Embed Size (px)
Citation preview

Ultrasound in Med. & Biol., Vol. 34, No. 9, pp. 1421–1433, 2008Copyright © 2008 World Federation for Ultrasound in Medicine & Biology
Printed in the USA. All rights reserved0301-5629/08/$–see front matter
doi:10.1016/j.ultrasmedbio.2008.01.016
● Original Contribution
ULTRASOUND-ENHANCED THROMBOLYSIS USING DEFINITY® AS ACAVITATION NUCLEATION AGENT
SAURABH DATTA,* CONSTANTIN-C. COUSSIOS,† AZZDINE Y. AMMI,* T. DOUGLAS MAST,*GABRIELLE M. DE COURTEN-MYERS,‡ and CHRISTY K. HOLLAND*
*Department of Biomedical Engineering, University of Cincinnati, Cincinnati, OH; †Institute of BiomedicalEngineering, Department of Engineering Science, University of Oxford, Oxford, UK; and ‡Department of
Pathology, University of Cincinnati, Cincinnati, OH
Abstract—Ultrasound has been shown previously to act synergistically with a thrombolytic agent, such asrecombinant tissue plasminogen activator (rt-PA) to accelerate thrombolysis. In this in vitro study, a commercialcontrast agent, Definity®, was used to promote and sustain the nucleation of cavitation during pulsed ultrasoundexposure at 120 kHz. Ultraharmonic signals, broadband emissions and harmonics of the fundamental weremeasured acoustically by using a focused hydrophone as a passive cavitation detector and used to quantify thelevel of cavitation activity. Human whole blood clots suspended in human plasma were exposed to a combinationof rt-PA, Definity® and ultrasound at a range of ultrasound peak-to-peak pressure amplitudes, which wereselected to expose clots to various degrees of cavitation activity. Thrombolytic efficacy was determined bymeasuring clot mass loss before and after the treatment and correlated with the degree of cavitation activity. Thepenetration depth of rt-PA and plasminogen was also evaluated in the presence of cavitating microbubbles usinga dual-antibody fluorescence imaging technique. The largest mass loss (26.2%) was observed for clots treatedwith 120-kHz ultrasound (0.32-MPa peak-to-peak pressure amplitude), rt-PA and stable cavitation nucleated byDefinity®. A significant correlation was observed between mass loss and ultraharmonic signals (r � 0.85, p <0.0001, n � 24). The largest mean penetration depth of rt-PA (222 �m) and plasminogen (241 �m) was observedin the presence of stable cavitation activity. Stable cavitation activity plays an important role in enhancementof thrombolysis and can be monitored to evaluate the efficacy of thrombolytic treatment. (E-mail:[email protected]) © 2008 World Federation for Ultrasound in Medicine & Biology.
Key Words: Ultrasound-assisted thrombolysis, Stroke therapy, Ultraharmonics, Stable cavitation, Therapeutic
ultrasound.INTRODUCTION
The use of ultrasound (US) to enhance thrombolysis hasmany potential benefits in treatment of diseases likeischemic stroke, myocardial infarction and deep veinthrombosis, which are caused by thrombus formation.Intravenous administration of recombinant tissue plas-minogen activator (rt-PA) is the only clinically approvedtherapy for limited cases of ischemic stroke (NINDSStroke Study Group 1995; Broderick et al. 2002). Inseveral in vitro studies, US has been used to demonstratethrombolytic enhancement when used as an adjuvant tort-PA (Lauer et al. 1992; Francis et al. 1992; Blinc et al.1993). Several studies have also shown that better pen-etration of US through skull, as well as enhanced fibri-
Address correspondence to: Christy K. Holland, Ph.D., Depart-ment of Biomedical Engineering, University of Cincinnati, Medical
Sciences Building, Room 6167, 231 Albert Sabin Way, Cincinnati, OH45267–0586. E-mail: [email protected]1421
nolysis can be achieved using frequencies in the 20 to500-kHz range (Blinc et al. 1993; Suchkova et al. 1998;Akiyama et al. 1998; Behrens et al. 1999; Coussios et al.2002). Theoretically, Diamond and Anand (1993) dem-onstrated that the process of thrombolysis is limited bydiffusion of fibrinolytic enzymes into the clot. This wasexperimentally demonstrated by Blinc et al. (1992). Inseveral mechanistic in vitro studies, it is speculated thatUS facilitates transport of fibrinolytic enzymes into theclot (Francis et al. 1995; Pieters et al. 2004; Devcic-Kuhar et al. 2004), along with mechanical effects likemicrostreaming (Sakharov et al. 2000) and acoustic cav-itation (Everbach and Francis 2000; Datta et al. 2005,2006; Prokop et al. 2007) among other possible mecha-nisms.
Tachibana (1995) introduced the use of micro-bubbles to augment thrombolysis using 170-kHz USadjuvant to urokinase in an in vitro human blood clot
model. They suggested the use of diagnostic contrast
1422 Ultrasound in Medicine and Biology Volume 34, Number 9, 2008
agents for therapeutic augmentation of thrombolyticdrugs. Xie et al. (2005) demonstrated the effectiveness oflipid-encapsulated microbubbles and 1-MHz US in therecanalization of arteriovenous graft thrombi in an ani-mal model. They observed a significantly greater clear-ing of thrombus using higher intensities (10 W/cm2)compared with lower intensities (0.4 to 0.6 W/cm2) andattributed this effect to the presence of cavitation. Molinaet al. (2006) administered microbubbles and rt-PA, alongwith 2-MHz US and accelerated clot lysis in clinicaltrials. Although this approach appears promising, themechanisms responsible for this US enhancement arestill not well understood. In a previous study, Datta et al.(2006) monitored subharmonic emissions as a result ofstable cavitation and correlated this type of bubble be-havior with clot mass loss. The detection of subharmonicor ultraharmonic signals provides a possible method tomonitor the progress of US enhancement of thromboly-sis. Such techniques to monitor and measure cavitationactivity during therapy are needed to monitor and per-haps even control thrombolytic progress.
The objective of this investigation was to determinewhether 120-kHz pulsed US and an infusion of an echocontrast agent could enhance clot lysis and penetration ofrt-PA into human whole blood clots in vitro. The hy-potheses tested in this study are (a) whether the use of acontrast agent (Definity®) with 120-kHz pulsed US re-sults in a measurable increase in stable cavitation activityover the treatment duration of 30 min and (b) whether thepresence of sustained stable cavitation activity results inenhanced thrombolysis and increased penetration ofrt-PA into the clots.
