Embed Size (px)
Citation preview

U L T R A S O U N DC L I N I C S
Ultrasound Clin 1 (2006) 457–469
457
Renal Failure in Neonates, Infants,and Children: The Role of UltrasoundMichael Riccabona, MD
- Imaging modalities- The use of imaging in typical pediatric
diseases and common clinical queries- Intrinsic renal conditions
Renal vein thrombosisCongenital hypodysplasiaHemolytic uremic syndrome
- Postrenal conditions- Prerenal conditions- Renal transplantation- Follow-up evaluation- Summary- References
Renal failure is a serious, acute or chronic, revers-ible or irreversible, total or partial loss of excretoryrenal function with potentially deleterious se-quelae, that unresolved may lead to dialysis or theneed for renal transplantation. Pathophysiologi-cally, there are three major causes:
� Intrinsic RF with a disease process affectingthe kidney itself
� Postrenal RF, usually secondary to obstruc-tive uropathy
� Prerenal RF secondary to a systemic or extra-renal disease without an essential intrinsickidney problem
There are some situations in which more than oneaspect is present or otherwise cannot be strictly clas-sified according to these categories: systemic lupuserythematosus (SLE) with renal involvement andRF; hemolytic uremic syndrome (HUS) with RF sec-ondary to bacterial or viral toxins and tubular con-gestion by hemolysis; hepatorenal syndrome; renalperfusion restriction in severe (bilateral) renal arterystenosis (RAS); traumatic renal vascular injury (tear,
1556-858X/06/$ – see front matter ª 2006 Elsevier Inc. All righultrasound.theclinics.com
dissection, embolus); or crush kidneys with RFcaused by tubular obstruction by myoglobin.
Clinically one can observe increased blood pres-sure and oliguria or anuria. Polyuria may precedeor follow these stages, producing so-called ‘‘polyu-ric RF.’’ Additionally there may be more or less gen-eralized edema secondary to fluid overload orprotein deficiency. Diagnosis is based on laboratoryfindings with elevated serum creatinine levels, elec-trolyte disturbances, low protein or albumin levels,and metabolic disturbances (such as acidosis). Ad-ditional symptoms or findings may be secondaryto fluid overload (eg, hypertension, cardiomegalyand cardiac insufficiency, ascites, or pleural effu-sion) and metabolic problems (eg, tachypnea insevere acidosis).
Treatment options vary depending on the under-lying condition, with supportive measures such asfluid and electrolyte balancing and hemofiltrationbeing common. Treating systemic conditions andrestoring circulation is necessary to overcome prere-nal RF, and relief of obstruction is the treatment inpostrenal RF. Intrinsic RF in general offers fewer
Department of Radiology, Division of Pediatric Radiology, University Hospital, LKH A–8036 Graz,Auenbruggenplatz, AustriaE-mail address: [email protected]
ts reserved. doi:10.1016/j.cult.2006.05.004

Riccabona458
treatment options, such as diet and fluid balance,antibiotics (in post- or parainfectious GN), steroidsin some GN entities or nephritic and nephrotic syn-drome (NS), and cytotoxic or immunosuppressivemedication (eg, cyclophosphamide or cyclosporinein some forms of GN or NS).
In RF the role of imaging (and of US in particu-lar) is initially to help differentiate acute fromchronic and prerenal from postrenal or intrinsicRF. In some conditions, US can offer a treatment ap-proach (eg, PCN, placing central lines for monitor-ing and dialysis), can assess the kidney duringfollow-up (eg, assessment of the amount of dilata-tion or by serial evaluation of renal perfusion usingDoppler sonography [DS]), and can help establishthe histologic diagnosis by offering a safe biopsy ap-proach. US may also be helpful in evaluation ofcomplications during the course of renal disease,to follow renal development and growth after re-covery, or to check for sequelae and progressionof a chronic disease under long-term treatment.
As this review focuses on pediatric US, severalspecific aspects important for diagnosis in neo-nates, infants, and children have to be mentioned.The neonatal kidney is still immature and thus onUS appears different from a normal adult kidney.Normal creatinine levels change with age (normalin newborns, <0.5 mg/dL) because of increasing re-nal maturation, different metabolism, and growingbody size. Different diseases occur than in adults:vascular disease is rare, although congenital malfor-mations with renal hypodysplasia or autosomal re-cessive polycystic kidney disease (ARPKD) withearly progression are more important in this agegroup. Sensitivity to radiation is higher in children,thus radiation-sparing imaging is even more impor-tant than in adults. Communication is different andthere may be reduced patient cooperation. The dif-ferent physiology and the different tissue composi-tion (less fat and fibrous components) and thesmall size, different anatomic relations, and higherheart and respiration rates need technically differ-ent imaging equipment (high temporal and spatialresolution, different transducers) and cause differ-ent imaging appearances. All of these factors neces-sitate adapted imaging algorithms. This requiresspecial knowledge and training and a dedicated in-frastructure, because infants require different han-dling than do adults (eg, swaddling facilities,breastfeeding room, pacifiers, heating, and placefor accompanying or assisting persons).
The aim of this article is to briefly list the variousimaging modalities applicable in pediatric RF, to re-flect on the task of imaging in infants and childrenwith RF, and then to discuss the potential of US inpediatric RF with special regard to effective use ofimaging.
Imaging modalities
Imaging is primarily based on US, supplemented byplain film, fluoroscopy, scintigraphy, and MR imag-ing in specific conditions and queries.
