Embed Size (px)
Citation preview

Treatment of the InfectedStone
Tracy Marien, MD, Nicole L. Miller, MD*KEYWORDS
� Struvite � Calcium carbonate apatite � Staghorn � Obstructive pyelonephritis � Kidney stones� Urinary tract infection
KEY POINTS
� Infection stones result from urease-producing bacteria and are struvite and/or calcium carbonateapatite in composition.
� Optimal management of infection stones is complete stone removal, and failure to achieve com-plete stone clearance results in a high recurrence rate.
� Obstructive pyelonephritis is a urologic emergency and can result in urosepsis and death.
� Emergent decompression with retrograde ureteral stent placement or percutaneous nephrostomytube (PCNT) placement and broad-spectrum antibiotics are imperative to treating patients withobstructive pyelonephritis.
INTRODUCTION
An infected kidney stone can refer to stones thatform because of urinary tract infections (UTIs)with urease-producing bacteria, secondarilyinfected stones of any composition, or stones ob-structing the urinary tract leading to pyelonephri-tis. Most commonly, kidney stones that formsecondary to urease-producing bacteria arecomposed of struvite or calcium carbonateapatite, and presentation is frequently incidentaland generally nonemergent. Secondarily infectedmetabolic stones have also been described. Thesestones are frequently colonized with non–urease-producing bacteria and often have discordant cul-ture results compared with the lower urinary tract.Obstructive pyelonephritis secondary to urinarytract calculi is considered a urologic emergency,and immediate treatment is indicated to avoidserious complications, including urosepsis anddeath. Given the difference in pathophysiologyand treatment approach, these entities are dis-cussed separately.
Department of Urologic Surgery, Administrative Office,Medical Center, Nashville, TN 37232-2765, USA* Corresponding author. Department of Urologic SurgNorth, Vanderbilt University Medical Center, Nashville, TE-mail address: [email protected]
Urol Clin N Am - (2015) -–-http://dx.doi.org/10.1016/j.ucl.2015.05.0090094-0143/15/$ – see front matter � 2015 Elsevier Inc. All
Infection Stones
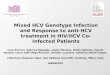
Infection stones are most commonly composed ofmagnesium ammonium phosphate (ie, struvite)and/or calcium carbonate apatite. These stonesresult from chronic infections with urease-producing bacterial pathogens and frequentlyform large branched stones known as staghorncalculi. The incidence of infection stones has over-all decreased during the last 30 years, likely due toimproved medical care. They are more common inwomen (10%–11% vs 4% in men) and elderly pa-tients.1,2 The pathogenesis of struvite and calciumcarbonate apatite stone formation is presented inFig. 1.3,4 Urease from bacteria splits urea intoammonia and carbon dioxide. Ammonia reactswith water to become ammonium and hydroxideions, which creates an alkaline milieu. In this alka-line environment, the ammonium combines withmagnesium, phosphate, and water to create mag-nesium ammonium phosphate stones. The carbondioxide eventually breaks down to carbonate,which combines with calcium and phosphate to
A-1302 Medical Center North, Vanderbilt University
ery, Administrative Office, A-1302 Medical CenterN 37232-2765.
rights reserved. urologic.th
eclinics.com

Urease spli�ng bacteria
UreaseCO(NH2)2 + H2O � 2NH3 + CO2
Urea
2NH3 + 2H2O � 2NH4+ + 2OH- CO2 + H2O � H+ + HCO3
-
Damage to glycosaminoglycanlayer covering the urothelial cells
Alkaliniza�on(pH > 7.2) H+ + HCO3
- � 2H+ + CO32-
Bacteria a�ach to urothelium and
6H2O + Mg2+ + PO43- + NH4
+ � (MgNH4PO4 · 6H2O) form a biofilm CO32- + 10Ca2+ + 6PO4
3- � Ca10(PO4)6CO3Struvite Calcium carbonate
apa�te
Fig. 1. Pathogenesis of infection stones. Urease from bacteria splits urea (ie, carbamide) into ammonia and car-bon dioxide. The ammonia combines with water to produce ammonium and hydroxide. Hydroxide results in analkalosis of the urine leading to the formation of magnesium ammonium phosphate (ie, struvite). The ammoniaalso damages the glycosaminoglycan layer causing urothelial damage, allowing the bacteria to attach to the ur-othelium and form a biofilm. Carbon dioxide complexes with water to form bicarbonate and then carbonate.Carbonate combines with calcium and phosphate forming calcium carbonate apatite.
Marien & Miller2
form calcium carbonate apatite stones. The mostcommon urease-producing bacterial pathogensare Proteus spp, Klebsiella spp, Providenciaspp, Morganella morganni, and Staphylococcusaureus.5,6 Infection stones are commonly asymp-tomatic or present with UTIs, flank or abdominalpain, fevers, gross hematuria, or less commonlywith sepsis or renal insufficiency.7 Patients withindwelling catheters, neurogenic bladder, and uri-nary diversion have the highest risk of developinginfection stones due to chronic bacterial coloniza-tion. The natural history of these stones is associ-ated with progressive morbidity and mortality,with the 10-year mortality rate reported at 28%with nonsurgical management versus 7%with sur-gical treatment.8
Secondarily infected stones, which are nonstru-vite and non–calcium carbonate apatite stonesassociated with infection, have been described.9
In a series of 125 patients undergoingpercutaneousnephrolithotomy (PCNL), de Cogain and col-leagues9 found that 24 (23%) of 106 patients withnonstruvite stones had positive stone cultures. Ahistory of neurogenic bladder was associated withpositive stone culture in both patients with infectednonstruvite and struvite stones in this series. Non–urease-producing bacteria, including Escherichiacoli and Enterococcus spp, are the predominant
organisms colonizing these metabolic stones.9,10
Whether these stones form and become second-arily infected or whether these stones result from anidus of infection that propagates stone formationis unclear. Theories for how bacteria could be anidus for nonstruvite and non–calcium carbonateapatite stones include kidney cell injury and inflam-mation potentiating crystal retention, alteration ofthe microenvironment by bacterial metabolic activ-ity, or biofilm that acts as amatrix for stone growth.9
In general, sending a sample for stone cultureshould be considered for all patients undergoingPCNL to help target antibiotic therapy in the eventof a postoperative infection. Patients should makeappropriate dietary modifications and receive spe-cific medical therapy based on metabolic studiesto prevent recurrent urolithiasis. Further studiesare necessary to elucidate the exact role andclinicalsignificance of bacteria in these stones.
