Embed Size (px)
Citation preview
Unequal extended families:
Internalizing behavioral problems of children in complex extended households
Jeehye Kang, University of Maryland at College Park
Philip N. Cohen, University of Maryland at College Park
Abstract
Using the Los Angeles Family and Neighborhood Survey (L.A. FANS), this paper examines the
impact of extended family living arrangements on children’s mental health. The study specifies
the types of household extension by their relation to the householder—vertical, horizontal, non-
kin, and mixed—and examines: what kinds of household extension are associated with mental
health problems; how stable are the different living arrangements, and; whether extended
families close the divide between immigrant and native families. The results indicate that
household extension, particularly involving two or more types of extended members, is more
likely to jeopardize child mental health. Non kin appears to increase internalizing behavior
problems only for children of undocumented immigrants, which might reflect parents’ low social
resources. We conclude household extension may reduce the disparity in youth emotional
development between natives and immigrants, but not effectively complementing disadvantages
facing children of immigrants.
Background
Research on the second generation children’s mental health has been challenging the
immigrant health paradox. While immigrant adults show paradoxically better physical and
mental health compared to US-born individuals, some findings suggest that children of
immigrants face greater risk of mental health problems (Gross et al. 2006; Sam et al. 2008).
Although there is contradicting evidence (Flores 2013; Gonzales et al. 2008), the studies using
samples from more disadvantaged populations consistently suggest the disadvantage of growing
up in immigrant families in the U.S (Jackson, Kiernan, and McLanahan 2012). The divergent
pattern supports the idea that risk and protective factors may operate differently by immigrant
generations (Landale et al. 2015).
In light of these generational discrepancies, extended families may be an important risk
or protective factor. Extended families provide important social ties especially for disadvantaged
population, but these social ties may both improve and harm health (Umberson, Crosnoe, and
Reczek 2010). The social support from extended families has been documented to explain
immigrants’ better than expected health status (Acevedo-Garcia et al. 2005; Harker 2001;
Mendoza 2009; Padilla, Hamilton, and Hummer 2009). However, the offspring of immigrants
may not benefit from the same protective factor that insulates adult immigrants from various
socioeconomic disadvantages (Landale et al. 2015; Landale, Thomas, and Van Hook 2011;
Turney and Kao 2009). In this context, we ask how extended families may contribute to the
disadvantages in children of immigrants.
Surprisingly little is known about extended family living arrangements for immigrant
families. First, the diversity of extended family living arrangements is largely neglected. Prior
research has been focused on vertical kin (grandparents) in single mother families, emphasizing
their child care assistance. Because of the heightened economic difficulties and the inability to
bring older parents during migration, immigrants’ extended family compositions are mainly
horizontal kin, other distant kin, non-kin, and mixtures of relatives and non-kin, whereas their
native counterparts consist of vertical kin (Glick, Bean, and Hook 1997; Landale et al. 2011;
Leach 2012). Horizontal-kin (siblings, cousins, nephews, nieces of the householder) or non-kin
have been excluded, despite their demographic prevalence among racial minority immigrants
(Blank and Torrecilha 1998; Glick et al. 1997; Hondagneu-Sotelo 1994; Leach 2012; Van Hook
and Glick 2007). How these different types of extended members play a different role in
children’s emotional health remains unknown (Harrison et al. 1990). Except for a handful of
studies examining differential impacts of extended members (Almeida et al. 2011; Kana’iaupuni
et al. 2005), the question of which kinds of extended members are associated with mental health
in children, has not been fully answered. Lastly, while it is known that extended households are
temporary arrangements (Glick and Van Hook 2007), we know little about how different kinds
of extended households have different transition pattern. If extended members have different
levels of stability, would they translate into different association with children’s mental health?
Some suggest that horizontal and complex extended family households are more likely to be
unstable and the instability of such arrangements among immigrants may not offer much
resource to children (Landale et al. 2011). However, this idea has not been tested. This lack of
knowledge is due to the prevalent definition of family as nuclear family (Gerstel 2011; Hunter
and Ensminger 1992; Richards, White, and Tsui 1987) and analytical complexity of identifying
different types of extended family (Landale et al. 2011).
Using L.A. FANS, we can study a substantial number of immigrant and native families
with children, their family household compositions, and we can trace changes in their household
compositions, for two time points over five to six years. This paper is exploratory, but we believe
its contribution will be significant.
Parental Nativity and Internalizing Behavioral Problems
Parental immigration status can influence the development of children (Glick and White
2004). Numerous studies on immigrant health indicate that foreign-born people have better
health than US-born Americans. Despite some variations across national origin, immigrant adults
tend to have lower mortality rates and lower levels of mental health problems (Cunningham,
Ruben, and Venkat Narayan 2008). In particular, Mexican immigrants report a significantly
lower level of anxiety disorders than US-born Mexicans, despite of their disadvantageous socio-
economic status (Grant et al. 2004). Many immigration scholars believe this health advantage is
due to positive selection by which healthier individuals migrate to the U.S, and due to the
support from extended families. Their offspring might also have better or equivalent mental
health, “if positive selection is present” (Landale et al. 2015: 4) and/or the provision of support
from extended families is stronger enough (Mendoza 2009) to outweigh their unfavorable social
environment.
However, researchers point to structural constraints facing many immigrants and the
children’s limited access to family and societal resources (Glick and White 2004; Menjívar 2000;
Perreira, Harris, and Lee 2006; Van Hook and Glick 2007). In particular, those children whose
parents have dark skin, originate from countries with low educational resources, and start with
low socioeconomic positions are more likely to confront stress from poverty, legal status
barriers, adverse residential conditions, and other adjustment problems (Portes and Rumbaut
2001; Rogler 1994; Stevens and Vollebergh 2008). Indeed, some findings suggest that children
of immigrants face greater risk of mental health problems (Gross et al. 2006; Jackson, Kiernan,
and McLanahan 2012; Sam, et al 2008). The results from the Fragile Families and Child Well-
Being Study reveal that the children of low-educated immigrant mothers have higher levels of
internalizing behavioral problems, compared to children of natives (Jackson, Kiernan, and
McLanahan 2012). Also, Latino (both Mexican and other Latino) children of undocumented
immigrants are at higher risk for internalizing behavioral problems, compared to other racial and
nativity groups (Landale et al. 2015: 10).
Household Extension and Differential Impacts of Extended Members by Their Relation
Given their disadvantageous profile, how do extended families play a role in the
psychological adjustment of children of immigrants? A recent study proposes that household
extension disadvantage children, especially those of poor immigrants (Kang and Philip,
dissertation). The finding suggests that extended families disadvantage children, in contrast to
prior research that supports the provision of additional social and economic resources by
extended family members to multigenerational single parent families (DeLeire and Kalil 2002;
Dressler 1985; Edin and Lein 1997; Sarkisian 2006). Possibly, the divergent pattern is due to the
inclusion of non-kin extended members in the definition of extended family households, unlike
previous studies. However, the researchers have not fully explained how the different types of
extended members play any differential role in children’s psychological development. In this
paper, we explore how vertical, horizontal, non-kin, and complex extended family members
impact on children’s internalizing behavioral problems.
a) Vertical kin
Grandparents (vertically extended kin members) may benefit children. Grandparents are
often invited to help their adult children to raise their kids and participate actively in the labor
force (Menjívar 2000; Treas 2008; Treas and Mazumdar 2004). Although there could be
disagreements between parents and grandparents about parenting values and associated practices
(Chase-Lansdale, Brooks-Gunn, and Zamsky 1994), which may interfere children’s mental well-
being, researchers generally found that grandparents provide economic and social support for the
mother (Angel and Tienda 1982; Cohen 2002; DeLeire and Kalil 2002; Edin and Lein 1997;
Glick et al. 1997; Hofferth, Boisjoly, and Duncan 1998), as well as additional sources of
affection, and a sense of security for the children (Castiglia 1999; Kellam et al. 1982; Kellam,
Ensminger, and Turner 1977). Indeed, grandparents are more common where younger children
are present (12 percent) than where children are older (8-9 percent; Hernandez 2004).
Children of immigrants who co-reside with grandparents are also likely to benefit from
grandparents, despite the smaller chance of living with grandparents. Although older immigrants
are limited in their capacity to participate in the labor force and provide financial assistance, they
help their children and grandchildren in other ways. Grandmothers and often grandfathers take
care of the children and do other household chores (Menjivar 2000: 199). Among Muslim and
Hindu families in U.K, children (age 5-11) were better adjusted in extended families, especially
with grandmother, than nuclear families (Sonuga-Barke and Mistry 2000). While the specific
generalizability to families in U.S is limited, this finding provides evidence for a positive link
between grandparents and child psychological adjustment. Thus, vertically extended kin
members are expected to provide assistance to children and families.
b) Horizontal kin
The literature on horizontally extended members, who are generally siblings of the
parents, or aunts and uncles to the child, is limited. Aunts and uncles can bring benefits to
children by offering care, supervision, and other various supports (Stanton-Salazar 2001). One
study focusing on family members' assistance to mothers documented parental siblings providing
emotional support to mothers whose children have special needs (Slaughter and Dilworth-
Anderson 1985; Wilson 1986, 1989). The ease of financial and emotional constraint for mothers
can be beneficial to children.
