Embed Size (px)
Citation preview

Moving Beyond Glycaemia
Fasting Diabetics .... Is It A Real Challenge !?!
Prof. Lobna ElToony
Head of Internal Medicine & Diabetes
Assuit University
.االسالم دين اليسر.
.ن أي ومن كان مريضا أو على سفر ام فعدة م
بكم اليسر ر وال يريد بكم العس أخر يريد الل

Ramadan Between Diabetes
and Fasting
Although the Koran exempts
sick people from the duty of
fasting, many Muslims with
diabetes may not perceive
themselves as sick and are
keen to fast.
43% of patients with type 1
and 86% of those with type 2
diabetes fasted during
Ramadan. EPIDIAR* study
1-IBRAHIM SALTI, et al . Diabetes Care 27:2306–2311, 2004
2-E Hui et al , BMJ, 26 june 2010 , Volume 340

Frequently asked questions during Ramadan
Can a diabetic patient fast?
What about diet and exercise?
How to adjust drugs?
Can a patient monitor blood sugar while fasting?

Can a diabetic patient fastduring Ramadan?

The Risks of Fasting Include:
Hypoglycemia
Hyperglycemia
Diabetic ketoacidosis
Dehydration and thrombosis
M. al-Arouj et al, “Recommendations for management of diabetes during Ramadan,” Diabetes Care, 28(2005), 2305-2311.
Ramadan Fasting and Diabetes Mellitus
The bulk of literature indicates that fasting
in Ramadan is safe for the majority of
diabetic patients, but…

Patient needs-
1. Pre-Ramadan assessment
2. Proper education
3. Management


Pre-Ramadan Medical Assessment
Management of Diabetic Patients During Ramadan
Safer Fasting

High
Moderate
Low risk of adverse events
•Poor glycemic control, Severe and recurrent
episodes of hypoglycemia.
• Experience ketoacidosis three months
before Ramadan.
• Elderly and Pregnant women
• Advanced complications
• Well controlled patients treated with short
acting insulin secretogogue,
sulphonylurea, insulin, or taking
combination oral or oral plus insulin
• Well controlled patients treated with
Metformin, Dipeptidyl peptidase-4 inhibitors, or thiazolidinediones who are
otherwise healthy
Pre-Ramadan Medical
Assessment
E Hui et al , BMJ 2010;340:c3053; Al-Arouj M. et al, Recommendations for management of diabetes during Ramadan. Diabetes Care. 2010;33: 1895-1902.
Patients classed as
high risk are advised
not to fast
Before Ramadan they must
make necessary changes to
their diabetes treatment
Those at low risk can
fast without healthcare
advice.

