Embed Size (px)
Citation preview

REVIEWARTICLE - HISTORY OF NEUROSURGERY
Trepanation and surgical infection in the 18th century
Jeremy C. Ganz
Received: 22 August 2013 /Accepted: 23 September 2013 /Published online: 8 October 2013# Springer-Verlag Wien 2013
AbstractBackground It is widely believed that trepanation prior tomodern surgical hygiene was dangerous because of surgicalinfection, especially in the hospital. There has been a widevariability in the success and risks of different historical studiesPurpose To obtain a more accurate assessment of the risks ofpost-operative infection following 18th-century cranial traumaand to note what factors were of prognostic significance.Material and methods Seven 18th-century texts on head injuryare reviewed and analyzed.Results Infection was the commonest cause of death (in over60% of patients) in five series but not in the other two. Hospitaladmission did not appear to be a major factor influencingmortality from infection. Delayed infection was the indicationfor patient referral and trepanation in more than two patients intwo series. In one series, the patients were helped by theprocedure, in the other they were not. The reasons for thedifference are discussed. The most striking finding was thatpatients treated in rural areas had a much better prognosis.Conclusions The risks of suffering a surgical infectionfollowing head injury and trepanation are multifactorial. Admis-sion to hospital seems to have been less risky than has beenpreviously thought. It seems that the greatest risk factor for alethal infection for these patients was living in an urbanenvironment.
Keywords Head injurymanagement . Trepanation .
Infection . Urbanization . 18th century
Introduction
It is a truism that prior to the invention of antisepsis andasepsis post-operative infections were much more of a risk
than since. One operation which was known to be riskierbecause of such infection was trepanation. There was andremains a widespread belief that hospitals could increase therisk. This was mentioned contemporaneously by Quesnay[34] and Desault [6] in France. Quesnay quotes the view ofa surgeon called Mr. Boudon writing: “Mr. Boudon howeverwould not upon these conjectures...hazard the trepan, whichseldom succeeded at the hospital, on account of the unwhole-some state of the air” [34]. Recent reviews confirm thecontinuation of this notion in the current literature [13, 17, 18].
However, a review of surgical series from the 18th centuryhad led the author to realize that while infection associatedwith trepanation was common in that century, it is not at allcertain that these were mostly hospital or surgical infections[16]. Nor is it clear that infection was so dangerous that it wasa genuine contraindication to trepanation. Moreover, there isan additional element to consider; something of a mystery.This is a remark of Arbosellius, mentioned by Kellett in theintroduction to the now out-of-print head injury text by G. F.Rowbotham and quoted by Dr. Teo Forcht Dagi in his chapter“The Management of Head Injuries” in the AANS publishedreference work “A History of Neurosurgery. The quotationruns as follows. “Arbosellius was wont to tease Vesalius andhis fellow surgeons asking them “Why is it that those whoreceive a head injury in Verona, no matter how slight cannotbe cured, and the unfortunate patient, forsaken by his physi-cians, dies miserably, but, as I have often seen, he is cured inPadua and Venice?” [13] It would be interesting to know thesolution to this inconsistency.
The 18th century saw the beginnings of the evolutionwhich led neurosurgery away from Galenic mythologytowards the acquisition of knowledge on which current prac-tice is based. The purpose of this paper is to present the patternof infection in the seven available English language seriesfrom that century. The influence of surgical hospital infectionwill be examined as will the value of trepanation in cases withestablished infections. Reasons for the variation of result withlocation will also be analyzed.
J. C. Ganz (*)53 Market Street, Ulverston, Cumbria LA12 7LT, UKe-mail: [email protected]
Acta Neurochir (2014) 156:615–623DOI 10.1007/s00701-013-1900-0

Background
At the beginning of the 18th century, there was considerableawareness of the processes now known to be due to infectionwhich are both local and systemic. The local components wereinflammation and pus. The components of inflammation,rubor, tumor, dolor and calor had been known since Celsusdescribed them [11]. This was understood in the same waythen as now, when applied to tissues which could be seen ortouched. However, in 18th-century texts the term inflamma-tion needs to be interpreted with caution when used withregard to invisible tissues such as the brain. A good exampleis provided by Sylvester O’Halloran, who mentions that “Nowevery one knows, that inebriety, which is a kind of temporaryinflammation of the brain, is most sensibly relieved by strongtea or coffee; and is it not surprizing, that such obvious effectsare not applied to practical cases” [30]. This is obviously notcurrent usage. In addition, the term sepsis was used. It isderived from the Greek word [σηψις] meaning “decomposi-tion of animal or vegetable organic matter” [8]. It includes theprocesses of necrosis as registered by changes in the color andconsistency of the tissues. Moreover, there was the evidenceof unpleasant odors. There was also awareness of at least twodifferent kinds of pus; white thick ‘laudable’ pus thought toassist healing by secondary intention and runny thin oftenbrown foul smelling fluid called ‘sanies’. It is seems unlikelythat sepsis and laudable pus were seen as related phenomena.The systemic features of sepsis included fever, fatigue andlistlessness. The full picture specific for infected cranialwounds was best described by Percivall Pott [32]. It consistedof deterioration following an initial improvement usuallyafter a latent interval of several days. Characteristically,there would be delirium, fever, fatigue, vomiting and oftenfocal and subsequently spreading headache. These reportedfindings are taken to indicate infection even though theoriginal authors did not use that term.
