Embed Size (px)
Citation preview
TRiM
Trauma Risk Management
An organisational approach to traumatic stress management
Neil Greenberg
Defence Professor of Mental Health
Surg Cdr RN
Overview
What are the effects of traumatic stress
Why bother doing anything
What is TRiM
Does it work
Why is mental health (MH) important?
• In 2008 ~ 13.5 million days were lost to work-related stress in the UK
• With MH conditions, reduced productivity accounts for 1.5 X as much working time lost as SA
Why is MH important?
Mean time certified for a person with MH problems (15/52) nearly twice as long as the mean for all conditions (8/52)
Recent examination of medically examined incapacity benefits claimants found 27% had only a mental health condition
53% had a MH primary condition & a physical condition
17% had MH as a secondary condition

MH and Incapacity benefit
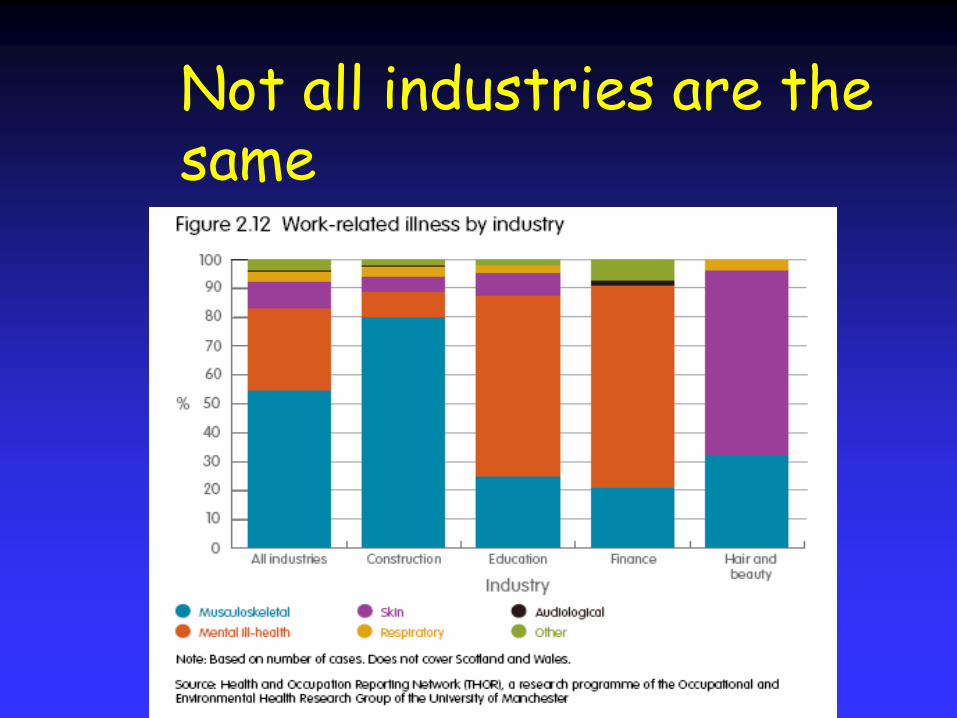
Not all industries are the same


Traumatic Events
Near Death, Road Traffic Accident, Serious Assault……
Primary and Secondary victims
Normal coping
Don‟t forget the other stressors too (hours, relationships, health etc)
Why use TRiM????
Moral
Legal
Economic
MOD Court Case

Case details
Evidence given in court Mar 2002- Oct 2002
Single Judge Lord Owens
>20 “expert witnesses”; teams of barristers
MOD won the case
MoD lesson‟s to be learned paper: More research
Commander need to be able to spot those with problems
Change culture
Number of important issues arose from the case
Why not screen people before starting work in order to only employ those who will not develop mental health disorders??
Screening