Ultrasound is the generally accepted basic imag-ing tool in RF. For a long time, however, US wasseen as a ‘‘roughly orienting’’ method that allowedfor depiction of collecting system dilatation or uri-nary tract malformations, but it did not offer anymore detailed information. This started to changeinitially with the advent of DS, then color Dopplersonography (CDS) and particularly amplitude-coded CDS (aCDS). These tools enabled assessmentof renal perfusion and helped in differentiatingvarious conditions, such as prerenal failure, focalrenal lesions, or renal vein thrombosis [1–3]. Gray-scale imaging was then improved by the introduc-tion of high-resolution US, image compounding,and harmonic imaging [3–6]. Upcoming tech-niques, such as intravenous US contrast agents, to-gether with refined sonographic contrast depictioncapabilities, will further enhance US potential, mak-ing US a comprehensive, noninvasive, portable im-aging tool that allows for anatomic and functional(ie, perfusion, vesicoureteral reflux [VUR]) evalua-tion of the urinary tract [3,7–12]. US thus has be-come the major imaging tool for pediatric RF.
Plain films are rarely useful or indicated in pa-tients who have RF. Evaluation of systemic sequelae,assessment of central line position, or the initial di-agnostic evaluation, however, often require a chestfilm, and diagnosing some underlying conditionssuch as urolithiasis still may require a plain film[13]. Note that film speed and exposure need tobe adapted to age and weight and that digital radi-ography may lack sufficient resolution, particularlyin neonates and infants. Fluoroscopy is applied inVCUG for diagnosing PUV or VUR with associatedrenal dysplasia and in angiography or intervention-al procedures, such as PCN [14–17].
The value of CT is limited in the pediatric urinarytract and in particular in RF, because RF is a contra-indication for the use of intravenous contrast mate-rial required in most pediatric urinary tract queries[18–20]. The primary indication for CT in the pedi-atric urinary tract is major trauma or work-up of re-nal tumors and tumorlike lesions, usually notpresenting with RF and as such beyond the scopeof this article.
The two other major imaging players in RF arescintigraphy and, increasingly, MR imaging. Staticrenal scintigraphy (Tc99m DMSA) is used for evalu-ating overall and split renal function. Diureticdynamic renal scintigraphy (Tc99m MAG3) is con-sidered the gold standard for assessment and grad-ing of obstructing uropathy. MRI has successfully
Ultrasound Role in Renal Failure in Children 459
been introduced into pediatric uroradiology[21–28]. New technical refinements and sequencemodifications promise to widen the potential ofMR urography (MRU) to become a comprehensive‘‘all in one’’ imaging tool, offering not only ana-tomic assessment but additionally providing de-tailed and quantitative functional information.MR contrast material may be given in RF becauseof its reduced nephrotoxicity, allowing assessmentof renal perfusion and residual function. Diffu-sion-weighted imaging and new intracellular con-trast materials promise to open yet unexploreddiagnostic fields for imaging diagnosis and prog-nostic assessment.
The use of imaging in typical pediatricdiseases and common clinical queries
Severe pediatric RF is a rare but serious and life-threatening condition that needs urgent diagnosisand treatment. The differential diagnoses of neona-tal RF include [29–35]:
� Intrinsic renal diseases, such as severe uri-nary tract infection, renal vein thrombosis,hypoxic and toxic renal parenchymal damage(including treatment- or drug-induced), con-genital hypodysplasia, bilateral renal agene-sis, ARPKD, congenital NS, syndromaticnephropathies, and neonatal GN
� Postrenal problems caused by bilateral severeobstructing uropathy (ie, PUV, megaureterwith uretero-vesicle junction obstruction,and uretero-pelvic junction obstruction)
� Prerenal RF caused by systemic problems,such as septicemia and multiorgan systemfailure, heart disease (particularly PDAand aortic coarctation), hypotension andhypovolemia (eg, after placental bleeding oruterine rupture), or dehydration andhyperviscosity
In older children, RF may evolve because of anunderlying chronic condition, some of them
syndromal or hereditary (eg, reflux nephropathy,[RNP]), juvenile nephronophthisis, or Alport syn-drome), and subsequent chronic RF is more com-mon. Additional intrinsic renal diseases that maycause acute RF entities have to be considered:HUS, NS, para- or postinfectious GN, tubular renalacidosis (or oxalosis and cystinosis) with consecu-tive progressive nephrocalcinosis, various tubulo-pathies, renal involvement in systemic diseasessuch as in Henoch-Schonlein disease or SLE, ortoxic- and drug-induced RF (ie, herbs and fungus,chemotherapy, antibiotics, or intravenous iodin-ated contrast agents) [20,36–42]. Furthermore,acute obstruction caused by urinary tract calculusor an abdominal tumor, renal destruction by tu-mors, or chronic infections, such as xanthogranu-lomatous pyelonephritis, and traumatic RF (eg,bladder rupture, crush kidney, or vascular injury)need to be mentioned as rare causes for pediatricRF to complete the list. Looking at all these entities,it becomes obvious that a thorough and detaileddiscussion of these diseases would fill a book andthus is beyond the scope of this brief overview. Mostnephropathies, however, have similar or even iden-tical imaging appearances. The author focuses onlyon modern US features in typical neonatal and pe-diatric conditions.
