Embed Size (px)
Citation preview

Version: 0 1
Trim:
Date of Inspection: 24 March 2010 Length of inspection: 5 hours Inspectors: Sarah Brain and Janet Kirkland Inspection details: The report covers the pre-inspection analysis, the visit and information provided about the centre received between 2 October 2008 and 25 March 2010. This was a randomly selected unannounced interim inspection of the centre. A small number of centres are randomly sampled in this way for quality assurance purposes. The inspection team had no indication or evidence of any critical areas of non-compliance at the centre prior to inspection. Date of Executive Licensing Panel: 3 June 2010 Purpose of the Inspection report The purpose of the inspection is to assess whether centres are complying with the HF&E Act 1990 (as amended), the HF&E Act 2008 and the Code of Practice to ensure that centres are providing a quality service for patients. The report summarises the findings of the licence interim inspection highlighting areas of good practice, as well as areas where further improvement is required to improve patient services and meet regulatory requirements. It is primarily written for the Authority’s Licence Committee/ Executive Licensing Panel which makes the decision about the continuation of the centre’s licence. Centre details Centre Name Royal Cornwall Hospital
Centre Number
0282
Licence Number
E0282/2/b
Centre Address
Cornwall Centre for Reproductive Medicine, Wheal Unity Clinic, Directorate of Obstetrics and Gynaecology, Princess Alexandra Wing Truro, TR1 3LJ
Telephone Number 01872 253044 Person Responsible
Mr Jonathan Lord
Licence Holder
None
Date Licence issued 01/10/2009
Licence expiry date
30/06/2012
Additional conditions applied to this licence
None
Unannounced Interim Inspection Report

Version: 0 2
Trim:
Contents
Page Centre details ......................................................................................................................... 1 Contents ................................................................................................................................. 2 Report to Executive Licensing Panel ................................................................................... 3
Recommendation to the Executive Licensing Panel
Details of Inspection findings............................................................................................... 4
Brief description of the centre and its licensing history Activities of the Centre Updated actions since the centre was inspected Focus of inspections for 2010-12 Changes / improvements since the last inspection Areas of concern
Areas of practice that require the attention of the Person Responsible……………17
Critical area of non compliance Major area of non compliance Other area of practice that requires consideration
Version: 0 3
Trim:
Report to the Executive Licensing Panel Recommendation to the Executive Licensing Panel: In assessing overall compliance, the inspectorate considers that it has sufficient information drawn from documentation submitted by the centre prior to the inspection and from observations and interviews conducted during the inspection visit to conclude that: • The Person Responsible (PR) is considered to have discharged his duties under S.17
of the HFE Act 1990 (as amended). • Premises, processes and procedures used in the conduct of licensed activities and
observed at the time of this inspection are considered largely suitable. Some improvements are required in relation to:
• Documented assessments of the competency of all staff • Witnessing training • Witnessing procedures and documentation • Validation of critical equipment • Audit of activities • Establishing quality indicators • Documentation of Standard Operating Procedures (SOPs) • Document control • Costed treatment plans • Calibration of critical measuring equipment
The inspectorate considers that, overall there is sufficient information available to recommend the continuation of the centre’s licence without additional conditions. The inspectorate also recommends that the Executive Licensing Panel requires that the PR complies with the recommendations detailed in this report within the prescribed timeframes. The Executive Licensing Panel are asked to note that a number of the recommendations related to witnessing require immediate action.

Version: 0 4
Trim:
Details of Inspection findings Brief description of the centre and its licensing history: The Cornwell Centre for Reproductive Medicine (CCRM) provides basic partner treatment services and is licensed to process gametes and perform Intra-Uterine Insemination (IUI). It also functions as a satellite IVF Centre for Peninsula Centre for Reproductive Medicine, Exeter (Centre 0005) South West Centre for Reproductive Medicine, Plymouth, (Centre 0179) and Bristol Centre for Reproductive Medicine (Centre 0295). The CCRM is housed within the Wheal Unity Clinic, Directorate of Obstetrics, Princess Alexandra Wing, The Royal Cornwall Hospital at Treliske on the outskirts of Truro. The hospital is administered by the Royal Cornwall Hospitals NHS Trust (RCHT) and the South West Peninsula Strategic Health Authority and managed as a partnership between the RCHT and Cornwall IVF Ltd. NHS funding is available in appropriate patients for 4 cycles of stimulated IUI treatment. If unsuccessful, patients are then referred for IVF via the satellite arrangements. The centre provides IUI and satellite IVF treatments for both NHS and self funding patients. The Centre has been licensed since 5th July 2007. It has been inspected twice since the licence was originally granted. A licence renewal inspection was conducted in March 2008 and on consideration of the inspection report a Licence Committee agreed to grant a licence for a further four years. The current licence therefore expires on the 30 June 2012. An additional inspection was carried out in October 2008 to assess the premises which had been recently refurbished. The Licence Committee was satisfied that the renovated premises were suitable for the activities licensed. There are no additional conditions on the centre’s licence. Activities of the Centre:
Type of treatment Number of treatment cycles for the period [for the year ending 1st quarter 2008]*
Intrauterine insemination with partner sperm
66 cycles
Other licensable activities � or Not applicable (N/A) Procurement and Distribution of Gametes
�
Processing of Gametes � Storage of eggs N/A Storage of sperm N/A Storage of embryos N/A Research N/A
*These data were extracted from the HFEA register for the period [for the year ending 1st quarter 2008]. The data in the Register may be subject to change as errors are notified to us by clinics, or picked up through our quality management systems.
Version: 0 5
Trim:
Updated actions since the centre was inspected on 24 March 2010: The PR responded to the inspection report on the 10 May 2010 and pages 19 onwards of this report have been updated accordingly.