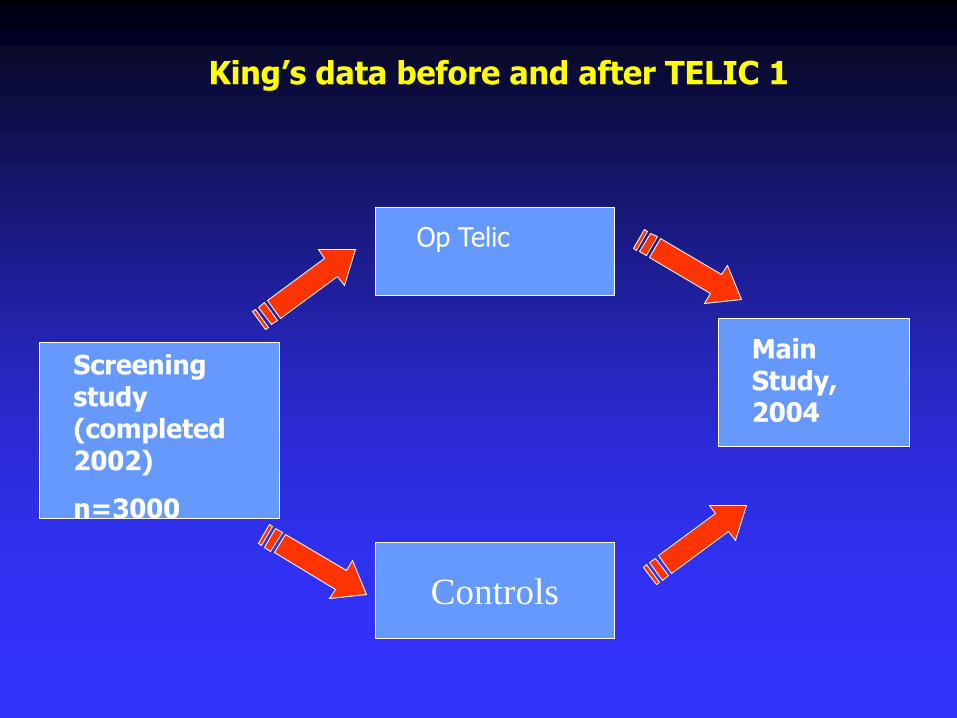
King‟s data before and after TELIC 1
Controls
Op Telic
Main Study, 2004
Screening study (completed 2002)
n=3000
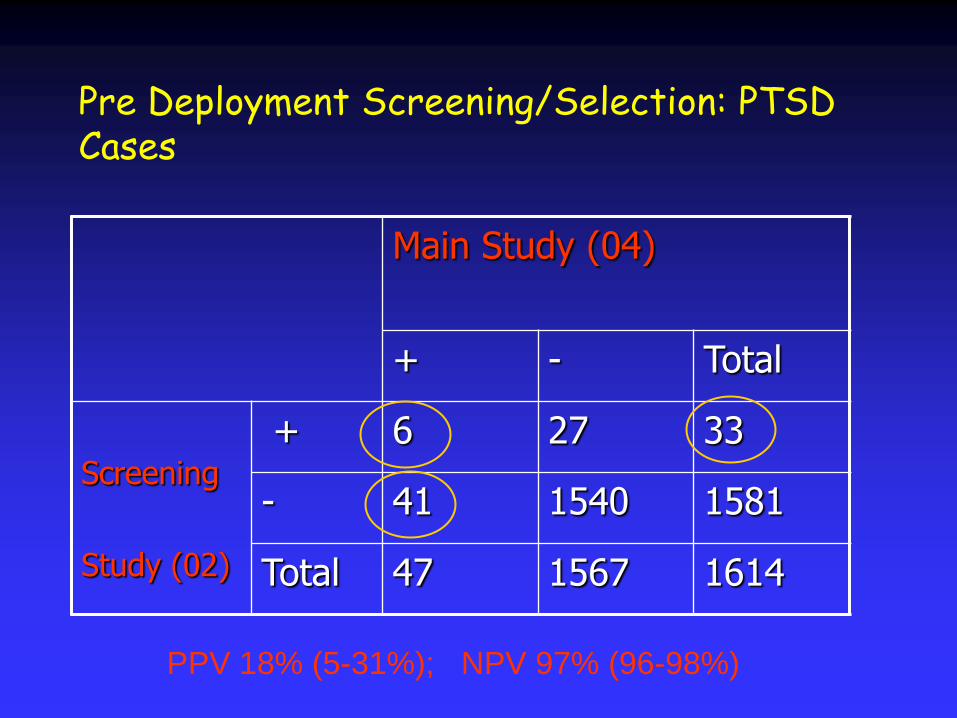
Pre Deployment Screening/Selection: PTSD Cases
Main Study (04)
+ - Total
Screening
Study (02)
+ 6 27 33
- 41 1540 1581
Total 47 1567 1614
PPV 18% (5-31%); NPV 97% (96-98%)
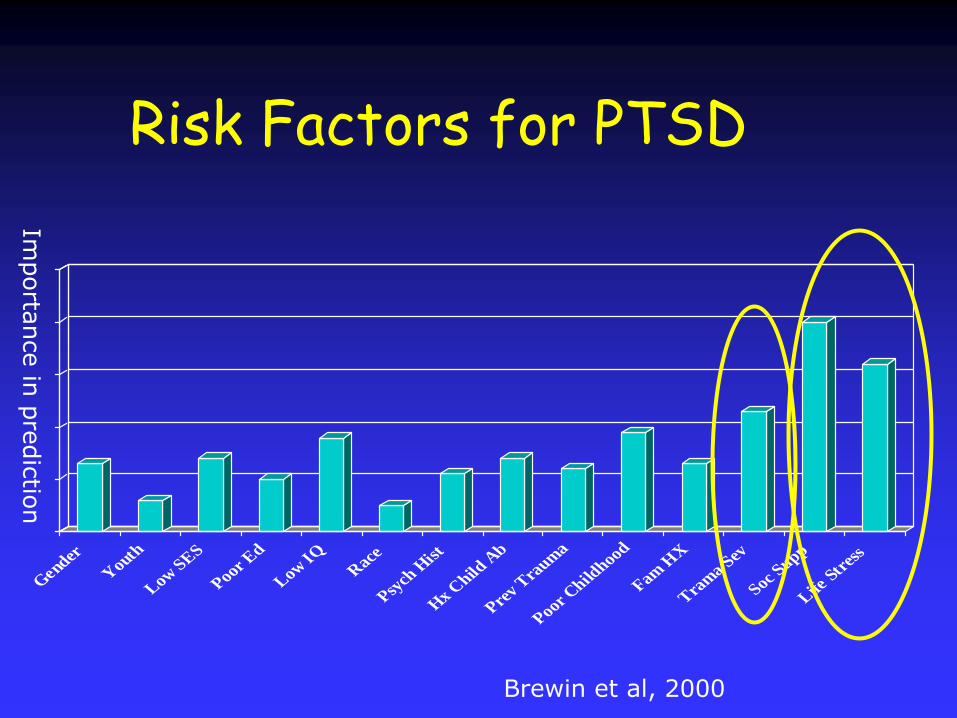
Risk Factors for PTSD
0
10
20
30
40
50
Gender
Youth
Low SES
Poor Ed
Low IQR
ace
Psych
Hist
Hx C
hild A
b
Prev T
raum
a
Poor Child
hood
Fam H
X
Tram
a Sev
Soc Supp
Life S
tres
s
Importa
nce in
pre
dic
tion
Brewin et al, 2000