Intrinsic renal conditions
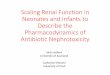
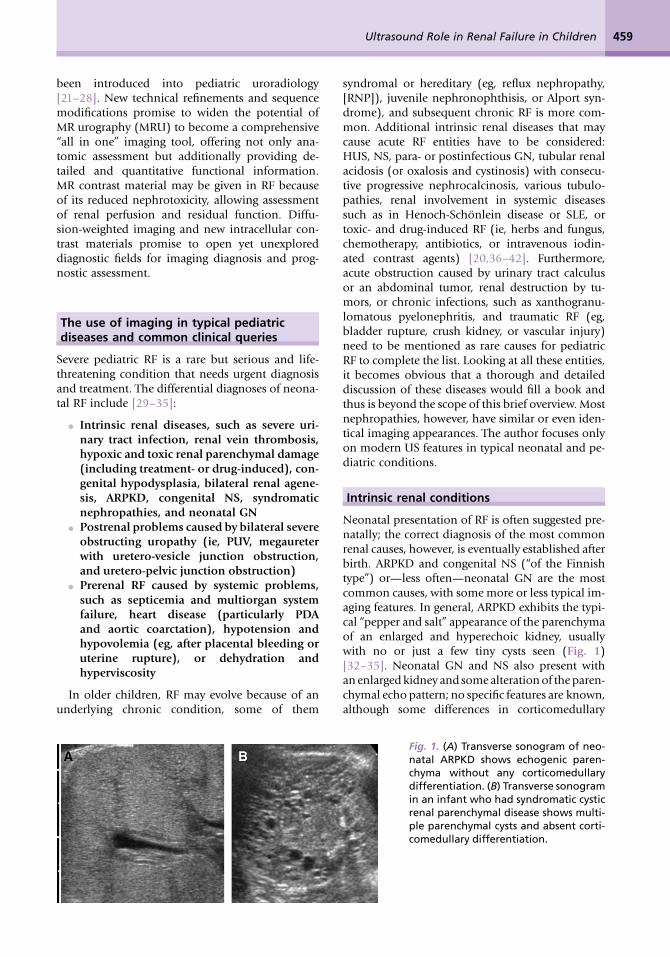
Neonatal presentation of RF is often suggested pre-natally; the correct diagnosis of the most commonrenal causes, however, is eventually established afterbirth. ARPKD and congenital NS (‘‘of the Finnishtype’’) or—less often—neonatal GN are the mostcommon causes, with some more or less typical im-aging features. In general, ARPKD exhibits the typi-cal ‘‘pepper and salt’’ appearance of the parenchymaof an enlarged and hyperechoic kidney, usuallywith no or just a few tiny cysts seen (Fig. 1)[32–35]. Neonatal GN and NS also present withan enlarged kidney and some alteration of the paren-chymal echo pattern; no specific features are known,although some differences in corticomedullary
Fig. 1. (A) Transverse sonogram of neo-natal ARPKD shows echogenic paren-chyma without any corticomedullarydifferentiation. (B) Transverse sonogramin an infant who had syndromatic cysticrenal parenchymal disease shows multi-ple parenchymal cysts and absent corti-comedullary differentiation.

Riccabona460
differentiation and in the amount and pattern ofechogenicity changes have been noted to be morecommon in some diseases [34,35,43]. Even DSfindings (reduced peripheral vasculature on aCDS,increased or decreased RI or velocities on DDS)are nonspecific and correspond better with renalfunction (degree of renal failure, modulated bytherapeutic aspects such as fluid load, drugs, bloodpressure modulation, and heart rate) than with theunderlying disease entity. This is also valid in otherforms of GN or NS as seen in older children, such aspara- and postinfectious GN, Henoch-Schonleinnephritis and IgA-nephropathy, lupus nephritis, or(familial) NS (Fig. 2) [3,38,40,41]. Usually kidneysize is enlarged or normal, and US appearance
depends on the relative echogenicity of the cortexand the parenchyma. Corticomedullary differentia-tion thus depends on whether both or only one ofthese structures is affected, how much each of themare affected and may be increased or decreased, orsometimes are even normal in mild disease. TheUS appearances are thus rather nonspecific, andthe value of US in these patients is not to specifya certain disease (although some suggestions con-cerning the underlying disease may be achievable),but rather to (1) rule out other potential causes forRF, (2) assess the amount of pleural effusion or as-cites and intravascular fluid load for balancing sup-portive measures, and (3) assess extrarenal diseaseaspects.
Fig. 2. (A) Unspecific renal parenchymal changes in severe Lupus nephritis. (B) Significantly reduced peripheralrenal perfusion in aRF shown by aCDS. (C) Reduced perfusion of the renal cortex (cursors) becomes even moreobvious when compared with the aCDS vascularity of the adjacent spleen. (D) Transverse sonogram througha right kidney in NS. (E) Peripherally reduced vasculature on aCDS (halo sign) indicating restricted peripheral re-nal perfusion.