Version: 0 6
Trim:
1. Focus of inspections for 2010-12 Witnessing Evidence of how the centre demonstrates compliance with the requirement to double check the identification of samples and the patients or donors to whom they relate at all critical points of the clinical and laboratory process. The Centre has a witnessing protocol in place and an interviewed member of staff was able to clearly explain the witnessing procedures followed at the centre. What the centre does well. What they could do better. Witnessing Practice The inspectorate noted that the centre’s witnessing practice is non-contemporaneous at some stages of sperm preparation. Centre staff explained that they cross check information on all the sperm preparation tubes and the sperm pot at the beginning of the procedure but thereafter, witnessing checks are not performed each time the sperm sample is moved between tubes. The final tube is then witnessed against patient identity and patient records at the time of IUI. Staff explained that they follow this approach as they only ever process one sample for IUI a day. Members of staff confirmed that the risks associated with this witnessing procedure have not been assessed. The PR was reminded of Standard Licence Condition T71 which requires that “Centres must have witnessing protocols in place to double check the identification of samples and the patients or donors to whom they relate at all critical points of the clinical and laboratory process. These checks must be completed and recorded at the time the relevant clinical or laboratory process/procedure takes place”. The PR should define the critical points of the laboratory process with reference to Code of Practice Guidance18.4 and review the witnessing procedures accordingly. The PR must take action to ensure witnessing is performed contemporaneously in a manner compliant with T71. Through discussions with centre staff and on evaluation of the witnessing SOP the inspectorate concluded that the centre’s witnessing process for collecting sperm is not fully compliant with Code of Practice Guidance. The cross-check between identifying information provided by the sperm providers against records, the laboratory data sheet and sperm receptacle does not involve an active identification check of the sperm provider. Staff explained that the identify of the patient is cross checked by reception staff when a patient attends for appointments, but that this check is conducted by a different person than the individual responsible for the witnessing check. Code of Practice 18.4b states that “When collecting eggs or sperm, transferring embryos and carrying out insemination, staff should ask patients and donors to give their own identifying information (full name and date of birth), rather than asking the donor or patient to confirm or reject information read out to them”. It is recommended that the PR ensures that this witnessing step involves active identification of the male partner.
Version: 0 7
Trim:
Witnessing documentation Two sets of patient records were audited for evidence of witnessing during the course of this inspection. During the audit it was found that:
• The witnessing documentation within the patient records included staff signatures but did not include the name and status of the person conducting each procedure or the name and status of the person who witnesses the procedure.
• The time of the procedure was also not seen to be recorded for all steps of the process.
• Whilst evidence was seen in both sets of records that the female patients had witnessed the actual insemination procedure, there was no signature and identifying information recorded for the person actually performing the procedure
This is non-compliant with Standard Licence Condition T71 and Code of Practice Guidance 18.7. Standard Licence Condition T71 requires that “Centres must have witnessing protocols in place to double check the identification of samples and the patients or donors to whom they relate at all critical points of the clinical and laboratory process. These checks must be completed and recorded at the time the relevant clinical or laboratory process/procedure takes place. A record must be kept in each patient’s/donor’s medical records. These records must include the name, status and signature of the person performing the activity and the name, status and signature of the person who witnesses the procedure”. Code of Practice Guidance 18.7 states that “When the procedure takes place, a record should be made in the patient or donor notes stating:(a) the procedure, (b) the date and time of the procedure, (c) the signature of the person doing the procedure, and (d) the signature of the witness. The PR must ensure that witnessing records are kept in accordance with both Standard Licence Condition T71 and Code of Practice Guidance 18.7. The PR is also reminded that Code of Practice Guidance 18.8 requires that there should be a separate record of the name, job title and signature of everyone who carries out or witnesses laboratory and clinical procedures. Such a record is not currently kept at the centre. The Centre’s witnessing SOP was reviewed by the inspectorate and through discussion with staff it was found that the SOP did not correctly reflect the witnessing procedures used by staff. The SOP included some steps which are not part of the procedure followed by staff and it also did not remind staff to include a check against patient records at each witnessing step. Code of Practice Guidance 18.2 states that “Centres should have witnessing protocols relevant to their local systems and conditions, based on HFEA model protocols”. It is recommended that the PR reviews the HFEA model protocols and updates the witnessing SOP to ensure compliance with CoP Guidance 18.2. Staff training and competence Staff explained that they have not yet had their competence to perform witnessing assessed. The team was also unable to provide evidence of their training on witnessing procedures. The PR should ensure that in accordance with Code of Practice Guidance 18.11 all staff members who act as witnesses have completed the centre’s training programme for new staff, and refresher training (as appropriate), to ensure they fully understand the principles of witnessing procedures and follow the centre’s protocols.

