . . . 49Accolate . . . . . . . . . . . . . . . . . . . . . . . . 45Accu-Chek Test Strips . . . . . . . . . . . . 32AccuNeb . . . . . . . . . . . . . . . . . . . . . . . 45Accuretic . . . . . . . . . . . . . . . . . . . . . . . 23Accutane . . . . . . . . . . . . . . . . . . . . . . . 26Acebutolol . . . . . . . . . . . . . . . . . . . . . . 21Acetaminophen/Caffeine/Butalbital
325-50-40 mg . . . . . . . . . . . . . . . . . 13Acetazolamide . . . . . . . . . . . . . . . . . . . 42Acetazolamide Sustained-Action
Capsule . . . . . . . . . . . . . . . . . . . . . . . 42Acetic Acid/Hydrocortisone . . . . . . . . 29Achromycin V . . . . . . . . . . . . . . . . . . . . . 7Aciphex . . . . . . . . . . . . . . . . . . . . . . . . . 33Acitretin . . . . . . . . . . . . . . . . . . . . . . . . 27Aclovate . . . . . . . . . . . . . . . . . . . . . . . . 26Actemra . . . . . . . . . . . . . . . . . . . . . . . . 36Acthar H .P . . . . . . . . . . . . . . . . . . . . . . . 30Acticlate . . . . . . . . . . . . . . . . . . . . . . . . . 7Actigall . . . . . . . . . . . . . . . . . . . . . . . . . 34Actimmune . . . . . . . . . . . . . . . . . . . . . . 35Actiq . . . . . . . . . . . . . . . . . . . . . . . . . . . 13Activella . . . . . . . . . . . . . . . . . . . . . . . . 40Actonel . . . . . . . . . . . . . . . . . . . . . . . . . 37Actoplus Met . . . . . . . . . . . . . . . . . . . . 31Actoplus Met XR . . . . . . . . . . . . . . . . . 31Actos . . . . . . . . . . . . . . . . . . . . . . . . . . . 31Acular . . . . . . . . . . . . . . . . . . . . . . . . . . 42Acular LS . . . . . . . . . . . . . . . . . . . . . . . 42Acyclovir Capsule . . . . . . . . . . . . . . . . . 8Acyclovir Ointment . . . . . . . . . . . . . . . 27Aczone 5% . . . . . . . . . . . . . . . . . . . . . . 26Aczone 7 .5% . . . . . . . . . . . . . . . . . . . . 26Adapalene Cream, Gel, Lotion . . . . . . 26Adapalene/Benzoyl Peroxide Gel
0 .1%-2 .5% . . . . . . . . . . . . . . . . . . . . 26Adcirca . . . . . . . . . . . . . . . . . . . . . . . . . 46Adderall . . . . . . . . . . . . . . . . . . . . . . . . 19Adderall XR . . . . . . . . . . . . . . . . . . . . . 19Addyi . . . . . . . . . . . . . . . . . . . . . . . . . . . 47Adefovir . . . . . . . . . . . . . . . . . . . . . . . . . 8Adempas . . . . . . . . . . . . . . . . . . . . . . . 45Adlyxin . . . . . . . . . . . . . . . . . . . . . . . . . . 31Adoxa . . . . . . . . . . . . . . . . . . . . . . . . . . . 7Adoxa, Monodox . . . . . . . . . . . . . . . . . . 7
Adrenaclick . . . . . . . . . . . . . . . . . . . . . . 44Advair Diskus . . . . . . . . . . . . . . . . . . . . 46Advair HFA . . . . . . . . . . . . . . . . . . . . . . 46Advate . . . . . . . . . . . . . . . . . . . . . . . . . . 21Adynovate . . . . . . . . . . . . . . . . . . . . . . . 21Adzenys ER Suspension . . . . . . . . . . . 19Adzenys XR-ODT . . . . . . . . . . . . . . . . 19Afinitor . . . . . . . . . . . . . . . . . . . . . . . . . 12Afstyla . . . . . . . . . . . . . . . . . . . . . . . . . . 21Aftera . . . . . . . . . . . . . . . . . . . . . . . . . . 39Agrylin . . . . . . . . . . . . . . . . . . . . . . . . . . 49AirDuo RespiClick . . . . . . . . . . . . . 45, 46Akynzeo . . . . . . . . . . . . . . . . . . . . . . . . 34Albenza . . . . . . . . . . . . . . . . . . . . . . . . . 10Albuterol . . . . . . . . . . . . . . . . . . . . . . . . 45Albuterol Inhalation Solution . . . . . . . . 45Albuterol Sulfate/Ipratropium
Inhalation Solution . . . . . . . . . . . . . . 45Alclometasone Dipropionate Cream,
Ointment . . . . . . . . . . . . . . . . . . . . . . 26Aldactazide 25-25 mg . . . . . . . . . . . . 21Aldactazide 50-50 mg . . . . . . . . . . . . 21Aldactone . . . . . . . . . . . . . . . . . . . . . . . 21Aldara . . . . . . . . . . . . . . . . . . . . . . . . . . 28Alecensa . . . . . . . . . . . . . . . . . . . . . . . . 12Alendronate . . . . . . . . . . . . . . . . . . . . . 37Alferon N . . . . . . . . . . . . . . . . . . . . . . . 35Alfuzosin HCl . . . . . . . . . . . . . . . . . . . . 47Alinia . . . . . . . . . . . . . . . . . . . . . . . . . . . 10Allopurinol . . . . . . . . . . . . . . . . . . . . . . . 36Almotriptan . . . . . . . . . . . . . . . . . . . . . . 14Alogliptin . . . . . . . . . . . . . . . . . . . . . . . . 31Alogliptin/Metformin . . . . . . . . . . . . . . 31Alogliptin/Pioglitazone . . . . . . . . . . . . 31Alora . . . . . . . . . . . . . . . . . . . . . . . . . . . 40Alosetron . . . . . . . . . . . . . . . . . . . . . . . 34Alphagan P . . . . . . . . . . . . . . . . . . . . . . 43Alphanate vonWillebrand . . . . . . . . . . 21Alphanine SD . . . . . . . . . . . . . . . . . . . . 21Alprazolam . . . . . . . . . . . . . . . . . . . . . . 19Alprazolam Sustained-Release
24 Hour Tablet . . . . . . . . . . . . . . . . . 19Alprolix . . . . . . . . . . . . . . . . . . . . . . . . . 21Alrex . . . . . . . . . . . . . . . . . . . . . . . . . . . 43Altace . . . . . . . . . . . . . . . . . . . . . . . . . . 22Altavera . . . . . . . . . . . . . . . . . . . . . . . . . 38Alunbrig . . . . . . . . . . . . . . . . . . . . . . . . 12Alupent . . . . . . . . . . . . . . . . . . . . . . . . . 45Alvesco . . . . . . . . . . . . . . . . . . . . . . . . . 45Alyacen 1/35 . . . . . . . . . . . . . . . . . . . . 38Alyacen 7/7/7 . . . . . . . . . . . . . . . . . . . 38Amantadine . . . . . . . . . . . . . . . . . . . 8, 15
Amantadine HCl . . . . . . . . . . . . . . . . . . 8Amaryl . . . . . . . . . . . . . . . . . . . . . . . . . . 31Ambien . . . . . . . . . . . . . . . . . . . . . . . . . 17Ambien CR . . . . . . . . . . . . . . . . . . . . . . 17Amcinonide Cream, Lotion . . . . . . . . . 25Amcinonide Ointment . . . . . . . . . . . . . 25Amerge . . . . . . . . . . . . . . . . . . . . . . . . . 14Amethia . . . . . . . . . . . . . . . . . . . . . . . . . 39Amethia Lo . . . . . . . . . . . . . . . . . . . . . . 39Amiloride . . . . . . . . . . . . . . . . . . . . . . . . 21Amiloride/Hydrochlorothiazide . . . . . . 21Amiodarone . . . . . . . . . . . . . . . . . . . . . 20Amitiza . . . . . . . . . . . . . . . . . . . . . . . . . 34Amitriptyline . . . . . . . . . . . . . . . . . . . . . 17Amlodipine . . . . . . . . . . . . . . . . . . . 22, 23Amlodipine-Valsartan . . . . . . . . . . . . . 23Amlodipine-Valsartan-
Hydrochlorothiazide . . . . . . . . . . . . . 23Amlodipine/Benazepril . . . . . . . . . . . . 23Amoxicillin Clavulanate ER Sustained-
Release 12 Hour Tablet . . . . . . . . . . . 7Amoxicillin Extended-Release Tablet . . 7Amoxicillin Trihydrate Capsule,
Chewable Tablet, Suspension, Tablet . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Amoxicillin Trihydrate/Potassium Clavulanate . . . . . . . . . . . . . . . . . . . . . 7
Amoxil . . . . . . . . . . . . . . . . . . . . . . . . . . . 7Amphetamine Aspartate/Amphetamine
Sulfate/Dextroamphetamine Sustained-Release 24 Hour Capsule . . . . . . . . . . . . . . . . . . . . . . . 19
Amphetamine Aspartate/Amphetamine Sulfate/Dextroamphetamine Tablet . . . . . . . . . . . . . . . . . . . . . . . . . 19
Ampyra . . . . . . . . . . . . . . . . . . . . . . . . . 16Anafranil . . . . . . . . . . . . . . . . . . . . . . . . 17Anagrelide HCl . . . . . . . . . . . . . . . . . . 49Analpram-HC . . . . . . . . . . . . . . . . . . . . 34Anaprox . . . . . . . . . . . . . . . . . . . . . . . . . 36Anastrozole Tablet . . . . . . . . . . . . . . . . 11Androderm . . . . . . . . . . . . . . . . . . . . . . 30Androgel . . . . . . . . . . . . . . . . . . . . . . . . 30Androgel 1 .62% . . . . . . . . . . . . . . . . . 30Android . . . . . . . . . . . . . . . . . . . . . . . . . 30Angeliq . . . . . . . . . . . . . . . . . . . . . . . . . 40Anoro Ellipta . . . . . . . . . . . . . . . . . . . . . 46Antabuse . . . . . . . . . . . . . . . . . . . . . . . 49Antara . . . . . . . . . . . . . . . . . . . . . . . . . . 24Antivert 50 mg . . . . . . . . . . . . . . . . . . . 34Anusol-HC . . . . . . . . . . . . . . . . . . . . . . 34Anusol-HC 2 .5% . . . . . . . . . . . . . . . . . 34
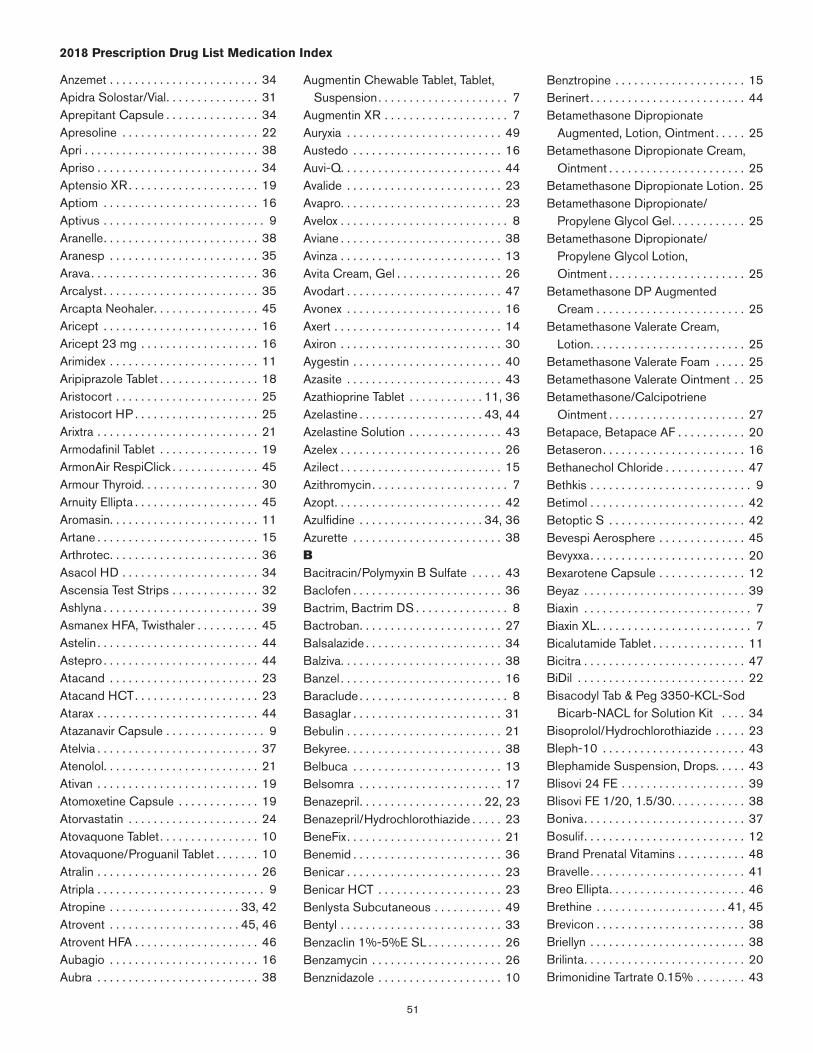
51
2018 Prescription Drug List Medication Index
Anzemet . . . . . . . . . . . . . . . . . . . . . . . . 34Apidra Solostar/Vial . . . . . . . . . . . . . . . 31Aprepitant Capsule . . . . . . . . . . . . . . . 34Apresoline . . . . . . . . . . . . . . . . . . . . . . 22Apri . . . . . . . . . . . . . . . . . . . . . . . . . . . . 38Apriso . . . . . . . . . . . . . . . . . . . . . . . . . . 34Aptensio XR . . . . . . . . . . . . . . . . . . . . . 19Aptiom . . . . . . . . . . . . . . . . . . . . . . . . . 16Aptivus . . . . . . . . . . . . . . . . . . . . . . . . . . 9Aranelle . . . . . . . . . . . . . . . . . . . . . . . . . 38Aranesp . . . . . . . . . . . . . . . . . . . . . . . . 35Arava . . . . . . . . . . . . . . . . . . . . . . . . . . . 36Arcalyst . . . . . . . . . . . . . . . . . . . . . . . . . 35Arcapta Neohaler . . . . . . . . . . . . . . . . . 45Aricept . . . . . . . . . . . . . . . . . . . . . . . . . 16Aricept 23 mg . . . . . . . . . . . . . . . . . . . 16Arimidex . . . . . . . . . . . . . . . . . . . . . . . . 11Aripiprazole Tablet . . . . . . . . . . . . . . . . 18Aristocort . . . . . . . . . . . . . . . . . . . . . . . 25Aristocort HP . . . . . . . . . . . . . . . . . . . . 25Arixtra . . . . . . . . . . . . . . . . . . . . . . . . . . 21Armodafinil Tablet . . . . . . . . . . . . . . . . 19ArmonAir RespiClick . . . . . . . . . . . . . . 45Armour Thyroid . . . . . . . . . . . . . . . . . . . 30Arnuity Ellipta . . . . . . . . . . . . . . . . . . . . 45Aromasin . . . . . . . . . . . . . . . . . . . . . . . . 11Artane . . . . . . . . . . . . . . . . . . . . . . . . . . 15Arthrotec . . . . . . . . . . . . . . . . . . . . . . . . 36Asacol HD . . . . . . . . . . . . . . . . . . . . . . 34Ascensia Test Strips . . . . . . . . . . . . . . 32Ashlyna . . . . . . . . . . . . . . . . . . . . . . . . . 39Asmanex HFA, Twisthaler . . . . . . . . . . 45Astelin . . . . . . . . . . . . . . . . . . . . . . . . . . 44Astepro . . . . . . . . . . . . . . . . . . . . . . . . . 44Atacand . . . . . . . . . . . . . . . . . . . . . . . . 23Atacand HCT . . . . . . . . . . . . . . . . . . . . 23Atarax . . . . . . . . . . . . . . . . . . . . . . . . . . 44Atazanavir Capsule . . . . . . . . . . . . . . . . 9Atelvia . . . . . . . . . . . . . . . . . . . . . . . . . . 37Atenolol . . . . . . . . . . . . . . . . . . . . . . . . . 21Ativan . . . . . . . . . . . . . . . . . . . . . . . . . . 19Atomoxetine Capsule . . . . . . . . . . . . . 19Atorvastatin . . . . . . . . . . . . . . . . . . . . . 24Atovaquone Tablet . . . . . . . . . . . . . . . . 10Atovaquone/Proguanil Tablet . . . . . . . 10Atralin . . . . . . . . . . . . . . . . . . . . . . . . . . 26Atripla . . . . . . . . . . . . . . . . . . . . . . . . . . . 9Atropine . . . . . . . . . . . . . . . . . . . . . 33, 42Atrovent . . . . . . . . . . . . . . . . . . . . . 45, 46Atrovent HFA . . . . . . . . . . . . . . . . . . . . 46Aubagio . . . . . . . . . . . . . . . . . . . . . . . . 16Aubra . . . . . . . . . . . . . . . . . . . . . . . . . . 38
Augmentin Chewable Tablet, Tablet, Suspension . . . . . . . . . . . . . . . . . . . . . 7
Augmentin XR . . . . . . . . . . . . . . . . . . . . 7Auryxia . . . . . . . . . . . . . . . . . . . . . . . . . 49Austedo . . . . . . . . . . . . . . . . . . . . . . . . 16Auvi-Q . . . . . . . . . . . . . . . . . . . . . . . . . . 44Avalide . . . . . . . . . . . . . . . . . . . . . . . . . 23Avapro . . . . . . . . . . . . . . . . . . . . . . . . . . 23Avelox . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Aviane . . . . . . . . . . . . . . . . . . . . . . . . . . 38Avinza . . . . . . . . . . . . . . . . . . . . . . . . . . 13Avita Cream, Gel . . . . . . . . . . . . . . . . . 26Avodart . . . . . . . . . . . . . . . . . . . . . . . . . 47Avonex . . . . . . . . . . . . . . . . . . . . . . . . . 16Axert . . . . . . . . . . . . . . . . . . . . . . . . . . . 14Axiron . . . . . . . . . . . . . . . . . . . . . . . . . . 30Aygestin . . . . . . . . . . . . . . . . . . . . . . . . 40Azasite . . . . . . . . . . . . . . . . . . . . . . . . . 43Azathioprine Tablet . . . . . . . . . . . . 11, 36Azelastine . . . . . . . . . . . . . . . . . . . . 43, 44Azelastine Solution . . . . . . . . . . . . . . . 43Azelex . . . . . . . . . . . . . . . . . . . . . . . . . . 26Azilect . . . . . . . . . . . . . . . . . . . . . . . . . . 15Azithromycin . . . . . . . . . . . . . . . . . . . . . . 7Azopt . . . . . . . . . . . . . . . . . . . . . . . . . . . 42Azulfidine . . . . . . . . . . . . . . . . . . . . 34, 36Azurette . . . . . . . . . . . . . . . . . . . . . . . . 38BBacitracin/Polymyxin B Sulfate . . . . . 43Baclofen . . . . . . . . . . . . . . . . . . . . . . . . 36Bactrim, Bactrim DS . . . . . . . . . . . . . . . 8Bactroban . . . . . . . . . . . . . . . . . . . . . . . 27Balsalazide . . . . . . . . . . . . . . . . . . . . . . 34Balziva . . . . . . . . . . . . . . . . . . . . . . . . . . 38Banzel . . . . . . . . . . . . . . . . . . . . . . . . . . 16Baraclude . . . . . . . . . . . . . . . . . . . . . . . . 8Basaglar . . . . . . . . . . . . . . . . . . . . . . . . 31Bebulin . . . . . . . . . . . . . . . . . . . . . . . . . 21Bekyree . . . . . . . . . . . . . . . . . . . . . . . . . 38Belbuca . . . . . . . . . . . . . . . . . . . . . . . . 13Belsomra . . . . . . . . . . . . . . . . . . . . . . . 17Benazepril . . . . . . . . . . . . . . . . . . . . 22, 23Benazepril/Hydrochlorothiazide . . . . . 23BeneFix . . . . . . . . . . . . . . . . . . . . . . . . . 21Benemid . . . . . . . . . . . . . . . . . . . . . . . . 36Benicar . . . . . . . . . . . . . . . . . . . . . . . . . 23Benicar HCT . . . . . . . . . . . . . . . . . . . . 23Benlysta Subcutaneous . . . . . . . . . . . 49Bentyl . . . . . . . . . . . . . . . . . . . . . . . . . . 33Benzaclin 1%-5%E SL . . . . . . . . . . . . 26Benzamycin . . . . . . . . . . . . . . . . . . . . . 26Benznidazole . . . . . . . . . . . . . . . . . . . . 10
Benztropine . . . . . . . . . . . . . . . . . . . . . 15Berinert . . . . . . . . . . . . . . . . . . . . . . . . . 44Betamethasone Dipropionate
Augmented, Lotion, Ointment . . . . . 25Betamethasone Dipropionate Cream,
Ointment . . . . . . . . . . . . . . . . . . . . . . 25Betamethasone Dipropionate Lotion . 25Betamethasone Dipropionate/
Propylene Glycol Gel . . . . . . . . . . . . 25Betamethasone Dipropionate/
Propylene Glycol Lotion, Ointment . . . . . . . . . . . . . . . . . . . . . . 25
Betamethasone DP Augmented Cream . . . . . . . . . . . . . . . . . . . . . . . . 25
Betamethasone Valerate Cream, Lotion . . . . . . . . . . . . . . . . . . . . . . . . . 25
Betamethasone Valerate Foam . . . . . 25Betamethasone Valerate Ointment . . 25Betamethasone/Calcipotriene
Ointment . . . . . . . . . . . . . . . . . . . . . . 27Betapace, Betapace AF . . . . . . . . . . . 20Betaseron . . . . . . . . . . . . . . . . . . . . . . . 16Bethanechol Chloride . . . . . . . . . . . . . 47Bethkis . . . . . . . . . . . . . . . . . . . . . . . . . . 9Betimol . . . . . . . . . . . . . . . . . . . . . . . . . 42Betoptic S . . . . . . . . . . . . . . . . . . . . . . 42Bevespi Aerosphere . . . . . . . . . . . . . . 45Bevyxxa . . . . . . . . . . . . . . . . . . . . . . . . . 20Bexarotene Capsule . . . . . . . . . . . . . . 12Beyaz . . . . . . . . . . . . . . . . . . . . . . . . . . 39Biaxin . . . . . . . . . . . . . . . . . . . . . . . . . . . 7Biaxin XL . . . . . . . . . . . . . . . . . . . . . . . . . 7Bicalutamide Tablet . . . . . . . . . . . . . . . 11Bicitra . . . . . . . . . . . . . . . . . . . . . . . . . . 47BiDil . . . . . . . . . . . . . . . . . . . . . . . . . . . 22Bisacodyl Tab & Peg 3350-KCL-Sod
Bicarb-NACL for Solution Kit . . . . 34Bisoprolol/Hydrochlorothiazide . . . . . 23Bleph-10 . . . . . . . . . . . . . . . . . . . . . . . 43Blephamide Suspension, Drops . . . . . 43Blisovi 24 FE . . . . . . . . . . . . . . . . . . . . 39Blisovi FE 1/20, 1 .5/30 . . . . . . . . . . . . 38Boniva . . . . . . . . . . . . . . . . . . . . . . . . . . 37Bosulif . . . . . . . . . . . . . . . . . . . . . . . . . . 12Brand Prenatal Vitamins . . . . . . . . . . . 48Bravelle . . . . . . . . . . . . . . . . . . . . . . . . . 41Breo Ellipta . . . . . . . . . . . . . . . . . . . . . . 46Brethine . . . . . . . . . . . . . . . . . . . . . 41, 45Brevicon . . . . . . . . . . . . . . . . . . . . . . . . 38Briellyn . . . . . . . . . . . . . . . . . . . . . . . . . 38Brilinta . . . . . . . . . . . . . . . . . . . . . . . . . . 20Brimonidine Tartrate 0 .15% . . . . . . . . 43
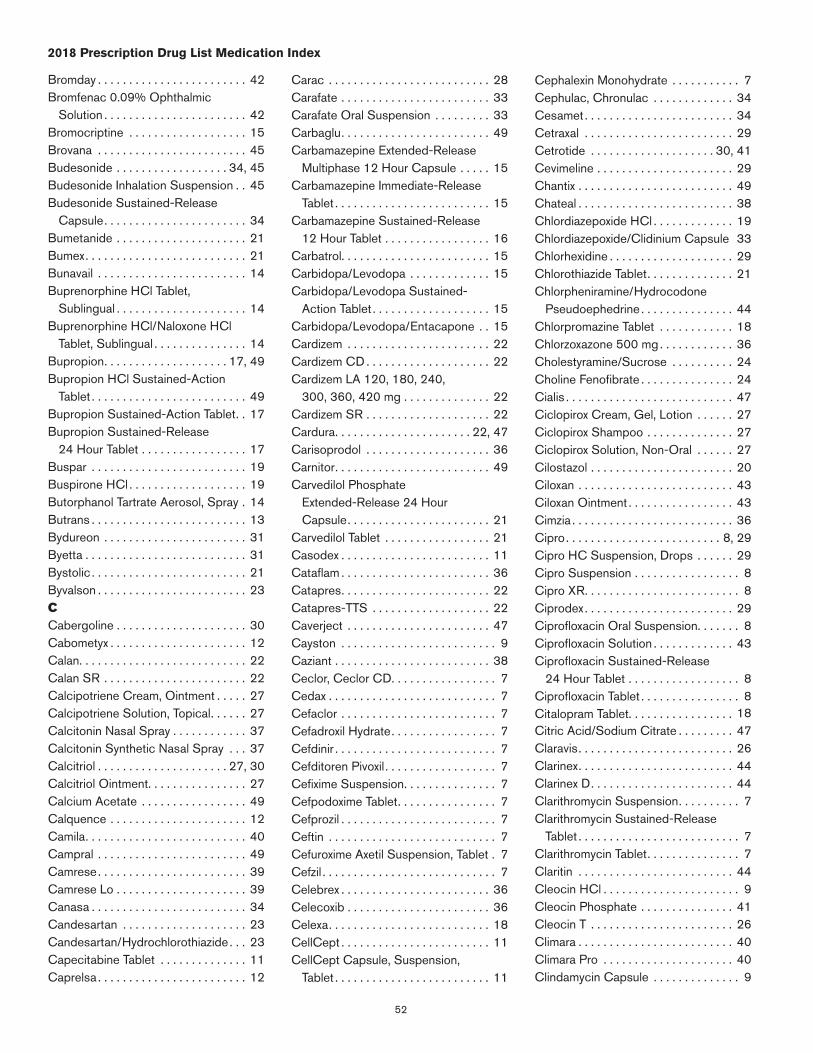
52
2018 Prescription Drug List Medication Index
Bromday . . . . . . . . . . . . . . . . . . . . . . . . 42Bromfenac 0 .09% Ophthalmic
Solution . . . . . . . . . . . . . . . . . . . . . . . 42Bromocriptine . . . . . . . . . . . . . . . . . . . 15Brovana . . . . . . . . . . . . . . . . . . . . . . . . 45Budesonide . . . . . . . . . . . . . . . . . . 34, 45Budesonide Inhalation Suspension . . 45Budesonide Sustained-Release
Capsule . . . . . . . . . . . . . . . . . . . . . . . 34Bumetanide . . . . . . . . . . . . . . . . . . . . . 21Bumex . . . . . . . . . . . . . . . . . . . . . . . . . . 21Bunavail . . . . . . . . . . . . . . . . . . . . . . . . 14Buprenorphine HCl Tablet,
Sublingual . . . . . . . . . . . . . . . . . . . . . 14Buprenorphine HCl/Naloxone HCl