MATERIALS AND METHODS
Ultrasound thrombolysis system overviewA prototype 6.14-cm-diameter single circular ele-
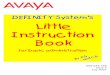
ment, unfocused, 120-kHz transducer (Sonic ConceptsInc., Woodinville, WA, USA) was used for sonication ofclots as described previously (Datta et al. 2006). Thetransducer used in this study has a –3 dB beamwidth of2.5 cm and a Rayleigh distance of 10.6 cm. An illustra-tion of the experimental set up is shown in Fig. 1. The120-kHz transducer was driven by a function generator(Agilent 33120A, Palo Alto, CA, USA), power amplifier(75A250, AR Amplifier Inc., Souderton, PA, USA) anda custom-built impedance matching–network (SonicConcepts Inc.). For all experiments described in thisstudy, the 120-kHz transducer was driven in pulsedmode, with an 80% duty cycle and 1,667-Hz pulse rep-etition frequency consistent with previous studies (Dattaet al. 2006; Holland et al. 2002). The sample chamber,consisting of an acoustically transparent latex condom,
was placed at the Rayleigh distance of the 120-kHztransducer using a three-axis translation stage (Newport423, Irvine, CA, USA). Human blood clots suspended in30 mL of plasma rested in the tip of condom. The samplechamber was placed in a Lucite tank filled with degassedwater at 37° C and dissolved oxygen level (PO2) main-tained below 40% saturation as measured by a dissolvedoxygen meter (Oakton DO100, Vernon Hills, IL, USA).The tank wall opposite the 120-kHz transducer was linedwith acoustically-matched absorbing material (AptflexF36, Precision Acoustics, Dorchester, UK) to preventreflection and the formation of standing waves.
Clot formation protocolHuman whole blood was drawn from four volun-
teers by sterile venipuncture after local Institutional Re-view Board approval. Clots were prepared by aliquoting1.5 mL of fresh human blood into 1.3-cm inner diameterVacutainer tubes, incubating the tubes in a 37° C waterbath for 3 h and storing the clots in a 5° C refrigerator forat least 72 h before use in the experiments to allowcomplete clot retraction. The clot formation and handlingprotocol has been described previously (Shaw et al.2006; Datta et al. 2006; Holland et al. 2007). The clotswere weighed initially before any treatment and wereplaced in the sample chamber containing 30 mL ofthawed human fresh frozen plasma and held at 37o C.Reconstituted rt-PA (96 �g/mL) was added to the plasmafor rt-PA-alone treatment and combined US and rt-PAtreatments. The treatment times were fixed at 30 min.The rt-PA dose and clinically relevant treatment durationis consistent with previous studies (Datta et al. 2006;Holland et al. 2007). After exposure, each clot wasweighed again and the extent of thrombolysis was deter-
120 kHzTransducer
Acoustic Absorber
Sample Chamber
FocusedHydrophone
ImpedanceMatching Circuit
Digital Oscilloscope Pre-amplifier
Function Generator Power
Amplifier
Computer for Data Acquisition
Fig. 1. Experimental setup for US exposure of human bloodclots placed in a sample holder containing plasma and Defin-ity®. A focused hydrophone placed 90° to the acoustic axis ofthe 120-kHz transducer and with its focus coincident with the
blood clot was used as a passive cavitation detector.
mined as a percent mass loss.

Thrombolysis using Definity® ● S. DATTA et al. 1423
Contrast agent preparationDefinity® vials were activated at room temperature
using the VialmixTM agent activator (Bristol-MyersSquibb Medical Imaging, MA, USA) according to themanufacturer’s instructions. After the 45-s activation cy-cle, the vials were left for 2 min to return to roomtemperature. The agent was drawn from the vial using a20-gauge needle from the base of the vial while ventingto the atmosphere with a second 22-gauge needle and a0.2-micron in-line filter. The volume of agent drawn at atime was 0.1 mL and this aliquot was diluted by a factorof 100 by volume in phosphate-buffered saline (PBS).Subsequently, 100-�l aliquots of the diluted Definity®
were infused as a series of bolus injections every 3 min,each at a rate of 80 �L/s, using a syringe pump (K.D.Scientific, model 230, Holliston, MA, USA). A 4F an-giographic catheter (Medi-tech Inc., Watertown, MA,USA) inside an air-filled 9F sheath catheter (CordisCorp., Miami, FL, USA) was used to deliver contrastagent next to the blood clot inside the sample chamber.The column of air surrounding the inner catheter pro-vided acoustic shielding to the contrast agent within thecatheter itself. The number density of microbubbles de-livered with each bolus infusion was 1.2 � 108 micro-bubbles/mL. This microbubble density is two orders ofmagnitude less than the maximum bolus concentrationrecommended by the manufacturer for diagnostic appli-cations. The recommended dose is 10 �L/kg activatedDefinity (1.2 � 1010 microbubbles/mL) by bolus injec-tion within 30–60 s. In treatments (rt-PA, US, PBSinfusions without Definity®) without the use of a contrastagent, an equivalent volume of PBS was infused in thesample chamber using the same catheter arrangement.
Cavitation detection systemA cylindrically focused broadband hydrophone
(Sonic Concepts Inc.), placed orthogonally to the 120-kHz beam axis, was used to passively detect cavitationactivity in the sample chamber as shown in Fig. 1. Thecavitation detection hydrophone was mounted on a mi-crometer-controlled 3-axis translation stage (Newport423, Irvine, CA, USA) for precise alignment with bloodclots. A 5-mm brass ball, positioned at the Rayleighdistance of the 120-kHz transducer, was used as anacoustic target for initial alignment of the broadbandcylindrically focused hydrophone. Finally, acoustic scat-tering from the clot itself was used to finalize the align-ment so that a volume encompassing the clot was mon-itored for cavitation by the focused hydrophone. Thecylindrically-focused hydrophone has a �6 dB focaldepth-of-field of 3.6 cm along its axis, a focal width of1.3 cm and thickness of 0.1 cm. Signal acquired by thehydrophone was gated to account for the travel time of
the pulse from the 120-kHz transducer and hydrophone.The signal received by the focused hydrophone wasamplified using a preamplifier (Signal Recovery 5185,Oak Ridge, TN, USA) and stored using a digital oscil-loscope (Lecroy Waver Surfer 424, Chestnut Ridge, NY,USA). The signal received by the hydrophone was gatedto ensure that cavitation was monitored over a regionencompassing the clot surface, interior of the clot andsurrounding fluid. The start of the gating window wasthus set to 102 �s, the time that corresponds to the traveltime of the ultrasound pulse from the 120-kHz transducerto the hydrophone. The duration of the gating windowwas set to 20 ms to ensure a frequency resolution of 5kHz. The cavitation detector signal therefore consisted of500,000 points acquired at a sampling rate of 25 MHzand recorded in binary format twice per second. Eachtime trace file thus consisted of 33 contiguous pulsesrecorded in a binary format. The binary files were con-verted to MATLAB (The MathWorks Inc., Natick, MA,USA) data files and zero padded to 16,384 points. AHanning window was subsequently applied before per-forming a fast Fourier transformation for each pulse. Thesquared frequency spectra for the 33 pulses were aver-aged in the frequency domain. A schematic of the signalprocessing is illustrated in Fig. 2.