So is it all about the “ stiff upper lip”
It has been alleged that „military culture‟ is hostile to admitting psychological distress
This is said to come from the top and is “wrong”
But is this true?

What is stigma?
“an attribute that is deeply discrediting” (Goffman,
1963)
“a mark that defines him/her as deviant, flawed, limited, spoiled or generally undesirable”(Jones,1984)
“may be more devastating, life-limiting and long-lasting than the primary illness” (Schulze et al,
2003)

The history of stigma in the military
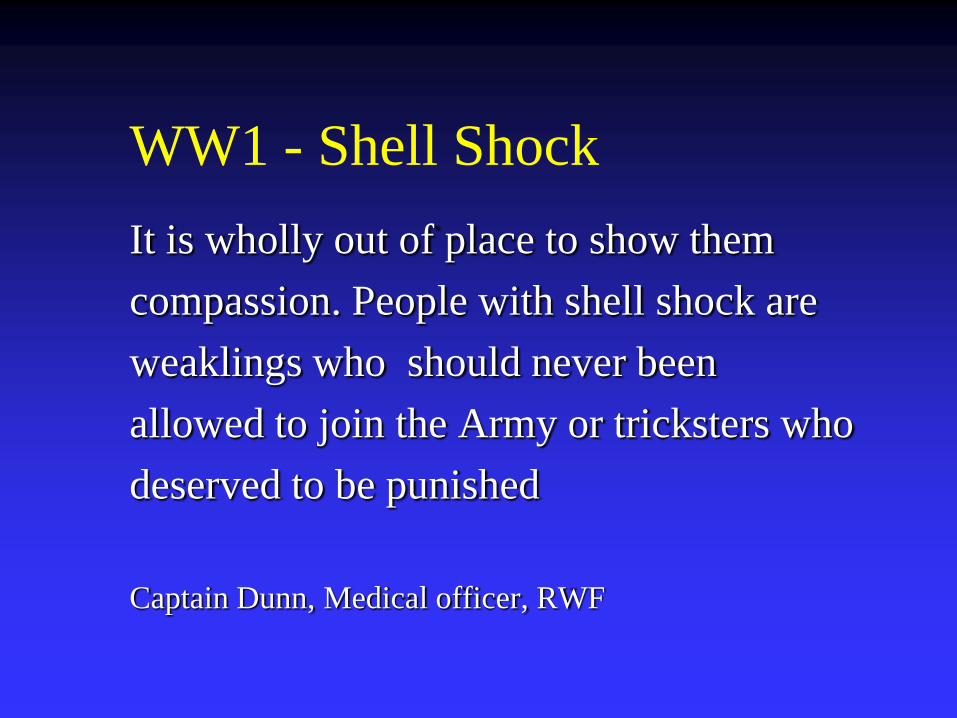
WW1 - Shell Shock
It is wholly out of place to show them
compassion. People with shell shock are
weaklings who should never been
allowed to join the Army or tricksters who
deserved to be punished
Captain Dunn, Medical officer, RWF

