Embed Size (px)
Citation preview

UK public health aspects: Impact of the pneumococcal
vaccination programme
Jim McMenamin, Eisin Shakir, Arlene Reynolds
Health Protection Scotland

What am I going to cover?• Background re pneumonia• Background re clinical spectrum of
pneumococcal disease & why burden so difficult to quantify
• Invasive Pneumococcal Disease (IPD)• Impact of the Pneumococcal Conjugate
Vaccination Programme on IPD

Pneumonia may be deadly, especially for children • More than 1.5 million children die from pneumonia each year.1 • Pneumonia is the leading cause of death among children under
5 years of age worldwide.2
• One child dies from pneumonia every 20 seconds. That’s 4,300 young lives lost every day.3
Most children who die of pneumonia live in developing countries
• An estimated 98% of children who die of pneumonia live in developing countries.4
• For every 1 child that dies of pneumonia in a developed country, more than 2000 children die of pneumonia in developing countries.4
1. Black R, Cousens S, Johnson H, et al. Global, regional, and national causes of child mortality in 2008: a systemic analysis. Lancet. 2010; 375:1969-87.2. World Health Organization. World Health Statistics 2009. Geneva: World Health Organization; 2008. http://www.who.int/whosis/whostat/EN_WHS09_Full.pdf. Accessed September 6, 2009.3. Black R, Cousens S, Johnson H, et al. Global, regional, and national causes of child mortality in 2008: a systemic analysis. Lancet. 2010; 375:1969-87.4. World Health Organization. World health statistics 2006. Geneva: World Health Organization; 2006. http://www.who.int/whosis/whostat2006.pdf. Accessed September 6, 2009.

What is pneumonia? • Pneumonia is an infection of the lungs • It causes cough and fever and can make breathing difficult. • Severe pneumonia can be deadly.
Who is most at risk?• In developing countries, children under 5 and especially under 2 years
of age are at risk, especially in the poorest communities.1
• In developed countries the elderly are often at highest risk. • Tobacco smoke and other indoor air pollution can also increase
chances of being more susceptible to pneumonia.2,3 • Some children and adults are at greater risk because they have other
illnesses, such as HIV/AIDS.4,5 People with HIV stand a much greater chance of dying from pneumonia than those who do not have HIV.6
• Children who are poorly nourished can also have weakened immune systems, putting them at higher risk of contracting pneumonia.7
1 UNICEF/WHO. Pneumonia: the Forgotten Killer of Children. Geneva: 2006. 2 U.S. Department of Health and Human Services. The Health Consequences of Involuntary Exposure to Tobacco Smoke: A Report of the Surgeon General. Atlanta, Georgia: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, Coordinating Center for Health Promotion, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2006. 3 Smith KR, Sarnet JM, Romieu I, Bruce N. Indoor air pollution in developing countries and acute lower respiratory infections in children. Thorax. 2000; 55:518-32. 4 SA Madhi, L Kuwanda, C Cutland and KP Klugman. The impact of a 9-valent pneumococcal conjugate vaccine on the public health burden of pneumonia in HIV-infected and –uninfected children. Clin Infect Dis. 2005; 40:1511-1518. 5 Feldman C. Pneumonia associated with HIV infection. Curr Opin Infect Dis. 2005; 18(2):165-70. 6 SA Madhi, K Petersen, A Madhi, A Wasas and KP Klugman. Impact of human immunodeficiency virus type I on the disease spectrum of Streptococcus pneumoniae in South African children. Pedatr Infect Dis J. 2000; 19:1131-1147.
7 Fishman SM, Caulfield LE, de Onix M, Blossner M, Hyder AA, Mullany L, et al,. Childhood and maternal underweight. In: Ezzati M, et al WHO; 2004.

