Embed Size (px)
Citation preview
TUCSON POLICE DEPARTMENTLESSONS IN BEHAVIORAL HEALTH COLLABORATION
Arizona Problem Solving Courts
Conference
Prescott, Arizona
April 28, 2015

TUCSON POLICE DEPARTMENT
Captain Paul Sayre
27 years law enforcement experience
Oversee TPD’s Central Investigations Division
Helped develop MHIST team, currently oversee MHIST Unit
Prior SWAT Commander
Sergeant Jason Winsky
10 years law enforcement experience
Supervises the Mental Health Investigation and Support Team (MHIST)

LAW ENFORCEMENT LINK TO BEHAVIORAL HEALTH SYSTEM
Kate Lawson
Criminal Justice Manager Team assists individuals in crisis and/or with
mental health disorders, wherever they are in the criminal justice system: court, jail, prison, probation, etc – including law enforcement
12 years experience in intersection of criminal justice and mental health

BIG PICTURETOPICS COVERED IN TODAY’S PRESENTATION
Concept: How can law enforcement, within it’s scope and mandate of community protection, work with individuals in crisis or with a mental
health disorder to improve public safety?
Catalyst for Change: Legal Issues Impacting Law Enforcement Interactions with Individuals with Behavioral Health Concerns
…Resulted in: Mental Health Investigative Support Team (MHIST) – Tucson Police Department
…And how it Fits into the larger continuum of Crisis and Behavioral Health Systems Crisis Intervention Team (CIT) Training vs. Mental Health First Aid (MHFA) Training
COURT RULINGS Regarding Law Enforcement and
“Emotionally Disturbed Persons”
EMOTIONALLY DISTURBED PERSON (EDP)
EDPCourt’s language
Terminology for anyone who has a mental illness or is in some other way inhibited/incapacitated by crisis

GLENN V. WASHINGTON COUNTY (2011)
Hillsboro, Washington County – 2006
18 year old Lukus Glenn, a popular high school athlete, was intoxicated and distraught over a recent break-up Returned home at 0300
Angry, intent on riding his motorcycle
Parents would not let him leave the house
He began damaging property, including doorway that led out to the garage
Prior to this event, Glenn had no history of violence or criminal activity
GLENN V. WASHINGTON COUNTY
Glenn held a 3 inch pocketknife to his neck and threatened to kill himself
Mom called 911believing that “the police would have the expertise and experience to deal with an emotionally distraught teenager.”
Call was dispatched as an armed domestic violence incident.

GLENN V. WASHINGTON COUNTY
Based on dispatch of “armed DV situation” Deputy goes directly to the house without conferring with other officers on scene or en route
Deputy finds family sitting with Glenn, who still has knife at his neck
Mother tells dispatcher “Don’t let him shoot him… They’re going to shoot him.”
Second deputy arrives and begins shouting at Glenn, like first deputy, “Drop the knife or you’re going to die!”
Second deputy also presented as “frantic and excited” and “only pursuing a course of screaming commands at Luke”.

GLENN V. WASHINGTON COUNTY
Family implored deputies to calm down
Deputies ordered family to go back inside the house
Sergeant radioed deputies to say “Remember your tactical breathing”
Ordered a officer from neighboring department to “beanbag him” Lucas defensively retreats from direction of
beanbag fire

GLENN V. WASHINGTON COUNTY
Deputies had independently determined if Glenn moved towards the house they would use deadly force Glenn (taking cover from bean bags) ran from
garage towards only exit—the house
Because he was headed toward house, where the other family members had been told to go, officers used deadly force
Deadly force occurred less than four minutes after the first deputy
arrived on scene
Seconds before he was fired upon, Glenn said “Why are you yelling?” and “Please tell them
to stop screaming at me!”

GLENN V. WASHINGTON COUNTY
Glenn bled out and died on the family porch within minutes.
In 2007, Washington County Sheriff Rob Gordon released their results of their shooting board and determined
No policies had been violated and
“WCSO deputies involved in this incident performed as trained, followed established policies, and acted in a professional manner.”
GLENN V. WASHINGTON COUNTY
Court’s decision….
“…we have made it clear that the desire to quickly resolve a potentially dangerous situation is not the type of governmental interest…that justifies the use of force that may cause serious injury (Deorle).”
“We also recognized in Deorle, that when dealing with EDP’s who is creating a disturbance or resisting arrest, as opposed to a dangerous criminal, officers typically use less forceful tactics.” (notice the change in language)