Obstructive Pyelonephritis
Pyelonephritis is an infection of the kidney withtypical presentation including but not limited to fe-ver, flank pain, and irritative lower urinary tractsymptoms. Obstructive pyelonephritis is a compli-cated UTI and considered a urologic emergencybecause of the significant risk of morbidity and

Treatment of the Infected Stone 3
mortality.11–13 Borofsky and colleagues12 identi-fied 1712 patients from the Nationwide InpatientSample between 2007 and 2009 who had ureteralcalculi and sepsis and found a 19% rate of mortal-ity if decompression was not performed versus9% for those who underwent surgical decompres-sion. Ureteral stones are responsible for approxi-mately two-thirds of the occurrences ofobstructive pyelonephritis.14
PATIENT EVALUATION OVERVIEWInfection Stones
Patients with infection stones typically do not pre-sentwith acute colic and instead are found inciden-tally or due to complaints of vague abdominal or
Box 1Initial evaluation of patients with suspicion for infec
History
� Symptoms
� Flank pain, abdominal pain, fevers, chills, gross h
� LUTS: dysuria, hematuria, urgency, frequency
� Urologic history
� UTI, pyelonephritis
� Urolithiasis
� Urinary diversion and/or neurogenic bladder
� Anatomic abnormalities (UPJO, strictures)
� Chronic indwelling catheters, SPT or CIC
� Urethral strictures
� Prior urologic surgeries
� Anticoagulation or antiplatelet therapy (and if the
Physical examination
� Fever/hypothermia, vital signs
� CVAT, abdominal/suprapubic tenderness
� Musculoskeletal deformities
Laboratory tests
� UA and urine culture
� BMP, CBC, coagulation panel
� � Blood cultures (if presenting acutely with fever/c
Radiology
� Noncontrast CT scan (gold standard)
� KUB and/or renal US (best used for follow-up)
� � Renogram
Abbreviations: BMP, basic metabolic panel; CBC, complete bcomputed tomography; CVAT, costovertebral angle tenderneurinary tract symptoms; SPT, suprapubic tube; UA, urinalyssonography; UTI, urinary tract infection.
backpain, recurrentUTIs, and/or grosshematuria.7
Box 1 provides a summary of the initial evaluationof these patients. A focused history and physicalexamination should be performed.
A urinalysis (UA) may show an alkaline pH (>7.0)and evidence of an infection, including leukocyteesterase, white blood cells (WBCs), nitrite, andblood. Magnesium ammonium phosphate crystals(which are coffin shaped) may also be noted on theUA of a patient with infection stones. Urine cultureshould be done, and is likely to grow a urease-producing bacteria. A basic metabolic panel isused to assess kidney function, as infectious stag-horn calculi have a high risk of causing renal insuffi-ciency.8Hematocrit, platelet count, and coagulationpanel values are necessary for surgical planning.
tion stones
ematuria
se can be held)
oncern for sepsis)
lood count; CIC, clean intermittent catheterization; CT,ss; KUB, kidney ureter bladder radiography; LUTS, loweris; UPJO, ureteropelvic junction obstruction; US, ultra-

Marien & Miller4
Imaging with noncontrast computerized tomog-raphy (CT) is the gold standard for both diagnosisand surgical planning. Kidney, ureter, and bladderradiography and/or renal ultrasonography (US)may be used for follow-up. A renogram shouldbe performed if poor function is suspected in theaffected kidney.
Obstructive Pyelonephritis
Initial evaluation of patients presenting withobstructive pyelonephritis most frequently beginsin the emergency room (ER). Box 2 provides asummary of the initial evaluation of these patients.A focused history and physical examination shouldbe performed, with careful attention paid to vitalsigns and hemodynamic stability. Findings of
Box 2Initial evaluation of patients with obstructive pyelon
History
� Symptoms
� Flank pain, abdominal pain, nausea, vomiting, fe
� LUTS: dysuria, hematuria, urgency, frequency
� Urologic history
� UTI, pyelonephritis
� Urolithiasis
� Anatomic abnormalities (UPJO, strictures)
� Urologic surgeries
� Past history of malignancy, irradiation, abdominal
� Risk factors for infection (DM, HIV/AIDS, performastates)
� Anticoagulation or antiplatelet therapy
Physical examination
� Fever/hypothermia, hemodynamic stability
� CVAT, abdominal pain/suprapubic pain
Laboratory tests
� UA, CBC, BMP, � albumin, � CRP
� Voided urine culture and blood culture at presenta
� Urine culture from the kidney(s) at the time of dec
Radiology
� Noncontrast CT abdomen and pelvis
� Ultrasonography (can consider as first line if pastone) � KUB
Abbreviations: AIDS, acquired immune deficiency syndrome;CRP, c-reactive protein; CVAT, costovertebral angle tendernevirus; KUB, kidney ureter bladder radiography; LUTS, loweobstruction.
poor performance status and a history of paralysisin patients with obstructive pyelonephritis shouldalert the medical practitioner to an increased riskfor sepsis.13 The use of anticoagulation or anti-platelet therapy must be assessed. For patientswith paralysis and contractures, physical examina-tion should also assess mobility of the patient’slower body and the ability to place them in lithot-omy position for cystoscopy. Patients with severelower extremity contractures that prohibitcystoscopic access may require PCNTs fordecompression.UA may show signs of infection, with positivity
for leukocyte esterase, WBCs, blood, and nitrite;however, a negative UA result does not rule outinfection. The urine proximal to an obstructingstone may be infected, whereas the voided urine
ephritis
vers, chills
surgeries (risks for ureteral obstruction)
nce status, paralysis, other immunocompromised
tion
ompression
tient is stable and there is low suspicion for
BMP, basic metabolic panel; CBC, complete blood count;ss; DM, diabetes mellitus; HIV, human immunodeficiencyr urinary tract symptoms; UPJO, ureteropelvic junction

Treatment of the Infected Stone 5
distal to this may be sterile. Glucosuria should alertthe clinician to poorly controlled or undiagnoseddiabetes mellitus. The practitioner should beaware that patients with thrombocytopenia13,15,16
and low serum albumin levels13,15 are at anincreased risk of developing septic shock andshould be monitored appropriately. Urine andblood cultures should be sent on presentation,and a urine culture from the kidney(s) should beobtained at the time of decompression. Althoughsome series have found C-reactive protein (CRP)levels helpful in distinguishing between infectedand sterile hydronephrosis17 as well as for identi-fying those patients who will develop urosepsis,13
the utility of CRP in the management of obstructivepyelonephritis is unclear.
Imaging is required to differentiate nonobstruc-tive from obstructive pyelonephritis. Although UScan detect hydronephrosis and has the advantageof avoiding ionizing radiation, it is user dependent,limited by body habitus, and frequently suboptimalin identifying the specific source of ureteralobstruction. Some advocate for bedside US inthe ER to screen for hydronephrosis before CTscan to avoid radiation and unnecessary costs.18
US performed in the ER has a reported sensitivityof 80% and specificity of 83%.19 A bedside US bythe ER physician may be reasonable as an initialevaluation for ureteral obstruction in a stable pa-tient. Ultimately, however, a CT scan should beobtained to confirm the diagnosis and clearly char-acterize the cause of obstruction, which affectsthe choice of decompression procedure as wellas guides future definitive surgical therapy.
PHARMACOLOGIC TREATMENT OPTIONSInfection Stones
Infection stones are optimally managed surgicallywith the goal of complete stone clearance. Aftersurgery, pharmacologic preventative measurescan be considered, including acidification of theurine, inhibition of urease, chemolysis via topicalapplication, and suppressive antibiotic therapy.Medical therapy alone can also be considered forthose unable to undergo surgery. Crystallizationof infection stones occurs at a pH greater than7.0 to 7.2. Acidification of the urine to less thanpH 6.5 can greatly increase the solubility of thistype of infection stone. Urinary acidification withascorbic acid, ammonium chloride, ammoniumsulfate, ammonium nitrite, and L-methionine hasbeen reported.6,20 L-Methionine is an oral medica-tion that is metabolized to sulfate and hydrogenions.21 In vitro studies using L-methionine haveshown excellent ability to dissolve infectionstones,22 and older in vivo series have shown
favorable urinary acidification.23 Contemporaryin vivo studies are needed to assess for safetyand efficacy. Urinary acidification is rarely imple-mented today.