Tablet, Sublingual . . . . . . . . . . . . . . . 14Bupropion . . . . . . . . . . . . . . . . . . . . 17, 49Bupropion HCl Sustained-Action
Tablet . . . . . . . . . . . . . . . . . . . . . . . . . 49Bupropion Sustained-Action Tablet . . 17Bupropion Sustained-Release
24 Hour Tablet . . . . . . . . . . . . . . . . . 17Buspar . . . . . . . . . . . . . . . . . . . . . . . . . 19Buspirone HCl . . . . . . . . . . . . . . . . . . . 19Butorphanol Tartrate Aerosol, Spray . 14Butrans . . . . . . . . . . . . . . . . . . . . . . . . . 13Bydureon . . . . . . . . . . . . . . . . . . . . . . . 31Byetta . . . . . . . . . . . . . . . . . . . . . . . . . . 31Bystolic . . . . . . . . . . . . . . . . . . . . . . . . . 21Byvalson . . . . . . . . . . . . . . . . . . . . . . . . 23CCabergoline . . . . . . . . . . . . . . . . . . . . . 30Cabometyx . . . . . . . . . . . . . . . . . . . . . . 12Calan . . . . . . . . . . . . . . . . . . . . . . . . . . . 22Calan SR . . . . . . . . . . . . . . . . . . . . . . . 22Calcipotriene Cream, Ointment . . . . . 27Calcipotriene Solution, Topical . . . . . . 27Calcitonin Nasal Spray . . . . . . . . . . . . 37Calcitonin Synthetic Nasal Spray . . . 37Calcitriol . . . . . . . . . . . . . . . . . . . . . 27, 30Calcitriol Ointment . . . . . . . . . . . . . . . . 27Calcium Acetate . . . . . . . . . . . . . . . . . 49Calquence . . . . . . . . . . . . . . . . . . . . . . 12Camila . . . . . . . . . . . . . . . . . . . . . . . . . . 40Campral . . . . . . . . . . . . . . . . . . . . . . . . 49Camrese . . . . . . . . . . . . . . . . . . . . . . . . 39Camrese Lo . . . . . . . . . . . . . . . . . . . . . 39Canasa . . . . . . . . . . . . . . . . . . . . . . . . . 34Candesartan . . . . . . . . . . . . . . . . . . . . 23Candesartan/Hydrochlorothiazide . . . 23Capecitabine Tablet . . . . . . . . . . . . . . 11Caprelsa . . . . . . . . . . . . . . . . . . . . . . . . 12
Carac . . . . . . . . . . . . . . . . . . . . . . . . . . 28Carafate . . . . . . . . . . . . . . . . . . . . . . . . 33Carafate Oral Suspension . . . . . . . . . 33Carbaglu . . . . . . . . . . . . . . . . . . . . . . . . 49Carbamazepine Extended-Release
Multiphase 12 Hour Capsule . . . . . 15Carbamazepine Immediate-Release
Tablet . . . . . . . . . . . . . . . . . . . . . . . . . 15Carbamazepine Sustained-Release
12 Hour Tablet . . . . . . . . . . . . . . . . . 16Carbatrol . . . . . . . . . . . . . . . . . . . . . . . . 15Carbidopa/Levodopa . . . . . . . . . . . . . 15Carbidopa/Levodopa Sustained-
Action Tablet . . . . . . . . . . . . . . . . . . . 15Carbidopa/Levodopa/Entacapone . . 15Cardizem . . . . . . . . . . . . . . . . . . . . . . . 22Cardizem CD . . . . . . . . . . . . . . . . . . . . 22Cardizem LA 120, 180, 240,
300, 360, 420 mg . . . . . . . . . . . . . . 22Cardizem SR . . . . . . . . . . . . . . . . . . . . 22Cardura . . . . . . . . . . . . . . . . . . . . . . 22, 47Carisoprodol . . . . . . . . . . . . . . . . . . . . 36Carnitor . . . . . . . . . . . . . . . . . . . . . . . . . 49Carvedilol Phosphate
Extended-Release 24 Hour Capsule . . . . . . . . . . . . . . . . . . . . . . . 21
Carvedilol Tablet . . . . . . . . . . . . . . . . . 21Casodex . . . . . . . . . . . . . . . . . . . . . . . . 11Cataflam . . . . . . . . . . . . . . . . . . . . . . . . 36Catapres . . . . . . . . . . . . . . . . . . . . . . . . 22Catapres-TTS . . . . . . . . . . . . . . . . . . . 22Caverject . . . . . . . . . . . . . . . . . . . . . . . 47Cayston . . . . . . . . . . . . . . . . . . . . . . . . . 9Caziant . . . . . . . . . . . . . . . . . . . . . . . . . 38Ceclor, Ceclor CD . . . . . . . . . . . . . . . . . 7Cedax . . . . . . . . . . . . . . . . . . . . . . . . . . . 7Cefaclor . . . . . . . . . . . . . . . . . . . . . . . . . 7Cefadroxil Hydrate . . . . . . . . . . . . . . . . . 7Cefdinir . . . . . . . . . . . . . . . . . . . . . . . . . . 7Cefditoren Pivoxil . . . . . . . . . . . . . . . . . . 7Cefixime Suspension . . . . . . . . . . . . . . . 7Cefpodoxime Tablet . . . . . . . . . . . . . . . . 7Cefprozil . . . . . . . . . . . . . . . . . . . . . . . . . 7Ceftin . . . . . . . . . . . . . . . . . . . . . . . . . . . 7Cefuroxime Axetil Suspension, Tablet . 7Cefzil . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7Celebrex . . . . . . . . . . . . . . . . . . . . . . . . 36Celecoxib . . . . . . . . . . . . . . . . . . . . . . . 36Celexa . . . . . . . . . . . . . . . . . . . . . . . . . . 18CellCept . . . . . . . . . . . . . . . . . . . . . . . . 11CellCept Capsule, Suspension,
Tablet . . . . . . . . . . . . . . . . . . . . . . . . . 11
Cephalexin Monohydrate . . . . . . . . . . . 7Cephulac, Chronulac . . . . . . . . . . . . . 34Cesamet . . . . . . . . . . . . . . . . . . . . . . . . 34Cetraxal . . . . . . . . . . . . . . . . . . . . . . . . 29Cetrotide . . . . . . . . . . . . . . . . . . . . 30, 41Cevimeline . . . . . . . . . . . . . . . . . . . . . . 29Chantix . . . . . . . . . . . . . . . . . . . . . . . . . 49Chateal . . . . . . . . . . . . . . . . . . . . . . . . . 38Chlordiazepoxide HCl . . . . . . . . . . . . . 19Chlordiazepoxide/Clidinium Capsule 33Chlorhexidine . . . . . . . . . . . . . . . . . . . . 29Chlorothiazide Tablet . . . . . . . . . . . . . . 21Chlorpheniramine/Hydrocodone
Pseudoephedrine . . . . . . . . . . . . . . . 44Chlorpromazine Tablet . . . . . . . . . . . . 18Chlorzoxazone 500 mg . . . . . . . . . . . . 36Cholestyramine/Sucrose . . . . . . . . . . 24Choline Fenofibrate . . . . . . . . . . . . . . . 24Cialis . . . . . . . . . . . . . . . . . . . . . . . . . . . 47Ciclopirox Cream, Gel, Lotion . . . . . . 27Ciclopirox Shampoo . . . . . . . . . . . . . . 27Ciclopirox Solution, Non-Oral . . . . . . 27Cilostazol . . . . . . . . . . . . . . . . . . . . . . . 20Ciloxan . . . . . . . . . . . . . . . . . . . . . . . . . 43Ciloxan Ointment . . . . . . . . . . . . . . . . . 43Cimzia . . . . . . . . . . . . . . . . . . . . . . . . . . 36Cipro . . . . . . . . . . . . . . . . . . . . . . . . . 8, 29Cipro HC Suspension, Drops . . . . . . 29Cipro Suspension . . . . . . . . . . . . . . . . . 8Cipro XR . . . . . . . . . . . . . . . . . . . . . . . . . 8Ciprodex . . . . . . . . . . . . . . . . . . . . . . . . 29Ciprofloxacin Oral Suspension . . . . . . . 8Ciprofloxacin Solution . . . . . . . . . . . . . 43Ciprofloxacin Sustained-Release
24 Hour Tablet . . . . . . . . . . . . . . . . . . 8Ciprofloxacin Tablet . . . . . . . . . . . . . . . . 8Citalopram Tablet . . . . . . . . . . . . . . . . . 18Citric Acid/Sodium Citrate . . . . . . . . . 47Claravis . . . . . . . . . . . . . . . . . . . . . . . . . 26Clarinex . . . . . . . . . . . . . . . . . . . . . . . . . 44Clarinex D . . . . . . . . . . . . . . . . . . . . . . . 44Clarithromycin Suspension . . . . . . . . . . 7Clarithromycin Sustained-Release
Tablet . . . . . . . . . . . . . . . . . . . . . . . . . . 7Clarithromycin Tablet . . . . . . . . . . . . . . . 7Claritin . . . . . . . . . . . . . . . . . . . . . . . . . 44Cleocin HCl . . . . . . . . . . . . . . . . . . . . . . 9Cleocin Phosphate . . . . . . . . . . . . . . . 41Cleocin T . . . . . . . . . . . . . . . . . . . . . . . 26Climara . . . . . . . . . . . . . . . . . . . . . . . . . 40Climara Pro . . . . . . . . . . . . . . . . . . . . . 40Clindamycin Capsule . . . . . . . . . . . . . . 9

53
2018 Prescription Drug List Medication Index
Clindamycin Phosphate Cream w/Applicator . . . . . . . . . . . . . . . . . . . 41
Clindamycin Phosphate Cream, Solution, Swab . . . . . . . . . . . . . . . . . 26
Clindamycin Phosphate Foam 1% . . . 26Clindamycin Phosphate Gel . . . . . . . . 26Clindamycin Phosphate Lotion . . . . . . 26Clindamycin Phosphate/Benzoyl
Peroxide Gel . . . . . . . . . . . . . . . . . . . 26Clindamycin Phosphate/Benzoyl
Peroxide Gel 1 .2%-5% . . . . . . . . . . 26Clindesse . . . . . . . . . . . . . . . . . . . . . . . 41Clinoril . . . . . . . . . . . . . . . . . . . . . . . . . . 36Clobetasol Propionate Cream . . . . . . 25Clobetasol Propionate Cream, Gel,
Ointment, Solution . . . . . . . . . . . . . . 25Clobetasol Propionate Foam . . . . . . . 25Clobetasol Propionate Lotion,
Shampoo . . . . . . . . . . . . . . . . . . . . . . 25Clobetasol Propionate Solution . . . . . 25Clobex . . . . . . . . . . . . . . . . . . . . . . . . . . 25Clocortolone . . . . . . . . . . . . . . . . . . . . 25Cloderm . . . . . . . . . . . . . . . . . . . . . . . . 25Clomid . . . . . . . . . . . . . . . . . . . . . . . . . 41Clomiphene . . . . . . . . . . . . . . . . . . . . . 41Clomipramine . . . . . . . . . . . . . . . . . . . . 17Clonazepam Tablet . . . . . . . . . . . . . . . 15Clonidine . . . . . . . . . . . . . . . . . . . . 19, 22Clonidine Extended-Release Tablet . . 19Clonidine Transdermal Weekly
Patch . . . . . . . . . . . . . . . . . . . . . . . . . 22Clopidogrel . . . . . . . . . . . . . . . . . . . . . . 20Clotrimazole Troche . . . . . . . . . . . . . . . . 9Clotrimazole/Betamethasone
Dipropionate . . . . . . . . . . . . . . . . . . . 27Clozapine Tablet . . . . . . . . . . . . . . . . . 18Clozaril . . . . . . . . . . . . . . . . . . . . . . . . . 18Coagadex . . . . . . . . . . . . . . . . . . . . . . . 21Coartem . . . . . . . . . . . . . . . . . . . . . . . . 10Codeine Phosphate/Acetaminophen . 13Codeine Sulfate . . . . . . . . . . . . . . . . . . 13Codeine/Promethazine . . . . . . . . . . . . 44Cogentin . . . . . . . . . . . . . . . . . . . . . . . . 15Colazal . . . . . . . . . . . . . . . . . . . . . . . . . 34Colcrys . . . . . . . . . . . . . . . . . . . . . . . . . 36Colestid . . . . . . . . . . . . . . . . . . . . . . . . 24Colestipol . . . . . . . . . . . . . . . . . . . . . . . 24Coly-Mycin S Suspension, Drops . . . 29Colyte . . . . . . . . . . . . . . . . . . . . . . . . . . 34Combigan . . . . . . . . . . . . . . . . . . . . . . . 42Combipatch . . . . . . . . . . . . . . . . . . . . . 40Combivent Respimat . . . . . . . . . . . . . . 46
Combivir . . . . . . . . . . . . . . . . . . . . . . . . . 9Cometriq . . . . . . . . . . . . . . . . . . . . . . . . 12Compazine . . . . . . . . . . . . . . . . . . . . . . 34Complera . . . . . . . . . . . . . . . . . . . . . . . . 9Concerta . . . . . . . . . . . . . . . . . . . . . . . 19Condylox Gel . . . . . . . . . . . . . . . . . . . . 28Condylox Liquid . . . . . . . . . . . . . . . . . . 28Contour Next . . . . . . . . . . . . . . . . . . . . 32Contour Next EZ . . . . . . . . . . . . . . . . . 32Contour Next One . . . . . . . . . . . . . . . . 32Contour Next Test Strips . . . . . . . . . . 32Contour Test Strips . . . . . . . . . . . . . . . 32Copaxone . . . . . . . . . . . . . . . . . . . . . . . 16Copegus . . . . . . . . . . . . . . . . . . . . . . . . . 8Cordarone . . . . . . . . . . . . . . . . . . . . . . 20Cordran . . . . . . . . . . . . . . . . . . . . . . . . 25Coreg . . . . . . . . . . . . . . . . . . . . . . . . . . 21Coreg CR . . . . . . . . . . . . . . . . . . . . . . . 21Corgard . . . . . . . . . . . . . . . . . . . . . . . . 21Corlanor . . . . . . . . . . . . . . . . . . . . . . . . 24Cortef . . . . . . . . . . . . . . . . . . . . . . . . . . 30Cortenema . . . . . . . . . . . . . . . . . . . . . . 34Cortifoam . . . . . . . . . . . . . . . . . . . . . . . 34Cortisporin . . . . . . . . . . . . . . . . . . . 29, 43Cosentyx . . . . . . . . . . . . . . . . . . . . . . . . 36Cosopt . . . . . . . . . . . . . . . . . . . . . . . . . 42Cotellic . . . . . . . . . . . . . . . . . . . . . . . . . 12Cotempla XR-ODT . . . . . . . . . . . . . . . 19Coumadin . . . . . . . . . . . . . . . . . . . . . . . 20Cozaar . . . . . . . . . . . . . . . . . . . . . . . . . 23Creon . . . . . . . . . . . . . . . . . . . . . . . . . . 34Cresemba . . . . . . . . . . . . . . . . . . . . . . . . 9Crestor . . . . . . . . . . . . . . . . . . . . . . . . . 24Crinone . . . . . . . . . . . . . . . . . . . . . . . . 40Crixivan . . . . . . . . . . . . . . . . . . . . . . . . . . 9Cryselle-28 . . . . . . . . . . . . . . . . . . . . . . 38Cutivate . . . . . . . . . . . . . . . . . . . . . . . . 25Cyclafem 1/35 . . . . . . . . . . . . . . . . . . . 38Cyclafem 7/7/7 . . . . . . . . . . . . . . . . . . 38Cyclesa . . . . . . . . . . . . . . . . . . . . . . . . . 38Cyclobenzaprine . . . . . . . . . . . . . . . . . 36Cyclocort . . . . . . . . . . . . . . . . . . . . . . . 25Cyclogyl . . . . . . . . . . . . . . . . . . . . . . . . 42Cyclopentolate . . . . . . . . . . . . . . . . . . . 42Cyclophosphamide Capsule . . . . . . . 11Cyclosporine, Modified . . . . . . . . . . . . 11Cymbalta . . . . . . . . . . . . . . . . . . . . . . . 17Cyproheptadine . . . . . . . . . . . . . . . . . . 44Cyred . . . . . . . . . . . . . . . . . . . . . . . . . . 38Cystagon . . . . . . . . . . . . . . . . . . . . . . . 47Cytomel . . . . . . . . . . . . . . . . . . . . . . . . 30Cytotec . . . . . . . . . . . . . . . . . . . . . . . . . 33
Cytovene . . . . . . . . . . . . . . . . . . . . . . . . 8DDaklinza . . . . . . . . . . . . . . . . . . . . . . . . . 8Daliresp . . . . . . . . . . . . . . . . . . . . . . . . 46Dapsone . . . . . . . . . . . . . . . . . . . . . . 9, 26Dapsone 5% Gel . . . . . . . . . . . . . . . . . 26Daraprim . . . . . . . . . . . . . . . . . . . . . . . . 10Darifenacin Extended-Release . . . . . . 47Dasetta 1/35 . . . . . . . . . . . . . . . . . . . . 38Dasetta 7/7/7 . . . . . . . . . . . . . . . . . . . 38Daypro . . . . . . . . . . . . . . . . . . . . . . . . . 36Daysee . . . . . . . . . . . . . . . . . . . . . . . . . 39Daytrana . . . . . . . . . . . . . . . . . . . . . . . . 19DDAVP . . . . . . . . . . . . . . . . . . . . . . . . . 30Deblitane . . . . . . . . . . . . . . . . . . . . . . . 40Decadron . . . . . . . . . . . . . . . . . . . . . . . 30Delya . . . . . . . . . . . . . . . . . . . . . . . . . . . 38Delzicol . . . . . . . . . . . . . . . . . . . . . . . . . 34Demerol . . . . . . . . . . . . . . . . . . . . . . . . 13Demulen . . . . . . . . . . . . . . . . . . . . . . . . 38Denavir . . . . . . . . . . . . . . . . . . . . . . . . . 27Depakene . . . . . . . . . . . . . . . . . . . . . . . 15Depakote . . . . . . . . . . . . . . . . . . . . 15, 16Depakote ER . . . . . . . . . . . . . . . . . 15, 16Depakote Sprinkle . . . . . . . . . . . . . . . . 15Depen . . . . . . . . . . . . . . . . . . . . . . . . . . 30Depo-Provera . . . . . . . . . . . . . . . . . . . . 40Depo-SubQ Provera 104 . . . . . . . . . . 40Derma-Smooth . . . . . . . . . . . . . . . . . . 25Derma-Smoothe/FS . . . . . . . . . . . . . . 26Dermatop . . . . . . . . . . . . . . . . . . . . . . . 25Descovy . . . . . . . . . . . . . . . . . . . . . . . . . 9Desipramine . . . . . . . . . . . . . . . . . . . . . 17Desloratadine . . . . . . . . . . . . . . . . . . . . 44Desmopressin . . . . . . . . . . . . . . . . . . . 30Desogen . . . . . . . . . . . . . . . . . . . . . . . . 38Desogestrel-Ethinyl Estradiol
0 .15/0 .03mg . . . . . . . . . . . . . . . . . . . 38Desogestrel-Ethinyl Estradiol/Ethinyl
Estradiol 0 .15/0 .02/0 .01mg . . . . . . 38Desonate . . . . . . . . . . . . . . . . . . . . . . . 26Desonide Cream, Ointment, Lotion . . 26DesOwen . . . . . . . . . . . . . . . . . . . . . . . 26Desoximetasone Cream . . . . . . . . . . . 25Desoximetasone Gel, Ointment . . . . . 25Desvenlafaxine Succinate
Sustained-Release Tablet . . . . . . . . 17Desyrel . . . . . . . . . . . . . . . . . . . . . . . . . 17Detrol LA . . . . . . . . . . . . . . . . . . . . . . . 47Dexamethasone . . . . . . . . . . . . . . . 30, 43Dexedrine . . . . . . . . . . . . . . . . . . . . . . . 19Dexilant . . . . . . . . . . . . . . . . . . . . . . . . . 33

54
2018 Prescription Drug List Medication Index
Dexmethylphenidate Extended-Release Capsule . . . . . . . 19
Dexmethylphenidate Immediate-Release Tablet . . . . . . . . 19
Dextroamphetamine Extended-Release Capsule . . . . . . . 19
Dextroamphetamine Immediate-Release Tablet . . . . . . . . 19
DiaBeta . . . . . . . . . . . . . . . . . . . . . . . . . 31Diamox . . . . . . . . . . . . . . . . . . . . . . . . . 42Diamox Sequel . . . . . . . . . . . . . . . . . . . 42Diastat Acudial . . . . . . . . . . . . . . . . . . . 15Diazepam . . . . . . . . . . . . . . . . . . . . 15, 19Diazepam, Rectal . . . . . . . . . . . . . . . . . 15Diclegis . . . . . . . . . . . . . . . . . . . . . . . . . 41Diclofenac 1 .5% Ophthalmic
Solution . . . . . . . . . . . . . . . . . . . . . . . 42Diclofenac 3% Gel . . . . . . . . . . . . . . . 28Diclofenac Sodium 1% Gel . . . . . . . . 36Diclofenac Sodium/Misoprostol . . . . . 36Diclofenac Sustained-Release 24 Hour
Tablet . . . . . . . . . . . . . . . . . . . . . . . . . 36Diclofenac Tablet . . . . . . . . . . . . . . . . . 36Dicyclomine Tablet . . . . . . . . . . . . . . . . 33Didanosine Enteric-Coated Capsule . . 9Differin . . . . . . . . . . . . . . . . . . . . . . . . . 26Dificid . . . . . . . . . . . . . . . . . . . . . . . . . . . 9Diflorasone Diacetate Cream . . . . . . . 25Diflorasone Diacetate Ointment . . . . . 25Diflucan . . . . . . . . . . . . . . . . . . . . . . . 9, 41Diflucan 150 mg . . . . . . . . . . . . . . . . . 41Digoxin . . . . . . . . . . . . . . . . . . . . . . . . . 20Dihydroergotamine Nasal Spray . . . . 14Dilacor XR . . . . . . . . . . . . . . . . . . . . . . 22Dilantin . . . . . . . . . . . . . . . . . . . . . . . . . 15Dilantin, Phenytek . . . . . . . . . . . . . . . . 15Dilaudid . . . . . . . . . . . . . . . . . . . . . . . . . 13Diltiazem . . . . . . . . . . . . . . . . . . . . . . . . 22Diltiazem Controlled-Release
