Embed Size (px)
Citation preview
Understanding and Addressing Medical
Necessity and Patient Status Denials
Presented To:
TAHFAApril 13, 2018
Joan C. Ragsdale, JD
Chief Executive Officer
(205) 970-8804
Inspiration from The Art of War
“If you know the enemy and know yourself, you need not fear the result of a hundred battles.” Sun Tzu
2
Regulatory Overview
Complying with changing health care regulations requires continuous education about regulatory changes, process flexibility to adjust to regulatory changes, and an ability to apply standards to a variety of fact patterns all while communicating clearly and transparently to patients, medical staff and regulators.
And…there is a requirement to get it right with every patient, every time!
3
Who is Looking at Medical Necessity
Recovery Auditors
Quality Improvement Organizations (QIOs)
Medicare Administrative Contractors
Zone Program Integrity Contractors
Office of Inspector General/DOJ
Medicaid Programs
Medicaid Integrity Contractors
Commercial Insurers, including Medicare Advantage programs
Private parties such as whistleblowers (and counsel)
4

Why Focus on Medical Necessity Denials?
Financial well-being: “no margin no mission”
Denials may be indicators of compliance challenges
Weak “front end processes” require costly “backend” fixes
Patterns of denials lead to additional audits and scrutiny
False Claims Liability gives rise to both civil and criminal liability—both from a corporate perspective and personal perspective
5
How Broad is the Medical Necessity Denial Process and Why Does It Matter?
Patient status errors are generally denied under the sanction of billing for services that are not medically necessary.
Criminal and civil liability under the False Claims Act exists for failure to comply with regulatory guidance and interpretations, such as billing for services that are not medically necessary.
6
Enhanced Individual Liability
Increased focus on individual liability and accountability from the Department of Justice (September 9, 2015 “Yates memo”)
Additional management and executive certifications as part of the corporate integrity process (including Board certifications for Corporate Integrity Agreements)
7
Common Risk Areas
1. Patient status determination: Inpatient versus outpatient status
2. Medical necessity defined
3. Documentation requirements
4. Technical requirements
8
KEPRO Reviews
Recognize that the process is not merely educational, but involves a recoupment if there is a denial
The original call is an opportunity to resolve questions of medical necessity as well as to provide missed documentation
KEPRO has physicians on the call and experience between our physicians and KEPRO staff on medical necessity denials has been collegial with generally positive outcomes. May be changing with increase in volume.
9

Importance Of Denial Management
Denials may provide a basis for an allegation of “knowing and willful” misconduct. The standard is “you knew” or “should have known.”
Where there is a denial, someone got it wrong, and the key issue is “who got it wrong” and why. Adjusting to an inappropriate denial can be devastating to the hospital because it adversely affects both revenue and appropriate process adjustments.
Compliance requires continuous measurement against a moving target
Must be coordination between revenue cycle management, medical staff, utilization review and compliance
10
CMS 1633 F (on QIOs and Audit Rules)
Hospitals that are found to exhibit a pattern of practices, including, but not limited to: having high denial rates and consistently failing to adhere to the 2-midnight rule (including having frequent inpatient hospital admissions for stays that do not span one midnight), or failing to improve their performance after QIO educational intervention, will be referred to the Recovery Auditors for further medical review
In addition to the formal QIO medical review process mentioned above, we intend to continuously monitor … applicable claims data… looking for trends and gaming
The number of claims that a Recovery Auditor will be allowed to review for patient status will be based on the claim volume of the hospital and the denial rate identified by the QIO (between 10 and 25 admissions)
11
Extrapolation
CMS will consider allowing Recovery Auditors to use Extrapolation to estimate overpayment amounts for:
Providers who maintain a high denial rate for an extended time period
Providers who have excessively high denial rates for a shorter time period
Providers with a moderate denial rate, whose improper payments equal a significantly high overpayment dollar amount
12
Source: Medicare Fee-For-Service Recovery Audit Program – Last updated 5/3/2016
Current Issues
DOJ investigations of Short Stay admissions
Corporate Integrity Agreements
Short Stay Admissions
Evaluation and Management Coding
KEPRO Denials of Short Stays
Review and Education regarding use of Electronic Health Records
13