GLENN V. WASHINGTON COUNTY
Ruling, continued:
“The facts in this case, viewed in the light most favorable to the plaintiff, bear this out: Lukus did not respond positively to the officers’ forceful tactics, and just before officers fired the beanbag gun, Lukus pled, “Tell them to stop screaming at me’” and “why are you yelling?”
The Court now expects a differentiated
response from law enforcement.
Or…
“No excuse now – train your officers”

LESSONS LEARNED FROM GLENN
The Family hired a Subject Matter Expert, a former Bellevue, Washington Chief of Police. His professional opinion forms the basis for what should be our response to these situations with EDPs:
1. Slow it down,
2. Do not increase the subject’s level of anxiety or excitement,
3. Attempt to develop a rapport,
4. Time is on the side of the police

SHEEHAN AND HAYES
9th Circuit Opinions
Duty to Care-Now Extends to Actions PRIOR to critical incident
ADA Application-If Upheld, Will Change American Policing Forever
SO – ON ONE HAND WE HAVE NEW EXPECTATIONS ON USE OF FORCE…
BUT – ON THE OTHER HAND, GROWING PUBLIC SAFETY CONCERNS…

CREATION OF THE MENTAL HEALTH INVESTIGATIVE SUPPORT TEAM
MHIST

Public Safety
Community Service
TYPICALLY POLICE HAVE TO BALANCE THE TWO...

…MHIST SEEKS TO FIND SOLUTIONS FOR BOTH
Community Safety
Accountability
Treatment
Recovery

CREATION
Pima County Sheriff’s Department – 2013
Tucson Police Department –2013
Teams:
Sergeant
Detective(s)
Patrol Officers (Transport)

WHY
Law enforcement recognized the need to take a different approach to mental health issues related to law enforcement
The wave of mass shootings and the increased mental health related calls served as a catalyst for taking a fresh look

PURPOSE
Public Safety
Community Service
Risk Management
But also…
It’s the right thing to do.

FUNCTION
Mental Health Court Order Transports
“Title 36” in Arizona
Specialized training to avoid going hands-on
Locate/transport before order expires
Investigations
Circumstance code
Patterns of behavior
Problem-solving with mental health treatment
Title 36 petitions

MHIST = CIT PHILOSOPHY IN ACTION
Has to be a better way to approach problem
Need to
Decrease risk to officers/deputies
Decrease risk to community
Decrease waste of taxpayer dollars
BREAK THE CYCLE

Many people suffering from mental health issues fall between the cracks of the system
They always become the burden of law enforcement
MHIST AREA OF INTERVENTION
MHIST
Law Enforcement
Behavioral Health
Justice System (Courts)

OUT WITH THE OLD…
Old Way
Patrol Officers Serving COE Orders Court Ordered Evaluations orders served
before expiring = 30%
Patrol officers would look for the quickest, easiest solution to a situation with a mental health nexus Often resulting in arrest and incarceration
As a result, the Pima County Jail is now the largest behavioral health facility in southern Arizona
The problems continue
New Way
100 % service rate on mental health orders
Mental health facilities and providers communicating with law enforcement
One central location for patrol to go to for answers to problems
Law enforcement talking to law enforcement
CALL TRIAGE
Calls where there is not a threat to public safety (danger to self) are handled as they always have been-referred to the appropriate mental health provider
Voluntary committal
Involuntary committal
Referral to various providers
Calls for service where there is a criminal component, and the person is a threat to others (public safety)
Routed to the MHST Unit for follow up
A full criminal/mental health investigation is conducted where appropriate
A unique 2-pronged process is initiated

MHST INVESTIGATION

“Jose”
Jose is a Marine veteran and a student at Pima Community college
Jose perceived he was assaulted in the school library (unfounded)
He began making threats towards PCC personnel
Outcome Kept out of jail
Compliant with treatment
SUCCESSES
SUCCESSES
“Maria”
Young woman in her 20s, lives at home with her parents
Tucson City Court – Mental Health Court Diversion (misdemeanor charges)
Repeatedly calls 911 requesting transport to the Crisis Response Center Find that she is bored and wants out of the house
TPD participate in Adult Recovery Team (ART) meeting, along with treatment provider
Develop crisis plan that includes TPD differentiated response
WITH A CIT TRAINING PROGRAM +A MENTAL ILLNESS/CRISIS RESPONSE PROTOCOL
A Best Case Scenario
Officer is able to de-escalate the situation
Person is taken to crisis center and/or referred to community treatment “Breaking the Cycle” – avoid future interactions
Positive Community Policing
Financial Savings Officer time
Jail Days
Criminal Case Proceedings
Avoid going “hands on” Improved liability
Improved safety
But If the Outcome Is Bad Anyway…
Officer should be able to say:
“I am knowledgeable of and considered use of de-escalation techniques and community resources.
I still could not have handled the situation any other way.”
PREPARING ALL OFFICERS FOR SOMEPREPARING SOME OFFICERS FOR ALL
Ensuring behavioral health and
crisis training needs are met for
public safety

