-
8/9/2019 UltrasoundTraumaCh02 Fast Exam
1/23
15
The FAST ExamRobert A. Jones, DO, RDMS, FACEP, and Robert D.
Welch, MD, FACEP
C H A P T E R 2
Evaluation of patients with thoracoabdominal trauma is often
a
diagnostic challenge for emergency physicians and trauma
surgeons, and
is made more difficult by the insensitivity of the physical
examination
for detecting major internal injuries. Studies have shown that
20% to
43% of patients with significant abdominal injuries may
initially have a
normal physical examination of the abdomen. Even patients
with
intraperitoneal hemorrhage can be alert and asymptomatic on
arrival. A
patient with a hemopericardium, hemothorax, or hemoperitoneum
can
deteriorate quickly despite a benign initial presentation.
Because of the
lack of reliability of the physical examination, physicians have
come to
depend on ancillary tests to detect potentially life-threatening
injuries.
-
8/9/2019 UltrasoundTraumaCh02 Fast Exam
2/23
-
8/9/2019 UltrasoundTraumaCh02 Fast Exam
3/23
17
The FAST Exam
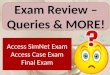
Figure 2-1C
A, Fluid in Morisons pouch. Blood or fluid in this pouch appears
as an anechoic (black) stripe between the liver and the right
kidney. Clotspresent within the blood may be echogenic (white).This
is the most dependent region of the upper abdomen. This region is
also referredto as the hepatorenal pouch or hepatorenal space. B,C,
Preferential locations for blood to accumulate. B, Locations on a
longitudinal view.C, Locations on an anteroposterior view of the
abdomen. D, Intraperitoneal free fluid. The pattern of free fluid
movement within theabdominal cavity is shown. E, Views of the FAST
exam. The FAST exam consists of pericardial (cardiac), perihepatic
(RUQ), perisplenic(LUQ), and pelvic views. Most physicians perform
the RUQ view first in patients with blunt abdominal trauma and the
cardiac view first inpatients with penetrating trauma to the chest.
(B,C, Reprinted with permission from Sanders RC. Clinical
Sonography: A Practical Guide.2nd ed. Boston, Mass: Little, Brown;
1991:257. E, Courtesy of William Mallon, MD.)
Figure 2-1B
Figure 2-1A
Figure 2-1D
Figure 2-1E
-
8/9/2019 UltrasoundTraumaCh02 Fast Exam
4/23
-
8/9/2019 UltrasoundTraumaCh02 Fast Exam
5/23
Sonographic Findings
Clinical findings associated with hemopericardium are
nonspecific and insensitive.
Even with pericardial tamponade, Becks triad and pulsus
paradoxus are not
consistently present. Hemopericardium is usually recognized
clinically only after
deterioration has occurred. Cardiac ultrasonography is sensitive
for detecting even
small amounts of fluid in the pericardial sac and allows for
early recognition at the
bedside. Early recognition of cardiac injuries leads to
immediate interventions that
decrease morbidity and mortality.20 Several studies have shown
that hemopericardium
can be detected accurately by emergency physicians and trauma
surgeons with limited
ultrasonography training.21,22
The subcostal window provides a four-chamber view of the heart
(Figure 2-3). A
small portion of the liver is seen closest to the probe, with
the heart behind it. The
hyperechoic pericardium is seen surrounding the heart. Normally,
there is a small
amount of fluid between the parietal and visceral pericardium.
This fluid is usually
not visualized; however, in some healthy patients, a small
amount of fluid can be seen
in the dependent aspect of the heart, so clinical correlation is
essential. If fluid is
present in a nondependent aspect of the heart, it should be
considered abnormal.The presence of pericardial fluid is
demonstrated by separation of the visceral and
parietal pericardial layers (Figure 2-4A). Acutely, blood will
appear anechoic (black);
however, echoes may be present if clotting has occurred (Figure
2-4B). When looking
at a pericardial window, the pericardium should be identified;
there should be only
one hyperechoic line surrounding the heart. If two lines are
seen surrounding the heart
and there is no evidence of anechoic fluid, then an isoechoic
fluid collection is
possible. The presence of clotting can result in fluid
collections that are isoechoic to
the surrounding cardiac muscle (Figure 2-4C). False-negative
results have been
attributed to this in the literature.21
19
The FAST Exam
Figure 2-2
Probe placement for subcostal pericardial view. The
probeindicator is directed toward the patients right side (9
oclock); thebeam is directed toward the left shoulder. The arrow
indicates thedirection of the probe indicator. Imaging may be
enhanced byhaving the patient take a deep breath and hold it.
