-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
1/44
Pharmacology of antifungal drugs
Dr.Datten Bangun MSc.SpFK
Dept.Farmakologi & TerapeutikFakultas Kedokteran U H N
M E D A N
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
2/44
Fungal Infection in Humans =
Mycosis
Fungal Infection in Humans =
Mycosis
Major Types of Mycoses
superficial
cutaneous
subcutaneous
systemic
opportunistic
Symptoms vary from cosmetic
to life threatening
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
3/44
Fungal infectionsFungal infections
Superficial mycosesSuperficial mycoses hair, skin, mucous
membraneshair, skin, mucous membranes
egegdermatophytosisdermatophytosis (ringworm),(ringworm),
candidacandida (thrush,(thrush, intertrigointertrigo))
andand malasseziamalassezia furfurfurfur ((pityriasispityriasis
versicolorversicolor))
Subcutaneous mycosesSubcutaneous mycoses dermis,dermis,
subcutsubcut and adjacentand adjacentbonesbones egeg
mycetomamycetoma,, chromoblastomycosischromoblastomycosis,,
sporotrichosissporotrichosis
Systemic mycosesSystemic mycoses
1.1. Inhalation =>pulmonary infection=>disseminated
(Inhalation =>pulmonary infection=>disseminated
(egeghistoplasmosishistoplasmosis,,
coccidioidomycosiscoccidioidomycosis,,
blastomycosisblastomycosis))
2.2. OpportunistOpportunist aspergillusaspergillus,,
candidacandida,, crytococcuscrytococcus. Patients. Patients
compromised by disease, drugscompromised by disease, drugs
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
4/44
4
FUNGAL INFECTIONS
Incidence ; increasing trend
Slow onset
Difficult to diagnose & eradicate
Long duration of therapy
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
5/44
BackgroundBackground -- FungiFungi
3 main groups:3 main groups:
MouldsMoulds reproduce by spores, which may producereproduce by
spores, which may produce
mycotoxinsmycotoxins
YeastsYeasts grow by budding, ferment sugarsgrow by budding,
ferment sugars
Dimorphic fungiDimorphic fungi capable of changing growthcapable
of changing growth
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
6/44
Facts on Fungi
= Fungal cell membranes have a unique sterol,ergosterol, which
replaces cholesterol found inmammalian cell membranes
= Tubule proteinproduction of a different type in
microtubules formed during nuclear division.
= Chitin biosynthesis occurs in fungi.
= Most fungi have very small nuclei, with littlerepetitive
DNA.
= Mitosis is generally accomplished withoutdissolution of the
nuclear envelope.
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
7/44
Fungal cell
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
8/44
BackgroundBackground -- fungifungi
May be:May be:
= pathogenic in all exposed patients (= pathogenic in all
exposed patients (egeg
histoplasmahistoplasma capsulatumcapsulatum,,
coccidioidescoccidioides immitisimmitis))
= opportunists (= opportunists (egeg candidacandida,,
aspergillusaspergillus))
= or cause illness via= or cause illness via
mycotoxinsmycotoxins or allergicor allergic
reaction after inhalation of sporesreaction after inhalation of
spores
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
9/44
Fungal infectionsFungal infections
Risks:Risks:
= Exposure (living conditions, occupation and leisure= Exposure
(living conditions, occupation and leisure
activities), animal contact, warm climates,activities), animal
contact, warm climates,
geographygeography
= AIDS= AIDS
== ImmunosupressionImmunosupression (transplant)(transplant)
= Broad spectrum antibiotics= Broad spectrum antibiotics
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
10/44
FUNGAL INFECTIONS
SYSTEMIC
HISTOPLASMOSIS
ASPERGILLOSIS
CRYPTOCOCCOSI
BLASTOMYCOSIS
MUCORMYCOSIS CANDIDIASIS
LOCAL
DERMATOPHYTOSIS
SPOROTRICHIOSIS
ZYGOMYCOSIS
CHROMOMYCOSIS
RHINOSPOIDIOSIS
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
11/44
Common fungal infections
Pityriasis versicolor
Candidiasis : intertrigo,
paronychia , stomatitis,vulvovaginitis
Tinea: corpis, cruris,
barbae, capitis, pedis,
manum, unguium
Histoplasmosis
coccidoiomycosis
blastomycosis
cryptococcosis
aspergillosis
mucormicosis mycetoma
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
12/44
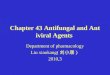
How do they work?
Image from
http://www.doctorfungus.org/thedrugs/antif_pharm.htm
Polyenes, triazoles, and imidazoles
target ergosterol destroying the cell
membranes integrity.