WW2 - Psychiatric casualties
Royal Air Force and Lack of Moral Fibre
(LMF)
General Patton & Italy
Vietnam veterans
Stigma - Legal
UK MOD Court Case 2002/2003
“there can be no doubt that….there was a stigma
attached to psychiatric/psychological disorder. It
was seen to be a sign of weakness which, if
revealed, would expose an individual to ridicule,
and would be the „kiss of death‟ to a military
career”
Learning Point
Stigma and Barriers to Care are not new
Until the end of WW2 stigma was a highly
institutional issue
Stigma is still recognised as a serious concern
by UK Courts
But stigma all about being in the
military??

0
5
10
15
20
25
30
35
40
45
Perceived as
weak by
managers
Adversly affect
promotion
Less chance of
being given
responsibility
Not trusted by
peers
Embarrassed abt
asking for help
Peers would
tease
Greenberg et al, Journal of Mental Health, 2009,In press
UK Journalists also report internal stigma
%
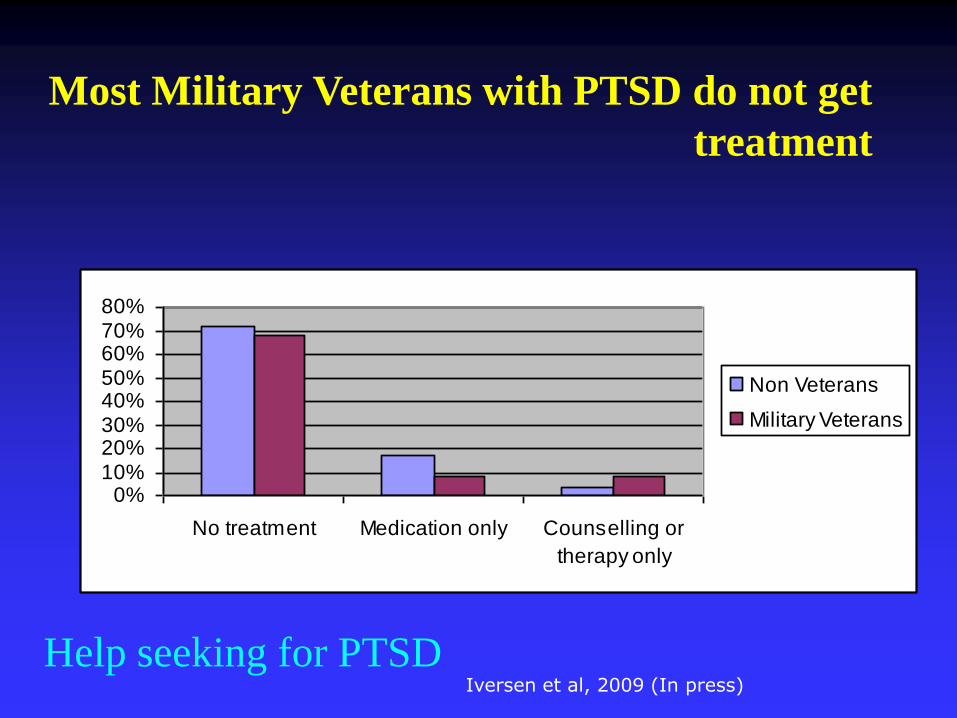
Help seeking for PTSD
0%10%20%30%40%50%60%70%80%
No treatment Medication only Counselling or
therapy only
Non Veterans
Military Veterans
Most Military Veterans with PTSD do not get
treatment
Iversen et al, 2009 (In press)

Learning point
Stigma is not just an issue for the military
Stigma does not go away when military
personnel leave service
Most UK military veterans who have PTSD
don’t get help (nor do civilians!)
So…if people don’t speak to medics
who do they speak to ?

0
10
20
30
40
50
60
70
80
90
100
military peer
group same
deployment
spouse or
partner
another
family
member
military peer
group not on
same
deployment
civilian
friends/peer
group
chain of
command
medical
services
w elfare
services
Greenberg et al, JMH, 2003
Why peers are important?

Why don‟t we provide “counselling for all”?

