Embed Size (px)
DESCRIPTION
l
Citation preview

591
• Tumorlysissyndromecanoccurinanypatientwithnewlydiagnosedorrelapsedcancer,andthusallpatientsshouldundergoriskstratificationandmanagementaccordingtotheirriskforclinicaltumorlysissyndrome.
• Laboratorytumorlysissyndromeisdefinedasthepresenceoftwoormoreofthefollowingabnormalitiespresentonthesameday:hyperuricemia,hyperkalemia,hyperphosphatemia,andhypocalcemiaasaresultofhyperphosphatemia.
• Clinicaltumorlysissyndromeisdefinedaslaboratorytumorlysissyndromeplusacutekidneyinjury,symptomatichyperkalemia,orsymptomatichypocalcemia,andit
shouldbepreventedwheneverpossible.
• Theincidenceofclinicaltumorlysissyndromedependsonthenumberofriskfactorspresentatpresentationandonthemanagementofpatientspotentiallyatrisk.
• Riskfactorsforclinicaltumorlysissyndromeincludealargecancermass,highcelllysispotential(chemosensitivity),andpatientfactors(e.g.,preexistingnephropathy,dehydration,acidosis,hypotension,andnephrotoxinexposure).
• Managementdependsontheriskofthedevelopmentofclinicaltumorlysissyndrome:⃝ Negligiblerisk—noprophylaxis,no
monitoring
⃝ Lowrisk(1%riskforclinicaltumorlysissyndrome)—hyperhydration,allopurinol,anddailylaboratoryevaluation
⃝ Intermediaterisk—hyperhydration,rasburicase,inpatientmonitoring,andlaboratoryevaluationevery8to12hours
⃝ Highrisk—hyperhydration,rasburicase,cardiacmonitoringontheinpatientward,laboratoryevaluationevery6to8hours,andrapidaccesstohemodialysis
⃝ Establishedclinicaltumorlysissyndromeatpresentation—hyperhydration,rasburicase,cardiacmonitoringintheintensivecareunit,laboratoryevaluationevery4to6hours,andrapidaccesstohemodialysis
S U M M A R Y O F K E Y P O I N T S
38 Tumor Lysis SyndromeScottC.Howard
EPIDEMIOLOGY AND DEFINITIONTumor lysis syndrome is a potentially fatal metabolic condition that occurs in patients with rapidly proliferating, bulky, or chemosensitive tumors (Table 38-1).1 It has been most commonly reported in patients with high-grade non-Hodgkin lymphomas (NHL) and acute leukemias, but it can occur in persons with virtually any type of cancer when a large cancer cell mass is present and the cancer is sensi-tive to initial therapy.
ETIOLOGY AND PATHOGENESISTumor lysis syndrome occurs most commonly after treatment with cytotoxic therapy, but it can also occur spontaneously in patients with highly proliferative tumors. By releasing tumor cellular components into the bloodstream, tumor lysis syndrome results in metabolic abnormalities including hyperphosphatemia, hyperkalemia, hypocal-cemia, hyperuricemia, and azotemia (Fig. 38-1). Acute kidney injury, seizures, cardiac arrhythmias, nausea, and vomiting may occur as a result of these metabolic abnormalities. To reduce morbidity and mortality, early diagnosis and identification of patients at risk for tumor lysis syndrome are of the utmost importance.1,2 The catabolism of nucleic acids ultimately results in the production of uric acid.3 Purines are first degraded into hypoxanthine, then xanthine, and finally into uric acid through the action of xanthine oxidase.4,5 Hyper-uricemia leads to the deposition of uric acid crystals in the renal
tubules because of the poor solubility of uric acid and can result in acute kidney injury.4 Hyperphosphatemia can also cause acute kidney injury. Phosphates combine with calcium, generating calcium phosphate salts that deposit in the renal tubules. The binding of calcium by phosphate leads to hypocalcemia, which in turn can cause vomiting, muscle cramps, tetany, paresthesias, seizures, and cardiac dysrhythmias.6 Hyperkalemia from cellular lysis can lead to cardiac dysrhythmias, ventricular tachycardia, fibrillations, or cardiac arrest.6
RISK FACTORS AND INCIDENCE OF TUMOR LYSIS SYNDROMESeveral risk factors for tumor lysis syndrome have been identified, including tumor-related factors, individual patient characteristics, and the type of chemotherapy used.7 Certain tumor types have his-torically been associated with an increased risk for the development of tumor lysis syndrome, including Burkitt leukemia, acute lympho-blastic leukemia (ALL), acute myeloid leukemia (especially those with inv(16) chromosomal translocation), and NHL (particularly Burkitt lymphoma)8-10; patients with these tumor types were the most frequently enrolled in compassionate-use trials of hypouricemic agents.11,12 However, tumor lysis syndrome can also develop in patients with chronic lymphocytic leukemia (CLL) and chronic myelogenous leukemia.13 Acute leukemias and high-grade lympho-mas often have a high proliferative rate, a large tumor burden, and