Ultrasound Role in Renal Failure in Children 461
Renal vein thrombosis
Renal vein thrombosis mostly occurs in neonateswho have adrenal gland hemorrhage, coagulopa-thies, femoral central lines, or dehydration and pol-yglobulic syndrome [3,44–46]. Note that unilateralrenal vein thrombosis usually presents with hyper-tension and hematuria and should not lead toglobal RF except for single systems or coexisting im-pairment of the other kidney. In neonates, throm-bosis usually starts in the peripheral veins, only
gradually growing into the central veins, behavingsimilarly to tumor thrombi (Fig. 3A). In older chil-dren, extrarenal origin of thrombosis or a primarythrombus of the major renal vein is more common.The basic and often single imaging tool is US, dem-onstrating a large, swollen, and hyperechoic kidneywith undifferentiated parenchyma (Fig. 3B). OnCDS, renal vein color signals are missing in the af-fected veins, although they may be demonstrablein patent central veins. DDS shows increased
Fig. 3. (A) Transverse sonogram showing renal vein thrombus (between cursors) reaching into the IVC. (B) Lon-gitudinal image showing a swollen kidney with hazy corticomedullary differentiation in neonatal renal veinthrombosis. Note the secondary ascites (A). (C) Longitudinal aCDS image demonstrates regionally diminishedperfusion in partial/peripheral neonatal renal vein thrombosis. CDS with DDS trace depicts the (D) increasinglyreduced and then (E) reversed diastolic flow with elevated RI.

Riccabona462
arterial resistance with high resistive indices (RI)and low or missing diastolic flow (Fig. 3C–E). Onfollow-up—even with some treatment success—one often observes shrinkage of the kidney with dif-fusely abnormal echo pattern of the parenchymaand reduced perfusion. These changes sometimesonly become apparent over time, as a lack of age-concordant renal growth with contralateral com-pensatory renal hypertrophy. Usually no otherimaging is needed except for tumor conditions, inwhich MR imaging (or CT) and MR angiography(MRA) are performed for overall assessment andstaging and preoperative planning.
Congenital hypodysplasia
Congenital hypodysplasia (with RF) may be some-what difficult to diagnose. Only the most severeforms (eg, bilateral multicystic dysplastic kidney)are easily and often prenatally recognizable, thoughsometimes not compatible with extrauterine life. Asdescribed by the name, the affected kidneys usuallyare small and present an altered echotexture withreduced corticomedullary differentiation and in-creased echogenicity; cysts of varying size may bepresent (Fig. 4A). The amount of these changes de-pends on the degree of dysplasia, however, andpure hypoplasia may initially even exhibit normalUS features, with the kidney size initially rangingwithin normal limits [32–34]. Only over time doesthe size deficit perhaps become obvious and thenmay eventually correspond to developing and pro-gressive chronic RF. This entity may be difficult tobe distinguished from RNP (a term that is increas-ingly under discussion). The underlying renal pa-thology in RNP usually is a combination ofcoexisting congenital renal dysplasia with renalgrowth retardation and acquired renal damagecaused by infection and scarring associated withVUR that may have vanished by the time of diagno-sis (Fig. 4B). The ‘‘water hammer theory’’ for RNP is(postnatally) probably only valid in some patients
who have severe, long lasting, high pressure VURusually associated with bladder dysfunction.
Hemolytic uremic syndrome
HUS is a condition in which acute RF is caused bytoxins of a certain Escherichia coli strain affectingthe renal cortical and glomerular capillaries causingvasculopathy, hemolysis, and thrombosis. It is a dis-ease that may occur as familial or endemic (in cer-tain areas and populations) and incidentally,preferably affecting young patients during earlysummer. Diagnosis is assumed in case of a recent,sometimes hemorrhagic enterocolitis with acuteRF, thrombocytopenia, anemia, hypertension, andtypical erythrocyte morphology on microscopy(fragmented cells called Burr cells or schistocytes),and is confirmed by culture results. Treatment op-tions are restricted to symptomatic measures andrenal replacement therapy. Prognosis varies; in a sin-gle event a good outcome is common. In pro-longed, chronic, and recurrent disease, prognosisconcerning renal functional outcome is poorer,though mortality has been nearly eradicated. USdemonstrates bilaterally enlarged kidneys witha large, hyperechoic cortex and increased cortico-medullary differentiation (Fig. 5A,B). RI is mark-edly increased (Fig. 5C), and aCDS exhibitsdiffusely reduced cortical perfusion with a markeduncolored peripheral halo [34,39–41]. Addition-ally, US examination may demonstrate regionalbowel wall thickening and secondary signs of acuteRF and bowel inflammation. During the course ofthe disease, improvement of DDS with graduallyimproving RI values precedes clinical improvementof renal function and thus may be useful for mon-itoring and for making therapy decisions.
Eventually US can help to establish the histologicdiagnosis in intrinsic renal conditions producingRF, which may be essential for treatment decisionsand prognostic estimation, by providing safe biopsyguidance [14–17,47–49]. Here US not only helps toguide the biopsy, thus increasing safety and
Fig. 4. (A) Transverse sonogram ofthe right kidney demonstrates asmall kidney (cursors) with atypicalparenchymal structure. (B) Trans-verse sonogram of a left kidneyshows cystic defects in a neonatalkidney with increased echogenicityand reduced corticomedullary dif-ferentiation in ‘‘congenital RNP.’’

Ultrasound Role in Renal Failure in Children 463
Fig. 5. (A) Longitudinal sonogram of an enlarged right kidney demonstrates the typical US appearance of anacutely affected kidney in HUS with increased cortical echogenicity and corticomedullary differentiation. (B)Transverse CDS with duplex tracing demonstrates the markedly reduced perfusion with reversed diastolic flowand increased RI.
enabling a satisfactory specimen harvest with a min-imum of needle passes, but is also essential for post-biopsy monitoring and identification of postbiopsycomplications, such as hemorrhage, urinary tractobstruction by clots, or postbiopsy arteriovenousfistula (AVF) (Fig. 6).