Capsule . . . . . . . . . . . . . . . . . . . . . . . 22Diltiazem Sustained-Action
Capsule . . . . . . . . . . . . . . . . . . . . . . . 22Diltiazem Sustained-Release 12 Hour
Capsule . . . . . . . . . . . . . . . . . . . . . . . 22Diltiazem Sustained-Release 24 Hour
Capsule . . . . . . . . . . . . . . . . . . . . . . . 22Diltiazem Sustained-Release 24 Hour
Tablet . . . . . . . . . . . . . . . . . . . . . . . . . 22Diovan . . . . . . . . . . . . . . . . . . . . . . . . . . 23Diovan HCT . . . . . . . . . . . . . . . . . . . . . 23Diphenoxylate/Atropine Sulfate . . . . . 33Diprolene . . . . . . . . . . . . . . . . . . . . . . . 25
Diprolene AF Cream . . . . . . . . . . . . . . 25Diprosone . . . . . . . . . . . . . . . . . . . . . . . 25Dipyridamole . . . . . . . . . . . . . . . . . . . . 20Disulfiram . . . . . . . . . . . . . . . . . . . . . . . 49Ditropan . . . . . . . . . . . . . . . . . . . . . . . . 47Ditropan XL . . . . . . . . . . . . . . . . . . . . . 47Diuril . . . . . . . . . . . . . . . . . . . . . . . . . . . 21Divalproex Sodium . . . . . . . . . . . . . . . . 15Divalproex Sodium Sustained-Release
Tablet . . . . . . . . . . . . . . . . . . . . . . . . . 15Divalproex Sodium Tablet . . . . . . . . . . 15Divigel . . . . . . . . . . . . . . . . . . . . . . . . . . 40Dofetilide . . . . . . . . . . . . . . . . . . . . . . . 20Dolophine HCl . . . . . . . . . . . . . . . . . . . 13Donepezil 23 mg . . . . . . . . . . . . . . . . . 16Donepezil Tablet . . . . . . . . . . . . . . . . . 16Doryx . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7Dorzolamide . . . . . . . . . . . . . . . . . . . . . 42Dorzolamide/Timolol . . . . . . . . . . . . . . 42Dostinex . . . . . . . . . . . . . . . . . . . . . . . . 30Dovonex . . . . . . . . . . . . . . . . . . . . . . . . 27Doxazosin . . . . . . . . . . . . . . . . . . . . 22, 47Doxazosin Mesylate . . . . . . . . . . . . . . . 47Doxepin . . . . . . . . . . . . . . . . . . . . . . . . . 17Doxercalciferol . . . . . . . . . . . . . . . . . . . 30Doxycycline Hyclate 20 mg Tablet . . . . 7Doxycycline Hyclate 50, 100 mg . . . . . 7Doxycycline Hyclate 75, 150 mg . . . . . 7Doxycycline Hyclate Enteric-Coated
Tablet . . . . . . . . . . . . . . . . . . . . . . . . . . 7Doxycycline Monohydrate 50, 100 mg
Capsule . . . . . . . . . . . . . . . . . . . . . . . . 7Doxycycline Monohydrate Capsule . . . 7Dronabinol . . . . . . . . . . . . . . . . . . . . . . 34Drospirenone/Ethinyl Estradiol/
Levomefolate 3/0 .02/0 .451mg . . . . 39Drospirenone/Ethinyl Estradiol/
Levomefolate 3/0 .03/0 .451mg . . . . 39Duac . . . . . . . . . . . . . . . . . . . . . . . . . . . 26Duavee . . . . . . . . . . . . . . . . . . . . . . . . . 40Duetact . . . . . . . . . . . . . . . . . . . . . . . . . 31Dulera . . . . . . . . . . . . . . . . . . . . . . . . . . 46Duloxetine . . . . . . . . . . . . . . . . . . . . . . . 17Duoneb . . . . . . . . . . . . . . . . . . . . . . . . . 45Dupixent . . . . . . . . . . . . . . . . . . . . . . . . 28Duragesic . . . . . . . . . . . . . . . . . . . . . . . 13Durezol . . . . . . . . . . . . . . . . . . . . . . . . . 43Duricef . . . . . . . . . . . . . . . . . . . . . . . . . . 7Dutasteride . . . . . . . . . . . . . . . . . . . . . . 47Dyanavel XR . . . . . . . . . . . . . . . . . . . . . 19Dyazide . . . . . . . . . . . . . . . . . . . . . . . . . 21Dymista . . . . . . . . . . . . . . . . . . . . . . . . . 45
Dynacin . . . . . . . . . . . . . . . . . . . . . . . . . . 7EE .E .S . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7Econazole . . . . . . . . . . . . . . . . . . . . . . . 27Econtra EZ . . . . . . . . . . . . . . . . . . . . . . 39EContra One Step . . . . . . . . . . . . . . . 39Edarbi . . . . . . . . . . . . . . . . . . . . . . . . . . 23Edarbyclor . . . . . . . . . . . . . . . . . . . . . . 23Edex . . . . . . . . . . . . . . . . . . . . . . . . . . . 47Edurant . . . . . . . . . . . . . . . . . . . . . . . . . . 9Efavirenz . . . . . . . . . . . . . . . . . . . . . . . . . 9Effexor XR . . . . . . . . . . . . . . . . . . . . . . 17Effient . . . . . . . . . . . . . . . . . . . . . . . . . . 20Efudex . . . . . . . . . . . . . . . . . . . . . . . . . . 28Egrifta . . . . . . . . . . . . . . . . . . . . . . . . . . 35Elavil . . . . . . . . . . . . . . . . . . . . . . . . . . . 17Eldepryl . . . . . . . . . . . . . . . . . . . . . . . . . 15Elestrin . . . . . . . . . . . . . . . . . . . . . . . . . 40Eletriptan . . . . . . . . . . . . . . . . . . . . . . . 14Elidel . . . . . . . . . . . . . . . . . . . . . . . . . . . 28Elimite . . . . . . . . . . . . . . . . . . . . . . . . . . 27Elinest . . . . . . . . . . . . . . . . . . . . . . . . . . 38Eliquis . . . . . . . . . . . . . . . . . . . . . . . . . . 20Ella . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39Elmiron . . . . . . . . . . . . . . . . . . . . . . . . . 47Elocon . . . . . . . . . . . . . . . . . . . . . . . . . . 25Eloctate . . . . . . . . . . . . . . . . . . . . . . . . 21Embeda . . . . . . . . . . . . . . . . . . . . . . . . 13Emend . . . . . . . . . . . . . . . . . . . . . . . . . . 34Emend Suspension . . . . . . . . . . . . . . . 34Emgel . . . . . . . . . . . . . . . . . . . . . . . . . . 26Emla . . . . . . . . . . . . . . . . . . . . . . . . . . . 26Emoquette . . . . . . . . . . . . . . . . . . . . . . 38Emsam . . . . . . . . . . . . . . . . . . . . . . . . . 17Emtriva . . . . . . . . . . . . . . . . . . . . . . . . . . 9Emverm . . . . . . . . . . . . . . . . . . . . . . . . . 10Enablex . . . . . . . . . . . . . . . . . . . . . . . . . 47Enalapril Maleate . . . . . . . . . . . . . . . . . 22Enalapril/Hydrochlorothiazide . . . . . . . 23Enbrel . . . . . . . . . . . . . . . . . . . . . . . . . . 36Endometrin . . . . . . . . . . . . . . . . . . . . . 40Enoxaparin . . . . . . . . . . . . . . . . . . . . . . 21Enpresse-28 . . . . . . . . . . . . . . . . . . . . 38Enskyce . . . . . . . . . . . . . . . . . . . . . . . . 38Enstilar . . . . . . . . . . . . . . . . . . . . . . . . . 27Entecavir . . . . . . . . . . . . . . . . . . . . . . . . . 8Entocort EC . . . . . . . . . . . . . . . . . . . . . 34Entresto . . . . . . . . . . . . . . . . . . . . . . . . 24Epclusa . . . . . . . . . . . . . . . . . . . . . . . . . . 8Epiduo . . . . . . . . . . . . . . . . . . . . . . . . . 26Epinephrine Auto-Injector . . . . . . . . . . 44Epinephrine Autoinjector . . . . . . . . . . . 44
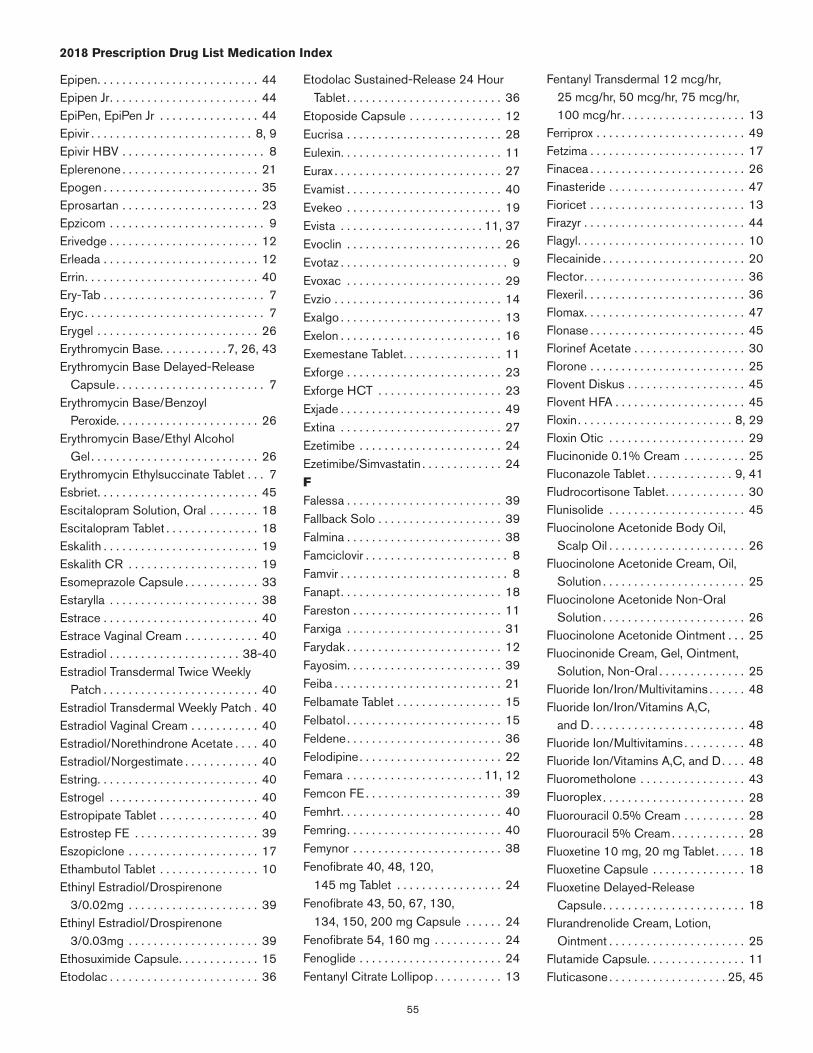
55
2018 Prescription Drug List Medication Index
Epipen . . . . . . . . . . . . . . . . . . . . . . . . . . 44Epipen Jr . . . . . . . . . . . . . . . . . . . . . . . . 44EpiPen, EpiPen Jr . . . . . . . . . . . . . . . . 44Epivir . . . . . . . . . . . . . . . . . . . . . . . . . . 8, 9Epivir HBV . . . . . . . . . . . . . . . . . . . . . . . 8Eplerenone . . . . . . . . . . . . . . . . . . . . . . 21Epogen . . . . . . . . . . . . . . . . . . . . . . . . . 35Eprosartan . . . . . . . . . . . . . . . . . . . . . . 23Epzicom . . . . . . . . . . . . . . . . . . . . . . . . . 9Erivedge . . . . . . . . . . . . . . . . . . . . . . . . 12Erleada . . . . . . . . . . . . . . . . . . . . . . . . . 12Errin . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40Ery-Tab . . . . . . . . . . . . . . . . . . . . . . . . . . 7Eryc . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7Erygel . . . . . . . . . . . . . . . . . . . . . . . . . . 26Erythromycin Base . . . . . . . . . . . 7, 26, 43Erythromycin Base Delayed-Release
Capsule . . . . . . . . . . . . . . . . . . . . . . . . 7Erythromycin Base/Benzoyl
Peroxide . . . . . . . . . . . . . . . . . . . . . . . 26Erythromycin Base/Ethyl Alcohol
Gel . . . . . . . . . . . . . . . . . . . . . . . . . . . 26Erythromycin Ethylsuccinate Tablet . . . 7Esbriet . . . . . . . . . . . . . . . . . . . . . . . . . . 45Escitalopram Solution, Oral . . . . . . . . 18Escitalopram Tablet . . . . . . . . . . . . . . . 18Eskalith . . . . . . . . . . . . . . . . . . . . . . . . . 19Eskalith CR . . . . . . . . . . . . . . . . . . . . . 19Esomeprazole Capsule . . . . . . . . . . . . 33Estarylla . . . . . . . . . . . . . . . . . . . . . . . . 38Estrace . . . . . . . . . . . . . . . . . . . . . . . . . 40Estrace Vaginal Cream . . . . . . . . . . . . 40Estradiol . . . . . . . . . . . . . . . . . . . . . 38-40Estradiol Transdermal Twice Weekly
Patch . . . . . . . . . . . . . . . . . . . . . . . . . 40Estradiol Transdermal Weekly Patch . 40Estradiol Vaginal Cream . . . . . . . . . . . 40Estradiol/Norethindrone Acetate . . . . 40Estradiol/Norgestimate . . . . . . . . . . . . 40Estring . . . . . . . . . . . . . . . . . . . . . . . . . . 40Estrogel . . . . . . . . . . . . . . . . . . . . . . . . 40Estropipate Tablet . . . . . . . . . . . . . . . . 40Estrostep FE . . . . . . . . . . . . . . . . . . . . 39Eszopiclone . . . . . . . . . . . . . . . . . . . . . 17Ethambutol Tablet . . . . . . . . . . . . . . . . 10Ethinyl Estradiol/Drospirenone
3/0 .02mg . . . . . . . . . . . . . . . . . . . . . 39Ethinyl Estradiol/Drospirenone
3/0 .03mg . . . . . . . . . . . . . . . . . . . . . 39Ethosuximide Capsule . . . . . . . . . . . . . 15Etodolac . . . . . . . . . . . . . . . . . . . . . . . . 36
Etodolac Sustained-Release 24 Hour Tablet . . . . . . . . . . . . . . . . . . . . . . . . . 36
Etoposide Capsule . . . . . . . . . . . . . . . 12Eucrisa . . . . . . . . . . . . . . . . . . . . . . . . . 28Eulexin . . . . . . . . . . . . . . . . . . . . . . . . . . 11Eurax . . . . . . . . . . . . . . . . . . . . . . . . . . . 27Evamist . . . . . . . . . . . . . . . . . . . . . . . . . 40Evekeo . . . . . . . . . . . . . . . . . . . . . . . . . 19Evista . . . . . . . . . . . . . . . . . . . . . . . 11, 37Evoclin . . . . . . . . . . . . . . . . . . . . . . . . . 26Evotaz . . . . . . . . . . . . . . . . . . . . . . . . . . . 9Evoxac . . . . . . . . . . . . . . . . . . . . . . . . . 29Evzio . . . . . . . . . . . . . . . . . . . . . . . . . . . 14Exalgo . . . . . . . . . . . . . . . . . . . . . . . . . . 13Exelon . . . . . . . . . . . . . . . . . . . . . . . . . . 16Exemestane Tablet . . . . . . . . . . . . . . . . 11Exforge . . . . . . . . . . . . . . . . . . . . . . . . . 23Exforge HCT . . . . . . . . . . . . . . . . . . . . 23Exjade . . . . . . . . . . . . . . . . . . . . . . . . . . 49Extina . . . . . . . . . . . . . . . . . . . . . . . . . . 27Ezetimibe . . . . . . . . . . . . . . . . . . . . . . . 24Ezetimibe/Simvastatin . . . . . . . . . . . . . 24FFalessa . . . . . . . . . . . . . . . . . . . . . . . . . 39Fallback Solo . . . . . . . . . . . . . . . . . . . . 39Falmina . . . . . . . . . . . . . . . . . . . . . . . . . 38Famciclovir . . . . . . . . . . . . . . . . . . . . . . . 8Famvir . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Fanapt . . . . . . . . . . . . . . . . . . . . . . . . . . 18Fareston . . . . . . . . . . . . . . . . . . . . . . . . 11Farxiga . . . . . . . . . . . . . . . . . . . . . . . . . 31Farydak . . . . . . . . . . . . . . . . . . . . . . . . . 12Fayosim . . . . . . . . . . . . . . . . . . . . . . . . . 39Feiba . . . . . . . . . . . . . . . . . . . . . . . . . . . 21Felbamate Tablet . . . . . . . . . . . . . . . . . 15Felbatol . . . . . . . . . . . . . . . . . . . . . . . . . 15Feldene . . . . . . . . . . . . . . . . . . . . . . . . . 36Felodipine . . . . . . . . . . . . . . . . . . . . . . . 22Femara . . . . . . . . . . . . . . . . . . . . . . 11, 12Femcon FE . . . . . . . . . . . . . . . . . . . . . . 39Femhrt . . . . . . . . . . . . . . . . . . . . . . . . . . 40Femring . . . . . . . . . . . . . . . . . . . . . . . . . 40Femynor . . . . . . . . . . . . . . . . . . . . . . . . 38Fenofibrate 40, 48, 120,
145 mg Tablet . . . . . . . . . . . . . . . . . 24Fenofibrate 43, 50, 67, 130,
134, 150, 200 mg Capsule . . . . . . 24Fenofibrate 54, 160 mg . . . . . . . . . . . 24Fenoglide . . . . . . . . . . . . . . . . . . . . . . . 24Fentanyl Citrate Lollipop . . . . . . . . . . . 13
Fentanyl Transdermal 12 mcg/hr, 25 mcg/hr, 50 mcg/hr, 75 mcg/hr, 100 mcg/hr . . . . . . . . . . . . . . . . . . . . 13
Ferriprox . . . . . . . . . . . . . . . . . . . . . . . . 49Fetzima . . . . . . . . . . . . . . . . . . . . . . . . . 17Finacea . . . . . . . . . . . . . . . . . . . . . . . . . 26Finasteride . . . . . . . . . . . . . . . . . . . . . . 47Fioricet . . . . . . . . . . . . . . . . . . . . . . . . . 13Firazyr . . . . . . . . . . . . . . . . . . . . . . . . . . 44Flagyl . . . . . . . . . . . . . . . . . . . . . . . . . . . 10Flecainide . . . . . . . . . . . . . . . . . . . . . . . 20Flector . . . . . . . . . . . . . . . . . . . . . . . . . . 36Flexeril . . . . . . . . . . . . . . . . . . . . . . . . . . 36Flomax . . . . . . . . . . . . . . . . . . . . . . . . . . 47Flonase . . . . . . . . . . . . . . . . . . . . . . . . . 45Florinef Acetate . . . . . . . . . . . . . . . . . . 30Florone . . . . . . . . . . . . . . . . . . . . . . . . . 25Flovent Diskus . . . . . . . . . . . . . . . . . . . 45Flovent HFA . . . . . . . . . . . . . . . . . . . . . 45Floxin . . . . . . . . . . . . . . . . . . . . . . . . . 8, 29Floxin Otic . . . . . . . . . . . . . . . . . . . . . . 29Flucinonide 0 .1% Cream . . . . . . . . . . 25Fluconazole Tablet . . . . . . . . . . . . . . 9, 41Fludrocortisone Tablet . . . . . . . . . . . . . 30Flunisolide . . . . . . . . . . . . . . . . . . . . . . 45Fluocinolone Acetonide Body Oil,
Scalp Oil . . . . . . . . . . . . . . . . . . . . . . 26Fluocinolone Acetonide Cream, Oil,
Solution . . . . . . . . . . . . . . . . . . . . . . . 25Fluocinolone Acetonide Non-Oral
Solution . . . . . . . . . . . . . . . . . . . . . . . 26Fluocinolone Acetonide Ointment . . . 25Fluocinonide Cream, Gel, Ointment,
Solution, Non-Oral . . . . . . . . . . . . . . 25Fluoride Ion/Iron/Multivitamins . . . . . . 48Fluoride Ion/Iron/Vitamins A,C,
and D . . . . . . . . . . . . . . . . . . . . . . . . . 48Fluoride Ion/Multivitamins . . . . . . . . . . 48Fluoride Ion/Vitamins A,C, and D . . . . 48Fluorometholone . . . . . . . . . . . . . . . . . 43Fluoroplex . . . . . . . . . . . . . . . . . . . . . . . 28Fluorouracil 0 .5% Cream . . . . . . . . . . 28Fluorouracil 5% Cream . . . . . . . . . . . . 28Fluoxetine 10 mg, 20 mg Tablet . . . . . 18Fluoxetine Capsule . . . . . . . . . . . . . . . 18Fluoxetine Delayed-Release
Capsule . . . . . . . . . . . . . . . . . . . . . . . 18Flurandrenolide Cream, Lotion,
Ointment . . . . . . . . . . . . . . . . . . . . . . 25Flutamide Capsule . . . . . . . . . . . . . . . . 11Fluticasone . . . . . . . . . . . . . . . . . . . 25, 45
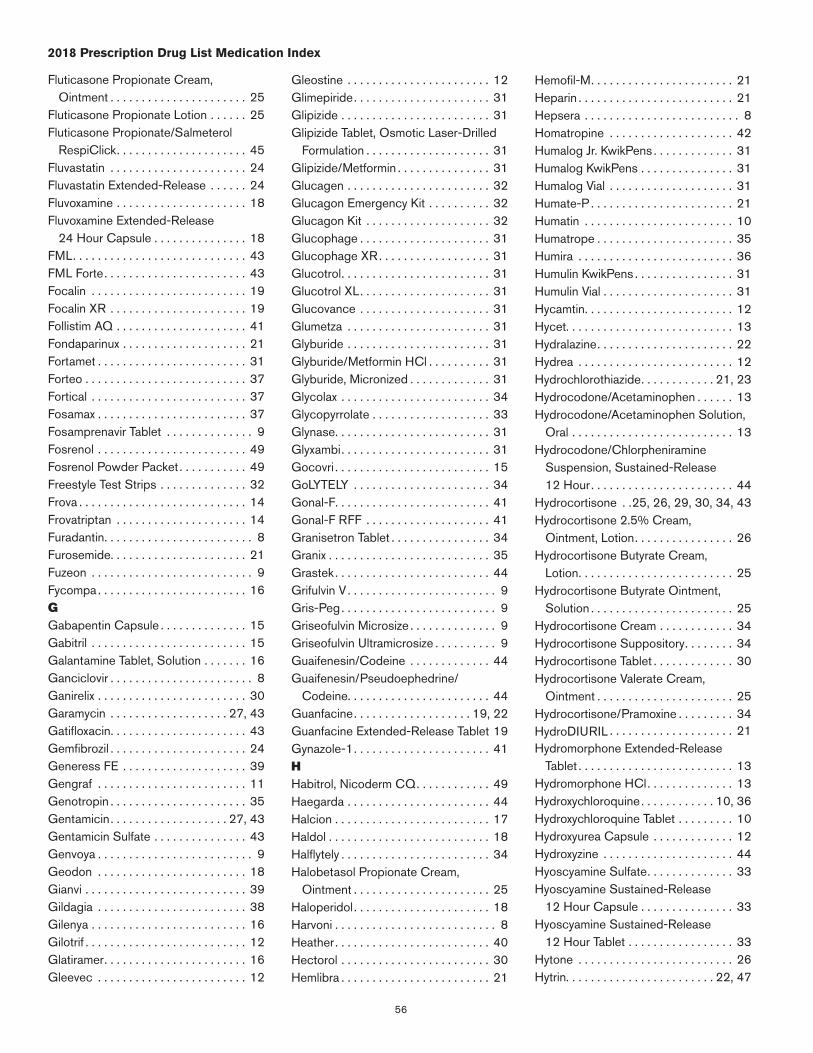
56
2018 Prescription Drug List Medication Index
Fluticasone Propionate Cream, Ointment . . . . . . . . . . . . . . . . . . . . . . 25
Fluticasone Propionate Lotion . . . . . . 25Fluticasone Propionate/Salmeterol
RespiClick . . . . . . . . . . . . . . . . . . . . . 45Fluvastatin . . . . . . . . . . . . . . . . . . . . . . 24Fluvastatin Extended-Release . . . . . . 24Fluvoxamine . . . . . . . . . . . . . . . . . . . . . 18Fluvoxamine Extended-Release
24 Hour Capsule . . . . . . . . . . . . . . . 18FML . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43FML Forte . . . . . . . . . . . . . . . . . . . . . . . 43Focalin . . . . . . . . . . . . . . . . . . . . . . . . . 19Focalin XR . . . . . . . . . . . . . . . . . . . . . . 19Follistim AQ . . . . . . . . . . . . . . . . . . . . . 41Fondaparinux . . . . . . . . . . . . . . . . . . . . 21Fortamet . . . . . . . . . . . . . . . . . . . . . . . . 31Forteo . . . . . . . . . . . . . . . . . . . . . . . . . . 37Fortical . . . . . . . . . . . . . . . . . . . . . . . . . 37Fosamax . . . . . . . . . . . . . . . . . . . . . . . . 37Fosamprenavir Tablet . . . . . . . . . . . . . . 9Fosrenol . . . . . . . . . . . . . . . . . . . . . . . . 49Fosrenol Powder Packet . . . . . . . . . . . 49Freestyle Test Strips . . . . . . . . . . . . . . 32Frova . . . . . . . . . . . . . . . . . . . . . . . . . . . 14Frovatriptan . . . . . . . . . . . . . . . . . . . . . 14Furadantin . . . . . . . . . . . . . . . . . . . . . . . . 8Furosemide . . . . . . . . . . . . . . . . . . . . . . 21Fuzeon . . . . . . . . . . . . . . . . . . . . . . . . . . 9Fycompa . . . . . . . . . . . . . . . . . . . . . . . . 16GGabapentin Capsule . . . . . . . . . . . . . . 15Gabitril . . . . . . . . . . . . . . . . . . . . . . . . . 15Galantamine Tablet, Solution . . . . . . . 16Ganciclovir . . . . . . . . . . . . . . . . . . . . . . . 8Ganirelix . . . . . . . . . . . . . . . . . . . . . . . . 30Garamycin . . . . . . . . . . . . . . . . . . . 27, 43Gatifloxacin . . . . . . . . . . . . . . . . . . . . . . 43Gemfibrozil . . . . . . . . . . . . . . . . . . . . . . 24Generess FE . . . . . . . . . . . . . . . . . . . . 39Gengraf . . . . . . . . . . . . . . . . . . . . . . . . 11Genotropin . . . . . . . . . . . . . . . . . . . . . . 35Gentamicin . . . . . . . . . . . . . . . . . . . 27, 43Gentamicin Sulfate . . . . . . . . . . . . . . . 43Genvoya . . . . . . . . . . . . . . . . . . . . . . . . . 9Geodon . . . . . . . . . . . . . . . . . . . . . . . . 18Gianvi . . . . . . . . . . . . . . . . . . . . . . . . . . 39Gildagia . . . . . . . . . . . . . . . . . . . . . . . . 38Gilenya . . . . . . . . . . . . . . . . . . . . . . . . . 16Gilotrif . . . . . . . . . . . . . . . . . . . . . . . . . . 12Glatiramer . . . . . . . . . . . . . . . . . . . . . . . 16Gleevec . . . . . . . . . . . . . . . . . . . . . . . . 12