PartII:ProblemsCommontoCancerandItsTherapy592
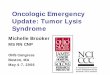
Figure 38-1 • Pathophysiology of tumor lysis syndrome. Lysis of cancer cells releases DNA, phosphate, potassium, and cytokines. DNA released from the lysed cells is metabolized into adenosine and guanosine, both of which are converted into xanthine. Xanthine is then oxidized by xanthine oxidase, leading to the production of uric acid, which is excreted by the kidneys. When the accumulation of phosphate, potassium, xanthine, or uric acid is more rapid than excretion, tumor lysis syndrome develops. Cytokines cause hypotension, inflammation, and acute kidney injury, which increase the risk for tumor lysis syn-drome. The bidirectional dashed line between acute kidney injury and tumor lysis syndrome indicates that acute kidney injury increases the risk of tumor lysis syndrome by reducing the ability of the kidneys to excrete uric acid, xanthine, phosphate, and potassium. By the same token, development of tumor lysis syndrome can cause acute kidney injury by renal precipitation of uric acid, xanthine, and calcium phosphate crystals and by crystal independent mechanisms. Allopurinol inhibits xanthine oxidase and prevents the conversion of hypoxanthine and xanthine into uric acid but does not remove existing uric acid. In contrast, rasburicase removes uric acid by enzymatically degrading it into allantoin, a highly soluble product that has no known adverse effects on health.
Inflammation
Acutekidney injury
HypotensionGuanosineAdenosine
Guanine
DNA
DNAase breaks downDNA, releasing purines
Xanthine oxidase
Xanthine oxidase
Xanthine
Uric acidAllantoin
Potassium CytokinesPhosphate
Potassium
AccumulationUrinary excretion
Phosphate
Inosine
Hypoxanthine
No tumor lysissyndrome
Allopurinol
Rasburicase
Tumor lysissyndrome
Lysis of cancer cells with release of intracellular contents
Table 38-1 Modified Cairo-Bishop Classification of Tumor Lysis Syndrome
Laboratory tumor lysis syndrome
Two or more of the metabolic abnormalities in the next column present on the same day
Occurring within 3 days before initiation of therapy or 7 days after initiation of therapy
Assumes the patient receives adequate hydration and a hypouricemic agent
Uric acid ≥476 µmol/L (8 mg/dL) in adults or the upper limits of normal in children
Potassium ≥6.0 mmol/LPhosphorus ≥1.5 mmol/L (4.5 mg/dL) in adults or ≥2.1 mmol/L (6.5 mg/dL) in children
Calcium ≤1.75 mmol/L (7 mg/dL) or ionized calcium <0.3 mmol/L (1.12 mg/dL)
Clinical tumor lysis syndrome
Laboratory tumor lysis syndrome plus any of the criteria in the next column (not attributable to other causes)
Acute kidney injury, defined as an increase in creatinine of 26.5 micromoles/L (0.3 mg/dL) or when no baseline creatinine is documented, a single value ≥1.5 times the upper limits of normal for the patient’s age and sex
Symptomatic hypocalcemia (e.g., tetany or paresthesias), seizure, cardiac dysrhythmia, or sudden death attributed to hypocalcemia or hyperkalemia
Data from reference 1.
are particularly sensitive to chemotherapy; the combination of high tumor bulk and sensitivity to therapy make tumor lysis syndrome more likely.14 The high nucleic acid, phosphorus content, and increased activity of purine metabolism in these tumors predispose patients to tumor lysis syndrome.7 In a study of 102 patients with high-grade NHL who received prophylactic hyperhydration and allo-purinol, the incidence of clinically significant tumor lysis syndrome was 6%, and one patient required dialysis.15 A retrospective study of
755 patients with NHL or acute leukemia who received rasburicase for prevention or treatment of tumor lysis syndrome documented a 5.3% incidence of tumor lysis syndrome (including both laboratory and clinical tumor lysis syndrome).16 Seven patients in this study died from tumor lysis syndrome (0.9% of all patients and 17.5% of patients with tumor lysis syndrome).16,17 In a multinational study of 235 pediatric patients with advanced-stage, B-cell NHL who were treated with the same chemotherapy regimen, 27% and 15% of U.S.