However, the finding of Slaughter and Dilworth-Anderson’s study (1985) came from
cases in which children were experiencing chronic pain from sickle cell anemia when the father
was absent in the home. Thus, it may not apply to families in general. In addition, Stanton-
Salazar (2001) also emphasized that the availability of kin did not always translate into social
support. “Intimate relations of trust and disclosure required …compact of trust, nonjudgmental
rapport, and confidentiality (p.75).”
To children of immigrants, aunts and uncles may be inaccessible due to his/her
circumstances. Findings on Mexican family networks indicate kin networks appear to drain
financial support resources, although they are not necessarily co-resident (Kana’iaupuni et al.
2005). The researchers suggest that the negative implications may be due to either the unmet

needs by relatives who are unable to offer support; or intensified stress between relatives and
host families. Considering the fact that co-resident aunts and uncles in immigrant families are
more likely to be recent arrivals, unable to afford independent housing, and likely to have their
own dependents, they might be incapable of child care, supervision, or provision of financial aid.
Therefore, horizontally extended kin members’ support for children should be limited.
c) Non-kin
There is no conclusive evidence that non-kin are either beneficial or harmful household
guests (Franzini and Fernandez-Esquer 2004; Pugliesi and Shook 1998; Schwartz 2007; Walen
and Lachman 2000). Some studies suggested non-kin (e.g. friends) extended members are
beneficial (Dean, Kolody, and Wood 1990; Kana’iaupuni et al. 2005; Matt and Dean 1993).
Kana'iaupuni et al. (2005) argued non-kin ties such as friends, and neighbors seem to support
poor households both emotionally and financially. The support from non-kin can be substantial
as it is “voluntary rather than obligatory” in nature (Almeida et al. 2009; see Dean et al., 1990).
However, friendship support may not compensate for kinship support. Recent empirical
studies suggest that friendship support is less protective on risk of depression among adults
compared to kinship support (Almeida et al. 2011). Besides, the adjusted effects of friend
support become marginal after introducing family support (Ibid). Similarly, an anthropological
study suggests that relatives provide more robust, quality support than do friends because they
are less inclined to exchange assistance when interactions cost than benefit (Xue 2015).
Although these two different studies do not address co-resident non-kin, the findings
provide some insights into non-kin extended households. Non-kin support would be subject to
various circumstances for the family. Non-kin can be more important for immigrants because
they tend to rely on friendships to compensate for the loss of kin support after migration
(Hammel 1968). However, to the extent that non-kin members tend to be temporary guests,
possessing low levels of human and economic capital, and more likely to be recent migrants
when it comes to immigrant families (Hernandez 2004:23), reciprocal interactions will be few
and far. Therefore, children, especially those in immigrant families may not benefit from non-kin
members.
e) Mixed
The association of living with two or more types of extended members with child health
is little known. Research on the health of children in such living arrangements is scarce because
researchers rarely recognize the households with mixed types of extended members. In addition,
household complexity has been differently measured by researchers. Some measures with the
presence of stepparents, custodial grandparents, and non kin foster parents (Ziol-Guest and
Dunifon 2014), the presence of adopted-, half-, or step-siblings (Brown, Manning, and Stykes
2015), or non-nuclear members in general (Van Hook and Glick 2007). Although some
researchers (Leach 2012; Van Hook and Glick 2007) recognized the households with two or
more types of extended members, how such arrangements are associated with children’s mental
health remains unknown.
While the measures of household complexity vary by researchers, complex living
arrangements have been associated with worse child well-being, independent of economic
insecurity (Brown et al. 2015; Ziol-Guest and Dunifon 2014). Family complexity may lead to
crowding housing, which is suggested to harm child psychological development of children
through increased family stress levels (Evans 2006; Krieger and Higgins 2002; Solari and Mare
2012). Thus, in this paper, we expect that co-residing with two or more types of extended
members would have a direct and unfavorable association with child mental health.

Children of immigrant families are expected to be more affected by mixed extended
family households. Although living with a variety of kin and non-kin indicates a hardship for
both natives and immigrants, immigrants are more likely to live in such living arrangements
(Glick and Van Hook 2007; Landale et al. 2011; Leach 2012). Even though the complex
household extension become less common as immigrants stay more time in the United States,
children of immigrants are still more likely to experience such living arrangement because of
their limited kin availability, compared to children of natives (Leach 2012). Considering that
friendship support is less robust, quality support compared to kinship support (Almeida et al.
2011; Xue 2015), children of immigrants may not receive benefit from their mixed extended
households.
In sum, the level of resources extended members possess differs, depending on their
relation to the family and children. Therefore, different types of extended family members
should have different meanings to the child.
Transitions among Extended Family Households
Not only the variation, but also fluidity characterizes extended family households.
Compared to nuclear family households, extended families are the least likely to stay intact,
mainly due to the frequent entrance or exit of extended members (Hunter and Ensminger 1992;
Richards et al. 1987). However, a great body of research focuses on changes in living
arrangements due to a vital event such as birth, marriage and divorce, and only a handful of
researchers examine the transitions by non-nuclear family members. Also, except for Glick and
Van Hook’s research (2011), previous researchers tend not to specify the transition patterns by
different types of extended members due to analytical complexities (Landale et al. 2011). This
neglect of extended families in the literature may attribute to the normative nuclear family notion
prevalent in family research (Hunter and Ensminger 1992; Richards et al. 1987).
Different types of extended family households have different transition patterns (Hunter
and Ensminger 1992). For example, extended family households with co-resident vertical kin are
more likely to stay intact, while those with other relatives and non-kin are more likely to dissolve
when extended members in need became more capable to live independently (Bethencourt and
Ríos-Rull 2009; Glick and Van Hook 2011). Because non-kin is more subject to various
circumstances of the family (Almeida et al. 2011; Xue 2015), their transition patterns may be
even more fluid. The patterns of transitions for households with a mixture of various extended
family members are less known (for exception, see Van Hook and Glick 2007), but they will be
also unstable, as such complex living arrangements indicate a hardship.
In addition, immigrant families would be more prone to transitions in the process of
migration adaptation (Landale et al. 2011; Van Hook and Glick 2007). Because recent arrivals
tend to rely on the previously arriving families to offer housing and assistance (Leach 2012;
Portes 1995), such extended family living arrangements are temporary. Thus, I expect that
immigrant families will experience more changes in their extended household compositions,
compared to native families.
Identifying how differential extended family transitions are associated with children’s
mental health development might help explain the mechanism of extended family effects. A
recent finding suggests that the negative child outcomes in non-traditional families are mostly
explained by family instability (Rosenfeld 2015). Family transitions including movement of non-
nuclear members in and out of households as well as parental breakup are found to be negatively
associated with child development. If different extended members do play different roles, as
hypothesized, it is crucial to understand how the different patterns of co-residential continuity are
related to the associations between child mental health and different types of household
extension. If the pattern differs by parental immigrant status, that might help explain the
immigrant (dis)advantage for child mental health.
Method
Data and Sample
The data come from the Los Angeles Family and Neighborhood Survey (L.A. FANS).
We chose the data because they contain detailed information on both immigrant parents and their
children. The information includes parents’ and children’s immigrant status, psychological health
status as well as the family’s composition and socioeconomic status. We both use the first wave
and the panel data in order to answer different questions. By using the two data, we answer what
kinds of household extension are associated with child mental health problems. If the patterns
differ by data, we discuss whether it derives from time or changes in variables. The panel data
show how stable the different living arrangements are and whether the instability of living
arrangements explains different household extension effects. Comparing the results between
immigrant and native families, we answer whether extended families close the divide between
them.
The first wave (L.A. FANS-1), which was fielded between April 2000 and January 2002,
interviewed adults and children living in 3,085 households in a diverse, stratified probability
sample of 65 neighborhoods throughout Los Angeles County. Fieldwork for the second wave
(L.A. FANS-2) took place between August 2006 and December 2008. In Wave 2 primary
respondents from Wave 1 who were still residing in Los Angeles County were interviewed,
regardless of their continuing to live in their Wave 1 neighborhoods. (Note that we exclude
individuals who moved into the sampled neighborhoods between Waves 1 and 2 because we do
not have information about their previous household compositions.) There is 68% attrition
between the first and second wave, including 37% of children who aged out of the sample.
Families with children and families living in poor neighborhoods were oversampled, which we
account for by using survey weights.
The sampled children are aged 3-11 at Wave 1 and aged 8-18 at Wave 2. Our sample
from the first wave sample includes 1538 children in 1177 households. The analytical sample is
limited to one randomly selected child per household and siblings, whose primary caregiver
completed an adult questionnaire, a parent questionnaire, and a primary caregiver questionnaire.