Figure 2-3
Normal subcostal pericardial view. RV, right ventricle; LV,
leftventricle; RA, right atrium; LA, left atrium. A portion of
liver will bevisualized in the near field. (Courtesy of Dr. Jones
and Dr.Welch.)
-
8/9/2019 UltrasoundTraumaCh02 Fast Exam
6/23
Ultrasonography in Trauma: The FAST Exam
20
Pericardial fluid can be mistaken for intraperitoneal or pleural
fluid. Fluid in the
subdiaphragmatic space between the diaphragm and the liver can
be visualized with
this window; therefore, it is important to make certain the
fluid is located between the
two pericardial layers (Figure 2-5). Even though the pleural
window is limited in this
view, a large hemothorax can be mistaken for hemopericardium22
(Figure 2-6). It is
also possible for a large hemothorax to obscure a small
pericardial fluid collection.22
In such cases, repeat studies should always be obtained after
tube thoracostomy
drainage.
Pericardial tamponade can be diagnosed based on the presence of
a circumferential
fluid collection with diastolic collapse of the right atrium or
ventricle seen on
real-time scanning (Figure 2-7). Patients with severe pulmonary
hypertension can
demonstrate clinical cardiac tamponade without right-sided
chamber collapse.
Figure 2-4CA, Small amount of pericardial fluid. This subcostal
(pericardial)view demonstrates a small amount of anechoic (black)
fluid in thepericardial space. B, Large amount of pericardial blood
with clots.This subcostal (pericardial) view demonstrates a large
amount ofblood in the pericardial space, and the right ventricle
iscompressed.The echoes (white) that are seen within the darkfluid
represent blood clots. On real-time imaging, there wasdiastolic
collapse of the right ventricle consistent with
pericardialtamponade. C, Stab wound to the chest with a large
amount ofpericardial clot. There is a large amount of clotted blood
presentin the pericardial space that is isoechoic to the
surroundingcardiac muscle.There also is some anechoic (black) fluid
presentin the pericardial space. (A,B, Courtesy of Dr. Jones and
Dr.Welch. C, Courtesy of Dr. Mandavia.)
Figure 2-4A
Figure 2-4B
-
8/9/2019 UltrasoundTraumaCh02 Fast Exam
7/23
-
8/9/2019 UltrasoundTraumaCh02 Fast Exam
8/23
Ultrasonography in Trauma: The FAST Exam
22
in a cephalad direction if visualization of the diaphragm and
pleural space is not
adequate. To visualize the paracolic gutter, the probe should be
oriented in a coronal
plane and moved caudally until the lower pole of the kidney is
seen (Figure 2-9).
The right subcostal technique is obtained with the probe at the
right infracostal
margin, lateral to the midclavicular line (Figure 2-10). Having
the patient take a deep
breath and hold it or push out the abdomen can help bring
structures below thecostal margin into view. This technique
requires significant patient cooperation
because respirations affect visualization. The presence of gas
in the hepatic flexure of
the colon may also limit the success of this technique.
Figure 2-9
Probe placement for perihepatic (RUQ) coronal view. This view
isused to visualize Morisons pouch and the right kidney. The
probeis moved caudally to image the inferior pole of the right
kidneyand the right paracolic gutter.
Figure 2-10
Probe placement for right subcostal view. Occasionally, it
isnecessary to obtain additional perpendicular views of the RUQ
toclarify findings present on prior RUQ views. This view requires
apatient to take a deep breath and hold it or push out theabdomen
to visualize the liver below the costal margin.