Salti E, et al. Diabetes Care 27:2306–2311, 2004

T2DM fasting during Ramadan are exposed to !?!
5 folds Increase in sever hyperglycemia with Ketoacidosis that required hospital admission
7.5 Folds Increase in the risk of sever hypoglycemia during Ramadan
2% Of fasting patients experienced at least one episode of sever hypoglycemia requiring hospitalization
Salti E, et al. Diabetes Care 27:2306–2311, 2004
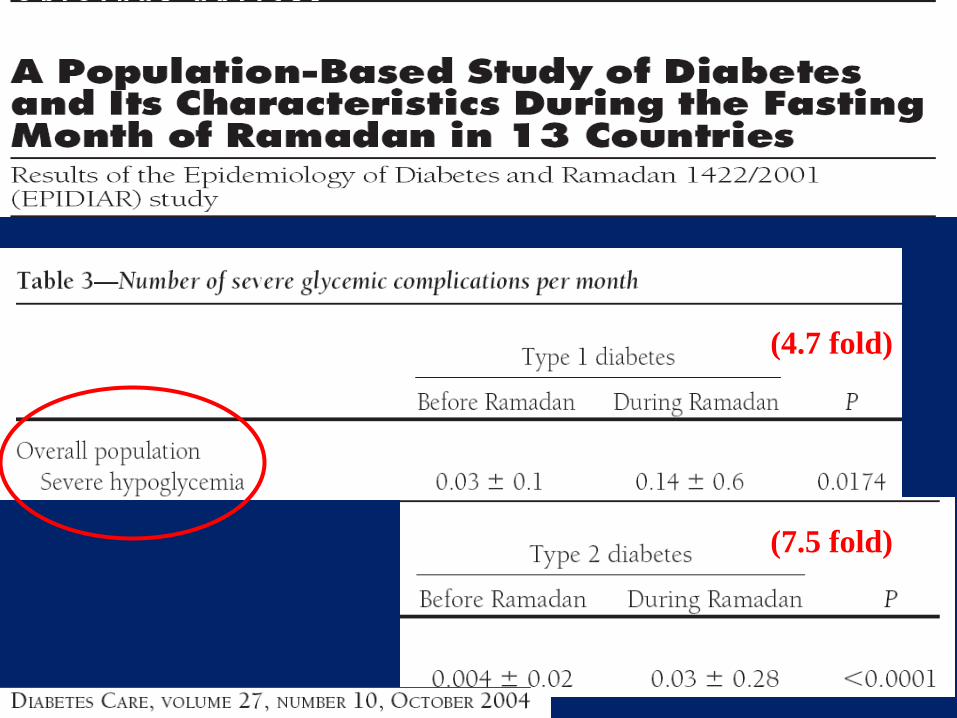
(4.7 fold)
(7.5 fold)

Potential Complications and Effects of
Severe Hypoglycemia
15
Plasma glucose level
10
20
30
40
50
60
70
80
90
100
110
1
2
3
4
5
6
mg/dL
mmol/L
1. Landstedt-Hallin L et al. J Intern Med. 1999;246:299–307.
2. Cryer PE. J Clin Invest. 2007;117:868–870.
Arrythmia1 Neuroglycopenia2
Abnormal prolonged
cardiac
repolarization — ↑
QTc and QT
dispersion
Sudden death
Cognitive impairment
Unusual behavior
Seizure
Coma
Brain death

Severe Hypoglycemia Causes QT
Prolongation
P=NS
P=0.0003
Landstedt-Hallin L et al. J Intern Med. 1999;246:299–307.
Euglycemic clamp(n=8)
Hypoglycemic clamp
2 weeks afterglibenclamide withdrawal
(n=13)
0
360
370
380
390
400
410
420
430
440
450
Me
an
QT
in
terv
al,
ms
Baseline (t=0)
End of clamp (t=150 min)
Significant QT prolongation
During hypoglycemic attacks

Summary of Hypoglycemia Results From
Major Clinical Trials: ACCORD,
ADVANCE, and VADT1–3
No benefit of intensive vs standard glycemic
control on macrovascular outcomes at the
end of the prospective study
Higher incidences of severe hypoglycemia in
the intensive therapy arms
Role of hypoglycemia in study outcomes is
uncertain
17
1. ACCORD Study Group. N Engl J Med. 2008;358:2545–2559.
2. Duckworth W et al. N Engl J Med. 2009;360:129–139.
3. ADVANCE Collaborative Group et al. N Engl J Med. 2008;358:2560–2572.

The Occurrence of Hypoglycemia Was
Associated With Negative Consequences
Decreased adherence1
Increased worry/fear of hypoglycemia2,3
Lower quality of life4
Lower health-related quality of life5
Decreased work productivity6
1. Álvarez Guisasola FA et al. Diab Obes Metab. 2008;10 (suppl 1):25–32.
2. Mohamed M. Curr Med Res Opin. 2008;24:507–514.
3. Leiter LA et al. Can J Diabetes. 2005;29:186–192.
4. Pettersson B et al. Diabetes Res Clin Pract. 2011;92:19-25.
5. Álvarez Guisasola F et al. Health Qual Life Outcomes 2010;8:86–93.
6. Brod M et al. Value Health. 2011;14:665–671.
18

Dehydration and Thrombosis
Limitation of fluid intake
Hot and humid
climates
Hard physical labor
Excessive perspiration.
Hyperglycemia•Osmotic
diuresis
&
•Volume and
electrolyte
depletion.
Adapted from : M. al-Arouj et al, “Recommendations for management of diabetes during Ramadan,” Diabetes Care, 28(2005), 2305-2311.