Current Issues
Medical Necessity and Certification
Inpatient Rehabilitation Facilities (IRF)
Inpatient Psychiatric Facilities (IPF)
Home Care
Hospice Services
Hyperbaric Oxygen and Wound Care
Compliance with National Coverage Determination (NCD) for Implantable Cardiac Defibrillators (ICDs)
14
Current Issues
Protocols and education for patient status
Assessment, protocols and education regarding Utilization Management review by Case Management staff
Board education and engagement regarding Compliance Program planning and on-going monitoring activities
15
Current Issues with MA Plans
Medicare Advantage is a private sector option for Medicare beneficiaries. Medicare coverage is provided by a private insurer (like United or Cigna), subject to CMS regulations
Medicare and Medicaid contract with commercial insurers to provide a covered benefit for a per member per month (PMPM) fee.
The PMPM payment is based upon the health status of the member determined by a “risk score.” Medicare Advantage covers approximately 31 percent of all Medicare beneficiaries and almost 60 percent of all Medicaid beneficiaries are in a managed care plan.
16
MA Plan design
Medicare Advantage enrollees are entitled to the identical benefit package available to traditional Medicare enrollees
MA Plans may alter the benefit design, such as altering copays and deductibles, limiting provider networks, and waiving wait periods
“An MA organization (MAO) offering an MA plan must provide enrollees in that plan with all Original Medicare-covered services.” (Section 10.2 of the Medicare Managed Care Manual, revised 5/2011). In particular, an “item or service… must be covered by every MA plan if: Its coverage is consistent with general coverage guidelines included in Original Medicare manuals and instructions”
17

MA Plan Design
“While an MA plan may offer additional coverage as a supplemental benefit, it may not limit the original Medicare coverage.”
18
What’s the Issue?
Hospitals report that Medicare Advantage Plans are failing to provide Part A coverage for medically necessary hospital stays
The rules defining which payments are appropriate for Part A payment are set forth in 42 CFR 412.3
19