Figure 2-8
Probe placement for perihepatic or RUQ view
(intercostalapproach). This provides excellent visualization of the
diaphragm,liver, and Morisons pouch. A slight posterior angulation
of theprobe reduces the amount of rib shadowing that is obtained
byimaging directly through an intercostal space. The probe
indicator
is directed toward the patients posterior axilla. The
arrowindicates the direction of the probe indicator.
-
8/9/2019 UltrasoundTraumaCh02 Fast Exam
9/23
23
The FAST Exam
Sonographic Findings
The perihepatic view provides fractional views of the liver and
right kidney and
allows visualization of fluid in Morisons pouch, the subphrenic
space, the right
pleural space, and the retroperitoneum (Figure 2-11A-D).
Hemoperitoneum appears as
an anechoic area in Morisons pouch or in the subphrenic space
(Figure 2-12A-D).
Fluid in adjacent structures such as the gallbladder, hepatic
flexure of the colon, and
duodenum can be mistaken for intraperitoneal fluid.23 To prevent
this error, the user
must identify peristalsis during real-time scanning and
demonstrate an echogenic
border surrounding the fluid. In addition, free fluid tends to
form spicules or
triangulate as it follows the path of least resistance, whereas
fluid within organs or
vessels has a rounded or cylindrical appearance (Figure
2-13A-C). Morisons pouch is
a pooling site for excess pelvic fluid and perisplenic fluid;
thus, it is particularly
important to adequately visualize this region.24-27 Placing the
probe in a coronal plane
Figure 2-11A Figure 2-11C
Figure 2-11B Figure 2-11D
A-D, Negative studies of RUQ. Normal perihepatic views
demonstrating diaphragm, liver, and kidney (left to right). The
renal capsuleappears as an echogenic line surrounding the
kidney.The renal cortex is slightly less echogenic than the
neighboring liver, and the renalpyramids appear as hypoechoic
regions that point toward the center of the kidney.The renal sinus
is a central echogenic portion of thekidney. There is no anechoic
(black) stripe visualized above the outer white border of the
kidney. (A, Courtesy of Dr. Jones and Dr. Welch.B, Courtesy of Dr.
Reardon.)
-
8/9/2019 UltrasoundTraumaCh02 Fast Exam
10/23
Ultrasonography in Trauma: The FAST Exam
24
and sliding it caudally until the inferior pole of the kidney is
seen will allow detection
of both supramesocolic and inframesocolic fluid around the tip
of the liver that has
not yet reached Morisons pouch (Figure 2-14A,B). Moving the
probe in a cephalad
direction permits visualization of subphrenic space, a common
site of fluid
accumulation.
Pleural fluid can be accurately detected using this limited
view. Studies have shownsensitivities in the range of 96.2% to
97.5% and specificities in the range of 99.7% to
100% for the detection of hemothoraces using ultrasonography.4,5
The patient should
be in the supine position, although reverse Trendelenburg
positioning intuitively
should improve detection. Free pleural fluid is represented by
the presence of an
anechoic area cephalad to the hyperechoic diaphragm (Figure
2-15A,B). Clearly
identifying the diaphragm prevents misdiagnosing a subphrenic
fluid collection or
other intraperitoneal fluid as a pleural fluid collection
(Figures 2-16 and 2-17). It has
been shown that, although supine and upright chest radiographs
require a minimum of
175 mL and 50 to 100 mL of pleural fluid, respectively, for
detection, ultrasonography
can detect a minimum of 20 mL of pleural fluid. 4 The
significance of a hemothorax
Figure 2-12A Figure 2-12C
Figure 2-12B Figure 2-12D
Perihepatic (RUQ) views with fluid in Morisons pouch. B,C, The
tip of the liver is free floating. (A,D, Courtesy of Dr. Jones and
Dr. Welch.B, Courtesy of Dr. Kendall. C, Courtesy of Dr.
Reardon.)
-
8/9/2019 UltrasoundTraumaCh02 Fast Exam
11/23
25
The FAST Exam
Figure 2-13A
Figure 2-14A Figure 2-14B
A, Longitudinal view (snowboarding injury with pelvic bleeding).