What causes pneumonia?• Many organisms can cause pneumonia. • Globally, bacteria such as Hib and pneumococcus are estimated to cause more
than 50% of pneumonia deaths in children under 5 years of age.8 • Viruses and fungi can also cause pneumonia infections.9
How is pneumonia diagnosed?• In resource-poor settings, pneumonia can be diagnosed by the symptoms it
causes, including cough, fever and difficulty or fast breathing.10 • Chest X-rays and laboratory tests can also diagnose pneumonia, but these tools
are often unavailable in developing countries, especially in remote rural communities, making it more difficult to diagnose and treat pneumonia.
How is pneumonia prevented and treated?• Some pneumonia can often be prevented with vaccines against Hib and
pneumococcus.11 • Measles and pertussis (whooping cough) infections can result in pneumonia
complications, so vaccinating against these childhood diseases can prevent some pneumonia cases.12
• Inexpensive antibiotics can effectively treat pneumonia at the community level.13
8 In settings where these vaccines are not used. O’Brien K, Wolfoson L, Watt J, et al,. Burden of Disease caused by Streptococcus pneumoniae in children younger than 5 years: global estimates. Lancet. 2009; 374:893-902. 9 Mandell Lionel A, Wunderink Richard. Pneumonia. In: Fauci AS, Braunwald E, Kasper DL, Hauser SL, Longo DL, Jameson JL, Loscalzo J. Harrison’s Principles of Internal Medicine (17th ed.) New York: McGraw-Hill, 2008. http://www.accessmedicine.com. Accessed September 7, 2009. 10 World Health Organization and UNICEF. Integrated Managemenet of Childhood Illness Handbook. Geneva: World Health Organization, 2005. 11 Mahdi SA, Levine OS, Hajjeh R, Mansoor OD, Cherian T. Vaccines to prevent pneumonia and improve child survival. Bull World Health Organ. 2008; 86:365-72. 12 Mahdi SA, Levine OS, Hajjeh R, Mansoor OD, Cherian T. Vaccines to prevent pneumonia and improve child survival. Bull World Health Organ. 2008; 86:365-72. 13 Sazawal S, Black RE, Pneumonia Case Management Trials Group. Effect of pneumonia case management on mortality in neonates, infants, and pre-school children: a meta-analysis of community based trials. Lancet Infect Dis. 2003; 3:547-56.

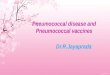
Clinical Spectrum & Burden of Pneumococcal Disease

Invasive PneumococcalDisease5924 Reported casesin 2004/05
Soft Tissue Infection (rare)
Arthritis (rare)
Sinusitis (common)
Otitis Media 1 in 3 childreneach year, 25-30% pneumococcal
Meningitis 247Reported cases in 2004/05
Pneumonia, most common cause of Community AcquiredPneumonia, 70-80,000 hospitaladmissions each year
Peritonitis (rare)
The Clinical Spectrum of Pneumococcal InfectionData relate to England and Wales in 2004/05

Source WHO Health Bulletin 2008; CI, confidence interval; DBRCT, double-blind randomized controlled trial; HibCV, Haemophilus influenzae type b conjugate vaccine; PCV, pneumococcal conjugate vaccine; USA, United States of America; VAR, vaccine attributable reduction per 1000 child years of observation; VE, vaccine efficacy based against radiologically confirmed pneumonia by use of per-protocol analysis when available.a All the studies evaluating PCV, as well as the HibCV studies in Indonesia and Bangladesh, used the WHO recommendations for interpreting and reporting on chest radiographs.23b The study from Colombia used an algorithm score which included radiologically confirmed pneumonia as one of the criteria.
Summary of pneumonia vaccine effectiveness with either conjugate
Hib or PCV

Invasive Pneumococcal Disease (IPD)
• Identification of S. pneumoniae in a normally sterile site by culture;
• Or, identification of S. pneumoniae DNA in CSF or pleural fluid by dual target PCR;
• (Or, reference laboratory identification of S. pneumoniae capsular polysaccharide and serotype-specific antigen in CSF or pleural fluid.)