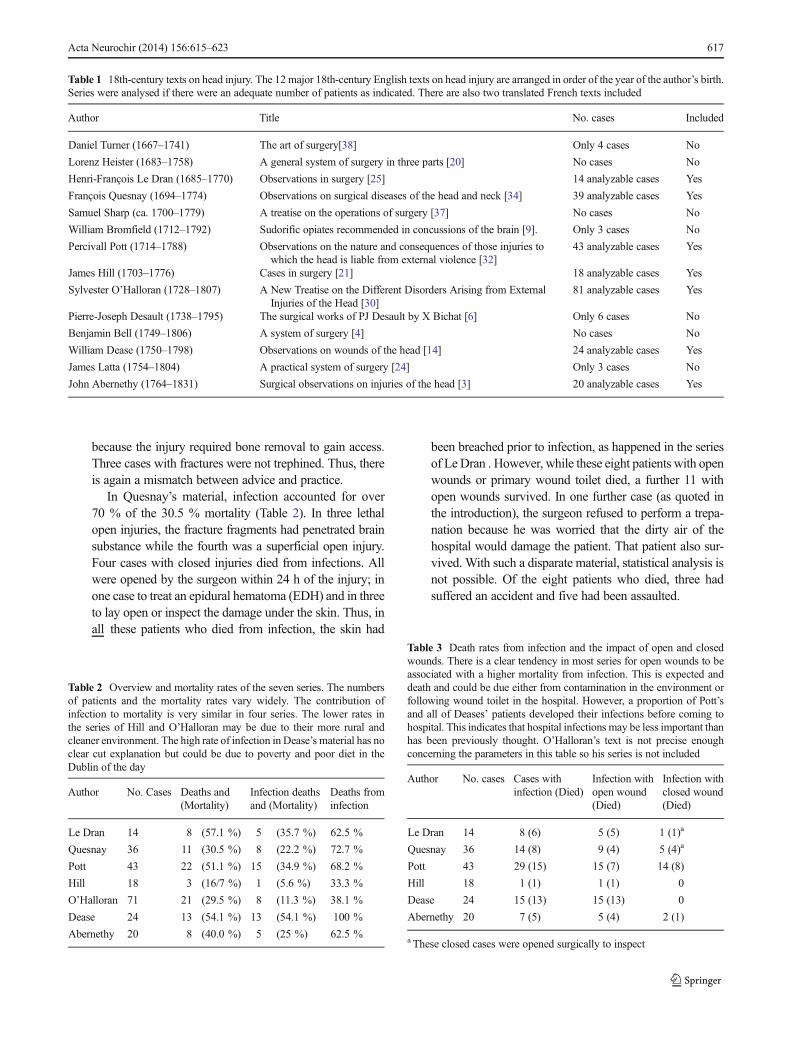
Twelve major English language texts were written on headinjuries in the 18th century. In addition, two French bookswritten in the 18th century and translated into English in the19th century made a significant contribution. These 14 textsare tabulated in Table 1. Of these writings, seven includesubstantial numbers of patients, making them suitable foranalysis in this article.
Spontaneous separation of the pericranium
One phenomenon which was of great concern in this contextwas separation of the pericranium from the skull. Separationof pericranium from the bone as a result of the mechanicaltrauma itself was not considered a cause for concern. However,it was believed that spontaneous separation of the pericraniuminterrupted or occluded the small blood vessels that passedthrough the cranium from the pericranium on the outside to the
dura on the inside. This led to damage of the bone with asimilar separation of the dura from the craniumwith the risk ofsecondary inflammation and putrefaction [32].
Management of sepsis associated with cranial trauma
The seven contributors had varying attitudes about appropriatesurgical management as outlined below.
Henri-François Le Dran (1685–1770)Le Dran was an enthusiastic proponent of trepanation
for depressed fractures and fissures because he believedthat the risk of inflammation and putrefaction of the duracould be avoided by this means. He also considered smallfissures more dangerous since wider fractures wouldpermit the escape of fluids trapped under the bone. Despitehis encouragement to perform trepanation whenever afracture was present, his actual practice was at variancesince he only trepanned four of his 14 patients, or 28.6 %.There were five fractures in his series and only two weretrephined. One patient refused surgery but the remainingtwo with fractures were simply not operated. Thus, LeDran’s teaching and practice were somewhat at odds.
Table 2 shows the distribution of infections in the sevenseries. It may be seen that infection was the commonestcause of death in all but two series, underlining its impor-tance. In Le Dran’s material, infection accounted forover 60 % of a total mortality of nearly 36 %. Five ofthe six patients who died from infections had openwounds, making it impossible to be sure of the sourceof the infection, which could have come from theoriginal wound, the wound toilet or subsequent woundmanagement. The sixth patient had a closed injury butthe skin was incised and skull inspected a short timeafter the injury. Thus, in essence all the injuries weretechnically open. There were two infected cases whosurvived. Table 3 shows the relationship between infec-tions and wound status.