Acetohydroxamic acid (AHA) is an oral agentthat acts as a urease inhibitor. AHA was initiallydescribed in the 1960s and is the only US Foodand Drug Administration (FDA)-approved ureaseinhibitor.24 Hydroxyurea was also investigated asan oral urease inhibitor but was found to be inferiorto AHA.25 AHAworks well because it achieves highlevels in the urine and can penetrate bacterial cellwalls. Randomized and placebo-controlledstudies have proved AHA’s ability to significantlyreduce stone growth; however, it does notdecrease existing stone burden.26–28 Griffith andcolleagues26 in a randomized, double-blind, pla-cebo-controlled trial of AHA in 210 patients withspinal cord injury reported a significant decreasein stone growth for those receiving AHA versusplacebo (33% and 60%, respectively). However,many patients experience psychoneurologic, he-matologic, and gastrointestinal side effects, with22% unable to tolerate AHA.27,29 The presenceof renal insufficiency increases the risk of toxicityand results in decreased efficacy. Thus, AHA iscontraindicated for patients with a creatinine levelgreater than 2.5 mg/dL2. It is also contraindicatedin pregnant women and women of childbearingage who are not using birth control. The AmericanUrological Association (AUA) guidelines state thatAHA may be offered only after surgical optionshave been exhausted for patients with residual orrecurrent struvite stones.30 They also encouragethe use of AHA in patients with abnormal lower uri-nary tracts (ie, neurogenic bladder or urinary diver-sion) and struvite and/or calcium carbonateapatite stones because of the high risk for recur-rent stone formation.31
Topical chemolysis and dissolution with Renaci-din irrigant (10% hemiacidrin) or Suby G solution(3.2% citric acid) into the collecting system hasalso been described.32–34 In the 1960s, 6 patientsdied after treatment with Renacidin, which led tothe ban of this irrigant by the FDA. Further investi-gation found that these deaths were related toadministration of the irrigant under high pressureresulting in pyelovenous back flow, systemic ab-sorption, urosepsis, and subsequent death.35
Dissolution therapy for infection stones via PCNTs,ureteral stents, and/or access sheaths is nowconsidered safe and effective as long as it is per-formed in the setting of sterile urine, with prophy-lactic antibiotics and at low renal pelvicpressures.34 Postoperative application is limitedfor multiple reasons including the need to knowthe stone composition before administration,

Marien & Miller6
difficulty maintaining a low-pressure system, needfor constant nursing care, need for replacement/exchange of ureteral stents and nephrostomytubes when they become obstructed, and needfor prolonged hospitalization. For those patientswith infection stones who are not cured with surgi-cal stone removal, dissolution therapy can beconsidered and is currently approved by the FDAfor use in this setting.In theory, the eradication of urease-producing
bacteria in the urinary tract with antibiotics shouldhalt the formation of infection stones, and older se-ries have even reported that infection stones maydissolve in sterile urine36,37; however, antibioticsdo not penetrate infection stones. Ultimately, sur-gical removal is required to achieve sterility. Thereare anecdotal reports of decreased recurrence ofinfection stones by placing patients on suppres-sive antibiotic therapy for several months after sur-gical stone removal, but there are no series in theliterature studying this approach. With increasingrates of antimicrobial resistance, evidence isneeded to justify the use of prolonged antimicro-bial therapy in this patient population. Anothersuggested approach is to check a urine cultureevery month for 3 months after surgical removalof infection stones and treat as needed.38 Furtherstudies are necessary to clearly state the role ofsuppressive antibiotics after surgical removal ofinfection stones.
Obstructive Pyelonephritis
Obstructive pyelonephritis requires dual therapywith broad-spectrum antibiotics and emergentdecompression. Selection of empiric antibiotic ther-apy can be complicated because of the increasingantimicrobial resistance both nationally and world-wide.39–42 Choice of empiric antibiotic therapy canbeguidedby reviewingprior urine culturedata, urineculturegram-staining result,43 thehospital’s antibio-gram, and antimicrobial stewardship’s recommen-dations.44 In general, the patient should beadministered broad-spectrum antibiotics to coverfor common gram-negative pathogens with orwithout antibiotics to cover gram-positive patho-gens. One series reported on their experience withobstructive pyelonephritis and found that 79% ofbacterial pathogens were gram-negative rods, withE coli being the most common (66%) and Entero-coccus spp making up two-thirds of the gram-positive pathogens.44 Of the 65 patients in thisseries, 2 had candida in their urine specimens.Coverage for gram-positive pathogens should beinitiated if the patient presents with sepsis, if gram-positive bacteria are noted on gram staining, and ifthe patient has a history of prior UTIs with
gram-positive pathogens. Once the organisms inthe urine and blood cultures are determined, thepatient should be switched to a 1- to 2-week courseof culture-specific antibiotics.45
NONPHARMACOLOGIC TREATMENTOPTIONSInfection Stones
Dietary modifications to prevent infection stoneshave generally focused on reducing urinary phos-phorous andmagnesium levels by avoiding dietaryfoods and vitamin supplements high in these ele-ments. Shorr and Carter46 proposed a regimen inthe 1940s of a low-phosphate, low-calcium dietwith oral estrogens (to decrease calcium excre-tion) and an aluminum hydroxide gel to bind phos-phate in the gut. Although studies found significantstone dissolution and reduced stone growth46 aswell as decreased stone recurrence followingPCNL47 on this regimen, the Shorr diet has beenshown to result in significant metabolic abnormal-ities related to the aluminum hydroxide, includingconstipation, anorexia, lethargy, bone pain, andhypercalciuria.48 The Shorr diet with aluminumhydroxide is not currently recommended.
Obstructive Pyelonephritis
There is no role for nonpharmacologic treatment ofobstructive pyelonephritis in the acute setting.Long-term efforts to decrease recurrent nephroli-thiasis and UTIs through dietary measures areindicated.