What’s the Issue, Continued
The failure to pay for the service as a Part A service harms the hospital because the reimbursement difference is substantial, with probably a $5000-$10,000 dollar a case differential for a short stay.
20
Statutory Language for Medical Necessity
21
The principle of providing and being paid for medically necessary care is the fundamental cornerstone of our health care delivery system.
What is “medically necessary care” for which payment should be made?
Medicare coverage is for “items and services that are reasonable and necessary for the diagnosis or treatment of illness or injury.” 42 US 1395y(a)(1)(A)
Providers must ensure that services are “provided economically and only when, and to the extent, medically necessary.”
Additional guidance may be provided through National Coverage Determinations (NCDs), Local Coverage Determinations (LCDs) and various forms of CMS/government guidance.
Do You Know What is Necessary?
So, What is Medical Necessity?
Title XVIII of the Social Security Act, Section 1862(a)(1) states:
“No Medicare payment shall be made for items or services
which are not reasonable and necessary for the diagnosis or treatment of illness or injury”
NotMedicallyNecessary
22
The Essence of the “Status” Challenge
Clearly an Inpatient Clearly an Outpatient (receiving observation)
“…consistent with medical review findings
that identical beneficiaries may receive
identical services as either inpatients or
outpatients in different hospitals. We
believe that this supports our proposed
continuation of our existing policy that
there are no prohibitions against a
patient receiving any individual service
as either an inpatient or an outpatient…” (78 Fed. Reg.
160, Aug. 19, 2013 50945)
• Same diagnosis
• Same treatment
• Same doctor
• Same patient
• Same hospital location
• And almost the same medical
record documentation23
Two Midnight Rule (§ 412.3(e))
Inpatient Admission appropriate when:
THE PHYSICIAN EXPECTS the patient to require a stay that crosses at least two midnights.
Exceptions for “rare and unusual” circumstances which do not require an expectation of 2 midnights, i.e. newly initiated mechanical ventilation.