Of the patients who died from infections one sufferedan accident and the other five were victims of assault.Francois Quesnay (1694 – 1784)
Quesnay was later to arouse the wrath of, amongstothers, John Bell of Edinburgh [5] for his advice to tre-phine any patient with a fissure or a depressed fracture. Headmitted that there were cases where trepanation could beavoided but they were rare and required experience andjudgment. He admitted other surgeons had a different viewbased on the perceived risks of trepanation. However,Quesnay argued that the risks of the operation were sub-stantially less than the risks of the unoperated injury. In hisseries, however, only 13 of 37 patients were trephined, or35 %. Quite a few patients did not require trepanation
616 Acta Neurochir (2014) 156:615–623
because the injury required bone removal to gain access.Three cases with fractures were not trephined. Thus, thereis again a mismatch between advice and practice.
In Quesnay’s material, infection accounted for over70 % of the 30.5 % mortality (Table 2). In three lethalopen injuries, the fracture fragments had penetrated brainsubstance while the fourth was a superficial open injury.Four cases with closed injuries died from infections. Allwere opened by the surgeon within 24 h of the injury; inone case to treat an epidural hematoma (EDH) and in threeto lay open or inspect the damage under the skin. Thus, inall these patients who died from infection, the skin had
been breached prior to infection, as happened in the seriesof Le Dran . However, while these eight patients with openwounds or primary wound toilet died, a further 11 withopen wounds survived. In one further case (as quoted inthe introduction), the surgeon refused to perform a trepa-nation because he was worried that the dirty air of thehospital would damage the patient. That patient also sur-vived. With such a disparate material, statistical analysis isnot possible. Of the eight patients who died, three hadsuffered an accident and five had been assaulted.
Table 2 Overview and mortality rates of the seven series. The numbersof patients and the mortality rates vary widely. The contribution ofinfection to mortality is very similar in four series. The lower rates inthe series of Hill and O’Halloran may be due to their more rural andcleaner environment. The high rate of infection in Dease’s material has noclear cut explanation but could be due to poverty and poor diet in theDublin of the day
Author No. Cases Deaths and(Mortality)
Infection deathsand (Mortality)
Deaths frominfection
Le Dran 14 8 (57.1 %) 5 (35.7 %) 62.5 %
Quesnay 36 11 (30.5 %) 8 (22.2 %) 72.7 %
Pott 43 22 (51.1 %) 15 (34.9 %) 68.2 %
Hill 18 3 (16/7 %) 1 (5.6 %) 33.3 %
O’Halloran 71 21 (29.5 %) 8 (11.3 %) 38.1 %
Dease 24 13 (54.1 %) 13 (54.1 %) 100 %
Abernethy 20 8 (40.0 %) 5 (25 %) 62.5 %
Table 3 Death rates from infection and the impact of open and closedwounds. There is a clear tendency in most series for open wounds to beassociated with a higher mortality from infection. This is expected anddeath and could be due either from contamination in the environment orfollowing wound toilet in the hospital. However, a proportion of Pott’sand all of Deases’ patients developed their infections before coming tohospital. This indicates that hospital infections may be less important thanhas been previously thought. O’Halloran’s text is not precise enoughconcerning the parameters in this table so his series is not included
Author No. cases Cases withinfection (Died)
Infection withopen wound(Died)
Infection withclosed wound(Died)
Le Dran 14 8 (6) 5 (5) 1 (1)a
Quesnay 36 14 (8) 9 (4) 5 (4)a
Pott 43 29 (15) 15 (7) 14 (8)
Hill 18 1 (1) 1 (1) 0
Dease 24 15 (13) 15 (13) 0
Abernethy 20 7 (5) 5 (4) 2 (1)
a These closed cases were opened surgically to inspect
Table 1 18th-century texts on head injury. The 12major 18th-century English texts on head injury are arranged in order of the year of the author’s birth.Series were analysed if there were an adequate number of patients as indicated. There are also two translated French texts included
Author Title No. cases Included
Daniel Turner (1667–1741) The art of surgery[38] Only 4 cases No
Lorenz Heister (1683–1758) A general system of surgery in three parts [20] No cases No
Henri-François Le Dran (1685–1770) Observations in surgery [25] 14 analyzable cases Yes
François Quesnay (1694–1774) Observations on surgical diseases of the head and neck [34] 39 analyzable cases Yes
Samuel Sharp (ca. 1700–1779) A treatise on the operations of surgery [37] No cases No
William Bromfield (1712–1792) Sudorific opiates recommended in concussions of the brain [9]. Only 3 cases No
Percivall Pott (1714–1788) Observations on the nature and consequences of those injuries towhich the head is liable from external violence [32]
43 analyzable cases Yes
James Hill (1703–1776) Cases in surgery [21] 18 analyzable cases Yes
Sylvester O’Halloran (1728–1807) A New Treatise on the Different Disorders Arising from ExternalInjuries of the Head [30]
81 analyzable cases Yes
Pierre-Joseph Desault (1738–1795) The surgical works of PJ Desault by X Bichat [6] Only 6 cases No
Benjamin Bell (1749–1806) A system of surgery [4] No cases No
William Dease (1750–1798) Observations on wounds of the head [14] 24 analyzable cases Yes
James Latta (1754–1804) A practical system of surgery [24] Only 3 cases No
John Abernethy (1764–1831) Surgical observations on injuries of the head [3] 20 analyzable cases Yes
Acta Neurochir (2014) 156:615–623 617

Percivall Pott (1714 – 1788)Pott was very aware of the dangers of secondary
inflammation and putrefaction and described them andpondered their pathogenesis at length. The observedchanges included a swelling where there was pericranialseparation, discolored bone, and epidural and duralputrefaction associated with fever, headache listlessnessand drowsiness. Pott advocated prophylactic trepanationto avoid these problems, again arousing the ire of JohnBell [5]. However, while there were 29 out of 43 caseswith trepanation in his series or 67 % of all cases, yet, henever actually recorded that he himself undertook a pro-phylactic trepanation. Once again there is a mismatchbetween advice and practice.