The parent of the randomly selected child was selected as a respondent and designated the
primary caregiver, most of whom are mothers of the children. Those missing on the measured
variables were excluded (n =135, 8.9%). The panel sample includes 1645 child-years; 653
children were captured in both waves.
Measures
Dependent Variable The Behavior Problems Index was designed to assess children’s
behavior problems including anxiety, depression, and aggression. This instrument was developed
by Peterson and Zill (1986) and consists of 28 questions derived from commonly used
questionnaires such as the Achenbach Child Behavior Checklist and others. The instrument
consists of three subscales: internalizing, externalizing, and total. It has been used extensively in
studies of behavior problems in children.
Children’s internalizing behavioral functioning represents a key developmental outcome
(King, Iacono, and McGue 2004). The Internalizing scale, a subset of the behavioral problems
index, assesses the presence of withdrawn and sad behaviors. The measure consists of eleven
items: felt or complained that no one loved him/her, too fearful or anxious, easily confused
and/or has seemed to be in a fog, felt worthless or inferior, not liked by other children, had a lot
of difficulty getting his/her mind off certain thoughts, unhappy, sad or depressed, withdrawn,
and/or has not gotten involved with others, clinging to adults, cried too much, too dependent on
others. Parents responded to the BPI questions using a three-point Likert scale, “1” if the
statement is often true, “2” if the statement is sometimes true, and “3” if the statement is not true.
A reliability test indicates a Cronbach’s alpha of .73.
The measures of internalizing behavior problem index scores are skewed, with most
children having low scores. Heteroscedasticity and inflated standard errors of the estimates in
regression analysis resulting from skewed variables can lead to reduced statistical power of
significance tests and larger confidence intervals (Berk 1983). To reduce these problems, the
behavior problem scores are logged (Hamilton 2005).
Independent Variables Extended family households are defined as households that
include non-nuclear family member(s) including grandparents, parents (in-law), siblings (in-
law), cousins, nephews, nieces, and friends of the householder or spouse of the householder.
a) Vertically extended households: refer to family households co-residing parents (in-law)
or grandparents of the householder. Also, aunts and uncles whose age is more than 19years older
than the householder are counted as vertical kin. In other words, they are grandparents or great
grandparents of the children.
b) Horizontally extended households: refer to family households co-residing siblings (in-
law), cousins, nieces and nephews of the householder. Aunts and uncles whose age is less than
19years the householder are counted as horizontal kin. In other words, they are uncles, aunts to
the child.
c) Non-kin extended households: refer to family households co-residing members who
are not related by blood or marriage, such as friends. They are friends of children’s parents.
Boarders or renters are excluded from non-kin extended members.
Importantly, because two or more types of extended members often coexist in extended
family households, I create another category that captures such cases.
d) Mixed extended households: refer to family households co-residing two or more types
of extended members. They include combinations such as vertical kin and horizontal kin together,
or horizontal kin and non-kin co-residing in one household, to name the two most popular types.
For descriptive purpose, we present two categories of mixed extended households: one
consisting only relatives, and the other consisting kin and non-kin.
These variables are dichotomous (0/1) and mutually exclusive.
Moderators: Primary Care Giver’s immigrant status. Using questions about primary care
giver’s place of birth, we identify their immigration status. The variable is dichotomous (0=US-
born/native, 1=foreign-born/immigrant). In addition, a dichotomous variable measures primary
care giver’s undocumented immigrant status (0=legal immigrant, 1=undocumented).
Covariates:
Primary Care Giver Single-parenthood. It is measured using marital status of the primary
care giver, (0= married or cohabiting, 1=never married).
Primary Care Giver Depressive symptom. A short form (CIDI-SF) questionnaire covers
major depressive episodes (MD) of the primary care givers. The CIDI-SF questions for MD
reports the respondents’ feeling sad, blue, or depressed for two weeks or more in the past 12
months (dysphoric); if they did, whether having lost interest in most things like hobbies, work, or
activities that usually give pleasure (anhedonic). The MD reports provide a probability between 0
and 1 that the person is suffering from major depression.
Primary Care Giver’s Educational attainment. The variable is used as a dichotomous
measure: 0=less than high school; 1=high school and greater. A majority primary care givers in
the L.A. FANS do not have a high school diploma, thus reflecting the distribution, high school
graduation is used as the cut-off.
Family income. The sum of income from head of household, spouse/partner of head,
children, and logged for the analysis.
Household Crowding. The number of total household members (all adults and children)
is divided by the number of bedrooms. More than two persons per bedroom is a standard
measure of overcrowding in housing.
Child sex, and age. Sex of child variable is dichotomous (0=female, 1=male), and age is
continuous.
Primary Care Giver Race/ethnicity. Race/ethnicity of the primary care giver was
determined by their report. The L.A. FANS did allow for disaggregating of “Latino” into
subgroups (Mexican American, Central American, Other Latino, etc.), as well as “Asians”
(Chinese, Korean, Pilipino, etc.), but total numbers for sub groups were too small for separate
analyses, except for Mexicans. Therefore, the 4 racial/ethnic groups that were used in these
analyses are white, black, Latino, and Asian.
Analytical plan
To explore how different types of household extension are associated with stability of the
living arrangements, we generate a 6 × 6 transition matrix, of which the 30 cells represent the
proportion of changes in household composition between Wave 1 and Wave 2; the six diagonal
cells denote the case for which the same household composition is observed during that period.
This method follows Richards and colleagues (1987: 81).
To measure the impact of living arrangements, we perform OLS linear regression
analyses using Wave1 data sample and fixed effect regression analyses using panel data sample.
A fixed effects model allows investigating the causal effect of family structural transitions on
individual child outcomes. Importantly, the fixed effect models “factor out” background
characteristics that may or may not be measured but affect the outcome variables (Allison 2005;
Conley, Pfeiffer, and Velez 2007; Teachman 2011). Variables that are the same for a child across
the two surveys such as race, sex, parental education, and other individual traits are controlled
for in the analysis, whether they are measured or not. Fixed effects estimations would determine
the more “pure” effects of independent variables on changes in the outcome across children
experiencing transitions in living arrangement.
Given the two-period panel data, the following the “first difference” equation represents
this model:
(yi2- yi1)= (μj2- μj1)+ β1(Fi2- Fi1 )+ (εi2-εi1), (2)
where yit equals the observed outcome variable for child i, in time t (1 or 2), β1 is the
coefficient for the family-varying covariate Fit, μj represents child and family characteristics (e.g.
race, sex of child) that are constant over time, and εit represents by time-varying unexplained
variation. This model makes no assumptions about the distribution of these child-specific terms.
They can be normally distributed (or not) and can be correlated with key explanatory variables,
such as living arrangements.
We compare the results between OLS and fixed effect estimations in order to more fully
understand the implications of extended living arrangements. OLS models measure the average
difference across groups, such as between children in vertically extended households and those
in horizontally extended households. Although the cross-sectional models of association may be
biased, we gain the efficiency with larger sample size. On the other hand, fixed effects models
provides superior estimates, allowing us to make a causal inference by controlling for variables
that are unobserved (Allison 2005). However, traits that do not change over time, such as race,
sex, and parental immigrant status are not included in fixed effects models, thus fixed effects
models are less efficient by limiting information.
Results
Table 1-A compares the sample characteristics of the first wave data by parental
immigrant status. We perform the significance test using bivariate regression analyses (OLS or
logistic) for all the variables on nativity status. The result reveals that the children of immigrants
have significantly higher level of internalizing behavioral problems, consistent with the poorer
mental health of the children of immigrants reported elsewhere (Gross et al. 2006; Jackson,
Kiernan, and McLanahan 2012; Landale et al. 2015; Sam, et al 2008). Many indicators suggested
relatively disadvantaged family environments would explain the worse mental health outcomes
of children of immigrants. First, immigrant families have the lower level of household incomes,
compared to the native counterparts (p<0.001). Less than half of immigrant mothers (46%)
graduated from high school (p<0.001), and this figure is strikingly lower than that of the native
sample (92%). Second, immigrant families are more likely to live in crowded housing
conditions. 58% of the children of immigrants are living in homes where more than two persons
share a bed room. The rate is more than two times of the children of natives.
Regarding family structure, there are some difference between U.S.-born and immigrant
parents. Children of immigrants are more likely to live in horizontally extended households (13%
vs. 7%, p<.05), and mixed extended households (5% vs. 3%, not significant) than are children of
natives. Note that about two thirds of mixed extended households consist of only relatives,
although such immigrant families tend to combine with non-kin more than natives. Similar
patterns are found in Landale, Thomas, and Van Hook’s study using the 2005-2009 Current
Population Survey (2011). On the other hand, children of native families are more likely to live
with non-kin than are children of immigrants (6% vs. 3%, p<.05). The result contradicts to the
expectation that immigrants tend to rely on friendships to compensate for the loss of kin support
after migration (Hammel 1968).