The appearance of ultraharmonics in the signal re-ceived by the hydrophone indicated stable cavitationactivity in the vicinity of the blood clot. In this stablecavitation detection scheme, ultraharmonics were fre-quency components at odd multiples of 60 kHz, half themain excitation frequency. The appearance of broadbandnoise emissions designated inertial cavitation in thatsame region. To determine the threshold for stable andinertial cavitation in this system, samples containing ahuman blood clot, plasma and Definity® were exposed to120-kHz pulsed US, with an 80% duty cycle and a1667-Hz pulse repetition frequency. The frequency con-tent of the signal received by the focused hydrophonewas analyzed for excitation pressure amplitudes in therange 0.06–0.75 MPa. A total of 20 files were recordedover a period of 10 s for each pressure and were analyzedfor ultraharmonic and broadband noise emissions. Thisprocess was repeated using three different samples ateach pressure amplitude. Ten consecutive odd ultrahar-monics of the subharmonic (60 kHz) component in thefrequency range of 300 kHz–1.5 MHz were extractedfrom the frequency spectrum using a digital band-passcomb filter. Each frequency band was centered at thecorresponding ultraharmonic frequency with a fixedbandwidth of 7.6 kHz, which is comparable to the �6 dBbandwidth of the 120-kHz tone bursts used. Spectralpower in 10 bands between the ultraharmonics and har-monics of the fundamental were used to determine thebaseline noise floor, as well as changes in the broadband
noise energy used as a measure of inertial cavitation
band-
1424 Ultrasound in Medicine and Biology Volume 34, Number 9, 2008
activity. The levels of ultraharmonic and broadbandnoise power as a function of excitation pressure areshown in Fig. 3.
During the clot mass loss experiments, a total of3,600 files were recorded over a period of 30 min.
Signal received by focused hydrophone
0 0.002 0.004 0.006 0.0-2
-1.5
-1
-0.5
0
0.5
1
1.5
2
Am
plitu
de (v
olts
)
Frequency domain transformation and
averaging
Integratioover 30 m
Energy in selected bands
(Cavitation Dose)
Fig. 2. Schematic of the signal processing algorithmreceived by the broad
Spectral power in the ultraharmonic bands was inte-
grated over the 30-min duration and used as a measure ofthe extent or dose of stable cavitation as illustrated con-ceptually in Fig. 2. The fraction of the exposure timeduring which the energy in ultraharmonic bands washigher than the baseline spectral components because of
0 1 2 3 4 5 6
x 10-4
-0.4
-0.3
-0.2
-0.1
0
0.1
0.2
0.3
0.4
Time (sec)A
mpl
itud
e (v
olts
)
0.012 0.014 0.016 0.018 0.02)
33 individual contiguous
pulses captured and windowed
Spectral power computation over
multiple bands
0 5 10 15 20 25 300
1
2
3
4
5x 10
-5
Time (min)
Am
plitu
de (V
2 -Hz)
rmine cavitation dose from scattered acoustic signalsfocused hydrophone.
08 0.01Time (sec
nin
to dete
scattering from the contents of the sample holder was

ars rep
Thrombolysis using Definity® ● S. DATTA et al. 1425
used as a measure of the duration of stable cavitationactivity. Spectral power in the bands between the ultra-harmonics and harmonics of the fundamental were usedas a measure of inertial cavitation activity. In this ap-proach, the selected spectral bands were sufficientlyclose to enable meaningful comparison without the needto correct for the frequency response of the hydrophone.
To evaluate the effect of Definity® on scatteredenergy, the harmonics of the fundamental detected fromthe contents of the sample holder including clot, plasmaand Definity® were also measured using a similar ap-proach. To estimate the fractional stable cavitation du-ration, the mean and standard deviation measurements ofspectral power in bands representing broadband or base-line emissions were used. The fractional stable cavitationduration was defined as the percentage of time the com-bined spectral power in the ultraharmonic bands wasgreater than two standard deviations above the mean ofbroadband or baseline spectral bands for that treatment.
Three rt-PA concentrations of 1.4 �g/mL, 11.0�g/mL and 96.0 �g/mL were used in this work to studythe effect of Definity® infusions on US enhancement ofthrombolysis. The lowest concentration chosen was ap-proximately eight times lower than the maximum allow-able human clinical dose (NINDS Stroke Study Group1995; Broderick et al. 2002). Similarly, the highest con-centration used was approximately eight times higherthan human dose as was used in previous study (Datta et
0 0.1 0.2 0.310
-6
10-5
10-4
10-3
Peak to Peak
Spe
ctra
l Pow
er L
evel
[Log
(V2 -H
z)]
Fig. 3. Spectral power levels in ultraharmonic and broadpressure amplitude. The scattered signal is received by afocus coincident with the region of the sample holder co
samples were exposed at each pressure, and error b
al. 2006). The approach of sustaining stable cavitation
throughout the treatment period was explored at thelower rt-PA concentrations (1.4 �g/mL and 11.0 �g/mL)using Definity® infusions every 3 min and US exposureswith a peak-to-peak pressure amplitude of 0.32 MPa.Both rt-PA alone and rt-PA, US, PBS infusions withoutDefinity® data were also acquired for the lower rt-PAconcentrations.
Fluorescence dual-antibody stainingAfter treatment, the clots were immersed in optimal
cutting temperature gel (Tissue Tek, Redding, CA, USA)and snap-frozen in liquid nitrogen and stored at �80°C.The clots were thawed to room temperature for patho-logic analysis and fixed by immersion in 3% paraformal-dehyde solution for 48 h and 30% sucrose solution for24 h. The clots were cut in 25-�m-thick sections using amicrotome for fluorescence dual-antibody staining. Theprimary antibodies used were monoclonal antibody(mouse immunoglobulin, IgG) against human plasmino-gen (1:1000 dilution; AB10178; Abcam Inc., Cambridge,MA, USA) and polyclonal antibody (goat IgG) againsthuman tissue plasminogen activator (1:1000 dilution;387; American Diagnostics Inc., Stamford, CT, USA).Dilutions were done in blocking buffer (2% horse serum,0.3% Triton and 0.1% bovine serum albumin in 0.1mol/L phosphate buffer). The two secondary antibodiesthat were used were donkey antigoat IgG (dilution 1:500;
0.5 0.6 0.7 0.8
tic Pressure (MPa)
UltraharmonicBroadband
bands as a function of increasing peak-to-peak acousticphone placed 90° to the source transducer axis with itsg a human clot in plasma and Definity®. Three differentresent the standard deviation of 60 measurements.
0.4
Acous
bandhydro
ntainin
A11055; Molecular Probes Inc., OR, USA) and donkey

1426 Ultrasound in Medicine and Biology Volume 34, Number 9, 2008
antimouse IgG (dilution 1:500; A31570; MolecularProbes Inc.).