Pott’s material is unique, being by far the most system-atically recorded series. Moreover, there were 29 infectedpatients, of whom only 15 died. This is a 34.9%mortalityrate due to infection, and infections accounted for 68.2 %of the deaths in the series. Of the lethal infections, six hadopen wounds and a further two were operated within 24 hof the trauma for a depressed fracture. In this series,however, there were far more closed injuries with infec-tion in this series than in any of the others as shown inTable 3. The numbers of infections with open and closedwounds were similar, as were the mortality rates. Pott’sseries also illuminates the importance of hospital admis-sion in relation to mortality. Table 4 shows the relation-ships between the initial care, hospital admission andinfection based mortality. It may be seen that hospitaladmission had no impact on the mortality from infections.Finally, in Table 5 it may be seen that half the infectedpatients who were trephined survived, whereas none ofthe infected patients who were not trephined survived. Soin Pott’s material, trepanation for infection would seem tocarry some benefit. Nine of the lethal infections wereassociated with an accident and five with assault.James Hill (1703 – 1776)
Hill pronounced no particular philosophy concerningindications for trepanation. He undertook the operation in
eight cases. In seven cases, this was for conditions asso-ciated with raised intracranial pressure. In the eighth heattempted to elevate a depressed fracture but it was tooimpacted. He was insistent that trepanation was not indi-cated for disturbances of the cranium but only for symp-toms indicating disturbances of the brain.
There is only one patient in Hill’s series that died froman infection. This was due to perforation of the skull closeto the orbit from a pair of scissors, where surgical treat-ment was refused. Infections are not mentioned in otherpatients so that the frequency is uncertain but therewere no other lethal infections. The overall mortalityrate was the lowest of any series, being 16.7 %, withone third of deaths due to an untreated infected case.Three of the patients may have been injured by violence,but they all survivedWilliam Dease (1752–1798)
Dease was critical of routine trepanation for fissures.He performed seven trepanations within 5 days of theinjury one for EDH, one for epilepsy and a dural tear and5 for depressed fractures. Two of the patients operated fordepressed fractures died of subsequent infection. Hetrephined a further 11 cases for established inflammationand putrefaction a week or more after the injury. They alldied. They had all suffered open injuries. Of these 11patients, 10 had suffered no fracture. Thus, he performedtrepanation on 20 of his 24 patients or 83.3 %, a higherproportion than any of the other series. However, thisdoes not represent a mismatch between advice andpractice. Dease mentions that trepanation was unpleasantand not without risk. Moreover, his advice to avoidtrephination in infected cases arose from the experiencehe describes and thus his teaching is in keeping with hisevolving experience.
In contrast to previous surgeons, especially Pott, hewas adamant that trepanation was of little use in caseswhere the dura was inflamed or putrefying unless theprocess was limited to the dura, which in his materialoccurred in only one patient who survived. Of the fivepatients who were not trephined, in four there was noindication for surgery and they all survived. In the fifth
Table 4 Relationship between the locations of primary treatment onmortality. This table shows that hospital treatment had no effect onthe mortality of the patients. Moreover, it did not increase the risk oflethal infections
Patient Nos.
Primary treatment Died Death frominfection
Death fromother causes
Survived Totals
Hospital admission 13 7 6 12 25
Local treatment 8 6 2 8 16
Outpatient 1 1 0 1 2
Total 22 21 0 21 43
Table 5 Influence of trepanation on infection in Pott’s series. Half of thepatients trephined for infection survived. All of those with an infectionwho were not trephined died. This indicates that trepanation was ofbenefit for these patients in this situation
Results of surgery in patients who suffered infection
Indication for surgery Died Survived
Depressed fracture 2 1
Infection trephined 7 7
Infection not trephined 6 0
618 Acta Neurochir (2014) 156:615–623

there was an indication, but the operation was refused bythe family and the patient died from an infection withepidural and subdural pus. The overall mortality rate frominfection was the highest of any series, being 54.1 %, andinfection was the only cause of death. It would seem thatsurgical infection was not a major cause of infectionsince the 11 patients operated for an infection onlycame to the surgeon once the infection was established.In two cases death from infection followed an accident,and in the remaining 11 cases the deaths followed anassault. Remarkably, in nine patients there was no fracture,only damage to the integuments, yet the lethal infectionwas in all cases intracranial.Sylvester O’Halloran (1728–1807)
O’Halloran performed trepanation on 25, or 35 %, ofhis cases. Of these cases, 22 were for depressed fractures,one for delayed inflammation and putrefaction and twofor coma. These last two were against O’Halloran’s prin-ciples, since he believed there was no way to distinguishbetween concussion and extravasation. Because the latterwas uncommon, he disapproved of operating on patientswith regard to disorders of consciousness, which hebelieved followed damage to the surgically inaccessiblemedulla oblongata. In the two cases mentioned, in onehe was pressured by a local aristocratic family and inthe other the operation was undertaken against hisadvice. Thus, he too is consistent in his practice andadvice. Moreover, like Dease he represents a directionaway from the excessive use of the trepan. He regarded itas a painful procedure to be avoided if possible.