B, Transverse view (motor vehicle crash with splenic laceration) of
thelower pole of liver and kidney. Blood is seen beside the
inferior pole of the liver and kidney that has not yet reached
Morisons pouch.
Figure 2-13B
Figure 2-13C
Perihepatic view with gallbladder visualized. A, Longitudinal
viewof a normal gallbladder. Note the echogenic wall surrounding
thegallbladder. B, Perihepatic view of 25-year-old patient involved
ina high-speed motor vehicle crash.This transverse view of
thegallbladder demonstrates free intraperitoneal blood above
the
gallbladder. C, Free intraperitoneal blood tends to form
trianglesor spicules, whereas fluid in organs or vessels is round,
oval, ortubular.There is free blood present to the right of the
gallbladder.(A, Courtesy of Dr. Stahmer. B, Courtesy of Dr. Jones
and Dr.Welch.)
-
8/9/2019 UltrasoundTraumaCh02 Fast Exam
12/23
Ultrasonography in Trauma: The FAST Exam
26
detected with ultrasonography and not visualized by plain
radiography is not known;
for this reason, the detection of hemothorax is not a primary
goal of FAST. Future
studies should examine the sonographic appearances of pulmonary
contusions,
because a false-positive study for hemothorax has been reported
in a patient with a
pulmonary contusion without hemothorax.5 When chest radiography
is unavailable or
delayed, ultrasonography should be used.
Perisplenic Window (Left Upper Quadrant)
Technique
The perisplenic view is obtained using an intercostal approach;
it is technically
more difficult for the novice sonographer than the perihepatic
view. With practice,
however, the user can obtain quality images in most cases. The
intercostal approach is
similar to that of the perihepatic view, with a few exceptions.
The probe should be
Figure 2-15B
Perihepatic view with fluid noted in the pleural space. A, Fluid
inthe pleural space makes a V shape on the longitudinal
view,whereas subdiaphragmatic fluid has a crescent shape. B,
Thehemothorax is compressing the adjacent lung tissue, and the
tipof the atelectatic lung is clearly visible. (A, Courtesy of Dr.
Jonesand Dr. Welch.)
Figure 2-16
Perihepatic view with a large amount of fluid noted in
thesubdiaphragmatic space. (Courtesy of Dr. Kendall.)
Figure 2-17
Perihepatic view with echogenic liver contusion. The
liverhematoma has a heterogeneous appearance, and there is
freeblood to the right of it between the liver and kidney.
(Courtesy ofDr. Jones and Dr. Welch.)
Figure 2-15A
-
8/9/2019 UltrasoundTraumaCh02 Fast Exam
13/23
placed in the intercostal space between ribs 9 and 10 or 10 and
11. The bulk of the
spleen is located more dorsal than the liver and the organ is
smaller; thus, the probe
placement must be more posterior. In a coronal plane, the probe
is placed near the
posterior axillary line with the probe indicator directed
cephalad (Figure 2-18A). To
place the probe in the proper plane, it is occasionally
necessary to either turn the
patient slightly on the right side (this can be done only if it
will cause no further
injury to the patient) or place the patient near the edge of the
stretcher. The probe can
be slightly rotated clockwise to reduce rib shadowing (image
beam parallel to ribs),
thus obtaining a better longitudinal view of the spleen and
kidney (Figure 2-18B). The
beam is then swept anterior and posterior, as well as cephalad
and caudal, to visualize
the regions of interest.
With more experience, the user can predict, with some certainty,
the best probe
position based on patient body habitus. In most patients, a
depth of 12 to 15 cm is
appropriate for this examination. More depth is useful if
finding the spleen is difficult
(more depth translates into a larger field of view), and is
required in very large
patients. Less depth helps magnify regions of interest. Asking
the patient to slowly
take a deep breath helps bring the spleen into view. A
significant amount of pressure
on the probe might be required to obtain a quality image in an
obese patient and, as a
result, may not be tolerated if injuries are present in that
region.
Ideally, portions of the left hemidiaphragm, spleen, and left
kidney appear in a
single view (Figure 2-19). Occasionally, the sonographer cannot
adequately visualize
the diaphragm (Figure 2-20). If this occurs, two (or more)
separate views are needed.