SURGICAL TREATMENT OPTIONSInfection Stones
Surgical management with the goal of completestone clearance is the standard of care for patientswith infection stones. Table 1 provides a summaryof surgical treatment options for infection stonesas recommended by AUA guidelines and reportedin the literature.For those well enough to undergo surgical inter-
vention, the current AUA guidelines recommendPCNL monotherapy as the treatment of choicefor staghorn calculi.31 PCNL in combination withflexible ureteroscopy results in less access tractsand decreased blood loss.59 PCNL and uretero-scopy may be performed simultaneously in theprone position with a split leg bed, avoiding timeneeded to reposition from dorsal lithotomy toprone.60,61 Combination therapy for the treatmentof infection stones refers to the use of PCNL withshockwave lithotripsy (SWL). Segura and col-leagues62 reported a disappointing stone freerate of 23% in their series of 16 consecutive

Table 1Surgical approaches for infection stones
Surgery Indication Evidence
PCNL (� URS, � flexiblenephroscopy)
First line per AUA guidelines Preminger et al,31 2005
PCNL 1 SWL When calyces cannot be accessedwith nephroscopy or additionalaccess tracts
Preminger et al,31 2005; Merhejet al,49 1998
SWL monotherapy(1stent or PCNT)
Stone burden <500 mm2 withno/minimal dilation of thecollecting system
Preminger et al,31 2005; Lam et al,50
1992
URS monotherapy May consider for partial staghornstones in patients unable toundergo PCNL
Healy & Ogan,51 2007
ANL (open or lap/RAL) PCNL failure, extremely large stones,aberrant collecting systemanatomy (ie, calyceal diverticulum,infundibular stenosis),unfavorable body habitus forPCNL (ie, morbid obesity, skeletaldeformities), pelvic or transplantkidneys
Preminger et al,31 2005; Bove et al,52
2012; Assimos,53 2001; King et al,54
2014; Ghani et al,55 2013;Giedelman et al,56 2012;Simforoosh et al,57 2008;Elbahnasy et al,58 2011
Abbreviations: ANL, anatrophic lithotripsy; lap, laparoscopic; RAL, robotic-assisted laparoscopic; SWL, shockwave litho-tripsy; URS, ureteroscopy.
Treatment of the Infected Stone 7
patients undergoing PCNL followed by SWL.Based on this study, the current AUA guidelinesstate that if SWL is to be performed with PCNL,PCNL should be the first modality used to treatthese patients as well as the last because clear-ance of all fragments after SWL is unlikely.31
SWL may be used in cases in which residualstones cannot be treated with flexible nephro-scopy or via another access tract. However, ingeneral, flexible nephroscopy and ureteroscopyobviates SWL for inaccessible calyces.31 Althougholder series have found SWL monotherapy withstent or PCNT acceptable treatment of smallerstone burden (<500 mm2) with no or minimal dila-tion of the renal collecting system, most urologistswho treat complex stone disease still performPCNL in this cohort.50 Open surgery with anatro-phic nephrolithotomy (ANL) is not appropriate formost patients with infection or staghorn stonesper the AUA guidelines, although it may be consid-ered for cases in which the stone is not expectedto be removed by a reasonable number of lessinvasive procedures. Although open stoneremoval results in stone free rates similar to thoseof PCNL, this approach is associated withincreased morbidity, convalescence period, hos-pital stay, narcotic requirement, and complica-tions.63 A minimally invasive alternative to openANL is laparoscopic and robotic ANL, whichhave recently been described.54–57
In preparation for surgery, a noncontrast CTscan is obtained to delineate the anatomy andguide the surgical approach. A renogram shouldbe obtained if there is concern for a poorly func-tioning renal unit, and nephrectomy considered ifpoor function is confirmed and the contralateralkidney is normal.
Patients with suspected infection stones are atincreased risk for infectious complications afterPCNL. Preplacement of PCNT allows for drainage,aspiration, and culture of stagnant and infectedurine. By administering a course of antibioticsbased on this pelvic urine culture, some haveshown a decreased rate of postoperative bacter-emia, systemic inflammatory response syndrome(SIRS), and sepsis,64,65 which is likely becausestone culture results correlates more closely withrenal pelvic than bladder culture results.66 In aretrospective review of 219 patients, Benson andcolleagues64 reported a 6% rate of SIRS/sepsisat the time of PCNL in those undergoing concur-rent PCNT placement versus none in those under-going preplaced PCNT.
If bladder urine culture results are positive, pa-tients undergoing stone treatment without pre-placed PCNT should be treated with a course ofpreoperative antibiotics with the goal of sterilizingthe urine. For those patients without positive re-sults on preoperative urine culture, current AUAguidelines recommend limiting perioperative

Marien & Miller8
antibiotics to less than 24 hours except for thosepatients with external urinary catheters presentbefore surgery, with risk factors (ie, advancedage, anatomic abnormalities of the urinary tract,poor nutritional status, tobacco use, chronic corti-costeroid use, immunodeficiency, or prolongedhospitalization), or with bacteriuria.67 However,several series have shown significant reduction inpostoperative sepsis by administering all patientsundergoing PCNL a prophylactic course of antibi-otics.68,69 Mariappan and colleagues69 found that52 patients who had dilated collecting systems,stone burden greater than 2 cm, and no confound-ing factors predisposing to UTIs who received a1-week course of ciprofloxacin before PCNL hada 3-fold lower risk of postoperative UTI and SIRSthan 46 patients who received standard perioper-ative antibiotics on the day of surgery. Bag andcolleagues68 prospectively randomized 101 pa-tients with greater than 2.5-cm kidney stonesand/or hydronephrosis with sterile preoperativeurine cultures to a 7-day course of nitrofurantoinversus no antibiotics before PCNL and found astatistically significant lower rate of postoperativeSIRS (19% vs 49%), endotoxemia (18% vs 42%),positive result on kidney urine culture (0% vs10%), and positive result on stone culture (8% vs30%) in the arm receiving nitrofurantoin. Althoughthese 2 small series support a week of preopera-tive antibiotics before PCNL, larger, prospective,randomized studies are underway to better eluci-date the risks and benefits of empiric antibioticsused in this setting.Given the known discordance between results
of bladder urine culture and stone culture, strongconsideration should be given to sending a samplefor stone culture to help target antibiotic therapy ifthe patient develops a postoperative infection.Multiple series have examined the relationship be-tween results of preoperative urine culture fromthe bladder and kidney stone culture and foundpoor correlation between the two.70,71 One series
Table 2Mode of decompression considerations for obstructi
Favoring Ureteral Stent F
� Interventional radiologist unavailable� Failed PCNT attempt� Uncorrected coagulopathy� Minimal hydronephrosis� Unfavorable anatomy for percutaneous access
���
�
���
by Eswara and colleagues70 reported on 328consecutive patients who underwent stone sur-gery and found for those 11 patients who devel-oped sepsis, readmission urine culture resultcorrelated with stone culture result in 64% ofcases and with preoperative urine culture resultin only 9% of cases (P 5 .02). A stone culture atthe time of surgery may be helpful to guide antibi-otic therapy in the setting of postoperative UTIand/or urosepsis.