Cases where Inpatient Admission is appropriate when there is not an expectation that the patient requires a stay crossing two midnights.
For procedure on Inpatient Only List.
Admitting physician clinical judgment exception.
24
Starting the Clock
The expectation that the patient requires care spanning two midnights should be based on all time that the patient is expected to continuously receive care in the hospital (and in a transferring hospital) receiving care.
The clock starts when the patient begins receiving treatment (beyond triage); and
The time includes all time in the hospital or a transferring hospital receiving services including outpatient services (such as services in the ED or in an outpatient treatment area).
25
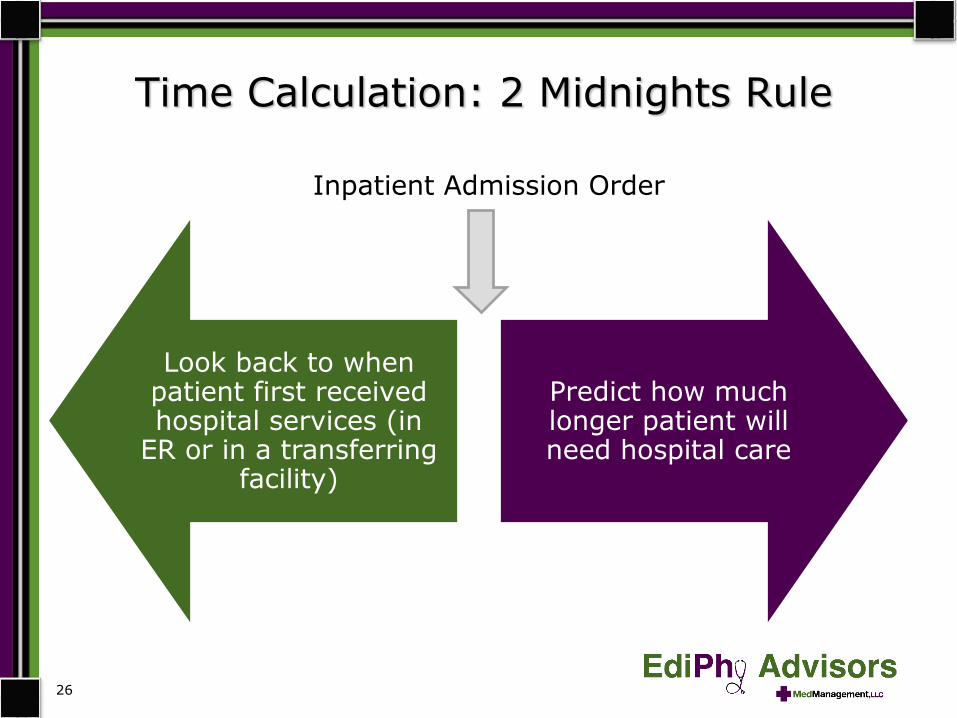
Time Calculation: 2 Midnights Rule
Look back to when patient first received hospital services (in
ER or in a transferring facility)
Predict how much longer patient will need hospital care
26
Inpatient Admission Order
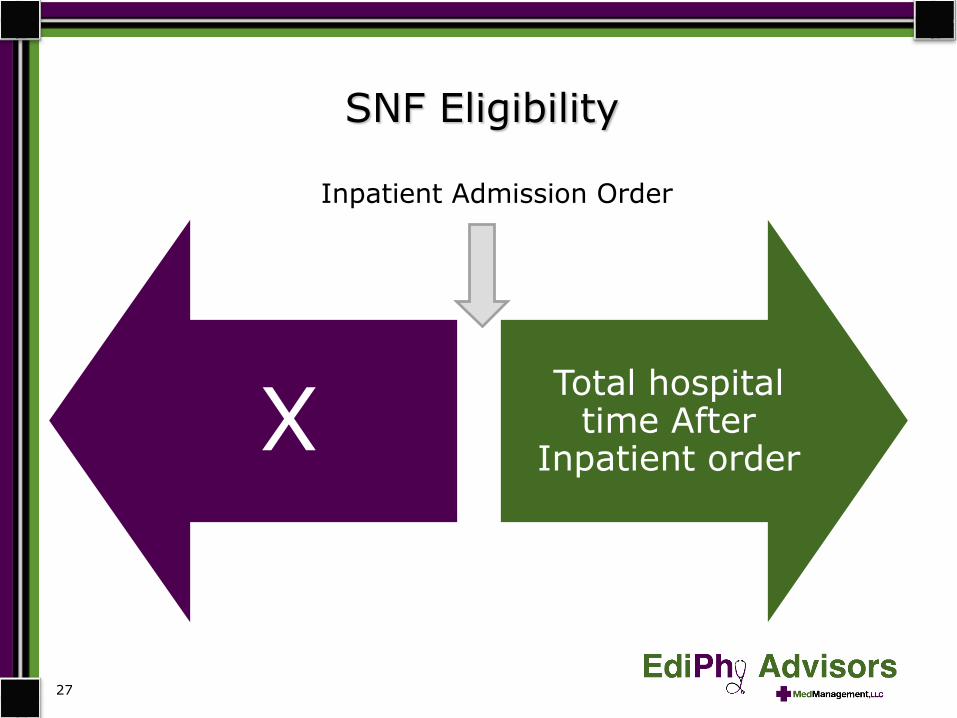
SNF Eligibility
XTotal hospital
time After Inpatient order
27
Inpatient Admission Order
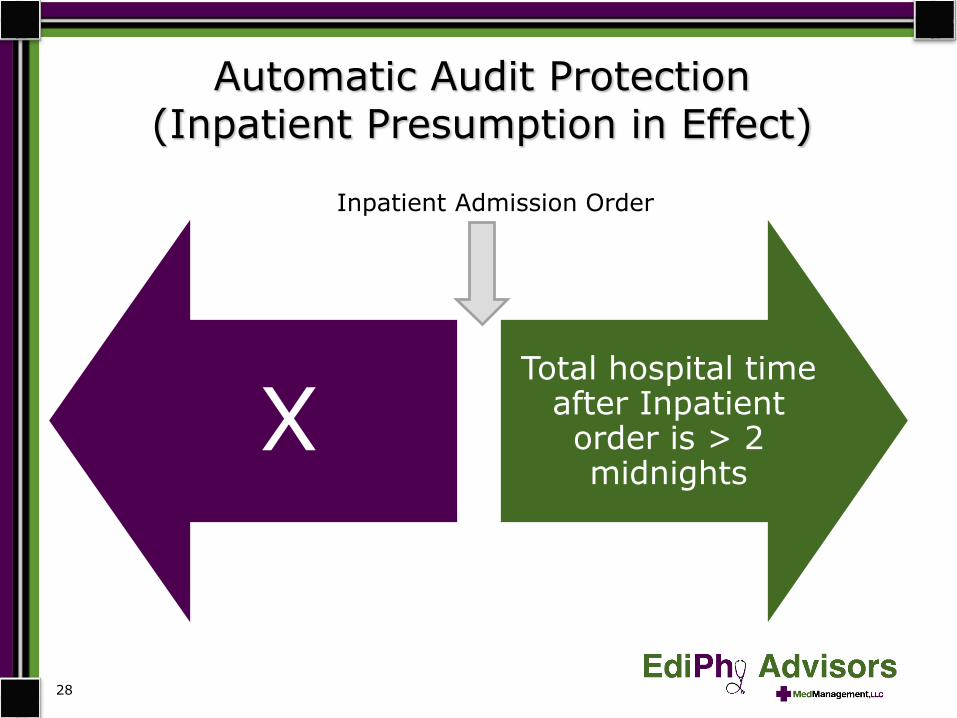
Automatic Audit Protection (Inpatient Presumption in Effect)
XTotal hospital time
after Inpatient order is > 2 midnights
28
Inpatient Admission Order
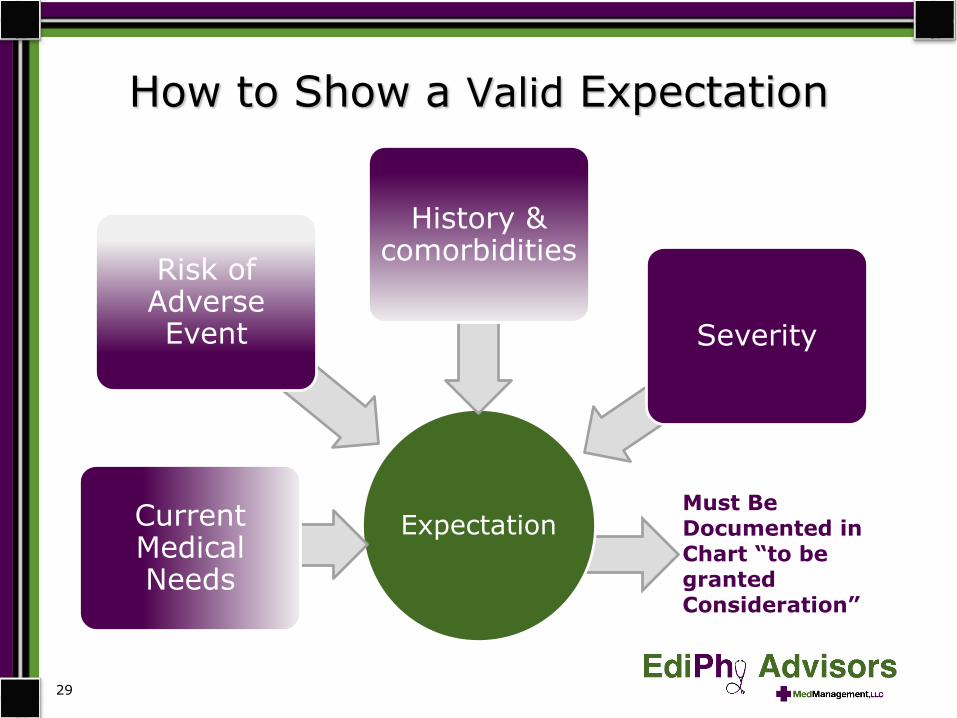
ExpectationCurrent Medical Needs
Risk of Adverse Event
History & comorbidities
Severity
How to Show a Valid Expectation
29
Must Be Documented in Chart “to be granted Consideration”
§ 412.3 Conditions of Payment
(a) “This physician order must be present in the medical record and be supported by the physician admission and progress notes, in order for the hospital to be paid for hospital inpatient services under Medicare Part A.”
(b) “The order must be furnished by a qualified and licensed practitioner who has admitting privileges at the hospital as permitted by State law, and who is knowledgeable about the patient’s hospital course, medical plan of care, and current condition.”
28
Practical Problems Related to Orders
Orders written by emergency department physicians who do not have admitting privileges.