IPD data linkage study 2008
HPS and ISD

Methods• Link enhanced surveillance (SPIDER) data to death
(GRO) and hospitalisation (SMR01 based on specified pneumococcal ICD9 & ICD10 codes) data– Death, prior medical conditions and clinical
manifestations– DoB, sex, surname, forename, CHI number
• Retrospective linkage 2002 to 2006• Complete dataset pre PCV-7and post PPV-23
– microbiology, clinical presentation, comorbidity, mortality
• Highly specialised and labour intensive exercise

BackgroundPrevious data linkage study
“IPD in Scotland, 1999-2001: Use of record linkage to explore associations between patients and disease in relation to future vaccination policy” Kyaw et al, CID 2003:37

What did 1999-2001 linkage tell us?
• 11.0 cases per 100,000 1999-2001• 1582 (92.2%) cases linked• <5yrs meningitis more likely• 5+yrs pneumonia and septicaemia
more likely• Incidence high in those with
underlying medical conditions

Results 2008
3515 IPD cases sent to ISD
122 duplicates
3393 IPD cases
2984 (88%) linked to GRO
409 unable to link

IncidenceIncidence of IPD in Scotland by age group 2002-2006
0
10
20
30
40
50
60
<1YR 1YR 2YR 3YR 4YR 5-14YR 15-34YR 35-64YR 65+
Age group
Inci
den
ce
Mean incidence 13.4 per 100,000
Highest in < 1year (52.6) 1 year (48.1) and >65s (34.8)

4 slides deleted as in process of submission

Impact of PCV• IPD = Isolation of Streptococcus pneumoniae from
blood, CSF or other sterile site (e.g. joint fluid)• Notifiable disease (but only since new PH act)• SPIDER surveillance scheme since 1999• Two vaccines available
– PPV-23 in 65+ years (& At risk groups)– PCV-7 (2006) then PCV-13 (2010) in childhood
immunisation schedule data• Enhanced surveillance since 2006• Impact of vaccination?

The pneumococcal conjugate vaccine (PCV) Prevenar™
•The 7 valent conjugate vaccine (Prevenar 7™) contains 7 serotypes:
– 14, 18C, 19F, 23F, 4, 6B , 9V•The 13 valent conjugate vaccine (Prevenar 13 ™) contains an additional 6 serotypes:
– 1, 3, 5, 6A, 7F, 19A
•
Over 90 serotypes of Streptococcus pneumoniae exist

Childhood immunisation uptake rates: PCV7
ScotlandQuarterly Primary Immunisation Uptake Rates by 12 Months
Mar-07 Jun-07 Sep-07 Dec-07 Mar-08 Jun-08 Sep-08
Diphtheria 96.4 96.5 96.5 96.6 96.8 96.8 97.0Tetanus 96.4 96.5 96.5 96.6 96.8 96.8 97.0
Pertussis 96.4 96.5 96.5 96.6 96.8 96.8 97.0Polio 96.3 96.4 96.4 96.6 96.8 96.8 97.0
Hib 96.2 96.3 96.3 96.4 96.7 96.7 97.0MenC 97.5 97.2 96.1 96.2 96.5 96.7 96.9
PCV .. .. 96.0 96.4 96.7 96.8 97.0
PCV was introduced in September 2006; children in this cohort should receive two doses of PCV at 2 and 4 months
Source: http://www.isdscotland.org/isd/1987.html

Childhood immunisation uptake rates: PCV7
Source: http://www.isdscotland.org/isd/1987.html
ScotlandQuarterly Primary and Booster Immunisation Uptake Rates by 24 Months
Mar-07 Jun-07 Sep-07 Dec-07 Mar-08 Jun-08 Sep-08Primary Course:
Diphtheria 97.7 97.9 98.0 98.1 98.2 98.3 98.2Tetanus 97.7 97.9 97.9 98.1 98.2 98.3 98.2
Pertussis 97.7 97.9 98.0 98.1 98.2 98.3 98.2Polio 97.6 97.8 97.9 98.0 97.9 98.1 98.1
Hib 97.3 97.6 97.6 97.7 97.6 97.8 97.8MenC 97.1 97.3 97.2 97.0 96.8 96.8 95.8
PCV .. .. .. .. .. .. 95.3MMR1 92.3 92.3 91.7 91.8 91.2 91.7 92.3
Booster:Hib/MenC .. .. .. 74.5 78.9 84.5 90.6
PCVB .. .. .. 91.0 90.6 91.8 93.0
PCV was introduced in September 2006;
children in this cohort would have been offered two doses at 2 and 4 months
and a booster dose of PCVB at around 13 months.

