Embed Size (px)
Citation preview

Twiddler’s syndrome in a patient with epilepsy treated with
deep brain stimulation*David L. Penn, yChengyuan Wu, zxChristopher Skidmore, zxMichael R. Sperling,
and yzAshwini D. Sharan
*Jefferson Medical College, Thomas Jefferson University, Philadelphia, Pennsylvania, U.S.A.; yDepartment of Neurosurgery, Thomas
Jefferson University, Philadelphia, Pennsylvania, U.S.A.; zJefferson Comprehensive Epilepsy Center, Thomas Jefferson University,
Philadelphia, Pennsylvania, U.S.A.; and xDepartment of Neurology, Thomas Jefferson University, Philadelphia, Pennsylvania, U.S.A.
SUMMARY
Twiddler’s syndrome is the conscious or unconscious
manipulation of implantable pulse generators (IPGs) or
associated wire systems by the patient. Most commonly,
this complication has been documented in patients with
cardiac pacemakers, but there are reported cases in
patients with deep brain stimulators. Twisting of stimula-
tor systems results in dislodgement or damage to leads
and loss of stimulation to the desired target. The present
case illustrates a rare complication that may have serious
consequences in patients with deep brain stimulators. A
21 year-old woman presented with recurrence of seizures
from failure of her deep brain stimulator targeting the
anterior nuclei of the thalamus to control refractory epi-
lepsy, 6 months after it was implanted. Radiographic
imaging revealed that the IPG had been twisted upon
itself causing coiling and looping of extension wires. The
patient denied any conscious manipulation of the system,
which was subsequently surgically revised. Surgical
revision achieved the desired stimulation and effects. On
4-month follow-up the deep brain stimulator remained
stable and untwisted; however, it was subsequently
removed in the fourth month because of infection at the
extension site. In conclusion, twiddler’s syndrome is a rare
complication occurring in patients with deep brain stimu-
lator implants and warrants awareness among neurologic
and neurosurgical epilepsy specialists.
KEY WORDS: Twiddler’s syndrome, Epilepsy, Deep
brain stimulator, Anterior thalamic nuclei stimulation.
Twiddler’s syndrome is a rare complication associatedwith implantation of electrical stimulation devices. Firstidentified in 1968 in a patient with a transvenous cardiacpacemaker, twiddler’s syndrome is the conscious or uncon-scious rotation of implantable pulse generators (IPGs) orassociated wire systems by the patient within the subcutane-ous pocket (Bayliss et al., 1968). It causes failure of the sys-tem brought on by disconnection of leads or physical traumathat damages the system.
Cases of twiddler’s syndrome have been reported primar-ily in patients with cardiac pacemakers and defibrillators(Nicholson et al., 2003; Bracke et al., 2005). Current litera-ture contains three reports of patients who experiencedtwiddler’s syndrome following implantation of deep brainstimulation (DBS) systems (Geissinger & Neal, 2007; Israel& Spivak, 2008; Gelabert-Gonzalez et al., 2010). This casereport demonstrates another presentation of this rare
complication in DBS patients and brings it to the attentionof neurologic and neurosurgical specialists who treatpatients undergoing DBS.
Case Report
The patient is a 21-year-old woman who presented withincreased seizure frequency after previously implantedDBS electrodes stopped functioning. She had medicallyrefractory epilepsy beginning at age 6 years with complexpartial and secondarily generalized tonic–clonic seizuresoccurring several times per day. Medical management withphenobarbital, phenytoin, carbamazepine, valproic acid,zonisamide, topiramate, lamotrigine, gabapentin, leveti-racetam, and the ketogenic diet were unsuccessful. Thepatient had no known history of psychiatric illness. Threeyears before her current presentation, an anterior corpuscallosotomy was performed and a year later the patient hada right anterior frontal lobectomy, both of which wereunsuccessful.
The patient was enrolled in the Stimulation of the Ante-rior Nucleus of the Thalamus for Epilepsy (SANTE) clinicaltrial sponsored by Medtronic (Medtronic, Minneapolis,MN, U.S.A.), and a DBS system was stereotactically
Accepted March 6, 2012; Early View publication May 3, 2012.Address correspondence to Ashwini D. Sharan, Department of Neuro-
logical Surgery, Thomas Jefferson University, 909 Walnut Street, 2ndFloor, Philadelphia, PA 19107, USA. E-mail: [email protected]
Wiley Periodicals, Inc.ª 2012 International League Against Epilepsy
Epilepsia, 53(7):e119–e121, 2012doi: 10.1111/j.1528-1167.2012.03489.x
BRIEF COMMUNICATION
e119

implanted bilaterally targeting the anterior nuclei of thethalamus (Fisher et al., 2010). Strain relief loops were usedto prevent traction on the leads. The patient was reposi-tioned for implantation of the IPG. A small subcutaneouspocket was created underneath the left pectoralis fascia. Theextension wires were tunneled subcutaneously and anchoredat two separate points to the fascia to prevent caudal migra-tion. In addition, the IPG was anchored at two separatepoints to the fascia. Before implantation, the patientreported 168 seizures over a 1-month period. Three monthsafter implantation, the patient reported having experienced196 seizure events. Based on the double-blind nature of theSANTE trial, it is unknown whether the device was turnedon at this point following implantation.