Table 1-B also compares the sample characteristics by parental immigrant status, but uses
the panel data from both waves. There is no difference between W1 and panel data samples in
the distributions of immigrants, the undocumented, race/ethnicity, child sex, mother's education,
and mother's depression. But the panel data sample has the higher family income, lower
crowding housing rate, and lower levels of household extension for both native and immigrant
families. In particular, the proportion of extended households with horizontal kin drops (from 10%
to 7%), as well as the non-kin only (from 4% to 3%), and mixed extended households (from 4%
to 2%). In addition, some nativity differences in family structure disappear in panel data. While
children of native families are more likely to live with non-kin than are children of immigrants in
Wave1, the difference is no more significant in panel data. Only the vertical kin households
maintain the prevalence as the first wave (7%).
Table2 describes the stability of the different types of household extension. The first
column indicates the extended family household types at Wave1, and the first row shows the
household types at Wave2. The second column and row indicate the proportion of simple
households without co-resident extended members, respectively for Wave1 and Wave2. The

third column and row specify the proportion of extended family households, which equals the
sum of vertical, horizontal, non-kin, and mixed family households. The results show that
vertically extended households are the most stable, and non-kin extended households are the
least stable living arrangements. Only 10 percent children residing in non-kin only extended
households still live in the same structure about five years later. About half (47%) of vertically
extended households remain the same household structure, and less than 25 percent of horizontal
kin and about 15 percent of mixed extended households maintain the same household structures.
There are clear nativity differences in the patterns of changes for each household
structure. Only two percent children of immigrants who had lived in mixed households at Wave1
stay in the same household structure at Wave2, when about a third children of natives do. That is,
children of immigrants in such households are experiencing more changes in their living
arrangements by entrances and exits of extended members. On the other hand, about 30 percent
of children of immigrants who had lived with horizontal kin at Wave1 still live in the same
household structures at Wave2, compared to only seven percent of children with US-born parents
do. Similarly, one hundred percent co-resident non-kin in native families left, leaving the family
households simple, while 20 percent immigrant families still live with non-kin. In other words,
immigrant families are less likely to return to simple nuclear family, suggesting their limited
ability to afford independent housing. We will discuss how the different patterns of instability of
living arrangements are related to any differential effect of household extension in later section.
Table3 presents the results of the sets of multivariate regression analyses for OLS and
fixed effects modeling. Model1 shows that the association between child outcomes and different
types of extended households, controlling for child characteristics. OLS estimation shows that
children living with horizontal kin (.38, p<.000) and two or more types of extended members
(.44, p<.000) are at increased risk for internalizing behaviors. Fixed effects estimations show that
children in mixed extended households but not in horizontally extended households are reported
to have higher levels of internalizing behavioral problems at marginal significance (.29, p<.10).
In Model2 covariates are added in order to examine whether other important covariates
explain the relationships seen in Model1. OLS estimation shows that the association with co-
resident horizontal kin decreases in the magnitude and significance (from .38, p<.000 to .18,
p<.10), while that of mixed extended households holds the significance, although the magnitude
of the effects reduces (from .44, p<.000 to .26 p<.05). Fixed effects estimations do not change
much from Model1. Children in mixed extended households apparently increase internalizing
behaviors by about logged .30 score points.
In Model 3, interaction terms between family structures and parental nativity are added in
order to examine whether the effects of each type of extended member are general across
immigrant and native families. The interaction terms between the type of household extension
and parental immigrant status (both legal and illegal) was not significant in both OLS and fixed
effects estimations. However, when specifying legal immigrant status (Model4), the fixed effects
estimates capture the disadvantage of living with non-kin to children of undocumented
immigrant parents. For those children, moving into non-kin extended household increases
internalizing behavioral problems by .88 logged score points (p<.01).
For covariates, child race, age and maternal depression are significant predictor of
children’s internalizing behavioral problems. Children with depressed mothers report about .66
logged point higher internalizing behavioral problems (OLS model), but also depressed mothers
cause about .31 logged point increase in children’s mental health problems (fixed effects). Latino
children show significantly higher internalizing behavioral problems (.17, p<.05) in OLS models.
As children get older, they are less likely to have internalizing behavioral problems by .02
logged points (p<.05) as seen in fixed estimations. Lastly, family income has no impact on
children’s mental health in OLS estimation, although an increase in family incomes marginally
decreases children’s mental health problems (-.05, p<.10).
Figure1 shows the predicted means of logged internalizing behavioral problem index
using the Model3 fixed effects estimation. (The predicted means are calculated using Stata’s
predict command.) We compare the predicted means with unadjusted means for children by
parental nativity in order to answer whether extended families close the divide between
immigrant and native families. When unadjusted, children of immigrants present .90 logged
internalizing behavioral index score, more than 30 percent higher than those of children with US-
born parents. After adjustment, the difference reduces to .02 logged score. Most of the changes
are accounted by children of natives’ increase in predicted internalizing behavioral score, while
children of immigrants’ predicted score is only .02 logged points lower than unadjusted score.
Discussion & Conclusion
The paper examines the relationship between household and children’s internalizing
behavioral problem, specifying which type of extended member is associated with healthier
children, for a representative sample of children in LA. It extends previous research on the
determinants of children’s mental health development by considering the diversity and fluidity of
extended family households. Different types of extended members exert differential influence on
children and their distinctive transition patterns differ by parental immigrant status. Although
these patterns seem to reduce the mental health gap in children between immigrant and native
families, they are not effectively complementing disadvantages facing children of immigrants.
In contrast to our hypothesis, children living in extended households with vertical kin do
not show better mental health status. Previous researchers have proposed that grandparents offer
economic and emotional support for children and the mothers (Castiglia 1999; Kellam,
Ensminger, and Turner, 1977; Kellam, Adams, Brown, and Ensminger, 1982). Possibly, the
assistance would be more direct to mothers than to the child (Harrison et al. 1990), thus the
relationship is not captured in this analysis. However, vertical household extension has no
significant association with children’s internalizing behavioral problem. Also, the influence of
vertical kin does not differ for children of immigrants.
Horizontally extended kin members are not significantly associated with child mental
health, inconsistent with our hypothesis. Although co-resident horizontal kin is apparently
deleterious, as seen in Model1 OLS estimates, the effects become marginal after introducing
covariates. The fixed estimation also shows that moving into horizontally extended households
does not increase children’s internalizing behaviors. This marginal effect does not support for the
kin support (Slaughter and Dilworth-Anderson 1985; Wilson 1986, 1989) or kin strain
(Kana’iaupuni et al. 2005; Leach 2012). As Stanton-Salazar (2001) suggests, the availability of
kin is not always translate into social support. At the same time, aunts and uncles do not cause
mental problems in children, despite their recent arrivals and lower amount of resources.
Non-kin extended members apparently are little associated with child internalizing
behavioral problem. For children of US-born and legal immigrant parents, non-kin appears to put
no benefit or harm, in contrast to Kana’iaupuni et al.’s findings (2005) and Dean and his
colleagues’ belief (1990; 1993) that non-kin support can be substantial. Possibly, it is because
our measurement of non-kin is restricted to the co-resident ones, not including friends and
neighbors living in separate households.
However, non-kin extended households significantly increase internalizing behaviors
only for the children of undocumented immigrants. The bifurcation implies that the meaning of
co-resident non kin differs for illegal migration. The co-resident non-kin members might imply
lack of robust, reliable social network for undocumented immigrants, consistent with the
argument that friendship support is less protective compared to kinship support (Almeida et al.
2011; Xue 2015). Another possibility is that joining non-kin is co-incidental with marital
breakups. About 85 percent of undocumented parents living with non-kin are single parents,
compared to 41-43 percent US-born and legal immigrant parents who are single parents; and the
former are educated less than high school (88%) than the native and legal immigrant parents
(14%, 25%, respectably, available upon request). This speculation should be further examined in
future research.
Mixed households with two or more types of co-residing extended members are
associated with the highest levels of youth internalizing behavioral problem. Moving into
complex (mixed extended) household actually increases mental problems in children, although
the effect is marginally significant (p<.10). Despite the compositional difference between native
and immigrant families, where the latter consist more of non-kin when the former consist of kin,
such living arrangements are not significantly deleterious to children of immigrants. Mixed
extended family structure in itself indicates a stark hardship, for both native and immigrant
families.
We find limited evidence that the patterns of instability or lack of ability to stay with
extended members explain the disadvantages of household extension. For example, the
instability of horizontally extended households, particularly among native families, is not
necessarily detrimental to children. Non-kin extended households, one of the most unstable types
does not exert a significantly deleterious effects. Note that these two types of extended
households show the highest likelihood of becoming simple living arrangements with no
extended members. For children of natives, 89% of horizontally- and 100% of non-kin extended
families at Wave1 now become simple at Wave2; for children of immigrants, 69% of
horizontally- and 65% of non-kin extended families become simple. On the other hand, mixed
extended households, another most unstable living arrangement is associated with increased
internalizing behaviors. Unlike the horizontal and non-kin extended households, the transitional
turnovers of mixed extended households occur across different types of extended household, less
likely to become simple. More important it seems the complexity of living arrangements than
transitions of them.