Verbal (i.e., oral) orders must be authenticated prior to patient discharge.
Care transitions create authentication/signing issues.
31
Admission Order Technicalities
32
WHO? Order must be by a practitioner with admitting privileges (or cosigned by one with admitting privileges) who is knowledgeable about the patient’s hospital course, medical plan of care and current condition.
WHEN? The order must be signed prior to discharge by a physicianfamiliar with the case and authority to admit inpatients.
WHAT? Must State “Admit to Inpatient” or otherwise clearly indicate “inpatient” status.
No delegation of the admission decision allowed.
The necessity of a proper order has been “codified” in the regulations: ALJ and CMS contractors are thus bound- no discretion. Hospital will not get paid no matter what.
When Does the Inpatient Order Have to be Signed?
The order must be signed prior to discharge.
“With regard to the time of discharge, a Medicare beneficiary is considered a patient of the hospital until the effectuation of activities typically specified by the physician as having to occur prior to discharge (e.g. “discharge after supper” or “discharge after voids”). So discharge itself can, but does not always, coincide exactly with the time that the discharge order is written -- rather it occurs when the physician’s order for discharge is effectuated.”
Source: CMS Guidance, January 30, 2014, “Hospital Inpatient Admission Order and Certification”
33
Factors One Must Consider
The reviewer shall consider, in his/her review of the medical record, any pre-existing medical problems or extenuating circumstances that make admission of the beneficiary medically necessary. Factors that may result in an inconvenience to a beneficiary or family do not, by themselves, justify inpatient admission. When such factors affect the beneficiary's health, consider them in determining whether inpatient hospitalization was appropriate.
Medicare Program Integrity Manual
Chapter 6 - Intermediary MR Guidelines for Specific Services
6.5.2 - Medical Review of Acute Inpatient Prospective Payment System (IPPS) Hospital or Long-term Care Hospital (LTCH) Claims
A. Determining Medical Necessity and Appropriateness of Admission
34