A single session intervention??
CISD/PD - What is it? A group meeting after a PTE
1-3 hours duration, seven stages including discussing
Thoughts
Feelings
Reactions
Future planning and coping
Aimed to promote normal recovery of normal people exposed to abnormal events
Aimed to prevent PTSD
Summary of Outcomes (after numerous RCTs)
CISD type SS PD with individual victims is generally ineffective
It may make some symptoms worse
Non intervention groups do better
Victims reporting that a session has felt helpful is not an indicator of symptom resolution
UK military SG banned CISD in 2000

And DoH
“Single session debriefing appears to be
unhelpful in preventing later disorders”
DOH, Treatment choice in Psychological
therapies and counselling, Feb 2001
How to deal with PTSD (NICE slide edited)
What isn’t recommended…
•“Psychological Debriefing”
•Ineffective psychological treatments
•For PTSD, drug treatments NOT a first line treatment (different
for depression)
What is recommended…
•“Watchful Waiting”
•Checking in after a month
•Trauma-focused treatments (CBT and EMDR) for adults and
children if unwell

Other important background
Social support
Cohesion
Leadership
Morale
„Normal‟ Symptoms
Vaillant study (Lee et al, 1995) 107 WW2 veterans who had served overseas 50 year prospective study
More combat exposure more PTSD Sx 40 years on
BUT better psychosocial outcomes (employment, social life
and marital satisfaction)more likely to be in “Who‟s Who in America”
So Sx are not the same as disability

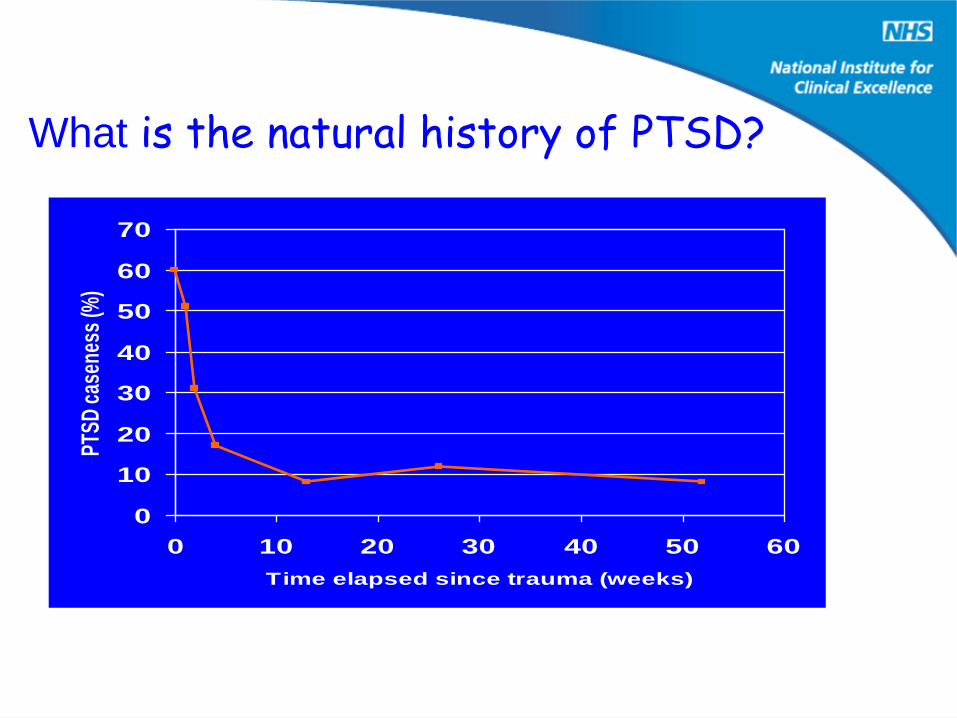
What is the natural history of PTSD?
0
10
20
30
40
50
60
70
0 10 20 30 40 50 60
Time elapsed since trauma (weeks)
PTS
D c
asen
ess
(%)
PTSD ‘caseness’ of patients directly involved in a raid over time. Data from Richards (1997) The Prevention of PTSD
after armed robbery: the impact of a training programme within Leeds Permanent Building Society.