AUDIENCE POLL
How familiar are you with CIT?
Do you have a CIT program in your community?
Who facilitates?
How long is the training?
How familiar are you with Mental Health First Aid (MHFA) training?
CONTINUUM OF MENTAL HEALTH TRAINING
CIT & MHFA
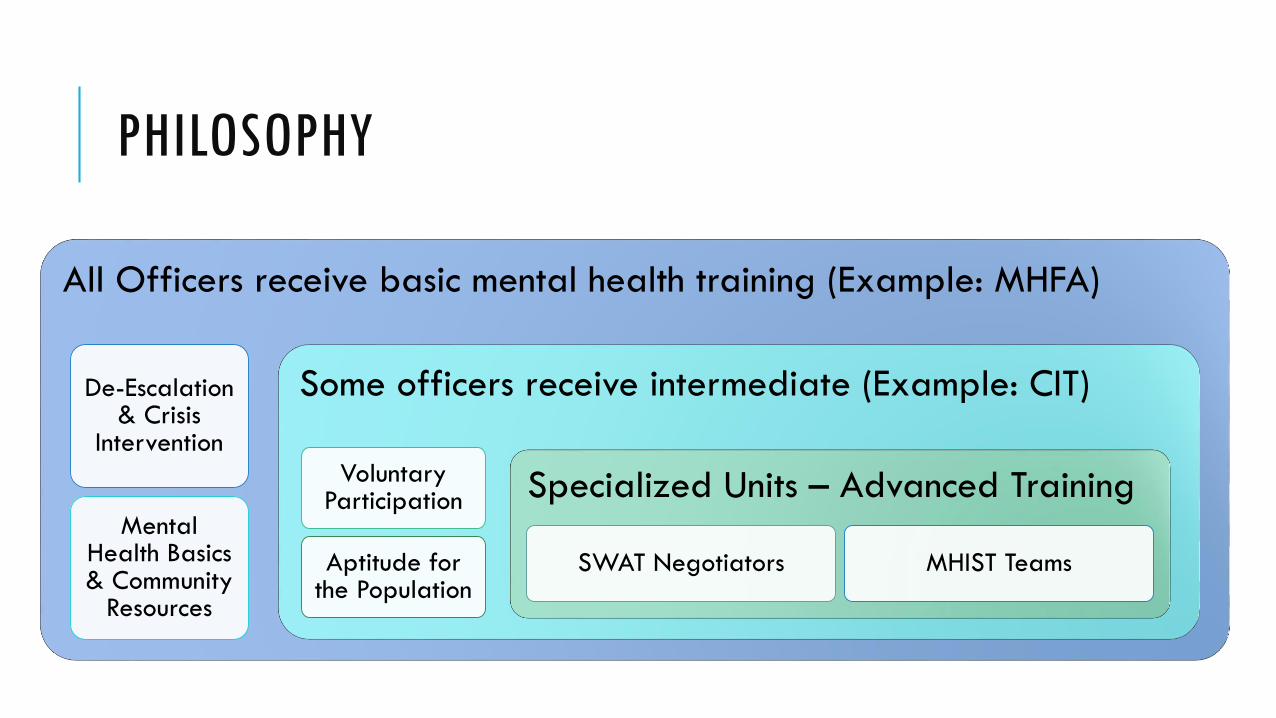
PHILOSOPHY
All Officers receive basic mental health training (Example: MHFA)
De-Escalation & Crisis
Intervention
Mental Health Basics & Community
Resources
Some officers receive intermediate (Example: CIT)
Voluntary Participation
Aptitude for the Population