Limitations
Our study is not free from limitations. First, due to data limitation, where only two waves
are available, neither the number of household transitions nor the types of transitions during the
period, except for those captured at the survey, can be assessed. Because the interval between
Wave 1 and Wave 2 is about five years, it is possible that multiple household transitions have
occurred during the period. Such detailed information, however, cannot be included in the
current analysis. Still, we sufficiently demonstrate the transitory nature of extended family
households.
Second, information about extended household members is limited, thus we do not know
their income, immigration status or duration of residence. Also, the present data do not allow
disaggregating household incomes by respective income earners, thus it is unknown whether the
additional member contributes income (Angel and Tienda 1982; Glick and Van Hook 1997) or
drains income from the host family (Kana’iaupuni et al. 2005; Leach 2012). If data allows, future
research should take into account the potential economic contribution by extended members.
Third, we narrowly defined extended family effects to only those of co-residing members
in the same household. However, extended families can be involved with family life through
frequent visits, phone calls, or other communication media, even if they do not live together.
Also, while friends and neighbors living nearby or faraway can offer social support, we count
only co-resident friends. For our purpose of the study to examine the diversity and fluidity of
family structures and their impacts on child mental health, we think the unit of analysis should be
household based on the relationships with the householder family. By doing so, we distinguish
the implications of extended family from general source of social support.
Contributions
We believe this paper make a substantial contribution to the literature. First, this paper
provides one way to resolve the analytical complexities related to different types of extension.
We specify the types of extended family households by the extended members’ relations to the
householder and the compositional complexity. Specifically, extended family households with
non-kin and two or more types of extended members are added to the previous measure (Glick
and Van Hook 2011; Landale et al. 2011), reflecting the diverse and dynamic living
arrangements among immigrants. Given, the increasing proportion of immigrant population, the
future researchers should consider these family factors in understanding child emotional
development.
To our best knowledge, this is the first systematic research that identifies different types
of household extension and tests the association with children’s mental health. We argue the
previous framework should be revised to consider the differential implications of extended
families in youth emotional development beyond the nuclear family based models. In reality, it is
common for children to live with vertical kin, horizontal kin, non-kin, or two or more types of
members in their childhood. We find that living with two or more types of extended members is
associated with and may cause worse mental health in children. And non-kin may indicate a
disadvantage particular to undocumented parents, such as lack of robust resources. The fact that
the proportion of extended family household with non-kin and two or more types of members are
not negligible calls for more attention to these marginalized extended families.
In addition, we shed light on the entrances and exits of non-nuclear members and show
the transition patterns differ by different types of extended members. We extend the family
literature by considering the movements of non-nuclear family members beyond the parental
breakup. Co-residence with non-kin and two or more types of extended members are the least
stable living arrangements, although volatility may not matter if extended members leave the
family simple. We argue that not all extended families are equal and this inequality should
inspire more discussions on supporting children living in extended family households.
References
Acevedo-Garcia, Dolores, Pan Jocelyn, Hee-Jin Jun, Theresa L. Osypuk, and Karen M. Emmons.
2005. “The Effect of Immigrant Generation on Smoking.” Social science & medicine.
61(6):1223–1223.
Allison, Paul D. 2002. “Missing Data. Series: Quantitative Applications in the Social Sciences.”
Thousand Oaks. CA: Sagе.
Allison, Paul D. 2005. Fixed Effects Regression Methods for Longitudinal Data Using SAS. SAS
Institute. Retrieved October 17, 2015
(https://books.google.com/books?hl=en&lr=&id=OIPExEh-
tcMC&oi=fnd&pg=PA1&dq=allison+fixed+effects+&ots=HpCi9WKGgl&sig=i4yy9Ar
RXJrhIb5Sjj64U0oBoTA).
Almeida, Joanna, S. V. Subramanian, Ichiro Kawachi, and Beth E. Molnar. 2011. “Is Blood
Thicker than Water? Social Support, Depression and the Modifying Role of
Ethnicity/nativity Status.” Journal of epidemiology and community health 65(1):51–56.
Angel, Ronald and Marta Tienda. 1982. “Determinants of Extended Household Structure:
Cultural Pattern or Economic Need?” American Journal of Sociology 87(6):1360–83.
Berk, Richard A. 1983. “Applications of the General Linear Model to Survey Data.” Pp. 495–
546 in Handbook of survey research. Academic Press New York.

Bethencourt, Carlos and José-Víctor Ríos-Rull. 2009. “On the Living Arrangements of Elderly
Widows.” International Economic Review 50(3):773–801.
Blank, Susan and Ramon S. Torrecilha. 1998. “Understanding the Living Arrangements of
Latino Immigrants: A Life Course Approach.” International Migration Review 32(1):3–
19.
Castiglia, Patricia T. 1999. “Extended Families: Social Support Systems for Children.” Journal
of Pediatric Health Care 13(3):139–41.
Chase-Lansdale, P. Lindsay, Jeanne Brooks-Gunn, and Elise S. Zamsky. 1994. “Young African-
American Multigenerational Families in Poverty: Quality of Mothering and
Grandmothering.” Child development 65(2):373–93.
Cohen, Philip N. 2002. “Extended Households at Work: Living Arrangements and Inequality in
Single Mothers’ Employment.” Pp. 445–63 in Sociological Forum, vol. 17. Springer.
Retrieved October 21, 2014 (http://link.springer.com/article/10.1023/A:1019631107686).
Conley, Dalton, Kathryn M. Pfeiffer, and Melissa Velez. 2007. “Explaining Sibling Differences
in Achievement and Behavioral Outcomes: The Importance of within- and between-
Family Factors.” Social Science Research 36(3):1087–1104.
Cunningham, Solveig Argeseanu, Julia D. Ruben, and K. M. Venkat Narayan. 2008. “Health of
Foreign-Born People in the United States: A Review.” Health & Place 14(4):623–35.
Dean, Alfred, Bohdan Kolody, and Patricia Wood. 1990. “Effects of Social Support from
Various Sources on Depression in Elderly Persons.” Journal of Health & Social Behavior
31(2):148–61.
DeLeire, Thomas and Ariel Kalil. 2002. “Good Things Come in Threes: Single-Parent
Multigenerational Family Structure and Adolescent Adjustment.” Demography
39(2):393–413.
Dressler, William W. 1985. “Extended Family Relationships, Social Support, and Mental Health
in a Southern Black Community.” jhealsocibeha Journal of Health and Social Behavior
26(1):39–48.
Edin, Kathryn and Laura Lein. 1997. Making Ends Meet : How Single Mothers Survive Welfare
and Low-Wage Work. New York: Russell Sage Foundation.
Evans, Gary W. 2006. “Child Development and the Physical Environment.” Annual Review of
Psychology 57(1):423–51.
Flores, Yvette G. 2013. Chicana and Chicano Mental Health. Tucson: University of Arizona
Press. Retrieved September 20, 2015 (http://muse.jhu.edu/books/9780816599950/).
Franzini, Luisa and Maria Eugenia Fernandez-Esquer. 2004. “Socioeconomic, Cultural, and
Personal Influences on Health Outcomes in Low Income Mexican-Origin Individuals in
Texas.” Social Science & Medicine 59(8):1629–46.
Gerstel, Naomi. 2011. “Rethinking Families and Community: The Color, Class, and Centrality of
Extended Kin Ties.” Sociological Forum 26(1):1–20.
Glick, JE, FD Bean, and JVW Van Hook. 1997. “Immigration and Changing Patterns of
Extended Family Household Structure in the United States: 1970-1990.” Journal of
Marriage and the Family 59:177–91.
Glick, Jennifer E. and Jennifer Van Hook. 2011. “Does a House Divided Stand? Kinship and the
Continuity of Shared Living Arrangements.” Journal of Marriage & Family 73(5):1149–
64.

Glick, Jennifer E. and Michael J. White. 2004. “Post-Secondary School Participation of
Immigrant and Native Youth: The Role of Familial Resources and Educational
Expectations.” Social Science Research 33(2):272–99.
Gonzales, Nancy A. et al. 2008. “Mexican American Adolescents’ Cultural Orientation,
Externalizing Behavior and Academic Engagement: The Role of Traditional Cultural
Values.” American Journal of Community Psychology 41(1/2):151–64.
Grant, BF et al. 2004. “Immigration and Lifetime Prevalence of DSM-IV Psychiatric Disorders
among Mexican Americans and Non-Hispanic Whites in the United States: Results from
the National Epidemiologic Survey on Alcohol and Related Conditions.” Archives of
general psychiatry 61(12):1226–33.
Gross, Deborah et al. 2006. “The Equivalence of the Child Behavior Checklist/1 1/2-5 across
Parent Race/ethnicity, Income Level, and Language.” Psychological Assessment
18(3):313–23.