TRiM - primarily a human resource initiative
Reinforces effective personnel management
TRiM does not aim to be a cure
Aims to assess need
Problem solving, mentoring & referral
Not psychological debriefing/CISD
Trauma Risk Management

It formed 12 (+) years ago
Began in Royal Marines units, now Tri-Service
They range in rank from Marine to Brigadier
Now used by BBC, FCO, St John and London Ambulance Services and some UK Police Forces
Trauma Risk Management
Why use Peer Group Practitioners?
Share common life experiences & ethos
Understand the language & jargon
Reduction of stigma because non medical
They are readily available
Organisations can „consume their own smoke‟

What Peer Practitioners are not!
Counsellors
Therapists
Pseudo-psychologists
Group Huggers
Scented Candle users
How TRiM is organised?
In the military 9-14 practitioner for 600
In the FCO based in major consulates & RDT
In LAS, is an additional LINC role
In media companies – based in major bureaus
TRiM training - Aims and Objectives
1. Psychological site management
2. Planning & filtering the event
3. Trauma Risk Assessment interviewing . 3/7
. 1/12
4. Psycho-educational briefing
5. Feedback to managers & facilitate referral

CH47 crash
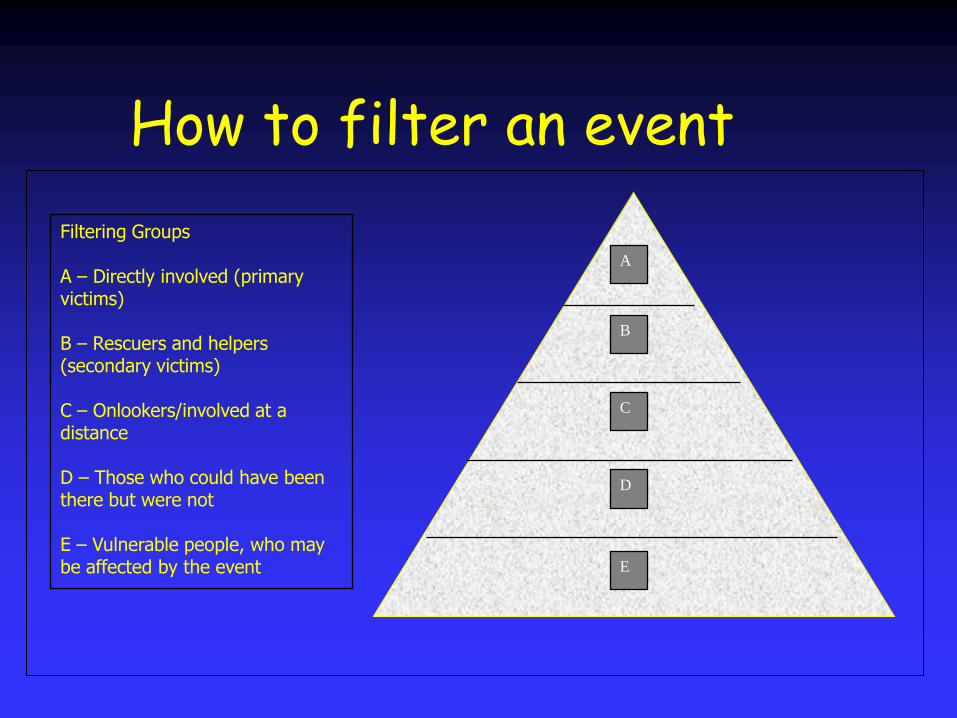
How to filter an event
Filtering Groups
A – Directly involved (primary victims)
B – Rescuers and helpers (secondary victims)
C – Onlookers/involved at a distance
D – Those who could have been there but were not
E – Vulnerable people, who may be affected by the event
B
D
C
A
E
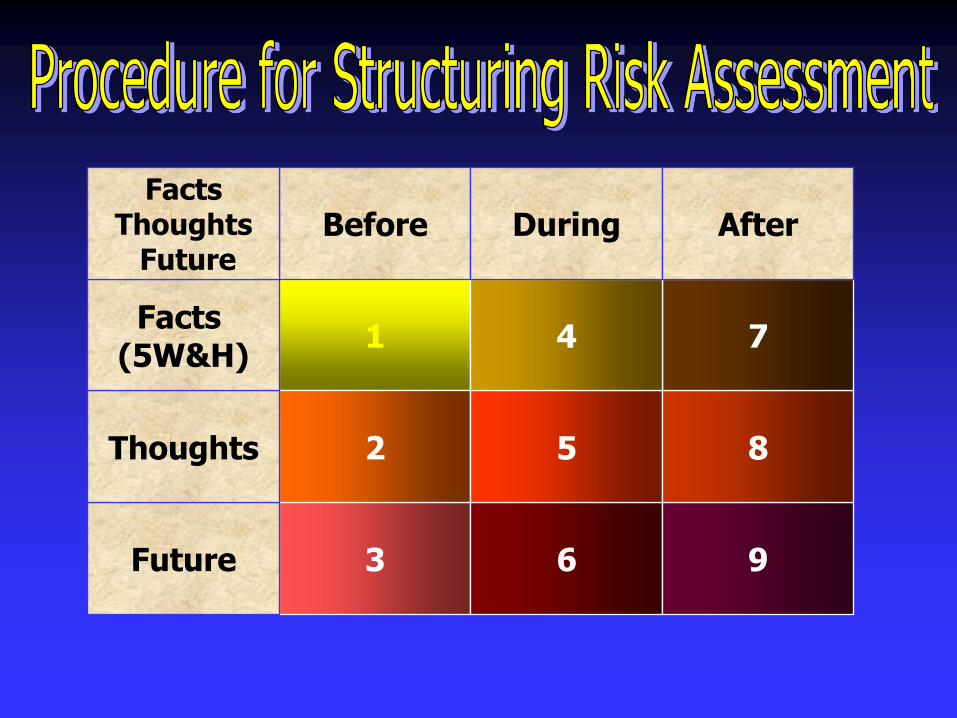
1
3 6 9
2 5 8
74
Future
Thoughts
Facts (5W&H)
Before During AfterFacts
ThoughtsFuture
How not to do it!!