Allylamines inhibit ergosterol
synthesis.
-3-glucan synthase inhibitorblock
the production of the -(1,3)-glucan
protein damaging the cell wall.
Every component of the cell wall and
membrane can be targeted. Drugs not
available in the market such as
Nikkomycin and Polyoxin target chitin
synthase. Mannoproteins are another
potential target.
Other antifungals such as flucytosine
inhibit DNA/RNA synthesis and
griseofulvin inhibit fungal cell mitosis
preventing cell proliferation and
function.
ANTIFUNGAL AGENTS
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
13/44
Antifungals
Polyenes Imidazoles Triazole
nystatin
amphotericin
B
miconazole
clotrimazole
ketoconazole
fluconazole
itraconazole
voriconazole
posaconazole
Allylamines
naftifine
terbinafine
butenafine
-3-glucan
synthase
inhibitors
caspofungin
micafungin
anidulafungin
Other
griseofulvin
flucytosine
tolnaftate
Classification in GeneMedRx
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
14/44
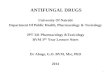
Why is this important?
36% of drugs are
metabolized by
CYP3A4and
antifungals are
largely3A4
inhibitors
Antifungals can
effect up to 60%ofall drugs due
to inhibition of
3A4, 2C9, 2C19,
1A2.Image from
http://www.doctorfungus.org/thedrugs/antif_pharm.htmImage from
http://www.doctorfungus.org/thedrugs/antif_pharm.htm
Antifungal metabolism
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
15/44
ANTIFUNGALAGENTS
SYSTEMIC ANTIFUNGALS
TOPICAL ANTIFUNGALS
Some are fungistatic,while others are fungicidal
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
16/44
PATKI 16
Systemic antifungals
1. GRISEOFULVIN
2. AMPHOTERICIN- B3. FLUCYTOSINE
4. IMIDAZOLES
5. TRIAZOLES
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
17/44
GRISEOFULVIN
FUNGISTATIC :
- MIcrosporum, Epidermophyton Trichophytons
MECHANISM : Inhibition Of Fungal Mitosis , Disruption Of
Mitotic Spindles
KINETICS : Fatty Meal & Microsized Particles -
Increases Absorption, Deposition In Keratin
Cells
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
18/44
PATKI 18
GRISEOFULVIN
INDICATIONS
Tenia Capitis,
Corporicruris Rubrum Athlets Foot
[Epidermophytosis]
DOSE-10-15 MG/Kg
ADRs-
Headache - 15%
Peripheral Neuropathy Confusion
Antabuse Reaction
Photo Sensitivity
Drug Interactions
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
19/44
AMPHOTERICINE B
= Member of polyene class of antibiotics.
= Antifungal effect due to interaction with
sterols in membrane, making membranes leaky.
= Has high affinity forergosterol, but also bindsto
cholesterol
= severe side effects.
Spectrum: ----
broad-spectrum= candida, Crypt. Blastomyces,Histoplasma,
Aspergillus.
= Limited Activity -Leishmania.
=
No Antibacterial
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
20/44
AMPHOTERICINE B
KINETICS
= No Git absorption,--- digunakan per-oral utk
infeksi jamur diusus
= 90% Bound To Proteins= Un Changed Elimination,
= Elimination Half Life-15 Days
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
21/44
Adverse drug reactions
I.Infusion related toxicity:
-chills & fever ,muscle spasm
vomitting,headache,hypotension
II. Slower toxicity:
- renal damage is the most significant toxic rx.