Specialized Units – Advanced Training
SWAT Negotiators MHIST Teams
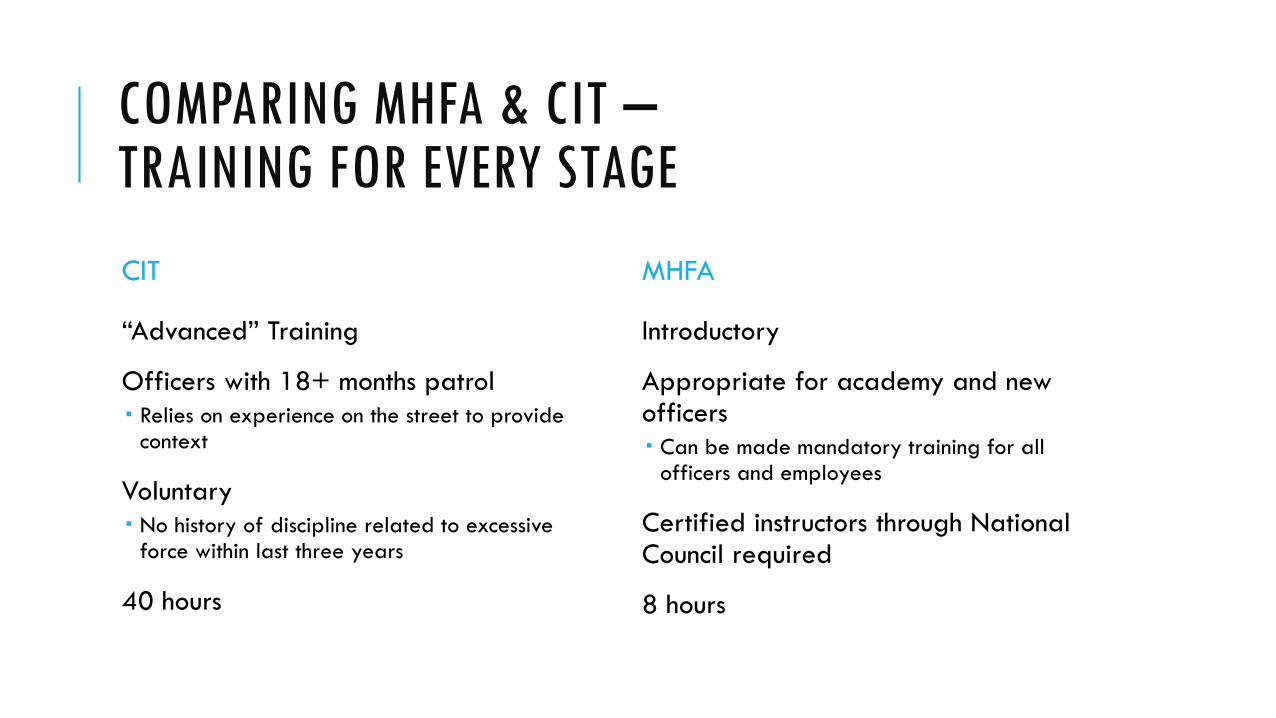
COMPARING MHFA & CIT –TRAINING FOR EVERY STAGE
CIT
“Advanced” Training
Officers with 18+ months patrol
Relies on experience on the street to provide context
Voluntary
No history of discipline related to excessive force within last three years
40 hours
MHFA
Introductory
Appropriate for academy and new officers
Can be made mandatory training for all officers and employees
Certified instructors through National Council required
8 hours