O’Halloran’s reporting is not as systematic as some ofthe other authors. Thus there is no reliable record ofwhich patients were infected and which were not. Inconsequence, he is excluded from Table 3. However,there is a record of who died from infection. Of the 21deaths in his series, eight were due to this cause and allfollowed open wounds. This gives an overall mortalityfrom infection of only 11.2 % and meant that infectioncontributed to 38.1 % or less than half of the deaths in theseries. Of the 8 patients who died from an infection, onlytwo had been operated, so that surgical infection was nota clear-cut contributor to the outcome.
Four of the eight patients who died from an infectionhad suffered an accident, and four had been the victims ofassault.John Abernethy (1764–1831)
Abernethy trephined five of his 20 patients, or 25%.Allwere operated within 24 h of the injury. Three were fordepressed fractures in unconscious patients. They all haddepressed fractures and EDH, and they all died. Theremaining twowere for depressed fractures alone, and theyboth died. Abernethy was of the opinion that trepanationwas overused. His practice and principles were consistent.
Seven of Abernethy’s cases were infected, and in fivecases the infection was fatal. Four of the lethal cases werefrom open injuries and one from a closed injury withimmediate wound toilet. There were no trepanations fordelayed infection. Infection accounted for 62.5 % of thedeaths in this series. All the deaths due to infection werethe results of accidents, not violence
Variations in practice and their significance
In the series of Le Dran, Quesnay and Abernethy the majorityof lethal infections occurred after an open injury. In the rest, awound toilet or skin incision with skull inspection was carriedout within 24 h of injury. Thus in these series the infectionscould have been either a result of contamination at the time ofinjury or a genuine surgical infection. These findings thussupport the notion that surgery was dangerous, especially asthe death from infections in these three series accounted forover 60 % of all deaths.
The series of Pott and Dease also had a similar or higherincidence of death from infection. However, the results inthese two series show that this is not the whole picture. Theyare the only two series in which trepanation was performed astherapy for an established post-traumatic infection. Thenagain, in Pott’s series eight of the deaths occurred in closedinjuries. In addition Pott’s series illuminates the role of hospi-tal admission in lethal infections. It would be expected that ifhospital admission contributed to mortality this would showup when the mortalities of patients treated in hospital andoutside hospital are compared. Table 4 clearly indicates thathospital admission played little part in the mortality rate.Further evidence that hospital admission was not a majorproblem in all situations is the series of Dease. There were13 lethal infections. Two followed surgery for a depressedfracture. However, the remaining 11 only arrived for treatmentafter an infection had developed. Thus, surgery and a hospitaladmission cannot have played a part in the development ofthese dangerous infections.
Table 6 shows that Pott and Dease trephined the greatestproportion of patients. Many of these trepanations were doneas indicated above for infections. In Pott’s series the trepana-tion appeared to have been helpful since all the infectedpatients who were not trephined died while half of thosewho had their skulls opened survived. On the other hand,Dease found that patients only survived after trepanation inthis context if the disease was limited to the dura. In hisexperience, in contrast with that of Pott, this limited infectiononly occurred in two patients who survived. The remaining11 died with suppuration extending beyond the dura. Thereis no reason given for this but it is tempting to wonder ifdiet and immunity in Dublin in the 18th century was not asgood as that in London.
Acta Neurochir (2014) 156:615–623 619

It is interesting that Pott advocated trepanation with enthu-siasm, even going so far as to support prophylactic proceduresalthough he never performed one. He considered that the
operation was a lesser evil when compared with the courseof the untreated disease. Dease on the other hand consideredthe trephine was used too often and considered trepanation farfrom a benign procedure. Nonetheless, while their statedviews differed their practice was almost identical. Table 6 alsoshows that frequency of trepanation did not have a clear cutrelationship with deaths from infection.
The type of injuries varied from series to series but thereseems little evidence to suggest injuries from accidents weremore or less likely to end with a lethal infection than thoseacquired following an assault.