Clot sections were incubated in the primary anti-bodies for 1 h, washed three times with saline solutionand blocked before incubating in secondary antibodiesfor 1 h. After incubation with secondary antibodies, clotsections were washed again three times with saline so-lution, mounted on glass slides (Fisher Scientific, Pitts-burgh, PA, USA), and sealed with glass cover slips. Clotsections were imaged using a fluorescent microscopeBX51 (Olympus America Inc., Melville, NY, USA) witha 10x objective, and images were acquired using SpotAdvanced software (Diagnostic Instruments Inc., Ster-ling Heights, MI, USA) and stored on a desktop com-puter. The exposure parameters (time and gain) wereadjusted to calibrate images of each clot section, and thesame fixed exposures parameters and filter were used toanalyze all the images for that particular section. A totalof five images were taken for each clot section, one at thecenter and one each at randomly selected 3, 6, 9 and 12o’clock positions encompassing clot edge and a portionof interior of the clot section. In the images, the area ofrt-PA localization appears bright green and the area ofplasminogen localization appears red. For each clot sec-tion, the image of the interior of the clot served as its owncontrol. The brightness level for the image obtained forclot center was adjusted using the window/level functionavailable in ImageJ software (National Institutes ofHealth, Bethesda, MD, USA) such that the whole imageappeared dark. The same values of the window/levelfunction were then applied to the remaining images ofthe same section. This ensured that only signal suffi-ciently stronger than the background brightness levelappears in the images. The measurements for penetrationdepth were performed on the processed images. Thepenetration depths of rt-PA and plasminogen were mea-sured using a line scan tool available in the software. Anaverage of six measurements per image per section wasused to evaluate penetration depth. Overlapping regionof rt-PA and plasminogen in the images represents theclot lysis zone, and the depth of this zone was measuredfrom the surface of the clot. Images of the clot sectionsobtained for the following treatments were analyzed toevaluate the difference is penetration depths of rt-PA andplasminogen: (i) no rt-PA, Definity® or US treatment; (ii)rt-PA alone treatment (no US or Definity®); (iii) rt-PA,US (0.32 MPa), PBS infusions without Definity® treat-ment; (iv) rt-PA, Definity® infusions; and (v) US (0.32MPa) treatment.
StatisticsCorrelation between mass loss, the energy in ultra-
harmonic bands, the energy in broadband bands, the
energy in harmonic bands and fractional stable cavitationduration was evaluated statistically using the “corr”function in MATLAB (The MathWorks, Inc.). The com-parison of mass loss for exposures to different combina-tions of rt-PA, US and Definity® was accomplished usinga one-way ANOVA and two sample Student’s t-testsusing MINITAB (MINITAB Inc., State College, PA,USA) statistical analysis software. A two-sample Stu-dent’s t-test was performed on penetration depth mea-
0 0.5 1 1.5 2 2.5 3
10-6
10-5
10-4
Time (Min)
Spec
tral
Pow
er L
evel
[Log
(V2 -H
z)]
UltraharmonicBroadband
(a)
0 0.5 1 1.5 2 2.5 3
10-6
10-5
10-4
Time (Min)
Spec
tral
Pow
er L
evel
[Log
(V2 -H
z)]
UltraharmonicBroadband
(b)
0 0.5 1 1.5 2 2.5 3
10-6
10-5
10-4
Time (Min)
Spec
tral
Pow
er L
evel
[Log
(V2 -H
z)]
UltraharmonicBroadband
(c)
Fig. 4. Representative ultraharmonic and broadband signal lev-els as function of time after a single infusion of Definity® withpeak-to-peak US exposure of (a) 0.32 MPa, (b) 0.50 MPa and
(c) 0.75 MPa.
surements from the images of clot sections.

(0.32
Thrombolysis using Definity® ● S. DATTA et al. 1427
RESULTS
The change in the level of spectral power in ultra-harmonic bands as function of increasing peak-to-peakpressure amplitude and their relative magnitude com-pared with spectral power in broadband bands is shownin Fig. 3. Each data point is an average of 60 measure-ments over three sample preparations, and the error barsrepresent the standard deviation of the measurements. Nosignificant difference between the levels of signal inultraharmonic or broadband signals was observed for thepressure steps up to 0.21 MPa. As the acoustic pressure
0 5 10 15 20 25
10-6
10-5
10-4
Time (min)
Sp
ectr
al P
ow
er L
evel
[L
og
(V2 -H
z)] (a)
0 5 10 15 20 25
10-7
10-6
10-5
Sp
ectr
al P
ow
er L
evel
[L
og
(V2 -H
z)]
Time (min)
(c)
Fig. 5. A representative example of the spectral power iDefinity® infusion but no cavitation (0.12 MPa peak-to-peak-to-peak), (c) with infusion of PBS alone at a peak-tois observed) and (d) with infusion of Definity®, resulti
pressure
Table 1. Effect of contrast agent Definity® on enhancthe ultraharmonic signals and
PBS, rt-PA and USat 0.32 MPa
Ultraharmonic energy (V2) 0.0162 � 0.0145Fractional stable cavitationDuration (%) 10.1 � 4.4
The p-value shown is for two sample Student’s t-test for a sample size of
is increased to 0.32 MPa peak-to-peak in the next step,the amplitude of both broadband and ultraharmonicpower bands increases, but the increase in the ultrahar-monic bands is significantly higher than the broadbandenergy. Thus, 0.32 MPa peak-to-peak pressure amplitudeis interpreted as the onset of stable cavitation for thisexperimental set up. At pressure steps greater than 0.32MPa, the level of ultraharmonic energy decreases.
An example of the effect of infusion of Definity®
can be observed in Fig. 4. When Definity® was infusedinitially, the spectral power in ultraharmonic bands in-
0 5 10 15 20 25 30
0-6
0-5
0-4
Time (min)
(b)
0 5 10 15 20 25 30
10-7
10-6
10-5
Time (min)
(d)
ltraharmonic band over the treatment duration (a) with(b) with Definity® infusion but no cavitation (0.21 MPapressure of 0.32 MPa (note only initial cavitation activityelatively sustained cavitation at the same peak-to-peakMPa).
of stable cavitation activity as measured by energy innal stable cavitation duration
Definity®, rt-PAand US at 0.32 MPa p-value
0.0482 � 0.031 0.046
20.8 � 6.8 0.003
30
1
1
1
Sp
ectr
al P
ow
er L
evel
[L
og
(V2 -H
z)]
30
Sp
ectr
al P
ow
er L
evel
[L
og
(V2 -H
z)]
n the upeak),-peakng in r
ementfractio
six for each treatment.

ally sign
1428 Ultrasound in Medicine and Biology Volume 34, Number 9, 2008
creased for approximately 2.5 min in the presence ofpulsed US at peak-to-peak pressure amplitude of 0.32MPa (Fig. 4a). At higher pressures, initial infusion ofDefinity® enhanced the level of ultraharmonic emissionsbut for shorter durations (Fig. 4b and c). This informa-tion was used to select the frequency of intermittentinfusions of Definity® (one infusion every 3 min) andpressure amplitude of 120 kHz US (0.32 MPa peak-to-peak) to sustain stable cavitation during the 30-min ex-posures. The effect of Definity® infusions on sustainingcavitation over a period of 30 min can be observed inFig. 5. The peak-to-peak pressure amplitudes used fordata plotted in Fig. 5 were 0.12 MPa, 0.21 MPa and 0.32MPa. In Fig. 5a, ultraharmonic spectral power level inthe presence of Definity® but without any detectablestable cavitation activity (0.12 MPa) is shown. Note thatno enhancement in the ultraharmonic spectral powerbands is observed. Fig. 5b shows ultraharmonic spectralpower level at a higher pressure (0.21 MPa). Fig. 5cshows the cavitation activity without Definity® at a high-er-pressure amplitude (0.32 MPa), which is closer to thepreviously reported stable cavitation threshold of 0.40MPa (Datta et al. 2006). Note that PBS was infused inthis treatment every 3 min. An increase in ultraharmonicsignal can be observed for the first 5 min, after whichsubsequent stable cavitation activity subsided. However,in Fig. 5d, when Definity® was infused intermittentlyevery 3 min, the cavitation activity is sustained through-out the 30-min exposure duration.