Gleostine . . . . . . . . . . . . . . . . . . . . . . . 12Glimepiride . . . . . . . . . . . . . . . . . . . . . . 31Glipizide . . . . . . . . . . . . . . . . . . . . . . . . 31Glipizide Tablet, Osmotic Laser-Drilled
Formulation . . . . . . . . . . . . . . . . . . . . 31Glipizide/Metformin . . . . . . . . . . . . . . . 31Glucagen . . . . . . . . . . . . . . . . . . . . . . . 32Glucagon Emergency Kit . . . . . . . . . . 32Glucagon Kit . . . . . . . . . . . . . . . . . . . . 32Glucophage . . . . . . . . . . . . . . . . . . . . . 31Glucophage XR . . . . . . . . . . . . . . . . . . 31Glucotrol . . . . . . . . . . . . . . . . . . . . . . . . 31Glucotrol XL . . . . . . . . . . . . . . . . . . . . . 31Glucovance . . . . . . . . . . . . . . . . . . . . . 31Glumetza . . . . . . . . . . . . . . . . . . . . . . . 31Glyburide . . . . . . . . . . . . . . . . . . . . . . . 31Glyburide/Metformin HCl . . . . . . . . . . 31Glyburide, Micronized . . . . . . . . . . . . . 31Glycolax . . . . . . . . . . . . . . . . . . . . . . . . 34Glycopyrrolate . . . . . . . . . . . . . . . . . . . 33Glynase . . . . . . . . . . . . . . . . . . . . . . . . . 31Glyxambi . . . . . . . . . . . . . . . . . . . . . . . . 31Gocovri . . . . . . . . . . . . . . . . . . . . . . . . . 15GoLYTELY . . . . . . . . . . . . . . . . . . . . . . 34Gonal-F . . . . . . . . . . . . . . . . . . . . . . . . . 41Gonal-F RFF . . . . . . . . . . . . . . . . . . . . 41Granisetron Tablet . . . . . . . . . . . . . . . . 34Granix . . . . . . . . . . . . . . . . . . . . . . . . . . 35Grastek . . . . . . . . . . . . . . . . . . . . . . . . . 44Grifulvin V . . . . . . . . . . . . . . . . . . . . . . . . 9Gris-Peg . . . . . . . . . . . . . . . . . . . . . . . . . 9Griseofulvin Microsize . . . . . . . . . . . . . . 9Griseofulvin Ultramicrosize . . . . . . . . . . 9Guaifenesin/Codeine . . . . . . . . . . . . . 44Guaifenesin/Pseudoephedrine/
Codeine . . . . . . . . . . . . . . . . . . . . . . . 44Guanfacine . . . . . . . . . . . . . . . . . . . 19, 22Guanfacine Extended-Release Tablet 19Gynazole-1 . . . . . . . . . . . . . . . . . . . . . . 41HHabitrol, Nicoderm CQ . . . . . . . . . . . . 49Haegarda . . . . . . . . . . . . . . . . . . . . . . . 44Halcion . . . . . . . . . . . . . . . . . . . . . . . . . 17Haldol . . . . . . . . . . . . . . . . . . . . . . . . . . 18Halflytely . . . . . . . . . . . . . . . . . . . . . . . . 34Halobetasol Propionate Cream,
Ointment . . . . . . . . . . . . . . . . . . . . . . 25Haloperidol . . . . . . . . . . . . . . . . . . . . . . 18Harvoni . . . . . . . . . . . . . . . . . . . . . . . . . . 8Heather . . . . . . . . . . . . . . . . . . . . . . . . . 40Hectorol . . . . . . . . . . . . . . . . . . . . . . . . 30Hemlibra . . . . . . . . . . . . . . . . . . . . . . . . 21
Hemofil-M . . . . . . . . . . . . . . . . . . . . . . . 21Heparin . . . . . . . . . . . . . . . . . . . . . . . . . 21Hepsera . . . . . . . . . . . . . . . . . . . . . . . . . 8Homatropine . . . . . . . . . . . . . . . . . . . . 42Humalog Jr . KwikPens . . . . . . . . . . . . . 31Humalog KwikPens . . . . . . . . . . . . . . . 31Humalog Vial . . . . . . . . . . . . . . . . . . . . 31Humate-P . . . . . . . . . . . . . . . . . . . . . . . 21Humatin . . . . . . . . . . . . . . . . . . . . . . . . 10Humatrope . . . . . . . . . . . . . . . . . . . . . . 35Humira . . . . . . . . . . . . . . . . . . . . . . . . . 36Humulin KwikPens . . . . . . . . . . . . . . . . 31Humulin Vial . . . . . . . . . . . . . . . . . . . . . 31Hycamtin . . . . . . . . . . . . . . . . . . . . . . . . 12Hycet . . . . . . . . . . . . . . . . . . . . . . . . . . . 13Hydralazine . . . . . . . . . . . . . . . . . . . . . . 22Hydrea . . . . . . . . . . . . . . . . . . . . . . . . . 12Hydrochlorothiazide . . . . . . . . . . . . 21, 23Hydrocodone/Acetaminophen . . . . . . 13Hydrocodone/Acetaminophen Solution,
Oral . . . . . . . . . . . . . . . . . . . . . . . . . . 13Hydrocodone/Chlorpheniramine
Suspension, Sustained-Release 12 Hour . . . . . . . . . . . . . . . . . . . . . . . 44
Hydrocortisone . .25, 26, 29, 30, 34, 43Hydrocortisone 2 .5% Cream,
Ointment, Lotion . . . . . . . . . . . . . . . . 26Hydrocortisone Butyrate Cream,
Lotion . . . . . . . . . . . . . . . . . . . . . . . . . 25Hydrocortisone Butyrate Ointment,
Solution . . . . . . . . . . . . . . . . . . . . . . . 25Hydrocortisone Cream . . . . . . . . . . . . 34Hydrocortisone Suppository . . . . . . . . 34Hydrocortisone Tablet . . . . . . . . . . . . . 30Hydrocortisone Valerate Cream,
Ointment . . . . . . . . . . . . . . . . . . . . . . 25Hydrocortisone/Pramoxine . . . . . . . . . 34HydroDIURIL . . . . . . . . . . . . . . . . . . . . 21Hydromorphone Extended-Release
Tablet . . . . . . . . . . . . . . . . . . . . . . . . . 13Hydromorphone HCl . . . . . . . . . . . . . . 13Hydroxychloroquine . . . . . . . . . . . . 10, 36Hydroxychloroquine Tablet . . . . . . . . . 10Hydroxyurea Capsule . . . . . . . . . . . . . 12Hydroxyzine . . . . . . . . . . . . . . . . . . . . . 44Hyoscyamine Sulfate . . . . . . . . . . . . . . 33Hyoscyamine Sustained-Release
12 Hour Capsule . . . . . . . . . . . . . . . 33Hyoscyamine Sustained-Release
12 Hour Tablet . . . . . . . . . . . . . . . . . 33Hytone . . . . . . . . . . . . . . . . . . . . . . . . . 26Hytrin . . . . . . . . . . . . . . . . . . . . . . . . 22, 47
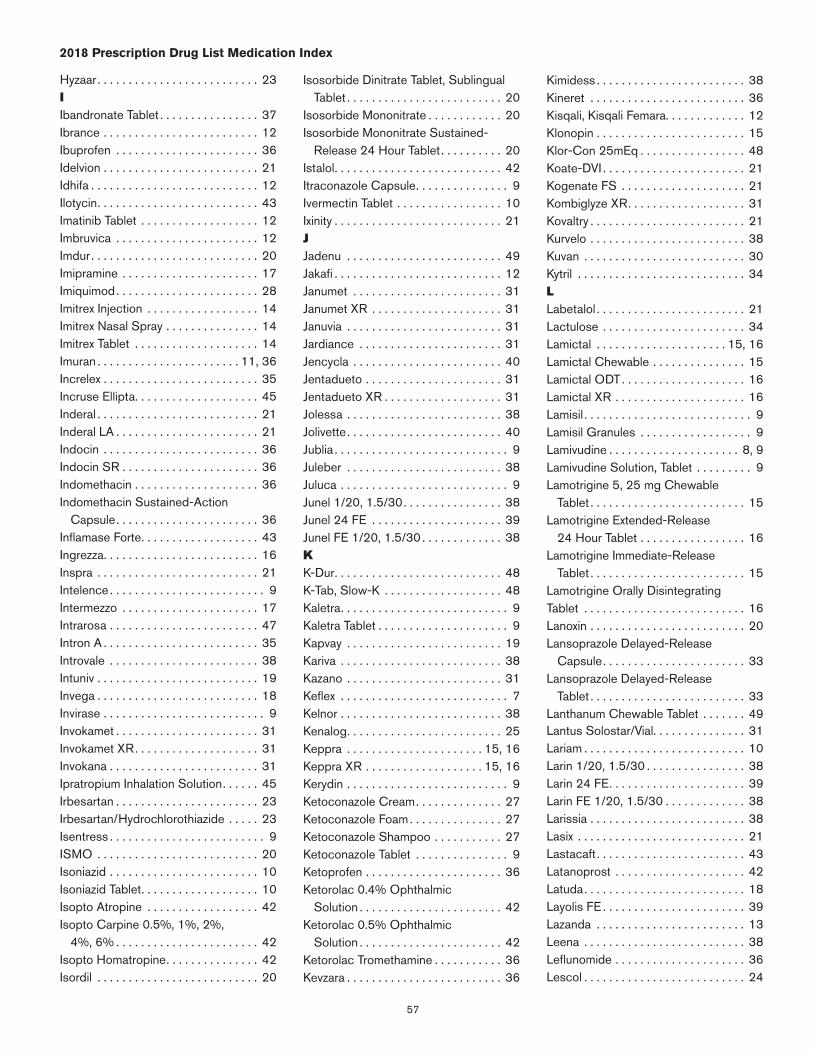
57
2018 Prescription Drug List Medication Index
Hyzaar . . . . . . . . . . . . . . . . . . . . . . . . . . 23IIbandronate Tablet . . . . . . . . . . . . . . . . 37Ibrance . . . . . . . . . . . . . . . . . . . . . . . . . 12Ibuprofen . . . . . . . . . . . . . . . . . . . . . . . 36Idelvion . . . . . . . . . . . . . . . . . . . . . . . . . 21Idhifa . . . . . . . . . . . . . . . . . . . . . . . . . . . 12Ilotycin . . . . . . . . . . . . . . . . . . . . . . . . . . 43Imatinib Tablet . . . . . . . . . . . . . . . . . . . 12Imbruvica . . . . . . . . . . . . . . . . . . . . . . . 12Imdur . . . . . . . . . . . . . . . . . . . . . . . . . . . 20Imipramine . . . . . . . . . . . . . . . . . . . . . . 17Imiquimod . . . . . . . . . . . . . . . . . . . . . . . 28Imitrex Injection . . . . . . . . . . . . . . . . . . 14Imitrex Nasal Spray . . . . . . . . . . . . . . . 14Imitrex Tablet . . . . . . . . . . . . . . . . . . . . 14Imuran . . . . . . . . . . . . . . . . . . . . . . . 11, 36Increlex . . . . . . . . . . . . . . . . . . . . . . . . . 35Incruse Ellipta . . . . . . . . . . . . . . . . . . . . 45Inderal . . . . . . . . . . . . . . . . . . . . . . . . . . 21Inderal LA . . . . . . . . . . . . . . . . . . . . . . . 21Indocin . . . . . . . . . . . . . . . . . . . . . . . . . 36Indocin SR . . . . . . . . . . . . . . . . . . . . . . 36Indomethacin . . . . . . . . . . . . . . . . . . . . 36Indomethacin Sustained-Action
Capsule . . . . . . . . . . . . . . . . . . . . . . . 36Inflamase Forte . . . . . . . . . . . . . . . . . . . 43Ingrezza . . . . . . . . . . . . . . . . . . . . . . . . . 16Inspra . . . . . . . . . . . . . . . . . . . . . . . . . . 21Intelence . . . . . . . . . . . . . . . . . . . . . . . . . 9Intermezzo . . . . . . . . . . . . . . . . . . . . . . 17Intrarosa . . . . . . . . . . . . . . . . . . . . . . . . 47Intron A . . . . . . . . . . . . . . . . . . . . . . . . . 35Introvale . . . . . . . . . . . . . . . . . . . . . . . . 38Intuniv . . . . . . . . . . . . . . . . . . . . . . . . . . 19Invega . . . . . . . . . . . . . . . . . . . . . . . . . . 18Invirase . . . . . . . . . . . . . . . . . . . . . . . . . . 9Invokamet . . . . . . . . . . . . . . . . . . . . . . . 31Invokamet XR . . . . . . . . . . . . . . . . . . . . 31Invokana . . . . . . . . . . . . . . . . . . . . . . . . 31Ipratropium Inhalation Solution . . . . . . 45Irbesartan . . . . . . . . . . . . . . . . . . . . . . . 23Irbesartan/Hydrochlorothiazide . . . . . 23Isentress . . . . . . . . . . . . . . . . . . . . . . . . . 9ISMO . . . . . . . . . . . . . . . . . . . . . . . . . . 20Isoniazid . . . . . . . . . . . . . . . . . . . . . . . . 10Isoniazid Tablet . . . . . . . . . . . . . . . . . . . 10Isopto Atropine . . . . . . . . . . . . . . . . . . 42Isopto Carpine 0 .5%, 1%, 2%,
4%, 6% . . . . . . . . . . . . . . . . . . . . . . . 42Isopto Homatropine . . . . . . . . . . . . . . . 42Isordil . . . . . . . . . . . . . . . . . . . . . . . . . . 20
Isosorbide Dinitrate Tablet, Sublingual Tablet . . . . . . . . . . . . . . . . . . . . . . . . . 20
Isosorbide Mononitrate . . . . . . . . . . . . 20Isosorbide Mononitrate Sustained-
Release 24 Hour Tablet . . . . . . . . . . 20Istalol . . . . . . . . . . . . . . . . . . . . . . . . . . . 42Itraconazole Capsule . . . . . . . . . . . . . . . 9Ivermectin Tablet . . . . . . . . . . . . . . . . . 10Ixinity . . . . . . . . . . . . . . . . . . . . . . . . . . . 21JJadenu . . . . . . . . . . . . . . . . . . . . . . . . . 49Jakafi . . . . . . . . . . . . . . . . . . . . . . . . . . . 12Janumet . . . . . . . . . . . . . . . . . . . . . . . . 31Janumet XR . . . . . . . . . . . . . . . . . . . . . 31Januvia . . . . . . . . . . . . . . . . . . . . . . . . . 31Jardiance . . . . . . . . . . . . . . . . . . . . . . . 31Jencycla . . . . . . . . . . . . . . . . . . . . . . . . 40Jentadueto . . . . . . . . . . . . . . . . . . . . . . 31Jentadueto XR . . . . . . . . . . . . . . . . . . . 31Jolessa . . . . . . . . . . . . . . . . . . . . . . . . . 38Jolivette . . . . . . . . . . . . . . . . . . . . . . . . . 40Jublia . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9Juleber . . . . . . . . . . . . . . . . . . . . . . . . . 38Juluca . . . . . . . . . . . . . . . . . . . . . . . . . . . 9Junel 1/20, 1 .5/30 . . . . . . . . . . . . . . . . 38Junel 24 FE . . . . . . . . . . . . . . . . . . . . . 39Junel FE 1/20, 1 .5/30 . . . . . . . . . . . . . 38KK-Dur . . . . . . . . . . . . . . . . . . . . . . . . . . . 48K-Tab, Slow-K . . . . . . . . . . . . . . . . . . . 48Kaletra . . . . . . . . . . . . . . . . . . . . . . . . . . . 9Kaletra Tablet . . . . . . . . . . . . . . . . . . . . . 9Kapvay . . . . . . . . . . . . . . . . . . . . . . . . . 19Kariva . . . . . . . . . . . . . . . . . . . . . . . . . . 38Kazano . . . . . . . . . . . . . . . . . . . . . . . . . 31Keflex . . . . . . . . . . . . . . . . . . . . . . . . . . . 7Kelnor . . . . . . . . . . . . . . . . . . . . . . . . . . 38Kenalog . . . . . . . . . . . . . . . . . . . . . . . . . 25Keppra . . . . . . . . . . . . . . . . . . . . . . 15, 16Keppra XR . . . . . . . . . . . . . . . . . . . 15, 16Kerydin . . . . . . . . . . . . . . . . . . . . . . . . . . 9Ketoconazole Cream . . . . . . . . . . . . . . 27Ketoconazole Foam . . . . . . . . . . . . . . . 27Ketoconazole Shampoo . . . . . . . . . . . 27Ketoconazole Tablet . . . . . . . . . . . . . . . 9Ketoprofen . . . . . . . . . . . . . . . . . . . . . . 36Ketorolac 0 .4% Ophthalmic
Solution . . . . . . . . . . . . . . . . . . . . . . . 42Ketorolac 0 .5% Ophthalmic
Solution . . . . . . . . . . . . . . . . . . . . . . . 42Ketorolac Tromethamine . . . . . . . . . . . 36Kevzara . . . . . . . . . . . . . . . . . . . . . . . . . 36
Kimidess . . . . . . . . . . . . . . . . . . . . . . . . 38Kineret . . . . . . . . . . . . . . . . . . . . . . . . . 36Kisqali, Kisqali Femara . . . . . . . . . . . . . 12Klonopin . . . . . . . . . . . . . . . . . . . . . . . . 15Klor-Con 25mEq . . . . . . . . . . . . . . . . . 48Koate-DVI . . . . . . . . . . . . . . . . . . . . . . . 21Kogenate FS . . . . . . . . . . . . . . . . . . . . 21Kombiglyze XR . . . . . . . . . . . . . . . . . . . 31Kovaltry . . . . . . . . . . . . . . . . . . . . . . . . . 21Kurvelo . . . . . . . . . . . . . . . . . . . . . . . . . 38Kuvan . . . . . . . . . . . . . . . . . . . . . . . . . . 30Kytril . . . . . . . . . . . . . . . . . . . . . . . . . . . 34LLabetalol . . . . . . . . . . . . . . . . . . . . . . . . 21Lactulose . . . . . . . . . . . . . . . . . . . . . . . 34Lamictal . . . . . . . . . . . . . . . . . . . . . 15, 16Lamictal Chewable . . . . . . . . . . . . . . . 15Lamictal ODT . . . . . . . . . . . . . . . . . . . . 16Lamictal XR . . . . . . . . . . . . . . . . . . . . . 16Lamisil . . . . . . . . . . . . . . . . . . . . . . . . . . . 9Lamisil Granules . . . . . . . . . . . . . . . . . . 9Lamivudine . . . . . . . . . . . . . . . . . . . . . 8, 9Lamivudine Solution, Tablet . . . . . . . . . 9Lamotrigine 5, 25 mg Chewable
Tablet . . . . . . . . . . . . . . . . . . . . . . . . . 15Lamotrigine Extended-Release
24 Hour Tablet . . . . . . . . . . . . . . . . . 16Lamotrigine Immediate-Release
Tablet . . . . . . . . . . . . . . . . . . . . . . . . . 15Lamotrigine Orally Disintegrating Tablet . . . . . . . . . . . . . . . . . . . . . . . . . . 16Lanoxin . . . . . . . . . . . . . . . . . . . . . . . . . 20Lansoprazole Delayed-Release
Capsule . . . . . . . . . . . . . . . . . . . . . . . 33Lansoprazole Delayed-Release
Tablet . . . . . . . . . . . . . . . . . . . . . . . . . 33Lanthanum Chewable Tablet . . . . . . . 49Lantus Solostar/Vial . . . . . . . . . . . . . . . 31Lariam . . . . . . . . . . . . . . . . . . . . . . . . . . 10Larin 1/20, 1 .5/30 . . . . . . . . . . . . . . . . 38Larin 24 FE . . . . . . . . . . . . . . . . . . . . . . 39Larin FE 1/20, 1 .5/30 . . . . . . . . . . . . . 38Larissia . . . . . . . . . . . . . . . . . . . . . . . . . 38Lasix . . . . . . . . . . . . . . . . . . . . . . . . . . . 21Lastacaft . . . . . . . . . . . . . . . . . . . . . . . . 43Latanoprost . . . . . . . . . . . . . . . . . . . . . 42Latuda . . . . . . . . . . . . . . . . . . . . . . . . . . 18Layolis FE . . . . . . . . . . . . . . . . . . . . . . . 39Lazanda . . . . . . . . . . . . . . . . . . . . . . . . 13Leena . . . . . . . . . . . . . . . . . . . . . . . . . . 38Leflunomide . . . . . . . . . . . . . . . . . . . . . 36Lescol . . . . . . . . . . . . . . . . . . . . . . . . . . 24
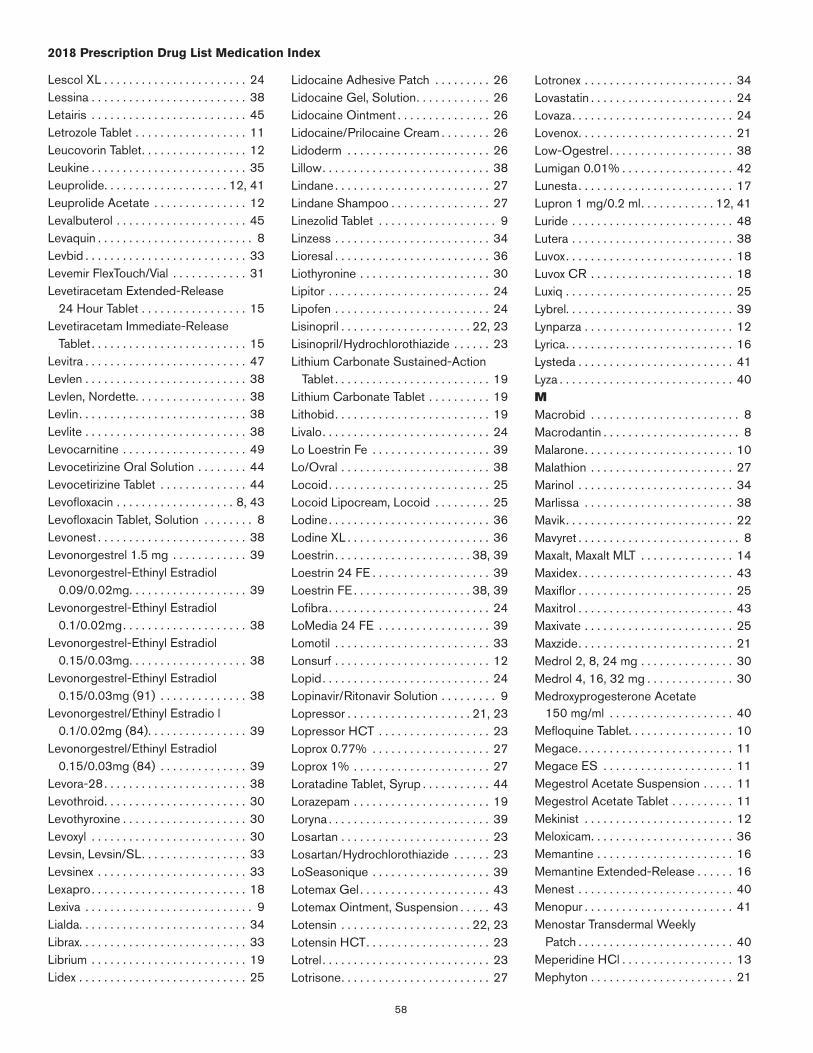
58
2018 Prescription Drug List Medication Index
Lescol XL . . . . . . . . . . . . . . . . . . . . . . . 24Lessina . . . . . . . . . . . . . . . . . . . . . . . . . 38Letairis . . . . . . . . . . . . . . . . . . . . . . . . . 45Letrozole Tablet . . . . . . . . . . . . . . . . . . 11Leucovorin Tablet . . . . . . . . . . . . . . . . . 12Leukine . . . . . . . . . . . . . . . . . . . . . . . . . 35Leuprolide . . . . . . . . . . . . . . . . . . . . 12, 41Leuprolide Acetate . . . . . . . . . . . . . . . 12Levalbuterol . . . . . . . . . . . . . . . . . . . . . 45Levaquin . . . . . . . . . . . . . . . . . . . . . . . . . 8Levbid . . . . . . . . . . . . . . . . . . . . . . . . . . 33Levemir FlexTouch/Vial . . . . . . . . . . . . 31Levetiracetam Extended-Release
24 Hour Tablet . . . . . . . . . . . . . . . . . 15Levetiracetam Immediate-Release
Tablet . . . . . . . . . . . . . . . . . . . . . . . . . 15Levitra . . . . . . . . . . . . . . . . . . . . . . . . . . 47Levlen . . . . . . . . . . . . . . . . . . . . . . . . . . 38Levlen, Nordette . . . . . . . . . . . . . . . . . . 38Levlin . . . . . . . . . . . . . . . . . . . . . . . . . . . 38Levlite . . . . . . . . . . . . . . . . . . . . . . . . . . 38Levocarnitine . . . . . . . . . . . . . . . . . . . . 49Levocetirizine Oral Solution . . . . . . . . 44Levocetirizine Tablet . . . . . . . . . . . . . . 44Levofloxacin . . . . . . . . . . . . . . . . . . . 8, 43Levofloxacin Tablet, Solution . . . . . . . . 8Levonest . . . . . . . . . . . . . . . . . . . . . . . . 38Levonorgestrel 1 .5 mg . . . . . . . . . . . . 39Levonorgestrel-Ethinyl Estradiol
0 .09/0 .02mg . . . . . . . . . . . . . . . . . . . 39Levonorgestrel-Ethinyl Estradiol
0 .1/0 .02mg . . . . . . . . . . . . . . . . . . . . 38Levonorgestrel-Ethinyl Estradiol
0 .15/0 .03mg . . . . . . . . . . . . . . . . . . . 38Levonorgestrel-Ethinyl Estradiol
0 .15/0 .03mg (91) . . . . . . . . . . . . . . 38Levonorgestrel/Ethinyl Estradio l
0 .1/0 .02mg (84) . . . . . . . . . . . . . . . . 39Levonorgestrel/Ethinyl Estradiol
0 .15/0 .03mg (84) . . . . . . . . . . . . . . 39Levora-28 . . . . . . . . . . . . . . . . . . . . . . . 38Levothroid . . . . . . . . . . . . . . . . . . . . . . . 30Levothyroxine . . . . . . . . . . . . . . . . . . . . 30Levoxyl . . . . . . . . . . . . . . . . . . . . . . . . . 30Levsin, Levsin/SL . . . . . . . . . . . . . . . . . 33Levsinex . . . . . . . . . . . . . . . . . . . . . . . . 33Lexapro . . . . . . . . . . . . . . . . . . . . . . . . . 18Lexiva . . . . . . . . . . . . . . . . . . . . . . . . . . . 9Lialda . . . . . . . . . . . . . . . . . . . . . . . . . . . 34Librax . . . . . . . . . . . . . . . . . . . . . . . . . . . 33Librium . . . . . . . . . . . . . . . . . . . . . . . . . 19Lidex . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
Lidocaine Adhesive Patch . . . . . . . . . 26Lidocaine Gel, Solution . . . . . . . . . . . . 26Lidocaine Ointment . . . . . . . . . . . . . . . 26Lidocaine/Prilocaine Cream . . . . . . . . 26Lidoderm . . . . . . . . . . . . . . . . . . . . . . . 26Lillow . . . . . . . . . . . . . . . . . . . . . . . . . . . 38Lindane . . . . . . . . . . . . . . . . . . . . . . . . . 27Lindane Shampoo . . . . . . . . . . . . . . . . 27Linezolid Tablet . . . . . . . . . . . . . . . . . . . 9Linzess . . . . . . . . . . . . . . . . . . . . . . . . . 34Lioresal . . . . . . . . . . . . . . . . . . . . . . . . . 36Liothyronine . . . . . . . . . . . . . . . . . . . . . 30Lipitor . . . . . . . . . . . . . . . . . . . . . . . . . . 24Lipofen . . . . . . . . . . . . . . . . . . . . . . . . . 24Lisinopril . . . . . . . . . . . . . . . . . . . . . 22, 23Lisinopril/Hydrochlorothiazide . . . . . . 23Lithium Carbonate Sustained-Action