The patient may take a deep breath, or the probe may be moved up
one intercostal
space, or the beam may be directed more cephalad to visualize
the spleen and left
hemidiaphragm. Moving the probe down one intercostal space and
directing the beam
more caudally might be required to visualize the spleen and
lower pole of the left
kidney (Figure 2-21A-C). If these structures are not visualized,
the study must beconsidered incomplete. The user must keep in mind
that the subphrenic space is the
most frequent site for fluid accumulation in this region;
failure to visualize the
diaphragm will result in a significant number of false-negative
studies.
27
The FAST Exam
Figure 2-18A Figure 2-18B
Probe placement for perisplenic views. Arrow indicates the
direction of the probe indicator. A, Coronal LUQ view. B, LUQ
intercostalapproach. The intercostal approach may provide a clearer
image with less rib shadowing than the coronal view.
-
8/9/2019 UltrasoundTraumaCh02 Fast Exam
14/23
Ultrasonography in Trauma: The FAST Exam
28
Figure 2-21C
Perisplenic views showing diaphragm and splenorenal
fossa.Multiple views of the LUQ often must be obtained to view
thediaphragm, spleen, and the entire kidney. A,B,
Subdiaphragmaticfluid/blood is seen in these views.The left kidney
is poorlydepicted in A but nicely imaged in B. C, A small stripe of
blood isvisualized in the splenorenal space.The diaphragm is not
seen.(Courtesy of Dr. Kendall.)
Figure 2-21AFigure 2-19
Normal perisplenic (LUQ) view with the structures as
labeled.(Courtesy of Dr. Jones and Dr. Welch.)
Figure 2-20
Perisplenic view showing spleen and kidney. The diaphragm isnot
well visualized in this view.There is fluid/blood seen at the tipof
the spleen. (Courtesy of Dr. Kendall.)
Figure 2-21B
-
8/9/2019 UltrasoundTraumaCh02 Fast Exam
15/23
29
The FAST Exam
Sonographic Findings
The perisplenic view provides fractional views of the spleen,
left kidney,
retroperitoneal region, and left pleural space (Figure 2-22).
Hemoperitoneum appears
as an anechoic area in the subphrenic space or in the
splenorenal fossa. Fluid in this
region preferentially goes to the subphrenic space, with
overflow going to the
splenorenal fossa and across the midline to Morisons pouch13
(Figure 2-23A-G). Onestudy found that, of 69 patients with isolated
spleen injuries, only 33.3% had a
positive perisplenic view, whereas 77.3% had a positive
perihepatic view.28 The
diaphragm must be clearly identified so that a pleural fluid
collection is not mistaken
for a subphrenic collection. Once blood coagulates, the
sonographic appearance is that
of varying echogenicity. With time, the clots can become
isoechoic and difficult to
differentiate from solid organs. Fluid in adjacent structures
such as the stomach or
splenic flexure of the colon can be mistaken for intraperitoneal
fluid.23 Careful
inspection for the presence of peristalsis during real-time
scanning and recognition of
the appearance of fluid in the gastrointestinal tract is crucial
to prevent this error.23
Pleural fluid (hemothorax) in the left pleural space can be
accurately detected on
this limited view as an anechoic region cephalad to the left
hemidiaphragm (Figure
2-24A-C). Clearly identifying the diaphragm prevents
misdiagnosing a subphrenic
fluid collection as a pleural fluid collection; this is
described in more detail in
Chapters 3 and 6.
Ultrasonography is not as sensitive as CT in the detection of
spleen injuries, but the
fractional view of the spleen seen on the perisplenic window
might provide
information about parenchymal injury (Figure 2-25). Because
intraparenchymal
hemorrhage can appear similar to the surrounding normal tissue,
it can be easily
missed.27, 28 A complete description of solid organ injuries is
provided in Chapter 5.
Figure 2-22
Normal perisplenic view. There is a mirror image of
spleenevident cephalad to the diaphragm (mirror artifact).
(Courtesy ofDr. Reardon.)