Five months postoperatively the patient experiencedincreased seizure frequency, reporting 292 seizures duringthe previous month. Plain films demonstrated 90 degrees ofcaudal rotation and a 180-degree inversion of the IPG in theaxial plane. Both chest and neck x-rays demonstrated coil-ing of the extension wires. The patient and caregiver deniedmanipulation of the device and experienced no significantfluctuation in weight during the course of treatment (bodymass index 27).
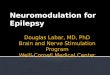
Again, 6 months postoperatively, the IPG continuedshifting in the subcutaneous pocket. Greater coiling of thewires was observed on radiographs to the point that a loopof coiled wire formed proximal to the IPG (Fig. 1). Because
of concern that continued braiding of the extension wirecould dislodge or weaken the proximal DBS wires, the sys-tem was surgically revised. During the surgical revision theproximal contact was observed to be nonfunctional; how-ever, the intracranial location of the electrodes was con-firmed to be optimal. Subsequently, new extensions weretunneled and connected to a new battery. Four nonabsorb-able, fascial sutures were used to anchor the IPG in a poly-ester pouch tied to the pectoralis fascia. Extensions wereanchored to the auricular incision using suture. The previousspace housing the original IPG was obliterated with Vicrylsutures. One month following revision, the patient reportedhaving had 193 seizure episodes. From the time of revision,follow-up images at 4 months showed that the systemremained stable; however, 4 months postoperatively thepatient developed an infection at the extension site and thesystem was explanted.
Discussion
Although many reports of patients experiencing twid-dler’s syndrome have been documented, little work has beendone to empirically define its causes and risks. Bayliss et al.(1968), who first reported this condition in a cardiac patient,suggested that inadequate fixation of the IPG and enlarge-ment of the subpectoral pocket may have contributed to thiscomplication. In addition, the authors hypothesized that lead
A B
C D
Figure 1.
Panels (A) and (C) are postopera-
tive x-rays obtained immediately
after implantation of direct brain
stimulation equipment. Panels (B)
and (D) represent imaging studies
conducted 6 months postopera-
tively after the patient began having
seizures again. (B) reveals significant
90-degree caudal rotation and 180-
degree inversion of the IPG, and (B)
and (D) demonstrate coiling and
looping of the extension system
(highlighted by arrows).
Epilepsia ILAE
e120
D. L. Penn et al.
Epilepsia, 53(7):e119–e121, 2012doi: 10.1111/j.1528-1167.2012.03489.x

wires exiting the IPG at right angles can enhance rotationalmovement. Others report that earlier postoperative time,increasing age, female gender, obesity, and neurologicaland psychiatric disorders such as dementia may be a risk forthe development of twiddler’s syndrome (Harel et al., 2008;Jaafari et al., 2009). Twiddler’s syndrome develops within ayear of device implantation and is more likely to develop inelderly women who tend to have loose subcutaneous tissue(Sidhu et al., 2009).
DBS systems are indicated for a variety of reasons, amongthem Parkinson’s disease, essential tremor, obsessive com-pulsive disorder, depression, and epilepsy. Loss of appropri-ate stimulation in these patients can result in the return ofdisabling tremors, worsening of psychiatric symptoms, andan exacerbation of seizures. In addition, movement and trac-tion of the lead wires can result in pain along the course ofthe wire leads, typically placed in the postauricular area.
In the present case, the patient and her mother firmlydenied any conscious manipulation of the implanted system.Mechanisms indicated in the development of twiddler’s syn-drome, especially in patients denying conscious manipula-tion of the device, are increased weight and physical activity(de Buitleir & Canver, 1996; Bracke et al., 2005). Ourpatient was somewhat overweight, which may have contrib-uted to rotation of the device during normal activity. Heryoung age may have predisposed her to more physicalactivity, which could have led to the development of twid-dler’s syndrome. The very high incidence of seizure in thispatient may also be a cause for concern. Bracke et al. (2005)demonstrated patients who developed twiddler’s syndromebecause of extensive movement of the upper limb fromexercise, particularly swimming. Geissinger and Neal(2007) reported one patient that they hypothesized devel-oped twiddler’s syndrome after resuming household choresand gardening.