Tablet . . . . . . . . . . . . . . . . . . . . . . . . . 19Lithium Carbonate Tablet . . . . . . . . . . 19Lithobid . . . . . . . . . . . . . . . . . . . . . . . . . 19Livalo . . . . . . . . . . . . . . . . . . . . . . . . . . . 24Lo Loestrin Fe . . . . . . . . . . . . . . . . . . . 39Lo/Ovral . . . . . . . . . . . . . . . . . . . . . . . . 38Locoid . . . . . . . . . . . . . . . . . . . . . . . . . . 25Locoid Lipocream, Locoid . . . . . . . . . 25Lodine . . . . . . . . . . . . . . . . . . . . . . . . . . 36Lodine XL . . . . . . . . . . . . . . . . . . . . . . . 36Loestrin . . . . . . . . . . . . . . . . . . . . . . 38, 39Loestrin 24 FE . . . . . . . . . . . . . . . . . . . 39Loestrin FE . . . . . . . . . . . . . . . . . . . 38, 39Lofibra . . . . . . . . . . . . . . . . . . . . . . . . . . 24LoMedia 24 FE . . . . . . . . . . . . . . . . . . 39Lomotil . . . . . . . . . . . . . . . . . . . . . . . . . 33Lonsurf . . . . . . . . . . . . . . . . . . . . . . . . . 12Lopid . . . . . . . . . . . . . . . . . . . . . . . . . . . 24Lopinavir/Ritonavir Solution . . . . . . . . . 9Lopressor . . . . . . . . . . . . . . . . . . . . 21, 23Lopressor HCT . . . . . . . . . . . . . . . . . . 23Loprox 0 .77% . . . . . . . . . . . . . . . . . . . 27Loprox 1% . . . . . . . . . . . . . . . . . . . . . . 27Loratadine Tablet, Syrup . . . . . . . . . . . 44Lorazepam . . . . . . . . . . . . . . . . . . . . . . 19Loryna . . . . . . . . . . . . . . . . . . . . . . . . . . 39Losartan . . . . . . . . . . . . . . . . . . . . . . . . 23Losartan/Hydrochlorothiazide . . . . . . 23LoSeasonique . . . . . . . . . . . . . . . . . . . 39Lotemax Gel . . . . . . . . . . . . . . . . . . . . . 43Lotemax Ointment, Suspension . . . . . 43Lotensin . . . . . . . . . . . . . . . . . . . . . 22, 23Lotensin HCT . . . . . . . . . . . . . . . . . . . . 23Lotrel . . . . . . . . . . . . . . . . . . . . . . . . . . . 23Lotrisone . . . . . . . . . . . . . . . . . . . . . . . . 27
Lotronex . . . . . . . . . . . . . . . . . . . . . . . . 34Lovastatin . . . . . . . . . . . . . . . . . . . . . . . 24Lovaza . . . . . . . . . . . . . . . . . . . . . . . . . . 24Lovenox . . . . . . . . . . . . . . . . . . . . . . . . . 21Low-Ogestrel . . . . . . . . . . . . . . . . . . . . 38Lumigan 0 .01% . . . . . . . . . . . . . . . . . . 42Lunesta . . . . . . . . . . . . . . . . . . . . . . . . . 17Lupron 1 mg/0 .2 ml . . . . . . . . . . . . 12, 41Luride . . . . . . . . . . . . . . . . . . . . . . . . . . 48Lutera . . . . . . . . . . . . . . . . . . . . . . . . . . 38Luvox . . . . . . . . . . . . . . . . . . . . . . . . . . . 18Luvox CR . . . . . . . . . . . . . . . . . . . . . . . 18Luxiq . . . . . . . . . . . . . . . . . . . . . . . . . . . 25Lybrel . . . . . . . . . . . . . . . . . . . . . . . . . . . 39Lynparza . . . . . . . . . . . . . . . . . . . . . . . . 12Lyrica . . . . . . . . . . . . . . . . . . . . . . . . . . . 16Lysteda . . . . . . . . . . . . . . . . . . . . . . . . . 41Lyza . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40MMacrobid . . . . . . . . . . . . . . . . . . . . . . . . 8Macrodantin . . . . . . . . . . . . . . . . . . . . . . 8Malarone . . . . . . . . . . . . . . . . . . . . . . . . 10Malathion . . . . . . . . . . . . . . . . . . . . . . . 27Marinol . . . . . . . . . . . . . . . . . . . . . . . . . 34Marlissa . . . . . . . . . . . . . . . . . . . . . . . . 38Mavik . . . . . . . . . . . . . . . . . . . . . . . . . . . 22Mavyret . . . . . . . . . . . . . . . . . . . . . . . . . . 8Maxalt, Maxalt MLT . . . . . . . . . . . . . . . 14Maxidex . . . . . . . . . . . . . . . . . . . . . . . . . 43Maxiflor . . . . . . . . . . . . . . . . . . . . . . . . . 25Maxitrol . . . . . . . . . . . . . . . . . . . . . . . . . 43Maxivate . . . . . . . . . . . . . . . . . . . . . . . . 25Maxzide . . . . . . . . . . . . . . . . . . . . . . . . . 21Medrol 2, 8, 24 mg . . . . . . . . . . . . . . . 30Medrol 4, 16, 32 mg . . . . . . . . . . . . . . 30Medroxyprogesterone Acetate
150 mg/ml . . . . . . . . . . . . . . . . . . . . 40Mefloquine Tablet . . . . . . . . . . . . . . . . . 10Megace . . . . . . . . . . . . . . . . . . . . . . . . . 11Megace ES . . . . . . . . . . . . . . . . . . . . . 11Megestrol Acetate Suspension . . . . . 11Megestrol Acetate Tablet . . . . . . . . . . 11Mekinist . . . . . . . . . . . . . . . . . . . . . . . . 12Meloxicam . . . . . . . . . . . . . . . . . . . . . . . 36Memantine . . . . . . . . . . . . . . . . . . . . . . 16Memantine Extended-Release . . . . . . 16Menest . . . . . . . . . . . . . . . . . . . . . . . . . 40Menopur . . . . . . . . . . . . . . . . . . . . . . . . 41Menostar Transdermal Weekly
Patch . . . . . . . . . . . . . . . . . . . . . . . . . 40Meperidine HCl . . . . . . . . . . . . . . . . . . 13Mephyton . . . . . . . . . . . . . . . . . . . . . . . 21
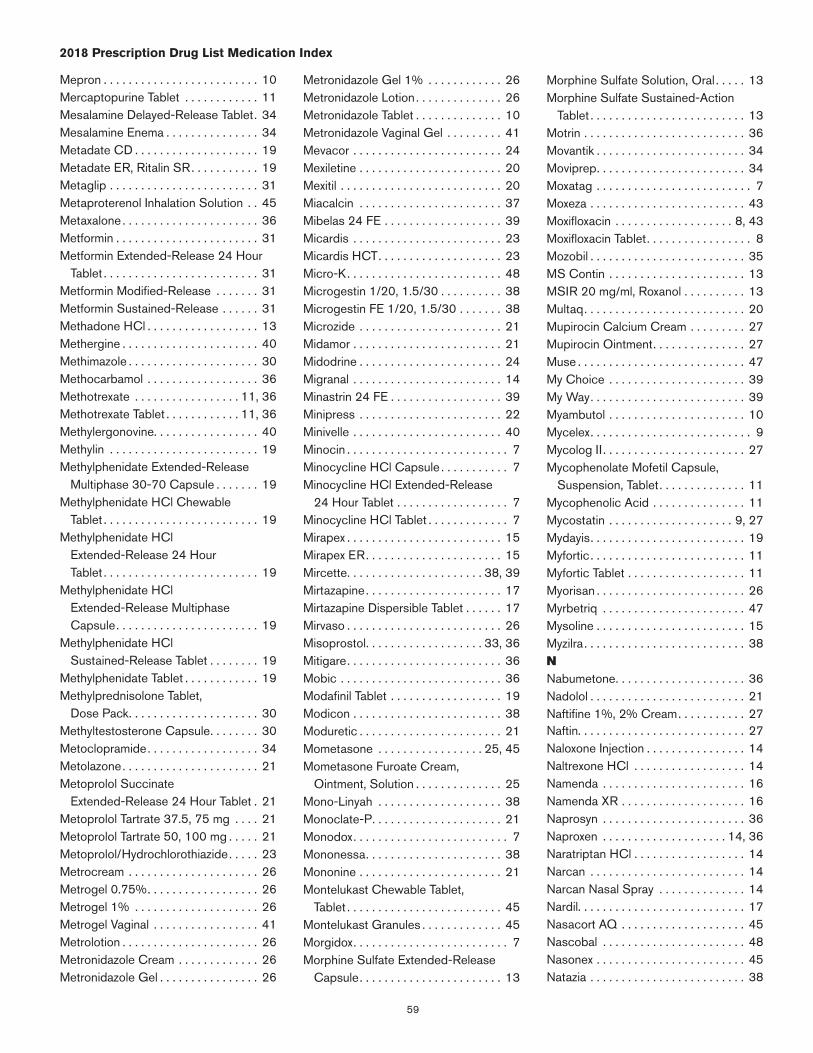
59
2018 Prescription Drug List Medication Index
Mepron . . . . . . . . . . . . . . . . . . . . . . . . . 10Mercaptopurine Tablet . . . . . . . . . . . . 11Mesalamine Delayed-Release Tablet . 34Mesalamine Enema . . . . . . . . . . . . . . . 34Metadate CD . . . . . . . . . . . . . . . . . . . . 19Metadate ER, Ritalin SR . . . . . . . . . . . 19Metaglip . . . . . . . . . . . . . . . . . . . . . . . . 31Metaproterenol Inhalation Solution . . 45Metaxalone . . . . . . . . . . . . . . . . . . . . . . 36Metformin . . . . . . . . . . . . . . . . . . . . . . . 31Metformin Extended-Release 24 Hour
Tablet . . . . . . . . . . . . . . . . . . . . . . . . . 31Metformin Modified-Release . . . . . . . 31Metformin Sustained-Release . . . . . . 31Methadone HCl . . . . . . . . . . . . . . . . . . 13Methergine . . . . . . . . . . . . . . . . . . . . . . 40Methimazole . . . . . . . . . . . . . . . . . . . . . 30Methocarbamol . . . . . . . . . . . . . . . . . . 36Methotrexate . . . . . . . . . . . . . . . . . 11, 36Methotrexate Tablet . . . . . . . . . . . . 11, 36Methylergonovine . . . . . . . . . . . . . . . . . 40Methylin . . . . . . . . . . . . . . . . . . . . . . . . 19Methylphenidate Extended-Release
Multiphase 30-70 Capsule . . . . . . . 19Methylphenidate HCl Chewable
Tablet . . . . . . . . . . . . . . . . . . . . . . . . . 19Methylphenidate HCl
Extended-Release 24 Hour Tablet . . . . . . . . . . . . . . . . . . . . . . . . . 19
Methylphenidate HCl Extended-Release Multiphase Capsule . . . . . . . . . . . . . . . . . . . . . . . 19
Methylphenidate HCl Sustained-Release Tablet . . . . . . . . 19
Methylphenidate Tablet . . . . . . . . . . . . 19Methylprednisolone Tablet,
Dose Pack . . . . . . . . . . . . . . . . . . . . . 30Methyltestosterone Capsule . . . . . . . . 30Metoclopramide . . . . . . . . . . . . . . . . . . 34Metolazone . . . . . . . . . . . . . . . . . . . . . . 21Metoprolol Succinate
Extended-Release 24 Hour Tablet . 21Metoprolol Tartrate 37 .5, 75 mg . . . . 21Metoprolol Tartrate 50, 100 mg . . . . . 21Metoprolol/Hydrochlorothiazide . . . . . 23Metrocream . . . . . . . . . . . . . . . . . . . . . 26Metrogel 0 .75% . . . . . . . . . . . . . . . . . . 26Metrogel 1% . . . . . . . . . . . . . . . . . . . . 26Metrogel Vaginal . . . . . . . . . . . . . . . . . 41Metrolotion . . . . . . . . . . . . . . . . . . . . . . 26Metronidazole Cream . . . . . . . . . . . . . 26Metronidazole Gel . . . . . . . . . . . . . . . . 26
Metronidazole Gel 1% . . . . . . . . . . . . 26Metronidazole Lotion . . . . . . . . . . . . . . 26Metronidazole Tablet . . . . . . . . . . . . . . 10Metronidazole Vaginal Gel . . . . . . . . . 41Mevacor . . . . . . . . . . . . . . . . . . . . . . . . 24Mexiletine . . . . . . . . . . . . . . . . . . . . . . . 20Mexitil . . . . . . . . . . . . . . . . . . . . . . . . . . 20Miacalcin . . . . . . . . . . . . . . . . . . . . . . . 37Mibelas 24 FE . . . . . . . . . . . . . . . . . . . 39Micardis . . . . . . . . . . . . . . . . . . . . . . . . 23Micardis HCT . . . . . . . . . . . . . . . . . . . . 23Micro-K . . . . . . . . . . . . . . . . . . . . . . . . . 48Microgestin 1/20, 1 .5/30 . . . . . . . . . . 38Microgestin FE 1/20, 1 .5/30 . . . . . . . 38Microzide . . . . . . . . . . . . . . . . . . . . . . . 21Midamor . . . . . . . . . . . . . . . . . . . . . . . . 21Midodrine . . . . . . . . . . . . . . . . . . . . . . . 24Migranal . . . . . . . . . . . . . . . . . . . . . . . . 14Minastrin 24 FE . . . . . . . . . . . . . . . . . . 39Minipress . . . . . . . . . . . . . . . . . . . . . . . 22Minivelle . . . . . . . . . . . . . . . . . . . . . . . . 40Minocin . . . . . . . . . . . . . . . . . . . . . . . . . . 7Minocycline HCl Capsule . . . . . . . . . . . 7Minocycline HCl Extended-Release
24 Hour Tablet . . . . . . . . . . . . . . . . . . 7Minocycline HCl Tablet . . . . . . . . . . . . . 7Mirapex . . . . . . . . . . . . . . . . . . . . . . . . . 15Mirapex ER . . . . . . . . . . . . . . . . . . . . . . 15Mircette . . . . . . . . . . . . . . . . . . . . . . 38, 39Mirtazapine . . . . . . . . . . . . . . . . . . . . . . 17Mirtazapine Dispersible Tablet . . . . . . 17Mirvaso . . . . . . . . . . . . . . . . . . . . . . . . . 26Misoprostol . . . . . . . . . . . . . . . . . . . 33, 36Mitigare . . . . . . . . . . . . . . . . . . . . . . . . . 36Mobic . . . . . . . . . . . . . . . . . . . . . . . . . . 36Modafinil Tablet . . . . . . . . . . . . . . . . . . 19Modicon . . . . . . . . . . . . . . . . . . . . . . . . 38Moduretic . . . . . . . . . . . . . . . . . . . . . . . 21Mometasone . . . . . . . . . . . . . . . . . 25, 45Mometasone Furoate Cream,
Ointment, Solution . . . . . . . . . . . . . . 25Mono-Linyah . . . . . . . . . . . . . . . . . . . . 38Monoclate-P . . . . . . . . . . . . . . . . . . . . . 21Monodox . . . . . . . . . . . . . . . . . . . . . . . . . 7Mononessa . . . . . . . . . . . . . . . . . . . . . . 38Mononine . . . . . . . . . . . . . . . . . . . . . . . 21Montelukast Chewable Tablet,
Tablet . . . . . . . . . . . . . . . . . . . . . . . . . 45Montelukast Granules . . . . . . . . . . . . . 45Morgidox . . . . . . . . . . . . . . . . . . . . . . . . . 7Morphine Sulfate Extended-Release
Capsule . . . . . . . . . . . . . . . . . . . . . . . 13
Morphine Sulfate Solution, Oral . . . . . 13Morphine Sulfate Sustained-Action
Tablet . . . . . . . . . . . . . . . . . . . . . . . . . 13Motrin . . . . . . . . . . . . . . . . . . . . . . . . . . 36Movantik . . . . . . . . . . . . . . . . . . . . . . . . 34Moviprep . . . . . . . . . . . . . . . . . . . . . . . . 34Moxatag . . . . . . . . . . . . . . . . . . . . . . . . . 7Moxeza . . . . . . . . . . . . . . . . . . . . . . . . . 43Moxifloxacin . . . . . . . . . . . . . . . . . . . 8, 43Moxifloxacin Tablet . . . . . . . . . . . . . . . . . 8Mozobil . . . . . . . . . . . . . . . . . . . . . . . . . 35MS Contin . . . . . . . . . . . . . . . . . . . . . . 13MSIR 20 mg/ml, Roxanol . . . . . . . . . . 13Multaq . . . . . . . . . . . . . . . . . . . . . . . . . . 20Mupirocin Calcium Cream . . . . . . . . . 27Mupirocin Ointment . . . . . . . . . . . . . . . 27Muse . . . . . . . . . . . . . . . . . . . . . . . . . . . 47My Choice . . . . . . . . . . . . . . . . . . . . . . 39My Way . . . . . . . . . . . . . . . . . . . . . . . . . 39Myambutol . . . . . . . . . . . . . . . . . . . . . . 10Mycelex . . . . . . . . . . . . . . . . . . . . . . . . . . 9Mycolog II . . . . . . . . . . . . . . . . . . . . . . . 27Mycophenolate Mofetil Capsule,
Suspension, Tablet . . . . . . . . . . . . . . 11Mycophenolic Acid . . . . . . . . . . . . . . . 11Mycostatin . . . . . . . . . . . . . . . . . . . . 9, 27Mydayis . . . . . . . . . . . . . . . . . . . . . . . . . 19Myfortic . . . . . . . . . . . . . . . . . . . . . . . . . 11Myfortic Tablet . . . . . . . . . . . . . . . . . . . 11Myorisan . . . . . . . . . . . . . . . . . . . . . . . . 26Myrbetriq . . . . . . . . . . . . . . . . . . . . . . . 47Mysoline . . . . . . . . . . . . . . . . . . . . . . . . 15Myzilra . . . . . . . . . . . . . . . . . . . . . . . . . . 38NNabumetone . . . . . . . . . . . . . . . . . . . . . 36Nadolol . . . . . . . . . . . . . . . . . . . . . . . . . 21Naftifine 1%, 2% Cream . . . . . . . . . . . 27Naftin . . . . . . . . . . . . . . . . . . . . . . . . . . . 27Naloxone Injection . . . . . . . . . . . . . . . . 14Naltrexone HCl . . . . . . . . . . . . . . . . . . 14Namenda . . . . . . . . . . . . . . . . . . . . . . . 16Namenda XR . . . . . . . . . . . . . . . . . . . . 16Naprosyn . . . . . . . . . . . . . . . . . . . . . . . 36Naproxen . . . . . . . . . . . . . . . . . . . . 14, 36Naratriptan HCl . . . . . . . . . . . . . . . . . . 14Narcan . . . . . . . . . . . . . . . . . . . . . . . . . 14Narcan Nasal Spray . . . . . . . . . . . . . . 14Nardil . . . . . . . . . . . . . . . . . . . . . . . . . . . 17Nasacort AQ . . . . . . . . . . . . . . . . . . . . 45Nascobal . . . . . . . . . . . . . . . . . . . . . . . 48Nasonex . . . . . . . . . . . . . . . . . . . . . . . . 45Natazia . . . . . . . . . . . . . . . . . . . . . . . . . 38
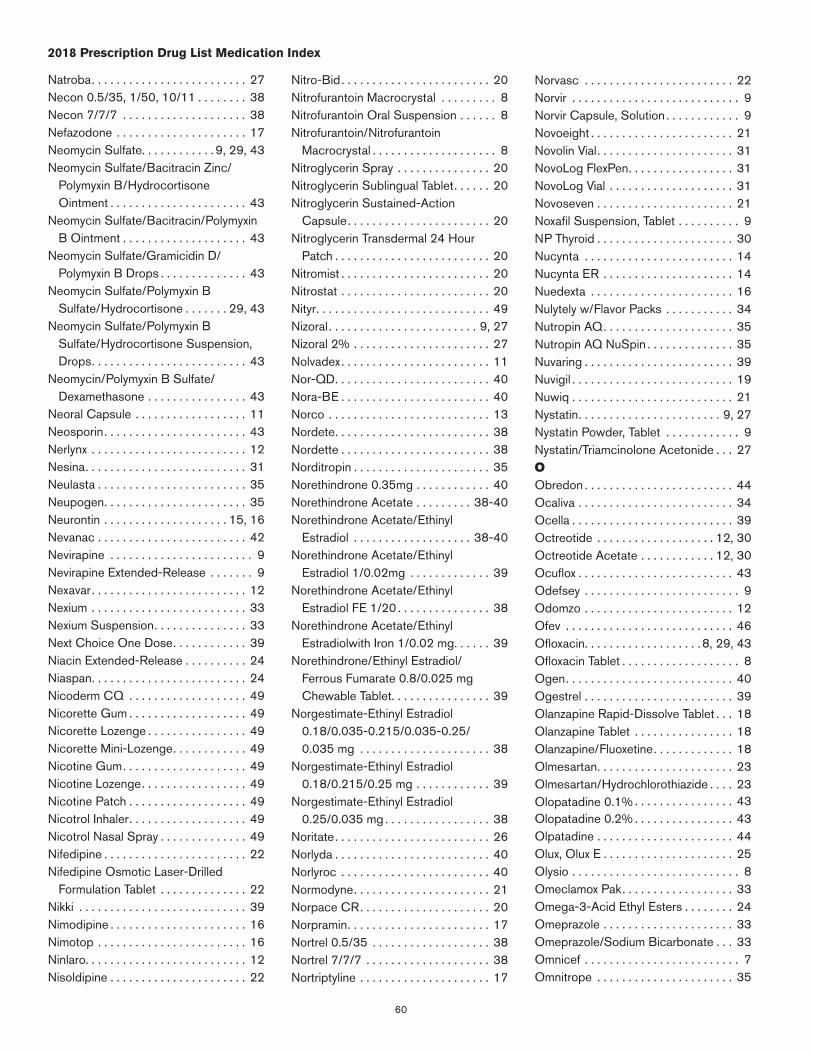
60
2018 Prescription Drug List Medication Index
Natroba . . . . . . . . . . . . . . . . . . . . . . . . . 27Necon 0 .5/35, 1/50, 10/11 . . . . . . . . 38Necon 7/7/7 . . . . . . . . . . . . . . . . . . . . 38Nefazodone . . . . . . . . . . . . . . . . . . . . . 17Neomycin Sulfate . . . . . . . . . . . . 9, 29, 43Neomycin Sulfate/Bacitracin Zinc/
Polymyxin B/Hydrocortisone Ointment . . . . . . . . . . . . . . . . . . . . . . 43
Neomycin Sulfate/Bacitracin/Polymyxin B Ointment . . . . . . . . . . . . . . . . . . . . 43
Neomycin Sulfate/Gramicidin D/Polymyxin B Drops . . . . . . . . . . . . . . 43
Neomycin Sulfate/Polymyxin B Sulfate/Hydrocortisone . . . . . . . 29, 43
Neomycin Sulfate/Polymyxin B Sulfate/Hydrocortisone Suspension, Drops . . . . . . . . . . . . . . . . . . . . . . . . . 43
Neomycin/Polymyxin B Sulfate/Dexamethasone . . . . . . . . . . . . . . . . 43
Neoral Capsule . . . . . . . . . . . . . . . . . . 11Neosporin . . . . . . . . . . . . . . . . . . . . . . . 43Nerlynx . . . . . . . . . . . . . . . . . . . . . . . . . 12Nesina . . . . . . . . . . . . . . . . . . . . . . . . . . 31Neulasta . . . . . . . . . . . . . . . . . . . . . . . . 35Neupogen . . . . . . . . . . . . . . . . . . . . . . . 35Neurontin . . . . . . . . . . . . . . . . . . . . 15, 16Nevanac . . . . . . . . . . . . . . . . . . . . . . . . 42Nevirapine . . . . . . . . . . . . . . . . . . . . . . . 9Nevirapine Extended-Release . . . . . . . 9Nexavar . . . . . . . . . . . . . . . . . . . . . . . . . 12Nexium . . . . . . . . . . . . . . . . . . . . . . . . . 33Nexium Suspension . . . . . . . . . . . . . . . 33Next Choice One Dose . . . . . . . . . . . . 39Niacin Extended-Release . . . . . . . . . . 24Niaspan . . . . . . . . . . . . . . . . . . . . . . . . . 24Nicoderm CQ . . . . . . . . . . . . . . . . . . . 49Nicorette Gum . . . . . . . . . . . . . . . . . . . 49Nicorette Lozenge . . . . . . . . . . . . . . . . 49Nicorette Mini-Lozenge . . . . . . . . . . . . 49Nicotine Gum . . . . . . . . . . . . . . . . . . . . 49Nicotine Lozenge . . . . . . . . . . . . . . . . . 49Nicotine Patch . . . . . . . . . . . . . . . . . . . 49Nicotrol Inhaler . . . . . . . . . . . . . . . . . . . 49Nicotrol Nasal Spray . . . . . . . . . . . . . . 49Nifedipine . . . . . . . . . . . . . . . . . . . . . . . 22Nifedipine Osmotic Laser-Drilled
Formulation Tablet . . . . . . . . . . . . . . 22Nikki . . . . . . . . . . . . . . . . . . . . . . . . . . . 39Nimodipine . . . . . . . . . . . . . . . . . . . . . . 16Nimotop . . . . . . . . . . . . . . . . . . . . . . . . 16Ninlaro . . . . . . . . . . . . . . . . . . . . . . . . . . 12Nisoldipine . . . . . . . . . . . . . . . . . . . . . . 22
Nitro-Bid . . . . . . . . . . . . . . . . . . . . . . . . 20Nitrofurantoin Macrocrystal . . . . . . . . . 8Nitrofurantoin Oral Suspension . . . . . . 8Nitrofurantoin/Nitrofurantoin
Macrocrystal . . . . . . . . . . . . . . . . . . . . 8Nitroglycerin Spray . . . . . . . . . . . . . . . 20Nitroglycerin Sublingual Tablet . . . . . . 20Nitroglycerin Sustained-Action
Capsule . . . . . . . . . . . . . . . . . . . . . . . 20Nitroglycerin Transdermal 24 Hour
Patch . . . . . . . . . . . . . . . . . . . . . . . . . 20Nitromist . . . . . . . . . . . . . . . . . . . . . . . . 20Nitrostat . . . . . . . . . . . . . . . . . . . . . . . . 20Nityr . . . . . . . . . . . . . . . . . . . . . . . . . . . . 49Nizoral . . . . . . . . . . . . . . . . . . . . . . . . 9, 27Nizoral 2% . . . . . . . . . . . . . . . . . . . . . . 27Nolvadex . . . . . . . . . . . . . . . . . . . . . . . . 11Nor-QD . . . . . . . . . . . . . . . . . . . . . . . . . 40Nora-BE . . . . . . . . . . . . . . . . . . . . . . . . 40Norco . . . . . . . . . . . . . . . . . . . . . . . . . . 13Nordete . . . . . . . . . . . . . . . . . . . . . . . . . 38Nordette . . . . . . . . . . . . . . . . . . . . . . . . 38Norditropin . . . . . . . . . . . . . . . . . . . . . . 35Norethindrone 0 .35mg . . . . . . . . . . . . 40Norethindrone Acetate . . . . . . . . . 38-40Norethindrone Acetate/Ethinyl
Estradiol . . . . . . . . . . . . . . . . . . . 38-40Norethindrone Acetate/Ethinyl