Dehydration and Thrombosis
• Patients with diabetes exhibit a hypercoagulable state
due to an increase in clotting factors, a decrease in
endogenous anticoagulants, and impaired fibrinolysis.
• Increased blood viscosity secondary to dehydration may
enhance the risk of thrombosis.
• A report from Saudi Arabia suggested an increased
incidence of retinal vein occlusion in patients who fasted
during Ramadan
M. al-Arouj et al, “Recommendations for management of diabetes during Ramadan,” Diabetes Care, 28(2005), 2305-2311.

DIABETES CARE, VOLUME 33, NUMBER 8, AUGUST 2010

Management of Diabetic Patients
During Ramadan
Patients Education
T2DM Pharmaceutical Management in
Ramadan

Four key areas in Ramadan
focused education
1-Meal planning and dietary advice
2-Exercise
3-Blood glucose monitoring
4-Recognizing and managing complications
E Hui et al , BMJ 2010;340:c3053;

Special precautions are recommended
to avoid hypoglycemic events
To take Suhur close to Suhur time
To change in the schedule, amount and composition of meals
To reduce physical activity during the day time. However
physical exercise can be performed about one hour after Iftar
To keep the same calorie during Ramadan as before
Management of diabetes during
Ramadan
1. All patients should understand that they will need to
break the fast if blood glucose is <3.3 mmol/L
(59.4mg/dL) or exceeds 16.7 mmol/L (300mg/dL).
They should be advised to break the fast if blood
glucose is <3.9mmol/L in the morning if the patient
is taking sulfonylurea or insulin
2. Nutrition: In terms of calori and composition diet
should remain same healthy and balanced as before
Ramadan.
3. Ingestion of large amount of foods rich in
carbohydrate , fried food and fats during ifter
should be avoided.

Nutrition
At IFTARI. ,a date or water is the first thing to be eaten .
A complex carbohydrate that delays in digestion and absorption is
good choice for sheuri and while food with more simple
carbohydrate may be taken during ifter.
Eat fibre rich foods including whole grain carbohydrates , fruits and
vegetables with skins.
.


Exercise
Avoid any physical activity that requires effort during the fasting hours
especially the last few hours before “Iftar” because that could lead
to hypoglycemia.
Praying 5 times a day and the
additional special night prayers
(Taraweeh , which can last anything
from 1-2 hours each night) is physical
activity. It is advised that you test
before and after prayers.

Benefits of Education & Counselingaccording to the READ study

REA
D

Adjustment of Drugs

Before Ramadan During Ramadan
Patients on “diet and exercise” - No change is needed - Modify time & intensity of exercise- Ensure adequate fluid intake
Treatment Recommendations

Before Ramadan During Ramadan
Sulfonylurea Once Daily: Morning dose.e.g., Gliclazide MR
Glimepiride
Iftar: Full Morning Dose
Sulfonylurea Twice Daily: Morning & Evening dose.e.g., Gliclazide
Glibenclamide
Iftar: Full Morning DoseSuhur: ½ Evening Dose
Treatment Recommendations
Majority of our type 2 diabetic patients are treated
with Sulfonylurea & Metformin

Before Ramadan During Ramadan
Metformin 500 mg thrice daily Iftar: 1,000 mg,Suhur: 500 mg
Treatment Recommendations