Documentation Requirements
The expectation of the physician should be based on such complex medical factors as:
Patient history and comorbidities
Severity of signs and symptoms
Current medical needs
Risk of an adverse event
“The factors that lead to a particular clinical expectation must be documented in the medical record in order to be granted consideration.”
“It has been longstanding Medicare policy to require physicians to admit . . . as a hospital inpatient based on their expected length of stay”…Based on “…information available to the admitting practitioner at the time of the admission.”
35

Unforeseen Circumstances That Lead to Actual Stay of Less Than Two Midnights
If there is a reasonable expectation that the patient requires care in the hospital for a period spanning two midnights at the time of a valid inpatient order, then Part A billing is appropriate even if unforeseen events lead to a stay crossing 0-1 midnights after the order.
Examples of unforeseen events include:
Death
Transfer
AMA
Unexpectedly rapid improvement
Cancelled surgery
36
Documentation Requirements Custodial care is excluded from coverage.
Custodial care serves to assist an individual in the activities of daily living, such as assistance in walking, getting in and out of bed, bathing, dressing, feeding, and using the toilet, preparation of special diets, and supervisionof medication that usually can be self-administered.
Custodial care essentially is personal care that does not require the continuing attention of trained medical or paramedical personnel.
The reviewer shall consider, in his/her review of the medical record, any pre-existing medical problems or extenuating circumstances that make admission of the beneficiary medically necessary. Factors that may result in an inconvenience to a beneficiary or family do not, by themselves, justify inpatient admission. When such factors affect the beneficiary's health, consider them in determining whether inpatient hospitalization was appropriate.
Source: Medicare Program Integrity Manual
Chapter 6 - Intermediary MR Guidelines for Specific Services
6.5.2 - Medical Review of Acute Inpatient Prospective Payment System (IPPS) Hospital or Long-term Care Hospital (LTCH) Claims
A. Determining Medical Necessity and Appropriateness of Admission
37
Admitting Practitioner’s Task
Decide if the patient should be admitted to IP status or placed in outpatient status based on a thorough understanding of Medicare law, regulations, and guidance.
If you think the patient meets inpatient status requirements:
Write/enter a clear “admit to inpatient status” order.
Ensure a practitioner with admitting privileges signs, dates, and times the order before the patient is discharged.
Document effectively the unique, patient specific facts that support the inpatient status order at the time the order is rendered.
Continue to document support for the inpatient status with every medical record entry until the patient is gone and the discharge summary is complete.
Clarify any ambiguities as to the patient status as soon as possible.
If the patient does not meet inpatient status, write an order to place in outpatient status, and, if appropriate, begin observation services.
If uncertain, place in outpatient status until you can make a reasonable decision as to the proper status.
38