Obstructive Pyelonephritis
Although older series may support withholdingemergency decompression in patients with feverand obstructing urolithiasis,72 it is clear thatdecompression with retrograde ureteral stentplacement or PCNT is imperative to decreasemorbidity and mortality.12 Some have theorizedthat ureteral stent placement is inferior to PCNTbecause of the risk of exacerbating infection viastone manipulation and by providing suboptimaldrainage compared with a larger-caliber nephros-tomy tube. Pearle and colleagues73 randomized42 consecutive patients with obstructing ureteralstones and clinical evidence of infection todrainage with PCNT or retrograde ureteral stentplacement and found that neither modality wassuperior in promoting rapid recovery afterdrainage, although ureteral stent placement wasfound to be more than twice as costly as PCNT($1137 vs $2401). The only benefit of PCNT versusureteral stent placement in this setting was foundas a secondary end point from a series out ofSyria, which reported that patients who underwentdecompression with PCNT required shorter antibi-otic courses than those managed with stents.74
Although ureteral stent placement and PCNThave both been shown to be effective methodsof decompression, in some circumstances onemethod is indicated over the other (Table 2). Thepresence of hemodynamic instability may limit
ve pyelonephritis
avoring PCNT
Urologist unavailableFailed ureteral stent attemptDifficult retrograde access (ie, urinary diversion,renal transplant)Inability to access the bladder (ie, urethralstricture, lower extremity contractures)Steinstrasse and/or large stone burdenConcern for impacted ureteral stoneInability to tolerate general anesthesia

Treatment of the Infected Stone 9
the use of general anesthesia. Although most urol-ogists place ureteral stents under general anes-thesia, several series have shown that retrogradeureteral stent placement under local anesthesiais safe and effective, with less than 10% rate offailure.75–77 A retrospective review of 119 primaryureteral stent placements reported by Sivalingamand colleagues75 compared 46 cases undergoingstent placement with local anesthesia with 73cases with general anesthesia and found no statis-tical difference in placement failure (1.3% for thoseunder general anesthesia vs 8.7% for those underlocal anesthesia, P 5 .07) and no complications ineither group. However, the cost was 4-fold greaterin the group undergoing stent placement with gen-eral anesthesia ($30,060 vs $7700).
When attempting ureteral stent placement underlocal anesthesia, the authors recommend the useof lidocaine jelly and a flexible cystoscope forimproved patient tolerance. Patient consent shouldbe obtained for both procedures before beingsedated or undergoing anesthesia in the event thatthe first attemptatdecompression fails. Thismethodprevents delay in implementing a secondary proce-dure that may be time sensitive and life saving.
At the time of decompression, a kidney urineculture should be done. Given the risk of urosepsisafter decompression, patients should be observedin a monitored setting such as an intensive careunit. A Foley catheter is also recommended formaximum decompression of the urinary collectingsystem. After a 1- to 2-week course of culture-specific antibiotics, the patient can be scheduledfor definitive stone treatment.45
TREATMENT RESISTANCE/COMPLICATIONSInfection Stones
Patients with infection stones undergoing surgicalstone removal are at increased risk of adverseevents compared with those undergoing surgeryfor metabolic stones. Higher rates of infectiousand bleeding complications are likely related tobacterial colonization of the stones and chronicinflammation related to persistent infection. Thus,although one would expect similar rates of urinaryextravasation (7%), renal pelvis perforation (3%),colonic injury (0.2%–0.8%), and pleural injury(0%–3%) for all patients undergoing PCNL, thosewith infection stones are likely to experiencehigher rates of infectious and bleeding complica-tions than the following rates that are typicallyreported: bleeding (8%), blood transfusion (6%–17%), fever (11%–32%), and sepsis (0.3%–5%).78,79
Similarly, although complications for all comersundergoing SWL includes bacteriuria (8%–24%),
bacteremia (14%), sepsis (<1–3%), steinstrasse(3%), perinephric hematomas (20%–25%), symp-tomatic perinephric hematoma (<1%), and gastro-intestinal tract injury (2%), patients undergoingSWL for infection stones have even higher risksof these postoperative infectious adverseevents.80–83 Some have even shown that perform-ing SWL in the setting of a staghorn stone with apositive urine culture result and urinary obstructionincreases the risk of postoperative sepsis.83 Simi-larly, if an infection stone is treated ureteroscopi-cally either because a more invasive approachcould not be safely performed or because therewas low suspicion for infection stone at the timeof surgical planning, these patients are at higherrisk for postoperative infectious complicationsand especially sepsis related to increased intrare-nal pressures secondary to irrigation. Use of a ure-teral access sheath at the time of ureteroscopymay decrease intrarenal pressures and risks ofpostoperative systemic infection. Otherwise thesepatients are at similar risks to other patients under-going ureteroscopy for urolithiasis, including risksof bleeding (0.3%–2%), stricture (0.5%–3%), ure-teral perforation (0%–15%), extravasation (<1%),ureteral avulsion (<0.5%), and steinstrasse(rare).84 Open ANL is now rarely performed giventhe development and success of minimally inva-sive techniques and the morbidity related to thisprocedure, including the risk of serious complica-tions such as pneumothorax, pulmonary embo-lism, wound infection, acute tubular necrosis,rhabdomyolysis, hemorrhage, vascular injuries,and urinoma.53 Of the small series publishing theiroutcomes of robotic and laparoscopic ANL, re-ported complications include gross hematuriarequiring continuous bladder irrigation, bloodtransfusion, splenic injury necessitating splenec-tomy, and vascular fistula.54,56,85
Obstructive Pyelonephritis
Patients with obstructive pyelonephritis are at riskto develop urosepsis and its sequelae, includingacute kidney injury and death. Mortality rates forpatients with obstructive pyelonephritis and sepsisare reported at 9% for those undergoing surgicaldecompression and 19% for those withoutdecompression.12 Potential complications relatedto nephrostomy tube placement include bleeding,although severe bleeding requiring transfusion israre (1%–3%); liver, splenic, or pleural injury(0.1%–0.3%); and rarely colonic or small-bowelinjury.86,87 Ureteral stent placement can becomplicated by ureteral perforation and malposi-tion requiring another procedure for decompres-sion. In addition, ureteral stents can cause

Marien & Miller10
significant bother specifically related to urinarysymptoms. Quality of life has been shown to besuperior for patients with ureteral stones managedwith PCNTs than for those with ureteral stents.74,88
EVALUATION OF OUTCOMES AND LONG-TERM RECOMMENDATIONSInfection Stones
PCNL monotherapy stone free rates range from82% to 93%.50,89 Lower stone free rates havebeen reported with SWL and PCNL combinationtherapy ranging from 67% to 78% even whenPCNL is last.49,50 Lam and colleagues50 report astone free rate of 92% for renal stones less than500mm2 thatwere in a nondilated collecting systemtreated with SWL monotherapy in a series of 12 pa-tients. Stone free rates after open ANL are reportedto be high, ranging from 80% to 100%.90,91 Stonefree rates after pure laparoscopic ANL are reportedat 80% to 88%,85,92 whereas early experience withthe robotic-assisted laparoscopic approach reportsfairly low stone free rates at 29% to 33%.54,55
The presence of residual stone fragments in pa-tients with infection stones composed of struviteand/or calcium carbonate apatite significantly in-creases the risk of stone recurrence, with a 0%to 10% recurrence rate for those who are stonefree postoperatively versus 40% to 85% in thesetting of residual stone fragments.20,29 Patientswho are rendered stone free have a lower rate ofpostoperative UTI (38%) versus those with resid-ual fragments (64%).29
After surgery, preventative measures may behelpful including dietary modifications as previ-ously described in the nonpharmacologic sectionand urinary acidification and urease inhibitors asdescribed in the pharmacologic section of thisarticle. Sterilization of the urine with antibioticsmay help decrease stone recurrence, as persistentinfection is known to increase the risk of stonerecurrence. However, there is not much morethan anecdotal evidence of this approach in theliterature, and the best regimen in terms of antibi-otic selection, duration, and dosing is unknown.Antibiotic use in this setting can be even morecomplicated when stone and/or renal pelvic urinecultures resistance patterns show no oral options.For those patients with secondarily infected meta-bolic stones, a full metabolic workup with a24-hour urine study should be performed. Meta-bolic evaluation may also be beneficial in patientswith infection stones given the findings of a recentseries comparing postoperative stone events inpatients with struvite stones with and withoutmetabolic evaluation and directed medical ther-apy. In this series, 39 patients with pure and mixed
struvite stones who underwent metabolic evalua-tion and directed treatment had significantly lessstone events postoperatively compared with 17patients with pure struvite stones and no meta-bolic workup or management.93
Obstructive Pyelonephritis
Vahlensieck and colleagues14 reported on theirexperience with 57 patients treated for obstructivepyelonephritis during a 5-year period and foundthat 32% go on to have recurrent UTIs and 11%experience recurrent obstructive pyelonephritisover a 5-year follow-up period. For those patientswith recurrent UTIs and no obvious cause thatcan be definitively treated (ie, incomplete bladderemptying secondary to benign prostatic hypertro-phy), prophylactic antibiotics may be beneficial.Metabolic evaluation is recommended even inpatients with first-time stone formation who havea history of obstructive pyelonephritis given thepotential risk of sepsis with future stone events.