593TumorLysisSyndrome • CHAPTER38
used prior to the initiation of chemotherapy (Fig. 38-3).4,25 However, allopurinol has several limitations. Allopurinol therapy is most effec-tive when it is used 24 to 48 hours before the start of chemotherapy, which may cause a delay in the initiation of cytotoxic therapy.22 Furthermore, it does not remove existing uric acid, which is a signifi-cant problem in patients who present with significant hyperuricemia. Finally, treatment with allopurinol increases xanthine concentrations in the urine, which can cause xanthine crystal formation and nephropathy.26 Hande and colleagues27 examined purine excretion in 11 patients with bulky lymphomas. All patients received allopurinol 2 to 5 days before chemotherapy. Although urinary concentrations of uric acid and hypoxanthine remained below solubility in all patients, concentrations of xanthine exceeded solubility in 6 patients (55%). Purine metabolism was studied in 19 children with ALL who received allopurinol for the prevention of tumor lysis syndrome before starting chemotherapy.28 Xanthine exceeded urine solubility in 16 patients (84%). Because xanthine is rarely measured, its contribu-tion to tumor lysis syndrome remains unknown,29 but its low solubil-ity at all urine pH values and high concentrations in the urine of patients treated with allopurinol suggest that xanthine nephropathy may occur commonly in patients with a high cancer cell mass, who produce large amounts of purines after initiation of chemotherapy.
RasburicaseRasburicase converts uric acid into allantoin, a highly soluble metab-olite that is excreted by the kidneys (see the light green line in Fig. 38-2). Unlike most other mammals, humans lack a functional urate oxidase enzyme because of a nonsense mutation in the genetic sequence. Rasburicase lowers serum uric acid levels quickly and has few adverse effects (Fig. 38-1).1,23,30 However, rasburicase is contrain-dicated in patients with glucose-6-phosphate dehydrogenase defi-ciency because of the high risk of the development of methemoglobinemia and hemolytic anemia after receiving these agents, because of the breakdown of uric acid into hydrogen peroxide.1
In an effort to reduce costs, some clinicians administer lower doses of rasburicase than the 0.15 to 0.2 mg/kg approved by the U.S. Food and Drug Administration (FDA), in the hope that the lower dose will effectively prevent or manage tumor lysis syndrome. Although no clinical trial results have validated the efficacy of this approach, several retrospective studies and case reports have been published in which lower doses of rasburicase were used successfully. Lee and col-leagues31 used a 4.5-mg fixed dose to treat three children with ALL. All three patients had a rapid reduction in uric acid, but when the weight-adjusted dose was determined for the 4.5-mg dose, it was found that one patient received a higher quantity than the FDA-approved dose (0.26 mg/kg), one patient received the approved dose (0.17 mg/kg); and one patient received 50% of the approved dose (0.08 mg/kg). Another case series examined 11 adults with hemato-logic malignancies at risk for tumor lysis syndrome.32 Eight patients had renal impairment as a result of tumor lysis syndrome at the time of presentation, and all were treated with a 6-mg, single dose of rasburicase (corresponding to a median weight-based dose of 0.08 mg/kg). In 10 of the 11 patients, single-dose rasburicase lowered and maintained normal uric acid levels; the mean pretreatment uric acid level, 11.7 mg/dL, was reduced to 2.0 mg/dL after treatment. One morbidly obese patient required a second dose of rasburicase (12 mg; 0.046 mg/kg, based on actual body weight) to control his uric acid levels. Among the eight patients with renal impairment, three had a return to baseline renal function after receiving rasburicase, one required hemodialysis, and four had no subsequent renal function data reported. Although the authors concluded that use of a fixed, 6-mg dose of rasburicase appeared to be safe and effective, the fact that one patient required a large second dose and one required dialysis implies inadequate uric acid control, especially when compared with the 98% to 100% efficacy reported in large studies using the
patients (who all received allopurinol) experienced tumor lysis syn-drome and required dialysis, respectively, whereas 11% and 3% of French patients (who all received rasburicase) experienced tumor lysis syndrome and required dialysis, respectively.18 Hence the risk for tumor lysis syndrome depends not only on tumor-related risk factors but also on the supportive care used (Fig. 38-1).