Seasonality of IPD
Infections peak in winter coinciding with flu season
IPD cases by financial year 1999-2009
0
20
40
60
80
100
120
140
13-16 17-20 21-24 25-28 29-32 33-36 37-40 41-44 45-48 49-52 01-04 05-08 09-12
Nu
mb
er
1999/2000
2000/2001
2001/2002
2002/2003
2003/2004
2004/2005
2005/2006
2006/2007
2007/2008
2008/2009

Number of cases and incidence of IPD 1999-2009
0100200300400
500600700800900
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
Year
Nu
mb
etr
of
case
s
02468
1012141618
Inci
den
ce p
er 1
00,0
00
po
pu
lati
on
Number of cases Incidence
• Approx 600-700 cases per year,
• Approx 11-15 cases per 100,000 population
• PPV-23 introduced in 2003, PCV-7 introduced in September 2006
Introduction of PPV-23 Introduction of PCV

Age of IPD cases reported to SPIDER
0
100
200
300
400
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
Year
Nu
mb
er o
f ca
ses
<5 yrs 5-14 yrs 15-64 yrs 65+ yrs

PPV-23 serogroups
Proportion of IPD cases caused by PPV-23 vaccine serotypes reported to SPIDER by age group, 2003-2009
60
65
70
75
80
85
90
95
100
2003 2004 2005 2006 2007 2008 2009
Year
0-4yrs
5-34yrs
35-64yrs
65+yrs

IPD Under 5’s 1999-2009
• Large reduction in numbers in vaccination age group in 2007
• Slight increase in 2008/2009
• Most common serogroups: 7F (6 cases) and 3 (4 cases)
0
10
20
30
40
50
60
70
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
Year
Inci
den
ce p
er 1
00,0
00 p
op
ula
tio
n
<2 years <5 years

• Dramatic reduction in incidence on targeted age group
IPD by age group 1999-2009
0
10
20
30
40
50
60
70
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009*
Year
Inci
den
ce p
er 1
00,0
00 p
op
ula
tio
n
<2 years <5 years 5+ years All ages

Reduction in coverage particularly in target age group
12% of cases in 2009 caused by PCV-7 serotypes
PCV7 Types trends with age group
Proportion of IPD cases caused by PCV-7 vaccine serotypes reported to SPIDER by age group, 2004-2009
0
10
20
30
40
50
60
70
80
2003 2004 2005 2006 2007 2008 2009
Year
0-4yrs 5-34yrs 35-64yrs 65+yrs

PCV-7 serotypesAll Ages

Cumulative IPD cases caused by PCV 7 serotypes reported to SPIDER 2004-2010*
0
50
100
150
200
250
300
350
1 4 7 10
13
16
19
22
25
28
31
34
37
40
43
46
49
52
Week number
Cu
mu
lati
ve c
ases
2004 2005 2006 2007 20082009 2010

Number and proportion of IPD cases caused by non-PCV serotypes, 2002-2009
0
100
200
300
400
500
600
2002 2003 2004 2005 2006 2007 2008 2009
Year
Nu
mb
er o
f ca
ses
0
10
20
30
40
50
60
70
80
90
100
Pro
po
rtio
n o
f ca
ses
Number
Proportion
Serotype replacement?

Conclusion re PCV vaccination Impact• Dramatic effect of PCV7 in reducing IPD
– Under 5’s + indirectly leading to reduction in other age groups (change in carriage…)
– Overall reduction in total IPD cases– Some evidence of serogroup replacement– Too early to say what impact will be of
PCV13 but likely further reduction in under 5’s (?will there also be an indirect effect on other age groups)

What did I cover?• Background re pneumonia • Background re clinical spectrum of
pneumococcal disease & why burden so difficult to quantify
• Invasive Pneumococcal Disease (IPD)• Impact of the Pneumococcal Conjugate
Vaccination Programme on IPD

Thank you!