-bronchospasm, azotemia, hypokalemia
- Liver function abnormalities
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
22/44
Amphotericin B
Resistance
Susceptibility testing methods have not been
standardized
Development of resistance in a previously
susceptible species is uncommon
Mechanisms of Resistance
Reductions in ergosterol biosynthesis
Synthesis of alternative sterols that lessen the
ability of amphotericin B to interact with the
fungal membrane
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
23/44
INDICATIONS-DOSE-
0.5-0.6 MG/kg
mucormicosis aspergillosis
sporotrichosis
cryptococcosis
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
24/44
Flucytosine
MOA Converted by cytosine
deaminase into 5-fluorouracil
which is then converted through
a series of steps to 5-fluorouridine triphosphate and
incorporated into fungal RNA
leading to miscoding
Also converted by a series of
steps to 5-fluorodeoxyuridine
monophosphate which is a
noncompetitive inhibitor of
thymidylate synthase, interfering
with DNA synthesis
Fluorinated pyrimidine
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
25/44
Flucytosine
Spectrum of Activity
Active against
Candida species except C. krusei
Cryptococcus neoformans
Aspergillus species Synergy with amphotericin B has been
demonstrated
The altered permeability of the fungal cell membraneproduced by
amphotericin allows enhanced uptake offlucytosine
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
26/44
Flucytosine
Mechanisms of Resistance Loss of cytosine permease that permits
flucytosine to cross
the fungal cell membrane
Loss of any of the enzymes required to produce the activeforms
that interfere with DNA synthesis
Resistance occurs frequently and rapidly when flucytosine
isgiven as monotherapy
Combination therapy is necessary
Half-life:= 2 to 5 hours in normal renal function= 85 hours in
patients with anuria
Distributes into tissues, CSF, and body fluids
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
27/44
Flucytosine
Toxicities Bone marrow suppression (dose dependent)
Hepatotoxicity (dose dependent)
Enterocolitis
Toxicities occur more commonly in patients with renal
impairment
Dose Administered orally (available in 250 and 500 mg
capsules)
100 to 150 mg/kg/day in 4 divided doses
Dose adjust for creatinine clearance
Flucytosine concentrations should be monitored especially
inpatients with changing renal function
Contraindicated in pregnancy
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
28/44
AzolesKetoconazole
Have 5-membered organic rings that contain eithertwo or three
nitrogen molecules (the imidazoles
and the triazoles respectively).
= The clinically useful imidazoles are clotrimazole,
miconazole, and ketoconazole.
=Two important triazoles are itraconazole and
fluconazole. In general, the azole antifungal agents
are thought to inhibit cytochrome P450-dependent
enzymes involved in the biosynthesis of cell
membrane sterols.
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
29/44
AzolesKetoconazole
Uses
Used in U.S. as an alternative Non-albicans candidiasis
Blastomycosis
Histoplasmosis
Not for immunocompromised hosts due to high failure rate
Coccidioidomycosis
Not for meningitis or for severely ill
Paracoccidioidomycosis
Inactive against non-albicans candida and Aspergillus
Needs acidic environment for absorption
Only available PO
Distributes into epidermis, synovial fluid, saliva, and lungs.
Poordistribution into CSF and eye.
Dose
200 to 400 mg once daily
Decrease dose for severe liver failure
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
30/44
AzolesKetoconazole
Adverse Effects
GI distress (17-43%) Rash (4-10%)
Increased transaminases (2-10%)
Hepatitis (1 in 10,000)
Can be fatal if drug is not DCd
Usually occurs within first 4 months of treatment Dose-dependent
inhibition of synthesis of testosterone (5-21%
of patients will have symptoms such as impotence
orgynecomastia)
Menstrual Irregularities (16% of women)
Alopecia (8%) Dose-related decrease in cortisol synthesis
Hypermineralocorticoid state
Can cause HTN in patients on long-term high doseketoconazole
Teratogenic in animals
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
31/44
AzolesKetoconazole
Drug Interactions:=Antacids, H2 blockers, proton pump
inhibitors,sucralfate----Decreases absorption ofketoconazole
= Rifampin decreases ketoconazole concentrations
by 33%= CYP inhibition-----
Cyclosporine levels
increasedWarfarinPhenytoinMethylprednisolone
IsoniazidTerfenadineAstemizoleCisapride
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
32/44
Triazoles MOA:
Inhibits 14--sterol demethylase, which is a microsomalCYP450
enzyme.
This enzyme is responsible for conversion of lanosterolto
ergosterol, the major sterol of most fungal cellmembranes
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
33/44
TriazolesADMEFluconazole Itraconazole Voriconazole
Posaconazole
Absorption IV and PO
Goodbioavailability
PO
Capsule SuspensionCapsules best
absorbed with food.
Suspension best
absorbed on emptystomach.