Thus, it would seem that frequency of trepanation, hospitaladmission and the reason for the injury had no clear cutrelationship with the incidence of infection in these studies.Yet there are two series which have a clearly lower rate ofinfection and deaths from infection than the other five. Thisraises the question as to why this should be the case and it isnot a question which can be answered with any degree of
Table 6 Frequency of trepanation in the seven series; four seriestrephined between 35 % and 45 % of patients. Two trephined over65 %, and one only 25 %. There is no clear cut relationship betweenfrequency of trepanation and incidence of lethal infections
Surgeon Numberpatients
Numbertrephined
Percentagetrephined
Deaths frominfection
Le Dran 14 5 35.7 62.5 %
Quesnay 37 13 35.1 72.7 %
Pott 43 29 67.4 68.2 %
Hill 18 8 44.4 33.3 %
Dease 24 19 79.2 100 %
O’Halloren 71 25 35.2 38.1 %
Abernethy 20 5 25.0 62.5 %
Fig. 1 Charts comparingmortalitypatterns in 1750 and 2011. Theupper chart is obtained from theBills of Mortality for London 1750[1]. The lower chart is derived fromthe UK government statistics forthe year 2011 [40]. The figureemphasizes how much mortalitydistributions according to age havechanged since the 18th century.It also indicates how lifeexpectancy figures are skewedbecause of the very high infantmortality and this must be takeninto account when consideringthe published low life expectancyfigures for the population asa whole
620 Acta Neurochir (2014) 156:615–623

certainty. However, there is what could be seen as circum-stantial evidence that has relevance.
Variations in results and their reasons
Many factors can have affected infection rates in differentcenters. It is not possible to assess 18th century practice withregard to infection with any degree of certainty. There is noknowledge of the hygiene of the surgeon, his team and hisplace of work. It is assumed that surgeons operated with barehands. There was authority for tidy fingernails and cleanlinessin respect of bandages fromHippocrates [22]. The first modernreference to surgical cleanliness comes in a book by Heinrichvon Pfolspeundt (dates unknown). He was a teutonic knightwho devised a rhinoplasty and also advised cleanliness in hisbook ‘Buch der Bundth-Ertznei’ published in 1460. He isdescribed as uneducated having no Latin and being onlymeagerly competent in his own tongue. He wrote of thedoctor “And especially, he should guard himself, if he haseaten onions or peas, or slept the previous night with anunclean woman, in the morning, against breathing intoanyone’s wound. Also, he should bind with clean whitecloths or harm results. He should also wash his handsbefore he treats anyone.” [42] This handbook was notprinted until the 19th century, so its message was notgenerally available in the 18th century. Moreover, theexperience of Semmelweis [33] in the next century whenhe tried to introduce routine hand hygiene suggests thatthere are no grounds for assuming routine surgical cleanli-ness in the period covered in this paper. There is also noinformation on how and where instruments were stored, noron how they were cleaned after an operation. The sameuncertainty extends to wound toilet and bandaging. There isno reason to believe that all surgeons followed similarroutines in respect of hygiene. Thus, local variation inpractice may well contribute to variations in the incidenceof surgical infection.
The mortality in these seven series has to be seen againstthe background of the contemporary mortality. Average lifeexpectancy in England between 1541 and 1871was 35.5 years(range 27.8 – 41.7 years [35]. In France the life expectancy ofmen between 1740 and 1790 was 24–28 years [35]. However,these bald figures need further interpretation. In the first place,the pattern of death in 1750 in London and 2011 in Englandand Wales illustrated in Fig. 1 shows that the distribution ofdeaths is very different. The cause of death in 1750 is some-what less precise than the number of deaths because the deathswere registered often by medically unqualified people andmany modern diagnoses did not exist. However, it is fair tosay that infections of various sorts were the main causes ofdeath. In the second place there must have been a sharp divideaccording to standard of living. Table 7 shows the ages at death
of 17 well to do 18th century citizens, including surgeonsreviewed in this paper and it is clear that their life expectancywas not so much lower than that of the average citizen in thetwenty-first century. It is thus worth mentioning that the over-whelming majority of the patients in 7 of the texts were notmembers of the genteel classes and thus likely to have beenamongst those with a lower life expectancy.