In addition to tumor-related risk factors for tumor lysis syndrome, patient-related factors affect tumor lysis syndrome risk, including leukocytosis, hyperuricemia, elevated serum lactate dehydrogenase, elevated serum creatinine, renal insufficiency, dehydration, acidic urine, and decreased urinary flow at the time of presentation.7,14 Finally, specific cytotoxic agents have been associated with tumor lysis syndrome in particular diseases, such as fludarabine and lenalidomide in patients treated for CLL.7,13,19,20 Because the risk of clinical tumor lysis syndrome is proportional to the rapidity of response to therapy, patients whose tumors respond quickly to a new therapeutic agent have an increased risk for the development of tumor lysis syndrome. Patients with diagnoses not typically associated with tumor lysis syndrome (e.g., metastatic colon cancer) can also be affected by tumor lysis syndrome when the treatment includes new, highly active agents, such as cetuximab.21 To successfully treat and prevent tumor lysis syndrome, it is necessary to identify patients at risk and tailor prevention according to risk, as described in the next section.6
PREVENTION AND MANAGEMENT OF TUMOR LYSIS SYNDROMEPublished guidelines for the diagnosis, prevention, and management of tumor lysis syndrome (Table 38-2) differ in many details. However, all guidelines agree that patients at risk for tumor lysis syndrome should undergo risk stratification and management on the basis of their risk. Clinical tumor lysis syndrome is the outcome that should be prevented, because by definition it is associated with morbidity. Standard prophylaxis includes close monitoring, hyperhydration to increase urine output and facilitate renal excretion of uric acid and phosphorus, and administration of a hypouricemic agent, such as allopurinol or rasburicase, to prevent the formation of uric acid crystals in the kidney, as well as administration of phosphate binders to reduce calcium phosphate precipitation in the kidneys.1,2,4,22 Both allopurinol and rasburicase have been used successfully to reduce the incidence of tumor lysis syndrome in pediatric and adult patients.1,23 Historically, urine has been alkalinized by the administra-tion of bicarbonate to improve the solubility of uric acid (Fig. 38-2)21,24; however, this step is not currently recommended, because the solubility of calcium phosphate decreases at higher pH values (Fig. 38-2), and therefore precipitation in the renal tubules may be exacerbated. As an alternative to urine alkalinization, the prophylactic administration of rasburicase has been shown to effectively reduce uric acid levels.7
All patients at intermediate or high risk for clinical tumor lysis syndrome should receive hyperhydration with intravenous fluids at 2500 mL/m2/day or higher with a goal of very high urine output to reduce the risk of uric acid and calcium-phosphate precipitation in renal tubules. If urine output is inadequate even after hyperhydration, a diuretic may be added to increase urine output, but only after the patient is very well hydrated.1 Patients at intermediate or high risk should be monitored in the hospital with serum electrolytes and uric measurement every 8 to 12 hours (intermediate risk) or 4 to 6 hours (high risk). Patients who present with tumor lysis syndrome should be connected to a cardiac monitor and observed in an intensive care or step-down unit.1
AllopurinolAllopurinol inhibits xanthine oxidase and prevents metabolism of hypoxanthine and xanthine into uric acid, thus reducing the forma-tion of uric acid and the incidence of tumor lysis syndrome when

PartII:ProblemsCommontoCancerandItsTherapy594
Table 38-2 Published Guidelines for Risk Classification and Management of Tumor Lysis Syndrome
SourceType of Tumor Lysis Syndrome
Cancer-Associated Risk Factors
Patient-Associated Risk Factors
Definition of Risk Groups
Management Recommendations
This chapter Clinical Established tumor lysis syndrome at presentation or high risk; intermediate risk; low risk; negligible risk
Established tumor lysis syndrome or high risk: IVF and rasburicase
Intermediate risk: IVF and single dose of rasburicase or daily allopurinol; close monitoring
Low risk: clinical judgment and monitoring
Negligible risk: no monitoring or prophylaxis