Version: 0 8
Trim:
Quality indicators The centre does not have quality indicators for witnessing activities, contrary to licence condition T35. Quality indicators must be established for all activities authorised by this licence and other activities carried out in the course of providing treatment services that do not require a licence. Parenthood Evidence of how the centre demonstrates compliance with the requirements in relation to legal parenthood The PR explained that they do not perform any IUI cycles with donor sperm and that any satellite patients planning IVF treatment with donor gametes are provided with information about legal parenthood and are consented at the treating centre (IVF Centre for Peninsula Centre for Reproductive Medicine, Exeter, South West Centre for Reproductive Medicine, Plymouth, and Bristol Centre for Reproductive Medicine). This theme is therefore not applicable to this centre and was not reviewed by the inspectorate. What the centre does well. N/A What they could do better. N/A Information about the cost of treatment Evidence of how the centre demonstrates that it has introduced personalised costed treatment plans for all patients What the centre does well. What they could do better. The PR explained that costs of treatment are explained verbally to IUI patients during consultation appointments. The centre’s policy is that a checklist is completed for each patient at consultations and this checklist includes a reminder to staff to provide cost information to patients. Copies of the checklist were seen to be stored in patient records. However, it was noted during an audit of patient records that in two records the section of the checklist relating to cost information had not been completed. The inspectors were therefore unable to confirm that patients are being provided with information about the cost of their treatment. Furthermore there was lack of clarity about whether the information provided to the patients is personalised. Centre staff stated that they give a general sum of what patients should expect to pay for a cycle of IUI but that this does not include the cost of medication. The inspectorate did not see any evidence to show that satellite patients are being
Version: 0 9
Trim:
provided with personalised costed treatment plans. Satellite patients are provided with a general leaflet on the expected costs of treatment at the three primary centres. This information leaflet was provided during the inspection and was seen to include detail on the cost of IVF, ICSI, surgical sperm retrieval, embryo freezing and FET cycles. The leaflet also explained that these charges did not include drug charges. Specific information about the drug charges was not provided but the leaflet did state that the drugs could vary from £400-£900. The PR should ensure compliance with Code of Practice guidance 4.3 which requires that “Before treatment, storage or both are offered, the centre should also give the person seeking treatment or storage, and their partner (if applicable) a personalised costed treatment plan. The plan should detail the main elements of the treatment proposed (including investigations and tests), the cost of that treatment and any possible changes to the plan, including their cost implications. The centre should give patients the opportunity to discuss the plan before treatment begins”. Patient consent to the disclosure of information, held on the HFEA Register, for use in Research Evidence of how the centre demonstrates that it provides information to patients about the use of information, held on the HFEA Register, for use in research. N/A for patients attending for IUI treatment at this centre. The PR confirmed that the satellite patients complete the HFEA MT1 and WT2 consent forms which allow patients to consent to, amongst other things, the disclosure of their registry data to researchers, before they attend the primary centre for treatment. The PR reported that their patients were not tending to refuse to consent to disclosure to researchers at this stage. What the centre does well. What they could do better. Consent issues in relation to the storage of embryos (including cooling off period) Evidence of how the centre demonstrates compliance with the requirements relating to the withdrawal of consent to storage of embryos intended for use in treatment. This centre is only licensed to perform IUI treatment and does not store embryos for patients. This theme is therefore not directly applicable to this centre. However, the centre does prepare patients for IVF treatment, and possible storage of embryos, by acting as a satellite centre for three IVF centres (IVF Centre for Peninsula Centre for Reproductive Medicine, Exeter, South West Centre for Reproductive Medicine, Plymouth, and Bristol Centre for Reproductive Medicine) Centre staff were therefore asked about the information they provide to these patients about storage of embryos. 1 WT form – “consent to the use of your eggs and embryos for your treatment and the storage or your embryos”. 2 MT form – “consent to the use of your sperm and embryos for your partner's treatment and the storage of your embryos”.
Version: 0 10
Trim:
What the centre does well. What they could do better. The PR provided the inspectorate with copies of the patient information leaflets that they provide to satellite IVF patients. These were reviewed by the inspectorate and it was found that the leaflets provided to patients planning to go to the IVF Centre for Peninsula Centre for Reproductive Medicine or South West Centre for Reproductive Medicine contained out of date information about the statutory storage regulations for embryos. This has been addressed directly with staff at these centres. The South West Centre for Reproductive Medicine has confirmed that the leaflets distributed by this centre were out of date and should not be in use. They plan to contact the PR at Centre 0282 to ensure that the correct information is being handed to patients. Staff at IVF Centre for Peninsula Centre have explained that they do provide patients with information about the new statutory storage periods and that they have discussed this with the team at Centre 0282. It is recommended that the PR ensures that the correct information is being distributed to patients. Multiple Births Evidence of how the centre demonstrates compliance with Guidance Note 7 of the Code of Practice in relation to multiple births: Not required for licence E0282/2/b which covers this IUI clinic With regard to the satellite patients the PR was aware of the single embryo transfer policy in use at the primary centres. The PR explained to the inspectorate that work is underway on a single embryo transfer policy for NHS funded treatment in the South West Peninsula region. The primary centres; Peninsula Centre for Reproductive Medicine (Centre 0005), South West Centre for Reproductive Medicine (Centre 0179) and Bristol Centre for Reproductive Medicine (Centre 0295) are responsible for monitoring and auditing multiple births, and subsequent review and revision of the multiple birth minimisation strategy. What the centre does well N/A What they could do better N/A
Version: 0 11
Trim:
2. Changes / improvements since the last inspection on 2 October 2008.
Area for improvement Action required Action taken as evidenced
during this inspection Minutes of staff meetings detailing staff discussion and consideration of the move to renovated premises were not available on the day of inspection. This is potentially non-compliant with HFEA Code of Practice, 7th edition, Standards 6.2.13.
The PR should present to HFEA the minutes of staff meetings detailing staff discussion and consideration of the move to renovated premises to confirm compliance with HFEA Code of Practice, 7th edition, Standards S.6.2.13. Alternatively, the PR should confirm to the inspectorate how the Centre complies with the requirement in S.6.2.13 for an ‘effective means for communicating information to and receiving suggestions from staff’. By 15th October 2008.
At this inspection the PR explained that the team aims to meet formally at least once a quarter. Copies of recent meeting minutes were provided as evidence of this. No further action required.
The air quality in the laboratory has not yet been assessed to determine whether gametes will be processed in air of appropriate quality, compliant with standard Licence Condition A.10.19 and Code of Practice, 7th Edition, S.7.8.5, G.9.4.2 and G.9.4.3.
The PR should provide the HFEA with air quality assessment results, to be performed before the start of licensed activities, to confirm that gametes will be processed in air of appropriate quality, compliant with standard Licence Condition A.10.19 and Code of Practice, 7th Edition, S.7.8.5, G.9.4.2 and G.9.4.3 By 15th October 2008.
Air quality results were sent to the HFEA on 13 October 2008 – this indicated grade D background air quality and B air quality in the hood. Further air quality test results (from February 2010) were provided at this inspection and these indicated that the air quality in the working environment is grade A with a background air quality of D. No further action required.