Before Ramadan During Ramadan
DPP4 inhibitor As usual at night
Glitazone As usual at night
Glinide As usual at night
Treatment Recommendations
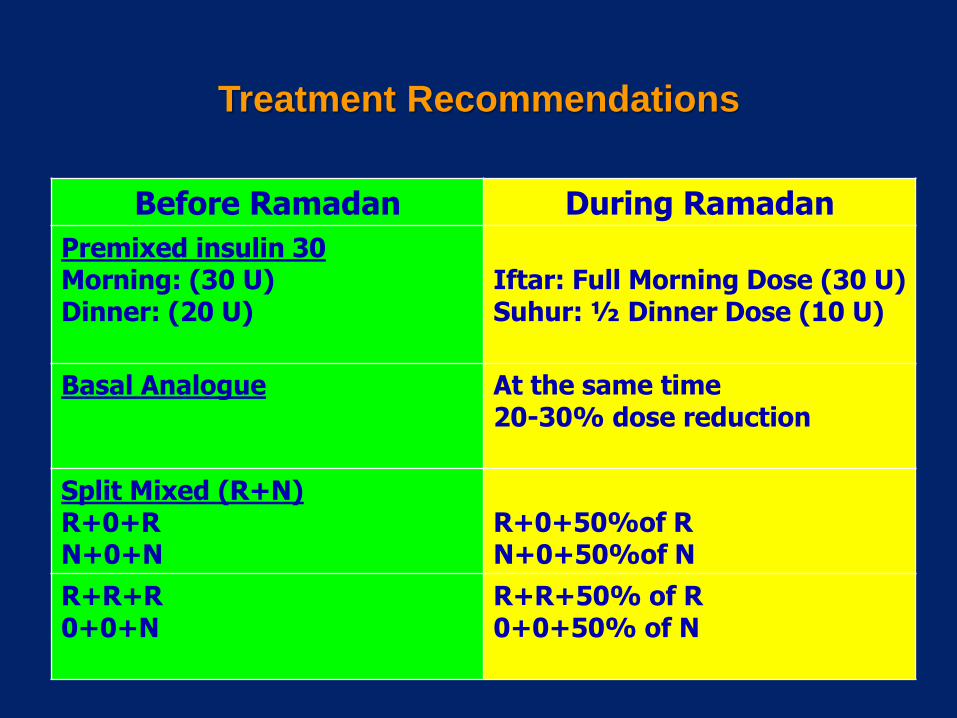
Before Ramadan During Ramadan
Premixed insulin 30 Morning: (30 U)Dinner: (20 U)
Iftar: Full Morning Dose (30 U)Suhur: ½ Dinner Dose (10 U)
Basal Analogue At the same time 20-30% dose reduction
Split Mixed (R+N)R+0+RN+0+N
R+0+50%of RN+0+50%of N
R+R+R0+0+N
R+R+50% of R0+0+50% of N
Treatment Recommendations

Oral hypoglycemic agents
Short actinginsulin SUs
Take twice daily at suhur and iftar
TZDsNo treatment adjustment required 2–4 weeks to exert substantial antihyperglycemic effects
DPP4 inhibitorsThe best tolerated drugs,
Consider DPP4i as an alternative to SUs if the risk of
hypoglycemia is high
SUsUnsuitable for use during fasting because of the
inherent risk ofHypoglycemia, use with caution. Consider dose
adjustment.
MetforminModify timing of doses:
Two thirds of dose at iftar
• One third at suhur.
E Hui et al , BMJ, 26 june 2010 , Volume 340; Al-Arouj M. et al, Recommendations for management of diabetes during Ramadan. Diabetes Care. 2010;33: 1895-1902.
ADA Recomedndation for T2DM Pharmaceutical
Management in Ramadan

Recommended changes to treatment regimen in
patients with type 2 diabetes who fast during
Ramadan
(MONIRA AL-AROUJ, MD. RADHIA BOUGUERRA, MD. JOHN BUSE, MD, PHD. SHERIF HAFEZ, MD, FACP. MOHAMED HASSANEIN, FRCP. MAHMOUD ASHRAF IBRAHIM, MD.
FARAMARZ ISMAIL-BEIGI, MD, PHD. IMAD EL-KEBBI, MD. OUSSAMA KHATIB, MD, PHD. SUHAIL KISHAWI, MD. ABDULRAZZAQ AL-MADANI, MD. ALY A. MISHAL, MD, FACP.
MASOUD AL-MASKARI, MD, PHD. ABDALLA BEN NAKHI, MD. KHALED AL-RUBEAN, MD)
Recommendations for Management of Diabetes During Ramadan; Reviews / Commentaries / ADA Statements ADA WORK GROUP REPORT; DIABETES CARE, VOLUME 28, NUMBER
9: 2305-2311, SEPTEMBER 2005