-
8/9/2019 UltrasoundTraumaCh02 Fast Exam
16/23
Ultrasonography in Trauma: The FAST Exam
30
Figure 2-23A Figure 2-23D
Figure 2-23F
Figure 2-23B Figure 2-23E
Figure 2-23G
A-G, Perisplenic views (LUQ) with freeintraperitoneal blood. In
contrast to theRUQ, blood appears most commonly inthe
subdiaphragmatic area and lessfrequently in the splenorenal
fossa.(A-D,F, Courtesy of Dr. Jones and Dr.Welch.)
Figure 2-23C
-
8/9/2019 UltrasoundTraumaCh02 Fast Exam
17/23
31
The FAST Exam
Figure 2-24C
Perisplenic views of left pleural fluid/hemothorax. A,B, A
largeamount of anechoic fluid in the chest. C, Patient with a
stabwound to the left chest that displays free blood and
echogenicclot within the hemothorax. (Courtesy of Dr. Jones and
Dr.Welch.)
Figure 2-24A
Figure 2-24B
Figure 2-25
Perisplenic view of a 19-year-old man who was assaulted with
abaseball bat. Note the lack of homogeneity of this injured
spleenwith a small stripe of free blood in the subdiaphragmatic
space.(Courtesy of Dr. Jones and Dr. Welch.)
-
8/9/2019 UltrasoundTraumaCh02 Fast Exam
18/23
Ultrasonography in Trauma: The FAST Exam
32
Pelvic Window
Technique
The pelvic view is best accomplished when the patients bladder
is filled. For this
reason, the FAST exam should be completed before Foley catheter
placement or
spontaneous bladder emptying. If a catheter is already in place,
retrograde filling with
saline can create a sonographic window (but this is often
impractical during a
resuscitation). Another option is to clamp the catheter long
enough to allow normal
bladder filling. This is performed most frequently when repeat
scans are done or when
a patient has been transferred from another facility. The goal
of this view is to detect
pelvic fluid (hemoperitoneum) in the most dependent part of the
peritoneum.
The pelvic view can be obtained in either a longitudinal or
transverse plane.
Although Rozycki et al29 recommend only a transverse view, most
recommend both
the transverse and longitudinal views as being necessary for
optimal sensitivity.30 To
obtain the longitudinal view, the probe is placed on the
patients abdomen in the
midline just above the pubic symphysis with the probe indicator
directed toward the
patients head (Figure 2-26). The probe can be angled in a
posteroinferior direction to
obtain better visualization of the pelvic structures. The
transverse view is obtained byplacing the probe in the midline just
above the pubic symphysis with the probe
indicator directed toward the patients right (Figure 2-27).
It has been noted that, in nontrauma patients, an overdistended
bladder may
obscure free pelvic fluid. Some urine is needed in the bladder
to create an acoustic
window, but a very large bladder can displace fluid from the
pouch of Douglas
(cul-de-sac) in females and cause a false-negative study.31 If
the bladder is noted to be
overdistended on the original scan, the bladder should be
partially drained with a
Foley catheter and the pelvis rescanned. Further study is needed
to determine if a
repeat partial void study increases sensitivity in injured
patients.
Figure 2-26
Probe placement for longitudinal pelvic view. Arrow indicates
thedirection of the probe indicator.
Figure 2-27
Probe placement for transverse pelvic view. Arrow indicates
thedirection of the probe indicator.
-
8/9/2019 UltrasoundTraumaCh02 Fast Exam
19/23
33
The FAST Exam
Figure 2-28C
Longitudinal pelvic views (female). A, Normal longitudinal
view.B,C, Longitudinal views with anechoic fluid/blood noted in
thepouch of Douglas. (B,C, Courtesy of Dr. Mandavia.)
Figure 2-28A
Figure 2-28B
Sonographic Findings
In a female patient, fluid appears in the pouch of Douglas just
posterior to the
uterus, with overflow fluid extending around the uterus (Figures
2-28A-C and
2-29A,B). A small amount of fluid may be present as a normal
finding in
premenopausal females, and clinical correlation is essential.
Although not a primary
indication of the FAST exam, the uterus should be observed for
the presence of anintrauterine pregnancy.