Version: 0 12
Trim:
The PR said that the refurbished premises have been certified by the local Trust Health and Safety and Fire Safety Managers as being safe for clinical activities. This certification was not present on the day of inspection thus compliance with HFEA Code of Practice, 7th edition, Standards 6.3.2 could not be evidenced.
The PR should present to the HFEA copies of the Health and Safety and Fire Safety certification, or communications from the Trust Safety Managers, to confirm that the premises are compliant with HFEA Code of Practice, 7th edition, Standards 6.3.2 By 15th October 2008.
This was sent to the HFEA on 13 October 2008. No further action required.
Version: 0 13
Trim:
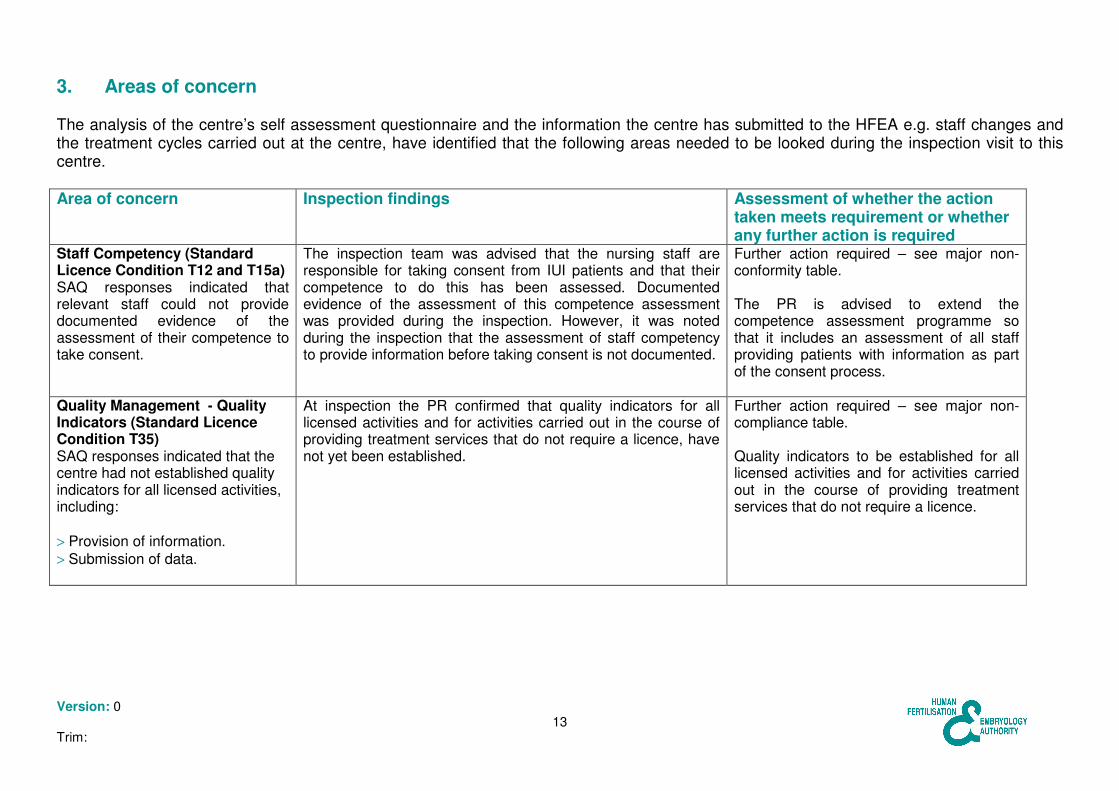
3. Areas of concern The analysis of the centre’s self assessment questionnaire and the information the centre has submitted to the HFEA e.g. staff changes and the treatment cycles carried out at the centre, have identified that the following areas needed to be looked during the inspection visit to this centre. Area of concern Inspection findings Assessment of whether the action
taken meets requirement or whether any further action is required
Staff Competency (Standard Licence Condition T12 and T15a) SAQ responses indicated that relevant staff could not provide documented evidence of the assessment of their competence to take consent.
The inspection team was advised that the nursing staff are responsible for taking consent from IUI patients and that their competence to do this has been assessed. Documented evidence of the assessment of this competence assessment was provided during the inspection. However, it was noted during the inspection that the assessment of staff competency to provide information before taking consent is not documented.
Further action required – see major non-conformity table. The PR is advised to extend the competence assessment programme so that it includes an assessment of all staff providing patients with information as part of the consent process.
Quality Management - Quality Indicators (Standard Licence Condition T35) SAQ responses indicated that the centre had not established quality indicators for all licensed activities, including: > Provision of information. > Submission of data.
At inspection the PR confirmed that quality indicators for all licensed activities and for activities carried out in the course of providing treatment services that do not require a licence, have not yet been established.
Further action required – see major non-compliance table. Quality indicators to be established for all licensed activities and for activities carried out in the course of providing treatment services that do not require a licence.
Version: 0 14
Trim:
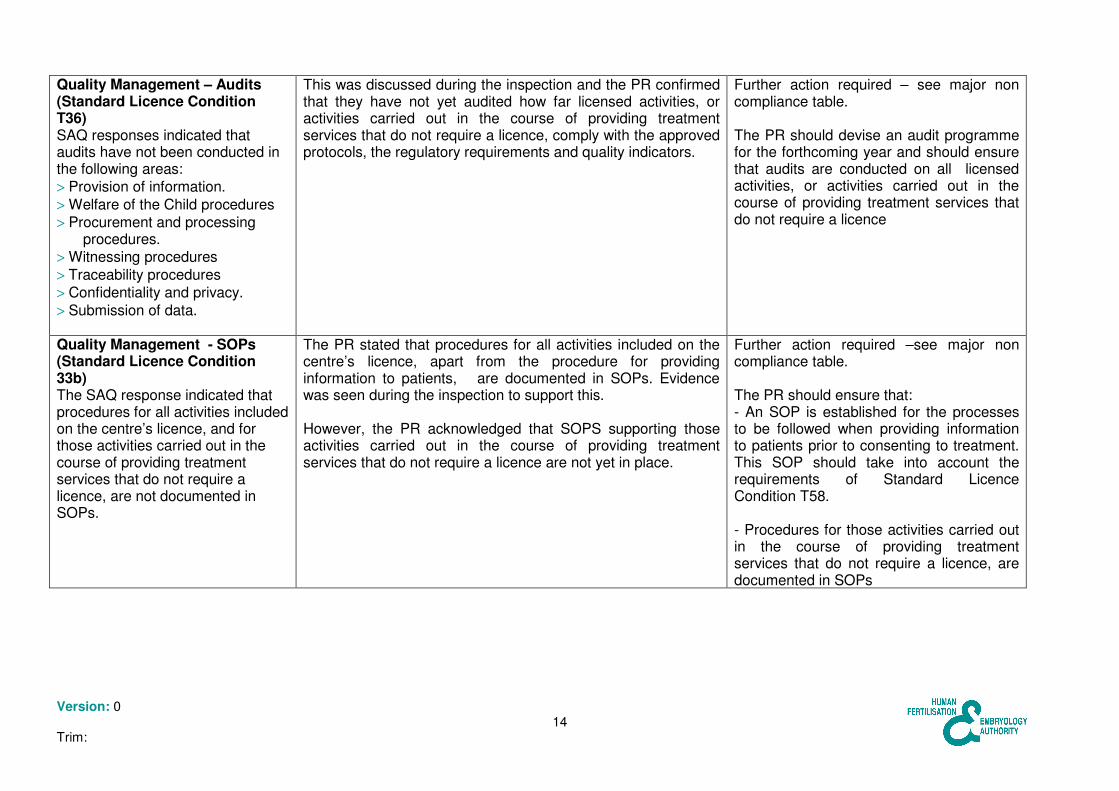
Quality Management – Audits (Standard Licence Condition T36) SAQ responses indicated that audits have not been conducted in the following areas: > Provision of information. > Welfare of the Child procedures > Procurement and processing
procedures. > Witnessing procedures > Traceability procedures > Confidentiality and privacy. > Submission of data.
This was discussed during the inspection and the PR confirmed that they have not yet audited how far licensed activities, or activities carried out in the course of providing treatment services that do not require a licence, comply with the approved protocols, the regulatory requirements and quality indicators.
Further action required – see major non compliance table. The PR should devise an audit programme for the forthcoming year and should ensure that audits are conducted on all licensed activities, or activities carried out in the course of providing treatment services that do not require a licence
Quality Management - SOPs (Standard Licence Condition 33b) The SAQ response indicated that procedures for all activities included on the centre’s licence, and for those activities carried out in the course of providing treatment services that do not require a licence, are not documented in SOPs.
The PR stated that procedures for all activities included on the centre’s licence, apart from the procedure for providing information to patients, are documented in SOPs. Evidence was seen during the inspection to support this. However, the PR acknowledged that SOPS supporting those activities carried out in the course of providing treatment services that do not require a licence are not yet in place.
Further action required –see major non compliance table. The PR should ensure that: - An SOP is established for the processes to be followed when providing information to patients prior to consenting to treatment. This SOP should take into account the requirements of Standard Licence Condition T58. - Procedures for those activities carried out in the course of providing treatment services that do not require a licence, are documented in SOPs
Version: 0 15
Trim:
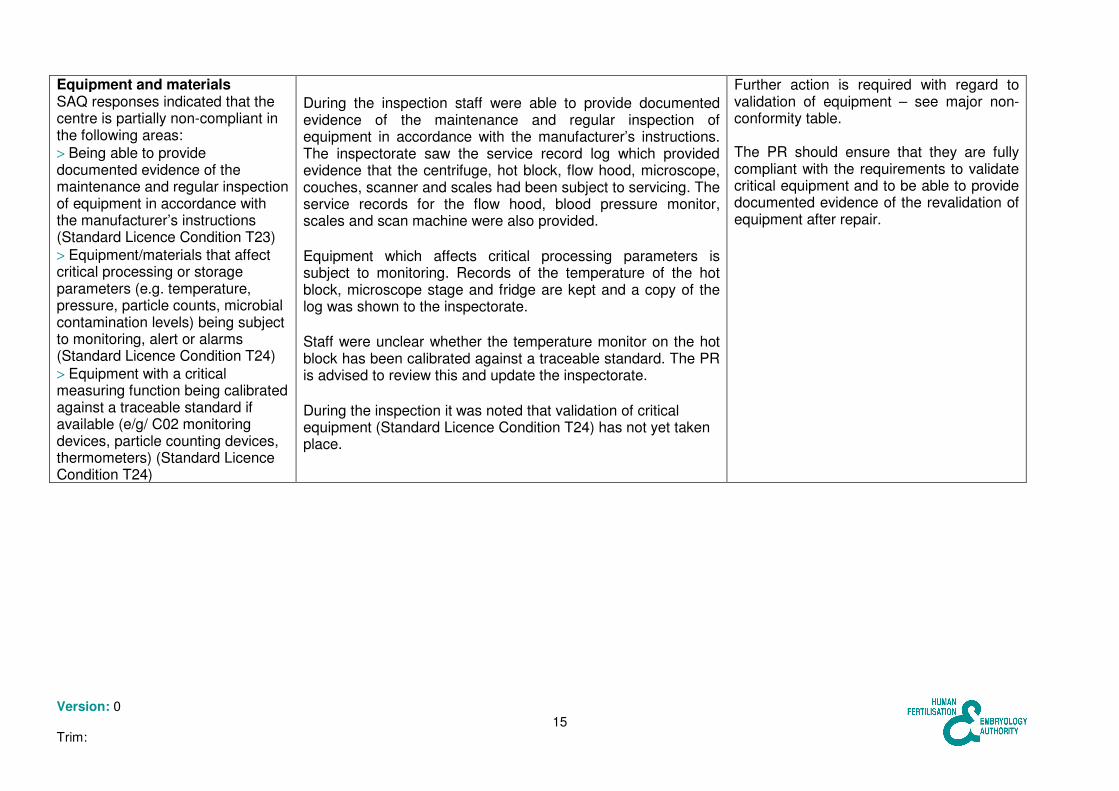
Equipment and materials SAQ responses indicated that the centre is partially non-compliant in the following areas: > Being able to provide documented evidence of the maintenance and regular inspection of equipment in accordance with the manufacturer’s instructions (Standard Licence Condition T23) > Equipment/materials that affect critical processing or storage parameters (e.g. temperature, pressure, particle counts, microbial contamination levels) being subject to monitoring, alert or alarms (Standard Licence Condition T24) > Equipment with a critical measuring function being calibrated against a traceable standard if available (e/g/ C02 monitoring devices, particle counting devices, thermometers) (Standard Licence Condition T24)
During the inspection staff were able to provide documented evidence of the maintenance and regular inspection of equipment in accordance with the manufacturer’s instructions. The inspectorate saw the service record log which provided evidence that the centrifuge, hot block, flow hood, microscope, couches, scanner and scales had been subject to servicing. The service records for the flow hood, blood pressure monitor, scales and scan machine were also provided. Equipment which affects critical processing parameters is subject to monitoring. Records of the temperature of the hot block, microscope stage and fridge are kept and a copy of the log was shown to the inspectorate. Staff were unclear whether the temperature monitor on the hot block has been calibrated against a traceable standard. The PR is advised to review this and update the inspectorate. During the inspection it was noted that validation of critical equipment (Standard Licence Condition T24) has not yet taken place.
Further action is required with regard to validation of equipment – see major non-conformity table. The PR should ensure that they are fully compliant with the requirements to validate critical equipment and to be able to provide documented evidence of the revalidation of equipment after repair.
Version: 0 16
Trim:
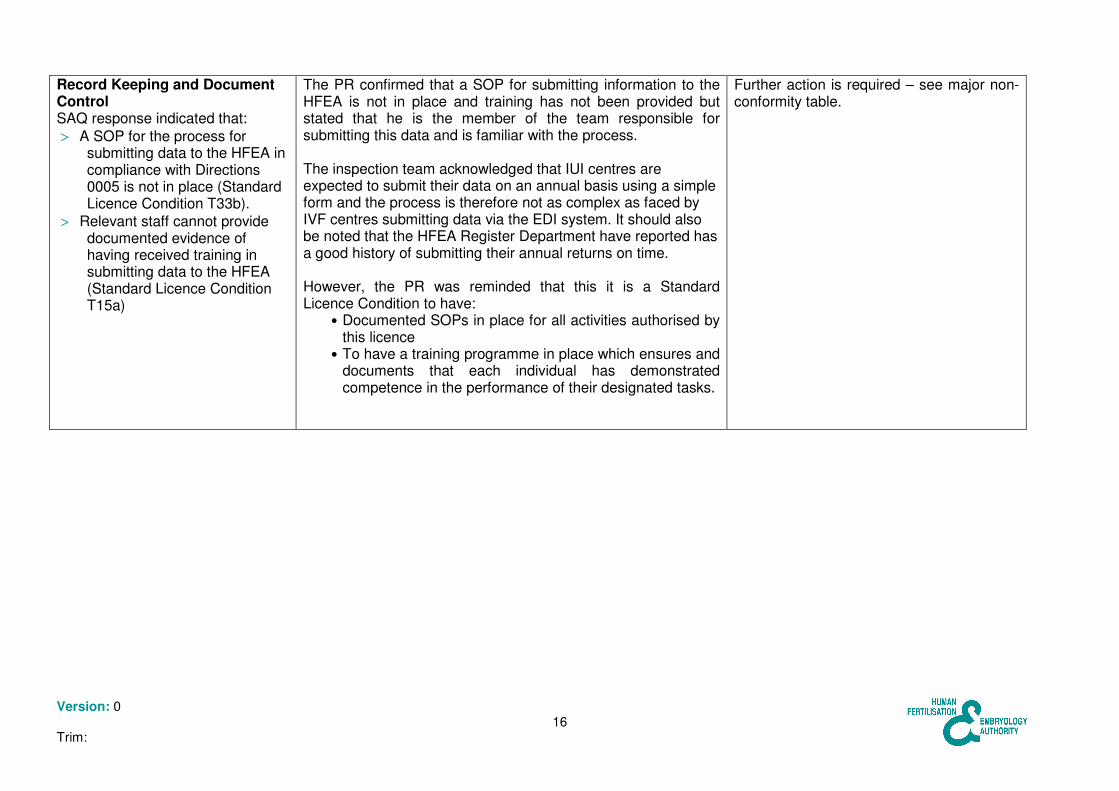
Record Keeping and Document Control SAQ response indicated that: > A SOP for the process for
submitting data to the HFEA in compliance with Directions 0005 is not in place (Standard Licence Condition T33b).
> Relevant staff cannot provide documented evidence of having received training in submitting data to the HFEA (Standard Licence Condition T15a)
The PR confirmed that a SOP for submitting information to the HFEA is not in place and training has not been provided but stated that he is the member of the team responsible for submitting this data and is familiar with the process. The inspection team acknowledged that IUI centres are expected to submit their data on an annual basis using a simple form and the process is therefore not as complex as faced by IVF centres submitting data via the EDI system. It should also be noted that the HFEA Register Department have reported has a good history of submitting their annual returns on time. However, the PR was reminded that this it is a Standard Licence Condition to have:
• Documented SOPs in place for all activities authorised by this licence
• To have a training programme in place which ensures and documents that each individual has demonstrated competence in the performance of their designated tasks.
Further action is required – see major non-conformity table.
Version: 0 17
Trim:
Areas of practice that require the attention of the Person Responsible The section sets out matters which the Inspection Team considers may constitute areas of non compliance. These have been classified into critical, major and others. Each area of non-compliance is referenced to the relevant sections of the Acts, Regulations, Standard Licence Conditions, Directions or the Code of Practice, and the recommended improvement actions require are given as well as the timescales in which these improvements should be carried out.
� Critical area of non compliance A critical are of non compliance is an area of practice which poses a significant direct risk of causing harm to a patient, donor or to an embryo. A critical area of non compliance requires immediate action to be taken by the Person Responsible
Area of practice Reference Action required Timescale for action
PR Response Executive Review