Twiddler’s syndrome should be considered when treatingepilepsy with DBS because these patients are often youngerand more active. Technical precautions available to sur-geons include aggressive anchoring of the IPG and wires tounderlying fascia with nonabsorbable suture. In addition,placement of IPGs into fixable polyester pouches within thesubpectoral region or placement subfascially may beattempted; however, these techniques may not always pre-vent movement when the patient is directly manipulatingthe system.
Without knowing the etiology of this patient’s twiddler’ssyndrome, patients who have intractable epilepsy shouldhave their implants monitored more frequently. A simplestrategy can include screening x-rays during the first fewmonths after implantation, before the implant has stabilized.
An additional preventative measure would be to instructpatients to limit activity for a few months following implan-tation, reducing physical stress on the system before it has achance to fully heal and scar.
In conclusion, twiddler’s syndrome is a rare complicationthat can occur in patients with DBS implants and is a com-plication that warrants awareness among neurologic andneurosurgical epilepsy specialists.
Disclosure
Drs Skidmore, Sperling, and Sharan were contracted by Medtronic toconduct the SANTE clinical trial. In addition, Dr. Sharan is a consultantfor St. Jude, Non Linear Technologies Spine, and Medtronic; and receivedstudy support from St. Jude, honoraria from St. Jude, Baxter, and Integra,and other financial support from Zimmer Spine. Finally, Dr. Sharan is anIntelect Medical, Inc. stockholder. The remaining authors report no con-flict of interest concerning the materials or methods used in this study orthe findings specified in this article.
We confirm that we have read the Journals position on issues involved inethical publication and affirm that this report is consistent with those guide-lines.
References
Bayliss CE, Beanlands DS, Baird RJ. (1968) The pacemaker-twiddler’ssyndrome: a new complication of implantable transvenous pacemakers.Can Med Assoc J 99:371–373.
Bracke F, van Gelder B, Dijkman B, Meijer A. (2005) Lead system causingtwiddler’s syndrome in patients with an implantable cardioverter-defibrillator. J Thorac Cardiovasc Surg 129:231–232.
de Buitleir M, Canver CC. (1996) Twiddler’s syndrome complicating atransvenous defibrillator lead system. Chest 109:1391–1394.
Fisher R, Salanova V, Witt T, Worth R, Henry T, Gross R, Oommen K,Osorio I, Nazzaro J, Labar D, Kaplitt M, Sperling M, Sandok E, Neal J,Handforth A, Stern J, DeSalles A, Chung S, Shetter A, Bergen D, BakayR, Henderson J, French J, Baltuch G, Rosenfeld W, Youkilis A, MarksW, Garcia P, Barbaro N, Fountain N, Bazil C, Goodman R, McKhannG, Babu Krishnamurthy K, Papavassiliou S, Epstein C, Pollard J, Ton-der L, Grebin J, Coffey R, Graves N. (2010) Electrical stimulation ofthe anterior nucleus of thalamus for treatment of refractory epilepsy.Epilepsia 51:899–908.
Geissinger G, Neal JH. (2007) Spontaneous twiddler’s syndrome in apatient with a deep brain stimulator. Surg Neurol 68:454–456; discus-sion 456.
Gelabert-Gonzalez M, Relova-Quinteiro JL, Castro-Garcia A. (2010)‘‘Twiddler syndrome’’ in two patients with deep brain stimulation. ActaNeurochir (Wien) 152:489–491.
Harel G, Georgeta E, Copperman Y. (2008) Twiddler’s syndrome: a rarecause of pacemaker failure. Isr Med Assoc J 10:160–161.
Israel Z, Spivak A. (2008) A tremulous twiddler. Stereotact Funct Neuro-surg 86:297–299.
Jaafari N, Bachollet MS, Paillot C, Amiel A, Rotge JY, Lafay N, Quentin S,Wassouf I, Camus V, Senon JL, El Hage W. (2009) Obsessive compul-sive disorder in a patient with twiddler’s syndrome. Pacing ClinElectrophysiol 32:399–402.
Nicholson WJ, Tuohy KA, Tilkemeier P. (2003) Twiddler’s Syndrome.N Engl J Med 348:1726–1727.
Sidhu GS, Seifi A, Zangiabadi AH, Reinig M. (2009) Follow your leads:a case of twiddler’s syndrome. South Med J 102:871–872.
e121
Twiddler’s Syndrome in DBS Epilepsy
Epilepsia, 53(7):e119–e121, 2012doi: 10.1111/j.1528-1167.2012.03489.x