The effect of Definity® on the enhancement ofcavitation activity as measured by ultraharmonic energyand fractional stable cavitation duration is shown inTable 1. Infusion of Definity® increased the ultrahar-monic energy from a mean value of 0.0162–0.0482 V2 (p
Table 2. Correlation coefficient (r) for
MassLoss
UltraharmonicEmissions
Mass Loss 1 0.85(p < 0.0001)
Ultraharmonic 1Emissions
BroadbandEmissions
Harmonic ofFundamental
Fractional StableCavitationDuration
The p-value for correlation is shown in parentheses and the statisticwas used to evaluate correlation coefficients.
� 0.046). The stable cavitation duration was also signif-
icantly increased from a mean of 10.1–20.8% (p �0.003). The effect of combinations of rt-PA at a concen-tration of 96 �g/mL, US and Definity® infusions with orwithout cavitation activity on clot mass loss is presentedin Fig. 6. The greatest clot mass loss of 26.2% wasobserved for the combination of rt-PA, Definity® infu-sions and US treatment at the peak-to-peak pressureamplitude of 0.32 MPa (p � 0.001). A significantlylower clot mass loss of 16.0% was observed for the samepeak-to-peak pressure amplitude of 0.32 MPa in rt-PA,US, PBS infusions without Definity® treatment. Theother rt-PA, Definity® infusions and US treatments atlower pressures (0.12 MPa and 0.21 MPa) resulted in a
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
Treatment
Mas
s Lo
ss (%
)
a Control
rt-PA alone
rt-PA, Definity infusionsand USDefinity infusions and USwithout rt-PArt-PA,US, PBS infusionswithout Definity
A B C D E F G
Fig. 6. Mass loss (%) as a function of peak-to-peak acousticpressure for different treatments: (a) No rt-PA, Definity® orUS, which is the control treatment; (b) rt-PA alone; (c) rt-PA,Definity® infusions and US (0.12 MPa peak-to-peak pressureamplitude); (d) rt-PA, Definity® infusions and US (0.21 MPapeak-to-peak pressure amplitude); (e) Definity® infusions andUS (0.32 MPa peak-to-peak pressure amplitude) without rt-PAtreatment; (f) rt-PA, PBS infusions without Definity® and US(0.32 MPa peak-to-peak pressure amplitude); and (g) rt-PA,Definity® infusions, and US (0.32 MPa peak-to-peak pressure
red acoustic emissions and mass loss
BroadbandEmissions
Harmonic ofFundamental
Fractional StableCavitationDuration
0.00 0.51 0.83(p � 1.0) (p � 0.01) (p < 0.0001)
0.01 0.34 0.84(p � 0.97) (p � 0.10) (p < 0.0001)
1 0.06 �0.19(p � 0.77) (p � 0.38)
1 0.29(p � 0.17)
1
ificant correlations are shown in bold. A combined sample size of 24
measu
amplitude). A sample size of six was used for each treatment.

Thrombolysis using Definity® ● S. DATTA et al. 1429
lower clot mass loss, which was not significantly differ-ent from the rt-PA alone treatment (without US). Treat-ment with Definity® infusions and US without rt-PA at apressure amplitude of 0.32 MPa resulted in a mean clotmass loss of 6.3%, which is higher than control (no US,no Definity®, no rt-PA) but lower than rt-PA alonetreatment.
The correlation between the fractional stable cavi-tation duration and clot mass loss is shown in Fig. 7a andthe correlation between ultraharmonic energy and clotmass loss is shown in Fig. 7b. The clot mass loss in-creased with both the fractional stable cavitation durationand ultraharmonic energy. Table 2 shows the values ofcorrelation coefficients between the measured mass loss,ultraharmonic energy, broadband emissions, harmonicenergy and stable cavitation duration, for a sample sizeof 24. A statistically significant correlation of r � 0.85 isobserved between clot mass loss and ultraharmonic en-ergy (p � 0.0001). Also, there was a significant corre-lation of r � 0.83 between stable cavitation duration and
Definity0.21 MPa
0.21 MPa
Definity0.32 MPa
0.32 MPa
PBS0.32 MPa
0.32 MPa
Definity0.12 MPa
0.12 MPa
0.0
10.0
20.0
30.0
40.0
0.0 10.0 20.0 30.0Fractional Stable Cavitation Duration (%)
Mas
s Lo
ss (%
)
Definity
Definity
Definity
PBS
0.0
10.0
20.0
30.0
40.0
0 0.02 0.04 0.06 0.08
Ultraharmonic Energy (V2)
Mas
s Lo
ss (%
)
(a)
(b)
Fig. 7. Mass loss (%) and cavitation activity relationship as afunction of (a) fractional stable cavitation duration, which is afraction of the total time for which the ultraharmonic energylevel was above the noise floor; and (b) ultraharmonic energyintegrated over a 30-min exposure. A sample size of six wasused for each treatment, and error bars represent standard
deviation of the measurements.
mass loss (p � 0.0001). A relatively weaker correlation
of r � 0.51 with harmonic emissions was also observed(p � 0.01).
Results of the dual antibody fluorescence imagingare shown in Fig. 8. The images in the left column showrt-PA localization in green and the right column showlocalization of plasminogen in red. The scale bar in theimages is 0.3 mm. Images in Fig. 8a show the controltreatment, Fig. 8b shows results for rt-PA alone treatedclots, Fig. 8c shows US, rt-PA and saline treated clotsand Fig. 8d shows US, rt-PA and Definity®-treated clots.It can be qualitatively observed that rt-PA penetration islargest for the combined US, rt-PA and Definity® treat-ment. Width of the clot lysis zone can be observed bypenetration depth of rt-PA in the images and accumula-tion of plasminogen in the same region, as measuredfrom the surface of the clot using the line scan tool in theSpot Advanced software. The penetration depth mea-surements are shown in Table 3 for three clots processedfor each treatment. Treatments with rt-PA, Definity®
infusions and US exhibited the greatest mean rt-PA pen-etration of almost 222 �m, which is statistically signif-icantly greater than any other treatment (p � 0.001).There was a greater variation of plasminogen penetrationdepth, and the mean value for combined US, rt-PA andDefinity® treatment was 241 �m, but the mean was notstatistically significantly greater than the rt-PA, US, PBSinfusions without Definity® (p � 0.05).