Estradiol 1/0 .02mg . . . . . . . . . . . . . 39Norethindrone Acetate/Ethinyl
Estradiol FE 1/20 . . . . . . . . . . . . . . . 38Norethindrone Acetate/Ethinyl
Estradiolwith Iron 1/0 .02 mg . . . . . . 39Norethindrone/Ethinyl Estradiol/
Ferrous Fumarate 0 .8/0 .025 mg Chewable Tablet . . . . . . . . . . . . . . . . 39
Norgestimate-Ethinyl Estradiol 0 .18/0 .035-0 .215/0 .035-0 .25/ 0 .035 mg . . . . . . . . . . . . . . . . . . . . . 38
Norgestimate-Ethinyl Estradiol 0 .18/0 .215/0 .25 mg . . . . . . . . . . . . 39
Norgestimate-Ethinyl Estradiol 0 .25/0 .035 mg . . . . . . . . . . . . . . . . . 38
Noritate . . . . . . . . . . . . . . . . . . . . . . . . . 26Norlyda . . . . . . . . . . . . . . . . . . . . . . . . . 40Norlyroc . . . . . . . . . . . . . . . . . . . . . . . . 40Normodyne . . . . . . . . . . . . . . . . . . . . . . 21Norpace CR . . . . . . . . . . . . . . . . . . . . . 20Norpramin . . . . . . . . . . . . . . . . . . . . . . . 17Nortrel 0 .5/35 . . . . . . . . . . . . . . . . . . . 38Nortrel 7/7/7 . . . . . . . . . . . . . . . . . . . . 38Nortriptyline . . . . . . . . . . . . . . . . . . . . . 17
Norvasc . . . . . . . . . . . . . . . . . . . . . . . . 22Norvir . . . . . . . . . . . . . . . . . . . . . . . . . . . 9Norvir Capsule, Solution . . . . . . . . . . . . 9Novoeight . . . . . . . . . . . . . . . . . . . . . . . 21Novolin Vial . . . . . . . . . . . . . . . . . . . . . . 31NovoLog FlexPen . . . . . . . . . . . . . . . . . 31NovoLog Vial . . . . . . . . . . . . . . . . . . . . 31Novoseven . . . . . . . . . . . . . . . . . . . . . . 21Noxafil Suspension, Tablet . . . . . . . . . . 9NP Thyroid . . . . . . . . . . . . . . . . . . . . . . 30Nucynta . . . . . . . . . . . . . . . . . . . . . . . . 14Nucynta ER . . . . . . . . . . . . . . . . . . . . . 14Nuedexta . . . . . . . . . . . . . . . . . . . . . . . 16Nulytely w/Flavor Packs . . . . . . . . . . . 34Nutropin AQ . . . . . . . . . . . . . . . . . . . . . 35Nutropin AQ NuSpin . . . . . . . . . . . . . . 35Nuvaring . . . . . . . . . . . . . . . . . . . . . . . . 39Nuvigil . . . . . . . . . . . . . . . . . . . . . . . . . . 19Nuwiq . . . . . . . . . . . . . . . . . . . . . . . . . . 21Nystatin . . . . . . . . . . . . . . . . . . . . . . . 9, 27Nystatin Powder, Tablet . . . . . . . . . . . . 9Nystatin/Triamcinolone Acetonide . . . 27OObredon . . . . . . . . . . . . . . . . . . . . . . . . 44Ocaliva . . . . . . . . . . . . . . . . . . . . . . . . . 34Ocella . . . . . . . . . . . . . . . . . . . . . . . . . . 39Octreotide . . . . . . . . . . . . . . . . . . . 12, 30Octreotide Acetate . . . . . . . . . . . . 12, 30Ocuflox . . . . . . . . . . . . . . . . . . . . . . . . . 43Odefsey . . . . . . . . . . . . . . . . . . . . . . . . . 9Odomzo . . . . . . . . . . . . . . . . . . . . . . . . 12Ofev . . . . . . . . . . . . . . . . . . . . . . . . . . . 46Ofloxacin . . . . . . . . . . . . . . . . . . . 8, 29, 43Ofloxacin Tablet . . . . . . . . . . . . . . . . . . . 8Ogen . . . . . . . . . . . . . . . . . . . . . . . . . . . 40Ogestrel . . . . . . . . . . . . . . . . . . . . . . . . 39Olanzapine Rapid-Dissolve Tablet . . . 18Olanzapine Tablet . . . . . . . . . . . . . . . . 18Olanzapine/Fluoxetine . . . . . . . . . . . . . 18Olmesartan . . . . . . . . . . . . . . . . . . . . . . 23Olmesartan/Hydrochlorothiazide . . . . 23Olopatadine 0 .1% . . . . . . . . . . . . . . . . 43Olopatadine 0 .2% . . . . . . . . . . . . . . . . 43Olpatadine . . . . . . . . . . . . . . . . . . . . . . 44Olux, Olux E . . . . . . . . . . . . . . . . . . . . . 25Olysio . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Omeclamox Pak . . . . . . . . . . . . . . . . . . 33Omega-3-Acid Ethyl Esters . . . . . . . . 24Omeprazole . . . . . . . . . . . . . . . . . . . . . 33Omeprazole/Sodium Bicarbonate . . . 33Omnicef . . . . . . . . . . . . . . . . . . . . . . . . . 7Omnitrope . . . . . . . . . . . . . . . . . . . . . . 35

61
2018 Prescription Drug List Medication Index
Ondansetron . . . . . . . . . . . . . . . . . . . . 34Ondansetron Rapid-Dissolve Tablet . 34OneTouch Test Strips . . . . . . . . . . . . . 32OneTouch Ultra 2 . . . . . . . . . . . . . . . . 32OneTouch Ultra Mini . . . . . . . . . . . . . . 32OneTouch Ultra Test Strips . . . . . . . . . 32OneTouch Verio . . . . . . . . . . . . . . . . . . 32OneTouch Verio IQ . . . . . . . . . . . . . . . 32OneTouch Verio Test Strips . . . . . . . . 32Onfi . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16Onglyza . . . . . . . . . . . . . . . . . . . . . . . . . 31Onzetra Xsail . . . . . . . . . . . . . . . . . . . . 14Opana . . . . . . . . . . . . . . . . . . . . . . . . . . 13Opana ER . . . . . . . . . . . . . . . . . . . . . . . 13Opcicon One-Step . . . . . . . . . . . . . . . 39Opsumit . . . . . . . . . . . . . . . . . . . . . . . . 45Option 2 . . . . . . . . . . . . . . . . . . . . . . . . 39Optivar . . . . . . . . . . . . . . . . . . . . . . . . . 43Oracea . . . . . . . . . . . . . . . . . . . . . . . . . . 7Oralair . . . . . . . . . . . . . . . . . . . . . . . . . . 44Orapred ODT . . . . . . . . . . . . . . . . . . . . 30Orencia . . . . . . . . . . . . . . . . . . . . . . . . . 36Orenitram . . . . . . . . . . . . . . . . . . . . . . . 46Orfadin . . . . . . . . . . . . . . . . . . . . . . . . . 49Orsythia . . . . . . . . . . . . . . . . . . . . . . . . 38Ortho Micronor . . . . . . . . . . . . . . . . . . 40Ortho Tri-Cyclen . . . . . . . . . . . . . . 38, 39Ortho Tri-Cyclen Lo . . . . . . . . . . . . . . . 39Ortho-Cept . . . . . . . . . . . . . . . . . . . . . . 38Ortho-Cyclen . . . . . . . . . . . . . . . . . . . . 38Ortho-Evra . . . . . . . . . . . . . . . . . . . . . . 39Ortho-Novum 1/35 . . . . . . . . . . . . . . . 38Ortho-Novum 10/11 . . . . . . . . . . . . . . 38Ortho-Novum 7/7/7 . . . . . . . . . . . . . . 38Ortho-Tri-Cyclen Lo . . . . . . . . . . . . . . 39Orudis . . . . . . . . . . . . . . . . . . . . . . . . . . 36Oseltamivir Capsule, Suspension . . . . 8Oseni . . . . . . . . . . . . . . . . . . . . . . . . . . 31Osmoprep . . . . . . . . . . . . . . . . . . . . . . 34Osphena . . . . . . . . . . . . . . . . . . . . . . . . 47Otezla . . . . . . . . . . . . . . . . . . . . . . . . . . 36Otrexup . . . . . . . . . . . . . . . . . . . . . . . . . 36Ovcon-35 . . . . . . . . . . . . . . . . . . . . 38, 39Ovide . . . . . . . . . . . . . . . . . . . . . . . . . . 27Ovidrel . . . . . . . . . . . . . . . . . . . . . . . . . 41Ovral . . . . . . . . . . . . . . . . . . . . . . . . 38, 39Oxandrin . . . . . . . . . . . . . . . . . . . . . 11, 30Oxandrolone Tablet . . . . . . . . . . . . 11, 30Oxaprozin . . . . . . . . . . . . . . . . . . . . . . . 36Oxcarbazepine Tablet . . . . . . . . . . . . . 15Oxiconazole Cream . . . . . . . . . . . . . . . 27Oxistat . . . . . . . . . . . . . . . . . . . . . . . . . . 27
Oxsoralen-Ultra . . . . . . . . . . . . . . . . . . 28Oxtellar XR . . . . . . . . . . . . . . . . . . . . . . 16Oxybutynin Chloride . . . . . . . . . . . . . . 47Oxybutynin Chloride
Sustained-Release Tablet . . . . . . . . 47Oxycodone Controlled-Release
Tablet . . . . . . . . . . . . . . . . . . . . . . . . . 13Oxycodone HCl . . . . . . . . . . . . . . . . . . 13Oxycodone HCl/Acetaminophen
Tablet . . . . . . . . . . . . . . . . . . . . . . . . . 13OxyContin . . . . . . . . . . . . . . . . . . . . . . 13OxyIR . . . . . . . . . . . . . . . . . . . . . . . . . . 13Oxymorphone HCl Sustained-Release
12 Hour Tablet . . . . . . . . . . . . . . . . . 13Oxymorphone Tablet . . . . . . . . . . . . . . 13PPaliperidone . . . . . . . . . . . . . . . . . . . . . 18Pamelor . . . . . . . . . . . . . . . . . . . . . . . . . 17Pancreaze . . . . . . . . . . . . . . . . . . . . . . . 34Pantoprazole . . . . . . . . . . . . . . . . . . . . 33Parafon Forte DSC . . . . . . . . . . . . . . . 36Paricalcitol . . . . . . . . . . . . . . . . . . . . . . 30Parlodel . . . . . . . . . . . . . . . . . . . . . . . . . 15Parnate . . . . . . . . . . . . . . . . . . . . . . . . . 17Paromomycin Capsule . . . . . . . . . . . . 10Paroxetine Sustained-Release
24 Hour Capsule . . . . . . . . . . . . . . . 18Paroxetine Tablet . . . . . . . . . . . . . . . . . 18Pataday . . . . . . . . . . . . . . . . . . . . . . . . . 43Patanase . . . . . . . . . . . . . . . . . . . . . . . . 44Patanol . . . . . . . . . . . . . . . . . . . . . . . . . 43Paxil . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18Paxil CR . . . . . . . . . . . . . . . . . . . . . . . . 18Pediapred . . . . . . . . . . . . . . . . . . . . . . . 30Pegasys . . . . . . . . . . . . . . . . . . . . . . . . 35Pen-V K . . . . . . . . . . . . . . . . . . . . . . . . . 7Penicillin V Potassium . . . . . . . . . . . . . . 7Penlac . . . . . . . . . . . . . . . . . . . . . . . . . . 27Pentasa . . . . . . . . . . . . . . . . . . . . . . . . . 34Percocet . . . . . . . . . . . . . . . . . . . . . . . . 13Perforomist . . . . . . . . . . . . . . . . . . . . . . 45Periactin . . . . . . . . . . . . . . . . . . . . . . . . 44Peridex . . . . . . . . . . . . . . . . . . . . . . . . . 29Periostat . . . . . . . . . . . . . . . . . . . . . . . . . 7Permethrin . . . . . . . . . . . . . . . . . . . . . . 27Perphenazine . . . . . . . . . . . . . . . . . . . . 18Persantine . . . . . . . . . . . . . . . . . . . . . . 20Pertzye . . . . . . . . . . . . . . . . . . . . . . . . . 34Phenazopyridine HCl . . . . . . . . . . . . . . 47Phenelzine . . . . . . . . . . . . . . . . . . . . . . 17Phenergan . . . . . . . . . . . . . . . . . . . 34, 44Phenergan VC w/Codeine . . . . . . . . . 44
Phenergan w/Codeine . . . . . . . . . . . . 44Phenobarbital . . . . . . . . . . . . . . . . . . . . 15Phenobarbital Tablet . . . . . . . . . . . . . . 15Phenylephrine/Codeine/
Promethazine . . . . . . . . . . . . . . . . . . 44Phenytoin Capsule . . . . . . . . . . . . . . . 15Phenytoin Sodium Extended-Release
Capsule . . . . . . . . . . . . . . . . . . . . . . . 15Philith . . . . . . . . . . . . . . . . . . . . . . . . . . 39PhosLo . . . . . . . . . . . . . . . . . . . . . . . . . 49Picato . . . . . . . . . . . . . . . . . . . . . . . . . . 28Pilocarpine . . . . . . . . . . . . . . . .29, 42, 49Pilocarpine HCl . . . . . . . . . . . . . . . . . . 49Pilocarpine Ophthalmic Solution . . . . 42Pimtrea . . . . . . . . . . . . . . . . . . . . . . . . . 39Pioglitazone . . . . . . . . . . . . . . . . . . . . . 31Pioglitazone/Glimepiride . . . . . . . . . . . 31Pioglitazone/Metformin . . . . . . . . . . . . 31Pirmella 1/35 . . . . . . . . . . . . . . . . . . . . 38Pirmella 7/7/7 . . . . . . . . . . . . . . . . . . . 38Piroxicam . . . . . . . . . . . . . . . . . . . . . . . 36Plan B One Step . . . . . . . . . . . . . . . . . 39Plan B One-Step . . . . . . . . . . . . . . . . . 39Plaquenil . . . . . . . . . . . . . . . . . . . . . 10, 36Plavix . . . . . . . . . . . . . . . . . . . . . . . . . . . 20Plegridy . . . . . . . . . . . . . . . . . . . . . . . . . 16Plendil . . . . . . . . . . . . . . . . . . . . . . . . . . 22Pletal . . . . . . . . . . . . . . . . . . . . . . . . . . . 20Podofilox Liquid . . . . . . . . . . . . . . . . . . 28Poly-Vi-Flor . . . . . . . . . . . . . . . . . . . . . . 48Poly-Vi-Flor w/Iron . . . . . . . . . . . . . . . . 48Polyethylene Glycol 3350 Powder . . 34Polymyxin B Sulfate/Trimethoprim . . . 43Polysporin . . . . . . . . . . . . . . . . . . . . . . . 43Polytrim . . . . . . . . . . . . . . . . . . . . . . . . . 43Pomalyst . . . . . . . . . . . . . . . . . . . . . . . . 12Portia-28 . . . . . . . . . . . . . . . . . . . . . . . . 38Potassium Chloride . . . . . . . . . . . . 34, 48Potassium Chloride Packet . . . . . . . . 48Potassium Chloride Sustained-Action
Capsule . . . . . . . . . . . . . . . . . . . . . . . 48Potassium Chloride Sustained-Action
Tablet . . . . . . . . . . . . . . . . . . . . . . . . . 48Pradaxa . . . . . . . . . . . . . . . . . . . . . . . . . 20Praluent . . . . . . . . . . . . . . . . . . . . . . . . 24Pramipexole . . . . . . . . . . . . . . . . . . . . . 15Pramipexole Extended-Release . . . . . 15Prandin . . . . . . . . . . . . . . . . . . . . . . . . . 31Prasugrel . . . . . . . . . . . . . . . . . . . . . . . 20Pravachol . . . . . . . . . . . . . . . . . . . . . . . 24Pravastatin . . . . . . . . . . . . . . . . . . . . . . 24Prazosin . . . . . . . . . . . . . . . . . . . . . . . . 22
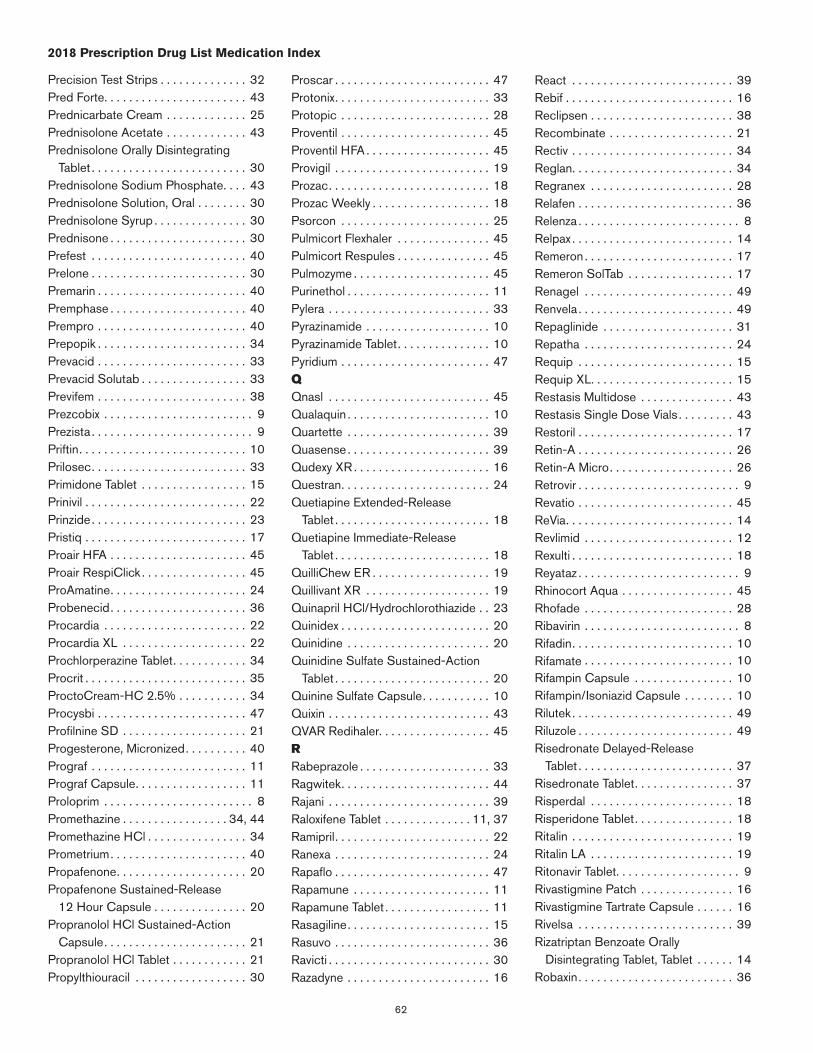
62
2018 Prescription Drug List Medication Index
Precision Test Strips . . . . . . . . . . . . . . 32Pred Forte . . . . . . . . . . . . . . . . . . . . . . . 43Prednicarbate Cream . . . . . . . . . . . . . 25Prednisolone Acetate . . . . . . . . . . . . . 43Prednisolone Orally Disintegrating
Tablet . . . . . . . . . . . . . . . . . . . . . . . . . 30Prednisolone Sodium Phosphate . . . . 43Prednisolone Solution, Oral . . . . . . . . 30Prednisolone Syrup . . . . . . . . . . . . . . . 30Prednisone . . . . . . . . . . . . . . . . . . . . . . 30Prefest . . . . . . . . . . . . . . . . . . . . . . . . . 40Prelone . . . . . . . . . . . . . . . . . . . . . . . . . 30Premarin . . . . . . . . . . . . . . . . . . . . . . . . 40Premphase . . . . . . . . . . . . . . . . . . . . . . 40Prempro . . . . . . . . . . . . . . . . . . . . . . . . 40Prepopik . . . . . . . . . . . . . . . . . . . . . . . . 34Prevacid . . . . . . . . . . . . . . . . . . . . . . . . 33Prevacid Solutab . . . . . . . . . . . . . . . . . 33Previfem . . . . . . . . . . . . . . . . . . . . . . . . 38Prezcobix . . . . . . . . . . . . . . . . . . . . . . . . 9Prezista . . . . . . . . . . . . . . . . . . . . . . . . . . 9Priftin . . . . . . . . . . . . . . . . . . . . . . . . . . . 10Prilosec . . . . . . . . . . . . . . . . . . . . . . . . . 33Primidone Tablet . . . . . . . . . . . . . . . . . 15Prinivil . . . . . . . . . . . . . . . . . . . . . . . . . . 22Prinzide . . . . . . . . . . . . . . . . . . . . . . . . . 23Pristiq . . . . . . . . . . . . . . . . . . . . . . . . . . 17Proair HFA . . . . . . . . . . . . . . . . . . . . . . 45Proair RespiClick . . . . . . . . . . . . . . . . . 45ProAmatine . . . . . . . . . . . . . . . . . . . . . . 24Probenecid . . . . . . . . . . . . . . . . . . . . . . 36Procardia . . . . . . . . . . . . . . . . . . . . . . . 22Procardia XL . . . . . . . . . . . . . . . . . . . . 22Prochlorperazine Tablet . . . . . . . . . . . . 34Procrit . . . . . . . . . . . . . . . . . . . . . . . . . . 35ProctoCream-HC 2 .5% . . . . . . . . . . . 34Procysbi . . . . . . . . . . . . . . . . . . . . . . . . 47Profilnine SD . . . . . . . . . . . . . . . . . . . . 21Progesterone, Micronized . . . . . . . . . . 40Prograf . . . . . . . . . . . . . . . . . . . . . . . . . 11Prograf Capsule . . . . . . . . . . . . . . . . . . 11Proloprim . . . . . . . . . . . . . . . . . . . . . . . . 8Promethazine . . . . . . . . . . . . . . . . . 34, 44Promethazine HCl . . . . . . . . . . . . . . . . 34Prometrium . . . . . . . . . . . . . . . . . . . . . . 40Propafenone . . . . . . . . . . . . . . . . . . . . . 20Propafenone Sustained-Release
12 Hour Capsule . . . . . . . . . . . . . . . 20Propranolol HCl Sustained-Action
Capsule . . . . . . . . . . . . . . . . . . . . . . . 21Propranolol HCl Tablet . . . . . . . . . . . . 21Propylthiouracil . . . . . . . . . . . . . . . . . . 30
Proscar . . . . . . . . . . . . . . . . . . . . . . . . . 47Protonix . . . . . . . . . . . . . . . . . . . . . . . . . 33Protopic . . . . . . . . . . . . . . . . . . . . . . . . 28Proventil . . . . . . . . . . . . . . . . . . . . . . . . 45Proventil HFA . . . . . . . . . . . . . . . . . . . . 45Provigil . . . . . . . . . . . . . . . . . . . . . . . . . 19Prozac . . . . . . . . . . . . . . . . . . . . . . . . . . 18Prozac Weekly . . . . . . . . . . . . . . . . . . . 18Psorcon . . . . . . . . . . . . . . . . . . . . . . . . 25Pulmicort Flexhaler . . . . . . . . . . . . . . . 45Pulmicort Respules . . . . . . . . . . . . . . . 45Pulmozyme . . . . . . . . . . . . . . . . . . . . . . 45Purinethol . . . . . . . . . . . . . . . . . . . . . . . 11Pylera . . . . . . . . . . . . . . . . . . . . . . . . . . 33Pyrazinamide . . . . . . . . . . . . . . . . . . . . 10Pyrazinamide Tablet . . . . . . . . . . . . . . . 10Pyridium . . . . . . . . . . . . . . . . . . . . . . . . 47QQnasl . . . . . . . . . . . . . . . . . . . . . . . . . . 45Qualaquin . . . . . . . . . . . . . . . . . . . . . . . 10Quartette . . . . . . . . . . . . . . . . . . . . . . . 39Quasense . . . . . . . . . . . . . . . . . . . . . . . 39Qudexy XR . . . . . . . . . . . . . . . . . . . . . . 16Questran . . . . . . . . . . . . . . . . . . . . . . . . 24Quetiapine Extended-Release
Tablet . . . . . . . . . . . . . . . . . . . . . . . . . 18Quetiapine Immediate-Release
Tablet . . . . . . . . . . . . . . . . . . . . . . . . . 18QuilliChew ER . . . . . . . . . . . . . . . . . . . 19Quillivant XR . . . . . . . . . . . . . . . . . . . . 19Quinapril HCl/Hydrochlorothiazide . . 23Quinidex . . . . . . . . . . . . . . . . . . . . . . . . 20Quinidine . . . . . . . . . . . . . . . . . . . . . . . 20Quinidine Sulfate Sustained-Action