Risk Assessment Checklist
1. The person perceives that they were out of control during the event
2. The person perceives that their life was threatened during the event
3. The person blames others for what happened
4. The person reports shame/guilt about their behaviour during the event
5*. The person experienced acute stress following the event
6. The person has been exposed to substantial stress since the event
7. The person has had problems with day to day activities since the event
8. The person has been involved in previous traumatic events
9. The person has poor social support, (family, friends, unit support)
10. The person has been drinking alcohol excessively to cope with distress

TRiM Training - Practitioner Profile
• They should be volunteers
• They should be „empathic‟ and have the ability to listen to his or her colleagues, not be overtly directive or opinionated.
• They should have good life experience & have sound common sense…like this!

TRiM
How might it and does it work?
TRiM
Two modes of functionPost incident formal activation
Informal access as and when
Trained personnel within units
Owned by line managers, supported by medical services

Potential benefits
Occupational To prevent LT sickness absence
Health PTI management Stigma reduction measure
Reputational/Political „do something‟ Research based
Avoidance of „snake charmers‟ e.g. TFT, flying in counsellors, NLP
Studies and data
RCT – qual and quant
TRiM practitioners
Through the deployment cycle
Diplomatic staff
Audit of military use
Can we measure recovery (or not) after traumatic events?

TRiM & IES change in scores
There was a strong correlation between the change in the IES score and the change in the TRiM score (r=0.59)
Greenberg et al,
JMH, 2009
Can you train TRiM practitioners?
TRiM practitioner trial
• Parallel group (n=~100) 1 month FU trial
• TRiM trained led to better attitudes to stress & help seeking and better health!
• Improvement maintained at one month
Gould et al, JTS, 2007

But does it make any difference?

Royal Navy TRiM Study
• 12 vessels (case(6) & control(6))
• Approx 200 people per ship
• Baseline measurements (Survey & interview)
• 12-18 months to „cook‟
• Examined:• attitudes towards stress
• occupational functioning
• potential to “harm”
TRiM RCT QuantitativeModest organisational benefit
• No sig effect on psych health or stigma
• Modest benefit to occupational functioning
0
50
100
150
200
250
Before After
TRiM
Non- TRiM
Greenberg et al, JTS, 2010

• Very acceptable in the few that used it
• Concern over the right people being trained
• Concern over leaders supporting its use
• Supplements rather than replaced other support
TRiM RCT – Interview data
Greenberg et al, Occ Med, Sub
Can TRiM improve social support?