ASCO22 Not specified Burkitt, lymphoblastic, or diffuse, large-cell lymphomas; ALL; solid tumors with high proliferative rates and rapid response to therapy; bulky disease, elevated LDH; WBC count >25,000/µL
Preexisting renal failure, oliguria, and hyperuricemia
Low-, intermediate-, and high-risk groups based on specific combinations of cancer- and patient-associated risk factors
High risk: IVF and rasburicase
Intermediate risk: IVF and allopurinol; rasburicase if hyperuricemia develops
Low risk: clinical judgment and monitoring
COG Supportive Care Guidelines version 6/20/0838
Not specified Bulky disease; high tumor burden; chemosensitive cancers; WBC count >100,000/µL; lymphadenopathy; hepatosplenomegaly; elevated LDH; large primary masses of the abdomen, thorax, or mediastinum; ALL; T-cell leukemias and non-Hodgkin lymphomas
Presentation with serum creatinine greater than 0.7 mg/dL (children) or 1.3 mg/dL (adults); hyperuricemia; signs of evolving tumor lysis syndrome
Not defined Prophylaxis: IVF and allopurinol daily
Patients with renal insufficiency, elevated creatinine, and/or hyperuricemia: rasburicase for 1-3 days
NCCN Practice Guidelines in Oncology: AML and NHL39,40
Not specified AML; lymphoblastic lymphoma; Burkitt lymphoma; a bulky presentation of diffuse, large, B-cell lymphoma; or chronic lymphocytic leukemia with high WBC count
Unable to tolerate oral medication, clinical tumor lysis syndrome, or problematic hyperuricemia
Not defined Prophylaxis: IVF with alkalinization and allopurinol
Patients with clinical tumor lysis syndrome and/or hyperuricemia: IVF and consider rasburicase
SFCE41 Need for additional rasburicase to control tumor lysis syndrome
WBC count >50,000/µL; large tumor burden (lymph nodes >5 cm, hepatosplenomegaly, mediastinal mass >5 cm); elevated LDH >2× ULN; AML; T-cell lymphomas; B-cell lymphomas; Burkitt leukemia
Creatinine >ULN for age and weight, uric acid >ULN for age, and phosphorus >ULN
High risk: presence of any cancer- or patient-associated risk factor
Low risk: absence of risk factors
High risk: daily rasburicase for 5 days
Low risk: 1 dose of rasburicase, then repeat as needed
Data from references 22 and 38-41.ALL, Acute lymphocytic leukemia; AML, acute myeloid leukemia; ASCO, American Society of Clinical Oncology; COG, Children’s Oncology Group; IVF, intravenous fluids;
LDH, lactate dehydrogenase; NCCN, National Comprehensive Cancer Network; NHL, non-Hodgkin lymphoma; SFCE, Société Française de Lutte contre les Cancers et Leucémies de l’Enfant et de l’Adolescent (French Pediatric Oncology Society); ULN, upper limit of normal; WBC, white blood cell.

595TumorLysisSyndrome • CHAPTER38
administered to 43 adult patients undergoing stem cell transplanta-tion (51%) or receiving chemotherapy (49%).34 The total doses of rasburicase administered were 3 mg (n = 37), 4.5 mg (n = 2), or 6 mg (n = 4), and uric acid levels were all within normal limits 48 hours after the first dose. Although three patients were already receiving dialysis at the time of the study, no additional patients required dialy-sis. What is not clear from this study is whether the patients were at risk for tumor lysis syndrome. Many patients undergoing stem cell transplantation already have a low bulk of disease and would not be expected to have tumor lysis syndrome, and the disease status of the patients in the study cohort was not described. The second cohort in which use of a reduced-dose of rasburicase was evaluated included 46 adults with hematologic cancers and four with solid tumors.35 Patients were eligible to receive rasburicase if they had bulky disease, an ele-vated white blood cell count, elevated lactate dehydrogenase in addi-tion to elevated uric acid, or a history of tumor lysis syndrome after a prior course of chemotherapy. Rasburicase dosing was at the discre-tion of the treating clinician, and the initial dose ranged from 1.5 to 16.5 mg. Nine patients had uric acid levels above the normal range after the initial rasburicase dose, despite a mean decrease of 41% from their baseline levels. Because of the heterogeneous cohort of patients (diagnoses included ALL, acute myeloid leukemia, CLL, myeloma, solid tumors, and both high- and low-grade lymphomas) and the wide range of rasburicase doses used, it is difficult to derive specific treatment recommendations from the data presented. However, the results do suggest that using doses of rasburicase that are lower than recommended may be effective for some patients.