Hamilton, Hayley A. 2005. “Extended Families and Adolescent Well-Being.” Journal of
Adolescent Health 36(3):260–66.
Hammel, Eugene A. 1968. Alternative Social Structures and Ritual Relations in the Balkans.
Prentice-Hall Englewood Cliffs. Retrieved June 28, 2015
(http://library.wur.nl/WebQuery/clc/1608396).
Harker, Kathryn. 2001. “Immigrant Generation, Assimilation, and Adolescent Psychological
Well-Being.” Social Forces 79(3):969–1004.
Hedeker, Donald, Robert D. Gibbons, and Brian R. Flay. 1994. “Random-Effects Regression
Models for Clustered Data with an Example from Smoking Prevention Research.”
Journal of Consulting and Clinical Psychology 62(4):757.
Hernandez, Donald J. 2004. “Demographic Change and the Life Circumstances of Immigrant
Families.” The Future of Children 14(2):17–47.
von Hippel, Paul T. 2007. “Regression with Missing Ys: An Improved Strategy for Analyzing
Multiply Imputed Data.” Sociological Methodology 37(1):83–117.
Hofferth, Sandra L., Johanne Boisjoly, and Greg J. Duncan. 1998. “Parents’ Extrafamilial
Resources and Children’s School Attainment.” Sociology of Education 246–68.
Hondagneu-Sotelo, Pierrette. 1994. Gendered Transitions : Mexican Experiences of
Immigration. Berkeley, Calif.: University of California Press.
Hunter, Andrea G. and Margaret E. Ensminger. 1992. “Diversity and Fluidity in Children’s
Living Arrangements: Family Transitions in an Urban Afro-American Community.”
Journal of Marriage and Family 54(2):418–26.
Jackson, Margot I., Kathleen Kiernan, and Sara McLanahan. 2012. “Immigrant-Native
Differences in Child Health: Does Maternal Education Narrow or Widen the Gap?:
Nativity, Maternal Education, and Child Health.” Child Development 83(5):1501–9.
Kana’iaupuni, Shawn Malia, Katharine M. Donato, Theresa Thompson-Colón, and Melissa
Stainback. 2005. “Counting on Kin: Social Networks, Social Support, and Child Health
Status.” Social Forces 83(3):1137–64.
Kellam, S. G., M. E. Ensminger, and R. J. Turner. 1977. “Family Structure and the Mental
Health of Children. Concurrent and Longitudinal Community-Wide Studies.” Archives of
general psychiatry 34(9):1012–22.
Kellam, Sheppard G., Rebecca G. Adams, C. Hendricks Brown, and Margaret E. Ensminger.
1982. “The Long-Term Evolution of the Family Structure of Teenage and Older
Mothers.” Journal of Marriage and Family 44(3):539–54.

King, Serena M., William G. Iacono, and Matt McGue. 2004. “Childhood Externalizing and
Internalizing Psychopathology in the Prediction of Early Substance Use.” ADD Addiction
99(12):1548–59.
Krieger, James and Donna L. Higgins. 2002. “Housing and Health: Time Again for Public
Health Action.” American Journal of Public Health 92(5):758–68.
Landale, Nancy S., Jessica Halliday Hardie, R. S. Oropesa, and Marianne M. Hillemeier. 2015.
“Behavioral Functioning among Mexican-Origin Children Does Parental Legal Status
Matter?” Journal of health and social behavior 56(1):2–18.
Landale, Nancy S., K. J. .. Thomas, and Jennifer Van Hook. 2011. “The Living Arrangements of
Children of Immigrants.” Future of Children 21:43–70.
Leach, M. a. 2012. “A Burden of Support? Household Structure and Economic Resources
Among Mexican Immigrant Families.” Journal of Family Issues 35:28–53.
Matt, Georg E. and Alfred Dean. 1993. “Social Support from Friends and Psychological Distress
Among Elderly Persons: Moderator Effects of Age.” Journal of Health and Social
Behavior 34(3):187–200.
Mendoza, F. S. 2009. “Health Disparities and Children in Immigrant Families: A Research
Agenda.” Pediatrics 124(Supplement):S187–95.
Menjívar, Cecilia. 2000. Fragmented Ties : Salvadoran Immigrant Networks in America.
Berkeley: University of California Press.
Padilla, Yolanda C., Erin R. Hamilton, and Robert A. Hummer. 2009. “Beyond the
Epidemiological Paradox: The Health of Mexican-American Children at Age Five*.”
Social science quarterly 90(5):1072–88.
Perreira, KristaM., Kathleen Mullan Harris, and Dohoon Lee. 2006. “Making It in America:
High School Completion by Immigrant and Native Youth.” Demography 43(3):511–36.
Portes, Alejandro. 1995. The Economic Sociology of Immigration : Essays on Networks,
Ethnicity, and Entrepreneurship. New York: Russell Sage Foundation.
Portes, Alejandro and Rubén G. Rumbaut. 2001. Legacies : The Story of the Immigrant Second
Generation. Berkeley; New York: University of California Press ; Russell Sage
Foundation.
Portes, Alejandro and Julia Sensenbrenner. 1993. “Embeddedness and Immigration: Notes on the
Social Determinants of Economic Action.” American Journal of Sociology 98(6):1320–
50.
Pugliesi, Karen and Scott L. Shook. 1998. “Gender, Ethnicity, and Network Characteristics:
Variation in Social Support Resources.” Sex Roles 38(3/4):215–38.
Richards, T., M. J. White, and A. O. Tsui. 1987. “Changing Living Arrangements: A Hazard
Model of Transitions among Household Types.” demography Demography 24(1):77–97.
Rogler, Lloyd H. 1994. “International Migrations: A Framework for Directing Research.”
American Psychologist 49(8):701–8.
Rosenfeld, Michael. 2015. “Revisiting the Data from the New Family Structure Study: Taking
Family Instability into Account.” Sociological Science 2:478–501.
Rubin, Donald B. 2003. “Discussion on Multiple Imputation.” International Statistical Review
71(3):619–25.
Sam, David L., Paul Vedder, Karmela Liebkind, Felix Neto, and Erkki Virta. 2008.
“Immigration, Acculturation and the Paradox of Adaptation in Europe.” European
Journal of Developmental Psychology 5(2):138–58.
Sarkisian, Natalia. 2006. “‘Doing Family Ambivalence’: Nuclear and Extended Families in
Single Mothers’ Lives.” Journal of Marriage and Family 68(4):804–11.
Schwartz, Seth J. 2007. “The Applicability of Familism to Diverse Ethnic Groups: A Preliminary
Study.” Journal of Social Psychology 147(2):101–18.
Slaughter, D. T. and P. Dilworth-Anderson. 1985. “Childcare of Black Sickle Cell Anemic
Children: Impact of Father’s Presence and Absence from Households.” in Biennial
Meeting of the Society for Research in Child Development, Toronto, Canada.
Solari, Claudia D. and Robert D. Mare. 2012. “Housing Crowding Effects on Children’s
Wellbeing.” Social Science Research 41(2):464–76.
Sonuga-Barke, E. J. and M. Mistry. 2000. “The Effect of Extended Family Living on the Mental
Health of Three Generations within Two Asian Communities.” The British Journal of
Clinical Psychology / the British Psychological Society 39 ( Pt 2):129–41.
Stanton-Salazar, Ricardo D. 2001. Manufacturing Hope and Despair : The School and Kin
Support Networks of U.S.-Mexican Youth. New York: Teachers College Press.
Stevens, Gonneke W. J. M. and Wilma A. M. Vollebergh. 2008. “Mental Health in Migrant
Children.” Journal of Child Psychology and Psychiatry 49(3):276–94.
Teachman, Jay. 2011. “Modeling Repeatable Events Using Discrete-Time Data: Predicting
Marital Dissolution.” JOMF Journal of Marriage and Family 73(3):525–40.
Treas, Judith. 2008. “Transnational Older Adults and Their Families*.” FARE Family Relations
57(4):468–78.
Treas, Judith and S. Mazumdar. 2004. “Kinkeeping and Caregiving: Contributions of Older
People in Immigrant Families.” Journal of comparative family studies. (35):105–22.
Turney, Kristin and Grace Kao. 2009. “Assessing the Private Safety Net: Social Support among
Minority Immigrant Parents.” Sociological Quarterly 50(4):666–92.
Umberson, Debra, Robert Crosnoe, and Corinne Reczek. 2010. “Social Relationships and Health
Behavior Across the Life Course.” Annual Review of Sociology 36(1):139–57.
Van Hook, J. and J. E. Glick. 2007. “Immigration and Living Arrangements: Moving beyond
Economic Need versus Acculturation.” Demography 44(2):225–49.
Walen, Heather R. and Margie E. Lachman. 2000. “Social Support and Strain from Partner,
Family, and Friends: Costs and Benefits for Men and Women in Adulthood.” Journal of
Social and Personal Relationships 17(1):5–30.