SUMMARY/DISCUSSIONInfection Stones
Infection stones are struvite and/or calcium car-bonate apatite in composition and occur as aresult of UTI with urease-producing bacteria. Sur-gery with the aim of complete stone removal is themainstay of treatment. PCNL is the treatment ofchoice for most patients with large infection stonesper AUA guidelines. In certain circumstances,other surgical approaches including combinationtherapy for SWL with PCNL, SWL monotherapy,ureteroscopy, and open and laparoscopic/roboticapproaches may be appropriate. A course of pre-operative antibiotics has been shown to decreasethe rate of SIRS/sepsis after PCNL. Nonsurgicalapproaches with dietary measures, urease inhibi-tors, and dissolution therapy may be useful ad-juncts to surgical intervention or as a primarytreatment of those who are medically unfit toundergo a surgical procedure.
Obstructive Pyelonephritis
Obstructing ureteral stones with concurrent UTI isa urologic emergency and requires immediatedecompression, broad-spectrum antibiotics, andclose monitoring for urosepsis. Obstructive pyelo-nephritis with sepsis without decompression has a19% mortality rate. PCNT and retrograde ureteralstenting are both adequate for decompression.Long-term interventions to prevent recurrent infec-tions and stones is useful given the high rate ofrecurrent UTIs and 10% risk of recurrent obstruc-tive pyelonephritis in these patients.

Treatment of the Infected Stone 11
REFERENCES
1. Knoll T, Schubert AB, Fahlenkamp D, et al. Urolithia-
sis through the ages: data on more than 200,000 uri-
nary stone analyses. J Urol 2011;185(4):1304–11.
2. Daudon M, Dore JC, Jungers P, et al. Changes in
stone composition according to age and gender of
patients: a multivariate epidemiological approach.
Urol Res 2004;32(3):241–7.
3. Choong S, Whitfield H. Biofilms and their role in in-
fections in urology. BJU Int 2000;86(8):935–41.
4. Rahman NU, Meng MV, Stoller ML. Infections and
urinary stone disease. Curr Pharm Des 2003;9(12):
975–81.
5. Hedelin H. Uropathogens and urinary tract concre-
tion formation and catheter encrustations. Int J Anti-
microb Agents 2002;19(6):484–7.
6. Bichler KH, Eipper E, Naber K, et al. Urinary infection
stones. Int J Antimicrob Agents 2002;19(6):488–98.
7. Schwartz BF, Stoller ML. Nonsurgical management
of infection-related renal calculi. Urol Clin North Am
1999;26(4):765–78, viii.
8. Koga S, Arakaki Y, Matsuoka M, et al. Staghorn
calculi – long-term results of management. Br J
Urol 1991;68(2):122–4.
9. de Cogain MR, Lieske JC, Vrtiska TJ, et al. Second-
arily infected nonstruvite urolithiasis: a prospective
evaluation. Urology 2014;84(6):1295–300.
10. Tavichakorntrakool R, Prasongwattana V,
Sungkeeree S, et al. Extensive characterizations of
bacteria isolated from catheterized urine and stone
matrices in patients with nephrolithiasis. Nephrol
Dial Transplant 2012;27(11):4125–30.
11. Yoshimura K, Utsunomiya N, Ichioka K, et al. Emer-
gency drainage for urosepsis associated with upper
urinary tract calculi. J Urol 2005;173(2):458–62.
12. Borofsky MS, Walter D, Shah O, et al. Surgical
decompression is associated with decreased mor-
tality in patients with sepsis and ureteral calculi.
J Urol 2013;189(3):946–51.
13. Yamamoto Y, Fujita K, Nakazawa S, et al. Clinical
characteristics and risk factors for septic shock in
patients receiving emergency drainage for acute py-
elonephritis with upper urinary tract calculi. BMC
Urol 2012;12:4.
14. Vahlensieck W, Friess D, Fabry W, et al. Long-term
results after acute therapy of obstructive pyelone-
phritis. Urol Int 2015;94(4):436–41.
15. Tambo M, Okegawa T, Shishido T, et al. Predictors of
septic shock in obstructive acute pyelonephritis.
World J Urol 2014;32(3):803–11.
16. Kamei J, Nishimatsu H, Nakagawa T, et al. Risk
factors for septic shock in acute obstructive pyelo-
nephritis requiring emergency drainage of the upper
urinary tract. Int Urol Nephrol 2014;46(3):493–7.
17. Angulo JC, Gaspar MJ, Rodriguez N, et al. The
value of C-reactive protein determination in patients
with renal colic to decide urgent urinary diversion.
Urology 2010;76(2):301–6.
18. Carnell J, Fischer J, Nagdev A. Ultrasound detection
of obstructive pyelonephritis due to urolithiasis in the
ED. Am J Emerg Med 2011;29(7):843.e1–3.
19. Watkins S, Bowra J, Sharma P, et al. Validation of
emergency physician ultrasound in diagnosing hy-
dronephrosis in ureteric colic. Emerg Med Australas
2007;19(3):188–95.
20. Flannigan R, Choy WH, Chew B, et al. Renal struvite
stones-pathogenesis, microbiology, and manage-
ment strategies. Nat Rev Urol 2014;11(6):333–41.
21. Hesse A, Heimbach D. Causes of phosphate stone
formation and the importance of metaphylaxis by
urinary acidification: a review. World J Urol 1999;
17(5):308–15.
22. Jacobs D, Heimbach D, Hesse A. Chemolysis of
struvite stones by acidification of artificial urine –
an in vitro study. Scand J Urol Nephrol 2001;35(5):
345–9.
23. Jarrar K, Boedeker RH, Weidner W. Struvite stones:
long-term follow up under metaphylaxis. Ann Urol
1996;30(3):112–7.
24. Bernardo NO, Smith AD. Chemolysis of urinary
calculi. Urol Clin North Am 2000;27(2):355–65.
25. Martelli A, Buli P, Cortecchia V. Urease inhibitor
therapy in infected renal stones. Eur Urol 1981;
7(5):291–3.