The malign effect of 18th century urbanization is wellknown [35]. Le Dran, Dease and Pott worked in big cities.London, with a population of around 750,000 [15] for exam-ple was appallingly dirty and unhygienic in the 18th century[12]. The nature and extent of this problem is presented asan appendix in a book by Alfred Russell Wallace (1823 –1913), famous for his pioneer studies into evolution. Writtenat the end of the 19th century, this appendix gives a lucidaccount of the changes in hygiene management which haddramatically improved the health of the poor in Londonfrom the end of the 18th century to the time of writing[41]. Wallace quotes extensively from 18th century sources.Poor building construction, poor waste disposal, absence ofsanitary facilities within the homes, and poor diet are amongthe most important of the long list of factors contributing toa high mortality which could be associated with the poorconditions [12]. One of his sources was Samuel Gale (1682–1754), a founder of the Society of Antiquaries who wrote in
Table 7 Births and deaths of some notable 18th-century people. Thistable illustrates the fact that while the mean life expectancy was between35 and 45 years, the well to do lived nearly as long as we do today. Thisunderlines howmany poorer people must die to keep the average down aslow as it was
Name Famous for Born Died Age atDeath
Sir Christopher Wren Architect andDraughtsman
1632 1723 91
Sir Samuel Pepys Diarist 1633 1703 70
Sir Robert Walpole Prime Minister 1676 1745 69
John Blachford Lord Mayor ofLondon
1682 1759 77
King George II King 1683 1760 77
George Frederick Handel Composer 1685 1759 74
William Hogarth Artist 1697 1764 67
James Hill Surgeon 1703 1776 73
William Pitt the Elder Prime Minister 1708 1778 70
Percival Pott Surgeon 1714 1788 74
Sir Joshua Reynolds Artist 1723 1792 69
Thomas Gainsborough Artist 1727 1788 61
Sylvester O’Halloran Surgeon 1728 1807 79
King George III King 1738 1820 82
William Dease Surgeon 1752 1798 46a
John Abernethy Surgeon 1764 1831 67
aDied from an injury or ruptured aneurysm
Acta Neurochir (2014) 156:615–623 621

1736 “In the churchyard of St. Paul’s Covent Garden, theburials are so frequent that the place is not capaciousenough to contain decently the crowds of dead, some ofwhom are not laid above a foot under the loose earth .”Another source was George Cheyne (1671–1743) a physi-cian originally from Aberdeen in Scotland who was a portlygourmand, later turned vegetarian. He had established apractice in London and was considered an expert on diet.The following quotation is from a piece written in 1724where it states that “There is no chronical distemper moreuniversal, more obstinate and more fatal in Britain thanscurvy”. A recent paper on scurvy states “Untreated, scurvyis inevitably fatal as a result of infection or sudden death”[31]. Thus, with scurvy together with abysmal hygiene deathfrom infections were to have been expected as illustrated in thecontemporary bills of mortality where infections accounted formore than half the deaths [2] compared with 1.5 % in 2011[39]. Nothing can more vividly convey the state of London’scitizens than William Blake’s poem ‘London’ the first verse ofwhich runs as follows.
I wander thro’ each charter’d street,Near where the charter’d Thames does flow.And mark in every face I meetMarks of weakness, marks of woe. [7]
One other thread of evidence is found in a single paper from1964 which in an in vivo study on birds indicates that Staphy-lococcus aureus survives much better in bruised than in healthytissue. This finding provides a mechanism whereby contusedtissue could be easily invaded from a filthy milieu and therebyexplains how contusion of the cranium and its integumentscould provide a ready source of bacteria, which in turn couldinfect the tissues of an immunologically weakened individual[19]. Could this be an explanation for the infections in Dease’scases of superficial injury complicated by subdural pus?
The lack of sanitation was as bad or worse in other largercities. Dublin had a population of around 150,000 [26] andwas,like London, seriously unhygienic [28]. Paris with its popula-tion between 600,000 and 700,000 [36] was also famouslyfilthy at this time [35].
On the other hand, the milieu was different outside the bigcities in areas like Limerick and Dumfries. O’Halloran sug-gested the reason for good results after cranial fracture inrespect of the milieu in which he lived. He states “Whether itproceeds from the natural intrepidity and robustness of ourpeople whose minds are not easily depressed, the purity ofthe air, or the goodness of our waters, which undoubtedlyapproach nearer to the pure element than any others I knowof, or let it arise from any other cause whatever;—the fact isthat fractured skulls amongst us, when attended to in anyreasonable time, are seldom or ever followed by fatal con-sequences; and that even when long neglected, the resourcesof nature are astonishing!” Limerick at that time was a small
city, with a population of 11,000 [27]. There is evidence forsimilar cleanliness at Hill’s area of practice in and aroundDumfries in Scotland, with a population of 4,517 souls in1755 [10]. The clean air and rising population is recordedfor three places where Hill is known to have lived namelyDumfries [10], Urr [29] and Kirkpatrick Durham [23].
Conclusions
The findings of this paper confirm that in many places infec-tions were the commonest cause of mortality in relation totrepanation. However, it is less clear that the infections werealways the result of the operation. It may also be suggestedthat in the 18th century, a hospital admission was not such amajor factor in the development of lethal surgical infections ashas been thought. On the other hand, the stews of the big citiesseem to have provided a ready milieu for secondary infectionsof injuries, closed or open. Thus the variability of resultsmentioned in the introduction could well be explained eitherby unrecorded variations in hygiene technique but also by thecleanliness in the milieu in which an injured patient lived.
Conflicts of interest None.