DPP-4 Inhibitors:
Smart Mode of Action
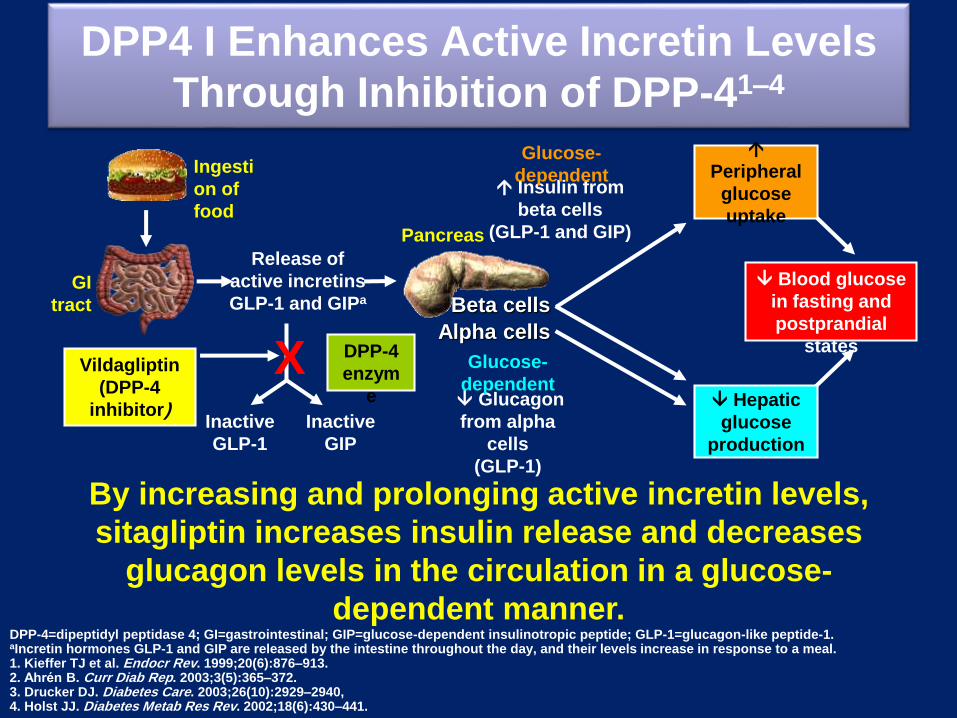
DPP4 I Enhances Active Incretin Levels
Through Inhibition of DPP-41–4
By increasing and prolonging active incretin levels,
sitagliptin increases insulin release and decreases
glucagon levels in the circulation in a glucose-
dependent manner.
Release of
active incretins
GLP-1 and GIPa
Blood glucose
in fasting and
postprandial
states
Ingesti
on of
food
Glucagon
from alpha
cells
(GLP-1)
Hepatic
glucose
production
GI
tract
DPP-4
enzym
e
Inactive
GLP-1
XVildagliptin
(DPP-4
inhibitor)
Insulin from
beta cells
(GLP-1 and GIP)
Glucose-
dependent
Glucose-
dependent
Pancreas
Inactive
GIP
Beta cells
Alpha cells
Peripheral
glucose
uptake
DPP-4=dipeptidyl peptidase 4; GI=gastrointestinal; GIP=glucose-dependent insulinotropic peptide; GLP-1=glucagon-like peptide-1.aIncretin hormones GLP-1 and GIP are released by the intestine throughout the day, and their levels increase in response to a meal. 1. Kieffer TJ et al. Endocr Rev. 1999;20(6):876–913. 2. Ahrén B. Curr Diab Rep. 2003;3(5):365–372. 3. Drucker DJ. Diabetes Care. 2003;26(10):2929–2940, 4. Holst JJ. Diabetes Metab Res Rev. 2002;18(6):430–441.