The use of reduced doses of rasburicase should be studied in defined cohorts of patients at an intermediate risk for the develop-ment of clinical tumor lysis syndrome to determine the optimal dose (i.e., the dose at which no patient experiences acute kidney injury or clinical tumor lysis syndrome and at which the least amount of ras-buricase is used). In patients receiving low-dose rasburicase to prevent tumor lysis syndrome, serum uric acid levels must be measured pre-cisely. Blood samples must be collected into chilled tubes, placed on ice immediately, and assayed promptly to avoid ex vivo breakdown of uric acid by rasburicase, which produces artificially low levels of uric acid.36
Although the optimal treatment for patients at intermediate risk for clinical tumor lysis syndrome has not been determined by ran-domized clinical trials, a prudent approach at present is the admin-istration of one standard dose of rasburicase (0.15 mg/kg), especially if hyperuricemia or laboratory tumor lysis syndrome develops. Patients at high risk for the development of tumor lysis syndrome should receive at least one standard dose of rasburicase. Repeat doses of rasburicase should be given to patients with elevated uric acid levels, and all patients with laboratory tumor lysis syndrome should receive at least one standard dose of rasburicase (0.15 mg/kg) to prevent progression to clinical tumor lysis syndrome. Although this strategy has not been validated by a prospective randomized trial, the one randomized trial comparing rasburicase to allopurinol docu-mented improved creatinine during the first 4 days of therapy in patients receiving rasburicase but not in patients receiving allopurinol.37
CONCLUSIONSAppropriate management of tumor lysis syndrome includes risk stratification of all patients; hydration; careful monitoring of serum metabolite levels; administration of rasburicase for patients at inter-mediate or high risk; and administration of allopurinol for patients at low risk of clinical tumor lysis syndrome. Hyperuricemia and hyperphosphatemia should be prevented and treated promptly when they do occur, because their deposition in the renal tubules can cause acute kidney injury. Risk-stratified management improves outcomes by preventing seizures, cardiac dysrhythmia, acute kidney injury, and the need for dialysis.
FDA-approved dose.11 Another report describes an obese woman with chronic myelomonocytic leukemia in blast crisis who was treated with 11 mg of rasburicase (a dose based on her ideal body weight), which adequately controlled her uric acid.33
Two retrospective studies of reduced-dose rasburicase have been reported recently.34,35 A fixed rasburicase dose of 3 mg, with repeated doses as needed based on subsequent uric acid levels, was
Figure 38-2 • Solubility of purine metabolites by urine pH. Uric acid solubility is highly pH dependent. As urine pH rises from 5 to 7, the solubility increases 25-fold, from 8 mg/dL to 200 mg/dL. This increased uric acid solu-bility and consequent decreased risk of crystal formation and acute kidney injury is the reason urine alkalinization was standard for patients at risk for tumor lysis syndrome before the advent of rasburicase. In contrast to uric acid, calcium phosphate becomes less soluble and more likely to crystallize as urine pH increases. Xanthine has low solubility and hypoxanthine relatively high solubility, regardless of urine pH. Note that the scale is logarithmic. (From Howard SC, Ribeiro RC, Pui CH. Acute complications. In: Pui CH, editor. Childhood leukemias. Cambridge, UK: Cambridge University Press; 2012.)
1000
100
10
14.5 5 5.5 6 6.5 7 7.5
Urine pH
Sol
ubili
ty (
mg/
dL)
AllantoinHypoxanthine
Uric acidCalcium phosphate
Xanthine
Figure 38-3 • Uric acid levels during the first 4 days of treatment in patients at risk for tumor lysis syndrome who were randomly assigned to receive rasburicase versus allopurinol. In patients at risk for tumor lysis syndrome, rasburicase was associated with a rapid decrease in uric acid and a corresponding lower area under the concentration time curve for uric acid, as measured during the first 4 days of therapy (128 ± 70 vs. 329 ± 129 mg/dL*hour, P < .0001). (Data from Goldman SC et al. A randomized comparison between rasburicase and allopurinol in children with lymphoma or leukemia at high risk for tumor lysis. Blood 2001;97(10):2998–3003.)