Study sample
Non-randomised parallel group comparison
Deployed to Afghanistan Sept/Oct 2007
Royal Marines Commandos (experienced)
Coldstream Guards (naiive)
Small sample size (between 46 and 94)
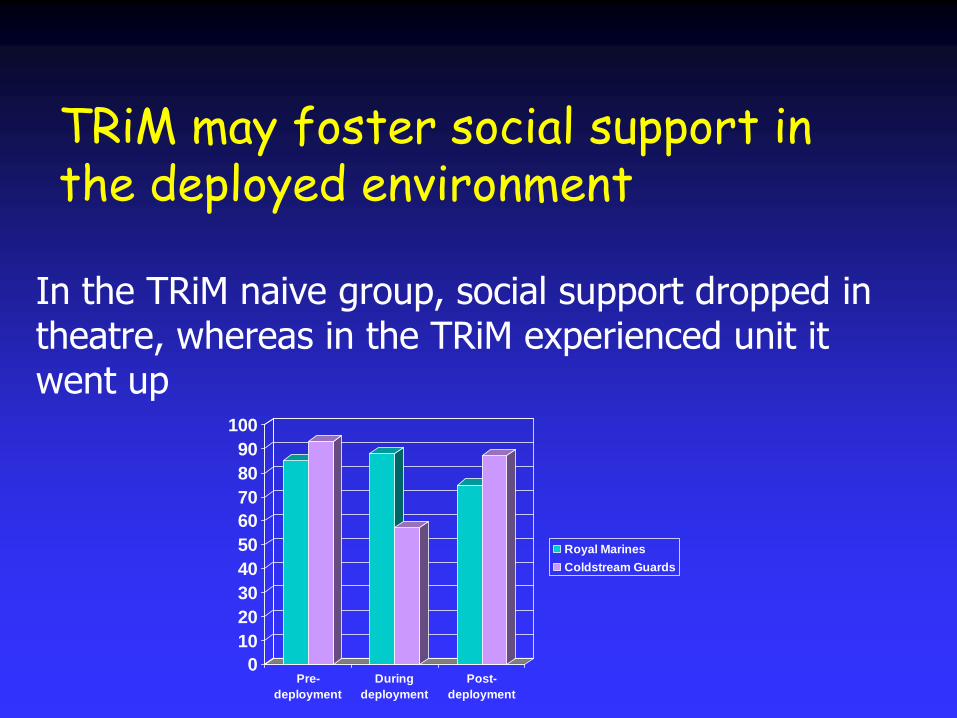
TRiM may foster social support in the deployed environment
0
10
20
30
40
50
60
70
80
90
100
Pre-
deployment
During
deployment
Post-
deployment
Royal Marines
Coldstream Guards
In the TRiM naive group, social support dropped in theatre, whereas in the TRiM experienced unit it went up
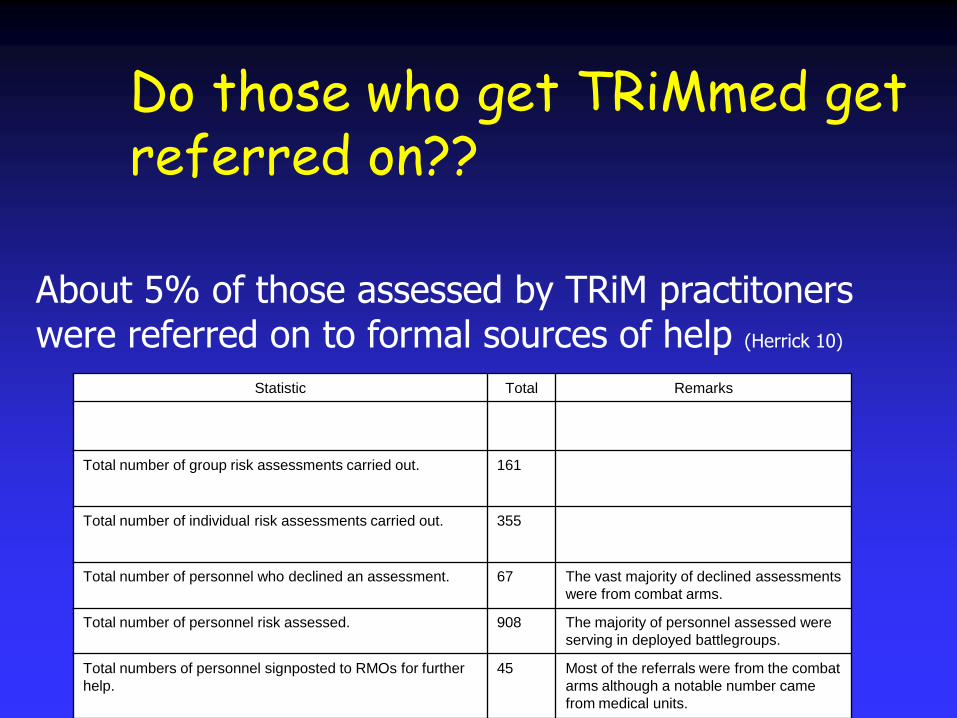
Do those who get TRiMmed get referred on??
Statistic Total Remarks
Total number of group risk assessments carried out. 161
Total number of individual risk assessments carried out. 355
Total number of personnel who declined an assessment. 67 The vast majority of declined assessments
were from combat arms.
Total number of personnel risk assessed. 908 The majority of personnel assessed were
serving in deployed battlegroups.
Total numbers of personnel signposted to RMOs for further
help.
45 Most of the referrals were from the combat
arms although a notable number came
from medical units.
About 5% of those assessed by TRiM practitoners were referred on to formal sources of help (Herrick 10)

So…
• TRiM may help spot people who are in need
• TRiM may help mobile social support
• TRiM may help with occupational functioning
• TRiM use appears acceptable
• TRiM may help with stigma/barriers to care

Any Questions??