Postrenal conditions
In obstructing uropathy, all features of acute orchronic urinary tract obstruction may be observed.Acute obstruction (eg, by a ureteral calculus) usuallyexhibits little dilatation, as may severe obstruction
Fig. 6. (A) US-guided biopsy with the needle (arrowheads) passing into the lower pole of the left kidney as pre-defined by the dotted needle trace of the guiding device. (B) Postbiopsy hematoma on the lower pole of the leftkidney (arrowheads), superiorly delineated by aCDS. (C) CDS depicts a postbiopsy AVF as shown by focal aliasingin the lower pole and elevated diastolic arterial flow.

Riccabona464
with subsequently deteriorated renal function. USdemonstration of dilatation of the renal collectingsystem or the ureter does not necessarily equal ob-struction. To exhibit a severely dilated system, goodurine production is needed and thus this findingmay indirectly indicate persisting renal function[31,32]. Polyuria (polyuric phase of RF, stimulateddiuresis, volume overload) and laxity of a collectingsystem (eg, in neonates or in infection) may causesome dilatation that should not be misinterpretedas urinary tract ‘‘obstruction.’’ In these conditionsRF only occurs in single obstructed systems or in bi-lateral disease (such as bilateral UPJO or PUV withbilateral obstructing or refluxing megaureter and re-nal dysplasia) (Fig. 7).
The role of US is to detect collecting system dila-tation and to suggest the cause and the level of ob-struction (urinary calculus, UPJO, accessory renalartery) (Fig. 8A,B). US may help to differentiateacute from chronic obstruction; in acute obstruc-tion DDS may reveal an asymmetrically elevatedRI at usually little dilatation and diffusely increasedechogenicity of the enlarged and swollen kidney[3,44–46,50–53]. In this setting, modern US toolssuch as aCDS, DDS, and 3D US may become help-ful. For example, the depiction of an ostial ureteraljet into the urinary bladder by CDS may demon-strate ureteral patency and the UVJ (see Fig. 7A);diffusely decreased (peripheral) renal perfusionon aCDS (halo sign) may hint toward more severe
Fig. 7. (A) Transverse CDS through the lower pelvis and urinary bladder demonstrates a right ostial ureteric jet,with lack of depictable urine inflow into the bladder on the left side caused by a distal ureteral calculus. (B) The‘‘twinkling sign’’: CDS demonstrates twinkling color signals within the distal ureter at the ureterovesical junctioncaused by a small distal ureteral calculus in the same patient as seen in (A). (C) Echo-enhanced urosonography(A). Initial longitudinal sonogram shows a dilated ureter (U) posterior to the urinary bladder (B). After instilla-tion of Levovist into the prefilled urinary bladder, VUR is seen as echogenic material in the dilated distal ureter(U). Furthermore, the initially narrow renal pelvis of the corresponding kidney (C) becomes markedly dilated andfilled with US contrast material (D), indicating high-grade VUR. (D) Longitudinal perineal US demonstrating PUV(arrow) with the typical dilated bladder neck appearance. B, bladder; A, anal canal. (E) 3D US in hydronephrosis:outlining of outer renal contour (green line) for volume calculation in three orthogonal sections, with deduc-tion of the segmented dilated collecting system as visualized in the right lower box for estimation of renal pa-renchymal volume.

Ultrasound Role in Renal Failure in Children 465
Fig. 8. (A) Longitudinal sonogram demonstrates marked dilatation of the collecting system with a kink at thepelviureteric junction and a megaureter (U). (B) Longitudinal CDS sonogram in a kidney with dilated renal pelvisdepicts an additional renal artery crossing the ureteropelvic junction and potentially causing obstruction.
conditions; the ‘‘twinkling sign’’ on CDS improvesdetection of ureteral calculi (see Fig. 7B); perinealUS may enable detection of a PUV (see Fig. 7C);echo-enhanced urosonography may enable differ-entiation of refluxing versus obstructing uropathy(see Fig. 7D); and relative renal parenchymal vol-ume assessment by 3D US may help estimate splitrenal parenchymal size (see Fig. 7E) [3,4,6–12].
In severe obstruction or pyohydronephrosis, USis the ideal imaging modality to guide percutaneousnephrostomy (PCN), potentially complimented byfluoroscopy for comprehensive visualization of theentire collecting system anatomy and for detectionof potential extravasations [10,14,15,17]. Note thatindications for operation and PCN have changedover the past decade; now only severe conditionswith acute threat to renal function or intractableurinary tract infection are considered indicationsfor these invasive treatment options.
Prerenal conditions
Prerenal RF is defined by an extrarenal conditioncausing renal hypoperfusion and hypoxia. The mostcommon causes are trauma with blood loss andshock or other causes of prolonged hypovolemiaand hypoxia (eg, drowning, complicated operation,asphyxia, vascular injury) and cardiac disease ormalformations, such as persisting duct of Botallo(patent ductus arteriosus) with left-to-right shunt,aortic coarctation, and heart failure. The US findingsare nonspecific, demonstrating normal kidneys(particularly in early stages) or bilaterally swollen,often diffusely hyperechoic kidneys. Perfusion alter-ations on DS, such as decreased flow velocities with‘‘pseudonormal’’ or elevated RI values, flattened sys-tolic flow curves, and pathologically delayed systolicflow acceleration can be seen (Fig. 9). US is used toassess the degree of perfusion disturbance, to find orrule out other renal conditions, to evaluate the sys-temic changes of the underlying condition, such asfree peritoneal or retroperitoneal fluid (in trauma),
cardiac function (by echocardiography), brainperfusion (by transfontanellar or transtemporalDDS), and to monitor renal perfusion as a prognos-tic indicator or for treatment guidance.