In a male patient, fluid appears in the rectovesicular pouch or
cephalad to the
bladder (Figures 2-30A-E and 2-31A,B). The seminal vesicles are
paired structures
that appear hypoechoic and lie posterior to the bladder; they
can easily be confused
with free intraperitoneal fluid23 (Figures 2-32 and 2-33). They
can be distinguished
from free fluid based on their appearance between the bladder
and prostate and by the
fact that, on the longitudinal view, the seminal vesicles taper
off in the cephalad
direction and do not extend beyond the bladder, in contrast to
free intraperitoneal
fluid.
-
8/9/2019 UltrasoundTraumaCh02 Fast Exam
20/23
Ultrasonography in Trauma: The FAST Exam
34
SummaryThis chapter summarizes the techniques and the
sonographic findings of the basic
FAST exam. The chapters that follow address clinical
applications of the FAST exam,
specific organ injuries, pitfalls, and additional applications
and provide a review of the
literature and issues regarding training and credentialing.
Figure 2-29A Figure 2-29B
Transverse pelvic views (female). A, Normal transverse view. B,
Transverse view with anechoic fluid/blood noted in the pouch of
Douglas.(Courtesy of Dr. Mandavia.)
-
8/9/2019 UltrasoundTraumaCh02 Fast Exam
21/23
35
The FAST Exam
Figure 2-30A
Figure 2-30B
Figure 2-30C
Figure 2-30D
Figure 2-30E
Longitudinal pelvic views (male) with large amount of
anechoicfluid/blood cephalad to bladder. Loops of bowel are
nicelyvisualized in A,D,E. (A,C, Courtesy of Dr. Jones and Dr.
Welch.D, Courtesy of Dr. Reardon.)
-
8/9/2019 UltrasoundTraumaCh02 Fast Exam
22/23
Ultrasonography in Trauma: The FAST Exam
36
Figure 2-31BTransverse pelvic views (male). A, Normal transverse
view of thepelvis demonstrating bladder and prostate. B, Anechoic
bloodposterior to the bladder in a patient with
intraperitonealhemorrhage.
Figure 2-32
Longitudinal pelvic view (male) with a hypoechoic region
posteriorto the bladder, which represents seminal vesicles.
(Courtesy ofDr. Jones and Dr. Welch.)
Figure 2-33
Transverse pelvic view (male) with hypoechoic seminal
vesiclesposterior to the bladder. Seminal vesicles vary in
appearance anddo not always have the classic paired profile.
(Courtesy of Dr.Jones and Dr. Welch.)
Figure 2-31A
-
8/9/2019 UltrasoundTraumaCh02 Fast Exam
23/23
37
The FAST Exam
References
1. Rozycki GS, Shackford SR. Ultrasound, what every trauma
surgeon should know.J Trauma. 1996;40:1-4.
2. Han DC, Rozycki GS, Schmidt JA, et al. Ultrasound training
during ATLS: an early start for surgical interns.J Trauma.
1996;41:208-213.
3. Scalea TM, Rodriguez A, Chiu WC, et al. Focused assessment
with sonography for trauma (FAST): results from an
international
consensus conference.J Trauma. 1999;46:466-472.
4. Ma OJ, Mateer JR. Trauma ultrasound examination versus chest
radiography in the detection of hemothorax.Ann Emerg Med.
1997;29:312-316.
5. Sisley AC, Rozycki GS, Ballard RB, et al. Rapid detection of
traumatic effusion using surgeon-performed ultrasonography.
J Trauma. 1998;44:291-297.
6. Dulchavsky SA, Hamilton DR, Diebel LN, et al. Thoracic
ultrasound diagnosis of pneumothorax.J Trauma. 1999;47:970-971.
7. Lorente-Ramos RM, Santiago-Hernando A, Del Valle-Sanz Y, et
al. Sonographic diagnosis of intramural duodenal hematomas.
J Clin Ultrasound. 1999;27:213-216.
8. Yoshii H, Sato M,Yamamoto S, et al. Usefulness and
limitations of ultrasonography in the initial evaluation of blunt
abdominal
trauma.J Trauma. 1998;45:45-51.