The effect of infusions of Definity® at lower rt-PAconcentrations on clot mass loss can be observed in Fig.9. At the lowest rt-PA concentration of 1.4 �g/mL,thrombolysis by rt-PA alone dropped to a mean value of7.9%. The use of Definity® at this concentration stillenhanced thrombolysis significantly (p � 0.001).
DISCUSSION
A strategy for the use of contrast agent micro-bubbles along with US and thrombolytics was exploredin this work. A simultaneous monitoring of cavitationactivity could help optimize therapeutic benefits of US-enhanced thrombolysis. The results suggest that an in-crease in stable cavitation activity resulted in a corre-sponding increase in clot mass loss. In the present work,simultaneous measurement of microbubble-enhancedcavitation activity showed a statistically significant cor-relation between ultraharmonic signals and mass loss.Earlier, Porter et al. (1996) observed thrombolytic en-hancement in vitro using perfluorocarbon-exposed soni-cated dextrose albumin microbubbles together with 20-kHz US (0.845 MPa peak negative pressure amplitude)and urokinase. Along the same lines, Mizushige et al.(1999) compared different contrast agents used withrt-PA and catheter-based 10-MHz US. They reported a
correlation between the persistence of microbubbles dur-
1430 Ultrasound in Medicine and Biology Volume 34, Number 9, 2008
rt-PA Staining Plasminogen Staining
0.3 mm 0.3 mm
(a)
(b)
(c)
(d)
Fig. 8. Representative examples of fluorescent dual-antibody–stained images of clot sections. The left column imagesare stained green for rt-PA by fluorescein isothiocyanate (FITC)–conjugated secondary antibody. For the same section,the right column images show accumulation of plasminogen stained red by Texas red (TRITC)–conjugated secondaryantibody. Representative clot section images are shown for (a) no rt-PA, Definity® or US (the control treatment); (b)rt-PA alone treatment; (c) rt-PA, PBS infusions and US (0.32 MPa peak-to-peak amplitude) treatment; and (d) rt-PA,
Definity® infusions and US (0.32 MPa peak-to-peak amplitude) treatment.

tment a
Thrombolysis using Definity® ● S. DATTA et al. 1431
ing the US exposure and thrombolysis in their in vitroexperiments. Several other in vitro studies have sinceshown US-assisted thrombolysis with and without rt-PAin the presence of microbubbles and have suggestedcavitation-related phenomena are responsible for thiseffect (Porter et al. 2001; Nedelmann et al. 2002; Cintaset al. 2004). Nedelmann et al. (2005) further demon-strated that US-induced blood clot dissolution without athrombolytic drug is more effective at 20 kHz whencompared with 40 or 60 kHz using the same acousticintensity (0.2 W/cm2). These studies have already dem-onstrated a potential therapeutic use of microbubbles inbreaking up blood clots mediated possibly by cavitationactivity. In an important contrast to the present study, nodirect or indirect measurement of cavitation activity wasreported in any of the studies mentioned above. Theresults of the present study demonstrate that a micro-bubble infusion was effective in sustaining stable cavi-tation activity and this treatment protocol resulted in thehighest mass loss. It is important to note that fullyretracted clots (3 to 14 d old) were used in this study.These clots tend to be more resistant to lysis than newlyformed clots (Holland et al. 2002, 2007).
Microbubbles and US have already been success-fully used to augment the recanalization of vessels oc-
05
101520253035
1.4 µg/ml 11 µg/ml 96 µg/ml
rt-PA Concentration
Mas
s Lo
ss (%
) rt-PA alone
rt-PA, US, PBS infusionswithout Definityrt-PA, Definity infusionsand US
Fig. 9. Effect of Definity® on clot mass loss as a function ofrt-PA concentration. The peak-to-peak pressure amplitude usedin all US treatments was 0.32 MPa. A significant enhancementover rt-PA alone treatment can be observed at lowest
Table 3. Penetration depth of rt-PA and pl
Treatment rt-PA p
Controlrt-PA alonert-PA, US, PBS infusions without Definity®
rt-PA, Definity® infusions and US
Measurements were made on dual antibody–stained clot sectionsmeasurements done on sections obtained from three clots for each treapeak-to-peak pressure amplitude for US was 0.32 MPa.
concentration.
cluded by small clots in an in vivo rabbit iliofemoralartery clot model without the use of lytic agents such asrt-PA (Birnbaum et al. 1998). In a canine coronary arterythrombus model, transcutaneous 27-kHz US along withrt-PA demonstrated significant recanalization (Siegel etal. 2000). Microbubble potentiation of thrombolysis inintracranial arteries was demonstrated in a porcine modelby Culp et al. (2003) using 1-MHz US. These resultswere repeated in other arteriovenous graft thrombi mod-els in canines (Xie et al. 2005) and in a porcine ascendingpharyngeal artery model (Culp et al. 2004) using platelet-targeted microbubbles. The authors in these studies at-tributed this enhancement to cavitation activity and sug-gested a possible additive effect when used with a throm-bolytic such as rt-PA. In contrast to these in vivo studies,a significant observation in our in vitro study is thatDefinity® infusions in the presence of US but withoutrt-PA did not result in significantly higher mass loss. Anexplanation of this enhancement in vivo could be attrib-uted to the presence of a sufficient quantity of endoge-nous tissue plasminogen activator and its synergisticeffect in the presence of US. We propose that this en-dogenous tissue plasminogen activator, together with thecavitation activity nucleated by a contrast agent, mayhave been sufficient to cause enough thrombolysis toresult in recanalization.
In human clinical trials Alexandrov et al. 2004a,2004b) demonstrated improved arterial recanalizationand improved clinical outcomes with the use of 2-MHztranscranial Doppler and rt-PA. Molina et al. (2006)added LevovistTM microbubbles to the transcranialDoppler and rt-PA treatment and reported further throm-bolytic enhancement. However, Daffertshofer et al.(2005) employed a low-frequency broad-beam 300-kHztherapeutic device in clinical trials and observed a sig-nificant increase in intracranial hemorrhage, and thestudy was stopped prematurely. The authors pursued thestudy of bioeffects in a rat model and reported no dele-terious effects as evaluated by histopathological evalua-tion of brain and temperature measurements (Fatar et al.2006). These studies highlight the importance of in vitro
gen measured from the surface of the clot
on depth (�m) Plasminogen penetration depth (�m)
7.5 64.2 � 51.57.8 65.2 � 36.221.5 149.9 � 56.954.9 240.9 �1 02.8
ch case. The data shown here is mean � standard deviation fornd 18 measurements of penetration depth made for each section. The
asmino
enetrati
15.2 �22.0 �52.5 �
221.8 �
for ea
and in vivo studies aimed at understanding the potential

1432 Ultrasound in Medicine and Biology Volume 34, Number 9, 2008
adverse bioeffects of US-assisted thrombolysis whileoptimizing US parameters to maximize thrombolysis.Monitoring the stable cavitation activity as demonstratedin this study could possibly be extended to an in vivosetting to have better control on therapy.