Renal transplantation
Increasingly, even small children who have terminalRF can now be treated by renal transplantation,with an improved long-term outcome and a betterlife quality compared with chronic dialysis, whichmay still be needed until a compatible transplantorgan is available. Imaging in these children isprimarily based on US. Initially, donor organs areevaluated by US before explantation. Then earlypostoperative surveillance uses serial US andDDS/CDS, particularly in evaluating transplantmalfunction (eg, tubular necrosis, early rejection,vascular problems, and obstructed urinary drain-age). Assessment of kidney size, renal parenchymalstructure, and potential dilatation of the collectingsystem is mandatory, as is visualization of the mainsupplying vessels, including a DDS and aCDS as-sessment of renal perfusion. Furthermore, evalua-tion of the vascular anastomosis is desirable todepict stenoses or aneurysm formation (Fig. 10).
During later post-transplant phases, routine USinvestigations are performed to monitor renalgrowth and to detect early stages of potential rejec-tion or (Cyclosporine-induced) vasculopathy, partic-ularly if clinical and laboratory findings indicatea potential problem. In this scenario, transplant or-gan size changes are one of the most sensitive,though unspecific, signs to detect transplant dis-ease. Additional findings in transplant disease arechanged parenchymal echogenicity and corticome-dullary differentiation, dilatation of the collectingsystem (in stenosis of ureteral anastomosis), in-creased RI values (in rejection and vasculopathy),flattened systolic flow acceleration (in renal arterystenosis, usually located near the anastomosis), re-gional venous flow turbulences (more likely in

Riccabona466
Fig. 9. (A) Normal gray scaleappearance of a neonatalright kidney, with some sur-rounding edematous softtissue. (B) aCDS demonstratesreduced peripheral vascula-ture (cursors) with a some-what patchy pattern ofvessel rarefaction. (C) CDSwith duplex tracing showsan elevated RI with a reverseddiastolic flow but a normalsystolic flow profile.
vasculopathy or partial renal vein thrombosis), AVF(after biopsies), and impaired peripheral perfusiondemonstrated by reduced peripheral color signalson aCDS (usually in significant functional impair-ment) or regional lack of aCDS-depictable perfu-sion (in segmental infarction). US, however, (andscintigraphy and MR imaging) often remains non-specific as to the disease entity, and US-guidedtransplant biopsy may become necessary for defin-itive diagnosis and further management decisions.Extrarenal complications, such as post-transplantlymphoproliferative disease, have to also be consid-ered in long-term imaging follow-up of transplantpatients.
Follow-up evaluation
Finally, follow-up is a critical aspect of managingpatients who have acute or chronic RF. US servesas a follow-up tool, allowing for noninvasive mon-itoring of renal perfusion, evaluation of collectingsystem dilatation, and assessment of renal paren-chymal growth. Even after renal transplantation or
during dialysis, the original kidneys, the urinarybladder, and the renal transplant may develop dis-ease that needs imaging, such as secondary cysticchanges, malignancy, infection, or transplant mal-function. Other imaging modalities, such as VCUG,IVU, plain film, scintigraphy, or MRU, may be indi-cated for a complete work-up of the underlyingcondition, particularly preoperatively and in com-plex urogenital malformations. Similarly, followingpatients who have chronic RF also may require theuse of other imaging modalities, such as plain filmor MR imaging, for diagnosis of systemic sequelaeor treatment complications, such as hypertensionand cardiomyopathy or osteonecrosis during ste-roid treatment.
Summary
US is the ideal and often single imaging modality ininfants and children who have acute or chronic RF.Modern US tools and US-guided renal biopsy offerextended diagnostic capabilities, eventually en-abling a safe histologic definition of a nephropathy

Ultrasound Role in Renal Failure in Children 467
Fig. 10. (A) Extended field of viewtechnique to properly cover theentire kidney for reliable lengthmeasurement not achievable bya conventional single US image, ifa large organ is located close tothe skin. (B–D) Aneurysm (arrow-heads) of a venous patch at theanastomosis of the transplant’s mainrenal artery, visualized by (B) con-ventional US and (C) CDS, confirmedby (D) MRA.
raphy for diagnosis. Radiology 1999;210:201–7.
that cannot be sufficiently diagnosed by clinical,laboratory, and imaging findings. The imaging ap-proach for children who have RF thus heavily relieson US as the primary imaging modality. It alwaysstarts with an initial US study (including DDSand CDS) to differentiate pre-, post-, or intrarenalorigin of RF and to assess the severity of renal perfu-sion (and thus functional) impairment. Uncom-monly, other imaging techniques, such as plainfilm, scintigraphy, or MR imaging are necessaryfor initial assessment and therapeutic decisions,depending on the initial US results, the generalpatient condition, and the underlying disease.Follow-up imaging assessment is primarily by US(focused on renal size, parenchyma, and perfu-sion), often complemented by scintigraphy (or, inthe future, increasingly by MR imaging) to assessoverall renal function and parenchymal scarring.Occasionally, specific diseases or complicationsmay indicate additional imaging; some conditionsmay be diagnosed or managed by US-guidedinterventions.