9. McKenney M, Lentz K, Nunez D, et al. Can ultrasound replace
diagnostic peritoneal lavage in the assessment of blunt trauma?
J Trauma. 1994;37:439-441.
10. McKenney MG, Martin L, Lentz K, et al. 1,000 Consecutive
ultrasounds for blunt abdominal trauma.J Trauma.
1996;40:607-612.
11. Rozycki GS, Ochsner MG, Schmidt JA, et al. A prospective
study of surgeon-performed ultrasound as the primary adjuvant
modality for injured patient assessment.J Trauma.
1995;39:325-330.
12. Meyers MA. Distribution of intra-abdominal malignancy
seeding: dependency on dynamic flow of ascitic fluid.AJR Am J
Roentgenol. 1973;119:198-206.
13. Meyers MA. The spread and localization of acute
intraperitoneal effusion.Radiology. 1970;95:547-554.
14. Overholt RH. Intraperitoneal pressure.Arch Surg.
1931;22:691-703.
15. Drye JC. Intraperitoneal pressure in the human. Surg Gynecol
Obstet. 1948;87:472-475.
16. Autio V. The spread of intraperitoneal infection. Studies
with roentgen contrast medium.Acta Chir Scand Suppl.
1964;321:1-31.
17. Srinualnad N, Dixon AK. Right anterior subphrenic space: an
important site for the early detection of intraperitoneal fluid
on
abdominal CT.Abdom Imaging. 1999;24:614-617.
18. Ma OJ, Kefer MP, Mateer JR, et al. Evaluation of
hemoperitoneum using a single- vs multiple-view ultrasonographic
examination.
Acad Emerg Med. 1995;2:581-586.
19. Abrams BJ, Sukumvanich P, Seibel R, et al. Ultrasound for
the detection of intraperitoneal fluid: the role of
Trendelenburg
positioning.Am J Emerg Med. 1999;17:117-120.
20. Plummer D. Principles of emergency ultrasound and
echocardiography.Ann Emerg Med. 1989;18:1291-1297.
21. Plummer D. The sensitivity, specificity, and accuracy of ED
echocardiography [abstract].Acad Emerg Med. 1995;2:339-340.
22. Rozycki GS, Feliciano DV, Ochsner MG, et al. The role of
ultrasound in patients with possible penetrating cardiac wounds:
a
prospective multicenter study.J Trauma. 1999;46:543-552.
23. McKenney KL, Nunez DB, McKenney MG, et al. Ultrasound for
blunt abdominal trauma: is it free fluid?Emerg Radiol.
1998;5:203-209.
24. Osyka GS, Chaser MG, Baffin JH, et al. Prospective
evaluation of surgeonsuse of ultrasound in the evaluation of trauma
patients.
J Trauma. 1993;34:516-527.
25. Lucciarini P, Ofner D, Weber F, et al. Ultrasonography in
the initial evaluation and follow-up of blunt abdominal injury.
Surgery.
1993;114:506-512.
26. Rozycki GS, Ochsner MG, Feliciano DV, et al. Early detection
of hemoperitoneum by ultrasound examination of the right upper
quadrant: a multicenter study.J Trauma. 1998;45:878-883.
27. Asher W, Parvin S, Virgiolio R, et al. Echographic
evaluation of splenic injury after blunt trauma.Radiology.
1976;118:411-415.
28. Shanmuganathan K, Mirvis SE, Sherbourne CD, et al.
Hemoperitoneum as the sole indicator of abdominal visceral
injuries: a
potential limitation of screening abdominal US for
trauma.Radiology. 1999;212:423-430.
29. Rozycki GS, Ballard RB, Feliciano DV, et al.
Surgeon-performed ultrasound for the assessment of truncal
injuries.Ann Surg.
1998;228:557-565.
30. Fernandez L, McKenney MG, McKenney KL, et al. Ultrasound in
blunt abdominal trauma.J Trauma. 1998;45:841-848.
31. Nyberg DA, Laing FC, Jeffrey RB. Sonographic detection of
subtle pelvic fluid collections.AJR Am J Roentgenol.
1984;143:261-263.