References
1. (1759) A collection of the yearly bills of mortality from 1657–1758inclusive. A Millar, London, p 144
2. (1759) A Collection of the yearly bills of mortality from 1657–1758inclusive. A Millar, London, pp 131 – 135
3. Abernethy J (1811) Surgical observations on injuries of the head.Thomas Dobson, Philadelphia
4. Bell B (1785) A system of surgery. Charles Elliot, Edinburgh5. Bell J (1826) On fractures of the skull with depression in the principles
of surgery. Thomas Tegg, London, pp 268–3286. Bichat X (1814) The surgical works or statement of the doctrine and
practice of P.J. Desault— in two volumes (trans: Smith ED. ThomasDobson). Philadelphia
7. BlakeW (1972) London inWilliam Blake complete writings. OxfordUniversity Press, Oxford, p 216
8. Botero JSH, Pérez MCF. (2012) The history of sepsis from ancientEgypt to the XIX Century. doi:10.5772/51484 accessed 2nd April2013
9. Bromfield B (1773) Sudorific opiates, recommended in concussionsof the brain in chirurgical observations and cases Vol 1. T Cadell,London, pp 9–23
10. Burnside W (1799) Dumfries. In: Sinclair J (ed) Statistical accountsof Scotland of 1791–1799. William Creech, Edinburgh, p 131
11. Celsus C (1938) De Medicina (trans: Spencer WG) Books I-IV.Harvard University Press, Cambridge, p 273
12. Cockayne E (2007) Hubbub, Filth, Noise & Stench in England. YaleUniversity Press, New Haven
13. Dagi TF (1997) The management of head trauma. In: Greenblatt SH(ed) A history of neurosurgery. American Association of NeurologicalSurgeons, Park Ridge Illinois, pp 301–302
622 Acta Neurochir (2014) 156:615–623

14. Dease W (1776) Observations on wounds of the head. G Robinson,London
15. Emsley C, Hitchcock T, Shoemaker R (2013) London history — apopulation history of London, Old Bailey Proceedings Online. http://www.oldbaileyonline.org, version 7.0. Accessed 16th March 2013
16. Ganz JC (2013) The lucid interval associated with epidural bleeding:evolving understanding. J Neurosurg 118(4):739–845
17. Gross C (2009) A hole in the head: more tales in the history ofneuroscience. The MIT Press, Cambridge Massachussetts, 23
18. Gross C (2003) Trepanation from the Paelaeolithic to the Internet.In: Arnott R, Finger S, Smith CUM (eds) Trepanation history,discovery, theory. Swets & Zeitlinger Lisse, Abingdon Exton,Tokyo, p 311
19. Hamdy MK, Barton ND (1965) Fate of staphylococcus aureus inbruised tissue. Appl Microbiol 1:15–21
20. Heister L (1750) A general system of surgery in three parts. W Innys,London
21. Hill J (1772) Cases in surgery. John Balfour, Edinburgh22. Hippocrates (1928) In the surgery IV in Hippocrates Volume III,
Loeb Classical Library, (trans: Withington ET). Harvard UniversityPress, Cambridge, pp 63 – 65
23. Lamont D (1799) Kirkpatrick-Durham, County of Kirkcudbright. In:Sinclair J (ed) Statistical accounts of Scotland of 1791–1799.WilliamCreech, Edinburgh, p 253
24. Latta J (1795) Of wounds and contusions of the head in a practicalsystem of surgery. G Mudie and Son, Edinburgh, pp 111–180
25. Le DranH-F (1740) Observations in surgery: containing one hundredand fifteen different cases with particular remarks on each for theimprovement of young students (trans: by Surgeon JS). JamesHodges at the Looking Glass, London Bridge
26. Lennon C (2008) Dublin part II 1610–1756. Royal Irish Academy,Dublin
27. Lovett P (1981) The Wellesley Bridge. The Old Limerick Journal;Winter (9), 28–31
28. Mapother ED (1864) The sanitary state of Dublin. J Stat Soc Inq SocIreland 4:62–76
29. Muirhead J (1799) Parish of Urr, county of Kirkcudbright — synodand presbytery of Dumfries. In: Sinclair (ed) Statistical accounts ofScotland of 1791–1799. William Creech, Edinburgh, p 76
30. O’Halloran (1793) A New treatise on the different disorders arisingfrom external injuries of the head. Zachariah Jackson, Dublin
31. Pimentel L (2004) Scurvy: historical review and current diagnosticapproach. Am J Emerg Med 21(4):328–332
32. Pott P (1768) Observations on the nature and consequences of thoseinjuries to which the head is liable from external violence. Hawes L,Clarke W and Collins, London
33. PutnamC (2007) Semmelweis Ignác Fülöp [Ignaz Philipp]. In: BynumWF, Bynum H (eds) Dictionary of medical biography Volume 5.Greenwood Press, London, pp 1133–1135
34. Quesnay F (1848) Summary of observations on the use of the trepan.In: Ottley D (ed) Observations on surgical diseases of the head andneck selected form the memoirs of the royal academy of surgery ofFrance. The Sydenham Society, London, pp 1–80
35. Riley JC (2001) Rising life expectancy: a global history. CambridgeUniversity Press, Cambridge, pp 32–34
36. Roche D (1987) The people of Paris: an essay in popular culture inthe 18th century. University of California Press, Berkeley, p21
37. Sharp S (1740) A treatise on the operations of surgery with a descrip-tion and representation of the instruments used in performing it. JBrotherton, W Innys and R Manby, London
38. Turner D (1736) The art of surgery. C Rivington, London39. UKNational Statistics, Publication Hub (2013) http://www.ons.gov.uk/
ons/publications/re-reference-tables.html?edition=tcm%3A77-276695,Accessed 15th March 2013
40. UKNational Statistics, Publication Hub. (2013) http://www.statistics.gov.uk/hub/population/deaths/mortality-rates [Accessed 15th March2013]
41. Wallace AR (1898) The wonderful century it’s successes and it’sfailures. George N. Morang, Toronto, pp 318–319
42. Zimmerman LM, Veith I (1967) Great ideas in the history of surgery.Chapter 22: GermanWound Surgeons, Dover Publications Inc., NewYork, pp 293–217
Acta Neurochir (2014) 156:615–623 623





