Wilson, Melvin N. 1986. “The Black Extended Family: An Analytical Consideration.”
Developmental Psychology 22(2):246.
Wilson, Melvin N. 1989. “Child Development in the Context of the Black Extended Family.”
American Psychologist 44(2):380.
Xue, Ming. 2015. “Social Support from Friends and Family in a Tibetan Village.” Personal
Relationships 22(1):30–44.
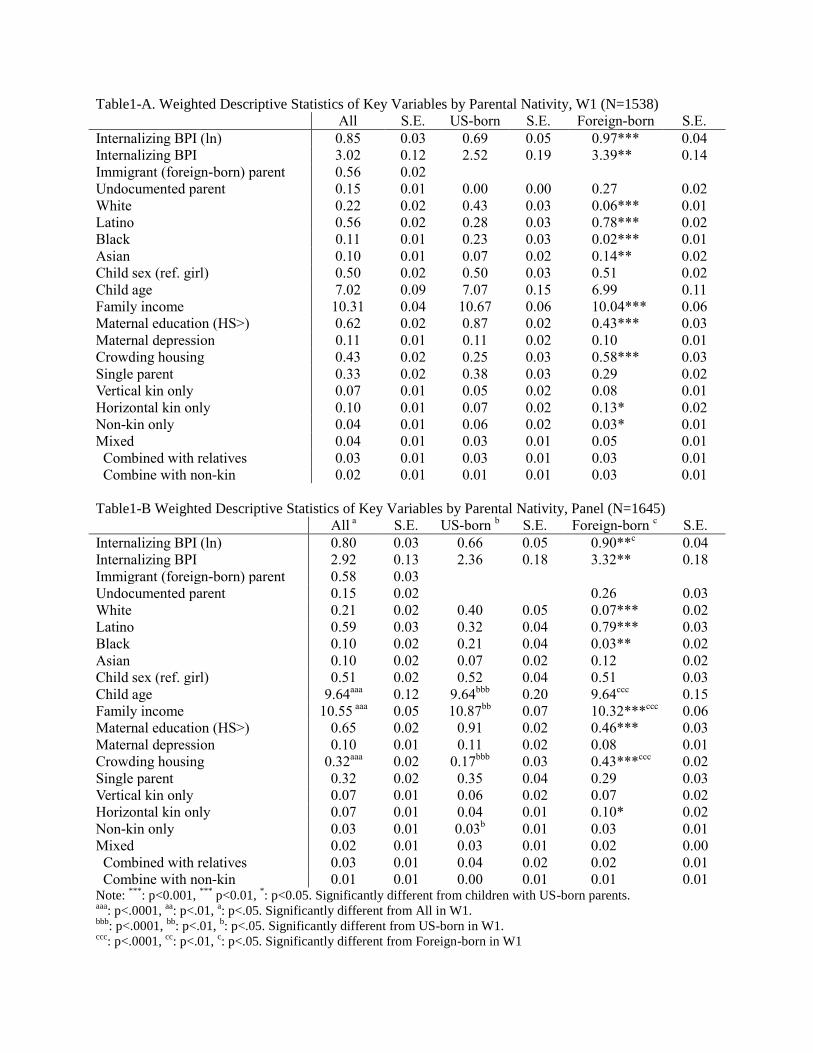
Table1-A. Weighted Descriptive Statistics of Key Variables by Parental Nativity, W1 (N=1538)
All S.E. US-born S.E. Foreign-born S.E.
Internalizing BPI (ln) 0.85 0.03 0.69 0.05 0.97*** 0.04
Internalizing BPI 3.02 0.12 2.52 0.19 3.39** 0.14
Immigrant (foreign-born) parent 0.56 0.02
Undocumented parent 0.15 0.01 0.00 0.00 0.27 0.02
White 0.22 0.02 0.43 0.03 0.06*** 0.01
Latino 0.56 0.02 0.28 0.03 0.78*** 0.02
Black 0.11 0.01 0.23 0.03 0.02*** 0.01
Asian 0.10 0.01 0.07 0.02 0.14** 0.02
Child sex (ref. girl) 0.50 0.02 0.50 0.03 0.51 0.02
Child age 7.02 0.09 7.07 0.15 6.99 0.11
Family income 10.31 0.04 10.67 0.06 10.04*** 0.06
Maternal education (HS>) 0.62 0.02 0.87 0.02 0.43*** 0.03
Maternal depression 0.11 0.01 0.11 0.02 0.10 0.01
Crowding housing 0.43 0.02 0.25 0.03 0.58*** 0.03
Single parent 0.33 0.02 0.38 0.03 0.29 0.02
Vertical kin only 0.07 0.01 0.05 0.02 0.08 0.01
Horizontal kin only 0.10 0.01 0.07 0.02 0.13* 0.02
Non-kin only 0.04 0.01 0.06 0.02 0.03* 0.01
Mixed 0.04 0.01 0.03 0.01 0.05 0.01
Combined with relatives 0.03 0.01 0.03 0.01 0.03 0.01
Combine with non-kin 0.02 0.01 0.01 0.01 0.03 0.01
Table1-B Weighted Descriptive Statistics of Key Variables by Parental Nativity, Panel (N=1645)
All a S.E. US-born
b S.E. Foreign-born
c S.E.
Internalizing BPI (ln) 0.80 0.03 0.66 0.05 0.90**c
0.04
Internalizing BPI 2.92 0.13 2.36 0.18 3.32** 0.18
Immigrant (foreign-born) parent 0.58 0.03
Undocumented parent 0.15 0.02 0.26 0.03
White 0.21 0.02 0.40 0.05 0.07*** 0.02
Latino 0.59 0.03 0.32 0.04 0.79*** 0.03
Black 0.10 0.02 0.21 0.04 0.03** 0.02
Asian 0.10 0.02 0.07 0.02 0.12 0.02
Child sex (ref. girl) 0.51 0.02 0.52 0.04 0.51 0.03
Child age 9.64aaa
0.12 9.64bbb
0.20 9.64ccc
0.15
Family income 10.55 aaa
0.05 10.87bb
0.07 10.32***ccc
0.06
Maternal education (HS>) 0.65 0.02 0.91 0.02 0.46*** 0.03
Maternal depression 0.10 0.01 0.11 0.02 0.08 0.01
Crowding housing 0.32aaa
0.02 0.17bbb
0.03 0.43***ccc
0.02
Single parent 0.32 0.02 0.35 0.04 0.29 0.03
Vertical kin only 0.07 0.01 0.06 0.02 0.07 0.02
Horizontal kin only 0.07 0.01 0.04 0.01 0.10* 0.02
Non-kin only 0.03 0.01 0.03b 0.01 0.03 0.01
Mixed 0.02 0.01 0.03 0.01 0.02 0.00
Combined with relatives 0.03 0.01 0.04 0.02 0.02 0.01
Combine with non-kin 0.01 0.01 0.00 0.01 0.01 0.01 Note:
***: p<0.001,
*** p<0.01,
*: p<0.05. Significantly different from children with US-born parents.
aaa: p<.0001,
aa: p<.01,
a: p<.05. Significantly different from All in W1.
bbb: p<.0001,
bb: p<.01,
b: p<.05. Significantly different from US-born in W1.