CORE ELEMENTS
Voluntary
Not “charm school”
No history of excessive force within 3 years
Some patrol experience
18 months+ recommended
No academy/post-academy
MHFA
Fidelity to Memphis Model


IS OBJECTIVE OF CIT TO ALWAYS USE DE-ESCALATION?
No, purpose of CIT is to give experiencedofficers:
TOOLS FOR
THE TOOL BOX
Objective:
Provide skills to be able to de-escalate individuals and situations, when appropriate
Does not override tactical training
Officer and citizen safety is always paramount

MENTAL HEALTH FIRST AID (MHFA)
Established in 2001 in Australia
Like CPR, designed to be quick response for emergent situations
“First responder”
8 hours
Includes certification
Specialized modules
Law Enforcement
Veterans
Spanish

RESULTS SUMMARY
Law Enforcement Training
Specialized LE Teams (MHST)
A responsive Crisis System Facility
24/7/365 phone line
MAC teams
Communication between Law Enforcement, Criminal Justice System & Mental Health Treatment
Support & Buy-In from Consumers & Advocates (NAMI)
WORKING AT AN INTERSECTION –NOT A PARALLEL
Behavioral Health working with
Law Enforcement to Achieve
Better Outcomes for Clients

WHOSE GOAL – TREATMENT, OR POLICE?
Engaged in TreatmentProductive Citizen

CHANGING OPINIONS - CHANGING LIVES
“If a mentally ill person has done something
wrong, they should go to jail”
“When a mentally ill person is arrested, it
represents a failure of the mental health system.”
“I’m not going to help the police catch my client.”
GOALS OF BEHAVIORAL HEALTH TREATMENT NOT AT ODDS WITH JUSTICE SYSTEM
“Accountability is therapeutic” -Kate Lawson
Involvement with the justice system can be the point of intervention for client
With the right interventions, and the right collaborations with the justice system, justice contact can become the support system needs to obtain recovery
Goals of the CJ Team
1. Improve client’s lives
2. Save taxpayer dollars
3. Improve public safety
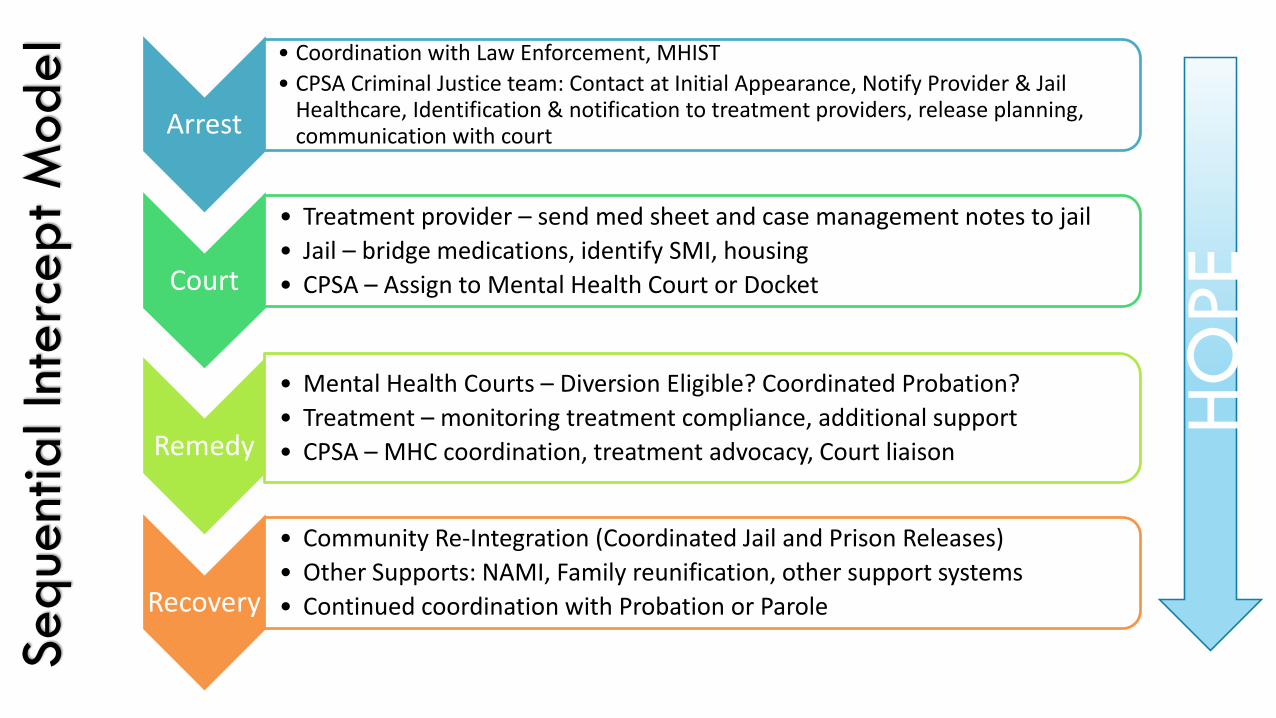
Seq
uent
ial In
terc
ep
t M
od
el
Arrest
• Coordination with Law Enforcement, MHIST
• CPSA Criminal Justice team: Contact at Initial Appearance, Notify Provider & Jail Healthcare, Identification & notification to treatment providers, release planning, communication with court
Court
• Treatment provider – send med sheet and case management notes to jail
• Jail – bridge medications, identify SMI, housing
• CPSA – Assign to Mental Health Court or Docket
Remedy
• Mental Health Courts – Diversion Eligible? Coordinated Probation?
• Treatment – monitoring treatment compliance, additional support
• CPSA – MHC coordination, treatment advocacy, Court liaison
Recovery
• Community Re-Integration (Coordinated Jail and Prison Releases)
• Other Supports: NAMI, Family reunification, other support systems
• Continued coordination with Probation or Parole
HO
PE