Several mechanistic in vitro studies have been con-ducted to investigate the interaction of US with throm-bolytic drugs (Francis et al. 1992; Blinc et al. 1993;Francis 1995; Suchkova et al. 1998; Akiyama et al. 1998;Behrens et al. 1999; Everbach et al. 2000; Holland et al.2007). Some of these studies have shown that US poten-tiation of fibrinolysis is related to increased transport ofreactants through cavitation-related mechanisms. Ourdual antibody staining results provide experimental evi-dence of a significantly broader lysis zone observed inthe presence of sustained stable cavitation. A similarresult was reported in an earlier study using a similarimmunohistochemistry technique but without any detec-tion of cavitation (Devcic-Kuhar et al. 2004). The rt-PApenetration depth reported in the study (21.2 � 7.2 �m)is comparable to our rt-PA, US, PBS infusions withoutDefinity® treatment (52.5 � 21.5 �m). In our study, thert-PA penetration depth in the presence of stable cavita-tion activity increased to almost 222 � 55 �m.
Onundarson et al. (1992) reported saturation inthrombolysis for rt-PA concentrations �5 �g/mL in hu-man whole blood clots. A similar value of 3 �g/mL wasreported by Trusen et al. (1998). In our study, we ob-served a significant thrombolytic enhancement at anrt-PA concentration as low as 1.4 �g/mL in the presenceof stable cavitation activity. The use of microbubbles atsuch low concentration of rt-PA was sufficient to en-hance thrombolysis significantly compared with treat-ment with rt-PA alone. This demonstrates a possibility oflowering the rt-PA dose and thus lowering the hemor-rhagic risk associated with the use of thrombolytics.
In our previous study, Datta et al. (2006) demon-strated that the largest increase in clot mass loss wasachieved in the presence of stable cavitation and showedthat inertial cavitation activity decreased thrombolyticefficacy. The presence of inertial cavitation could haveserved as a limiter of sustained stable cavitation. In thepresent study cavitation activity was measured and cor-related significantly with the enhancement of thrombol-ysis. It is also important to note that, for treatments withrt-PA, Definity® infusions at lower US peak to peakpressures (0.12 and 0.21 MPa) did not cause any en-hancement of thrombolysis over rt-PA alone treatment inthe absence of ultraharmonic signals.
This study demonstrates an approach to nucleatestable cavitation with a contrast agent for therapeuticbenefit. The serial bolus injection protocol used in thisstudy does not allow for detailed knowledge of the
concentration of acoustically-activated microbubblesaround the clot. Thus, a limitation of the study is that therelationship between density of cavitation nuclei (i.e., thecontrast agent) and the number of activated micro-bubbles is unknown. In addition, the specific effects ofmicrobubble aggregation as a result of secondaryBjerknes forces, acoustic radiation forces, microbubblecoalescence and fluid mixing as a result of streamingwere not investigated and could all contribute to theenhanced thrombolytic efficacy.
CONCLUSIONS
Stable cavitation activity can be sustained using anintermittent infusion of a commercial contrast agent,Definity®. Ultraharmonic emissions can be used to mon-itor and measure cavitation activity, and such signals aresignificantly correlated with increased clot mass loss.Treatments with Definity® infusion along with rt-PA andUS below any detectable cavitation activity did not resultin any increase in mass loss compared with rt-PA alonetreatment. An increased penetration of rt-PA and plas-minogen was also observed in clots exposed to stablecavitation nucleated by Definity®. The synergistic effectof sustained cavitation activity was also observed at asignificantly lower concentration of rt-PA. Ultrahar-monic emissions could potentially be used to monitorthrombolytic efficacy during treatment, and further stud-ies are still warranted to develop in vivo cavitation de-tection techniques.
Acknowledgements—This research was supported by the National In-stitutes of Health, grant number NIH/NINDS R01-NS047603. Wegratefully acknowledge the assistance of Drs. George Shaw and JasonMeunier for the human whole blood clot model and valuable discus-sions. We also acknowledge the assistance of Stella Nicolaou andSampada Vaidya for developing the fluorescent imaging technique.
REFERENCES
Akiyama M, Ishibashi T, Yamada T, Furuhata H. Low –frequencyultrasound penetrates the cranium and enhances thrombolysis invitro. Neurosurgery 1998;43:828–833.
Alexandrov AV, Molina CA, Grotta JC, Garmi Z, Ford SR, Alvarez-Sabin J, Montaner J, Saqqur M, Demchuk AM, Moye LA, Hill MD,Wojner AW. Ultrasound-enhanced systemic thrombolysis for acuteischemic stroke. N Engl J Med 2004a;351(21):2170–2178.
Alexandrov AV, Demchuk AM, Burgin WS, Robinson DJ, Grotta JC.Ultrasound-enhanced thrombolysis for acute ischemic stroke: PhaseI. Findings of the CLOTBUST trial. J Neuroimaging 2004b;14(2):113–117.
Behrens S, Daffertshofer M, Spiegel D, Hennerici M. Low-frequency,low-intensity ultrasound accelerates thrombolysis through the skull.Ultrasound Med Biol 1999;25:269–273.
Birnbaum Y, Luo H, Nagai T, Fishbein MC, Peterson TM, Li S,Kricsfeld D, Porter TR, Siegel RJ. Noninvasive in vivo clot disso-lution without a thrombolytic drug: Recanalization of thrombosediliofemoral arteries by transcutaneous ultrasound combined withintravenous infusion of microbubbles. Circulation 1998;97:130–134.
Blinc A, Keber D, Lahajnar G, Stegnar M, Zidansek A, Demsar F.Lysing patterns of retracted blood-clots with diffusion or bulk flow

Thrombolysis using Definity® ● S. DATTA et al. 1433
transport of plasma with urokinase into clots—Amagnetic-resonance-imaging study in vitro. Thromb Haemost1992;68:667–671.
Blinc A, Francis CW, Trudnowski JL, Carstensen EL. Characterizationof ultrasound-potentiated fibrinolysis in vitro. Blood 1993;81:2636–2643.
Broderick JP, Hacke W. Treatment of acute ischemic stroke—Part I:Recanalization Strategies. Circulation 2002;106(12):1563–1569.
Coussios C-C, Holland CK, Shaw GJ. Transmission of a large unfo-cussed 120-kHz and 1-MHz ultrasound beam through the humanskull. J Acoust Soc Am 2002;112:2433.
Cintas P, Nguyen F, Boneu B Larrue V. Enhancement of enzymaticfibrinolysis with 2-MHz ultrasound and microbubbles. J ThrombHaemost 2004;2:1163–1166.
Culp WC, Erdem E, Roberson PK Husain MM. Microbubble potenti-ated ultrasound as a method of stroke therapy in a pig model:Preliminary findings. J Vasc Intervent Radiol 2003;14:1433–1436.
Culp WC, Porter TR, Lowery J, Xie F, Roberson PK, Marky L.Intracranial clot lysis with intravenous microbubbles and transcra-nial ultrasound in swine. Stroke 2004;35:2407–2411.