ccc: p<.0001,
cc: p<.01,
c: p<.05. Significantly different from Foreign-born in W1
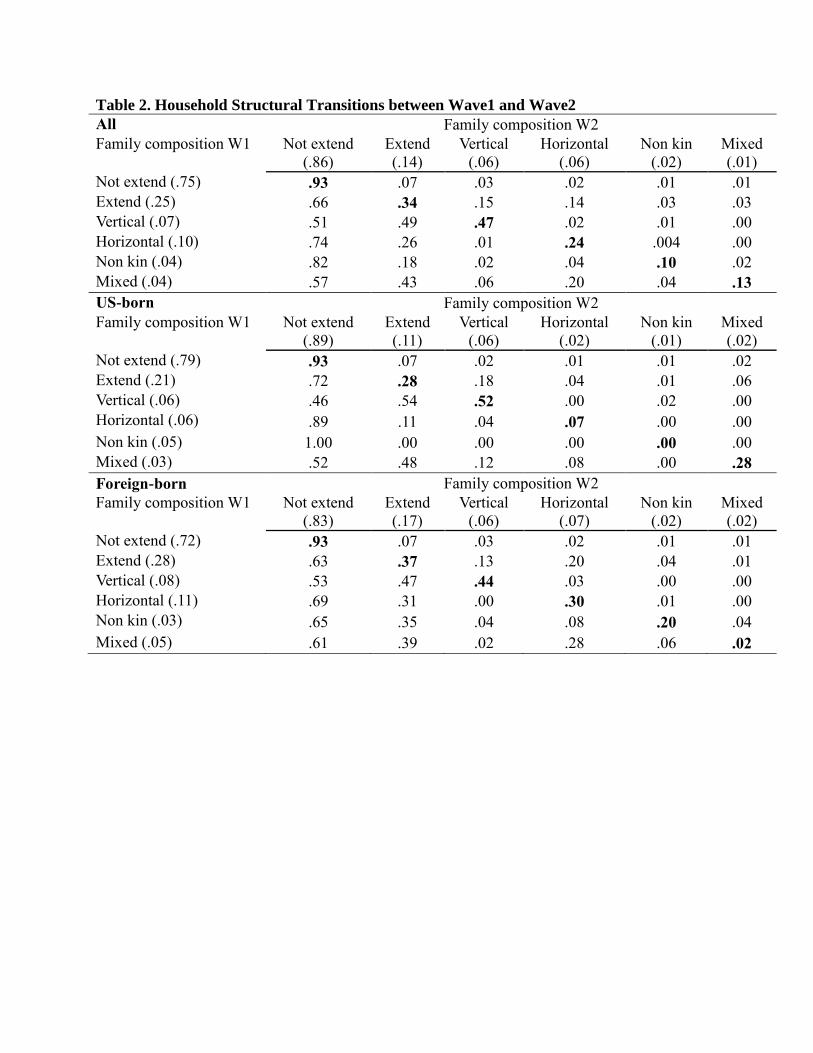
Table 2. Household Structural Transitions between Wave1 and Wave2
All Family composition W2
Family composition W1 Not extend
(.86)
Extend
(.14)
Vertical
(.06)
Horizontal
(.06)
Non kin
(.02)
Mixed
(.01)
Not extend (.75) .93 .07 .03 .02 .01 .01
Extend (.25) .66 .34 .15 .14 .03 .03
Vertical (.07) .51 .49 .47 .02 .01 .00
Horizontal (.10) .74 .26 .01 .24 .004 .00
Non kin (.04) .82 .18 .02 .04 .10 .02
Mixed (.04) .57 .43 .06 .20 .04 .13
US-born Family composition W2
Family composition W1 Not extend
(.89)
Extend
(.11)
Vertical
(.06)
Horizontal
(.02)
Non kin
(.01)
Mixed
(.02)
Not extend (.79) .93 .07 .02 .01 .01 .02
Extend (.21) .72 .28 .18 .04 .01 .06
Vertical (.06) .46 .54 .52 .00 .02 .00
Horizontal (.06) .89 .11 .04 .07 .00 .00
Non kin (.05) 1.00 .00 .00 .00 .00 .00
Mixed (.03) .52 .48 .12 .08 .00 .28
Foreign-born Family composition W2
Family composition W1 Not extend
(.83)
Extend
(.17)
Vertical
(.06)
Horizontal
(.07)
Non kin
(.02)
Mixed
(.02)
Not extend (.72) .93 .07 .03 .02 .01 .01
Extend (.28) .63 .37 .13 .20 .04 .01
Vertical (.08) .53 .47 .44 .03 .00 .00
Horizontal (.11) .69 .31 .00 .30 .01 .00
Non kin (.03) .65 .35 .04 .08 .20 .04
Mixed (.05) .61 .39 .02 .28 .06 .02
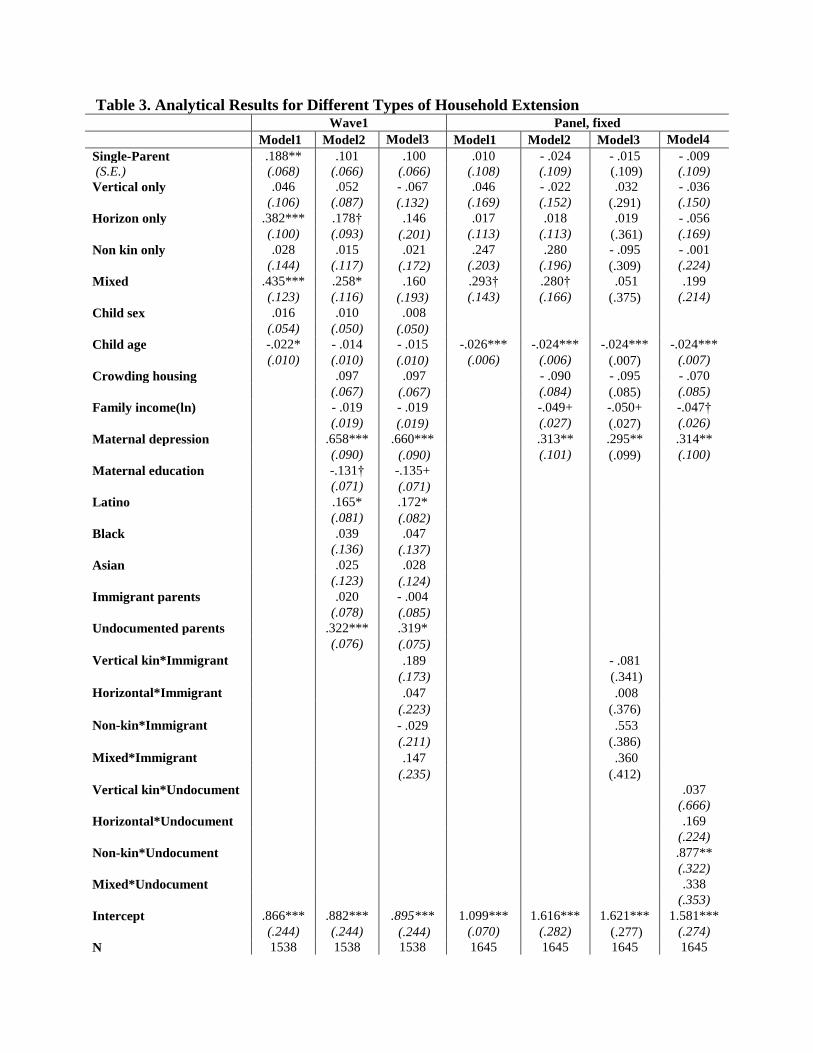
Table 3. Analytical Results for Different Types of Household Extension Wave1 Panel, fixed
Model1 Model2 Model3 Model1 Model2 Model3 Model4
Single-Parent .188** .101 .100 .010 - .024 - .015 - .009
(S.E.) (.068) (.066) (.066) (.108) (.109) (.109) (.109)
Vertical only .046 .052 - .067 .046 - .022 .032 - .036
(.106) (.087) (.132) (.169) (.152) (.291) (.150)
Horizon only .382*** .178† .146 .017 .018 .019 - .056
(.100) (.093) (.201) (.113) (.113) (.361) (.169)
Non kin only .028 .015 .021 .247 .280 - .095 - .001
(.144) (.117) (.172) (.203) (.196) (.309) (.224)
Mixed .435*** .258* .160 .293† .280† .051 .199
(.123) (.116) (.193) (.143) (.166) (.375) (.214)
Child sex .016 .010 .008
(.054) (.050) (.050)
Child age -.022* - .014 - .015 -.026*** -.024*** -.024*** -.024***
(.010) (.010) (.010) (.006) (.006) (.007) (.007)
Crowding housing
.097 .097
- .090 - .095 - .070
(.067) (.067)
(.084) (.085) (.085)
Family income(ln)
- .019 - .019
-.049+ -.050+ -.047†
(.019) (.019)
(.027) (.027) (.026)
Maternal depression
.658*** .660***
.313** .295** .314**
(.090) (.090)
(.101) (.099) (.100)
Maternal education
-.131† -.135+
(.071) (.071)
Latino
.165* .172*
(.081) (.082)
Black
.039 .047
(.136) (.137)
Asian
.025 .028
(.123) (.124)
Immigrant parents
.020 - .004
(.078) (.085)
Undocumented parents
.322*** .319*
(.076) (.075)
Vertical kin*Immigrant .189 - .081
(.173) (.341)
Horizontal*Immigrant .047 .008
(.223) (.376)
Non-kin*Immigrant - .029 .553
(.211) (.386)
Mixed*Immigrant .147 .360
(.235) (.412)
Vertical kin*Undocument
.037
(.666)
Horizontal*Undocument
.169
(.224)
Non-kin*Undocument
.877**
(.322)
Mixed*Undocument
.338
(.353)
Intercept .866*** .882*** .895*** 1.099*** 1.616*** 1.621*** 1.581***
(.244) (.244) (.244) (.070) (.282) (.277) (.274)
N 1538 1538 1538 1645 1645 1645 1645

R2 .050 .182 .183 .014 .048 .055 .055
Rho
.544 .539 .537 .539
Note: ***
: p<0.001, ***
p<0.01, *: p<0.05, †: p<.10.

Figure1. Unadjusted/Adjusted Differences between Native and Immigrant families
Note: Significantly different from children with US parents. The results are based on Model 3
fixed effects estimation. ***
: p<0.001, **
p<0.01, *: p<0.05
.66
.90** .86 .88
.00
.10
.20
.30
.40
.50
.60
.70
.80
.90
1.00
US Foreign
unadjusted Full (m3)





