Version: 0 18
Trim:
� Major area of non compliance A major are of non compliance is a non critical are of non compliance:
• which poses an indirect risk to the safety of a patient, donor or to an embryo through the procurement, use, storage or distribution of gametes and embryos, which do not comply with the centre’s licence;
• which indicates a major shortcoming from the statutory requirements; • which indicates a failure of the Person Responsible to carry out his/her legal duties • a combination of several “other” areas of non compliance, none of which on their own may be major but which together
may represent a major area of non compliance. Area of practice Reference Action required Timescale
for action PR Response Executive Review
Version: 0 19
Trim:
Documentation of staff competence Staff were unable to provide documented evidence of the assessment of their competence in: • Carrying out
witnessing • Providing
information to patients consenting to treatment
• Submitting
information to the HFEA
Standard Licence Condition T12: Personnel in the centre must be available in sufficient number and be qualified and competent for the tasks they perform. The competency of the personnel must be evaluated at appropriate intervals. Standard Licence Condition T15a: The training programme must ensure and document that each individual has demonstrated competence in the performance of their designated tasks.
The PR should extend the programme of competence assessments to ensure that all personnel have demonstrated competence in the performance of all their designed tasks.
By 24 June 2010
Witnessing. Clearly this is a critically important part of our routine work. Whilst we do have clear policies as to how the process should work, and our induction and training policy explicitly covers witnessing, we accept that in our current system we do not explicitly record assessment of compentency. We have created a new category for witnessing competency in our assessment framework. This is not an addition to the nursing competencies, as clerical staff can also act as second witnesses on occasions.
The Executive considers this to be a suitable response. Ongoing progress against this requirement will be monitored by the Executive.
Version: 0 20
Trim:
Consent does form part of our current competency framework and all nurses have been assessed and signed off. Our consent policy states that the provision of information is an integral part of the consent process and should not be separate. We have amended the terminology in our assessment framework to ensure that it is clear that it is both provision of information and taking of consent that is being assessed.