IV and PO
90% oralbioavailability
PO--Absorption
enhanced withhigh fat meal
Distribution Wide.Good CNS
penetration
Low urinary levelsPoor CNS
penetration
Wide.Good CNS
penetration
Widelydistributed into
tissues
Metabolism Hepatic/Renal Hepatic CYP 2C9, 2C19,3A4
Saturablemetabolism
Not a substrate of
or metabolized by
P450, but it is anInhibitor of 3A4
Elimination 80% excreted
unchanged in the
urine
Excreted in feces Minimal renal
excretion
Minimal renal
excretion of parent
compound
66% excreted in
feces
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
34/44
TriazolesFluconazole Dose
100 to 400 mg daily
Renal impairment:
CrCl >50 ml/min, give full dose
CrCl
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
35/44
TriazolesItraconazole Dose
200 to 400 mg/day (capsules)
doses exceeding 200 mg/day are given in 2 divided doses
Loading dose: 200 mg 3 times daily can be given for the first 3
days
Oral solution is 60% more bioavailable than the capsules
Drug Interactions
Major substrate of CYP 3A4
Strong inhibitor of CYP 3A4
Many Drug Interactions
Adverse Drug Reactions
Contraindicated in patients with CHF due to negative inotropic
effects
QT prolongation, torsades de pointes, ventricular tachycardia,
cardiac
arrest in the setting of drug interactions Hepatotoxicity
Rash
Hypokalemia
Nausea and vomiting
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
36/44
TriazolesVoriconazole Dose
IV 6 mg/kg IV for 2 doses, then 3 to 4 mg/kg IV every 12
hours
PO
> 40 kg200-300 mg PO every 12 hours
< 40 kg100-150 mg PO every 12 hours
Cirrhosis: IV
6 mg /kg IV for 2 doses, then 2 mg/kg IV every 12 hours
PO
> 40 kg100 mg PO every 12 hours
< 40 kg 50 mg PO every 12 hours
Renal impairment:
if CrCl
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
37/44
TriazolesVoriconazole
Common Adverse Effects
Peripheraledema
Rash (6%)
N/V/D Hepatotoxicity
Headache
Visual disturbance (30%)
Fever
Serious Adverse Events
Stevens-Johnson Syndrome
Live
r fa
ilure
Anaphylaxis
Renal failure
QTc prolongation
Drug InteractionsDrug Interactions
Major substrate ofCYP 2CD and 2C19Major substrate ofCYP 2CD and
2C19
Minor substrate ofCYP 3A4Minor substrate ofCYP 3A4
Weak inhibitor ofCYP 2C9 and 2C19Weak inhibitor ofCYP 2C9 and
2C19
Moderate inhibitor ofCYP 3A4Moderate inhibitor ofCYP 3A4
Dose AdjustmentsDose Adjustments
EfavirenzEfavirenz
PhenytoinPhenytoin
CyclosporineCyclosporine
WarfarinWarfarin
TacrolimusTacrolimus
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
38/44
TriazolesPosaconazole
Dosing (only available PO)
Prophylaxis of invasive Aspergillus and Candida species 200 mg 3
times/day
Treatment of oropharyngeal candidiasis
100 mg twice daily for 1 day, then 100 mg once daily for
13days
Treatment or refractory oropharyngeal candidiasis 400 mg twice
daily
Treatment of refractory invasive fungal infections (unlabeled
use)
800 mg/day in divided doses
Drug Interactions
Moderate inhibitor of CYP3A4 Adverse Reactions
Hepatotoxicity
QTc prolongation
GI: Diarrhea
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
39/44
PATKI 39
TOPICAL ANTIFUNGAL
AZOLES-CLOTRIMAZOLE,ECONAZOLE,
MICONAZOLE,TERCONAZOLE
.BUTOCONAZOLE
CICLOPIROX OLAMINE
HALOPROGIN,BENZOIC+SALICYLIC,TOLN
AFTATE,TERBINAFINE, NYSTATIN
UNDECYLENIC ACID,
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
40/44
PATKI 40
CLOTRIMAZOLE
fungicidal,1% cream,lotion,vaginal cream
100mg -vaginal tab-o.d-7 days
cure for dermatophytes ,vulvovaginitis, cut.candidiasis-80%
success
ADRs-erythema,pruritis,burning sensations
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
41/44
PATKI 41
Local antifungals
MICONAZOLE
Cream,powder,lotion
,100mg Pessaries, Teniasis,vulvovaginitis
,-80% Success.
Terconazole
Butoconazole-
CICLOPIROX
OLAMINE,
HALOPROGIN , TOLNAFTATE-
TRICHOPHYTONS
AND MICROSPORUM.
TERBINAFINE CREAM
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
42/44
PATKI 42
NYSTATIN
Useful Only For Candidiasis-cutanious,Oral
Or Vaginal
100,000Units/GmCream,powder.
VaginalTab-twiceADay-2weeks
ADRs- RARE
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
43/44
PATKI 43
OLDER LOCAL ANTIFUNGALS
BENZOIC ACID 6% &SALICYLIC ACID 3%-
WHITFIELD OINTMENT-TINEA PEDIS.
KERTOLYTIC TOO,
POTASSIUM IODIDE-1 GM/ML-CUTANIOUS
SPOROTRICHIOSIS
GENTIAN VOILET,IODINE,SULPHUR
-
8/7/2019 UHN Maret 2011,Pharmacology of antifungal drugs
44/44
ANYQUESTION ??
Thank you