26. Griffith DP, Khonsari F, Skurnick JH, et al.
A randomized trial of acetohydroxamic acid for the
treatment and prevention of infection-induced uri-
nary stones in spinal cord injury patients. J Urol
1988;140(2):318–24.
27. Griffith DP, Gleeson MJ, Lee H, et al. Randomized,
double-blind trial of Lithostat (acetohydroxamic
acid) in the palliative treatment of infection-induced
urinary calculi. Eur Urol 1991;20(3):243–7.
28. Williams JJ, Rodman JS, Peterson CM.
A randomized double-blind study of acetohydroxa-
mic acid in struvite nephrolithiasis. N Engl J Med
1984;311(12):760–4.
29. Iqbal MW, Youssef R, Neisius A, et al. Contemporary
management of struvite stones using combined en-
dourological and medical treatment: predictors of
unfavorable clinical outcome. J Endourol 2013.
[Epub ahead of print].
30. Pearle MS, Goldfarb DS, Assimos DG, et al. Medical
management of kidney stones: AUA guideline.
J Urol 2014;192(2):316–24.
31. Preminger GM, Assimos DG, Lingeman JE, et al.
Chapter 1: AUA guideline on management of stag-
horn calculi: diagnosis and treatment recommenda-
tions. J Urol 2005;173(6):1991–2000.
32. Kachrilas S, Papatsoris A, Bach C, et al. The current
role of percutaneous chemolysis in the management
of urolithiasis: review and results. Urolithiasis 2013;
41(4):323–6.

Marien & Miller12
33. Angermeier K, Streem SB, Yost A. Simplified infusion
method for 10% hemiacidrin irrigation of renal pelvis.
Urology 1993;41(3):243–6.
34. Gonzalez RD, Whiting BM, Canales BK. The history
of kidney stone dissolution therapy: 50 years of opti-
mism and frustration with Renacidin. J Endourol
2012;26(2):110–8.
35. Mulvaney WP, Henning DC. Solvent treatment of uri-
nary calculi: refinements in technique. J Urol 1962;
88:145–9.
36. Griffith DP, Bragin S, Musher DM. Dissolution of stru-
vite urinary stones. Experimental studies in vitro.
Invest Urol 1976;13(5):351–3.
37. Griffith DP, Moskowitz PA, Carlton CE Jr. Adjunctive
chemotherapy of infection-induced staghorn calculi.
J Urol 1979;121(6):711–5.
38. Bichler KH, Eipper E, Naber K. Infection-induced
urinary stones. Urologe A 2003;42(1):47–55 [in
German].
39. GoettschW, vanPeltW,NagelkerkeN, et al. Increasing
resistance to fluoroquinolones in Escherichia coli from
urinary tract infections in theNetherlands. JAntimicrob
Chemother 2000;46(2):223–8.
40. Cullen IM, Manecksha RP, McCullagh E, et al. An 11-
year analysis of the prevalent uropathogens and the
changing pattern of Escherichia coli antibiotic resis-
tance in 38,530 community urinary tract infections,
Dublin 1999–2009. Ir J Med Sci 2013;182(1):81–9.
41. Cullen IM, Manecksha RP, McCullagh E, et al. The
changing pattern of antimicrobial resistance within
42,033 Escherichia coli isolates from nosocomial,
community and urology patient-specific urinary tract
infections, Dublin, 1999–2009. BJU Int 2012;109(8):
1198–206.
42. Karlowsky JA, Kelly LJ, Thornsberry C, et al. Trends
in antimicrobial resistance among urinary tract infec-
tion isolates of Escherichia coli from female outpa-
tients in the United States. Antimicrob Agents
Chemother 2002;46(8):2540–5.
43. MacFadden DR, Ridgway JP, Robicsek A, et al. Pre-
dictive utility of prior positive urine cultures. Clin
Infect Dis 2014;59(9):1265–71.
44. Marien T, Mass AY, Shah O. Antimicrobial resistance
patterns in cases of obstructive pyelonephritis sec-
ondary to stones. Urology 2015;85(1):64–8.
45. Nicolle LE. A practical guide to the management of
complicated urinary tract infection. Drugs 1997;
53(4):583–92.
46. Shorr E, Carter AC. Aluminum gels in the manage-
ment of renal phosphatic calculi. J Am Med Assoc
1950;144(18):1549–56.
47. Lavengood RW Jr, Marshall VF. The prevention of
renal phosphatic calculi in the presence of infection
by the Shorr regimen. J Urol 1972;108(3):368–71.
48. Lotz M, Zisman E, Bartter FC. Evidence for a
phosphorus-depletion syndrome in man. N Engl J
Med 1968;278(8):409–15.
49. Merhej S, Jabbour M, Samaha E, et al. Treatment of
staghorn calculi by percutaneous nephrolithotomy
and SWL: the Hotel Dieu de France experience.
J Endourol 1998;12(1):5–8.
50. Lam HS, Lingeman JE, Barron M, et al. Staghorn
calculi - analysis of treatment results between initial
percutaneous nephrostolithotomy and extracorpo-
real shock-wave lithotripsy monotherapy with refer-
ence to surface-area. J Urol 1992;147(5):1219–25.
51. Healy KA, Ogan K. Pathophysiology and manage-
ment of infectious staghorn calculi. Urol Clin North
Am 2007;34(3):363.
52. Bove AM, Altobelli E, Buscarini M. Indication to open
anatrophic nephrolithotomy in the twenty-first cen-
tury: a case report. Case Rep Urol 2012;2012:
851020.
53. Assimos DG. Anatrophic nephrolithotomy. Urology
2001;57(1):161–5.
54. King SA, Klaassen Z, Madi R. Robot-assisted ana-
trophic nephrolithotomy: Description of technique
and early results. J Endourol 2014;28(3):325–9.
55. Ghani KR, Rogers CG, Sood A, et al. Robot-assisted
anatrophic nephrolithotomy with renal hypothermia
for managing staghorn calculi. J Endourol 2013;
27(11):1393–8.
56. Giedelman C, Arriaga J, Carmona O, et al. Laparo-
scopic anatrophic nephrolithotomy: developments
of the technique in the era of minimally invasive sur-
gery. J Endourol 2012;26(5):444–50.
57. Simforoosh N, Aminsharifi A, Tabibi A, et al. Laparo-
scopic anatrophic nephrolithotomy for managing
large staghorn calculi. BJU Int 2008;101(10):1293–6.
58. Elbahnasy AM, Elbendary MA, Radwan MA, et al.
Laparoscopic pyelolithotomy in selected patients
with ectopic pelvic kidney: a feasible minimally inva-
sive treatment option. J Endourol 2011;25(6):985–9.
59. Marguet CG, Springhart WP, Tan YH, et al. Simulta-
neous combined use of flexible ureteroscopy and
percutaneous nephrolithotomy to reduce the num-
ber of access tracts in the management of complex
renal calculi. BJU Int 2005;96(7):1097–100.
60. Landman J, Venkatesh R, Lee DI, et al. Combined
percutaneous and retrograde approach to staghorn
calculi with application of the ureteral access sheath
to facilitate percutaneous nephrolithotomy. J Urol
2003;169(1):64–7.