Modern US techniques, a US facility and equip-ment adapted and suited for pediatric needs, spe-cific knowledge, and education are compulsory tomake the utmost use of the great potential of US.Children are not just small adults, but present
specific diseases and different imaging appearances,and deserve special, focused, and skilled care.
References
[1] Riccabona M, Schwinger W, Ring E, et al. Ampli-tude coded color Doppler sonography in pediat-ric renal disease. Eur Radiol 2001;11:861–6.
[2] Riccabona M. Pediatric ultrasound. I. Abdomen.Eur Radiol 2001;11:2354–68.
[3] Riccabona M. Potential of modern sonographictechniques in paediatric uroradiology. Eur J Ra-diol 2002;43:110–21.
[4] Aytac SK, Ozcan H. Effect of color Doppler sys-tem on the twinkling sign associated with uri-nary tract calculi. J Clin Ultrasound 1999;27:433–9.
[5] Bartram U, Darge K. Harmonic versus conven-tional ultrasound imaging of the urinary tractin children. Pediatr Radiol 2005;35:655–60.
[6] Cehfouh N, Grenier N, Higueret D. Characteriza-tion of urinary calculi: in vitro study of twinklingartifact revealed by color-flow sonography. Am JRadiol 1998;171:1055–60.
[7] Darge K, Troger J, Duetting T, et al. Reflux inyoung patients: comparison of voiding US ofthe bladder and the retrovesical space withechoenhancement versus voiding cystourethrog-

Riccabona468
[8] Darge K, Moeller RT, Trusen A, et al. Diagnosisof vesicoureteric reflux with low-dose contrast-enhanced harmonic ultrasound imaging. PediatrRadiol 2005;35:73–8.
[9] Riccabona M, Uggowitzer M, Klein E, et al. Con-trast enhanced color Doppler sonography inchildren and adolescents. J Ultrasound Med2000;19:783–8.
[10] Riccabona M, Mache CJ, Lindbichler F. Echo-enhanced color Doppler cystosonography ofvesico-ureteral reflux in children: improvementby stimulated acoustic emission. Acta Radiol2003;44:18–23.
[11] Riccabona M, Fritz G, Ring E. Potential applica-tions of three-dimensional ultrasound in the pe-diatric urinary tract: pictorial demonstrationbased on preliminary results. Eur Radiol 2003;13:2680–7.
[12] Riccabona M, Fritz GA, Schollnast H, et al. Hy-dronephrotic kidney: pediatric three-dimension-al US for relative renal size assessment–initialexperience. Radiology 2005;236:276–83.
[13] Riccabona M, Lindbichler F, Sinzig M. Conven-tional imaging in paediatric uroradiology. Eur JRadiol 2002;43:100–9.
[14] Riccabona M, Sorantin E, Hausegger K. Imagingguided interventional procedures in paediatricuroradiology—a case-based overview. Eur J Ra-diol 2002;43:167–79.
[15] Riccabona M. Interventional uroradiology inpaediatrics: a potpourri of diagnostic and thera-peutic options. Minerva Pediatr 2004;56:497–505.
[16] Riccabona M, Mache CJ, Dell’Acqua A, et al. Re-nal biopsy. In: Fotter R, editor. Pediatric uroradi-ology. Berlin–Heidelberg–New York: Springer;2001. p. 272–4.
[17] Stanely P, Diamet MJ. Pediatric percutaneousnephrostomy: experience with 50 patients. J Urol1986;135:1223–6.
[18] Marcos SK. Contrast media induced nephrotoxi-city—questions and answers. Br J Radiol 1998;71:357–65.
[19] Maudgil DD, McHugh K. The role of CT in mod-ern pediatric uroradiology. Eur J Radiol 2002;43:129–38.
[20] Murphy SW, Barrett BJ, Parfrey PS. Contrast ne-phropathy. J Am Soc Nephrol 2000;11:177–82.
[21] Avni FE, Nicaise N, Hall M, et al. The role of MRimaging for the assessment of complicated du-plex kidneys in children: preliminary report. Pe-diatr Radiol 2001;31:215–23.
[22] Borthne A, Nordshus T, Reiseter T, et al. MR ur-ography: the future gold standard in paediatricurogenital imaging? Pediatr Radiol 1999;29:694–701.
[23] Borthne A, Pierre-Jerome C, Nordshus T, et al.MR urography in children: current status and fu-ture development. Eur Radiol 2000;10:503–11.
[24] Riccabona M, Simbrunner J, Ring E, et al. Feasi-bility of MR-urography in neonates and infants
with anomalies of the upper urinary tract. EurRadiol 2002;12:1442–50.
[25] Riccabona M. Pediatric MRU—its potential andits role in the diagnostic work-up of upper uri-nary tract dilatation in infants and children.World J Urol 2004;22:79–87.
[26] Rohrschneider WK, Haufe S, Wiesel M, et al.Functional and morphologic evaluation of con-genital urinary tract dilatation by using com-bined static-dynamic MR urography: findingsin kidneys with a single collecting system. Radi-ology 2002;224:683–94.