Version: 0 21
Trim:
The provision of data to the HFEA is currently the sole responsibility of the PR (as an IUI unit, we make annual returns). Should this change, we will introduce a competency framework
Staff Training - witnessing procedures Staff were unable to provide evidence of their training on witnessing procedures.
Code of Practice Guidance 18.11: Centres should consider who is the most appropriate person to witness clinical and laboratory procedures. This will usually be someone who has completed the centre’s training programme for new staff, and refresher training (as appropriate), to ensure
The PR should ensure that in accordance with Code of Practice Guidance 18.11 all staff members who act as witnesses have completed the centre’s training programme for new staff, and refresher training (as appropriate), to ensure they fully understand the principles of witnessing procedures and follow the centre’s protocols.
Immediately Having sought advice from our licensed neighbours as to how they comply with the condition, we will adopt their system to ensure that evidence is documented.
The Executive considers this to be a suitable response. Ongoing progress against this requirement will be monitored by the Executive.
Version: 0 22
Trim:
they fully understand the principles of witnessing procedures and follow the centre’s protocols. For exceptions to this, refer to paragraphs 18.13 and 18.14 (of the Code of Practice.

Version: 0 23
Trim:
Witnessing Procedures The centre’s witnessing practice is to cross check information on all the sperm preparation tubes and the sperm pot at the beginning of the procedure and not to perform witnessing checks each time the sperm sample is moved between tubes. This is non-contemporaneous witnessing.
Standard Licence Condition T71: Centres must have witnessing protocols in place to double check the identification of samples and the patients or donors to whom they relate at all critical points of the clinical and laboratory process. These checks must be completed and recorded at the time the relevant clinical or laboratory process/procedure takes place. A record must be kept in each patient’s/donor’s medical records. These records must include the name, status and signature of the person performing the activity and the name, status and signature of the person who witnesses the procedure.
The PR should define the critical points of the laboratory process with reference to Code of Practice Guidance18.4 and review the witnessing procedures accordingly. The PR must take action to ensure witnessing is performed contemporaneously in a manner compliant with T71.
Immediately Clarification on these processes is welcome from the inspection team. Our standard operating procedure did specify checks each time the sample was moved between tubes, but owing to the fact we only processed one sample at a time and that as a small unit we often did not have a second staff member immediately available, we changed our procedure to double witnessing all tubes were correctly labelled at the outset. At the last inspection we inferred that this was acceptable. Since the clarification in the latest code of practice, we will change the
The Executive considers this to be a suitable response but ask that the PR submits a copy of the amended laboratory pro forma as evidence of the action taken.