Time (hours)
P < 0.0001
Number of samples at each time point
AllopurinolRasburicase
2527
2527
2527
2426
2225
8
0
1
2
3
4
5
6
7
0 4 12 24 36 48 60 72 84 96
Uric
aci
d m
g/dL
Allopurinol AUC0-96hr = 329 ± 129 mg/dL*hrRasburicase AUC0-96hr = 128 ± 70 mg/dL*hr

PartII:ProblemsCommontoCancerandItsTherapy596
R E F E R E N C E S1. Howard SC, Jones DP, Pui CH. The tumor lysis
syndrome. N Engl J Med 2011;364(19):1844–54.2. Cairo MS, et al. Recommendations for the evalua-
tion of risk and prophylaxis of tumour lysis syn-drome (TLS) in adults and children with malignant diseases: an expert TLS panel consensus. Br J Haematol 2010;149(4):578–86.
3. Pui CH. Rasburicase: a potent uricolytic agent. Expert Opin Pharmacother 2002;3(4):433–42.
4. Hochberg J, Cairo MS. Rasburicase: future direc-tions in tumor lysis management. Expert Opin Biol Ther 2008;8(10):1595–604.
5. Cairo MS, Bishop M. Tumour lysis syndrome: new therapeutic strategies and classification. Br J Haematol 2004;127(1):3–11.
6. Rampello E, Fricia T, Malaguarnera M. The man-agement of tumor lysis syndrome. Nat Clin Pract Oncol 2006;3(8):438–47.
7. Coiffier B, Riouffol C. Management of tumor lysis syndrome in adults. Expert Rev Anticancer Ther 2007;7(2):233–9.
8. Cohen LF, Balow JE, Magrath IT, et al. Acute tumor lysis syndrome. A review of 37 patients with Burkitt’s lymphoma. Am J Med 1980;68(4): 486–91.
9. Fenaux P, Lai JL, Miaux O, et al. Burkitt cell acute leukaemia (L3 ALL) in adults: a report of 18 cases. Br J Haematol 1989;71(3):371–6.
10. Tiu RV, Mountantonakis SE, Dunbar AJ, Schreiber Jr MJ. Tumor lysis syndrome. Semin Thromb Hemost 2007;33(4):397–407.
11. Jeha S, Kantarjian H, Irwin D, et al. Efficacy and safety of rasburicase, a recombinant urate oxidase (Elitek), in the management of malignancy-associated hyperuricemia in pediatric and adult patients: final results of a multicenter compassionate use trial. Leukemia 2005;19(1):34–8.
12. Smalley RV, Guaspari A, Haase-Statz S, et al. Allopurinol: intravenous use for prevention and treatment of hyperuricemia. J Clin Oncol 2000; 18(8):1758–63.
13. Cheson BD, Frame JN, Vena D, Quashu N, Sorensen JM. Tumor lysis syndrome: an uncommon complication of fludarabine therapy of chronic lym-phocytic leukemia. J Clin Oncol 1998;16(7): 2313–20.
14. Navolanic PM, Pui CH, Larson RA, et al. Elitek-rasburicase: an effective means to prevent and treat hyperuricemia associated with tumor lysis syn-drome, a Meeting Report, Dallas, Texas, January 2002. Leukemia 2003;17(3):499–514.
15. Hande KR, Garrow GC. Acute tumor lysis syn-drome in patients with high-grade non-Hodgkin’s lymphoma. Am J Med 1993;94(2):133–9.
16. Annemans L, Moeremans K, Lamotte M, et al. Pan-European multicentre economic evaluation of
recombinant urate oxidase (rasburicase) in preven-tion and treatment of hyperuricaemia and tumour lysis syndrome in haematological cancer patients. Support Care Cancer 2003;11(4):249–57.
17. Cheson BD, Dutcher BS. Managing malignancy-associated hyperuricemia with rasburicase. J Support Oncol 2005;3(2):117–24.
18. Cairo MS, Gerrard M, Sposto R, et al. Results of a randomized international study of high-risk central nervous system B non-Hodgkin lymphoma and B acute lymphoblastic leukemia in children and adolescents. Blood 2007;109(7):2736–43.
19. Moutouh-de Parseval LA, Weiss L, DeLap RJ, et al. Tumor lysis syndrome/tumor flare reaction in lenalidomide-treated chronic lymphocytic leuke-mia. J Clin Oncol 2007;25(31):5047.
20. Hussain K, Mazza JJ, Clouse LH. Tumor lysis syn-drome (TLS) following fludarabine therapy for chronic lymphocytic leukemia (CLL): case report and review of the literature. Am J Hematol 2003;72(3):212–15.