Medicaid Status Determinations
Medicaid agencies
Typically Medicaid agencies remain tied to a “24 hour” or “overnight” standard
Temporal analysis remains important
Intensity of service likewise remains important
Typically “outpatient” procedures are unlikely to be paid on an inpatient basis
39

OIG Recommendations to CMS
Conduct routine analysis of hospital billing and target for review the hospitals with high or increasing numbers of short inpatient stays that are potentially inappropriate under the 2-midnight policy;
Identify and target for review the short inpatient stays that are potentially inappropriate under the 2-midnight policy;
Analyze the potential impacts of counting time spent as an outpatient toward the 2-night requirement for SNF services so that beneficiaries receiving similar hospital care have similar access to these services;
Explore ways of protecting beneficiaries in outpatient stays from paying more than they would have paid as inpatients.
40

Timing is Critical
UR Staff should analyze the patient’s status at four (4) critical points in the Throughput Process
At the time a decision is made to place the patient in a bed
Prior to the second midnight if the patient remains in Outpatient Status AND is expected to stay a second midnight
Each day until discharge if patient remains in Outpatient Status
Prior to actual discharge
41
Important Points to Consider
Capture the date and time services began
Include Time from Transferring facility
Include all time in the emergency department
Focus on plan of care
Number of midnights passed at the time new orders are written and/or treatments are initiated
Expectation of time to complete services
Apply Inpatient Screening Criteria first
Remember the difference between time based analysis and IS/SI criteria of InterQual
42

Commercial Payer Status Determinations
Commercial Payers
Health plans typically utilize evidence based criteria as screening criteria
Important to stress medical necessity of hospital setting and intensity of service as well as temporal analysis
Medicare Advantage plans must provide Medicare “inpatient services”
43
Function and Value of the Physician Advisor
A Strong Physician Advisor Program:
Starts with ‘Practicing physicians who are Board certified’
Supports the facility’s Compliance efforts through compliance with CMS regulations
Promotes education through peer to peer (collegial) discussions re: Status and medical necessity documentation
Uses complex medical judgment to render accurate Status determinations
44

Surgery Cases –Same Clinical Analysis
Because a procedure is NOT on the Inpatient Only list does NOT mean it must be done on an outpatient
basis, and it does NOT change the standard of review.
• If the attending expects that the surgical procedure will keep the patient in the hospital for a period of time spanning more than two midnights, then inpatient care is needed for that particular patient.
• Documentation should clearly support the rationale for this expectation in order to meet CMS inpatient criteria.
45

Denial Management
Concurrent Process:
Identify the denial rationale and validate reason based on the supporting evidence found in the medical record and/or process components that may contribute to a denial
Identify Concurrent Patients
Onsite reviewer dialogue
Peer to Peer conversation
Identify Retrospective Patients
Appeals
46

Denial Reasons
Most frequently identified reasons to deny an Inpatient Stay:
Did not meet Medical Necessity
Late Admission Notification
Clinicals not sent/not sent timely/not on file
Authorization Error (IP vs OP)
No Pre-cert
Status order must match the claim
47
Evaluate Every Denial
Do not accept “payer prefers to pay obs”
Criteria based reasoning provided by the medical director
Pre-cert information varies from clinical data that was submitted to payer
Evaluate procedures for complications and/or changes to the procedure that was planned
Consider process components that impact contract compliance (notification within specified timeframe, prior to bed assignment)
Premature closure of payer’s Web Portal
48

Do Not Change a Status from Inpatient to Outpatient Because:
The patient stayed less than two midnights (short stay)
You don’t see documentation that states ‘the patient had unexpected improvement’
You accept a denial without researching the case specifics
The payer ‘prefers to pay obs’
Patient expires or leaves AMA
Patient elects hospice
49
Impact of Status Changes
Inpatient to outpatient status change for Medicare patients must include Condition Code 44.
CMS set the policy for the use of Condition Code 44
to address those relatively infrequent occasions,
such as a late-night weekend admission when no
case manager is on duty to offer guidance, when
internal review subsequently determines that an
inpatient admission does not meet hospital criteria
and that the patient would have been registered as
an outpatient under ordinary circumstances.
50
Back to the Art of War
“In the midst of chaos, there is also opportunity.”
51






