Tablet . . . . . . . . . . . . . . . . . . . . . . . . . 20Quinine Sulfate Capsule . . . . . . . . . . . 10Quixin . . . . . . . . . . . . . . . . . . . . . . . . . . 43QVAR Redihaler . . . . . . . . . . . . . . . . . . 45RRabeprazole . . . . . . . . . . . . . . . . . . . . . 33Ragwitek . . . . . . . . . . . . . . . . . . . . . . . . 44Rajani . . . . . . . . . . . . . . . . . . . . . . . . . . 39Raloxifene Tablet . . . . . . . . . . . . . . 11, 37Ramipril . . . . . . . . . . . . . . . . . . . . . . . . . 22Ranexa . . . . . . . . . . . . . . . . . . . . . . . . . 24Rapaflo . . . . . . . . . . . . . . . . . . . . . . . . . 47Rapamune . . . . . . . . . . . . . . . . . . . . . . 11Rapamune Tablet . . . . . . . . . . . . . . . . . 11Rasagiline . . . . . . . . . . . . . . . . . . . . . . . 15Rasuvo . . . . . . . . . . . . . . . . . . . . . . . . . 36Ravicti . . . . . . . . . . . . . . . . . . . . . . . . . . 30Razadyne . . . . . . . . . . . . . . . . . . . . . . . 16
React . . . . . . . . . . . . . . . . . . . . . . . . . . 39Rebif . . . . . . . . . . . . . . . . . . . . . . . . . . . 16Reclipsen . . . . . . . . . . . . . . . . . . . . . . . 38Recombinate . . . . . . . . . . . . . . . . . . . . 21Rectiv . . . . . . . . . . . . . . . . . . . . . . . . . . 34Reglan . . . . . . . . . . . . . . . . . . . . . . . . . . 34Regranex . . . . . . . . . . . . . . . . . . . . . . . 28Relafen . . . . . . . . . . . . . . . . . . . . . . . . . 36Relenza . . . . . . . . . . . . . . . . . . . . . . . . . . 8Relpax . . . . . . . . . . . . . . . . . . . . . . . . . . 14Remeron . . . . . . . . . . . . . . . . . . . . . . . . 17Remeron SolTab . . . . . . . . . . . . . . . . . 17Renagel . . . . . . . . . . . . . . . . . . . . . . . . 49Renvela . . . . . . . . . . . . . . . . . . . . . . . . . 49Repaglinide . . . . . . . . . . . . . . . . . . . . . 31Repatha . . . . . . . . . . . . . . . . . . . . . . . . 24Requip . . . . . . . . . . . . . . . . . . . . . . . . . 15Requip XL . . . . . . . . . . . . . . . . . . . . . . . 15Restasis Multidose . . . . . . . . . . . . . . . 43Restasis Single Dose Vials . . . . . . . . . 43Restoril . . . . . . . . . . . . . . . . . . . . . . . . . 17Retin-A . . . . . . . . . . . . . . . . . . . . . . . . . 26Retin-A Micro . . . . . . . . . . . . . . . . . . . . 26Retrovir . . . . . . . . . . . . . . . . . . . . . . . . . . 9Revatio . . . . . . . . . . . . . . . . . . . . . . . . . 45ReVia . . . . . . . . . . . . . . . . . . . . . . . . . . . 14Revlimid . . . . . . . . . . . . . . . . . . . . . . . . 12Rexulti . . . . . . . . . . . . . . . . . . . . . . . . . . 18Reyataz . . . . . . . . . . . . . . . . . . . . . . . . . . 9Rhinocort Aqua . . . . . . . . . . . . . . . . . . 45Rhofade . . . . . . . . . . . . . . . . . . . . . . . . 28Ribavirin . . . . . . . . . . . . . . . . . . . . . . . . . 8Rifadin . . . . . . . . . . . . . . . . . . . . . . . . . . 10Rifamate . . . . . . . . . . . . . . . . . . . . . . . . 10Rifampin Capsule . . . . . . . . . . . . . . . . 10Rifampin/Isoniazid Capsule . . . . . . . . 10Rilutek . . . . . . . . . . . . . . . . . . . . . . . . . . 49Riluzole . . . . . . . . . . . . . . . . . . . . . . . . . 49Risedronate Delayed-Release
Tablet . . . . . . . . . . . . . . . . . . . . . . . . . 37Risedronate Tablet . . . . . . . . . . . . . . . . 37Risperdal . . . . . . . . . . . . . . . . . . . . . . . 18Risperidone Tablet . . . . . . . . . . . . . . . . 18Ritalin . . . . . . . . . . . . . . . . . . . . . . . . . . 19Ritalin LA . . . . . . . . . . . . . . . . . . . . . . . 19Ritonavir Tablet . . . . . . . . . . . . . . . . . . . . 9Rivastigmine Patch . . . . . . . . . . . . . . . 16Rivastigmine Tartrate Capsule . . . . . . 16Rivelsa . . . . . . . . . . . . . . . . . . . . . . . . . 39Rizatriptan Benzoate Orally
Disintegrating Tablet, Tablet . . . . . . 14Robaxin . . . . . . . . . . . . . . . . . . . . . . . . . 36
63
2018 Prescription Drug List Medication Index
Robinul, Robinul Forte . . . . . . . . . . . . . 33Robitussin A-C . . . . . . . . . . . . . . . . . . 44Robitussin-DAC . . . . . . . . . . . . . . . . . . 44Rocaltrol . . . . . . . . . . . . . . . . . . . . . . . . 30Ropinirole . . . . . . . . . . . . . . . . . . . . . . . 15Ropinirole Extended-Release
24 Hour Tablet . . . . . . . . . . . . . . . . . 15Rosuvastain . . . . . . . . . . . . . . . . . . . . . 24Rowasa . . . . . . . . . . . . . . . . . . . . . . . . . 34Roxicet . . . . . . . . . . . . . . . . . . . . . . . . . 13Roxicodone . . . . . . . . . . . . . . . . . . . . . 13Rozerem . . . . . . . . . . . . . . . . . . . . . . . . 17Rubraca . . . . . . . . . . . . . . . . . . . . . . . . 12Ruconest . . . . . . . . . . . . . . . . . . . . . . . 44Rydapt . . . . . . . . . . . . . . . . . . . . . . . . . 12Rytary . . . . . . . . . . . . . . . . . . . . . . . . . . 15Rythmol . . . . . . . . . . . . . . . . . . . . . . . . . 20Rythmol SR . . . . . . . . . . . . . . . . . . . . . 20SSabril . . . . . . . . . . . . . . . . . . . . . . . . . . . 15Safyral . . . . . . . . . . . . . . . . . . . . . . . . . . 39Saizen . . . . . . . . . . . . . . . . . . . . . . . . . . 35Salagen . . . . . . . . . . . . . . . . . . . . . 29, 49Salagen 5 mg . . . . . . . . . . . . . . . . . . . . 29Salflex . . . . . . . . . . . . . . . . . . . . . . . . . . 36Salsalate . . . . . . . . . . . . . . . . . . . . . . . . 36Samsca . . . . . . . . . . . . . . . . . . . . . . . . . 30Sanctura XR . . . . . . . . . . . . . . . . . . . . . 47Sandimmune Capsule . . . . . . . . . . . . . 11Sandostatin . . . . . . . . . . . . . . . . . . . . . 12Santyl . . . . . . . . . . . . . . . . . . . . . . . . . . 27Saphris . . . . . . . . . . . . . . . . . . . . . . . . . 18Savaysa . . . . . . . . . . . . . . . . . . . . . . . . 20Savella . . . . . . . . . . . . . . . . . . . . . . . . . 16Scopolamine Transdermal Patch . . . . 34Seasonale . . . . . . . . . . . . . . . . . . . . 38, 39Seasonique . . . . . . . . . . . . . . . . . . . . . 39Sectral . . . . . . . . . . . . . . . . . . . . . . . . . 21Selegiline . . . . . . . . . . . . . . . . . . . . . . . 15Selzentry . . . . . . . . . . . . . . . . . . . . . . . . . 9Sensipar . . . . . . . . . . . . . . . . . . . . . . . . 30Septra, Septra DS . . . . . . . . . . . . . . . . . 8Serevent Diskus . . . . . . . . . . . . . . . . . . 45Serophene . . . . . . . . . . . . . . . . . . . . . . 41Seroquel . . . . . . . . . . . . . . . . . . . . . . . . 18Seroquel XR . . . . . . . . . . . . . . . . . . . . . 18Serostim . . . . . . . . . . . . . . . . . . . . . . . . 35Sertraline . . . . . . . . . . . . . . . . . . . . . . . 18Serzone . . . . . . . . . . . . . . . . . . . . . . . . 17Setlakin . . . . . . . . . . . . . . . . . . . . . . . . . 39Sevelamer . . . . . . . . . . . . . . . . . . . . . . . 49Sharobel . . . . . . . . . . . . . . . . . . . . . . . . 40
Sildenafil . . . . . . . . . . . . . . . . . . . . . 45, 47Silenor . . . . . . . . . . . . . . . . . . . . . . . . . . 17Siliq . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36Silvadene . . . . . . . . . . . . . . . . . . . . . . . 27Silver Sulfadiazine . . . . . . . . . . . . . . . . 27Simbrinza . . . . . . . . . . . . . . . . . . . . . . . 42Simponi . . . . . . . . . . . . . . . . . . . . . . . . . 36Simvastatin . . . . . . . . . . . . . . . . . . . . . . 24Sinemet . . . . . . . . . . . . . . . . . . . . . . . . 15Sinemet CR . . . . . . . . . . . . . . . . . . . . . 15Sinequan . . . . . . . . . . . . . . . . . . . . . . . 17Singulair . . . . . . . . . . . . . . . . . . . . . . . . 45Sirolimus . . . . . . . . . . . . . . . . . . . . . . . . 11Skelaxin . . . . . . . . . . . . . . . . . . . . . . . . . 36Sklice . . . . . . . . . . . . . . . . . . . . . . . . . . 27Sod Chloride/NaHCO3/KCl/PEGs . 34Sodium Fluoride . . . . . . . . . . . . . . . . . . 48Sodium Sulamyd . . . . . . . . . . . . . . . . . 43Sodium Sulfate/Sodium/Sodium
Bicarbonate/Potassium Chloride/Polyethylene Glycols . . . . . . . . . . . . 34
Sodium Sulfate/Sodium/Sodium Bicarbonate/Potassium Chloride/Polyethylene Glycols Solution, Reconstituted, Oral . . . . . . . . . . . . . 34
Solaraze . . . . . . . . . . . . . . . . . . . . . . . . 28Solia . . . . . . . . . . . . . . . . . . . . . . . . . . . 38Soliqua . . . . . . . . . . . . . . . . . . . . . . . . . 31Solodyn . . . . . . . . . . . . . . . . . . . . . . . . . . 7Solodyn 45, 65, 90, 115, 135 mg . . . . 7Soma 350 mg . . . . . . . . . . . . . . . . . . . 36Somatuline Depot . . . . . . . . . . . . . . . . 12Sonata . . . . . . . . . . . . . . . . . . . . . . . . . 17Soolantra . . . . . . . . . . . . . . . . . . . . . . . 26Soriatane . . . . . . . . . . . . . . . . . . . . . . . 27Sotalol HCl . . . . . . . . . . . . . . . . . . . . . . 20Sovaldi . . . . . . . . . . . . . . . . . . . . . . . . . . 8Spectazole 1% . . . . . . . . . . . . . . . . . . 27Spectracef . . . . . . . . . . . . . . . . . . . . . . . 7Spinosad . . . . . . . . . . . . . . . . . . . . . . . 27Spiriva Handihaler . . . . . . . . . . . . . . . . 46Spiriva Respimat . . . . . . . . . . . . . . . . . 46Spironolactone . . . . . . . . . . . . . . . . . . . 21Spironolactone/
Hydrochlorothiazide . . . . . . . . . . . . . 21Sporanox Capsule . . . . . . . . . . . . . . . . . 9Sporanox Solution, Oral . . . . . . . . . . . . 9Sprintec-28 . . . . . . . . . . . . . . . . . . . . . 38Sprycel . . . . . . . . . . . . . . . . . . . . . . . . . 12Sronyx . . . . . . . . . . . . . . . . . . . . . . . . . . 38Stadol . . . . . . . . . . . . . . . . . . . . . . . . . . 14Stalevo . . . . . . . . . . . . . . . . . . . . . . . . . 15
Stavudine Capsule . . . . . . . . . . . . . . . . 9Staxyn . . . . . . . . . . . . . . . . . . . . . . . . . . 47Stelara . . . . . . . . . . . . . . . . . . . . . . . . . 36Stendra . . . . . . . . . . . . . . . . . . . . . . . . . 47Stiolto Respimat . . . . . . . . . . . . . . . . . 46Stivarga . . . . . . . . . . . . . . . . . . . . . . . . . 12Strattera . . . . . . . . . . . . . . . . . . . . . . . . 19Stribild . . . . . . . . . . . . . . . . . . . . . . . . . . 9Striverdi Respimat . . . . . . . . . . . . . . . . 45Stromectol . . . . . . . . . . . . . . . . . . . . . . 10Suboxone . . . . . . . . . . . . . . . . . . . . . . . 14Suboxone Film . . . . . . . . . . . . . . . . . . . 14Subutex . . . . . . . . . . . . . . . . . . . . . . . . . 14Sucralfate Tablet . . . . . . . . . . . . . . . . . 33Sular . . . . . . . . . . . . . . . . . . . . . . . . . . . 22Sulfacetamide Sodium . . . . . . . . . . . . 43Sulfacetamide Sodium/Prednisolone
Sodium Phosphate . . . . . . . . . . . . . . 43Sulfamethoxazole/Trimethoprim . . . . . . 8Sulfasalazine Enteric-Coated
Tablet . . . . . . . . . . . . . . . . . . . . . . 34, 36Sulfasalazine Tablet . . . . . . . . . . . . 34, 36Sulindac . . . . . . . . . . . . . . . . . . . . . . . . 36Sumatriptan Succinate Injection . . . . 14Sumatriptan Succinate Nasal Spray . 14Sumatriptan Succinate Tablet . . . . . . 14Sumatriptan/Naproxen 85-500 mg . . 14Suprax . . . . . . . . . . . . . . . . . . . . . . . . . . . 7Suprax Tablet, Chewable Tablet,
Capsule . . . . . . . . . . . . . . . . . . . . . . . . 7Suprep . . . . . . . . . . . . . . . . . . . . . . . . . 34Sustiva . . . . . . . . . . . . . . . . . . . . . . . . . . 9Sutent . . . . . . . . . . . . . . . . . . . . . . . . . . 12Syeda . . . . . . . . . . . . . . . . . . . . . . . . . . 39Sylatron . . . . . . . . . . . . . . . . . . . . . . . . . 12Symbicort . . . . . . . . . . . . . . . . . . . . . . . 46Symbyax . . . . . . . . . . . . . . . . . . . . . . . . 18Symmetrel . . . . . . . . . . . . . . . . . . . . 8, 15Synalar . . . . . . . . . . . . . . . . . . . . . . 25, 26Synarel . . . . . . . . . . . . . . . . . . . . . . 30, 41Synjardy . . . . . . . . . . . . . . . . . . . . . . . . 31Synjardy XR . . . . . . . . . . . . . . . . . . . . . 31Synthroid . . . . . . . . . . . . . . . . . . . . . . . 30Syprine . . . . . . . . . . . . . . . . . . . . . . . . . 30TTaclonex . . . . . . . . . . . . . . . . . . . . . . . . 27Taclonex Suspension . . . . . . . . . . . . . . 27Tacrolimus . . . . . . . . . . . . . . . . . . . 11, 28Tacrolimus Anhydrous . . . . . . . . . . . . . 11Tafinlar . . . . . . . . . . . . . . . . . . . . . . . . . . 12Take Action . . . . . . . . . . . . . . . . . . . . . . 39Taltz . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36
64
2018 Prescription Drug List Medication Index
Tambocor . . . . . . . . . . . . . . . . . . . . . . . 20Tamiflu . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Tamoxifen Tablet . . . . . . . . . . . . . . . . . . 11Tamsulosin HCl . . . . . . . . . . . . . . . . . . 47Tanzeum . . . . . . . . . . . . . . . . . . . . . . . . 31Tapazole . . . . . . . . . . . . . . . . . . . . . . . . 30Tarceva . . . . . . . . . . . . . . . . . . . . . . . . . 12Targretin . . . . . . . . . . . . . . . . . . . . . . . . 12Targretin Capsule . . . . . . . . . . . . . . . . 12Targretin Gel . . . . . . . . . . . . . . . . . . . . . 12Tarina FE 1/20 . . . . . . . . . . . . . . . . . . . 38Tarka . . . . . . . . . . . . . . . . . . . . . . . . . . . 23Tasigna . . . . . . . . . . . . . . . . . . . . . . . . . 12Taytulla . . . . . . . . . . . . . . . . . . . . . . . . . 39Tazarotene 0 .1% Cream . . . . . . . . . . . 26Tazorac . . . . . . . . . . . . . . . . . . . . . . . . . 26Tazorac 0 .1% Cream . . . . . . . . . . . . . . 26Tazorac Gel, 0 .05% Cream . . . . . . . . 26Tecfidera . . . . . . . . . . . . . . . . . . . . . . . . 16Technivie . . . . . . . . . . . . . . . . . . . . . . . . . 8Tegretol . . . . . . . . . . . . . . . . . . . . . . 15, 16Tegretol XR . . . . . . . . . . . . . . . . . . . . . . 16Tekturna . . . . . . . . . . . . . . . . . . . . . . . . 23Tekturna HCT . . . . . . . . . . . . . . . . . . . . 23Telmisartan . . . . . . . . . . . . . . . . . . . . . . 23Telmisartan/Hydrochlorothiazide . . . . 23Temazepam . . . . . . . . . . . . . . . . . . . . . 17Temodar . . . . . . . . . . . . . . . . . . . . . . . . 11Temovate . . . . . . . . . . . . . . . . . . . . . . . 25Temovate E . . . . . . . . . . . . . . . . . . . . . . 25Temozolamide Capsule . . . . . . . . . . . . 11Tenex . . . . . . . . . . . . . . . . . . . . . . . . . . . 22Tenofovir Tablet . . . . . . . . . . . . . . . . . . . 9Tenormin . . . . . . . . . . . . . . . . . . . . . . . . 21Terazol . . . . . . . . . . . . . . . . . . . . . . . . . . 41Terazosin . . . . . . . . . . . . . . . . . . . . . 22, 47Terazosin HCl . . . . . . . . . . . . . . . . . . . . 47Terbinafine Tablet . . . . . . . . . . . . . . . . . . 9Terbutaline . . . . . . . . . . . . . . . . . . . 41, 45Terconazole Cream w/Applicator . . . . 41Terconazole Suppository, Vaginal . . . . 41Testim . . . . . . . . . . . . . . . . . . . . . . . . . . 30Testosterone 1% Gel . . . . . . . . . . . . . 30Testosterone Solution . . . . . . . . . . . . . 30Tetrabenazine . . . . . . . . . . . . . . . . . . . . 16Tetracycline HCl . . . . . . . . . . . . . . . . . . 7Teveten . . . . . . . . . . . . . . . . . . . . . . . . . 23Thalomid . . . . . . . . . . . . . . . . . . . . . . . . 12Theochron . . . . . . . . . . . . . . . . . . . . . . 45Theophylline Anhydrous Extended-
Release 12 Hour Tablet . . . . . . . . . . 45Thorazine 200 mg . . . . . . . . . . . . . . . . 18
Thrive Gum . . . . . . . . . . . . . . . . . . . . . . 49Tiagabine Tablet . . . . . . . . . . . . . . . . . . 15Tiazac . . . . . . . . . . . . . . . . . . . . . . . . . . 22Tikosyn . . . . . . . . . . . . . . . . . . . . . . . . . 20Tilia FE . . . . . . . . . . . . . . . . . . . . . . . . . 39Timolol 0 .5% Ophthalmic Solution . . 42Timolol Ophthalmic Gel . . . . . . . . . . . 42Timolol Ophthalmic Solution . . . . . . . . 42Timoptic . . . . . . . . . . . . . . . . . . . . . . . . 42Timoptic-XE . . . . . . . . . . . . . . . . . . . . . 42Tindamax . . . . . . . . . . . . . . . . . . . . . . . . 10Tinidazole . . . . . . . . . . . . . . . . . . . . . . . 10Tirosint . . . . . . . . . . . . . . . . . . . . . . . . . 30Tivicay . . . . . . . . . . . . . . . . . . . . . . . . . . . 9Tizanidine Capsule . . . . . . . . . . . . . . . 36Tizanidine Tablet . . . . . . . . . . . . . . . . . . 36Tobi . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9Tobi Podhaler . . . . . . . . . . . . . . . . . . . . . 9Tobradex . . . . . . . . . . . . . . . . . . . . . . . . 43Tobramycin Nebulized Solution . . . . . . 9Tobramycin Sulfate Drops . . . . . . . . . . 43Tobramycin/Dexamethasone
Suspension . . . . . . . . . . . . . . . . . . . . 43Tobrex . . . . . . . . . . . . . . . . . . . . . . . . . . 43Tobrex Ointment . . . . . . . . . . . . . . . . . . 43Tofranil-PM . . . . . . . . . . . . . . . . . . . . . . 17Tolterodine Extended-Release . . . . . . 47Topamax . . . . . . . . . . . . . . . . . . . . . 15, 16Topicort . . . . . . . . . . . . . . . . . . . . . . . . . 25Topiramate Capsule, Sprinkle . . . . . . . 15Topiramate Tablet . . . . . . . . . . . . . . . . . 15Toprol XL 25 mg . . . . . . . . . . . . . . . . . 21Toprol XL 50, 100, 200 mg . . . . . . . . 21Toradol . . . . . . . . . . . . . . . . . . . . . . . . . 36Toujeo Solostar . . . . . . . . . . . . . . . . . . 31Toviaz . . . . . . . . . . . . . . . . . . . . . . . . . . 47Tracleer . . . . . . . . . . . . . . . . . . . . . . . . . 45Tradjenta . . . . . . . . . . . . . . . . . . . . . . . . 31Tramadol HCl . . . . . . . . . . . . . . . . . . . . 14Tramadol HCl Sustained-Release 24
Hour Tablet . . . . . . . . . . . . . . . . . . . . 14Tramadol HCl/Acetaminophen . . . . . . 14Trandolapril . . . . . . . . . . . . . . . . . . . 22, 23Trandolapril/Verapamil . . . . . . . . . . . . . 23Tranexamic Acid . . . . . . . . . . . . . . . . . . 41Transderm Scop . . . . . . . . . . . . . . . . . 34Transderm-Nitro . . . . . . . . . . . . . . . . . . 20Tranylcypromine . . . . . . . . . . . . . . . . . . 17Travatan . . . . . . . . . . . . . . . . . . . . . . . . 42Travatan Z . . . . . . . . . . . . . . . . . . . . . . . 42Travoprost . . . . . . . . . . . . . . . . . . . . . . . 42Trazodone . . . . . . . . . . . . . . . . . . . . . . . 17