21. Krishnan G, D’Silva K, Al-Janadi A. Cetuximab-related tumor lysis syndrome in metastatic colon carcinoma. J Clin Oncol 2008;26(14):2406–8.
22. Coiffier B, Altman A, Pui CH, Younes A, Cairo MS. Guidelines for the management of pediatric and adult tumor lysis syndrome: an evidence-based review. J Clin Oncol 2008;26(16):2767–78.
23. Cortes J, Moore JO, Maziarz RT, et al. Control of plasma uric acid in adults at risk for tumor Lysis syndrome: efficacy and safety of rasburicase alone and rasburicase followed by allopurinol compared with allopurinol alone—results of a multicenter phase III study. J Clin Oncol 2010;28(27): 4207–13.
24. Howard SC, Ribeiro RC, Pui CH. Acute complica-tions. In CH Pui, editor. Childhood Leukemias. New York, NY: Cambridge University Press; 2006. p. 709–49.
25. Catalytica Pharmaceuticals. Aloprim [package insert]. Greenville, NC: Catalytica Pharmaceuticals; 2000.
26. LaRosa C, McMullen L, Bakdash S, et al. Acute renal failure from xanthine nephropathy during management of acute leukemia. Pediatr Nephrol 2007;22(1):132–5.
27. Hande KR, Hixson CV, Chabner BA. Postchemo-therapy purine excretion in lymphoma patients receiving allopurinol. Cancer Res 1981;41(6): 2273–9.
28. Andreoli SP, Clark JH, McGuire WA, Bergstein JM. Purine excretion during tumor lysis in children with acute lymphocytic leukemia receiving allopurinol: relationship to acute renal failure. J Pediatr 1986; 109(2):292–8.
29. Truong TH, Beyene J, Hitzler J, et al. Features at presentation predict children with acute lympho-blastic leukemia at low risk for tumor lysis syn-drome. Cancer 2007;110(8):1832–9.
30. Hochberg J, Cairo MS. Tumor lysis syndrome: current perspective. Haematologica 2008;93(1): 9–13.
31. Lee AC, Li CH, So KT, Chan R. Treatment of impending tumor lysis with single-dose rasburicase. Ann Pharmacother 2003;37(11):1614–17.
32. McDonnell AM, Lenz KL, Frei-Lahr DA, et al. Single-dose rasburicase 6 mg in the management of tumor lysis syndrome in adults. Pharmacotherapy 2006;26(6):806–12.
33. Arnold TM, Reuter JP, Delman BS, Shanholtz CB. Use of single-dose rasburicase in an obese female. Ann Pharmacother 2004;38(9):1428–31.
34. Trifilio S, Gordon L, Singhal S, et al. Reduced-dose rasburicase (recombinant xanthine oxidase) in adult cancer patients with hyperuricemia. Bone Marrow Transplant 2006;37(11):997–1001.
35. Hummel M, Reiter S, Adam K, et al. Effective treatment and prophylaxis of hyperuricemia and impaired renal function in tumor lysis syndrome with low doses of rasburicase. Eur J Haematol 2008;80(4):331–6.
36. Sanofi-Synthelabo. Elitek. New York, NY: Sanofi-Synthelabo; 2007.
37. Goldman SC, Holcenberg JS, Finklestein JZ, et al. A randomized comparison between rasburicase and allopurinol in children with lymphoma or leukemia at high risk for tumor lysis. Blood 2001;97(10): 2998–3003.
38. Children’s Oncology Group. Supportive care guide-lines, <https://members.childrensoncologygroup.org/prot/reference_materials.asp/>; 2008 [accessed 12.07.09].
39. National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: non-Hodgkins lymphoma (v.2.2009), <http://www.nccn.org/professionals/physician_gls/PDF/nhl. pdf/>; 2009 [accessed 28.04.09].
40. National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: acute myeloid leukemia (v.1.2009), <http://www.nccn.org/professionals/physician_gls/PDF/aml.pdf/>; 2009 [accessed 13.07.09].
41. Bertrand Y, Mechinaud F, Brethon B, et al. SFCE (Société Française de Lutte contre les Cancers et Leucémies de l’Enfant et de l’Adolescent) recom-mendations for the management of tumor lysis syn-drome (TLS) with rasburicase: an observational survey. J Pediatr Hematol Oncol 2008;30(4): 267–71.