[27] Rohrschneider WK, Hoffend J, Becker K, et al.Combined static-dynamic MR urography forthe simultaneous evaluation of morphologyand function in urinary tract obstruction. I. Eval-uation of the normal status in an animal model.Pediatr Radiol 2000;30:511–22.
[28] Sigmund G, Stoever B, Zimmerhackl LB, et al.RARE-MR-urography in the diagnosis of upperurinary tract abnormalities in children. PediatrRadiol 1991;21:416–20.
[29] Bratton VS, Ellis EN, Seibert JT. Ultrasonographicfindings in congenital nephrotic syndrome. Pe-diatr Nephrol 1990;4:515–6.
[30] Feitz WFJ, Cornellissen EAM, Blickman JG. Renaldisease and renal failure. In: Carty H, Brunelle F,Stringer DA, et al, editors. 2nd edition, Imagingchildren, Vol. 1. Edinburgh-London-New York-Oxford-Philadelphia-St. Louis-Sydney-Toronto:Elsevier; 2005. p. 617–42.
[31] Gordon I, Barratt TM. Imaging the kidneys andurinary tract in the neonate with acute renal fail-ure. Pediatr Nephrol 1987;1:321–9.
[32] Gordon I, Riccabona M. Investigating the new-born kidney—update on imaging techniques.Semin Neonatol 2003;8:269–78.
[33] Riccabona M, Ring E. Renal agenesis, dysplasia,hypoplasia and cystic diseases of the kidney.In: Fotter R, editor. Pediatric uroradiology.Berlin-Heidelberg-New York: Springer; 2001.p. 229–52.
[34] Riccabona M, Mache CJ, Dell’Aqua A, et al. Renalparenchymal disease. In: Fotter R, editor. Pediat-ric uroradiology. Berlin-Heidelberg-New York:Springer; 2001. p. 253–80.
[35] Ring E, Fotter R. The newborn with oligoanuria.In: Fotter R, editor. Pediatric uroradiology.Berlin-Heidelberg-New York: Springer; 2001.p. 313–20.
[36] Cameron JS. Lupus nephritis. J Am Soc Nephrol1999;10:413–24.
[37] Chesney RW. The idiopathic nephrotic syn-drome. Curr Opin Pediatr 1999;11:158–61.
[38] Gershen RS, Brody AS, Duffy LC, et al. Prognos-tic value of sonography in childhood nephroticsyndrome. Pediatr Nephrol 1994;8:76–8.
[39] Choyke PL, Grant EG, Hoffer FA, et al. Corticalechogenicity in the hemolytic uremic syndrome:clinical correlation. J Ultrasound Med 1988;7:439–42.

Ultrasound Role in Renal Failure in Children 469
[40] Garel L, Habib R, Babin C, et al. Hemolytic uremicsyndrome. Diagnosis and prognostic value of ul-trasound. Ann Radiol (Paris) 1983;26:169–74.
[41] Patriquin HB, O’Regan S, Robitaille P, et al.Hemolytic-uremic syndrome: intrarenal arterialDoppler patterns as a useful guide to therapy.Radiology 1989;172:625–8.
[42] Repetto HA. Epidemic hemolytic-uremic syn-drome in children. Kidney Int 1997;52:1708–19.
[43] Salame H, Damry N, Vandenhoudt K, et al. Thecontribution of ultrasound for the differential di-agnosis of congenital and infantile nephroticsyndrome. Eur Radiol 2003;13:2674–9.
[44] Errington ML, Hendry GM. The rare associationof right adrenal haemorrhage and renal veinthrombosis diagnosed with duplex ultrasound.Pediatr Radiol 1995;25;157–8.
[45] Hibbert J, Howlett DC, Greenwood KL, et al. Theultrasound appearances of neonatal renal veinthrombosis. Br J Radiol 1997;70:1191–4.
[46] Wright NB, Blanch G, Walkinshaw S, et al. Ante-natal and neonatal renal vein thrombosis: newultrasonic features with high frequency trans-ducers. Pediatr Radiol 1996;26:686–9.
[47] Gainza FJ, Minguela I, Lopez-Vidaur I, et al. Eval-uation of complications due to percutaneous
renal biopsy in allograft and native kidneys withcolor-coded Doppler sonography. Clin Nephrol1995;43:303–8.
[48] Obek SS, Memis A, Killi R, et al. Image directedand color Doppler ultrasonography in the diag-nosis of postbiopsy arteriovenous fistula of na-tive kidneys. J Clin Ultrasound 1995;23:239–42.
[49] Riccabona M, Schwinger W, Ring E. Arteriove-nous fistula after renal biopsy in children. J Ul-trasound Med 1998;17:505–8.
[50] Kessler RM, Quevedo H, Lankau CA, et al. Ob-structive vs. nonobstructive dilatation of the re-nal collecting system in children: distinctionwith duplex sonography. Am J Roentgenol1993;160:353–7.
[51] Miletic D, Fuckar Z, Sustic A, et al. Resistance andpulsatility indices in acute renal obstruction.J Clin Ultrasound 1998;26:79–84.
[52] Riccabona M, Ring E, Fueger G, et al. Dopplersonography in congenital ureteropelvic junctionobstruction and congenital multicystic kidneydisease. Pediatr Radiol 1993;23:502–5.
[53] Vade A, Dudiak C, McCarthy P, et al. Resistiveindices in the evaluation of infants with obstruc-tive and nonobstructive pyelocaliectasis. J Ultra-sound Med 1999;18:357–61.