The goal remains......but
The
is
glycaemic
control
“how?” and “whether we reach or not” is the question?

The challenge of blood glucose control in
diabetes mellitus
Hypoglycaemia/
weight gain
HbA1c
Jacob AN, et al. Diabetes Obes Metab 2007;9:386–93;
Kahn SE, et al. N Engl J Med 2006;355:2427–43;
Wright AD, et al. J Diabetes Complications 2006;20:395–401
Moving beyond glycaemia
Challenges to reach target HbA1c goals

Targeting beyond glycaemia: challenges
Sustainability
Hypoglycaemia
Confused
Shaking
Sweating
Feels hungry
Feels weak
Adherence to therapy
Helping
patients stick
to their
therapy!
Weight gain/obesity
Diabesity: The new epidemic
Vildagliptin in Ramanda
Does it add any benefits over Sulphonylurea !?!

A multinational non-interventional study to assess the effects of
vildagliptin relative to sulphonylurea as dual therapy with metformin
(or as monotherapy*) in Muslim patients with type 2 diabetes fasting
during Ramadan
*in countries with approved monotherapy
Al-Arouj M, et al. Int J Clin Pract. 2013 Oct;67(10):957-63. Epub 2013 Sep 3
The VIRTUE study
VildagliptIn expeRience compared wiTh sulfonylUreas
obsErved during Ramadan

Egypt
Bangladesh
Pakistan
Oman
Lebanon
Saudi
Arabia
Indonesia
India
Kuwait
T2DM = Type 2 diabetes mellitus
Al-Arouj M, et al. Int J Clin Pract. 2013 Oct;67(10):957-63. Epub 2013 Sep 3

†single pill combination allowed when available
*if applicable, as per local approved prescribing information
SU=sulphonylurea
vildagliptin plus metformin† or vildagliptin monotherapy*
SU plus metformin† or SU monotherapy*
End of fasting
period
Start of fasting
period6 weeks before
fasting
6 weeks after
fasting
Data collection
opportunity 1
-6 weeks to day prior
to start of fasting
Data collection
opportunity 2
End of study Fasting period
approx. 4 weeks
Observational period of approximately 16 weeks
Two patient cohorts:
Patients on
stable diabetes
treatment (1:1)
Al-Arouj M, et al. Int J Clin Pract. 2013 Oct;67(10):957-63. Epub 2013 Sep 3

0
20
40
60
80
100
120
140
Pa
tie
nts
(n
) w
ith
≥1
hyp
og
lyc
ae
mic
eve
nt
Vildagliptin (n=669†) SU (n=621†)
~3.5
-fold
P<0.001‡
†Number of patients with a post baseline assessment of hypoglycaemic events. Hypoglycaemia defined as grade 1 (mild): reported symptoms by the patient
and/or blood glucose measurement of <3.9 mmol/L (70 mg/dL) or grade 2 (severe): need for third party assistance ‡Fisher’s exact test
Patients with ≥1 hypoglycaemic event Patients with grade 2
hypoglycaemic events
SU = sulphonylurea
123
(19.8%)
36
(5.4%)
Pa
tie
nts
(n
) w
ith
gra
de
2
hyp
og
lyc
ae
mic
eve
nt
0
20
40
4
P=0.053‡
0
Al-Arouj M, et al. Int J Clin Pract. 2013 Oct;67(10):957-63. Epub 2013 Sep 3