Version: 0 24
Trim:
procedure to call through a staff member to double check contemporaneously, and our laboratory proformas have already been amended to action this.
Active witnessing check The centre’s witnessing process for collecting sperm is not fully compliant with Code of Practice Guidance. The cross-check between identifying information provided by the sperm provider, the records, the laboratory data sheet and sperm receptacle is not an active identification check.
Code of Practice Guidance 18.4b: When collecting eggs or sperm, transferring embryos and carrying out insemination, staff should ask patients and donors to give their own identifying information (full name and date of birth), rather than asking the donor or patient to confirm or reject information read out to them.
It is recommended that the PR ensures that this witnessing step involves active identification of the male partner.
Immediately We do already hold on record photo-ID confirmation of both partners and check this against their record whenever they attend. However the suggested change of asking the male partner to confirm his details (rather than him simply answer "yes") has been implemented. Our proforma has been amended to record this.
The Executive considers this to be a suitable response.
Version: 0 25
Trim:
Witnessing documentation Witnessing documentation within the patient records does not include the name and status of the person conducting each procedure or the name and status of the person who witnesses the procedure. The time of the procedure has not been recorded for all steps of the process
Standard Licence Condition T71: Centres must have witnessing protocols in place to double check the identification of samples and the patients or donors to whom they relate at all critical points of the clinical and laboratory process. These checks must be completed and recorded at the time the relevant clinical or laboratory process/procedure takes place. A record must be kept in each patient’s/donor’s medical records. These records must include the name, status and signature of the person performing the activity and the name, status and signature of the person who witnesses the procedure.
The PR must ensure that witnessing records are kept in accordance with both Standard Licence Condition T71 and Code of Practice Guidance 18.7 and 18.8.
Immediately We had assumed that the status could be cross-checked against the staff file should this be necessary in the future. However it is now included on the proforma, and staff reminded of the importance of ensuring that all the details are completed.
The Executive considers this to be a suitable response but ask that the PR submits a copy of the amended laboratory pro forma as evidence of the action taken.
Version: 0 26
Trim:
Code of Practice Guidance 18.7: When the procedure takes place, a record should be made in the patient or donor notes stating: (a) the procedure (b) the date and time of the procedure (c) the signature of the person doing the procedure, and (d) the signature of the witness. A hard copy of electronic witnessing should be retained

Version: 0 27
Trim:
Witnessing SOP The Centre’s witnessing SOP was reviewed by the inspectorate and through discussion with staff it was found that the SOP did not correctly reflect the witnessing procedures used by staff. The SOP included some steps which are not followed by staff and it also did not remind staff to include a check against patient records at each witnessing step.
Code of Practice Guidance 18.2: Centres should have witnessing protocols relevant to their local systems and conditions, based on HFEA model protocols.
It is recommended that the PR reviews the HFEA model protocols and updates the witnessing SOP to ensure compliance with CoP Guidance 18.2.
Immediately The SoP was due to be updated and revised, and the processes as outlined have been incorporated
The Executive considers this to be a suitable response but ask that the PR submits a copy of the amended SOP as evidence of the action taken.

Version: 0 28
Trim:
Validation of critical equipment The centre is not yet fully compliant with the requirement to validate critical equipment.
Standard Licence Condition T24: All critical equipment and technical devices must be identified and validated, regularly inspected and maintained in accordance with the manufacturer’s instructions.
Critical equipment must be validated in accordance with T24.
By 24 March 2011. The PR should submit to the HFEA a quarterly report on, progress until it is complete.
As an IUI unit, we have little equipment that is genuinely "critical" in comparison to IVF laboratories. The equipment we do have was procured prior to the validation regulations, but is regularly inspected and maintained as outlined in our equipment policy. We are very grateful for the help and advice of the inspection team over this complex area and for the provision of HFEA-validated templates developed by ACE. We will incorporate these into an updated equipment policy.
The Executive considers this to be a suitable response. The Executive will monitor the centre’s compliance with this requirement through review of the quarterly progress reports.
Version: 0 29
Trim:
Audit of activities At inspection it was noted that audits have not yet been conducted on how far licensed activities, or activities carried out in the course of providing treatment services that do not require a licence, comply with the approved protocols, the regulatory requirements and quality indicators. This was an issue at the renewal inspection in March 2008.
Standard Licence Condition T36: Trained and competent persons must audit the activities authorised by this licence, and other activities carried out in the course of providing treatment services that do not require a licence, against compliance with the approved protocols, the regulatory requirements and quality indicators. These audits must be performed in an independent way, at least every two years. Findings and corrective actions must be documented.
The PR must ensure that licensed activities and other activities related to unlicensed treatment services are audited at least every two years. It is recommended that the PR devises an audit programme for the forthcoming year and should ensure that audits are conducted on all licensed activities, or activities carried out in the course of providing treatment services that do not require a licence
By 24 September 2010
We accept that formal, published audit has taken a low priority owing to the clinical workload, but our aim as outlined at the last inspection of starting a programme to capture patient-feedback has been successful. Our department is working towards implementing a rolling audit using clinical dashboards, and we will ensure that those aspects required by the regulations are included within this framework
The Executive considers this to be a suitable response. Progress against this requirement will be further monitored in September 2010.
Version: 0 30
Trim:
We have succeeded in running a clincal dashboard in maternity services that complies with CNST requirements, and will now expand this to incorporate gynaecology services. Although this does not preclude additional, major audit projects, we feel that the dashboard philosophy of a continuous, rolling audit is a robust way of capturing data and identifying trends.