Tremfya . . . . . . . . . . . . . . . . . . . . . . . . . 36Tresiba FlexTouch . . . . . . . . . . . . . . . . 31Tretinoin 0 .05% Gel . . . . . . . . . . . . . . 26Tretinoin Capsule . . . . . . . . . . . . . . . . . 12Tretinoin Cream . . . . . . . . . . . . . . . . . . 26Tretinoin Gel . . . . . . . . . . . . . . . . . . . . . 26Tretinoin Microspheres . . . . . . . . . . . . 26Trexall . . . . . . . . . . . . . . . . . . . . . . . . . . 11Treximet . . . . . . . . . . . . . . . . . . . . . . . . . 14Trezix . . . . . . . . . . . . . . . . . . . . . . . . . . . 13Tri-Estarylla . . . . . . . . . . . . . . . . . . . . . . 38Tri-Legest FE . . . . . . . . . . . . . . . . . . . . 39Tri-Levlen . . . . . . . . . . . . . . . . . . . . . . . 38Tri-Linyah . . . . . . . . . . . . . . . . . . . . . . . 38Tri-Lo Sprintec . . . . . . . . . . . . . . . . . . . 39Tri-Lo-Estarylla . . . . . . . . . . . . . . . . . . . 39Tri-Lo-Marzia . . . . . . . . . . . . . . . . . . . . 39Tri-Norinyl . . . . . . . . . . . . . . . . . . . . . . . 38Tri-Previfem . . . . . . . . . . . . . . . . . . . . . 38Tri-Sprintec . . . . . . . . . . . . . . . . . . . . . . 38Tri-Vi-Flor . . . . . . . . . . . . . . . . . . . . . . . 48Tri-Vi-Flor w/Iron . . . . . . . . . . . . . . . . . 48Tri-Vylibra . . . . . . . . . . . . . . . . . . . . . . . 38Triamcinolone . . . . . . . . . . . . . .25, 27, 45Triamcinolone Acetonide Cream . . . . 25Triamcinolone Acetonide Cream,
Ointment, Lotion . . . . . . . . . . . . . . . . 25Triamcinolone Acetonide Ointment . . 25Triamterene/Hydrochlorothiazide . . . . 21Triazolam . . . . . . . . . . . . . . . . . . . . . . . . 17Tricor . . . . . . . . . . . . . . . . . . . . . . . . . . . 24Tridesilon . . . . . . . . . . . . . . . . . . . . . . . 26Trientine HCl . . . . . . . . . . . . . . . . . . . . 30Trifluridine . . . . . . . . . . . . . . . . . . . . . . . 43Trihexyphenidyl . . . . . . . . . . . . . . . . . . . 15Trilafon . . . . . . . . . . . . . . . . . . . . . . . . . 18Trileptal . . . . . . . . . . . . . . . . . . . . . . 15, 16Trilipix . . . . . . . . . . . . . . . . . . . . . . . . . . 24Trimethoprim . . . . . . . . . . . . . . . . . . . 8, 43Trinessa . . . . . . . . . . . . . . . . . . . . . 38, 39Trinessa Lo . . . . . . . . . . . . . . . . . . . . . . 39Trintellix . . . . . . . . . . . . . . . . . . . . . . . . . 17Triphasil . . . . . . . . . . . . . . . . . . . . . . . . . 38Triphsil . . . . . . . . . . . . . . . . . . . . . . . . . . 38Triumeq . . . . . . . . . . . . . . . . . . . . . . . . . . 9Trivora-28 . . . . . . . . . . . . . . . . . . . . . . . 38Trizivir . . . . . . . . . . . . . . . . . . . . . . . . . . . 9Trokendi XR . . . . . . . . . . . . . . . . . . . . . 16Trospium Chloride Sustained-Release
24 Hour Capsule . . . . . . . . . . . . . . . 47Trulicity . . . . . . . . . . . . . . . . . . . . . . . . . 31Trusopt . . . . . . . . . . . . . . . . . . . . . . . . . 42

65
2018 Prescription Drug List Medication Index
Truvada . . . . . . . . . . . . . . . . . . . . . . . . . . 9Tudorza Pressair . . . . . . . . . . . . . . . . . 45Tussionex . . . . . . . . . . . . . . . . . . . . . . . 44Tuzistra XR . . . . . . . . . . . . . . . . . . . . . . 44Tybost . . . . . . . . . . . . . . . . . . . . . . . . . . . 9Tykerb . . . . . . . . . . . . . . . . . . . . . . . . . . 12Tylenol w/Codeine . . . . . . . . . . . . . . . . 13Tymlos . . . . . . . . . . . . . . . . . . . . . . . . . . 37Tyvaso . . . . . . . . . . . . . . . . . . . . . . . . . . 45UUceris Foam . . . . . . . . . . . . . . . . . . . . . 34Uceris Tablet . . . . . . . . . . . . . . . . . . . . 34Uloric . . . . . . . . . . . . . . . . . . . . . . . . . . . 36Ultracet . . . . . . . . . . . . . . . . . . . . . . . . . 14Ultram . . . . . . . . . . . . . . . . . . . . . . . . . . 14Ultram ER . . . . . . . . . . . . . . . . . . . . . . . 14Ultravate . . . . . . . . . . . . . . . . . . . . . . . . 25Ultravate Lotion . . . . . . . . . . . . . . . . . . 25Ultresa . . . . . . . . . . . . . . . . . . . . . . . . . 34Umecta . . . . . . . . . . . . . . . . . . . . . . . . . 28UniStrip Test Strips . . . . . . . . . . . . . . . 32Uptravi . . . . . . . . . . . . . . . . . . . . . . . . . . 46Urea 40% Emulsion . . . . . . . . . . . . . . 28Urecholine . . . . . . . . . . . . . . . . . . . . . . 47Uroxatral . . . . . . . . . . . . . . . . . . . . . . . . 47Ursodiol . . . . . . . . . . . . . . . . . . . . . . . . 34Utibron Neohaler . . . . . . . . . . . . . . . . . 46VVagifem . . . . . . . . . . . . . . . . . . . . . . . . . 40Valacyclovir Tablet . . . . . . . . . . . . . . . . . 8Valchlor . . . . . . . . . . . . . . . . . . . . . . . . . 12Valcyte . . . . . . . . . . . . . . . . . . . . . . . . . . 8Valganciclovir Tablet . . . . . . . . . . . . . . . 8Valisone . . . . . . . . . . . . . . . . . . . . . . . . 25Valium . . . . . . . . . . . . . . . . . . . . . . . . . . 19Valproic Acid Capsule . . . . . . . . . . . . . 15Valsartan . . . . . . . . . . . . . . . . . . . . . . . . 23Valsartan/Hydrochlorothiazide . . . . . . 23Valtrex . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Vancocin HCl . . . . . . . . . . . . . . . . . . . . . 9Vancomycin Capsule . . . . . . . . . . . . . . . 9Vanos . . . . . . . . . . . . . . . . . . . . . . . . . . 25Vantin . . . . . . . . . . . . . . . . . . . . . . . . . . . 7Varubi . . . . . . . . . . . . . . . . . . . . . . . . . . 34Vascepa . . . . . . . . . . . . . . . . . . . . . . . . 24Vaseretic . . . . . . . . . . . . . . . . . . . . . . . . 23Vasocidin . . . . . . . . . . . . . . . . . . . . . . . 43Vasotec . . . . . . . . . . . . . . . . . . . . . . . . . 22Vectical . . . . . . . . . . . . . . . . . . . . . . . . . 27Velivet . . . . . . . . . . . . . . . . . . . . . . . . . . 38Velphoro . . . . . . . . . . . . . . . . . . . . . . . . 49Veltassa . . . . . . . . . . . . . . . . . . . . . . . . 49
Veltin . . . . . . . . . . . . . . . . . . . . . . . . . . . 26Vemlidy . . . . . . . . . . . . . . . . . . . . . . . . . . 8Venclexta . . . . . . . . . . . . . . . . . . . . . . . 12Venlafaxine Sustained-Release
24 Hour Capsule . . . . . . . . . . . . . . . 17Ventavis . . . . . . . . . . . . . . . . . . . . . . . . 45Ventolin . . . . . . . . . . . . . . . . . . . . . . . . . 45Ventolin HFA . . . . . . . . . . . . . . . . . . . . 45VePesid . . . . . . . . . . . . . . . . . . . . . . . . . 12Verapamil . . . . . . . . . . . . . . . . . . . . 22, 23Verapamil Sustained-Action Tablet . . 22Verapamil Sustained-Release
24 Hour Capsule, Pellets . . . . . . . . 22Verelan . . . . . . . . . . . . . . . . . . . . . . . . . 22Verelan PM . . . . . . . . . . . . . . . . . . . . . . 22Verzenio . . . . . . . . . . . . . . . . . . . . . . . . 12Vesanoid . . . . . . . . . . . . . . . . . . . . . . . . 12Vesicare . . . . . . . . . . . . . . . . . . . . . . . . 47Vestura . . . . . . . . . . . . . . . . . . . . . . . . . 39Vfend . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9Viagra . . . . . . . . . . . . . . . . . . . . . . . . . . 47Viberzi . . . . . . . . . . . . . . . . . . . . . . . . . . 34Vibramycin . . . . . . . . . . . . . . . . . . . . . . . 7Vibratab . . . . . . . . . . . . . . . . . . . . . . . . . 7Vicodin, Vicodin ES, Vicodin HP . . . . 13Victoza 2-Pak . . . . . . . . . . . . . . . . . . . . 31Victoza 3-Pak . . . . . . . . . . . . . . . . . . . . 31Videx EC . . . . . . . . . . . . . . . . . . . . . . . . . 9Viekira Pak . . . . . . . . . . . . . . . . . . . . . . . 8Viekira XR . . . . . . . . . . . . . . . . . . . . . . . . 8Vienva . . . . . . . . . . . . . . . . . . . . . . . . . . 38Vigabatrin . . . . . . . . . . . . . . . . . . . . . . . 15Vigamox . . . . . . . . . . . . . . . . . . . . . . . . 43Viibryd . . . . . . . . . . . . . . . . . . . . . . . . . . 17Vimpat . . . . . . . . . . . . . . . . . . . . . . . . . . 16Viokace . . . . . . . . . . . . . . . . . . . . . . . . . 34Viorele . . . . . . . . . . . . . . . . . . . . . . . . . . 39Viracept . . . . . . . . . . . . . . . . . . . . . . . . . . 9Viramune . . . . . . . . . . . . . . . . . . . . . . . . . 9Viramune XR . . . . . . . . . . . . . . . . . . . . . 9Viread . . . . . . . . . . . . . . . . . . . . . . . . . . . 9Viroptic . . . . . . . . . . . . . . . . . . . . . . . . . 43Vistaril . . . . . . . . . . . . . . . . . . . . . . . . . . 44Vivelle-Dot . . . . . . . . . . . . . . . . . . . . . . 40Voltaren . . . . . . . . . . . . . . . . . . . . . . 36, 42Voltaren Gel . . . . . . . . . . . . . . . . . . . . . 36Voltaren-XR . . . . . . . . . . . . . . . . . . . . . 36Vonvendi . . . . . . . . . . . . . . . . . . . . . . . . 21Voriconazole Tablet . . . . . . . . . . . . . . . . 9Vosevi . . . . . . . . . . . . . . . . . . . . . . . . . . . 8VoSol HC . . . . . . . . . . . . . . . . . . . . . . . 29Votrient . . . . . . . . . . . . . . . . . . . . . . . . . 12
Vraylar . . . . . . . . . . . . . . . . . . . . . . . . . . 18Vyfemla . . . . . . . . . . . . . . . . . . . . . . . . . 39Vylibra . . . . . . . . . . . . . . . . . . . . . . . . . . 38Vytorin . . . . . . . . . . . . . . . . . . . . . . . . . . 24Vyvanse . . . . . . . . . . . . . . . . . . . . . . . . . 19WWarfarin . . . . . . . . . . . . . . . . . . . . . . . . 20Welchol . . . . . . . . . . . . . . . . . . . . . . . . . 24Wellbutrin . . . . . . . . . . . . . . . . . . . . . . . 17Wellbutrin SR . . . . . . . . . . . . . . . . . . . . 17Wellbutrin XL . . . . . . . . . . . . . . . . . . . . 17Wera . . . . . . . . . . . . . . . . . . . . . . . . . . . 38Westcort . . . . . . . . . . . . . . . . . . . . . . . . 25Wymzya FE . . . . . . . . . . . . . . . . . . . . . . 39XXadago . . . . . . . . . . . . . . . . . . . . . . . . . 15Xalatan . . . . . . . . . . . . . . . . . . . . . . . . . 42Xalkori . . . . . . . . . . . . . . . . . . . . . . . . . . 12Xanax . . . . . . . . . . . . . . . . . . . . . . . . . . 19Xanax XR . . . . . . . . . . . . . . . . . . . . . . . 19Xarelto . . . . . . . . . . . . . . . . . . . . . . . . . 20Xatmep . . . . . . . . . . . . . . . . . . . . . . . . . 36Xeljanz/Xeljanz XR . . . . . . . . . . . . . . . . 36Xeloda . . . . . . . . . . . . . . . . . . . . . . . . . . 11Xenazine . . . . . . . . . . . . . . . . . . . . . . . . 16Xerese . . . . . . . . . . . . . . . . . . . . . . . . . . 27Xermelo . . . . . . . . . . . . . . . . . . . . . . . . . 34Xibrom . . . . . . . . . . . . . . . . . . . . . . . . . 42Xifaxan . . . . . . . . . . . . . . . . . . . . . . . . . 34Xigduo XR . . . . . . . . . . . . . . . . . . . . . . 31Xiidra . . . . . . . . . . . . . . . . . . . . . . . . . . . 43Xodol . . . . . . . . . . . . . . . . . . . . . . . . . . . 13Xolegel . . . . . . . . . . . . . . . . . . . . . . . . . 27Xopenex HFA . . . . . . . . . . . . . . . . . . . . 45Xopenex Vial, Nebulizer . . . . . . . . . . . . 45Xtampza ER . . . . . . . . . . . . . . . . . . . . . 13Xtandi . . . . . . . . . . . . . . . . . . . . . . . . . . 12Xulane . . . . . . . . . . . . . . . . . . . . . . . . . . 39Xultophy . . . . . . . . . . . . . . . . . . . . . . . . 31Xylocaine . . . . . . . . . . . . . . . . . . . . . . . 26Xyntha . . . . . . . . . . . . . . . . . . . . . . . . . . 21Xyrem . . . . . . . . . . . . . . . . . . . . . . . . . . 19Xyzal . . . . . . . . . . . . . . . . . . . . . . . . . . . 44YYasmin . . . . . . . . . . . . . . . . . . . . . . . . . 39Yaz . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39Yuvafem . . . . . . . . . . . . . . . . . . . . . . . . 40ZZafirlukast . . . . . . . . . . . . . . . . . . . . . . . 45Zaleplon . . . . . . . . . . . . . . . . . . . . . . . . 17Zanaflex . . . . . . . . . . . . . . . . . . . . . . . . 36Zarah . . . . . . . . . . . . . . . . . . . . . . . . . . . 39
66
2018 Prescription Drug List Medication Index
Zarontin . . . . . . . . . . . . . . . . . . . . . . . . 15Zaroxolyn . . . . . . . . . . . . . . . . . . . . . . . 21Zarxio . . . . . . . . . . . . . . . . . . . . . . . . . . 35Zegerid . . . . . . . . . . . . . . . . . . . . . . . . . 33Zejula . . . . . . . . . . . . . . . . . . . . . . . . . . 12Zelboraf . . . . . . . . . . . . . . . . . . . . . . . . 12Zembrace SymTouch . . . . . . . . . . . . . 14Zemplar . . . . . . . . . . . . . . . . . . . . . . . . . 30Zenatane . . . . . . . . . . . . . . . . . . . . . . . 26Zenchent . . . . . . . . . . . . . . . . . . . . . . . 39Zenchent FE . . . . . . . . . . . . . . . . . . . . . 39Zenpep . . . . . . . . . . . . . . . . . . . . . . . . . 34Zepatier . . . . . . . . . . . . . . . . . . . . . . . . . 8Zerit . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9Zestoretic . . . . . . . . . . . . . . . . . . . . . . . 23Zestril . . . . . . . . . . . . . . . . . . . . . . . . . . 22Zetia . . . . . . . . . . . . . . . . . . . . . . . . . . . 24Zetonna . . . . . . . . . . . . . . . . . . . . . . . . 45Ziac . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23Ziagen . . . . . . . . . . . . . . . . . . . . . . . . . . . 9Zidovudine . . . . . . . . . . . . . . . . . . . . . . . 9Zidovudine/Lamivudine . . . . . . . . . . . . . 9Zioptan . . . . . . . . . . . . . . . . . . . . . . . . . 42Ziprasidone . . . . . . . . . . . . . . . . . . . . . 18Zirgan . . . . . . . . . . . . . . . . . . . . . . . . . . 43Zithromax . . . . . . . . . . . . . . . . . . . . . . . . 7Zocor . . . . . . . . . . . . . . . . . . . . . . . . . . 24Zofran . . . . . . . . . . . . . . . . . . . . . . . . . . 34Zofran ODT . . . . . . . . . . . . . . . . . . . . . 34Zohydro ER . . . . . . . . . . . . . . . . . . . . . 13Zolinza . . . . . . . . . . . . . . . . . . . . . . . . . . 12Zolmitriptan Orally Disintegrating
Tablet . . . . . . . . . . . . . . . . . . . . . . . . . 14Zolmitriptan Tablet . . . . . . . . . . . . . . . . 14Zoloft . . . . . . . . . . . . . . . . . . . . . . . . . . . 18Zolpidem . . . . . . . . . . . . . . . . . . . . . . . . 17Zolpidem Sublingual Tablet . . . . . . . . 17Zolpidem Tartrate
Multiphasic-Release Tablet . . . . . . . 17Zomacton . . . . . . . . . . . . . . . . . . . . . . . 35Zomig . . . . . . . . . . . . . . . . . . . . . . . . . . 14Zomig Nasal Spray . . . . . . . . . . . . . . . 14Zomig-ZMT . . . . . . . . . . . . . . . . . . . . . 14Zonegran . . . . . . . . . . . . . . . . . . . . 15, 16Zonisamide Capsule . . . . . . . . . . . . . . 15Zorbtive . . . . . . . . . . . . . . . . . . . . . . . . . 35Zovia 1/35E . . . . . . . . . . . . . . . . . . . . . 38Zovia 1/50E . . . . . . . . . . . . . . . . . . . . . 38Zovirax . . . . . . . . . . . . . . . . . . . . . . . . 8, 27Zovirax Cream . . . . . . . . . . . . . . . . . . . 27Zubsolv . . . . . . . . . . . . . . . . . . . . . . . . . 14Zurampic . . . . . . . . . . . . . . . . . . . . . . . 36
Zutripro . . . . . . . . . . . . . . . . . . . . . . . . . 44Zyban . . . . . . . . . . . . . . . . . . . . . . . . . . 49Zydelig . . . . . . . . . . . . . . . . . . . . . . . . . 12Zykadia . . . . . . . . . . . . . . . . . . . . . . . . . 12Zylet . . . . . . . . . . . . . . . . . . . . . . . . . . . 43Zyloprim . . . . . . . . . . . . . . . . . . . . . . . . 36Zymaxid . . . . . . . . . . . . . . . . . . . . . . . . . 43Zyprexa . . . . . . . . . . . . . . . . . . . . . . . . . 18Zyprexa Zydis . . . . . . . . . . . . . . . . . . . . 18Zytiga . . . . . . . . . . . . . . . . . . . . . . . . . . 12Zyvox . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
67
Nondiscrimination notice and access to communication servicesUnitedHealthcare® does not discriminate on the basis of race, color, national origin, age, disability, or sex in its health programs or activities .
If you think you were treated unfairly because of your sex, age, race, color, disability or national origin, you can send a complaint to the Civil Rights Coordinator .
Online: UHC_Civil_Rights@uhc .com
Mail: Civil Rights Coordinator UnitedHealthcare Civil Rights Grievance P .O . Box 30608 Salt Lake City, Utah 84130
You must send the complaint within 60 days of your experience . A decision will be sent to you within 30 days . If you disagree with the decision, you have 15 days to ask us to look at it again . If you need help with your complaint, please call the toll-free phone number listed on your ID card, TTY 711, Monday through Friday, 8 a .m . to 8 p .m .
You can also file a complaint with the U .S . Dept . of Health and Human Services .
Online: https://ocrportal .hhs .gov/ocr/portal/lobby .jsf Complaint forms are available at http://www .hhs .gov/ocr/office/file/index .html
Phone: Toll free 1-800-368-1019, 1-800-537-7697 (TDD)
Mail: U .S . Dept . of Health and Human Services 200 Independence Avenue SW Room 509F, HHH Building Washington, D .C . 20201
We provide free services to help you communicate with us, including letters in other languages or large print . Or, you can ask for an interpreter . To ask for help, please call the toll-free phone number listed on your ID card TTY 711, Monday through Friday, 8 a .m . to 8 p .m .
68

UnitedHealthcare Physician PDL Booklet 7/18 Created April, 201872332-022018 © 2018 UnitedHealthCare Services, Inc . All rights reserved .





