†The within and between treatment differences were based only on patients with HbA1c levels
assessed at both baseline and end of study. ‡Two-sample t test
–1
Me
an
ch
an
ge
in
Hb
A1c
fro
m b
as
eli
ne
(%
)
SUs (n=417†)Vildagliptin (n=485†) Between-treatment
difference
–0.24
0.02
–0.26
P<0.001‡
Mean change in HbA1c (%) pre- to post-Ramadan
SU = sulphonylurea; HbA1c = haemoglobin A1c
–0.5
0
0.5
Al-Arouj M, et al. Int J Clin Pract. 2013 Oct;67(10):957-63. Epub 2013 Sep 3

M. Hassanein, et al. Curr Med Res Opin 2011; 27:1367–74

Metformin 2000 + Gliclazide 80 mg* per daily n 36
Ramadan
Metformin 2000 + Vildagliptin 50 mg bid daily n23
• Observational, two-cohort study, Conducted in the UK.
• Primary objectives: The incidence of hypoglycemic events.
• Secondary objectives: The change in HbA1c levels; The
change in weight; and The treatment adherence during
Ramadan.
• The average duration of fasting in this study was 16 hours
6 weeks post Ramadan 6weeks pre Ramadan
*Different formulations were used for gliclazide therefore the following conversion factor was used:
80 mg standard formulation 30 mg modified release formulation.
M. Hassanein, et al. Curr Med Res Opin 2011; 27:1367–74

0
34
Number of Hypoglycemic Events
Vildagliptin
SU
0
1
Number of Severe Hypoglycemic Events
Vildagliptin
SU
N=23 N=36
M. Hassanein, et al. Curr Med Res Opin 2011; 27:1367–74

Me
an
ch
an
ge
in
Hb
A1
c
pre
-to
po
st-
Ram
ada
n
–0.5; P=0.0262
–0.4 (NS)
0.2
0.0
–0.2
–0.4
–0.6
0.1 (NS)
Vildagliptin
(n=20)
SU‡
(n=32)
Between-group
difference
HbA1c reduction for vildagliptin vs. gliclazide pre- to post Ramadan;
between-group difference −0.5% (P=0.0262)
Prospective observational study of up to 16 weeks duration in 72 fasting Muslim patients with T2DM observed in UK clinical practice, receiving vildagliptin or
SU as an add-on treatment to metformin; per protocol set with pre- and post Ramadan HbA1c assessments, HbA1c; safety set, AEs and SAEs. ‡ SU = Sulfonylurea (gliclazide); VECTOR= Vildagliptin Experience Compared To gliclazide Observed during Ramadan; AE = adverse event; SAE = severe
adverse event; NS = non-significant difference pre- to post Ramadan
Hassanein M et al. Curr Med Res Opin 2011;27:1367–74
• Mean number of missed doses was lower with vildagliptin (mean between-group difference –7.4;
P=0.0204)
• Body weight remained unchanged in both groups

1
Patient with
vildagliptin
10
Patient with
SU
Significant difference in treatment adherence
during Ramadan between the 2 groups
(Number of patients missed at least one dose)
Vs
M. Hassanein, et al. Curr Med Res Opin 2011; 27:1367–74

Safety of Vildagliptin is Well Established
• In meta – analysis of 38 clinical trials include more than 14.000 patients vildagliptin shows no increased risk of:
• Pancreatitis-related AEs
• ALT / AST or Bilirubin elevation
• Renal AEs and SAEs in patients with normal renal function and mild renal impairment patients
• Infection and skin related adverse events
vs. comparators (placebo, insulin and other OAD)
Ligueros-Saylan et al. DIABETES, OBESITY AND METABOLISM Volume 12 No. 6 June 2010

Today's Conclusion:
Regardless The Stage of Diabetes, or Medical
Condition, Vildagliptin Is Favorite Option For Better
Glycemic Control

Last but not least...
ADA considers DPP4 inhibitors as the best tolerated drugs in Ramadan
Vildagliptin is well studied in Muslim
patients during Ramadan supported
by huge evidence for its efficacy and
safety making it a very good option
during fasting

Knowing is not enough
We must APPLY!
Willing is not enough
We must DO!

Safe Fast
LOBNA





