Version: 0 31
Trim:
Documented SOPs The procedure for providing information to patients and the procedure for submitting information to the HFEA are not documented in SOPs. The PR also acknowledged that SOPS supporting those activities carried out in the course of providing treatment services that do not require a licence are not yet in place.
Standard Licence Condition 33b: The following documentation must form part of the quality management system: a. a quality manual b. standard operating procedures (SOPs) for all activities authorised by this licence and other activities carried out in the course of providing treatment services that do not require a licence c. guidelines d. training and reference manuals, and e. reporting forms.
The PR should ensure that: • An SOP is established
for the processes to be followed when providing information to patients prior to consenting to treatment
• An SOP is established
for submitting information to the HFEA in compliance with General Direction 0005.
• Procedures for those
activities carried out in the course of providing treatment services that do not require a licence, are documented in SOPs.
SOPs for providing information to patients and submitting information to the HFEA to be documented by 24 May 2010. SOPs for activities carried out in the course of providing treatment services that do not require a licence to be in place by 24 September 2010.
We apologise for not being clear over the policies for provision of information to patients. We already have guidelines regarding the process for developing patient information in our document control policy, and in what information needs to be given to patients in our "superovulation and intrauterine insemination (SO/IUI) – clinical guidelines". This will be clarified and the provision of written information explicitly recorded on the updated treatment checklist.
The Executive is satisfied with the response provided regarding an SOP for provision of information to patients and submission of information to the HFEA. The PR should ensure that all procedures conducted for patients attending the Cornwall Centre for Reproductive Medicine for treatment, licensed or not, are documented in SOPs. Ongoing progress against this requirement will be further monitored by the Executive in September 2010.

Version: 0 32
Trim:
The HFEA data is submitted by the PR as we only provide IUI services, but the procedure will be added to our document control policy.
We already have guidelines for many of our departmental non-licensed work, but our general philosophy is to follow NICE and RCOG guidelines and to provide individualised care. We are part of a large department that provides a wide range of obstetric and gynaecological services, and it would not be realistic for us to provide SoPs for all clinical activities provided by the department
Version: 0 33
Trim:
- for example we have just completed an integrated care pathway for management of dysfunctional bladder that has taken three years to develop with our primary care and PCT colleagues. Nevertheless we support the development of quality integrated care pathways but see this as an ongoing process.
Establishing Quality Indicators. Quality indicators for all licensed activities and for activities carried out in the course of providing treatment services that do not require a licence, have not yet been established.
Standard Licence Condition T35: Required standards of quality and safety, in the form of quality indicators for all activities authorised by this licence and other activities carried out in the course of providing treatment services that do not require a licence, must be established.
Quality indicators must be established for all activities authorised by this licence and other activities carried out in the course of providing treatment services that do not require a licence.
By 24 September 2010
We have defined the parameters needed and will include these within the clincal dashboard as descirbed above
The Executive considers this to be a suitable response. Progress against this requirement will be further monitored in September 2010.

Version: 0 34
Trim:
� Other areas of practice that requires improvement Areas of practice that requires improvement is any area of practice, which cannot be classified as either a critical or major area of non compliance, but which indicates a departure from good practice.
Area of practice Reference Action required Timescale for action
PR Response Executive Review
Document control It was noted during the inspection that the centre’s Quality Manual and documented SOPs had not been subject to 12 monthly review.
Code of Practice Guidance 31.6 Documents should be reviewed, revised and reapproved at a frequency that ensures they remain fit for purpose. The maximum interval between reviews should be 12 months.
It is recommended that the PR identifies all the documents which are overdue a review and then starts the process of review, revision and re-approval as per Code of Practice Guidance 31.6.
Update to be provided to the Executive on the documents requiring review by 24 June 2010. Further progress to be monitored by 24 March 2011.
Although the documents were reviewed and did not need revision, this was not recorded nor was a new review date created. We will incorporate this review into our management meetings which are now minuted in order to ensure the process is recurring and tracked.
The Executive notes that the PR has confirmed that the documents were reviewed but due to an administrative oversight the document control information had not been updated. The PR is asked to confirm that this information has now been updated. The Executive are satisfied to see that a process for ensuring that document review is ongoing has now been introduced.
Version: 0 35
Trim:
Costed treatment plans The inspectorate did not see evidence to show that patients are being provided with personalised costed treatment plans.
Code of Practice Guidance 4.3: Before treatment, storage or both are offered, the centre should also give the person seeking treatment or storage, and their partner (if applicable) a personalised costed treatment plan. The plan should detail the main elements of the treatment proposed (including investigations and tests), the cost of that treatment and any possible changes to the plan, including their cost implications. The centre should give patients the opportunity to discuss the plan before treatment begins.
The PR should ensure compliance with Code of Practice guidance 4.3. It is also recommended that evidence is kept to show that this information is being provided to patients as this will assist future procedural audits.
By 24 June 2010
All patients are provided with written details of the costs, including for services which may become necessary (e.g. cryopreservation). Although this has always been recorded on our checklist for IVF patients, we have amended our IUI checklist to ensure we confirm we have given costings to the patients. We will also update our training policy to include this.
The Executive considers this to be a suitable response.

Version: 0 36
Trim:
Calibration of critical measuring equipment Staff were unclear whether the temperature monitor on the hot block has been calibrated against a traceable standard.
Standard Licence Condition T24: All critical equipment and technical devices must be identified and validated, regularly inspected and maintained in accordance with the manufacturer’s instructions.
The PR is advised to review whether or not the hot block, which has a critical measuring function, has been calibrated against a traceable standard. If the equipment has not been calibrated the PR should ensure that this takes place in accordance with Standard Licence Condition T24.
24 June 2010
The PR confirms it was calibrated when first commissioned. We will ensure that calibration is also recorded within the service plan.
The Executive considers this to be a suitable response but remind the PR to ensure that the equipment is recalibrated at the intervals recommended by the manufacturer.
Where equipment or materials affect critical processing or storage parameters (eg, temperature, pressure, particle counts, microbial contamination levels) they must be identified and be the subject of appropriate monitoring, alerts, alarms and corrective action, as required, to detect malfunctions and defects, and to ensure that the critical parameters are maintained within acceptable limits at all times.

Version: 0 37
Trim:
All equipment with critical measuring function must be calibrated against a traceable standard if available.
Additional Information from the Person Responsible This was our first unnannouced inspection, and clearly there were concerns that we could not provide the inspection team the time and attention they deserved as there was little clinical activity scheduled that day and staff were rostered elsewhere within the department, with one clinician off-site and the other on-call for obstetrics. We thank the team for their patience and understanding. We were delighted by the feedback they gave us, especially the encouragement over the measures we'd introduced since the last inspection, and were pleased to be able to show them the first formal patient responses to our rolling evaluation and feedback programme. We found the process useful and are grateful for the advice and resources that the team provided. We have already implemented most of the recommendations, and are confident we can comply with the remainder within the required timescales. Our only concern is that as we are part of a large department, the requirement to have SOPs for activities that do not require a licence could in theory be applied to any part of our service. In general we operate a philosophy of complying with NICE and RCOG guidelines and of individualising care for patients, and whilst we encourage the development of integrated care pathways to ensure best practice both in the hospital and in primary care, these pathways do not necessarily translate well to SOPs and the development of good quality pathways cannot be rushed.