Daffertshofer M, Gass A, Ringleb P, Sitzer M, Sliwka U, Els T,Sedlaczek O, Koroshetz WJ, Hennerici MG. Transcranial low-frequency ultrasound-mediated thrombolysis in brain ischemia: In-creased risk of hemorrhage with combined ultrasound and tissueplasminogen activator—Results of a phase II clinical trial. Stroke2005;36:1441–1446.
Datta S, McAdory LE, Tan J, Holland CK. Cavitation detection duringultrasound-assisted thrombolysis in porcine blood clots. J AcoustSoc Am 2005;117:2558.
Datta S, Coussios C-C, McAdory LE, Tan J, Porter T, de Courten-Myers G, Holland CK. Correlation of cavitation with ultrasoundenhancement of thrombolysis. Ultrasound Med Biol 2006;32:1257–1267.
Devcic-Kuhar B, Pfaffenberger S, Gherardini L, Mayer C, Groschl M,Kaun C, Benes E, Tschachler E, Huber K, Maurer G, Wojta J,Gottsauner-Wolf M. Ultrasound affects distribution of plasminogenand tissue-type plasminogen activator in whole blood clots in vitro.Thromb Haemost 2004;92:980–985.
Diamond SL, Anand S. Inner clot diffusion and permeation duringfibrinolysis. Biophys J 1993;65:2622–2643.
Everbach EC, Francis CW. Cavitational mechanisms in ultrasound-accelerated thrombolysis at 1 MHz. Ultrasound Med Biol 2000;26:1153–1160.
Fatar M, Stroick M, Griebe M, Alonso A, Hennerici MG, DaffertshoferM. Brain temperature during 340-kHz pulsed ultrasound in-sonation: A safety study for sonothrombolysis. Stroke 2006;37:1883–1887.
Francis CW, Onundarson PT, Carstensen EL, Blinc A, Meltzer RS,Schwarz K, Marder VJ. Enhancement of fibrinolysis in vitro byultrasound. J. Clin Invest 1992;90:2063–2068.
Francis CW, Blinc A, Lee S, Cox C. Ultrasound accelerates of recom-binant tissue plasminogen activator into clots. Ultrasound Med Biol1995;21:419–424.
Holland CK, Vaidya SS, Coussios C-C, Shaw GJ. Thrombolytic effectsof 120-kHz and 1-MHz ultrasound and tissue plasminogen activatoron porcine whole blood clots. J Acoust Soc Am 2002;112:2370.
Holland CK, Vaidya SS, Datta S, Coussios C-C, Shaw GJ. Ultrasound-enhanced tissue plasminogen activator thrombolysis in an in vitroporcine clot model. Thromb Res 2007;in review.
Lauer CG, Burge R, Tang DB, Bass BG, Gomez ER, Alving BM.Effect of ultrasound on tissue-type plasminogen activator-induced
thrombolysis. Circulation 1992;86:1257–1264.Mizushige K, Kondo I, Ohmori K, Hirao K Matsuo H. Enhancement ofultrasound-accelerated thrombolysis by echo contrast agents: De-pendence on microbubble structure. Ultrasound Med Biol 1999;25:1431–1437.
Molina CA, Ribo M, Rubiera M, Montaner J, Santamarina E, Delgado-Mederos R, Arenillas JF, Huertas R, Purroy F, Delgado P, Alvarez-Sabin J. Microbubble administration accelerates clot lysis duringcontinuous 2-MHz ultrasound monitoring in stroke patients treatedwith intravenous tissue plasminogen activator. Stroke 2006;37:425–429.
The National Institute of Neurological Disorders and Stroke rt-PAStroke Study Group. Tissue plasminogen activator for acute isch-emic stroke. N Engl J Med 1995;333:1581–1588.
Nedelmann M, Eicke BM, Lierke EG, Heimann A, Kempski O, HopfHC. Low-frequency ultrasound induces nonenzymatic thromboly-sis in vitro. J Ultrasound Med 2002;21:649–656.
Nedelmann M, Brandt C, Schneider F, Eicke BM, Kempski O, Krum-mernauer F, Dieterich M. Ultrasound-induced blood clot dissolu-tion without a thrombolytic drug is more effective with lowerfrequencies. Cerebrovasc Dis 2005;20:18–22.
Onundarson PT, Francis CW, Marder VJ. Depletion of plasminogen invitro or during thrombolytic therapy limits fibrinolytic potential.J Lab Clin Med 1992;120:120–128.
Pieters M, Hekkenberg RT, Barrett-Bergshoeff M, Rijken DC. Theeffect of 40 kHz ultrasound on tissue plasminogen activator-in-duced clot lysis in three in vitro models. Ultrasound Med Biol 2004;30:1545–1552.
Porter TR, LeVeen RF, Fox R, Kricsfeld A Xie F. Thrombolyticenhancement with perfluorocarbon-exposed sonicated dextrose al-bumin microbubbles. Am Heart J 1996;132:964–968.
Porter TR, Kricsfeld D, Lof J, Everbach EC Xie F. Effectiveness oftranscranial and transthoracic ultrasound and microbubbles in dis-solving intravascular thrombi. J Ultrasound Med 2001;20:1313–1325.
Prokop AF, Soltani A Roy RA. Cavitational mechanisms in ultrasound-accelerated fibrinolysis. Ultrasound Med Biol 2007;33:924–933.
Sakharov DV, Hekkenberg RT, Rijken DC. Acceleration of fibrinolysisby high frequency ultrasound: The contribution of acoustic stream-ing and temperature rise. Thromb Res 2000;100:333–340.
Shaw GJ, Bavani N, Dhamija A, Lindsell CJ. Effect of mild hypother-mia on the thrombolytic efficacy of 120 kHz ultrasound enhancedthrombolysis in an in-vitro human clot model. Thromb Res 2006;117:603–608.
Siegel RJ, Atar S, Fishbein MC, Brasch AV, Peterson TM, Nagai T, PalD, Nishioka T, Chae JS, Birnbaum Y, Zanelli C, Luo H. Noninva-sive, transthoracic, low-frequency ultrasound augments thrombol-ysis in a canine model of acute myocardial infarction. Circulation2000;101:2026–2029.
Suchkova V, Siddiqi FN, Carstensen EL, Dalecki D, Child S, FrancisCW. Enhancement of fibrinolysis with 40 kHz ultrasound. Circu-lation 1998;98:1030–1035.
Tachibana K, Tachibana S. Albumin microbubble echo-contrast mate-rial as an enhancer for ultrasound accelerated thrombolysis. Circu-lation 1995;92:1148–1150.
Trusen B, Ries M, Zenker M, Rauh M, Beinder E, Keuper H, Harms D.Whole blood clot lysis in newborns and adults after adding differentconcentrations of recombinant tissue plasminogen activator (rt-PA). Sem Thromb Hemost 1998;24:599–604.
Xie F, Tsutsui JM, Lof J, Unger EC, Johanning J, Culp WC, MatsunagaT, Porter TR. Effectiveness of lipid microbubbles and ultrasound in
declotting thrombosis. Ultrasound Med Biol 2005;31:979–985.