61. Hamamoto S, Yasui T, Koiwa S, et al. Successful re-
sults of endoscopic combined intrarenal surgery
against large calculi; simultaneous use of flexible
ureteroscopy and mini-percutaneous nephrolithot-
omy overcame the drawbacks of the monotherapy
of percutaneous nephrolithotomy. J Urol 2013;
189(4):E626–7.
62. Segura JW, Patterson DE, Leroy AJ. Combined
percutaneous ultrasonic lithotripsy and extracorpo-
real shock-wave lithotripsy for struvite staghorn
calculi. World J Urol 1987;5(4):245–7.

Treatment of the Infected Stone 13
63. Rodrigues Netto N Jr, Lemos GC, Palma PC, et al.
Staghorn calculi: percutaneous versus anatrophic
nephrolithotomy. Eur Urol 1988;15(1–2):9–12.
64. Benson AD, Juliano TM, Miller NL. Infectious out-
comes of nephrostomy drainage before percuta-
neous nephrolithotomy compared to concurrent
access. J Urol 2014;192(3):770–4.
65. Eswara JR, Lee H, Dretler SP, et al. The effect of de-
layed percutaneous nephrolithotomy on the risk of
bacteremia and sepsis in patients with neuromus-
cular disorders. World J Urol 2013;31(6):1611–5.
66. Mariappan P, Smith G, Bariol SV, et al. Stone and
pelvic urine culture and sensitivity are better than
bladder urine as predictors of urosepsis following
percutaneous nephrolithotomy: A prospective clin-
ical study. J Urol 2005;173(5):1610–4.
67. Wolf JS, Bennett CJ, Dmochowski RR, et al. Best
practice policy statement on urologic surgery antimi-
crobial prophylaxis. J Urol 2008;179(4):1379–90.
68. Bag S, Kumar S, Taneja N, et al. One week of nitro-
furantoin before percutaneous nephrolithotomy
significantly reduces upper tract infection and uro-
sepsis: a prospective controlled study. Urology
2011;77(1):45–9.
69. Mariappan P, Smith G, Moussa SA, et al. One week
of ciprofloxacin before percutaneous nephrolithot-
omy significantly reduces upper tract infection and
urosepsis: a prospective controlled study. BJU Int
2006;98(5):1075–9.
70. Eswara JR, Sharif-Tabrizi A, Sacco D. Positive stone
culture is associated with a higher rate of sepsis af-
ter endourological procedures. Urolithiasis 2013;
41(5):411–4.
71. Margel D, Ehrlich Y, Brown N, et al. Clinical implica-
tion of routine stone culture in percutaneous nephro-
lithotomy - a prospective study. Urology 2006;67(1):
26–9.
72. Klein LA, Koyle M, Berg S. The emergency manage-
ment of patients with ureteral calculi and fever. J Urol
1983;129(5):938–40.
73. Pearle MS, Pierce HL, Miller GL, et al. Optimal
method of urgent decompression of the collecting
system for obstruction and infection due to ureteral
calculi. J Urol 1998;160(4):1260–4.
74. Mokhmalji H, Braun PM, Martinez Portillo FJ, et al.
Percutaneous nephrostomy versus ureteral stents
for diversion of hydronephrosis caused by stones:
a prospective, randomized clinical trial. J Urol
2001;165(4):1088–92.
75. Sivalingam S, Tamm-Daniels I, Nakada SY. Office-
based ureteral stent placement under local anes-
thesia for obstructing stones is safe and efficacious.
Urology 2013;81(3):498–502.
76. McFarlane JP, Cowan C, Holt SJ, et al. Outpatient
ureteric procedures: a new method for retrograde
ureteropyelography and ureteric stent placement.
BJU Int 2001;87(3):172–6.
77. Adeyoju AB, Collins GN, Brooman P, et al. Outpa-
tient flexible cystoscope-assisted insertion of
ureteric catheters and ureteric stents. BJU Int
1999;83(7):748–50.
78. Michel MS, Trojan L, Rassweiler JJ. Complications in
percutaneous nephrolithotomy. Eur Urol 2007;51(4):
899–906.
79. de la Rosette J, Assimos D, Desai M, et al. The clin-
ical research office of the endourological society
percutaneous nephrolithotomy global study: indica-
tions, complications, and outcomes in 5803 patients.
J Endourol 2011;25(1):11–7.
80. D’Addessi A, Vittori M, Racioppi M, et al. Complica-
tions of extracorporeal shock wave lithotripsy for uri-
nary stones: to know and to manage them – a
review. ScientificWorldJournal 2012;2012:619820.
81. Wazir BG, Iftikhar ul Haq M, Faheem ul H, et al.
Experience of extracorporeal shockwave lithotripsy
for kidney and upper ureteric stones by electromag-
netic lithotriptor. J Ayub Med Coll Abbottabad 2010;
22(2):20–2.
82. Razvi H, Fuller A, Nott L, et al. Risk factors for peri-
nephric hematoma formation after shockwave litho-
tripsy: a matched case-control analysis. J Endourol
2012;26(11):1478–82.
83. Skolarikos A, Alivizatos G, de la Rosette J. Extracor-
poreal shock wave lithotripsy 25 years later: compli-
cations and their prevention. Eur Urol 2006;50(5):
981–90.
84. D’Addessi A, Bassi P. Ureterorenoscopy: avoiding
and managing the complications. Urol Int 2011;
87(3):251–9.
85. Aminsharifi A, Hadian P, Boveiri K. Laparoscopic
anatrophic nephrolithotomy for management of
complete staghorn renal stone: clinical efficacy
and intermediate-term functional outcome.
J Endourol 2013;27(5):573–8.
86. Uppot RN. Emergent nephrostomy tube placement
for acute urinary obstruction. Tech Vasc Interv Ra-
diol 2009;12(2):154–61.
87. Winer AG, Hyams ES, Shah O. Small bowel injury
during percutaneous nephrostomy tube placement
causing small bowel obstruction. Can J Urol 2009;
16(6):4950–2.
88. Joshi HB, Okeke A, Newns N, et al. Characterization
of urinary symptoms in patients with ureteral stents.
Urology 2002;59(4):511–6.
89. Desai M, Jain P, Ganpule A, et al. Developments in
technique and technology: the effect on the results
of percutaneous nephrolithotomy for staghorn
calculi. BJU Int 2009;104(4):542–8.
90. Assimos DG, Wrenn JJ, Harrison LH, et al.
A comparison of anatrophic nephrolithotomy and
percutaneous nephrolithotomy with and without
extracorporeal shock wave lithotripsy for manage-
ment of patients with staghorn calculi. J Urol 1991;
145(4):710–4.

Marien & Miller14
91. Morey AF, Nitahara KS, McAninch JW. Modified ana-
trophic nephrolithotomy for management of stag-
horn calculi: is renal function preserved? J Urol
1999;162(3 Pt 1):670–3.
92. Simforoosh N, Radfar MH, Nouralizadeh A, et al.
Laparoscopic anatrophic nephrolithotomy for
management of staghorn renal calculi.
J Laparoendosc Adv Surg Tech A 2013;23(4):
306–10.
93. Kaplan A, Shin R, Iqbal M, et al. Patients with struvite
stones. SESAUA presentation. Savannah (GA),
March 19, 2015.